southwest idaho dental society
TRANSCRIPT

1/27/2019
1
Southwest Idaho Dental SocietyOral Medicine in Clinical PracticePart 1 – Medical Management of Common Orofacial Conditions
David Dean, DDS, MSD, DABOM, FDS RCSEd
Graduate Program Director & Assistant Professor Department of Oral MedicineUniversity of Washington School of DentistrySeattle Cancer Care Alliance
Declarations
• I am not a physician
• I have no conflicts of interest to disclose
• Medication recommendations include “off label” uses
• Recommendations are consistent with current literature & standard of care within Oral Medicine/Orofacial Pain
Disclaimer
• All opinions expressed are my own
• They do not reflect official policies of the University of Washington, UWSOD, the department of Oral Medicine, or esteemed Husky former Boise State football coach Chris Petersen
Objectives • Identify clinical situations in which non-surgical interventions,
such as pharmacotherapy and/or behavioral management, may be indicated in the treatment of common oral conditions.
• Recognize items in a patient’s medical history, including topical and systemic medications, which may impact your intervention choice.
• Outline specific medication protocols that could be applied in each clinical scenario.
Case-based scenarios
Oral mucosal disorders▫ Oral candidiasis▫ Lichenoid mucositis (OLP, GVHD, desquamative gingivitis)▫ Recurrent aphthous stomatitis
TMD with limited opening▫ Myofascial pain with limited opening▫ Disc displacement without reduction
Case-based scenarios
Medication-related osteonecrosis of the jaw (MRONJ)
Oral burning disorders▫ Burning mouth syndrome▫ Hyposalivation/xerostomia▫ Oral burning related to other causes (systemic disease,
parafunctional habits, etc.)

1/27/2019
2
Oral mucosal disorders (Stomatitis)
Case
• 58-year-old Filipino female
• Referred to Oral Medicine clinic at SCCA by heme-oncology for management of Graft-versus-Host disease (GVHD)
• Chief concern: Mucosal sensitivity & increasing “lichenoid” changes while tapering immunosuppressive medications
CASE 1
• Sensitivity began approximately 4 weeks ago
• Increased by orange juice, spicy foods, & mouthwash
• Sensitivity is absent (or “very low”) at rest
• Dexamethasone rinse was initially helpful, but not burns when applied
• Concurrent symptoms:▫ Xerostomia (“My mouth is very dry all the time”)
CASE 1
• Past medical history▫ AML▫ DM2▫ HTN▫ History of pulmonary
embolism
• Family history▫ Non-contributory
• Social history▫ Originally from the
Philippines▫ Immigrated to US 10
years ago▫ Primary language is
Tagalog
CASE 1
• Medications▫ Acyclovir▫ Bactrim DS▫ Dexamethasone elixir 0.5mg/5mL rinse for 5 min QID
▫ Prednisone 5 day “pulse” dose
▫ Tacrolimus 0.5mg BID
▫ Warfarin 2mg QD
• Adverse medication reactions▫ None
CASE 1
What are the key symptoms?
• Sensitivity to acids, spices, & mouthwash (mint, alcohol?)
• Xerostomia
• Lack of improvement with dexamethasone rinse & pulse prednisone
CASE 1

1/27/2019
3
Mucosal symptomsPatients develop sensitivity due to thinning of mucosa Common triggers:▫ Acids▫ Spices▫ Carbonated beverages▫ Strong flavors (ex. mint in toothpaste)▫ Rough textures
Key questions
• If her symptoms are related to GVHD, why isn’t she improving with topical & systemic steroids?
▫ Is she using the medication as prescribed?
▫ Are there other factors that would make the medications less effect?
▫ Do we have the correct diagnosis?...
CASE 1
Head & neck exam▫ (-) extraoral swelling or asymmetry▫ (-) lymphadenopathy▫ (-) sinus pain (maxillary or frontal)▫ (-) thyromegaly▫ (-) TMJ dysfunction▫ (-) pain in muscles of mastication or cervical muscles▫ (+) skin dryness
CASE 1
What tests should be performed next?1) Inspection of the oral cavity
▫ Oral mucosa, salivary expression, etc.2) Additional tests based on clinical findings
▫ Biopsy(?), culture, salivary flow testing, etc.
CASE 1
CASE 1
© SCCA
CASE 1
© SCCA

1/27/2019
4
CASE 1
© SCCA
Oral Candidiasis: Chronicity & Invasion
Pseudomembranous
Atrophic Mucositis
Erythematous Mucositis
Hyperplastic Lesions
Invasive Candidiasis
Superficial
Invasive
Acute
Chronic
• Establish correct diagnosis▫ What condition are we treating?▫ Are their multiple co-occurring conditions the need to be
addressed simultaneously?
• Address contributing factors ▫ Factors increasing risk for infection/re-infection
What are the key factors in treatment?
CASE 1
• Plan of Care – Manage contributing factors▫ Dry mouth▫ Immunosuppression ▫ Topical & systemic steroids▫ Endocrine dysfunction (DM2)▫ Antibiotic therapy (change in normal flora)▫ Dentures▫ Others: steroid inhalers, smoking
CASE 1
• Plan of Care – Manage contributing factors▫ Dry mouth▫ Immunosuppression ▫ Topical & systemic steroids▫ Endocrine dysfunction (DM2)▫ Antibiotic therapy (change in normal flora)▫ Dentures▫ Others: steroid inhalers, smoking
CASE 1
Deal with the dry mouth!• Adequate hydration (frequent sips of water)
• Salivary stimulants (sugar-free candies, mints, gum, etc.)
• Normal saline rinses (¾ TSP salt in 32 oz. water)
• Coating agents (Aquoral, Biotene, Xerostom, Xylimelts, OraMoist, MouthKote, etc.)

1/27/2019
5
Consider objective salivary measurement before starting a sialagogue
• Stimulated & unstimulated salivary flow▫ No food/drink for 2 hours prior to exam▫ Unstimulated (WNL >0.5ml/min)▫ Stimulated (WNL = 1-1.5ml/min)
http://www.mah.se/
Medications to increase salivary flow
• Sialagogues▫ Cevimeline (Evoxac®) – 3omg TID*▫ Pilocarpine (Salagen®) – 5mg TID
*FDA approved for Sjögren’s Syndrome only
Sialagogue therapy
• Contraindications▫ Narrow angle glaucoma▫ Uncontrolled asthma
Figure © Webeyeclinic.com
Sialagogue therapy
• Cautions▫ Arrhythmia, Beta blocker use, &/or other significant cardiac
disease (e.g. MI, angina)
▫ Respiratory illnesses (controlled asthma, mod/severe COPD)
▫ Gallstones/Kidney stones
▫ Severe hepatic impairment
▫ Anti-cholinergic meds (diphenhydramine, bupropion
oxybutynin, etc.)
Sialagogue hacks…
• Warn patients about potential flushing & sweating▫ Titrate up to minimize side effects ▫ Sample instructions:
Begin with 30mg dose before bed, after 5 days add a second dose in the morning. After an additional 5 days increase to recommended 30mg TID
• 3-month trial required for maximum effect
• Plan of Care – Candidiasis• Clotrimazole Troches (10 mg)▫ Dissolve slowly in mouth 5x/day
▫ If dry, rinse mouth with water first
• Nystatin oral suspension (100,000 IU/mL)▫ 5 mL swish & hold for 2 minutes 4x/day▫ 33-50% sucrose (caries risk with chronic use)
www.wockhardtusa.com
West Coast Pharmaceuticals
CASE 1

