solid tumors reveal their secrets - sciencemag.org slides_solid tumors... · brought to you by the...
TRANSCRIPT
Change the size of any window by dragging the lower right corner. Use controls in top right corner to close or maximize each window.
What each widget does:
Facebook login
if you need help
shows speaker bios
download slides and more info
LinkedIn login
shows slide window
opens the Ask a Question box
Twitter login (#ScienceWebinar)
search Wikipedia
shows the audio media player
Solid Tumors Reveal Their SecretsPredictive and Prognostic Evidence from Copy Number Analysis
Instructions for Viewers
Webinar Series

Brought to you by the Science/AAAS Custom Publishing Office
Sponsored by:
June 11, 2014
Participating Experts
Solid Tumors Reveal Their SecretsPredictive and Prognostic Evidence from Copy Number Analysis
Webinar Series
Paul C. Boutros, Ph.D.Ontario Institute for Cancer ResearchToronto, Canada
Ajay Pandita, D.V.M., Ph.D.Core DiagnosticsPalo Alto, CA
3
Copy-Number Based Biomarkers for Intermediate
Risk Prostate Cancer
Dr. Paul C. BoutrosOntario Institute for Cancer Research
June 12, 2014
4
Problem Formulation
CPC-GENE: A Prostate Cancer ICGC Intra-tumoural Heterogeneity Inter-tumoural Heterogeneity
Pathway
5
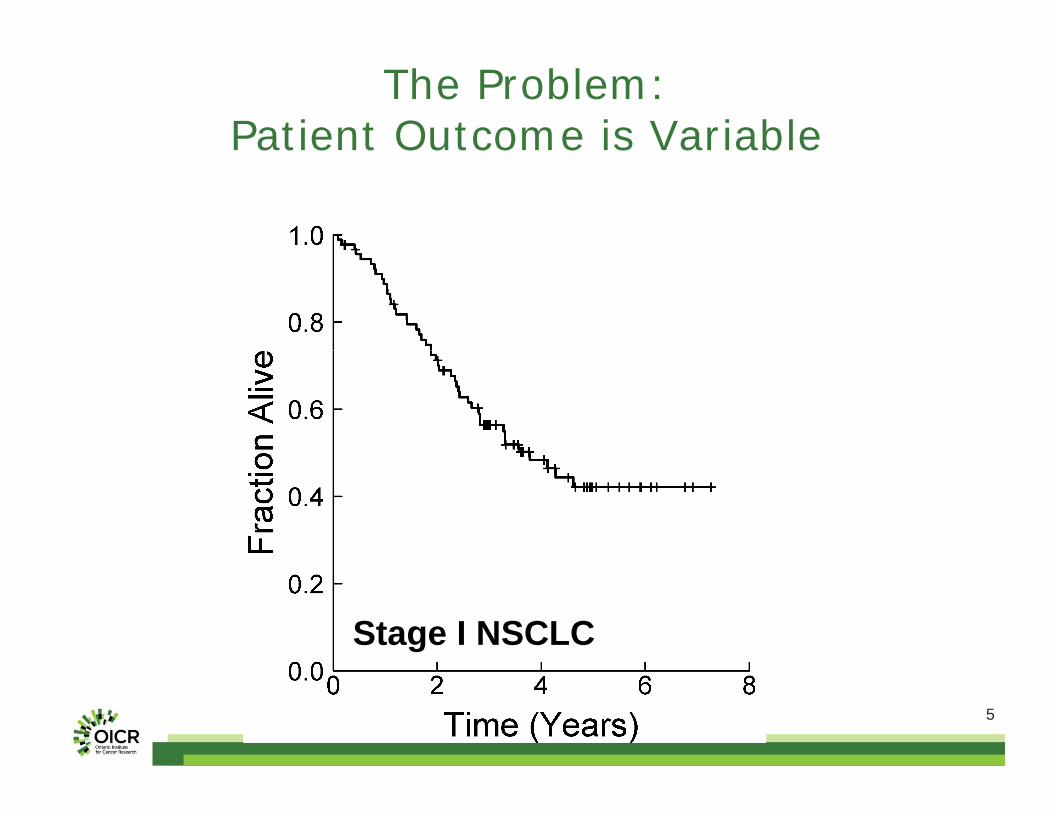
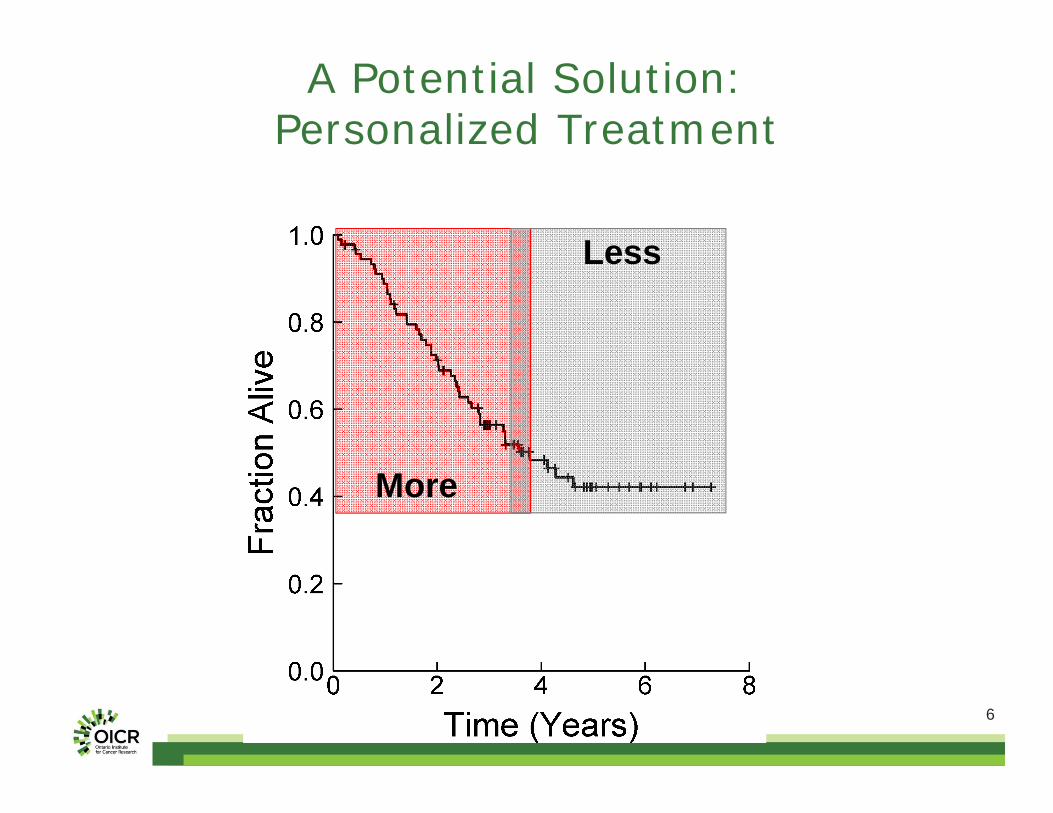
