spinal cord monitoring: somatosensory- and motor-evoked potentials
TRANSCRIPT

MONITORING DURING CRITICAL EVENTS 0889-8537/01 $16.00 + .00
SPINAL CORD MONITORING:SOMATOSENSORY- AND MOTOR
EVOKED POTENTIALS
Peter de Haan, MD, PhD, and Cor J. Kalkman, MD, PhD
Several surgical procedures are associated with a definite risk ofspinal cord injury. The incidence of lower limb neurologic deficits varieswidely between procedures. After elective abdominal aortic aneurysmsurgery, the incidence of lower extremity neurologic deficits is 0.16% to0.25%.25, 50 After repair for coarctation of the aorta, the incidence ofparaplegia is 0.4% to 1.5%.2,41 In contrast, Svensson et al63 found that theoverall incidence of neurologic deficits was 16% in 1509 patients whohad undergone repair for the treatment of thoracoabdominal aortic aneurysms.v In another large series of patients with thoracoabdominal aorticaneurysms, distributed equally between aneurysm types I to IV, thelong-term survivors (> 30 days) had a 4.4% incidence of paraplegia anda 5% incidence of paraparesis.' Repair of aneurysms confined to thedescending thoracic aorta resulted in paraplegia and paraparesis in6.5% of the patients." The incidence of neurologic complications aftercorrection of scoliosis with spinal instrumentation ranges between 0.4%and 1.6%,7,51
This article addresses spinal cord function monitoring with evokedpotentials in the operating room. The aim of spinal cord function monitoring is threefold: to detect spinal cord dysfunction early to applycorrective measures before irreversible damage occurs, to assess theefficacy of protective strategies, and to acquire knowledge of the pathophysiologic processes involved to improve subsequent procedures. Spinal cord damage can result from ischemia, disruption, compression,
From the Department of Anesthesiology, Onze Lieve Vrouwe Gasthuis, Amsterdam (PdH);and the Department of Anesthesiology, University Medical Center, Utrecht, The Netherlands (CJK)
ANESTHESIOLOGY CLINICS OF NORTH AMERICA
VOLUME 19 • NUMBER 4 • DECEMBER2001 923

924 DE HAAN & KALKMAN
concussion, and distraction. Each of these insults gives rise to functionalalterations that may be neurophysiologically evident, suggesting thepotential usefulness of evoked potential monitoring. Monitoring spinalcord function during procedures with a risk for spinal cord injury isbelieved to improve outcome. For example, a large, multicenter surveyreveals that experienced spinal cord monitoring teams have fewer thanhalf as many neurologic deficits per 100 cases after scoliosis surgery thanteams with little monitoring experience." The evidence that monitoringactually improves outcome, however, has not been established conclusively in prospective, randomized clinical trials. Despite this limitation,monitoring the spinal cord with evoked potentials has gained widespread acceptance; based on the response to corrective measures, oneassumes that monitoring spinal cord function is beneficial.
The type, intensity, duration, and location (gray or white matter, orthoracic or lumbar cord) of the imminent injury influences the extent ofdamage (confined to a small area of the spinal cord or gray and whitematter infarction over several segments). Therefore, the part of thespinal cord at risk should be monitored. For example, the anterior hommotoneuronal system is believed to be most vulnerable to ischemia, andoften primarily is affected after an interruption of spinal cord bloodflow," A monitoring modality should assess anterior hom motor function if ischemic damage is anticipated. If the involved pathophysiologicprocess is compression or. distraction, white and gray matter are probably equally vulnerable.
Somatosensory-evoked potentials (SSEPs) and motor unit evokedpotentials (motor EPs) are distinct modalities to monitor the spinal cord.SSEPs reflect axonal conduction in the ascending sensory tracts in theposterior columns. Motor EPs monitor the descending motor systemlocated in the anterior and lateral corticospinal tracts and the anteriorhom motoneuronal system, including the function of the ischemia sensitive ex motor neurons. The different conductive pathways of SSEPs andmotor EPs result in different characteristics of SSEPs and motor EPs asindicators of spinal cord function, with respect to response time to spinalcord ischemia, false-positive and false-negative results, and potentialbenefits and inherent limitations during scoliosis surgery and aorticrepair. In this article, the techniques of SSEP and motor EP monitoringare described, and anesthetic and other nonsurgical influences on evokedpotentials are provided. The use and limitations of SSEPs and motorEPs during aortic repair and spinal surgery are discussed. Monitoringtechniques only improve outcome when protective strategies are readilyavailable. Several possible spinal cord protective measures also are described.
SOMATOSENSORY-EVOKED POTENTIALS
Acqulsltlon
Monitoring SSEPs is a noninvasive technique that can be appliedreadily in the operating room. SSEPs are the electrical response of the

SPINAL CORD MONITORIl'\G 925
eNS, resulting from stimulation of a peripheral nerve. An intact conducting pathway between the sites of stimulation and recording is requiredfor SSEPs to be monitored. SSEPs are transmitted ma inly by.the sensorytracts of the dorsal columns. SSEPs representing the ascending volley canbe recorded along the pathway from the nerve, spinal cord, subcorticalstructures, and the cerebral cortex. Figure 1 is an example of a corticalSSEP. To elicit cortical SSEPs for intraoperative monitoring, lower limbperipheral nerves are stimulated electrically with brief pulses. Electricalstimuli used to elicit SSEPs are square wave pulses with short duration(10G-200·f.Lsec). A constant current stimulator ensures constant stimulusdelivery, even when electrode impedance changes over time . Stimulusintensity should be at least 20 milliamps to obtain a supramaximalresponse. Stimulation electrodes can be subcutaneous needle electrodesor standard electroencephalographic (EEG) electrodes. The signal istransmitted by way of the dorsal columns and, to a lesser extent, byway of the anterolateral tracts, and can be recorded from the scalp(cortical and subcortical SSEPs) with silver-silver chloride surface electrodes filled with electrode jelly.: Electrode impedance should be keptless than 2 kf], SSEPs also can be recorded invasively from electrodesplaced in the epidural space of the high thoracic or cervical cord. A
Somatosensory
cortex ---------.... ~fiS;:::==1
Dorsalcolumns
Dorsalsensoryganglion
Posteriortibial nerve
Cortical SSEP
Constant currentstimulator
Figure 1. Cortical somatosensory- evoked potential (EP). Constant current stimulat ion ofthe posterior tibial nerves at the ankle with recording of the responses from the somatosensory cortex.