1/27/2019
6
• Plan of Care – Treating the denture• Nystatin ointment (100,000 IU/g)
▫ Apply liberally to all surfaces of denture TID• Remove denture at night soak in denture cleaner
www.dentexgroup.com
CASE 1
• Plan of Care – Treating the denture (alternative)• Bleach (1 TSP in 32 oz of water)
▫ May bleach denture• Zephiram 1:770 (cold sterile solution)
CASE 1
RINSE THOROUGHLY AFTER USE (!)
• Clotrimazole cream (1%)▫ Available OTC (Lotrimin AF ®)
• Nystatin ointment (100,000 IU/g)▫ Yellow color may impact
compliance• Apply to corners of mouth TID• Continue for 4 days after
resolution of redness/cracking© SCCA
• Plan of Care – Angular cheilitis
CASE 1
• Bacterial co-infection is possible• Yellow crusting = Staph
Treat with:▫ 2% Ketoconazole▫ 2% Mupirocin
© SCCA
• Plan of Care – Angular cheilitis (alternative)
CASE 1
Photo: © Dr. Jerry Bouquot, The Maxillofacial Center, Morgantown, West Virginia
• Plan of Care – Systemic therapy (alternative) • Fluconazole ▫ Sample instructions:
200mg on day 1 & 100mg for next 6 days
What is a disadvantage to a systemic azole antifungal in this case?
CASE 1
Azoles have MANY drug interactions (!)

1/27/2019
7
• In this case the most significant interaction is with warfarin
• Elevated bleeding risk▫ 39-44% increase in PT w/ 7 day dosing(1,2)
▫ 34% with single 150mg dose(3)
▫ 2x risk of hospitalization for GI bleed(4)
• Contact physician (possible dose adjustment?)
1) Crussell-Porter L et al. (Arch Intern Med, 1993)2) Black D et al. (Clin Pharmacol Ther, 1992)3) Turrentin M (Obstet Gynecol, 2006)4) Schelleman H, et al. (Clin Pharmacol Ther, 2008)
Fluconazole – Drug interactions Fluconazole – Drug interactions (cont.)
• See: Hersch & Moore, “Drug Interactions in Dentistry: The Importance of Knowing your CYPs” (JADA, 2004)▫ Statins▫ Anti-psychotics▫ Benzodiazepines▫ Calcium channel blockers▫ HIV medications▫ Etc., etc., etc.
• Pregnancy Category X
Oral mucosal GVHD is a lichenoid condition that is diagnosed clinically.
How would this case differ if this was oral lichen planus?
© OMCS
Oral Lichen Planus
Differential diagnosis (Oral lichen planus)
• Primary lichen planus (oral +/- mucocutaneous involvement)• Lichenoid mucositis
▫ Medication-induced (NSAIDs, anti-hypertensive, anti-diabetes medications)▫ Hypersensitivity reactions (dental materials, OH products)▫ Graft-versus-Host disease (allogeneic transplants only)
• Autoimmune/Vesiculobullous disorders (PV, MMP, Lupus, etc.)• Trauma (Mechanical - e.g. cheek biting; Thermal - e.g. burn; Chemical - e.g.
cinnamon oil, SLS-toothpaste, etc.)• Candidiasis • Oral dysplasia/carcinoma
Diagnostic tests (Oral lichen planus)• Mucosal biopsy (H&E + Direct immunofluorescence)
• Elimination trials (medications, dietary factors, etc.)
• Patch testing (dental materials)
• Laboratory testing (Hepatitis C, thyroid disease?)

1/27/2019
8
Oral lichen planus - Management• Oral lichenoid lesions should be treated if:▫ Symptoms are affecting quality of life (e.g. general comfort,
food choice, etc.)▫ Tissues are ulcerated
Patients with non-oral signs/symptoms should be evaluated & treated by an
appropriate physician
Oral lichen planus - Management• Remove potential irritants ▫ Smooth potentially traumatic teeth & appliances▫ Avoid potentially traumatic habits▫ Discontinue tobacco▫ Decrease foods/beverages that increase symptoms▫ Practice good oral hygiene
Goals = improve comfort & decrease general inflammation
Adapted from Mirowski et al. (UpToDate, 3.2018)
Topical steroid therapy – Whole mouth
• Dexamethasone elixir (0.5mg/5mL)▫ Rinse with 5-10mL for 5 minutes, QID.▫ Taper down to lowest effective dose▫ Preferably alcohol-free (though hard to find!)
• Compounded rinses ▫ Clobetasol 0.05%, rinse with 5 mL BID-TID▫ Triamcinolone acetonide 0.1% (micronized), rinse with 5 mL QID
Topical steroid therapy - Instructions
• Spit out after use• Do not eat, drink, rinse for 30 minutes
1 month compounded clobetasol rinse (0.05%)
Severe lichenoid stomatitis (GVHD)
Treister et al. (Blood, 2012)
Topical steroid therapy – Localized
• Fluocinonide gel (0.05%)▫ Dry lesion. Apply a thin film of gel. Cover with gauze. Leave for 10
minutes. Repeat TID-QID.
• Clobetasol gel (0.05%)▫ Dry lesion. Apply “bb-sized” amount of gel. Cover with gauze. Leave
for 10 minutes. Repeat BID.
Can also be used in combination with a rinse

1/27/2019
9
© Dr. K’la Benson
Mini-case
© Dr. K’la Benson
Mini-case
Topical steroid considerations
• Custom trays can be helpful for direct application of corticosteroid gels to gingival tissues
Photo: © UpToDate 2018Mirowski et al. (UpToDate, 3.2018) © OMCS © OMCS
© OMCS © OMCS
Topical steroid considerations
• Ultrapotent steroids (clobetasol, halobetasol)▫ Not meant for continuous use (2 weeks on, 1+ week off)▫ Limit use on external lip due to risk of permanent atrophy Desonide ointment is a good alternative
▫ Cost has dramatically increased in the last 2 years; Ointments may be more cost effective

1/27/2019
10
Topical steroid considerations
• Kenalog (triamcinolone) in Orabase is irritating to tissues ▫ Not recommended in OLP▫ Also very expensive: $80(!) for 5 grams
• Rivelin (clobetasol) patch▫ Direct application to lesion site▫ FDA/EMA approved ▫ Currently in phase II trials in Europe
• Increased risk for secondary candidiasis ▫ Especially in pts with other risk factors for yeast infection▫ Risk factors: hyposalivation, broad-spectrum antibiotic
use, steroid inhalers, poor glycemic control, other causes of immunosuppression, etc.
• Consider prophylactic anti-fungal▫ e.g. Clotrimazole troches (10mg, 1-2x daily)
Topical steroid considerations
When should a patient with lichen planus be referred to a specialist?
Lichen Planus – Indications for Referral
Patients with non-oral signs/symptoms should be evaluated & treated by an
appropriate physician.
e.g. Dermatology, Gynecology, etc.
• Unclear diagnosis
• Concern for malignancy or OLP subtype with higher risk
for transformation (e.g. erosive & hyperplasic)
• Poor or incomplete response to therapy
Oral lichen planus – Indications for Referral
© OMCS

