south sudan ewarn and disease surveillance … · malakal renk ogod man-awan akoka man-anguei early...
TRANSCRIPT
Early Warning and Dise
This Bulletin is produced by MOH, RSS with Technical support from WHO
Republic of South Sudan
EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN
(IDP CAMPS AND COMMUNITIES)
Week 32
General Overview
Completeness of weekly reporting in
week 32 when compared to week 3
Measles cases continue to be reported
measles vaccination is ongoing.
During week 32, Torit County in Eastern Equatoria
per 10,000) of 2.8, which represents a decline from the incidence of 29 in week 30
Hepatitis E Virus (HEV) cases in Mingkaman
[CFR] of 4.9%). During weeks 4 -
Syndrome (AJS) were reported in Bentiu, Lul,
other camps. All new AJS cases should be investigated and HEV prevention activities need to be prioritised
in all the camps.
Malaria, Acute Respiratory Infections
the highest disease risk in the Internally Displaced Persons (
During week 32, the under-5 and crude mortality rates
all the camps. Malnutrition remains the main cause of
Completeness and Timeliness of Reporting
2 1
5 68
1315
21
1720
17
0
5
10
15
20
25
30
35
40
51 52 01 02 03 04 05 06 07 08 09
Nu
mb
er
of
site
s
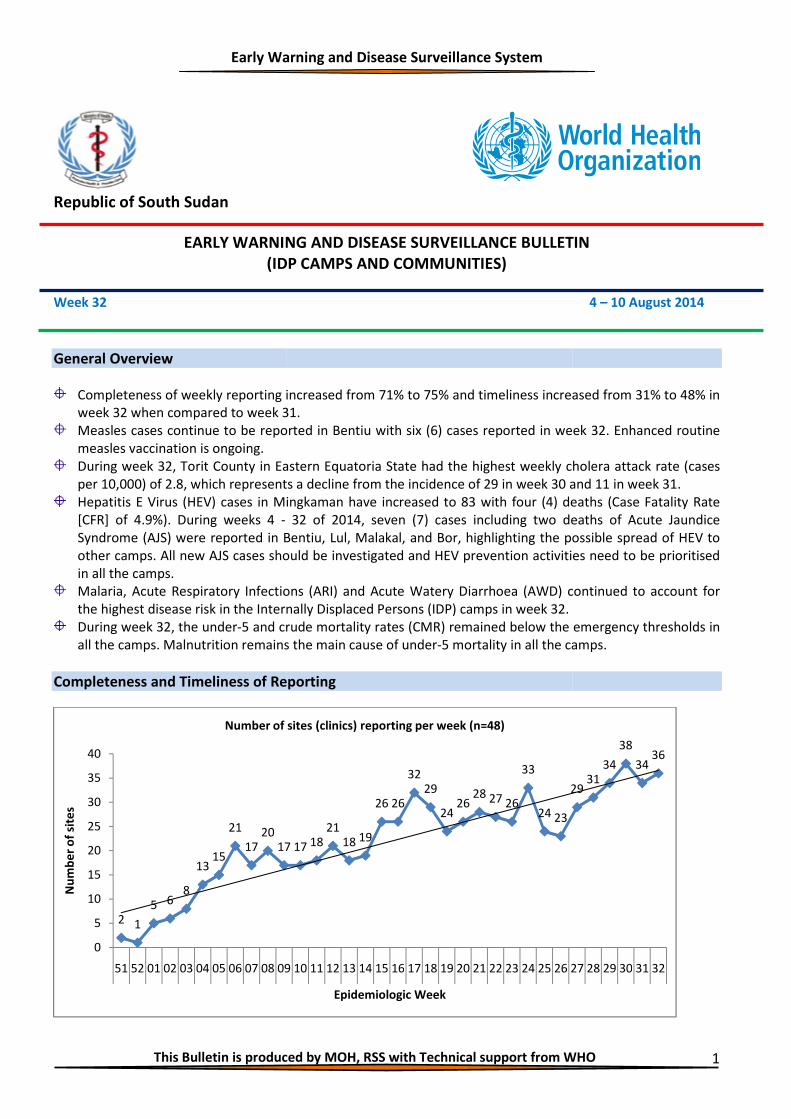
Number of sites (clinics) reporting per week (n=48)
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN
(IDP CAMPS AND COMMUNITIES)
increased from 71% to 75% and timeliness increased from 3
31.
reported in Bentiu with six (6) cases reported in week
in Eastern Equatoria State had the highest weekly cholera
, which represents a decline from the incidence of 29 in week 30 and 11 in week 31
Mingkaman have increased to 83 with four (4) deaths
32 of 2014, seven (7) cases including two death
reported in Bentiu, Lul, Malakal, and Bor, highlighting the possible spread of HEV to
All new AJS cases should be investigated and HEV prevention activities need to be prioritised
Acute Respiratory Infections (ARI) and Acute Watery Diarrhoea (AWD) continue
Internally Displaced Persons (IDP) camps in week 32.
and crude mortality rates (CMR) remained below the emergency thr
Malnutrition remains the main cause of under-5 mortality in all the camp
Completeness and Timeliness of Reporting
17 17 1821
18 19
26 26
3229
2426
28 27 26
33
24 23
29
09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Epidemiologic Week
Number of sites (clinics) reporting per week (n=48)
This Bulletin is produced by MOH, RSS with Technical support from WHO 1
EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN
4 – 10 August 2014
creased from 31% to 48% in
in week 32. Enhanced routine
cholera attack rate (cases
and 11 in week 31.
deaths (Case Fatality Rate
deaths of Acute Jaundice
ng the possible spread of HEV to
All new AJS cases should be investigated and HEV prevention activities need to be prioritised
continued to account for
remained below the emergency thresholds in
rtality in all the camps.
2931
34
38
3436
27 28 29 30 31 32
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
2
Completeness of weekly reporting increased from 34 (71%) in week 31, to 36 (75%) in week 32. Similarly,
timeliness for weekly reporting increased from 15 (31%) in week 31 to 23 (48%) in week 32.
Health facilities are reminded to submit their IDP consultation and mortality reports by COB on Monday.