926 DE HAAN & KALKMAN
typical SSEP has an amplitude of 1 to 3 fLV. SSEPs from the CNS have asmaller amplitude than the combined noise of other biologic signals andnoise generated by electrical equipment in the operating room. Signalaveraging techniques are necessary to extract the response from thebackground noise. The principle of averaging relies on the fact thatthe signal of interest can be time-locked to the stimulus, whereas thebackground noise is random. At least 100 stimuli must be averaged toobtain a reproducible cortical-evoked potential. In most centers, a stimulus rate between 3.1 and 5 Hz is used during spinal cord SSEP monitoring. Cortical SSEPs show a progressive decline in amplitude with increasing stimulus rates above 5 Hz. Various artifacts may be present inthe SSEP response. Artifacts that originate outside the patient includeline-frequency interference, artifacts caused by the use of diathermy(electrocautery), and other electrical apparatus connected to the patient.Measures to prevent these artifacts include the proper electrode preparation, grounding, and positioning of other electronic equipment. Contamination of the SSEP waveform by diathermy may be prevented by automatic interruption of the averaging process immediately beforeactivation of the diathermy generator." Muscle activity disturbing theSSEP can be eliminated by the use of muscle relaxants.
Influence of Anesthetic Agents andPhysiologic Factors
The effect of anesthetic agents may be indistinguishable from progressive spinal cord dysfunction (i.e., an increase in latency with asimultaneous decrease in amplitude). One must be aware of the effectsof the various anesthetic drugs on the ' SSEP to optimize the signalstrength. Changes in the level of anesthesia should be avoided to minimize variability. Preferably, anesthetics should be given as continuousinfusion or low concentrations of inhaled agents. Volatile anestheticagents, such as halothane, enflurane, and isoflurane, produce markeddose-dependent depression of SSEP amplitude and prolongation of thelatency," Subcortical and spinal potentials are less sensitive to depressionby volatile anesthetics than cortical potentials. Although data regardingSSEP monitoring during sevoflurane anesthesia are limited, recent evidence suggests that sevoflurane is compatible with SSEPS.24 Nitrousoxide decreases SSEP amplitude by 50% without affecting latency." Theopioid analgesic drugs, such as fentanyl and morphine, produce onlyminimal amplitude depression and latency prolongation.P-" The intravenous anesthetic drugs (i.e., barbiturates, benzodiazepines, propofol, ketamine) have only minor effects on SSEP amplitude, whereas etomidateincreases SSEP amplitude. Anesthetic techniques compatible with reproducible SSEPs are propofol/opioid, ketamine/opioid, or benzodiazepine/opioid. Nitrous oxide can be added as a background anesthetic inconcentrations below 50%. Avoidance of volatile anesthetics and nitrousoxide increases SSEP amplitude and reduces variability. For example,

SPINALCORDMONITOIill\'G 927
propofol/sufentanil anesthesia produces higher SSEP amplitudes thannitrous oxide/sufentanil anesthesia."
Hypothermia reduces conduction velocity in peripheral nerves andincreases synaptic delay. The SSEP latency increases linearly with decreasing temperatures, whereas the amplitude of the cortical SSEP isunchanged with moderate hypothermia/"
Spinal cord blood flow is autoregulated between 50 and 120 rnmHg mean arterial blood pressure.P Controlled hypotension to a meanarterial pressure of 60 mm Hg, in itself, does not change SSEP. Whenspinal cord blood flow is already compromised as a result of distraction,compression, or ligation of segmental arteries feeding the spinal cord,however, the effect of hypotension becomes addictive. Changes in endtidal Pco, between 20 and 50 rnm Hg do not alter cortical SSEPs significantly."
Clinical Application
When spinal cord function is impaired intraoperatively, there isusually an increase in latency, paralleled by a decrease in amplitude. Onempiric grounds, an increase in the latency to the first positive peak (PI)of more than 10% or a decrease in cortical PINI peak-to-peak amplitudeof more than 50% is considered a reason for intervention.v'" No prospective studies have been performed to assess the validity of the criteriaused for intervention. In some early studies, however, no protectivemeasures were taken after recognition of SSEP changes; these changesreliably predicted lower limb neurologic deficits." Spontaneous amplitude variability of the cortical posterior tibial nerve SSEp, however, is ashigh as 40% to 50%:" In the individual patient, variability can be reducedby using a supramaximal stimulus intensity, by a proper anestheticregime, and by high pass filtering to remove frequencies below 30HZ.33 In a recent series of patients undergoing thoracoabdominal aorticaneurysm surgery, a gradual and progressive SSEP amplitude decreaseto 50% of baseline was observed in 40% of patients." SSEP latencies didnot accompany amplitude changes. None of these patients experiencedlower limb neurologic deficits. Exhaustion of the peripheral nerve excitability, hypothermia, or anesthetic effects might explain this phenomenon.
MOTOR-EVOKED POTENTIALS
Modalities to Monitor Motor-Evoked Potentials
Motor EPs can be elicited by electrical or magnetic transcranialstimulation. Transcranial stimulation has not been approved by the Foodand Drug Administration. Another option to elicited motor EPs is theelectrical stimulation of descending motor tracts at the level of the

928 DE HAAN & KALKMAN
cervical or high thoracic spinal cord with an epidural wire electrode orneedle electrodes. Responses can be recorded from the epidural spaceover the lower lumbar spinal cord (epidural motor EPs), the peripheralnerve (neurogenic motor EPs), or from limb muscles as compoundmuscle action potentials using standard electromyographic (EMG) techniques (myogenic motor EPs) (Fig. 2). Magnetic transcranial stimulationhas the disadvantage over electrical transcranial stimulation in thatcontinuous access to the head is required and small displacements ofthe magnet result in amplitude variability.
Myogenic Motor-Evoked Potentials
Recording of myogenic motor EPs is believed to be exclusivelyspecific for motor tract conduction, including the ischemia sensitiveanterior hom ex motor neurons. Myogenic motor EPs can be elicited bytranscranial or spinal cord stimulation. The limitation of the myogenicmotor EPs after spinal cord stimulation is that invasive electrode placement is required. The muscle response also might be elicited partly by
electrical stimulator
Epidural Motor EP
Myogenic Motor EP
50
-ili%o 100
Neurogenic Motor EP
~5PvI
transcranial stimulationfowerlimbmotor cortex
corticospinaltract _-I-_~
a - motorneuron
peripheralnerve ---il.-
anterior tibialmuscle --~~
Figure 2. The sites used for recording motor EPs and accompanying terminology. Aftertranscranial electrical stimulation the motor cortex is activated. The signal travels along thecorticospinal tract and activates the anterior horn motor neuron.

SPINALCORD MONITORI!'\G 929
antidromic sensory conduction. As a consequence, this modality is notentirely specific for the spinal cord motoneuronal system. The authors'group used recording of myogenic responses after electrical transcranialstimulation (myogenic motor EPs). This modality can detect spinal cordischemia within minutes."
Epidural Motor-Evoked Potentials
The epidural recording of motor EPs after electrical transcranialstimulation from the lower lumbar spinal cord is characterized by aninitial direct (D) wave followed by a series of indirect waves. The 0wave is the result of direct activation of pyramidal cells in the motorcortex and is resistant to anesthetics. Muscle relaxants do not interferewith epidural motor EP recording. The main disadvantage of this technique is that only conduction in the corticospinal tracts is monitored,and axonal conduction is resistant to ischemia." No information isprovided on function of the anterior hom gray matter. Epidural motorEPs disappear slowly after interruption of spinal cord blood flow.to. 21. 56
After experimental aortic occlusion in the rabbit, myogenic responsesto transcranial stimulation disappeared within 2 minutes, whereas theepidural recordings required 11 minutes to decrease 50% in amplitude."In two studies describing a model of spinal cord ischemia in the dog,epidural responses to transcranial stimulation disappeared in 21 ± 6.6minutes and 24 ± 4 minutes, respectlvely.v- " The observed time between onset and detection of spinal cord ischemia with epidural motorEPs is too long to allow prompt interventions during aortic surgery.When epidural motor EPs are elicited secondary to spinal cord stimulation at a cervical or high thoracic level·(in the literature, also describedas spinal cord-evoked potential or spinal-evokedpotential), there is noanesthetic interference. Using this technique, however, the motor tractsare not monitored exclusively because ascending and descending tractsare activated. The spinal response consists of mixed sensory and motorsignals. Conflicting results with this technique were described. Ischemicspinal cord dysfunction could be detected in 11 to 17 minutes afteraortic occlusion in dogs.'? After progressive ligation of intercostal arteries(including the Adamkiewicz artery) in the dog, epidural recordingsremained unchanged."
Neurogenic Motor-Evoked Potentials
The peripheral nerve response (recorded from the sciatic nerve) tospinal cord stimulation is small (-1 IJ.V). It is necessary to average atleast 100 responses to obtain a reproducible signal. Although the neurogenic motor EP after spinal cord stimulation is insensitive to anestheticinterference, this modality is not entirely specific for the motor tractsbecause it contains components produced by antidromic conduction insensory tracts. Spinally elicited peripheral nerve responses are sensoryrather than motor/" Deficits confined to the motor tracts might not be