1/27/2019
11
Oral lichen planus – Follow-up
• Patient education is crucial due to low (but significant) risk for malignant transformation
• Recommend follow-up every 3-4 months▫ Photos▫ Adjunctive diagnostic testing (?)▫ Biopsy/Re-Biopsy (?)
More on OLP & cancer risk this afternoon
Stay tuned…
Oral lichen planus – Malignant transformation
Oral mucosal lesions (Recurrent Aphthous Stomatitis)
Case
• 34-year-old Vietnamese female
• Referred to the Oral Dysplasia clinic (UW Otolaryngology)
• Chief concern: recurrent, painful mucosal ulcers since immigrating to the US five years ago
Mini-case
© EL Truleove
Mini-case
Differential diagnosis (Aphthous Stomatitis)• Stress (!)• Trauma (including loss of mucin layer)• Hypersensitivity (OH products, cinnamon oil, chocolate,
strawberries, tomatoes, nuts, coffee, dairy/lactose, wheat/celiac)• Medication reaction (NSAIDs, beta blockers, birth control, sulfa)
• GI disease (Crohn’s, ulcerative colitis, celiac disease, H. pylori)• Hematologic diseases (leukemia, cyclic neutropenia, HIV)• Syndromes (Behcet’s, Sweet’s, PFAPA, MAGIC)
Mini-case

1/27/2019
12
Aphthous management
• Minor aphthous usually resolves within 7-14 days and may not require management
• Rule out contributing factors (previous slide)
Mini-case
Aphthous management
• Avoid irritants & maintain salivary coating▫ Foaming (SLS) & anti-tartar (pyrophosphate)
additives cause dose-dependent desquamation
▫ Alternatives: Prevident Gel Biotene Gentle Mint Squiggle Enamel Saver (online only)
Mini-case
Aphthous management – Supportive care
• Palliative interventions can be employed for symptom management (e.g. bland rinses, topical anesthetics, analgesics)
• Supportive care important in younger patients (e.g. hydration, nutrition)
Remember…
• Palliative interventions can be helpful in managing symptoms in most mucosal disorders
• Minimal therapeutic benefit, BUT can improve comfort with low risk for adverse effects
Aphthous management – Palliative therapy
• Bland rinses
▫ Normal saline (“Salt water rinses”, “Salt & soda”)
▫ No limit (“rinse as often as comfortable”)
▫ Don’t make too salty (!) (3/4 tsp salt in 32 oz water)
▫ Can warm or cool per patient preference
▫ May add 1 Tbsp NaHCO3 (helpful in neutralizing acid, e.g. if lesions accompanied by thick salivary secretions)
Aphthous management – Palliative therapy
• Topical anesthetics
▫ 2% viscous lidocaine
▫ 20% benzocaine (Orajel TM)
▫ Magic mouthwash
Many formulations available
Most common is a 1:1:1 mixture of diphenhydramine, viscous lidocaine, & milk of magnesia

1/27/2019
13
Remember…
• Cautions with topical anesthetics▫ Avoid traumatizing soft tissues while numb (e.g. during
eating, drinking, oral hygiene, etc.)▫ Gargling/swallowing can cause temporary paralysis of
the gag reflex (increased risk for choking, aspiration)▫ Avoid excessive/chronic (methemoglobinemia risk)
Aphthous management
• Topical steroids (see previous slides)
• Mucosal protectants (Orabase®, Zilactin-B®)
• Canker-melts® (Glycyrrhiza extract) or B12-melts®
• H2 blockers (e.g. Cimetidine 600mg TID)
• Tetracycline rinse (short-term only)
• Stress management
Mini-case
Aphthous management
• Cautery/caustic agents (e.g. laser, silver nitrate, etc.) and antibiotics (e.g. tetracycline) aren’t recommended in chronic therapy
• Major aphthous may require additional systemic interventions (under the guidance of a specialist)
Mini-case
Recommended resource
TMD with limited opening

1/27/2019
14
Case
• 46-year-old Caucasian female
• Referred to SCCA Oral Medicine by Oncology to “rule out emerging Medication-related Osteonecrosis of the Jaw”▫ History of Multiple Myeloma with 13 doses of pamidronate
(Aredia®)▫ Autologous PBSCT (January 2015)
• Chief concern: Left-sided jaw pain with limited opening
CASE 2
History of chief concern
• Initial symptoms▫ “Sharp” pain near maxillary left first molar (#14)
▫ Onset immediately after eating a Milk Dud while driving to Portland in a “torrential downpour”
▫ Intensity rated as moderate (6 out of 10)
CASE 2
History of chief concern
• Evaluated by dentist No clinical or radiographic evidence of odontogenic infection
• Sharp pain has not recurred since her initial episode
CASE 2
• Chief concern (current)▫ Constant “aching” pain in the left jaw which has been
present for the past 6 weeks▫ Intensity = 3 to 7 out of 10▫ Aggravated by jaw function, clenching, stress, & poor sleep
• Secondary concerns▫ Difficulty eating a cheeseburger last week
(“I couldn’t open enough. It was too painful.”)▫ Audible clicking (bilateral TMJs)
CASE 2
• Past medical history▫ Multiple myeloma▫ Anxiety▫ Insomnia
• Family history▫ Parents + 5 siblings are
alive and in good health
• Social history▫ Part-time teaching
assistant at a University▫ Married (x20 years),
husband attends medical visits
▫ 12 year old daughter
CASE 2
• Medications▫ Lorazepam▫ Zolpidem ▫ Calcium ▫ Multivitamin without iron ▫ Vitamin D
• Adverse medication reactions▫ Nausea with dental
anesthetic
CASE 2

1/27/2019
15
What are the key symptoms?
• Constant “aching” pain that is aggravated by jaw function, clenching, & stressors
• Limited opening due to pain
• Audible clicking (bilateral TMJs)
• Initial episode of sharp pain that has not recurred
CASE 2
Differential diagnosis
• Myofascial pain (with limited opening)
• Disc displacement with reduction
• Daytime parafunction (clenching +/- nocturnal bruxism?)
• Occult dental pathology (e.g. “cracked tooth syndrome”)
• Referred pain (?)
CASE 2
• Head & neck exam▫ (-) extraoral swelling or asymmetry▫ (-) lymphadenopathy▫ (-) sinus pain (maxillary or frontal)▫ (-) salivary gland abnormality▫ (-) thyromegaly▫ (+) visible distress related to CC
CASE 2
What tests should be performed next?
1) TMD examination (range of motion, muscle & joint palpation)
2) Inspection of the oral cavity (mucosa, gingiva, dentition)
3) Dental testing (radiographs, endodontic testing, percussion, palpation, perio probing, etc.)
CASE 2
Functional measurements
• Maximum Opening1) Unassisted without pain2) Unassisted with pain3) Assisted with pain
▫ Normal: >40mm▫ Abnormal: <30mm
• TMD exam▫ Maximum opening without pain = 19mm▫ Maximum opening with pain = 37mm
Maximum opening produced:• Pain in bilateral masseters • Spasm in left masseter • Decrease in maximum opening (37mm 34mm)
CASE 2

1/27/2019
16
Joint sounds
• Click/pop• Crepitus (audible, soft)
▫ Maximum opening▫ Right & left lateral▫ Protrude jaw open/close in protrusion• Does click go away? disc reducing normally
• TMD exam (cont.)
Audible clicking (R/L) TMJs▫ Maximum opening▫ Lateral excursions▫ Click eliminated in protrusion
CASE 2
Muscles palpation = 2 pounds of pressure
Masseter
Sternocleidomastoid
Trapezius
Frontalis
Temporalis
Orbicularis oris
Zygomaticus
Buccinator
Orbicularis oculi
Q: Are any structures painful to standardized palpation?
CASE 2
Masseter
Sternocleidomastoid
Trapezius
Frontalis
Temporalis
Orbicularis oris
Zygomaticus
Buccinator
Orbicularis oculi
CASE 2
Q: Are any structures painful to standardized palpation?
TMJ palpation = • 1 lbs lateral pole• 2 lbs around pole
Masseter
TRIGGER POINT
CASE 2

