southern california chapter healthcare financial management association chapter education program #...
TRANSCRIPT

Southern California ChapterHealthcare Financial Management Association
Chapter Education Program # 3
March 18, 2008
Long Term Care Track
Skilled Nursing FacilityAB 1629 Reimbursement Update
Darryl Nixon, CAHF
Mike Harrold, DHCS
Dan Giardinelli, DHCS

Presenter Contact Information
Darryl Nixon, Director of Reimbursement and Data Systems, California Association of Health Facilities (CAHF), [email protected], 916-441-6400, ext. 112
Mike Harrold, Chief, Financial Audits Section-Fresno, [email protected]
Dan Giardinelli, Chief, Financial Audits Section – Burbank,1405 N. San Fernando Blvd., Room 203Burbank, CA 91504, [email protected],818-295-2626

Overview/Historical Perspective
Public Policy Intent Methodology Refresher Fiscal Impact Summary Reporting Issues
– Ongoing– Supplemental Reporting
Other Issues– Rate Development Issues– QA fee Payment/Collection– Audits
Public Policy Intent
Reimbursement system needed reform because the flat rate system:– Did not promote quality.– Rewarded providers that kept or cut costs to
absolute minimums. – Did not truly recognize the cost impact of new
mandates or extraordinary cost increases (staffing, workers compensation, liability, energy).
– Did not provide resources to improve the aging infrastructure.
Methodology Refresher
New reimbursement model– Facility-specific– Labor cost driven– Sum of cost components (actual projected cost
subject to Caps)– Fair Rental Value for Property/Capital– 2 Year hold-harmless (Through 7/31/07)– Controlled by Gross Budget Caps
Fiscal Impact Summary
Average Rates 2003 = $118 + QAF $0 = $118 2004 = $125 +QAF $4 = $129 2005 = $135 + QAF $7 =$142 CAP $142 2006 = $141 + QAF $8 = $149 CAP $150 2007 = $144 + QAF $8 = $152 CAP $158 2008 = ? + QAF $9 = ? CAP $160

Reporting Issues
Cost Report Submission– Timeliness– Errors – Amended Reports
Supplemental Reports– Information Required– Timely Submission– Failure to Submit
Other Issues
Rate Development Issues– Rate Formula– Rate Review
QA fee Payment/Collection– Delinquency Follow up– Consequence
QA Fee – Legal Challenge Audits

Follow Up Issues
2007/08 Rates– Updating Rates– Retroactive Rate Adjustments– Collection of Overpayments
Share of Cost Corrections– February 20 EDS Notification
DHCS responses to Rate Issues– Subacute

Current Issues
2008/09 Rates– Supplemental Schedules– Labor Supplemental– Rate Projection
Reauthorization of AB 1629– Strategic Issues– Technical Issues
Audits

AB 1629 ReauthorizationStrategic Issues
Current Sunset Date Extension– Minimum 3 to 5 years
Funding– Global Rate CAP (s)
Improve Efficiency in Rate Determination– Cost Reporting– Rate Review (Include Audit Appeal)
Quality Award Rate Enhancement

AB 1629 Technical Issues - General
Current cost report doesn’t meet AB 1629 parameters, thus the supplemental reporting requirements.
AB 1629 Law, State Plan Amendment (SPA,) and Medi-Cal Provider bulletins don’t provide clear guidance.
Audit results impact AB 1629 rates therefore, policy guidance has to be clear.

AB 1629 ReauthorizationTechnical Issues
Resolved– Contract labor clarification– Proper classification of DON and MDS Nurse– Proper classification of Home Office capital costs
Recognition– Insurance issues– Cost Reporting
Unresolved– Liability insurance, Pharmacy consultant fees, FRVS –small
item/equipment capitalization or expense.