930 DE HAAN & KALKMAN
detected using neurogenic motor EPs. Monitoring neurogenic motor EPsafter transcranial stimulation is not clinically feasible because of thelarge number of transcranial stimuli that must be averaged.
Application of Myogenic Motor-Evoked Potentials afterTranscranial Electrical Stimulation
Transcranial Stimulation
The motor EPs can be evoked by applying stimuli to the scalp byway of (9-mm silver EEG disc) electrodes or adhesive gel Ag/AgClelectrodes. The use of a circumferential cathode of interconnected EEGelectrodes improves stimulus efficiency and increases response amplitude." The anode can be placed at Cz, and three interconnected cathodesare placed at Fpz, AI, and A2 (international 10-20 system). The problemof amplitude variability of myogenic motor EPs can be overcome furtherby using multipulse transcranial stimulation paradigms. Each stimulushas a duration of 50 usee, If multiple stimuli are applied with aninterstimulus interval of 2 to 3 ms, temporal summation of the excitatorypostsynaptic potential substantially amplifies myogenic responses andreduces variability." Multipulse transcranial stimulators providing atrain of up to 10 successive stimuli are commercially available.
Muscle Action Potential Recording
Compound muscle action potentials can be recorded from the skinover the left and right anterior tibial muscles and from the skin over theleft and right thenar muscles by using adhesive gel Ag/AgCl electrodes.The signals must be filtered between 30 and 1500 Hz. A stimulusintensity that produces maximal motor EP amplitude should be used.Single sweep responses are obtained after each multipulse stimulustrain, and signal averaging is not necessary. When imminent injury isconfined to the thoracic or lumbar cord and the lower limb motor EPamplitude is decreased, the thenar muscles can be used to distinguishbetween spinal cord ischemia and systemic factors or technical problems.
Influence of Anesthetic Agents
Many commonly used anesthetics, especially the volatile agents,readily depress myogenic responses." Anesthetics not only decrease theexcitability of cortical motor neurons but also depress spinal cord motorneuron excitability. Complete neuromuscular blockade is not compatiblewith myogenic motor EP monitoring, and if neuromuscular blockers areavoided, patient movement might be disturbing. Careful planning andadjustment of the anesthetic technique are necessary. Etomidate, ketamine, and opioids hardly depress myogenic motor EP amplitudes.w "Because motor EP amplitude also is influenced by the level of neuromus-

SPlJ'JALCORD MONITORING 931
cular blockade, a stable level of neuromuscular blockade should bemaintained. Using a closed-loop vecuronium infusion, the authors couldmaintain the level of neuromuscular blockade within a narrow rangeand minimize the influence of fluctuations in relaxation levels on thevariability of the motor EP signapo. 28. 62
Peripheral Ischemia
Evoked potential techniques that rely on stimulation and recordingfrom nerves and muscles in the leg lose their predictive values whenlower limb ischemia occurs during aortic surgery, especially when simple aortic cross-clamping without distal aortic perfusion is used. Ischemia of the peripheral nerve and muscle results in loss of myogenic motorresponses (and SSEPs) approximately 30 minutes after discontinuation oflimb perfusion. When distal aortic perfusion is used, at least one leg isperfused normally, but peripheral ischemia may occur in the leg usedfor femoral artery cannulation. This limitation can be overcome, andreliability of the myogenic motor EPs increased by inserting a secondcannula to perfuse the periphery of the femoral artery used for distalaortic perfusion."
Hypothermia
Hypothermia might influence motor EP signals and ischemia detection time. In a porcine model of spinal cord ischemia, however, clampingof critical lumbar arteries during moderate hypothermia (28°C) did notaffect the time necessary to detect ischemic spinal cord dysfunctionwith motor EPs, compared with normothermia." In the pig, progressivecooling resulted in a motor EP amplitude increase to 30°C, and wasfollowed by a progressive decrease." Response amplitudes decreasedbelow 25% at 14.0°C. Motor EP latencies increased linearly with decreasing temperatures."
Nonanesthetics
The use of magnesium for priming the bypass circuit completelyabolishes the motor EP by potentiation of neuromuscular blockade.Some agents used to decrease blood pressure depress motor EP amplitude (e.g., u2-receptor antagonists and ketanserin), whereas the 13-receptor antagonists-labetalol, sodium nitroprusside, and nitroglycerine--donot affect motor EP amplitude and latency (unpublished data).
With the multipulse stimulation paradigm, a circumferential cathode, a ketamine-hlgh-dose opioid-based anesthesia, and a continuouslevel of neuromuscular blockade, the median amplitude recorded fromthe tibial anterior muscle is 600 f.1V with a coefficient of variation of26%.10 This level of reproducibility allows continuous monitoring ofanterior hom function.

932 DE HAAN & KALKMAN
MONITORING DURING SPINAL SURGERY
Significant risk factors for major intraoperative neurologic deficitsinclude combined anterior and posterior surgery, severe rigid curves,pre-existing neurologic impairment, and hyperkyphosis. Intraoperativeawakening to test voluntary motor function during scoliosis surgery isprobably the gold standard for detecting motor deficits. This techniquehas several limitations, however. A cooperative patient is required., Asignificant time may elapse between a potentially dangerous surgicalmanipulation and the ability of an anesthesiologist to awaken the patientfrom anesthesia enough to be examined. The test provides only a snapshot of motor function. At time of the wake-up test, an irreversibleinjury of the spinal cord already may have occurred.
Somatosensory-Evoked Potentials
Several reports on the use of SSEPs during various spinal procedures have been published during the last 2 decades. Cortical andepidural SSEPs seem to be sensitive to changes in spinal cord functionduring spinal surgery. In a large, multicenter. survey, the negative predictive value of SSEPs was 99.93%.51 This sensitivity can be explainedby the fact that spinal cord damage caused by distraction and rotationand compression results from diffuse damage involving the anterior andposterior spinal cord. False-negative monitoring results with SSEPs canbe attributed to focal anterior lesions or by delayed pathologies. In theseries of over 50,000 procedures described by Nuwer et al," the overallincidence of neurologic deficits was 0.55%: The years of experience withSSEP monitoring of the team was one of the factors affecting outcome.Teams with the least experience had an incidence of neurologic deficitsof 1.04%, as opposed to teams with the most experience with 0.46% ofdeficits. Nuwer et a}Sl concluded that SSEP monitoring prevents onecase of major persistent neurologic deficits in 200 cases monitored. Thetendency ofSSEPs toward false alarms is reflected by a positive predictive value of only 42%.51 In most series, however, immediate measureswere taken to restore spinal cord conduction after SSEPs were lost,such as reducing distraction, removal of instrumentation, and increasingblood pressure. The reported false-positive cases include those in whichthe evoked potentials warned the surgeon to intervene and a neurologicdeficit successfully was avoided." Several reasons for false-positive monitoring results are available. A mild decrease in SSEP amplitude withoutneurologic deficits may be observed after distraction; also, spinal cordconcussion transiently may alter SSEPs.I False-positive results also canbe attributed to a bolus of anesthetic medication and systemic ortechnical factors unrelated to surgical manipulation. An excessive rate of falsepositive monitoring results should be avoided because this results in atendency to question the validity of response degradation, and may