1/27/2019
17
Muscle examination increased baseline pain from 3 to 7 (out of 10)
CASE 2
© Dr. C.D. Johnson, UT Houston
• Intraoral examCASE 2
• Intraoral exam▫ Fractured amalgam (Tooth#14)▫ Teeth painful to percussion in multiple quadrants
(UR, UL, LR)▫ No evidence of exposed bone (i.e. no MRONJ)
© Dr. C.D. Johnson, UT Houston
CASE 2
Problem Differential DiagnosisConstant, aching pain (Left jaw)
1) Myofascial pain with referral• Daytime parafunction• Nocturnal bruxism
2) Left TMJ arthralgia3) Occlusal traumatism4) Odontogenic pain
(referred)
CASE 2
Problem Differential Diagnosis
Sharp pain (region of tooth #14)
1) Myofascial pain with referral (left masseter)
2) Occlusal traumatism3) Cracked tooth #144) Maxillary sinusitis
Simons DG, et al., Myofascial Pain and Dysfunction: The Trigger Point Manual
TMD – Diagnostic categories
• Group 1: Muscle Disorders• Group 2: Disc Displacements• Group 3: Other Disorders (Joint & Bone)

1/27/2019
18
Muscle, Disc,& Joint
Muscle & Joint
Seeking CareClinic TMD Cases n=247
Not Seeking CareCommunity TMD Cases n=120
Muscle
MuscleNo Dx
No Dx
Disc
Joint
Muscle & Joint
Muscle, Disc,& Joint
Disc
Joint
RDC-TMD TMD – Muscle disorders (RDC for TMD)Myalgia, Myofascial Pain, Myofascial pain w/ limited opening
1) Pain2) ≥3 painful muscle sites
Myofascial pain3) Maximum opening
Myofascial painw/ limited opening
<40mm
Familiar pain with: 1) Jaw opening OR2) Muscle palpation
Myalgia
1) Local Myalgia▫ Pain at site only
2) Myofascial pain▫ aka “MFP w/ spreading”▫ Pain beyond area of
stimulation
3) Myofascial pain w/ referral▫ Pain beyond muscle
boundary
SUBTYPE EVALUATION5 second palpation at site
+ confirmation of site
• Muscle pain
TMD – Muscle disorders (DC for TMD) TMD – Disc displacementsDisc displacement with & without reduction
Kelley's Textbook of Rheumatology (8th ed.)Copyright © 2008 W. B. Saunders Company
Reciprocal click = DD w/ reduction
1) Joint pain1) Ongoing2) On palpation3) On opening or excursion
TMD – Other disorders (Joint & bone)Arthralgia, Osteoarthritis, Osteoarthosis
Coarse Crepitus
Osteoarthritis
Arthralgia

1/27/2019
19
0
5
10
15
20
18-24yo 25-44yo 45-64yo >65yo
Males
Females
TMD pain – Prevalence in last 6mo
Van Korpff, 1988
N = 1016N = 1016
TMD-RELATED PAINDECREASES WITH AGE
Conservative TMD protocol
• Most patients with TMD improve over time
• Conservative management is usually effective in decreasing pain & increasing function
• Avoid irreversible treatment if possible▫ Surgery is reserved for very select cases
• Plan of Care – Conservative TMD protocol
1010
3
310
CASE 2
Key questions
• What are you trying to treat with recommended/prescribed medications?▫ General pain?▫ Muscle pain?▫ Inflammatory pain?▫ Contributing factors? Bruxism/Parafunction Axis II factors (depression, anxiety, somatization, stressors)
• Plan of Care – Pharmacotherapy▫ Low-dose Amitriptyline (10mg before bed)
CASE 2
Tricyclic antidepressants (TCAs)
• Amitriptyline & nortriptyline • Short-term effect in myalgia & arthralgia
▫ Starting doses 10 (to 30) mg before bed▫ Up to 3-month trial for maximum effect
• Especially useful in cases with: ▫ Bruxism▫ Sleep dysfunction▫ Concurrent, depression, anxiety, somatization

1/27/2019
20
• Hyposalivation (dose dependent)▫ Increased caries risk at higher doses & in patients taking
multiple xerogenic medications
• Sedation▫ Increased fall risk in elderly patients (esp. those taking other
CNS depressants)
• Arrhythmia ▫ Increased risk in elderly patients (don’t prescribe over age 65)
• Off-label use / Within scope of practice (?)
TCA considerations • Plan of Care – Pharmacotherapy (alternative)▫ Short-term muscle relaxant Effective in management of acute Myalgia & MFP,
but less effective in chronic TMD*
*May still be used as part of a chronic management protocol
CASE 2
• Only effective if the patient has muscle pain
Muscle relaxant considerations
© Fox Searchlight & Paramount Pictures
Muscle relaxants
• Cyclobenzaprine (Flexeril®)▫ 5-10mg (up to TID)
• Tizanidine (Zanaflex®)▫ 2mg (up to) TID
• Methocarbamol (Robaxin®)▫ 500-1500mg (up to) QID
• Diazepam (Valium®)▫ 2-4mg (up to) TID
• Metaxalone (Skelaxin®)• Carisoprodol (Soma®)
• Cyclobenzaprine (Flexeril®)▫ “Hangover” effect▫ Can minimize SEs by starting at low dose
(e.g. 5-10 mg before bed) on a “weekend”▫ Drug interactions with TCAs & SSRIs due to
serotonin effects
Muscle relaxant considerations
© Photo: Legendary Pictures
• Tizanidine (Zanaflex®)▫ Alpha-2 adrenergic antagonist▫ Generally well-tolerated SE: sedation, hypotension, hepatic effects
▫ Caution with beta blockers & in elderly patients▫ Always check drug interactions
• Methocarbamol (Robaxin®)▫ Less potent (OTC in Canada)▫ Titration advantage in pts sensitive to sedating meds
Muscle relaxant considerations

1/27/2019
21
• Diazepam (Valium®)▫ Especially helpful in short-term management of patients
with muscle-based pain & concurrent anxiety▫ All benzodiazepine considerations apply (e.g. caution
with driving, dependence, cognitive decline)• Carisoprodol (Soma®)
▫ Dependence/addiction risk
Muscle relaxant considerations• Drug interactions
▫ Sedating & centrally-acting medications▫ Narcotics▫ Anti-depressants▫ Anti-psychotics▫ Barbiturates▫ MAO inhibitors▫ H2 blockers
Muscle relaxant considerations
• Plan of Care – “Boil & bite” soft nightguard
CASE 2
Occlusal guards
• May decrease clenching (do not stop it)• Protect teeth & decrease force on joint
• Most useful in patients waking with pain ▫ E.g. myalgia, arthralgia, pain in teeth, headache
• Avoid in cases of open bite if attempting to regain contact
Both custom acrylic & soft “sports guards” are
effective(1)
1) Truelove (JADA, 2006)
Soft guards
• Buy the least expensive guard that covers all the teeth▫ Expensive soft guards are too
bulky & may increase pain• Soft guards do not fit as well
▫ Some patients report ↑clenching
▫ D/C guard if pain increases
Photo: Truelove (JADA, 2006)