Consultations (All patients seen at Outpatient and Inpatient)
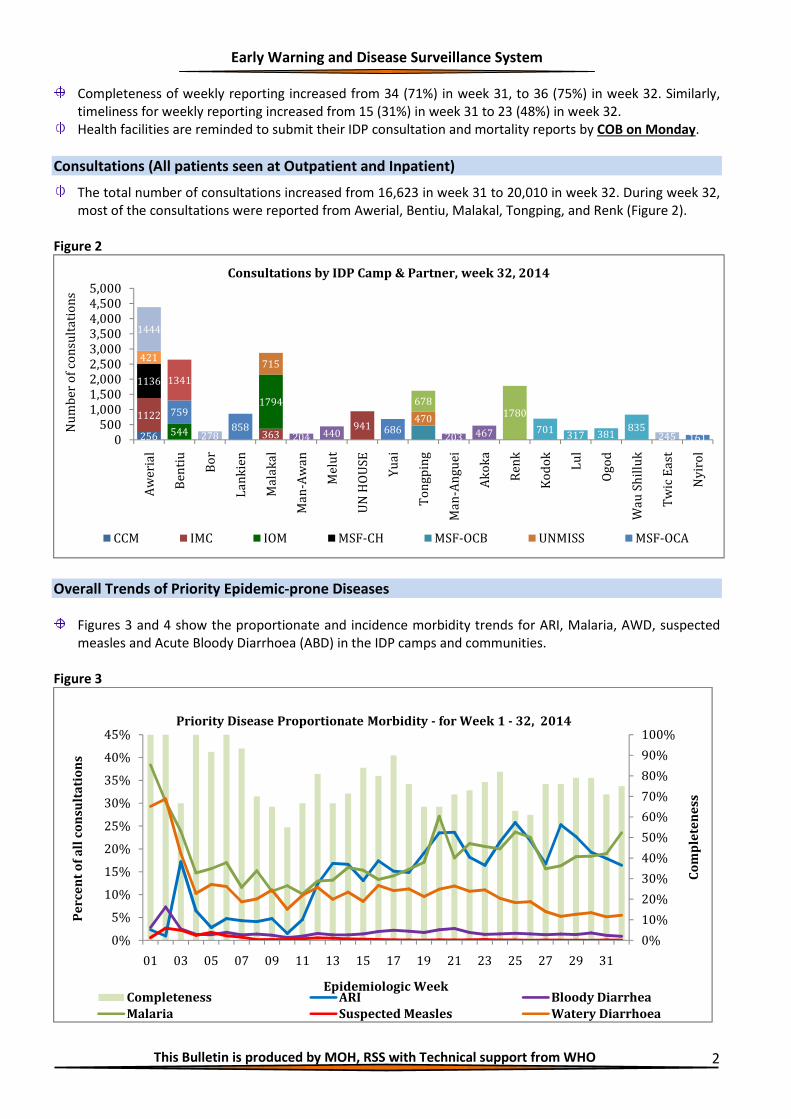
The total number of consultations increased from 16,623 in week 31 to 20,010 in week 32. During week 32,
most of the consultations were reported from Awerial, Bentiu, Malakal, Tongping, and Renk (Figure 2).
Figure 2
Overall Trends of Priority Epidemic-prone Diseases
Figures 3 and 4 show the proportionate and incidence morbidity trends for ARI, Malaria, AWD, suspected
measles and Acute Bloody Diarrhoea (ABD) in the IDP camps and communities.
Figure 3
256
1122
363941
544
1794
1136
715
470759
858 686161
1341
6781780
204 440 203 467 701317 381
835
421
1444
278 2450500
1,0001,5002,0002,5003,0003,5004,0004,5005,000
Aw
eri
al
Be
nti
u
Bo
r
La
nk
ien
Ma
lak
al
Ma
n-A
wa
n
Me
lut
UN
HO
US
E
Yu
ai
To
ng
pin
g
Ma
n-A
ng
ue
i
Ak
ok
a
Re
nk
Ko
do
k
Lu
l
Og
od
Wa
u S
hil
luk
Tw
ic E
ast
Ny
iro
l
Nu
mb
er
of
con
sult
ati
on
s
Consultations by IDP Camp & Partner, week 32, 2014
CCM IMC IOM MSF-CH MSF-OCB UNMISS MSF-OCA
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss
Pe
rce
nt
of
all
co
nsu
lta
tio
ns
Epidemiologic Week
Priority Disease Proportionate Morbidity - for Week 1 - 32, 2014
Completeness ARI Bloody Diarrhea
Malaria Suspected Measles Watery Diarrhoea
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
3
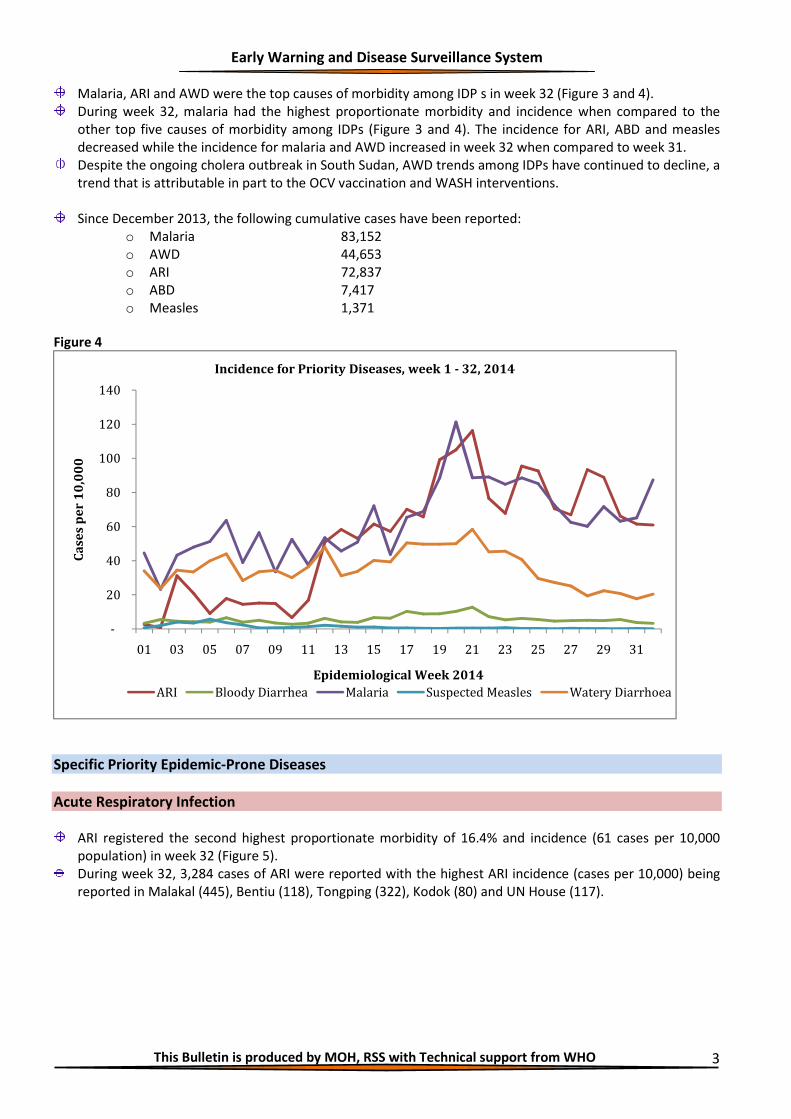
Malaria, ARI and AWD were the top causes of morbidity among IDP s in week 32 (Figure 3 and 4).