SPINALCORD MONITORL"'G 933
result in unnecessary changes in the operative strategy and incompletecorrection.
Motor-Evoked Potentials
Several reports have discussed intraoperative motor EPs duringspinal surgery. Comparison of these studies, however, is difficult becauseof wide variations in technique. Until recently, clinical experience wasconfined to few centers, and the number of patients undergoing spinalsurgery with motor EP monitoring is only a fraction of the patientsmonitored with SSEPs. From the limited available evidence, neurogenicmotor EPs have a level of sensitivity that is comparable with SSEPs.5-IThe neurogenic motor EPs seem to be more reliable (less within-patientvariability) than SSEPS.S2 False-positive rates exceed and are below therate observed with SSEPs. During spinal surgery, the other modalities ofmotor EPs have been described, with an insufficient number of patientsto draw conclusions. These smaller series of patients with descriptionsof individual cases, however, offer an elucidating glimpse of the specificity of motor EPs to predict postoperative motor deficits.": 49, 52, 53, 61 Forthe neurogenic motor EPs, a warning threshold was defined as a latencyincrease of 10% and an amplitude reduction to 20% of baseline." Inexperimental scoliosis in the rat, warning criteria for impending injuryfor myogenic motor EPs after transcranial stimulation were a 10% delayin onset latency and a complete disappearance.'! In surgery of the spineusing myogenic motor EP monitoring, these criteria for interventionwere applied.v" An incomplete loss of myogenic motor EPs seems tohave no predictive value for postoperative motor function.'?
In the future, motor EP monitoring will be used increasingly forintraoperative monitoring of spinal cord function. Similar rates of neurologic deficit however, may be encountered after spinal surgery withSSEP or motor EP monitoring.
Does motor EP in combination with SSEP monitoring have anadditional value over only SSEP monitoring? On theoretic grounds,motor and sensory tracts are at risk for injury. Selective damage to thedescending corticospinal tracts and anterior hom may go undetectedwhen only sensory conduction in the spinal cord is monitored. Owen eta152described postoperative loss of motor function without loss of SSEPs.Conversely, a case of sensory deficits with preserved motor function alsohas been described." These reported cases of selective damage mainlyconcern neurosurgical operations of the spinal cord (tumor and arteriovenous malformation). In 500 patients undergoing scoliosis surgery,SSEPs and neurogenic motor EP simultaneously were monitored. Although the warning criteria of both monitoring modalities were appliedstrictly, the reported incidence of neurologic deficits remained as highas 0.4%.5-1 Probably, neurologic deficits cannot be prevented completelyduring scoliosis surgery because, in some cases, the damage is alreadyirreversible at the time electrophysiologic evidence of impaired spinal

934 DE HAAN & KALKMAN
cord function is detected. Combined SSEP and motor EP monitoring hasadvantages for patients with pre-existing neurologic deficits. Reliableresponses (neurogenic motor EP or SSEP) could be obtained in 96% ofthe cases, as opposed to 27% if only SSEP was monitored." A disadvantage of combined monitoring is the increased possibility of false-positive results.
Without assessing the clinical motor status of the patient, it is notpossible to determine whether a response degradation constitutes a trueischemic event or a false-positive result. Removal of instrumentationor accepting less correction of the scoliosis curve based solely on theelectrophysiologic data may result in a suboptimal outcome. To decreasethe incidence of false-positive monitoring results, a wake-up test can beperformed if the intraoperative data meet the warning criteria. Padberget alS-l obtained false-positive rates of 1.4% by using the wake-up test ifthe warning criteria for response degradation were reached.
Spinal cord function monitoring irrespective of the method is beneficial during surgery for spinal deformities. The combination of SSEPand motor EP likely offers additional benefit in the case of neurosurgeryof the spinal cord or when SSEPs cannot be recorded reliably. If doubtexists regarding the neurophysiologic evidence of spinal cord dysfunction during the procedure, the wake-up test is useful. Precious time islost in the case of impending spinal cord damage, however. No patientshould leave the operating room without clinical assessment of lowerlimb motor function.
MONITORING DURING THORACOABDOMINALANEURYSM SURGERY
The cause of neurologic injury after aortic operations is believed tobe temporary or permanent interruption of spinal cord blood supply,resulting in neuronal hypoxia. Such as brain tissue, the anterior hommotor neurons and the spinal motoneuronal system have a high metabolic rate. As a result, the anterior hom gray matter is selectively vulnerable to ischemia. Although white matter is resistant to brief periods ofischemia, selective axonal vulnerability to ischemic damage has beendescribed." When the descending aorta is simply cross-clamped andreplaced without adjuncts to protect the spinal cord, there is a sigmoidrelationship between duration of thoracic aortic cross-clamping and theprobability of spinal cord injury. If the time of aortic clamping does notexceed 30 minutes, the risk of postoperative neurologic deficits is small.The probability of paraplegia increases linearly between 30 and 60 minutes of ischemia, to almost 90% after 1 hour of thoracic occlusion."
The prevention of irreversible ischemic spinal cord injury is basedon three principles. First, degree and duration of ischemia during aorticcross-clamping should be minimized by means of techniques that maintain spinal cord blood flow. Distal aortic perfusion using atriofemoral

SPINAL CORD MONITORlI\:G 935
bypass seems to be protective, especially if sequential aortic damping isperformed." Distal aortic perfusion allows preservation of spinal cordblood flow while the proximal anastomosis of the graft is being performed. It also may be beneficial to use cerebrospinal fluid drainage toprevent a rise in cerebrospinal fluid pressure and a subsequent decreasein perfusion pressure following aortic cross-clamping." These measures,however, do not prevent paraplegia if spinal cord blood supply isdestroyed permanently. Vascular restoration may require reanastomosisof segmental arteries/" Third, if a period of spinal cord ischemia cannotbe avoided (e.g., if the critical segmental arteries are located betweenthe aortic damps), ischemic tolerance can be increased by inducinghypothermia or the previously enumerated neuroprotective measures.In the authors' institution, the technique used for aortic replacementconsists of sequential aortic damping and staged repair while maintaining distal aortic perfusion and selective organ perfusion with acentrifugal pump (left atrial to femoral artery). Cerebrospinal fluid pressure is maintained below 10 mm Hg, and mild hypothermia (33°-34° C)is used.
Monitoring does not decrease the incidence of neurologic deficitsduring thoracoabdominal aortic aneurysm surgery. When a monitoringtechnique is used that allows rapid detection of spinal cord ischemiaand protective strategies are applied immediately, however, irreversibleneuronal damage can be decreased.
Somatosensory-Evoked Potentials
To guide spinal cord protective strategies, the monitoring techniqueshould afford a short interval between onset and detection of the spinalcord ischemia. Information regarding the functional status of the ischemia-sensitive motoneuronal system also should be provided becauseafter an interruption of spinal cord blood flow, the ischemia-sensitivecentral gray matter and lateral and ventral fasciculi often are affectedprimarily.P: 56 SSEP monitoring does not meet these requirements. First,the SSEP conducts afferent information nonsynaptically, which results ina long delay between onset and detection of ischemia because of therelative resistance (8-18 minutes) of axonal conduction to ischemia(propagation of an action potential with little expenditure of energy)."Simple cross-damping results in disappearance of SSEPs in 17 ± 8minutes," This SSEP loss is preceded 4 to 6 minutes by an increase inlatency of 10% from baseline position." In general, 10 minutes areallowed for SSEPs, to detect ischemia." Second, SSEPs reflect the functional status of the sensory tracts, which mainly are located in the dorsalcolumns (supplied from the posterior spinal arteries), and ischemialimited to the motor tracts or anterior hom (supplied from the anteriorspinal artery) may go undetected. As a consequence, false-negativemonitoring results with SSEPs have been reported by several investigators." 16,36,42,65,70