1/27/2019
22
Custom guards
1) Acrylic exterior with thermoplastic intaglio2) Flat plane3) Balanced occlusion 4) Avoid indexing of opposing teeth
• “locking in” may increase pain5) Avoid heavy anterior contact
• “Masseteric reflex”http://www.pddsmile.com/services/sleep-appliances-44747/rem-e-deze.html
How would this case look different if limited opening was caused by
disc displacement?
Case
• 31-year-old Caucasian female
• Referred by her dentist to UW Oral Medicine due to acute onset limited opening.
• Chief concern: “My jaw locked last week, now I can’t open wide”
CASE 3
History of chief concern
• Asymptomatic “popping” in the jaw for many years
• No history of pain or locking
• Went skiing with friends (after final exams)
• She was laughing while riding the chairlift▫ Immediate sharp pain in front of right ear▫ Unable to open wide since that time
• Current pain with yawning, laughing, & chewing
CASE 3
• Past medical history▫ Depression▫ Situational anxiety
• Family history▫ Breast cancer (mother)
• Social history▫ College student at
Seattle Pacific University
▫ Studying psychology▫ Very active (running,
skiing, outdoor activities)
CASE 3
1/27/2019
23
• Medications• Fluoxetine▫ 20mg daily
• Multivitamin
• Adverse medication reactions▫ Penicillin (rash)
CASE 3
What are the key symptoms?
• Acute onset pre-auricular pain• Acute onset, persistent limited opening• Pain with function (e.g. opening wide, chewing)
• Loss of clicking (?)
CASE 3
Head & neck exam• (-) extraoral swelling or asymmetry• (-) lymphadenopathy• (-) sinus pain (maxillary or frontal)• (-) salivary gland abnormality• (-) thyromegaly
CASE 3
What tests should be performed next?
1) TMD examination2) Advanced imaging - MRI (TMJ series)
CASE 3
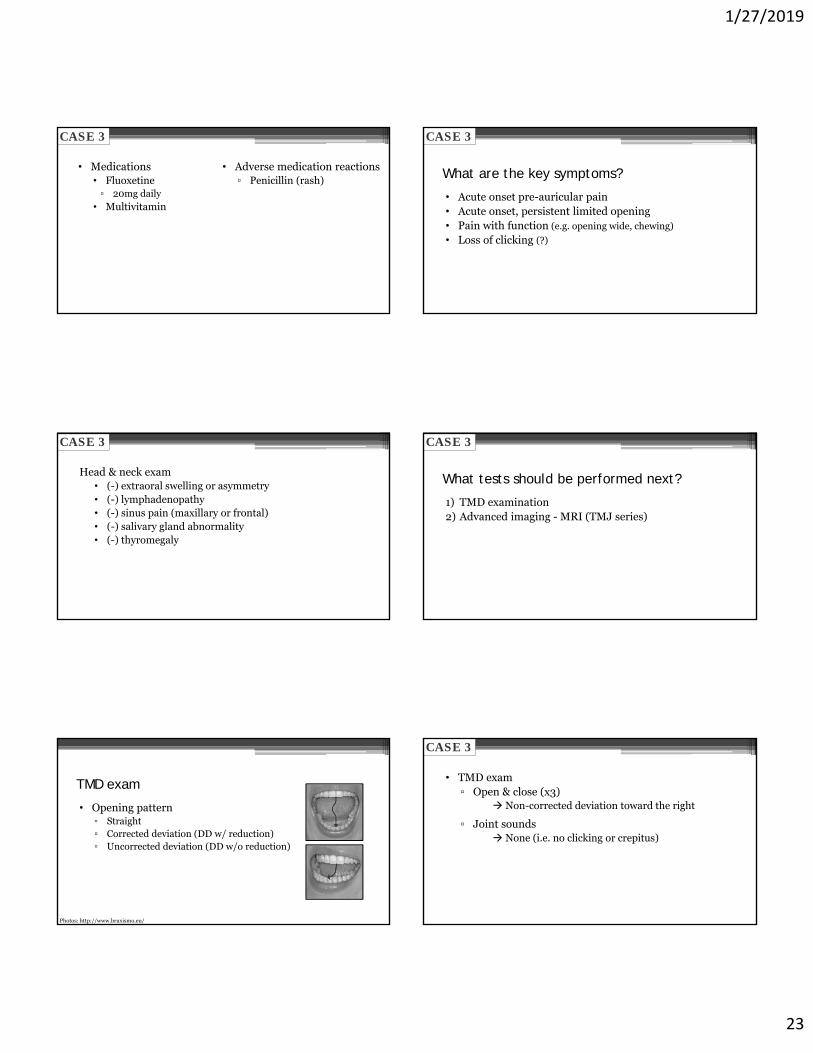
TMD exam
• Opening pattern▫ Straight▫ Corrected deviation (DD w/ reduction)▫ Uncorrected deviation (DD w/o reduction)
Photos: http://www.bruxismo.eu/
• TMD exam▫ Open & close (x3)
Non-corrected deviation toward the right
▫ Joint sounds None (i.e. no clicking or crepitus)
CASE 3

1/27/2019
24
• TMD exam▫ Maximum opening without pain = 20 mm
▫ Maximum opening with pain = 21 mm
Maximum opening produced:• Pain in right pre-auricular region
CASE 3
• TMD exam▫ Right lateral = 10 mm▫ Left lateral = 4 mm WNL = ≥6 mm (including midline discrepancy)
▫ Protrusion = 4 mm WNL = 8-11 mm (including overjet)
Left lateral & protrusion produced:• Pain in right pre-auricular region
CASE 3
What are the key signs?
• Limited opening (<30mm)
• History of clicking/popping which stopped w/ onset
CASE 3
What are the key signs?
• Deviation on opening (to the right)▫ In disc displacement w/o reduction the jaw deviates
TOWARD the side of displacement▫ The opposite condyle is still able to translate normally
• Limited contralateral excursion (to the left)▫ The condyle on the side of displacement CANNOT translate
CASE 3
Problem(s) Differential DiagnosisAcute onset: • Right preauricular pain • Limited opening• Limited left excusive
movement
1) Disc displacement without reduction with limited opening (right)
2) TMJ arthralgia (right)
CASE 3

1/27/2019
25
Disc displacements
Have you ever had your jaw lock so that it won’t open all the
way, and was this limitation in jaw
opening severe enough to interfere with your ability
to eat?
Disc Displacement w/o reduction
Key differences between cases
• Maximum Opening▫ Muscle (Myofascial pain w/ limited opening) Assisted >> Unassisted No physical blockage, pain inhibits opening
▫ Disc (Disc displacement w/o reduction) Assisted = Unassisted + <35mm Displaced disc inhibits opening
Key differences between cases
• Joint noise▫ Present in ~1/3 of general population
▫ Muscle (Myofascial pain w/ limited opening) May or may not be present
▫ Disc (Disc displacement w/o reduction) Loss of click with onset of limited opening
Key differences between cases
• Pain location▫ Muscle (Myofascial pain w/ limited opening) Bilateral muscles of mastication (e.g. masseters)
▫ Disc (Disc displacement w/o reduction) Preauricular area, side of displacement (e.g. right TMJ)
IMMEDIATE GOAL:Resolve inflammatory pain
CASE 3
• Plan of Care – Conservative TMD protocol
10 3
CASE 3