During week 32, malaria had the highest proportionate morbidity and incidence when compared to the
other top five causes of morbidity among IDPs (Figure 3 and 4). The incidence for ARI, ABD and measles
decreased while the incidence for malaria and AWD increased in week 32 when compared to week 31.
Despite the ongoing cholera outbreak in South Sudan, AWD trends among IDPs have continued to decline, a
trend that is attributable in part to the OCV vaccination and WASH interventions.
Since December 2013, the following cumulative cases have been reported:
o Malaria 83,152
o AWD 44,653
o ARI 72,837
o ABD 7,417
o Measles 1,371
Figure 4
Specific Priority Epidemic-Prone Diseases
Acute Respiratory Infection
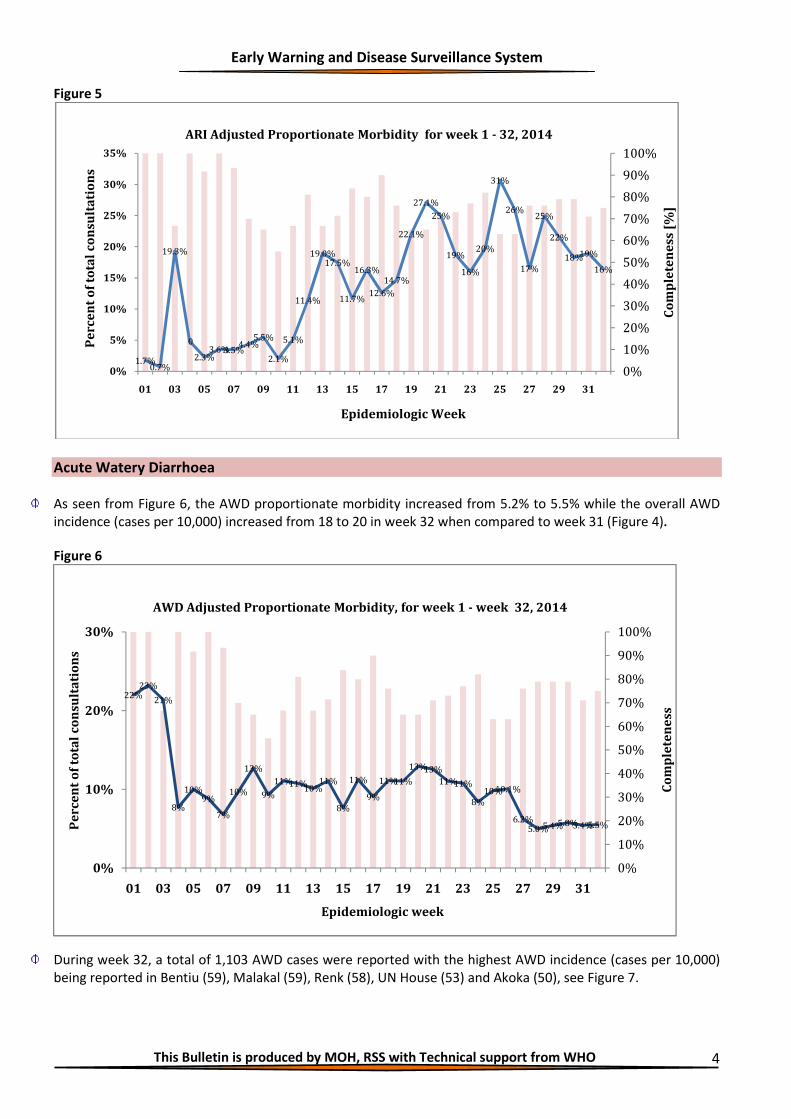
ARI registered the second highest proportionate morbidity of 16.4% and incidence (61 cases per 10,000
population) in week 32 (Figure 5).
During week 32, 3,284 cases of ARI were reported with the highest ARI incidence (cases per 10,000) being
reported in Malakal (445), Bentiu (118), Tongping (322), Kodok (80) and UN House (117).
-
20
40
60
80
100
120
140
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Ca
ses
pe
r 1
0,0
00
Epidemiological Week 2014
Incidence for Priority Diseases, week 1 - 32, 2014
ARI Bloody Diarrhea Malaria Suspected Measles Watery Diarrhoea
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
4
Figure 5
Acute Watery Diarrhoea
As seen from Figure 6, the AWD proportionate morbidity increased from 5.2% to 5.5% while the overall AWD
incidence (cases per 10,000) increased from 18 to 20 in week 32 when compared to week 31 (Figure 4).