936 DE HAAN & KALKMAN
Although SSEP monitoring improved the surgical strategy in severalstudies," 8.l5, 16, 58 in a prospective study of 198 patients, SSEP monitoringin combination with distal aortic perfusion could not improve neurologicoutcome significantly because of the high incidence of false-negative(13%) and false-positive responses (67%).5 In a series of 38 patients withthroacoabdominal aortic aneurysms, monitoring SSEPs were comparedwith myogenic motor EPs.4s Motor EP evidence of spinal cord ischemiawas accompanied by SSEP changes only in a few cases and always witha considerable delay. Although motor EPs predicted lower limb functioncorrectly in all patients, SSEPs demonstrated false-positive results in 40%of the patients.
SSEP changes similar to those resulting from spinal cord ischemiacan result from hypothermia, peripheral ischemia, and halogenated anesthetics. ls, 6S Using a modality with spinal cord stimulation decreased theincidence of these false-positive responses,"
In the postoperative phase, SSEPs may provide useful information.In a large series of patients, SSEPs detected compromised cord bloodflow resulting from a decrease in spinal cord perfusion pressure inseveral occasions." In that study, the evidence of spinal cord ischemiasuccessfully was reversed by measures that increased spinal cord perfusion pressure, and none of these patients developed lower limb neurologic deficits.
Motor-Evoked Potentials
Neurogenic or myogenic motor EPs after transcranial or spinal cordstimulation require the intact function of the motoneuronal system inthe gray matter of the anterior hom of the spinal cord, and are moresensitive to ischemia than responses recorded from the axons of thedescending tracts (epidural motor EPs). As previously described, responses recorded from the epidural space are slow to disappear afterthe onset of spinal cord ischemia, and responses recorded distal to theanterior hom cells (i.e., from peripheral nerve in previous investigationsand from muscle in the current study) disappear rapidly after the onsetof spinal cord ischemia.to, 21, 56 Epidural motor EPs do not provide information about the functional status of the central gray matter. In accordance, epidural motor EPs have a low sensitivity (46%) in predictingneurologic deficits after temporary aortic cross-clamping in the dog.'?Only motor EPs recorded from a site distal to the anterior hom motorneuron respond sufficiently rapidly to guide protective strategies duringthoracoabdominal aortic aneurysm surgery. Although the neurogenicmotor EPs are compatible with complete neuromuscular blockade, thedisadvantages are invasive electrode placement in the epidural space,the need for signal averaging, and the fact that the neurogenic motor EPis not specific for the motor system. Hence, the authors monitor myogenic motor EPs after transcranial electrical stimulation.
In the authors' experience, myogenic motor EPs are safe and accu-

SPL'JAL CORD MONITORL"G 937
rate. No false-positive or false-negative monitoring results were observed.s- 23. 48 This modality is sensitive to spinal cord ischemia. Ischemiainduced by an interruption of spinal cord blood supply can be detectedwithin minutes (Fig. 3). On empiric grounds, a reduction of motor EPamplitude of the tibial anterior muscle during or after the aortic cross-
Technical failure of Bypass flowbypass pump -.. ~ restored
1000Motor EP of left tibialis
-- anterior muscle800
> -0-Motor EP of right tibialis
.:; 600 anterior muscle
Q)"0
~ 4000..E-c 200
0 .......................................................................................... .......... ..............................................
0 6 12 18 24 30 36
120 Placement of
Ci aortic clampsIE 100
E-CJ) 80Q)....:lCJ)CJ) 60Q)
0::"0
400 -0- Systemic blood pressure0il5c: 20 Blood pressure distalco -- of aortic clampsQ)
~
00 6 12 18 24 30 36
Time (min)
Figure 3. Myogenic motor-evoked potentials in a patient with a type II thoracoabdominalaneurysm. An intraoperative technical failure caused temporary interruption of the atriofemoral bypass flow. The amplitude of the myogenic motor EPs after transcranial electricalstimulation of the left and right anterior tibial muscle, the systemic blood pressure, and thepressure distal of the clamp versus time. Within minutes after distal aortic pressure decreased, motor EPs demonstrated ischemic changes. Immediately after restoration ofbypass flow the responses returned to baseline values.

938 DE HAAN & KALKMAN
clamping period to less than 25% of baseline is considered an indicationof ischemic spinal cord dysfunction." Because the coefficient of variationin this series of patients is 26%, this criterion is similar to a decrease tomore than 3 sensory deficits below average baseline values. This criterionis not exact. If the amplitude is decreased to less than 25% of baseline, theauthors assume that a substantial part of the anterior hom motoneuronalsystem is insufficiently perfused to maintain neuronal transmission.Residual flow at that point, however, might be compatible with neuronalsurvival. The velocity of amplitude reduction might offer additionalinformation in conjunction with the 25% amplitude criterion. The clinicaldata of Meylaerts et al~8 suggest that a complete interruption of bloodflow results in a rapid disappearance of motor EPs, whereas a borderlinespinal cord perfusion results in a gradual motor EP amplitude decrease.To complicate matters further, a gradual amplitude decrease also mightrepresent complete ischemia at the midthoracic level (i.e., confined tothe long corticospinal tracts with adequate perfusion of lumbar motorneurons), although evidence in this area is lacking. After a period ofspinal cord ischemia and disappearance of motor EPs, the absolutepercentage of motor EP recovery probably has no significance; instead,the function of motor EPs is binary. The reappearance of motor EPssuggests reperfusion of the spinal cord, and has predicted lower limbmotor function in all of the authors' patients, whereas the persistent lossof motor EPs reflects insufficient spinal cord blood flow leading to spinalcord damage. Loss of motor EPs at the end of the procedure alwayspredicts lower limb neurologic deficits in the authors' experience." 23, ~8
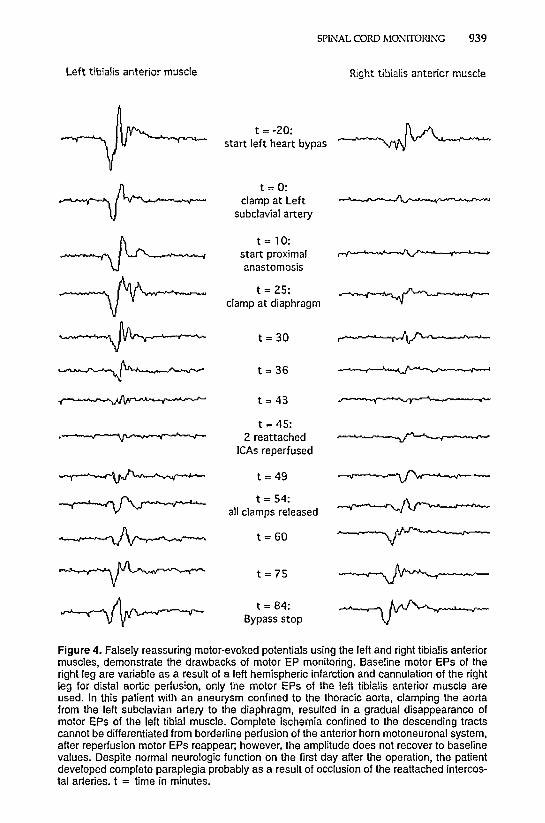
Some practical problems with motor EP monitoring are shown in Figure4. This patient had an aneurysm confined to the thoracic aorta. Baselinemotor EPs of the right leg were variable as a result of a left hemisphericinfarction and cannulation of the right leg for distal aortic perfusion.During aortic cross-clamping, the motor EPs gradually disappeared,which can be interpreted as borderline perfusion of the anterior homgray matter and complete ischemia of the corticospinal tracts. Motor EPsrecovered (but not to baseline values) after reimplantation and perfusionof two intercostal arteries, consistent with reperfusion. Neurologic function was normal after 14 hours. Pulmonary complications, however,necessitated prolonged ventilation and sedation. Two days later, thepatient awoke with complete paraplegia. The postoperative deteriorationof motor function could have resulted from reperfusion injury-unlikelybecause the ischemic duration was only 20 minutes. The most likelyexplanation is an occlusion of one or both of the reattached intercostalarteries. Neurologic deficits frequently develop in the postoperative period. Although the predominant cause of postoperative occlusion isunknown, some occlusions occur as a result of thrombosis of reattachedintercostal arteries, hypotension, hypoxia, raised cerebrospinal fluidpressure, and vasospasm. Postoperative neurologic function should betested early, and neurologic function should be evaluated frequently.Prolonged monitoring of spinal cord function in the postoperative period
Left tibialis anterior muscle
SPINAL CORD MONITORIl"G 939
Right tibialis anterior muscle
t = -20:
~start left heart bypas
~t = 0:
clamp at Leh~subclavial artery
.~t = 10:
start proximal~anastomosis
~t = 25:~clamp at diaphragm
~ t = 30 ~
~ t = 36 ~
~ t = 43 ~
t = 45:.~ 2 reattached~
leAs reperfused
~ t = 49 ~
~t = 54:~all clamps released
~ t = 60 ~
~ t = 75 ~
~t = 84:
~Bypass stop
Figure 4. Falsely reassuring motor-evoked potentials using the left and right tibialis anteriormuscles, demonstrate the drawbacks of motor EP monitoring. Baseline motor EPs of theright leg are variable as a result of a left hemispheric infarction and cannulation of the rightleg for distal aortic perfusion, only the motor EPs of the left tibialis anterior muscle areused. In this patient with an aneurysm confined to the thoracic aorta, clamping the aortafrom the left subclavian artery to the diaphragm, resulted in a gradual disappearance ofmotor EPs of the left tibial muscle. Complete ischemia confined to the descending tractscannot be differentiated from borderline perfusion of the anterior horn motoneuronal system,after reperfusion motor EPs reappear; however, the amplitude does not recover to baselinevalues. Despite normal neurologic function on the first day after the operation, the patientdeveloped complete paraplegia probably as a result of occlusion of the reattached intercostal arteries. t = time in minutes.