1/27/2019
26
CASE 3
• Plan of Care – Pharmacotherapy▫ Piroxicam, 10mg daily for 7-10 days
Anti-inflammatory medications
• Very effective in managing Arthralgia, DJD, & pain related to acute trauma ▫ E.g. sprain/strain, trauma, post-dental work
• Corticosteroids severe arthralgia ▫ E.g. disc displacement w/0 reduction, DJD
Muscle pain is usually NOT inflammatory• NSAID serving as analgesic only
NSAID considerations
• Lowest GI side effects▫ Celebrex (Cox-2 selective)▫ Etodolac
• Relative risk of GI side effects1
▫ Ibuprofen (low dose) = 1.0▫ ASA = 1.6▫ Naproxen = 2.2▫ Piroxicam = 3.8
1) Henry et al. (Brit Med J, 1996)
• Piroxicam▫ 10mg daily▫ Once daily dosing aids in
compliance
NSAIDs (Rx)
• Piroxicam (Feldene)*▫ 10mg daily
• Meloxicam (Mobic)*▫ 7.5mg tab ▫ 5mg cap
*Once daily dosing improves compliance
• Etodolac (Lodine)▫ 200mg TID-QID
• Diclofenac (Voltaren)▫ 50mg TID (max)**
**Adverse effects limits utility
NSAIDs (OTC)
• Ibuprofen▫ 400-800 mg TID-QID▫ MAX doses
Analgesic (1200 mg/d)Anti-inflammatory (3200 mg/d)
• Naproxen▫ 220-440 mg BID▫ MAX dose (660 mg)
• Advantages▫ “Familiar”▫ Easy to find (OTC)▫ Lower side effects
NSAID considerations
1) Richy et al. (Ann Rheum Dis, 2004)
GI side effects generally take 84 days (!) to develop(1)

1/27/2019
27
• NSAID cautions/contraindications▫ Active GI ulcers/bleeding▫ Bleeding disorders or anticoagulants▫ Kidney dysfunction (dose adjustment)▫ Elderly (dose adjustment)▫ Aspirin triad (asthma, chronic urticarial, nasal polyps)▫ Pregnancy (avoid in 1st/3rd trimester; very short-term use
ibuprofen/naproxen in 2nd)
Anti-inflammatory considerations • Plan of Care – Pharmacotherapy (alternative)▫ Medrol dosepak (6 day taper)▫ Especially helpful in cases of severe arthralgia▫ DOSE IN MORNING (different than package instructions)
CASE 3
healthy.kaiserpermanente.org
Systemic corticosteroid considerations
• Adrenal suppression• Elevated blood glucose • Increased BP• Insomnia• Mood lability▫ Contraindicated in patients
with bipolar disorder, schizophrenia, severe depression, suicide risk
• Immunosuppression• GI bleeding• Decreased bone
density*• Cataracts
*Ask about bisphosphonates in patients taking long-term corticosteroids
SECONDARY GOALS:• Improve Range of Motion
• Minimize risk for recurrence
CASE 3
CASE 3
• Plan of Care – Patient education
Encourage patient that opening will improve over time
1) Disc will reduce OR 2) Posterior ligaments will remodel
• Plan of Care – Stretching exercises• Begin stretching AFTER joint pain has improved • Passive▫ Maximum opening without pain Hold 10 secs close halfway Repeat 10x
• Active▫ Evenly distributed, sustained pressure on chin/incisors▫ Tongue depressors/Popsicle sticks
CASE 3

1/27/2019
28
OTHER CONSIDERATIONS:• Predisposing factors?
• Factors influencing prognosis?
CASE 3
Problem(s) Differential DiagnosisParafunction habits 1) Stress-related (daytime)
parafunction2) Nocturnal bruxism3) Medication side effect(?)
Axis II considerations 1) Depression2) Situational anxiety3) Stress (school-related)
CASE 3
Anti-Depressants
• SSRIs have been linked to parafunctional habits (e.g. clenching & grinding)(1,2)
• Paroxetine (Paxil) & Fluoxetine (Prozac) appear to be the main offenders
CASE 3
1) Lobbezoo et al. (J Orofac Pain, 20012) Romanelli F et al. (Ann Pharmacother, 1996)
web.stanford.edu/group/hopes/cgibin/hopes_test/ssris
Axis I(Physical)
Axis II(Psychosocial)
Maladaptive ThinkingDisturbed Emotions
Dysfunctional Behavior
MuscleMyalgia/MPD
DiscDisc Displacement
w/ or w/o reductionBone/Joint
DJD/OA
Dworkin, 1998
Axis I vs. Axis II
Both Axis I & II must be effectively managed or treatment will be
ineffective
• Plan of Care – Contributing factors• Address Axis II factors• Consult with psych about alternative to SSRI
CASE 3

1/27/2019
29
TMD resources
TMD - Risk factors
1) Level 1 studies• Female Gender
2) Level 2 studies• Other Chronic Pains▫ Migraines, Back Pain, TTHA, FMS, IBS
• “Axis II” Disorders▫ Depression, Somatization▫ High perceived stress
• History of TraumaDrangsholt and LeResche (Epidemiology of TMD, 2012)
TMD - Risk factors
Other traditional risk factors have lower association/levels of evidence
• Nocturnal bruxism• Occlusal interferences• Class II/III occlusion• Joint hypermobility• Sleep dysfunction• Sexual/Physical/Emotional abuse
Drangsholt and LeResche (Epidemiology of TMD, 2012)
TMD - Indications for referral
• Moderate-to-severe psychological dysfunction or disability along with chronic pain
• Moderate-to-severe unremitting pain
• Multiple failed surgical inventions with continued chronic pain
Protocols for minimizing TMD flare related to dental care
Intervention Dose Freq. Duration
Ice 15min BID24hrs before
+ 2d after
Ibuprofen 400mg QID24hrs before
+ 2d after
Diazepam 2-5mgNight before + 1 hr prior
Frequent Breaks
Q5minor PRN
comfort
Pediatric Handpiece
PRN
http://www.rdc-tmdinternational.org/

1/27/2019
30
Medication-related osteonecrosis of the jaw (MRONJ)
1) Current or previous treatment with anti-resorptive or antiangiogenic agents;
2) Exposed bone (or bone that can be probed through a fistula) in the maxillofacial region that has persisted for more than 8 weeks; and
3) No history of radiation therapyor obvious metastatic disease to the jaws.
Medication-related osteonecrosis of the jaw (MRONJ)
© SCCA© SCCA
• Zoledronic acid (Zometa®)▫ IV Bisphosphonate▫ Inhibits osteoclast activity▫ Used to prevent hypercalcemia & decrease risk for fracture
in patients with Multiple Myeloma
1) AAOMS Position Paper (2014)2) Coleman et al. (Breast Cancer Res Treat, 2011)3) Vahtsevanos et al. (J Clin Oncol, 2009)
4) Qi et al. (Int J Clin Oncol, 2013)5) Mauri et al. (Breast Cancer Res Treat, 2009)
6) Scagliotti et al, (J Thorac Oncol, 2012)
• MRONJ risk in cancer patients exposed to Zometa®
= 50-100X higher than placebo(1)
▫ Incidence ranges from 0.7% - 6.7% (2,3)
▫ ~1% when limited to Level 1 studies(2, 4-6)
1) Fizazi et al. (Lancet, 2011)2) Stopeck et al (EJC supplements, 2009)
3) Henry (J Clin Oncol, 2011)
• Denosumab (Xgeva®)▫ RANK-L inhibitor used in the setting of bony metastasis (e.g.
breast cancer, prostate cancer) & Multiple Myeloma (approved 1/2018)
▫ MRONJ risk = comparable to Zometa®
• There are two different forms of both zoledronic acid (Zometa® & Reclast®) & denosumab (Xgeva® & Prolia®)▫ Cancer = Zometa® & Xgeva®
▫ Osteoporosis = Reclast® & Prolia®
Don’t let the name fool you…