Figure 6
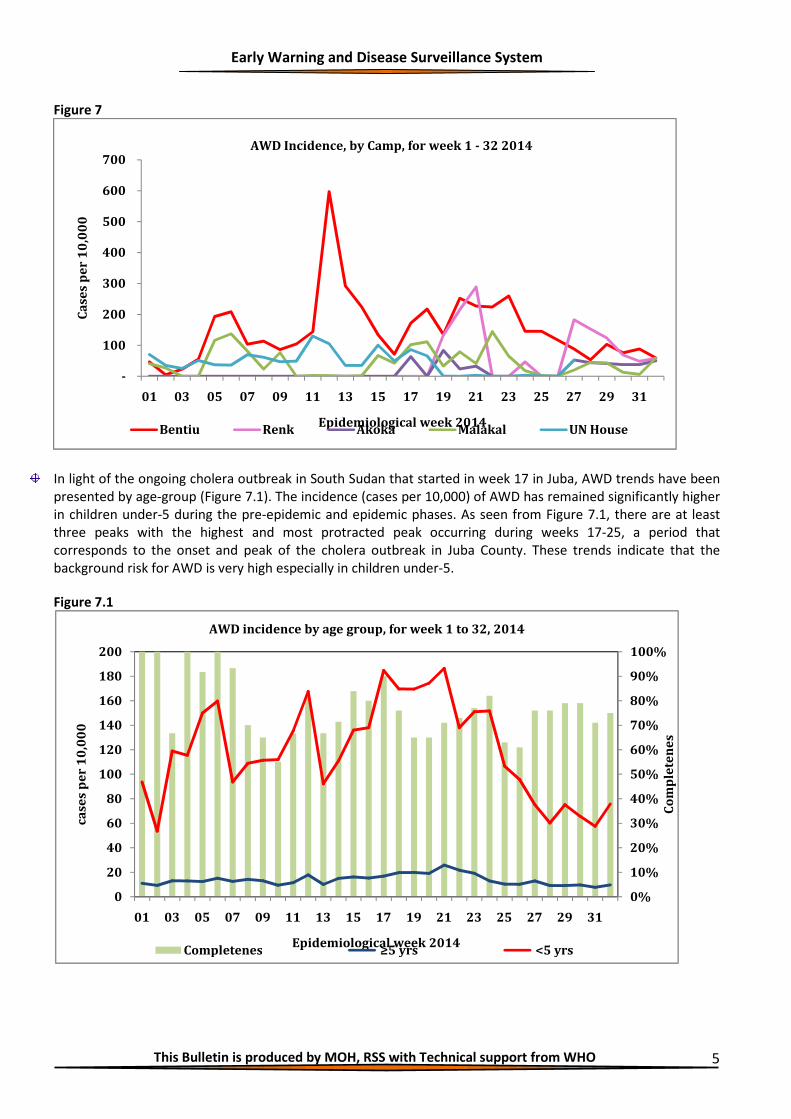
During week 32, a total of 1,103 AWD cases were reported with the highest AWD incidence (cases per 10,000)
being reported in Bentiu (59), Malakal (59), Renk (58), UN House (53) and Akoka (50), see Figure 7.
1.7%0.7%
19.3%
0
2.3%3.6%3.5%
4.4%5.5%
2.1%
5.1%
11.4%
19.0%17.5%
11.7%
16.3%
12.6%
14.7%
22.1%
27.1%
25%
19%
16%
20%
31%
26%
17%
25%
22%
18%19%
16%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
5%
10%
15%
20%
25%
30%
35%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss [
%]
Pe
rce
nt
of
tota
l c
on
sult
ati
on
s
Epidemiologic Week
ARI Adjusted Proportionate Morbidity for week 1 - 32, 2014
22%23%
21%
8%
10%9%
7%
10%
13%
9%
11%11%10%
11%
8%
11%
9%
11%11%
13%13%
11%11%
8%
10%10.1%
6.2%5.0%5.4%5.8%5.4%5.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
10%
20%
30%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss
Pe
rce
nt
of
tota
l c
on
sult
ati
on
s
Epidemiologic week
AWD Adjusted Proportionate Morbidity, for week 1 - week 32, 2014
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
5
Figure 7
In light of the ongoing cholera outbreak in South Sudan that started in week 17 in Juba, AWD trends have been
presented by age-group (Figure 7.1). The incidence (cases per 10,000) of AWD has remained significantly higher
in children under-5 during the pre-epidemic and epidemic phases. As seen from Figure 7.1, there are at least
three peaks with the highest and most protracted peak occurring during weeks 17-25, a period that
corresponds to the onset and peak of the cholera outbreak in Juba County. These trends indicate that the
background risk for AWD is very high especially in children under-5.