Audits
Audit Organization Process Overview Provider Preparation Provider Issues – Audit Perspective Provider Rights
– Ongoing communication– Exit conference– Audit appeal
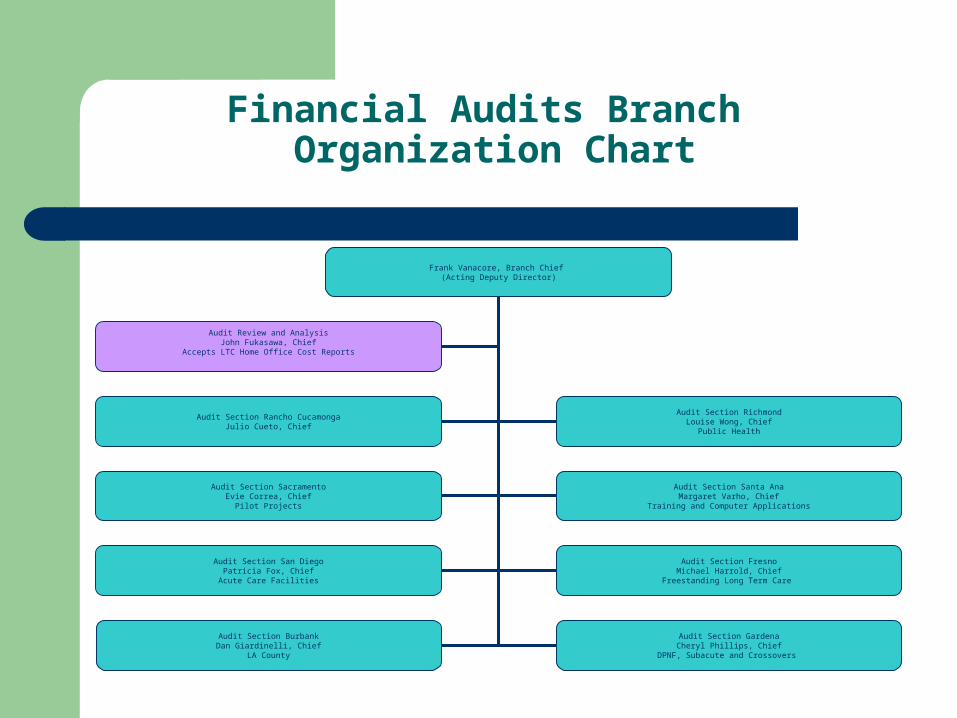
Financial Audits Branch Organization Chart
Frank Vanacore, Branch Chief (Acting Deputy Director)
Audit Section Rancho CucamongaJulio Cueto, Chief
Audit Section RichmondLouise Wong, Chief
Public Health
Audit Section SacramentoEvie Correa, Chief
Pilot Projects
Audit Section Santa AnaMargaret Varho, Chief
Training and Computer Applications
Audit Section San DiegoPatricia Fox, Chief
Acute Care Facilities
Audit Section FresnoMichael Harrold, Chief
Freestanding Long Term Care
Audit Section BurbankDan Giardinelli, Chief
LA County
Audit Section GardenaCheryl Phillips, Chief
DPNF, Subacute and Crossovers
Audit Review and AnalysisJohn Fukasawa, Chief
Accepts LTC Home Office Cost Reports
Rate Setting Process Overview
A cost report is filed and accepted by OSHPD OSHPD batches this data and sends it electronically
to FAB FAB performs audit FAB transfers audit data electronically to Rate
Development Branch (RDB) RDB Calculates Rates RDB forwards rates to EDS EDS installs rate for specific rate year
Rate Changes as a Result of AppealOverview
Office of Hearings and Appeals issues a Report of Findings
If Report of Findings results in changes to the audit, FAB issues an appeal recomputation
FAB forwards appeal recomputation to RDB RDB recalculates rate RDB forwards new rate to EDS EDS installs new rate and reprocesses claims for
dates of service within rate year the audit effected
Provider Preparation
We try to accommodate scheduling problems, but we cannot always reschedule an audit because of issuance due dates imposed upon us, thus we will not always be able to agree to a requested rescheduling of the audit.

Provider Preparation
Review the entrance letter and gather the records and materials that are identified. The following are examples:
Financial Statements General Ledger and Working Trial Balance Cash Receipts and Disbursements Journal with
Supporting Documents Working Papers and Supporting Documentation Used
in the Cost Report and/or OSHPD Report Preparation Cost Report Grouping Schedule Payroll Records

Provider Preparation
Census Report Billing Records Medi‑Cal Program Remittance Advice Details
(RADs) Billing Procedures for Share of Cost Charges Chart of Accounts and, if the facility is not using the
account numbers established by the Office of Statewide Health Planning and Development (OSHPD), a cross reference of the facility's account numbers to OSHPD's account numbers and vice versa

Provider Preparation
Please use the contact person identified on the entrance letter if there are any questions or problems; it will facilitate the audit if we can respond to questions or concerns before we go to the field
Timely submission of other requested information during the audit.
Identify contact person who will be available during the audit.

Provider Preparation
Incorporate prior year audit adjustments into current year’s filed cost report.
Freestanding Subacute facilities should properly identify the ancillary charges for the Subacute and SNF.
Provider being prepared for appeals.

Provider Issues
Reimbursement consultants and cost report preparers – You are responsible to ensure that records are
made available to the auditors, not the consultants
– If requested records are not made available the auditor will make an audit adjustment disallowing the relevant costs.

Provider Issues
The LTC Disclosure Report from OSHPD has not yet been revised to reflect the changes resulting from AB 1629
– Make the supplemental worksheets available to the auditors– The number of audit adjustments must go up to
accommodate the AB1629 reclassifications– If possible review the audit adjustments prior to the exit
conference – Carefully review the audit adjustments during the exit

Provider Issues
Cost Shifting From A&G to Skilled Nursing– Medical Directors– Admissions clerks – Software costs and other IT costs– Central Supply personnel – Telephone costs
Provider Issues
Quality Assurance Fees– Please segregate them so that they can be
easily identified by the audit staff Quality Assurance Fees are an add-on and therefore
not reimbursed based on the cost report information The objective of the audit is to segregate QAF fees
from other reimbursable costs

Provider Issues
Liability insurance please keep the following things separately identified– Liability insurance– Trust Bonds – Legal Fees– Finance Charges associated with liability
insurance– Losses and Deductibles
Provider Issues
Daily Rate Items– Please keep legend drugs separate – Please keep separately billable supplies separate– Only include things that are included in the rate

Provider Rights
Ongoing communication Exit Conference
– Title 22, Section 51021 The provider shall be afforded a reasonable opportunity to participate in an exit conference after the conclusion of any field audit or examination of records or reports of a provider…prior to the issuance of the Audit Report.
– The provider must make available to the Department any records which were identified as unavailable for review or missing within 15 calendar days of the exit conference to be included in the Audit Report.

Provider Rights
Informal Appeal Title 22, Section 51022 – A written request (Statement of Disputed Issues)
shall be filed with the Department within 60 calendar days of the receipt of the written notice of the audit or examination findings.
– Usually does not involve lawyers, the provider and the DHCS staff interact freely to resolve issues and support positions
Provider Rights
Formal Audit AppealTitle 22, Section 51024
– An Institutional provider shall have 30 calendar days following the receipt of the written Report of Findings within which to file a request for formal hearing with the Director.
– Usually but not always involves lawyers
Questions?
And
Answers