940 DE HAAN & KALKMAN
should be considered whenever postoperative sedation is required in apatient that experiences evidence of spinal cord ischemia during theprocedure (suggesting a vulnerable blood supply to the cord).
The rapid assessment of the adequacy of spinal cord blood flowwith myogenic motor EPs offers several advantages in a surgical approach that includes spinal cord protective measures. In the authors'initial experience, motor EPs were used to identify critical segmentalarteries in the cross-clamped aortic segment." Reattachment of onlythese critical arteries can provide permanent restoration of spinal cordblood supply while reducing aortic clamp time. This approach, however,does not prevent neurologic deficits. Probably reimplantation of only thecritical segmental arteries increases the vulnerability of the spinal cordto a compromised blood supply (i.e., hypotension or thrombosis of thegrafted arteries). Porcine experiments reveal that noncritical segmentalarteries become crucial to spinal cord circulation when spinal cordperfusion pressure is compromised." Although past surgical strategyfocused on the importance of preserving the rami spinales arteriaevertebralis (i.e., Adamkiewicz's arteries), the noncritical segmental arteries act as a back-up if spinal cord blood flow is compromised. Consequently, the management of segmental arteries in the authors' hospitalhas changed in recent years. Meticulous preservation of segmental arteries results in "dedicated intercostal care," according to Jacobs et al.23This strategy does not imply merely the reattachment of most of thesegmental arteries. If necessary, separate grafts are used to revascularizesegmental arteries and, on some occasions, these grafts are perfusedduring aneurysm replacement with the centrifugal bypass pump thatalso is used for distal aortic perfusion. Motor EPs also are scrutinized assegmental arteries are reattached, and the technique is adjusted according to the monitoring and the physical appearance of the graft todecrease postoperative occlusions. With this technique, no lower limbneurologic deficits were encountered in 52 types I and II patients."
Although one might argue that the technique of dedicated intercostal care obviates the need for motor EP monitoring to identify criticalsegmental arteries, the functional approach of monitoring motor EPsand the anatomic approach to reattach segmental arteries remaininseparable for several reasons. The technique to reattach segmentalarteries liberally prolongs the duration of cross-clamping, which is animportant predictor of lower limb neurologic deficits. Distal aortic perfusion is believed to preserve spinal cord integrity if distal aortic pressuresare maintained above 60 mm Hg.6 In the authors' experience, however,maintaining distal pressure or mean arterial pressure above 60 mm Hgis not always sufficient. In several patients, distal pressure had to beincreased above 70 mm Hg (in one patient, distal aortic pressure had tobe increased up to 110 mm Hg to preserve motor EPS).20.23 The bloodpressures necessary to maintain sufficient spinal cord blood flow mayvary among patients. Motor EPs help the authors to determine theoptimal pressures required to preserve spinal cord perfusion; therefore,motor EP monitoring is indispensable to guide the timely management