Figure 7.1
-
100
200
300
400
500
600
700
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Ca
ses
pe
r 1
0,0
00
Epidemiological week 2014
AWD Incidence, by Camp, for week 1 - 32 2014
Bentiu Renk Akoka Malakal UN House
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0
20
40
60
80
100
120
140
160
180
200
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
s
ca
ses
pe
r 1
0,0
00
Epidemiological week 2014
AWD incidence by age group, for week 1 to 32, 2014
Completenes ≥5 yrs <5 yrs
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
6
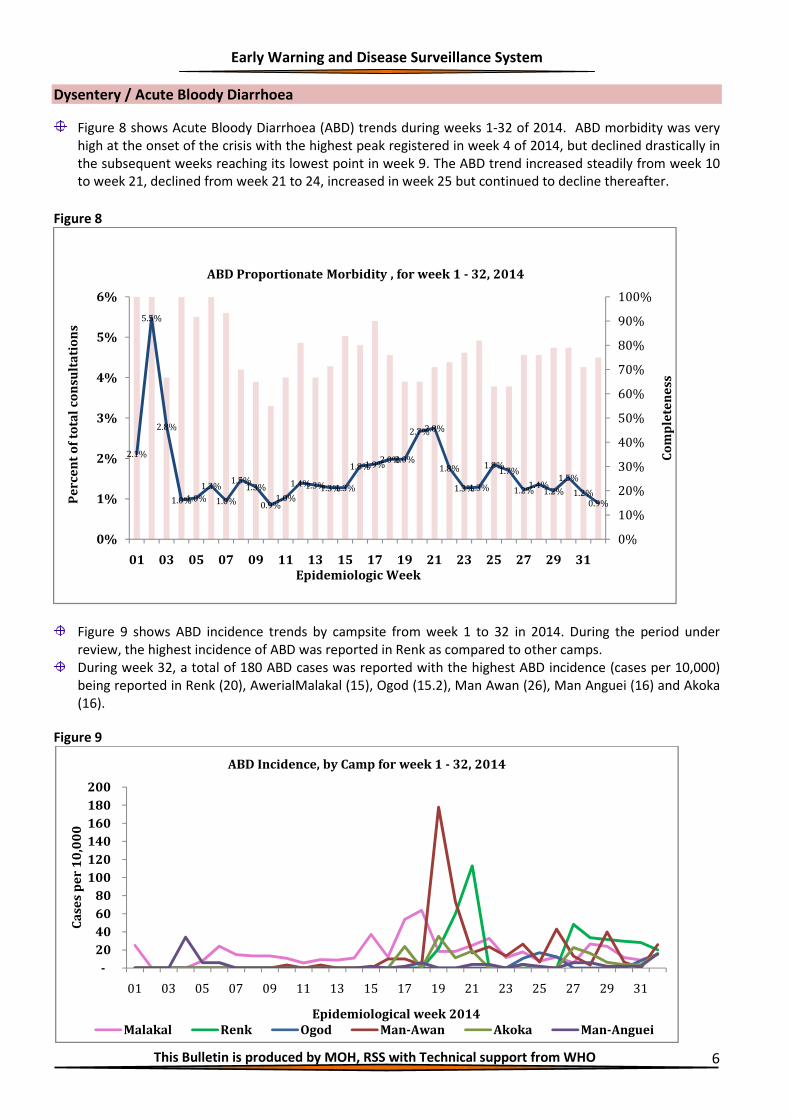
Dysentery / Acute Bloody Diarrhoea
Figure 8 shows Acute Bloody Diarrhoea (ABD) trends during weeks 1-32 of 2014. ABD morbidity was very
high at the onset of the crisis with the highest peak registered in week 4 of 2014, but declined drastically in
the subsequent weeks reaching its lowest point in week 9. The ABD trend increased steadily from week 10
to week 21, declined from week 21 to 24, increased in week 25 but continued to decline thereafter.
Figure 8
Figure 9 shows ABD incidence trends by campsite from week 1 to 32 in 2014. During the period under
review, the highest incidence of ABD was reported in Renk as compared to other camps.
During week 32, a total of 180 ABD cases was reported with the highest ABD incidence (cases per 10,000)
being reported in Renk (20), AwerialMalakal (15), Ogod (15.2), Man Awan (26), Man Anguei (16) and Akoka
(16).
Figure 9
2.1%
5.5%
2.8%
1.0%1.0%
1.3%
1.0%
1.5%1.3%
0.9%1.0%
1.4%1.3%1.3%1.3%
1.8%1.9%2.0%2.0%
2.7%2.8%
1.8%
1.3%1.3%
1.8%1.7%
1.2%1.4%
1.2%
1.5%
1.2%0.9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
1%
2%
3%
4%
5%
6%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss
Pe
rce
nt
of
tota
l c
on
sult
ati
on
s
Epidemiologic Week
ABD Proportionate Morbidity , for week 1 - 32, 2014
-
20
40
60
80
100
120
140
160
180
200
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Ca
ses
pe
r 1
0,0
00
Epidemiological week 2014
ABD Incidence, by Camp for week 1 - 32, 2014
Malakal Renk Ogod Man-Awan Akoka Man-Anguei

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
7
Measles
Figure 10
The measles trend peaked at the beginning of the crisis with the highest peak occurring in week 3, followed
by a declining trend with subsequently shorter peaks in week 5 and 13 (Figure 10). This trend is attributed
to a series of reactive measles vaccination campaigns conducted to contain the outbreaks in UN House,
Tongping IDP camp, Bor, Yuai, Lankien, Cueibet, and in Thol Payam (Nyirol) County, Jonglei State.
During week 32, a total of eight (8) measles cases were reported with six (6) cases being reported from
Bentiu, while Awerial reported two (2) cases.
In response to the measles cases in Bentiu, accelerated routine measles vaccination is being implemented.
An integrated measles and Polio vaccination campaign is slated for 18 August 2014 in Chotbora and Wudier
Payam, Longochuk County in Upper Nile State with support from MedAir. The target population is 50,000.
Malaria
Figure 11
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
1%
2%
3%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss
Pe
rc
en
t o
f to
tal
co
nsu
lta
tio
ns
Epidemiologic week
Suspected Measles Proportionate Morbidity, for week 1 - 32 2014
Completeness Suspected Measles Adj.
28.8%
22.8%
26.8%
11.1%12.8%12.8%
9.3%
16.3%
12.4%
16.3%
11.4%12.0%
14.8%16.7%
13.7%12.5%11.8%
15.4%
19.7%
31.3%
19.1%
21.8%20.0%
18.3%
28.2%26.8%
15.5%16.1%17.4%17.5%
20.0%
23.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
5%
10%
15%
20%
25%
30%
35%
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Co
mp
lete
ne
ss
Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic week
Suspected Malaria Adjusted Proportionate Morbidity , week 1 - 32 2014
Completeness Malaria Adj.