1/27/2019
31
• Lower dose = Lower risk for MRONJ▫ “The risk for ONJ among patients [with osteoporosis] treated
with either zoledronate or denosumab (0.017 – 0.04%) approximates the risk for ONJ of patients enrolled in placebo groups (0%-0.02%)
Remember… Other medications associated with MRONJ
• VEGF inhibitors ▫ Bevacizumab (aka Avastin®)▫ Lung, colorectal, metastatic renal cancers
• Multiple tyrosine kinase inhibitors▫ Sunitinib (aka Sutent®)▫ Renal cell carcinoma
AAOMS Position Paper (2014)
Zometa® & denosumab are usually given every 3-4 weeks in cancer patients
Patients may not report on current med list if not taking daily
▫ Solid tumors with bony metastasis (esp. breast & prostate cancer)
▫ Multiple Myeloma
Don’t forget to ask…
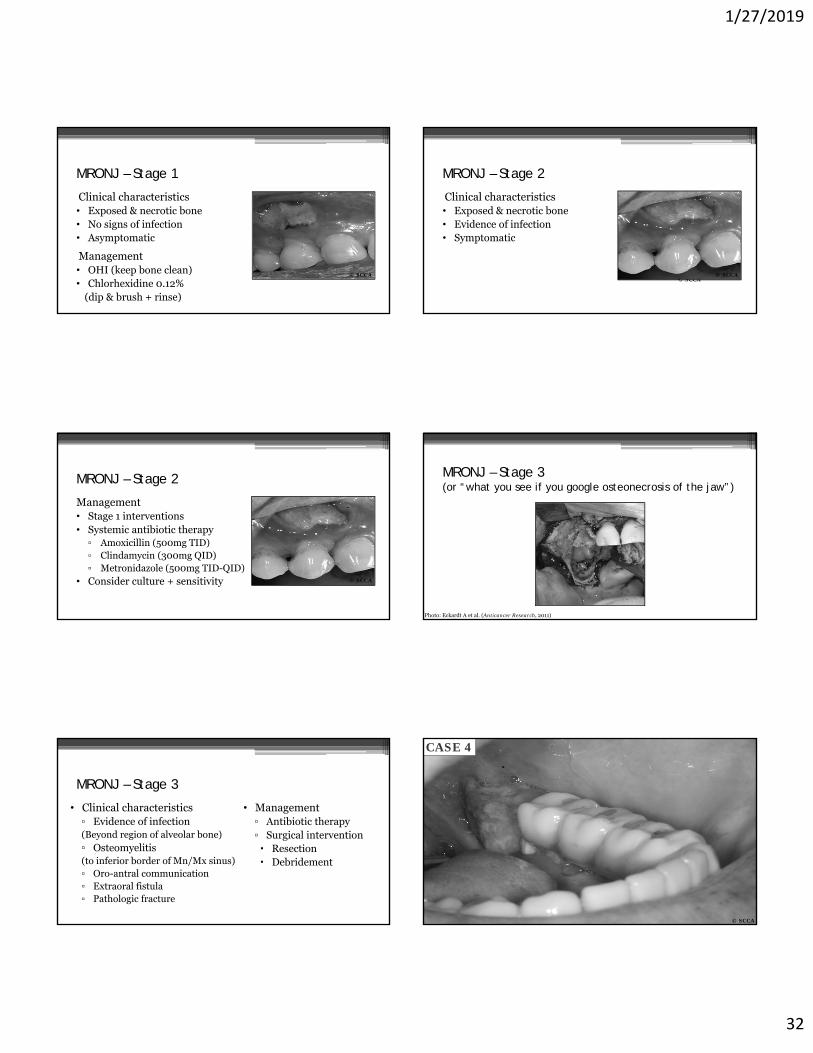
• 78-year-old Caucasian male• Stage IV metastatic prostate cancer• 3 years of denosumab therapy
© SCCA
Case
CASE 4
MRONJ - Management• Keep area as clean as possible▫ Decreases infection risk▫ Promotes “re-growth” of gingiva beneath area of exposed bone promotes sequestration
• Assess bone mobility remove mobile sequestra• Avoid invasive surgery (unless stage 3) ▫ Conservative bony re-contouring is OK▫ Recontouring is recommended in cases of trauma, excess
plaque build-up, etc.
CASE 4
MRONJ – Follow-up
Symptoms• Pain• Drainage and/or bad
taste/bad breath• Neurologic symptoms ▫ Dysesthesia, paresthesia,
numbness
Signs• Local inflammation
(erythema, edema)• Bleeding and/or purulence
on probing• Signs of progressive infection▫ Fever, lymphadenopathy,
swelling, limited openingMawardi et al. (UpToDate, 3.2018)
Monitor for:
CASE 4
1/27/2019
32
MRONJ – Stage 1
Clinical characteristics• Exposed & necrotic bone• No signs of infection• Asymptomatic
Management• OHI (keep bone clean)• Chlorhexidine 0.12%
(dip & brush + rinse)
© SCCA
MRONJ – Stage 2
Clinical characteristics• Exposed & necrotic bone• Evidence of infection• Symptomatic
© SCCA© SCCA
MRONJ – Stage 2
Management• Stage 1 interventions• Systemic antibiotic therapy ▫ Amoxicillin (500mg TID)▫ Clindamycin (300mg QID)▫ Metronidazole (500mg TID-QID)
• Consider culture + sensitivity © SCCA
MRONJ – Stage 3(or “what you see if you google osteonecrosis of the jaw”)
Photo: Eckardt A et al. (Anticancer Research, 2011)
MRONJ – Stage 3
• Clinical characteristics▫ Evidence of infection(Beyond region of alveolar bone)▫ Osteomyelitis (to inferior border of Mn/Mx sinus)▫ Oro-antral communication▫ Extraoral fistula▫ Pathologic fracture
• Management▫ Antibiotic therapy▫ Surgical intervention Resection Debridement
© SCCA
CASE 4

1/27/2019
33
Would stopping the medication be beneficial?
Drug holidays• Limited evidence for drug holidays in cancer therapy prior to
EXTs, but oncologist may consider if MRONJ present
• More likely to be effective in patient’s taking denosumab
Half-life = 6 months vs. 10-15 years
AAOMS Position Paper (2014)
• Plan of Care▫ Consult with Oncologist “Will the patient’s systemic health support a drug holiday?” Oncologist elected to hold denosumab due to active MRONJ
▫ Follow-up/assessment every 4-12 weeks based on signs & symptoms
CASE 4 CASE 4
© SCCA
CASE 4
© SCCA
CASE 4
© SCCA

1/27/2019
34
© SCCA
Mini-case
Mini-Case: 56yo female
• Stage IV Breast Cancer• 50 doses of denosumab
© SCCA
Mini-case
© SCCA
Mini-case
Oral burning disorders
Case
• 52-year-old Caucasian male
• Referred to UW Oral Medicine by Otolaryngology for evaluation & management of oral burning
• Chief concern: Continuous burning sensation, primarily in the tongue
CASE 5
History of chief concern
• Oral burning developed 2 months after left thumb surgery▫ After surgery, he was prescribed oxycodone for post-op
pain, which led to full body pruritus▫ Itching had a significant negative impact on sleep (total
duration decreased to 1.5 hours per night)▫ Oral burning developed first noticed during late
night/early morning hours
CASE 5