SPINAL CORD MONITORL"-'G 941
of proximal and distal pressures. Motor EP monitoring also can assesswhether relevant intercostal or lumbar arteries originate from a clampedaortic segment. In the authors' series, motor EPs disappeared on severaloccasions when segmental arteries were located in a mushy aorta andnot directly visible. Without motor EP information, no attempts at revascularization would have been made." If evidence of spinal cord ischemiais detected while segmental arteries cannot be found readily, an endarterectomy of the aorta is warranted, with subsequent reattachment ofintercostal arteries. The authors described seven patients in whom motorEPs disappeared and no segmental arteries were available." In thesecases, an aggressive surgical approach, including aortic endarterectomy,selective bypass grafting, and rapid reperfusion, resulted in the recoveryof motor EPs. Motor EPs also can determine perioperatively whetherreattached segmental arteries can maintain adequate spinal cord perfusion.
SUMMARY
Monitoring myogenic motor EPs after transcranial electrical stimulation is effective in detecting spinal cord ischemia. During thoracoabdominal aortic aneurysm surgery, this technique is sufficiently rapid to allowtimely interventions aimed at correcting ischemic conditions and preserving spinal cord blood flow: If strategies are applied to protect thespinal cord during thoracoabdominal aortic aneurysm repair (e.g., distalbypass, cerebrospinal fluid drainage, reattachment of segmental arteries),motor EP monitoring should be included in this protocol to improveneurologic outcome further. Although SSEPs provide information regarding the adequacy of spinal cord blood flow, monitoring SSEPsduring thoracoabdominal aortic aneurysm repair has serious limitations.The response time is too slow to be of practical use. SSEPs also do notprovide information regarding anterior hom motor function and supply,whereas the motor neurons in the anterior hom are most likely to sustainischemic injury.
References
1. Albanese SA, Spadaro JA, Lubicky JP, et al: Somatosensory cortical-evoked potentialchanges after deformity correction. Spine 16(suppl):371-374, 1991
2. Brewer LA, Fosburg RG, Mulder GA, et al: Spinal cord complications following surgeryfor coarctation of the aorta. J Thorac Cardiovasc Surg 64:368-379, 1972
3. Brown RH, Nash CL, Berilla JA, et al: Cortical-evoked potential monitoring: A systemfor intraoperative monitoring of spinal cord function. Spine 9:256-261, 1984
4. Crawford ES,Crawford JL, Safi HJ, et al: Thoracoabdominal aortic aneurysms: Preoperative and intraoperative factors determining immediate- and long-term results ofoperations in 605 patients. J Vase Surg 3:389-404, 1986
5. Crawford ES, Mizrahi EM, Hess KR, et al: The impact of distal aortic perfusion andsomatosensory-evoked potential monitoring on prevention of paraplegia after aorticaneurysm operation. J Thorac Cardiovasc Surg 95:357-367, 1988
942 DE HAAN & KALKMAN
6. Cunningham 11, Laschinger JC, Spencer FC: Monitoring of somatosensory-evokedpotentials during surgical procedures on the thoracoabdominal aorta: Clinical observations and results (part 4). J Thorac Cardiovasc Surg 94:275-285, 1987
7. Dawson EG, Sherman JE, Kanim LE, et al: Spinal cord monitoring: Results of theScoliosis Research Society and the European Spinal Deformity Society survey. Spine16(Suppl): 361-364, 1991
8. de Mol BD, Hamerlijnck R, Boezeman E, et al: Prevention of spinal cord ischemia insurgery of thoracoabdominal aneurysms: The Bio Medicus pump, the recording ofsomatosensory-evoked potentials, and the impact on surgical strategy. Eur J Cardiathorac Surg 4:658-664, 1990
9. Drenger B, Parker SO, McPherson RW,et al: Spinal cord stimulation-evoked potentialsduring thoracoabdominal aortic aneurysm surgery. Anesthesiology 76:689--{j95, 1992
10. Elmore JR, Gloviczki P, Harper CM, et al: Failure of motor-evoked potentials topredict neurologic outcome in experimental thoracic aortic occlusion. J Vase Surg14:131-139, 1991
11. Erwin CW, Erwin AC: Up and down the spinal cord: Intraoperative monitoring ofsensory and motor spinal cord pathways. J Clin Neurophysiol 10:425-436, 1993
12. Follis F, Scremin OU, Blisard KS, et al: Selective vulnerability of white matter duringspinal cord ischemia. J Cereb Blood Flow Metab 13:170-178, 1993
13. Freid LC, Aparicio 0: Experimental ischemia of the spinal cord. Neurology 23:289293,1973
14. Glassman SO, Zhang YP,Shields CB, et al: An evaluation of motor-evoked potentialsfor detection of neurologic injury with correction of an experimental scoliosis. Spine20:1765-1775,1995
15. Grabitz K, Sandmann W, Stuhmeier K, et al: The risk of ischemic spinal cord injury inpatients undergoing graft replacement for thoracoabdominal aortic aneurysms. J VaseSurg 23:230-240, 1996
16. Griepp RB, Ergin MA, Galla JD, et al: Looking for the artery of Adamkiewicz: A questto minimize paraplegia after operations for aneurysms of the descending thoracic andthoracoabdominal aorta . J Thorac Card iovasc Surg 112:1202-1213, 1996
17. Grundy BL, Nelson PB, Doyle E, et al: Intraoperative loss of somatosensory-evokedpotentials predicts loss of spinal cord function. Anesthesiology 57:321-32, 1982
18. Gugino LD, Kraus KH, Heino R, et al: Peripheral ischemia as a complicating factorduring somatosensory-and motor-evoked potential monitoring of aortic surgery. JCardiothorac Vase Anesth 6:715-719, 1992
19. de Haan P, Kalkman CJ, Meylaerts SA, et al: Development of spinal cord ischemiaafter clamping of noncritical segmental arteries in the pig. Ann Thorac Surg 68:12781284,1999
20. de Haan P, Kalkman CJ, de Mol BD, et al: Efficacy of transcr anial motor-evokedmyogenic potentials to detect spinal cord ischemia during operations for thoracoabdominaI aneurysms. J Thorac Card iovasc Surg 113:87-100, 1997
21. de Haan P, Kalkman CJ. Ubags LH, et al: A comparison of the sensitivity of epiduraland myogenic transcranial motor-evoked responses in the detection of acute spinalcord ischemia in the rabbit. Anesth Analg 83:1022-1027, 1996
22. Hickey R, Albin MS, Bunegin L, et al: Autoregulation of spinal cord blood flow: Is thecord a microcosm of the brain? Stroke 17:1183-1189, 1986
23. Jacobs M, Meylaerts SA, de Haan P, et al: Strategies to prevent neurologic deficit basedon motor-evoked potentials in type I and II thoracoabdominal aortic aneurysm repair.J Vase Surg 29:48-57, 1999
24. [antti V, Sonkajarvi E, Mustola S, et al: Single-sweep cortical somatosensory-evokedpotentials: N20 and evoked bursts in sevoflurane anaesthesia. Electroencephalogr ClinNeurophysiol 108:320-324,1998
25. Joseph MG, Langsfeld MA, Lusby RJ: Infrarenal aortic aneurysm: Unusual cause ofparaparesis. Aust N Z J Surg 59:743-744, 1989
26. Kalkman CJ, Boezeman EH, Ribberink AA, et al: Influence of changes in arterial carbondioxide tension on the electroencephalogram and posterior tibial nerve somatosensorycortical-evoked potentials during alfentanil/nitrous oxide anesthesia. Anesthesiology75:68-74, 1991