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
8
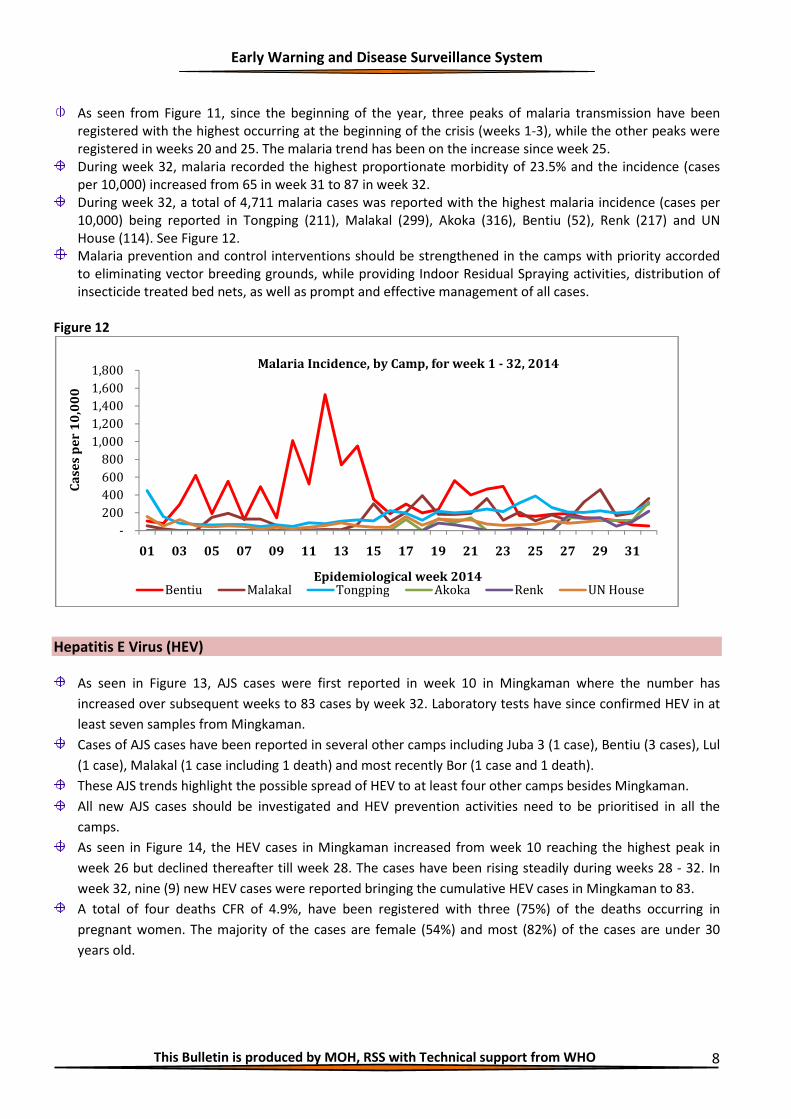
As seen from Figure 11, since the beginning of the year, three peaks of malaria transmission have been
registered with the highest occurring at the beginning of the crisis (weeks 1-3), while the other peaks were
registered in weeks 20 and 25. The malaria trend has been on the increase since week 25.
During week 32, malaria recorded the highest proportionate morbidity of 23.5% and the incidence (cases
per 10,000) increased from 65 in week 31 to 87 in week 32.
During week 32, a total of 4,711 malaria cases was reported with the highest malaria incidence (cases per
10,000) being reported in Tongping (211), Malakal (299), Akoka (316), Bentiu (52), Renk (217) and UN
House (114). See Figure 12.
Malaria prevention and control interventions should be strengthened in the camps with priority accorded
to eliminating vector breeding grounds, while providing Indoor Residual Spraying activities, distribution of
insecticide treated bed nets, as well as prompt and effective management of all cases.
Figure 12
Hepatitis E Virus (HEV)
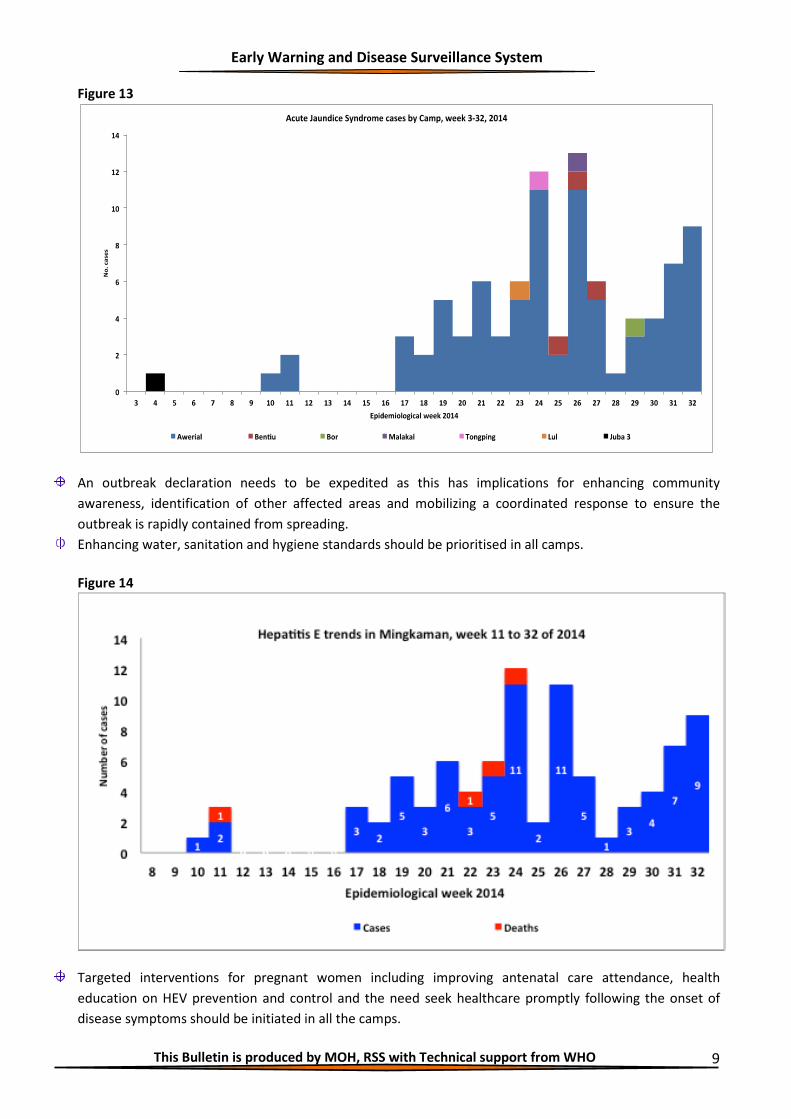
As seen in Figure 13, AJS cases were first reported in week 10 in Mingkaman where the number has
increased over subsequent weeks to 83 cases by week 32. Laboratory tests have since confirmed HEV in at
least seven samples from Mingkaman.