1/27/2019
35
• Primarily affects “tip and sides” of tongue, anterior palate, & lips
• Minimal intensity on waking; “ramps up” during the day
• Symptoms are increased with coffee, strawberries, & work stress
• Concurrent symptoms:▫ Dysguesia (“metallic”)▫ Xerostomia (“mild”)
CASE 5
• Evaluated by his PCP who prescribed Nystatin suspension for presumed candidiasis▫ Minimal benefit with the rinse
• Referred to ENT to rule out GERD
CASE 5
• Past medical history▫ Benign paroxysmal
positional vertigo▫ Anxiety▫ Depression▫ Sleep Dysfunction▫ Bilateral thumb
surgeries
• Family history▫ Non-contributory
• Social history▫ Married w/o children▫ Recycling truck driver▫ High work stress
(applying for union position)
▫ Healthy lifestyle distressed by recent health problems
CASE 5
• Medications• Nexium • Nystatin suspension▫ 1oo,ooo IU/mL▫ 5mL “swish & spit” QID
• B vitamin complex
• Adverse medication reactions▫ None▫ Environmental sensitivities
(cats, dust)
CASE 5
What are the key symptoms?
• Oral burning with well-defined, bilateral distribution
• Symptoms that are absent in the morning, but increase as the day goes on
• Acute onset during a time of high stress
• No response to topical antifungal/anti-yeast therapy
CASE 5
What tests should be performed next?
1) Inspection of the oral cavity (mucosa, gingiva, dentition)2) Cranial nerve assessment including qualitative sensory
testing of the Trigeminal nerve (Q-tip, pin prick, temperature)
3) Laboratory testing4) Advance imaging
CASE 5

1/27/2019
36
Head & neck exam▫ (-) extraoral swelling or asymmetry▫ (-) lymphadenopathy▫ (-) sinus pain (maxillary or frontal)▫ (-) salivary gland abnormality▫ (-) thyromegaly▫ (-) TMJ dysfunction▫ (-) pain in muscles of mastication or cervical muscles
CASE 5
• Intraoral exam▫ Decreased tissue wetting & salivary expression▫ Tongue hyperactivity (involuntary movement)▫ Subtle atrophy at the tip of tongue
CASE 5
Problem Differential DiagnosisContinuous burning pain-Sides & “tip” of Tongue-Anterior hard palate-Upper & Lower lip
1) Primary Burning Mouth Syndrome
2) Hyposalivation3) Atrophic Candidiasis4) Lingual parafunction5) Systemic condition (e.g. GERD, DM, hypothyroidism, nutritional deficiency)
CASE 5
Problem Differential DiagnosisPsychosocial factors impacting CC 1) Work stress
2) Health concerns3) Anxiety (suspected)4) Sleep dysfunction
• Primary insomnia• Depression (suspected)• Sleep apnea
CASE 5
1° BMS
Patton, et al. (OOOOE, 2007)Grushka, et al. (Am Fam Physician, 2002)
Unremitting
An
noy
ing
Scalded
TinglingBurning
Nu
mb
SpontaneousDis
tres
sin
g
Clinical descriptors

1/27/2019
37
Ward, R. (UW Master’s Thesis, 2014)
• Bilateral & symmetric distribution▫ “Tip” & sides of
tongue▫ Anterior palate▫ Lower lip
Location
Bergdahl et al. (J Oral Pathol Med, 1999)DaSilva et al. (Orofac Pain Rounds, 2005)
Primary Care Provider
Dermatologist
Neurologist
DentistGI Specialist
ENTPsychGrushka, et al. (Am Fam Physician, 2002) Mignogna, et al. (J Orofac Pain, 2005)
AVG 14 months & 3.1 misdiagnosesbefore reaching diagnosis of primary BMS
Mignogna, et al. (J Orofac Pain, 2005)
• Plan of Care▫ Avoid irritating substances* Hot, spicy foods Acidic foods/drinks Oral hygiene products (SLS, Pyrophosphates, flavoring agents) Alcohol (including mouthwash) Tobacco
▫ Rule out other potential causes of oral burning
*These interventions are also helpful in all mucosal diseases
CASE 5
©MGM studios
“Dry Mouth”Systemic
ConditionsParafunctional
HabitsBurning Mouth
Syndrome
Mucosal Disorders
Secondary BMS Primary
Scala et al. (Crit Rev Oral Biol Med 2003)
Rule out other potential cause of oral burning
Differential diagnosis – Hyposalivation
Treister et al. (Blood, 2012)

1/27/2019
38
Photo: c/o Dr. Win-Mei Lin
Differential diagnosis – Hyposalivation Differential diagnosis – Atrophic candidiasis
Photos: © Mark Schubert, SCCA
Differential diagnosis – Atrophic candidiasis
© Mark Schubert, SCCA
Differential diagnosis – Migratory glossitis
Will see signs of mucosal diseaseAtrophy
ErythemaStriae
Ulcerations
© OMCS
Differential diagnosis – Systemic disorders
• Diabetes mellitus(1)
• Hypothyroidism• GI problems(1,2)
▫ GERD, H. pylori infection
• Neurologic disease(1)
▫ Multiple sclerosis▫ Trigeminal neuropathies
1) Brailo, et al. (Med Oral Patol Oral Cir Bucal, 2006)2) Netto, et al. (Clin Oral Investig, 2011)
© C.D. JohnsonUT Houston
© J.E. BouquotWest Virginia Univ.
1) Klasser, et al. (JCDA, 2011)
Nutritional Deficiencies(1)
• Anemia▫ Iron▫ B vitamins
(esp. B12)• Other▫ Zinc
Differential diagnosis – Systemic disorders

1/27/2019
39
• Laboratory tests▫ Diabetes: Blood glucose, HbA1c▫ Thyroid: T3, T4, TSH▫ Vitamins: Iron, B vitamins, Zinc
www.cbslaboratories.com
Differential diagnosis – Systemic disorders Differential diagnosis – Medical therapies
• Medications(1)
▫ Anti-Hypertensives ACE inhibitors (“-prils”) Angiotensin receptor blockers
(“-sartans”) Diuretics
• Smoking cessation(2)
1) Salort-Llorca, et al. (Med Oral Patol Oral Cir Bucal, 2008)2) Gao, et al. (J Oral Pathol Med, 2009)
Differential dagnosis – Parafunctional habits
• Denture issues(1,2)
▫ Poor fit or poor design
• Tongue habits▫ Dyskinesia▫ “Checking” behaviors
1) Brown, et al. (Gen Dent, 2006)2) Svensson, et al. (J Oral Rehab, 1995)
© J.E. Bouquot
Differential diagnosis – Parafunctional habits• Clinical exam
▫ Witnessed tongue habits▫ Irritation of anterior tongue▫ “Truelove mirror test”
• “Stent” trial
© EL Truelove
• Plan of Care – Pharmacotherapy▫ Topical clonazepam (dissolve 0.5mg BID) Randomized trial (France) Dissolve 1 mg in mouth TID (spit out excess)
Gremeau-Richard (Pain, 2004)
CASE 5
• Plan of Care – Cognitive behavioral therapy▫ Randomized trial (Sweden)▫ 1 hour of CBT per week of 12-15 weeks
Intensity = 1 (endurable) to 7 (unendurable)
CASE 5
Pre-Tx Post-Tx 6mo f/u
CBT (N = 15)
5.0±0.8 2.2±1.0 1.4±1.1
Placebo (N =15)
4.3±1.7 4.6±1.7 4.7±1.2
Bergdahl et al. (J Oral Pathol Med, 1995)

1/27/2019
40
Prognosis
• 2/3s of patients experience spontaneous, partial recovery within 6-7 years(1,2)
1) Ship, et al. (JADA, 1995)2) Grushka, et al. (Am Fam Physician, 2002)
Constant episodic pain-free(1,2)
Recommended resource
World Workshop of Oral Medicine IV
Oral Surg Oral Med Oral Pathol Oral Radiol Endod2007;103(suppl 1):S39.e1-S39.e13)
• Clonazepam• Cognitive Behavioral
Therapy• Alpha-lipoic acid• Capsaicin
Thank You
David DeanEmail: [email protected]