SPINAL CORD MONITO~G 943
27. Kalkman C], Drummond JC, U HS: Severe sensory deficits with preserved motorfunction after removal of a spinal arteriovenous malformation: Correlation with simultaneously recorded somatosensory- and motor-evoked potentials. Anesth Analg 78:165-168, 1994
28. Kalkman C], Drummond JC, Kennelly NA, et al: Intraoperative monitoring of tibialisanterior muscle motor-evoked responses to transcranial electrical stimulation duringpartial neuromuscular blockade. Anesth Analg 75:584-589, 1992
29. Kalkman C], Drummond JC, Patel PM, et al: Effects of droperidol, pentobarbital, andketamine on myogenic transcranial magnetic motor-evoked responses in humans.Neurosurgery 35:1066-1071,1994
30. Kalkman C], Drummond JC, Ribberink AA, et al: Effects of propofol, etomidate,midazolam, and fentanyl on motor-evoked responses to transcranial electrical or magnetic stimulation in humans. Anesthesiology 76:502-509, 1992
31. Kalkman C], Drummond JC, Ribberink AA: Low concentrations of isoflurane abolishmotor-evoked responses to transcranial electrical stimulation during nitrous oxide/opioid anesthesia in humans. Anesth Analg 73:41Q-415, 1991
32. Kalkman C], Romijn K, Denslagen W: Eliminating diathermy-induced artifacts duringintraoperative monitoring of somatosensory-evoked potentials: A hardware solution. JClin Monit 7:320--324, 1991
33. Kalkman C], ten Brink SA, Been HD, et al: Variability of somatosensory cortical-evokedpotentials during spinal surgery: Effects of anesthetic technique and high-pass digitalfiltering. Spine 16:924-929, 1991
34. Kalkman C], Ubags LH, Been HD, et al: Improved amplitude of myogenic motorevoked responses after paired transcranial electrical stimulation during sufentanil/nitrous oxide anesthesia. Anesthesiology 83:270--276,1995
35. Kalkman C], van Rheineck Leyssius AT, Bovill JG: Influence of high-dose opioidanesthesia on posterior tibial nerve somatosensory cortical-evoked potentials: Effectsof fentanyl, sufentanil, and alfentanil. J Cardiothorac Vasc Anesth 2:75&-764, 1988
36. Kaplan BJ,Friedman WA, Alexander JA, et al: Somatosensory-evoked potential monitoring of spinal cord ischemia during aortic operations. Neurosurgery 19:82-90, 1986
37. Katz NM, Blackstone EH, Kirklin JW, et al: Incremental risk factors for spinal cordinjury following operation for acute traumatic aortic transection. J Thorac CardiovascSurg 81:669-674, 1981
38. Kobrine AI, Evans DE, Rizzoli H: The effects of ischemia on long-tract neural conduction in the spinal cord. J Neurosurg 50:639-644, 1979
39. Lang EW,Beutler AS, Chesnut RM, et al: Myogenic motor-evoked potential monitoringusing partial neuromuscular blockade in surgery of the spine. Spine 21:1676-1686,1996
40. Laschinger [C, Owen J, Rosenbloom M, et al: Direct noninvasive monitoring of spinalcord motor function during thoracic aortic occlusion: Use of motor-evoked potentials.J Vasc Surg 7:161-171, 1988
41. Lerberg DB, Hardesty RL, Siewers R: Coarctation of the aorta in infants and children:25 years of experience. Ann Thorac Surg 33:159-170,1982
42. Lesser RP, Raudzens P, Luders H, et al: Postoperative neurological deficits may occurdespite unchanged intraoperative somatosensory-evoked potentials. Ann Neurol19:22-25, 1986
43. Livesay J], Cooley DA, Ventemiglia RA, et al: Surgical experience in descendingthoracic aneurysmectomy with and without adjuncts to avoid ischemia. Ann ThoracSurg 39:37-46, 1985
44. Lubicky JP, Spadaro JA, Yuan HA, et al: Variability of somatosensory cortical-evokedpotential monitoring during spinal surgery. Spine 14:790--798,1989
45. Machida M, Yamada T, Ross M, et al: Effect of spinal cord ischemia on compoundmuscle action potentials and spinal-evoked potentials following spinal cord stimulationin the dog. J Spinal Disord 3:345-352, 1990
46. McCullough JL, Hollier LH, Nugent M: Paraplegia after thoracic aortic occlusion:Influence of cerebrospinal fluid drainage: Experimental and early clinical results. JVasc Surg 7:153-160, 1988
47. Meylaerts SA, De Haan P, Kalkman C], et al: The influence of regional spinal cordhypothermia on transcranial myogenic motor-evoked potential monitoring and the
944 DE HAAN & KALKMAN
efficacy of spinal cord ischemia detection. J Thorac Cardiovasc Surg 118:1038-1045,1999
48. Meylaerts SA, Jacobs M], van Iterson V, et al: Comparison of transcranial motorevoked potentials and somatosensory-evoked potentials during thoracoabdominal aortic aneurysm repair. Ann Surg 230:742-749, 1999
49. Mochida K, Komori H, Okawa A, et al: Evaluation of motor function during thoracicand thoracolumbar spinal surgery based on motor-evoked potentials using train spinalstimulation. Spine 22:1385--1393, 1997
50. Noirhomme P, Buche M, Louagie Y, et al: Ischemic complications of abdominal aorticsurgery. J Cardiovasc Surg (Torino) 32:451-455, 1991
51. Nuwer MR, Dawson EG, Carlson LG, et al: Somatosensory-evoked potential spinalcord monitoring reduces neurologic deficits after scoliosis surgery: Results of a large,multicenter survey. Electroencephalogr Gin Neurophysiol 96:6-11, 1995
52. Owen JH, Bridwell KH, Grubb R, et al: The clinical application of neurogenic motorevoked potentials to monitor spinal cord function during surgery. Spine 16(suppl):385-390, 1991
53. Owen JH, Sponseller PD, Szymanski J, et al: Efficacy of multimodality spinal cordmonitoring during surgery for neuromuscular scoliosis. Spine 20:1480-1488, 1995
54. Padberg AM, Wilson-Holden TJ, Lenke LG, et al: Somatosensory- and motor-evokedpotential monitoring without a wake-up test during idiopathic scoliosis surgery: Anaccepted standard of care. Spine 23:1392-1400, 1998
55. Peterson DO, Drummond JC, Todd MM: Effects of halothane, enflurane, isoflurane,and nitrous oxide on somatosensory-evoked potentials in humans. Anesthesiology65:35--40, 1986
56. Reuter DG, Tacker WJ, Badylak SF, et al: Correlation of motor-evoked potential response to ischemic spinal cord damage. J Thorac Cardiovasc Surg 104:262-272, 1992
57. Robertazzi RR, Cunningham IN Jr: Monitoring of somatosensory-evoked potentials: Aprimer on the intraoperative detection of spinal cord ischemia during aortic reconstructive surgery. Semin Thorac Cardiovasc Surg 10:11-17, 1998
58. Schepens MA, Boezeman EH, Hamerlijnck RP, et al: Somatosensory-evoked potentialsduring exclusion and reperfusion of critical aortic segments in thoracoabdominal aorticaneurysm surgery. J Card Surg 9:692-702, 1994
59. Schubert A, Drummond JC, Peterson 00, et al: The effect of high-dose fentanyl onhuman median nerve somatosensory-evoked responses. Can J Anaesth 34:35--40, 1987
60. Sebel PS, Flynn PJ, Ingram DA: Effect of nitrous oxide on visual, auditory, andsomatosensory-evoked potentials. Br J Anaesth 56:1403-1407, 1984
61. Stephen JP,Sullivan MR, Hicks RG, et al: Cotrel-Dubousset instrumentation in childrenusing simultaneous motor- and somatosensory-evoked potential monitoring. Spine21:2450-2457, 1996
62. Stinson LW[r, Murray MJ, Jones KA, et al: A computer-controlled, closed-loop infusionsystem for infusing muscle relaxants: Its use during motor-evoked potential monitoring. J Cardiothorac Vase Anesth 8:40-44, 1994
63. Svensson LG, Crawford ES, Hess KR, et al: Experience with 1509 patients undergoingthoracoabdominal aortic operations. J Vasc Surg 17:357-368, 1993
64. Svensson LG, Hess KR, Coselli JS, et al: Influence of segmental arteries, extent, andatriofemoral bypass on postoperative paraplegia after thoracoabdominal aortic operations. J Vasc Surg 20:255--262, 1994
65. Takaki 0, Okumura F: Application and limitation of somatosensory-evoked potentialmonitoring during thoracic aortic aneurysm surgery: A case report. Anesthesiology63:700-703, 1985
66. Toleikis JR, Skelly JP, Carlvin AO, et al: Spinally elicited peripheral nerve responsesare sensory rather than motor. Clin Neurophysiol 111:736--742, 2000
67. Ubags LH, Kalkman C], Been HD, et al: The use of a circumferential cathode improvesamplitude of intraoperative electrical transcranial myogenic motor-evoked responses.Anesth Analg 82:1011-1014,1996
68. van Rheineck Leyssius AT, Kalkman C], Bovill JG: Influence of moderate hypothermiaon posterior tibial nerve somatosensory-evoked potentials. Anesth Analg 65:475--480,1986

SPINAL CORD MONITORI!'\G 945
69. York DH, Chabot RJ,Gaines RW:Response variability of somatosensory-evoked potentials during scoliosis surgery. Spine 12:864-876, 1987
70. Zomow MH, Drummond IC: Intraoperative somatosensory-evoked responses recordedduring onset of the anterior spinal artery syndrome. J Clin Monit 5:243-245, 1989
Address reprint requests to
Peter de Haan, MD, PhDDepartment of Anesthesiology
Onze Lieve Vrouwe GasthuisPostbus g 5500
1090 HM Amsterdam, The Netherlands
e-mail: [email protected]