Cases of AJS cases have been reported in several other camps including Juba 3 (1 case), Bentiu (3 cases), Lul
(1 case), Malakal (1 case including 1 death) and most recently Bor (1 case and 1 death).
These AJS trends highlight the possible spread of HEV to at least four other camps besides Mingkaman.
All new AJS cases should be investigated and HEV prevention activities need to be prioritised in all the
camps.
As seen in Figure 14, the HEV cases in Mingkaman increased from week 10 reaching the highest peak in
week 26 but declined thereafter till week 28. The cases have been rising steadily during weeks 28 - 32. In
week 32, nine (9) new HEV cases were reported bringing the cumulative HEV cases in Mingkaman to 83.
A total of four deaths CFR of 4.9%, have been registered with three (75%) of the deaths occurring in
pregnant women. The majority of the cases are female (54%) and most (82%) of the cases are under 30
years old.
-
200
400
600
800
1,000
1,200
1,400
1,600
1,800
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31
Ca
ses
pe
r 1
0,0
00
Epidemiological week 2014
Malaria Incidence, by Camp, for week 1 - 32, 2014
Bentiu Malakal Tongping Akoka Renk UN House
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
9
Figure 13
An outbreak declaration needs to be expedited as this has implications for enhancing community
awareness, identification of other affected areas and mobilizing a coordinated response to ensure the
outbreak is rapidly contained from spreading.
Enhancing water, sanitation and hygiene standards should be prioritised in all camps.
Figure 14
Targeted interventions for pregnant women including improving antenatal care attendance, health
education on HEV prevention and control and the need seek healthcare promptly following the onset of
disease symptoms should be initiated in all the camps.

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
10
Cholera
The Ministry of Health, working with partners, rolled out a comprehensive response to the cholera outbreak
that started in Juba in week 17 of 2014. The national cholera taskforce is coordinating the implementation of
comprehensive interventions for cholera prevention and control. By the close of week 32, a total of 5,682
cholera cases including 123 deaths (CFR 2.16%) had been reported from five (5) states and 12 counties in South
Sudan (table 1). The outbreak has declined in Juba County but satellite outbreaks have been reported in 11
other counties.
Table 1: Cholera Statistics by County, South Sudan, week 17-32, 2014
No. State County
New cases by epi-week Cumulative
No. cases
2014
Cumulative
No. Deaths
Case
Fatality Rate
[%}
28
29
30
31
32
1.0
CES
(IDP)
Juba - Tongping
UNMISS
4
7
3
4 0 70 3 4.3
2.0
Juba - Juba 3
UN House
8
12
19
5 2 85 - -
3.0
CES
Juba
57
40
22
23 14 2,002 36 1.8
4.0 Kajo-Keji
5
-
10
5 1 70 4 5.7
5.0 Yei River
-
-
-
- 0 47 2 4.3
6.0 JS Bor
-
-
-
- 0 1 - -
7.0
EES
Torit
414
271
400
156 39 1,955 37 1.9
8.0 Lopa-Lafon
4
24
17
23 31 164 9 5.5
Kapoeta North
11
6
12
3 2 68 1 1.5
9.0 Magwi
20
28
13
21 15 208 10 4.8
10.0
UNS
Manyo
-
-
- 0 1 - -
11.0 Malakal
302
59
53
7 15 1,008 21 2.1
12.0 WES Mundri East
-
-
- 3 - -
Total South Sudan
825
447
549
247 119 5,682 123 2.2
Figure 15 shows the cumulative attack rates (cases per 10,000) for cholera with the most affected counties
being Torit (141.6), Malakal (68.4) and the two IDP camps in Juba County.
During week 32, Torit had the highest weekly attack rate for cholera of 2.8 cases per 10,000, which
represents a significant decline from the attack rate of 11.3 cases per 10,000 registered during week 31
(Figure 16).
These trends highlight the need to enhance and sustain the recommended interventions for cholera
prevention and control.

Early Warning and Dise
This Bulletin is produced by MOH, RSS with Technical support from WHO
Figure15
The sustained transmission of cholera in Eastern Equatoria
coverage for social mobilisation, WASH, and early case
oral rehydration points, and at the designated cholera treatment centres.
Figure 16
48.0 49.0 40.5
2.6
-
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0 Ju
ba
-T
on
gp
ing
UN
MIS
S
Jub
a -
Jub
a 3
UN
Ho
use
Jub
a
Ka
jo-K
eji
Ca
ses
pe
r 1
0,0
00
Cumulative attack rate for cholera by county, week 17
Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
ed transmission of cholera in Eastern Equatoria State calls for enhanced efforts to improve the
, WASH, and early case identification and initiation of treatment at home
oral rehydration points, and at the designated cholera treatment centres.
2.6 1.8 0.1
141.6
12.5 5.8 10.3
0.2 Y
ei
Riv
er
Bo
r
To
rit
Lo
pa
-La
fon
Ka
po
eta
No
rth
Ma
gw
i
Ma
ny
o
Cumulative attack rate for cholera by county, week 17-32, 2014
This Bulletin is produced by MOH, RSS with Technical support from WHO 11
calls for enhanced efforts to improve the
and initiation of treatment at home,
68.4
0.5
Ma
lak
al
Mu
nd
ri E
ast
32, 2014

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
12
Acute Flaccid Paralysis (AFP)
During week 32, no new AFP cases were reported from the IDP camps although nine cases were reported from
rest of the population living outside the camps. Since the beginning of 2014, a cumulative of 161 AFP cases has
been notified (Table 2). The annualised non-Polio AFP (NPAFP) rate is 3.18 cases per 100,000 population
children 0-14 years (national target ≥4 per 100,000 children 0-14 years). Only four(40%) of the states, namely
Lakes, Western Bahr el Ghazal, Eastern Equatoria and Western Equatoria have attained the targeted NPAFP rate
(Table 2). The non-Polio Enterovirus (NPEV) isolation rate (a measure of the quality of the specimen cold chain)
is 13%, which is above the national target of ≥10%. Stool adequacy is 90%, a rate that is higher than the national
target of ≥80% (Table 2).
Table 2: Summary of AFP indicators by state for 2013 and 2014
Other diseases of public health importance
There were no new cases of Guinea Worm or Viral Haemorrhagic Fever (VHF) reported during week 32.
In response to the escalating global threat of Ebola virus disease, the following actions have been prioritised
to enhance preparedness and response in South Sudan:
o A multi-sectoral national taskforce has been established to coordinate the response;
o A national contingency plan has been developed to facilitate the mobilisation of resources and
implementation of activities to improve readiness;
o A health screening desk has been established at Juba International Airport and this will be escalated
to other major border entry points;
o Isolation facilities have been designated at Juba Teaching Hospital and UNMISS;

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
13
o Additional state level activities are planned and are well articulated in the contingency plan.
All-Causes Mortality Data
During week 32, mortality lists were received from Mingkaman, Juba 3, Bentiu, Tongping, Bor and Malakal.
A total of eight (8) deaths were reported in week 32; with the majority 6 (75%) of the deaths reported from
Bentiu, one from Malakal and one from Tongping. During week 32, four (50%) of the deaths occurred in
children under five years of age. The major causes of death during week 32 are shown in the table below:
Table 2: Causes of death by IDP camp during week 32 of 2014
Deaths by camp & cause
Deaths by age-group
Total deaths <5yrs ≥5yrs
Bentiu 3 3 6
Tuberculosis 1 1
Unknown 2 2
SAM 2 2
Septic burns 1 1
Malakal 1 1
Kala azar/anaemia 1 1
Tomping 1 1
Perinatal death 1 1
Total deaths 4 4 8
Under-5 Mortality Rate
The under-5 mortality rates (U5MR) from week 51 of 2013 to week 32 of 2014 are shown in Figure 17. A
decline in under-5 mortality rates was observed in all IDP camps except from weeks 21 to 26 in Bentiu.
During week 32, the under-5 mortality for Bentiu was 0.53 deaths per 10,000 per day, which is lower than
the emergency threshold of 2 deaths per 10,000 per day. The major cause of death in under-5 year olds in
week 32 was Severe Acute Malnutrition (SAM), see Table 2.
Figure 17
0
2
4
6
8
10
12
14
16
18
51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33
Ra
te p
er
10
,00
0
Epidemiologic Week
Under-5 Mortality by Site - week 51 of 2013 to week 32 of 2014
Bentiu Bor Juba 3 Malakal

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
14
Crude Mortality Rate
The crude mortality rates (CMR) for week 32 are shown in Figure 18. During week 32, the CMR was below
the emergency threshold for the six camps that submitted mortality statistics.
Figure 18
Disease specific mortality
Acute watery diarrhoea related deaths
Figure 19
0
1
2
3
4
5
6
7
8
52 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32
Ra
te p
er
10
,00
0
Epidemiologic week
Crude Mortality Rate per 10,000 persons per day, week 51 of 2013 to week 32 of
2014
Bentiu Bor Juba 3 Malakal
Mingkaman Tongping Melut Threshold
0
5
10
15
20
25
51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 18 19 20 22 21 23 24 25 26 27 28
2013 2014
No
. de
ath
s
Epidemiological week 2014
AWD Deaths by Camp week 51 of 2013 to week 32 of 2014
Bentiu Bor Juba 3 Malakal Mingkaman Tomping

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
15
Figure 19 shows mortality due to AWD from week 52 in 2013 to week 32 in 2014. No new AWD deaths have
been reported since week 28 of 2014. AWD has caused the highest number of deaths with a cumulative of 140
deaths since the onset of the crisis. The majority of AWD related deaths have been reported from Mingkaman,
Tongping, Malakal and Bentiu.
Overall Mortality
Since the onset of the crisis, at least 1,033 deaths have been reported from the IDP camps. Children under five
years of age have accounted for 526 (51%) of the deaths. The majority of the deaths occurred in Tongping,
Bentiu, Malakal and Bor. The top causes of mortality during the period included AWD, measles, severe
pnuemonia and malnutrition (Table 3).
Table 3
Camp TB
SA
M
Pn
eu
mo
nia
Pe
rin
ata
l
de
ath
Me
asl
es
Ma
tern
al
de
ath
Ma
lari
a
Gu
nsh
ot
wo
un
d
Blo
od
y
dia
rrh
oe
a
Acu
te w
ate
ry
dia
rrh
oe
a
AJS
Oth
ers
Gra
nd
To
tal
Bentiu 7 44 37 2 10 11 6 2 43 104 266
Bor 2 3 9 2 42 1 2 58 119
Juba 3 4 3 6 11 1 3 1 5 1 14 49
Malakal 13 14 2 8 8 38 27 1 99 210
Melut 1 3 3 1 2 7 9 26
Mingkaman 3 2 8 7 4 1 7 4 30 6 44 116
Tomping 1 14 20 15 37 9 6 2 32 109 245
(Blank) 1 0 1
Kodok 1 0 1
Grand Total 31 83 86 46 94 3 46 51 8 140 8 437 1033
General recommendations
Consolidate cholera response interventions in the 12 counties where cholera has been confirmed and
enhance epidemic readiness and prevention in the rest of the counties.
Alerts of suspected cholera should be reported to the Ministry of Health cholera alert desk by calling
0912000098.
Obtain stools samples from all new suspect cases in the IDP camps to allow microbiological culturing.
Scale up coverage for social mobilization and WASH interventions in Eastern Equatorial State where
cholera trends have remained persistently high.
Submit biological samples to allow laboratory confirmation of emerging outbreaks of suspect measles,
AJS and cholera.
Partners are urged to strengthen public health prevention and control measures for malaria, ARI, AWD
(including cholera), ABD and HEV.
Please send all disease surveillance information and any outbreak rumours to
IDSR reports and mortality line lists should be submitted by COB Monday after the close of each
epidemiologic week.

Early Warning and Disease Surveillance System
This Bulletin is produced by MOH, RSS with Technical support from WHO
16
For comments or questions, please contact
Department of Epidemics, Preparedness and Response, MoH-RSS
E-mail: [email protected],
HF radio frequency: 8015 USP; Selcall: 7002