The Problem:Patient Outcome is Variable
Stage I NSCLC
6
A Potential Solution:Personalized Treatment
More
Less
7
The (Old) Hypothesis
There are a small number of distinct tumour subtypes.
Which each have distinct molecular profiles.
And distinct prognoses.
Pattern Discovery Techniques
8
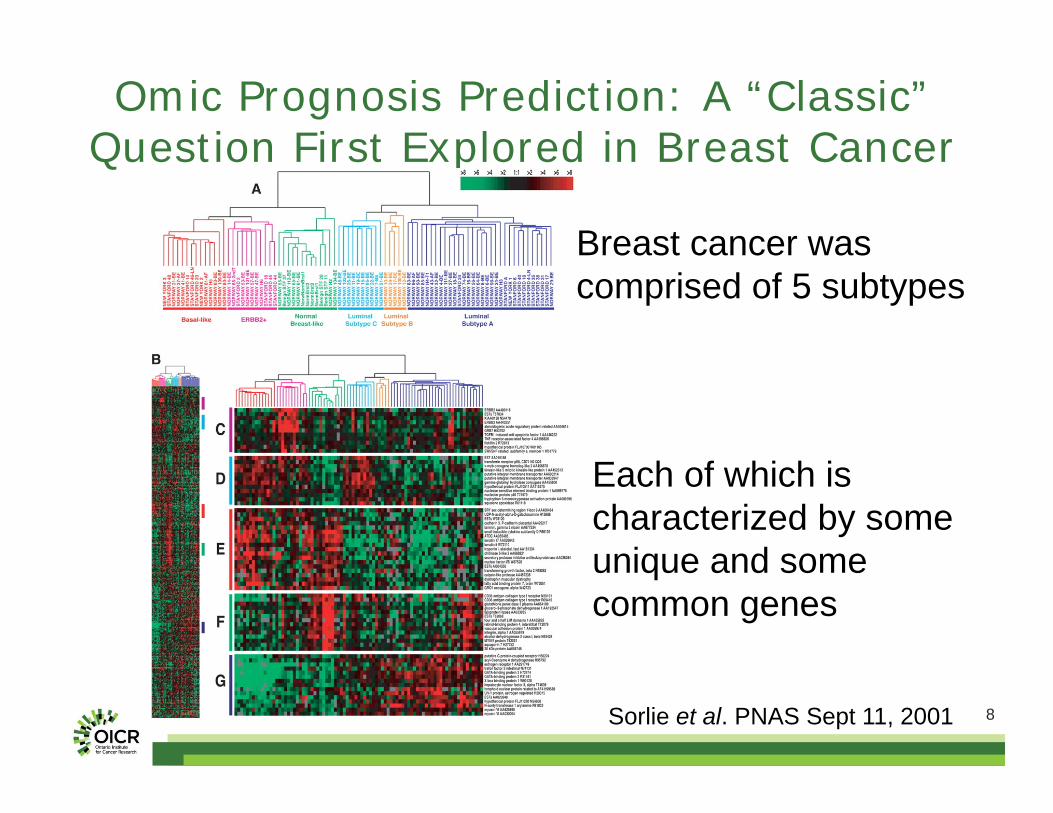
Omic Prognosis Prediction: A “Classic” Question First Explored in Breast Cancer
Sorlie et al. PNAS Sept 11, 2001
Breast cancer was comprised of 5 subtypes
Each of which is characterized by some unique and some common genes
9
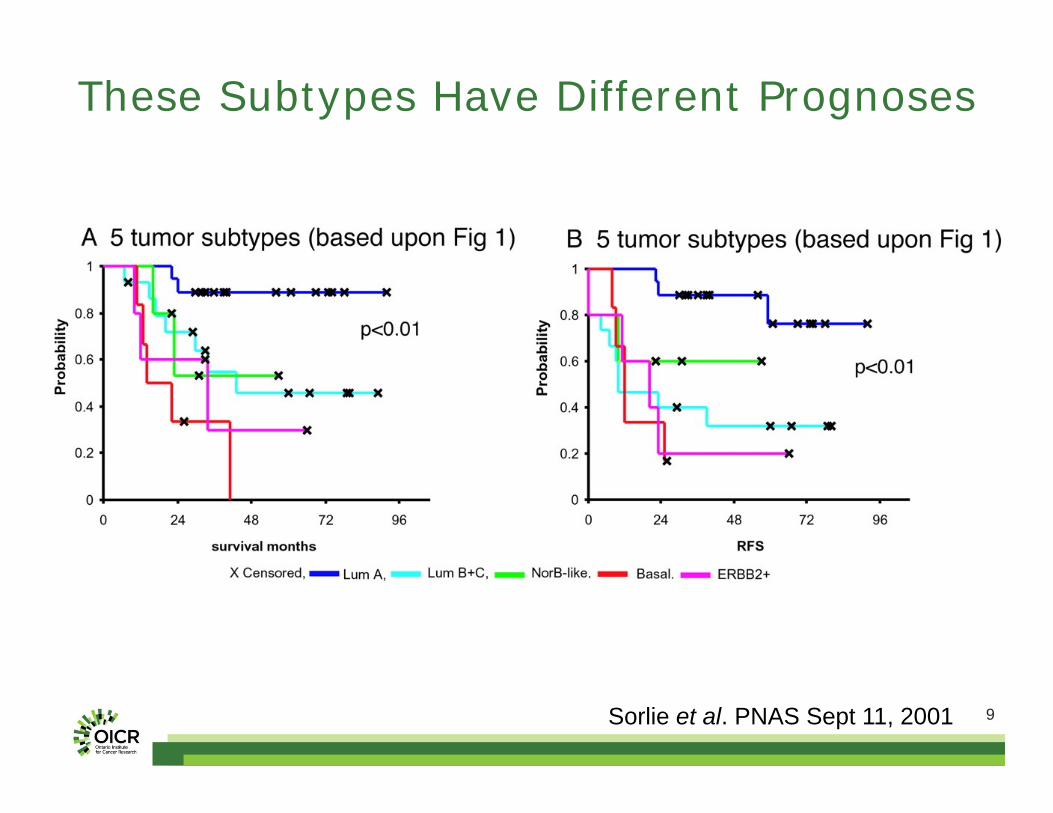
These Subtypes Have Different Prognoses
Sorlie et al. PNAS Sept 11, 2001
10
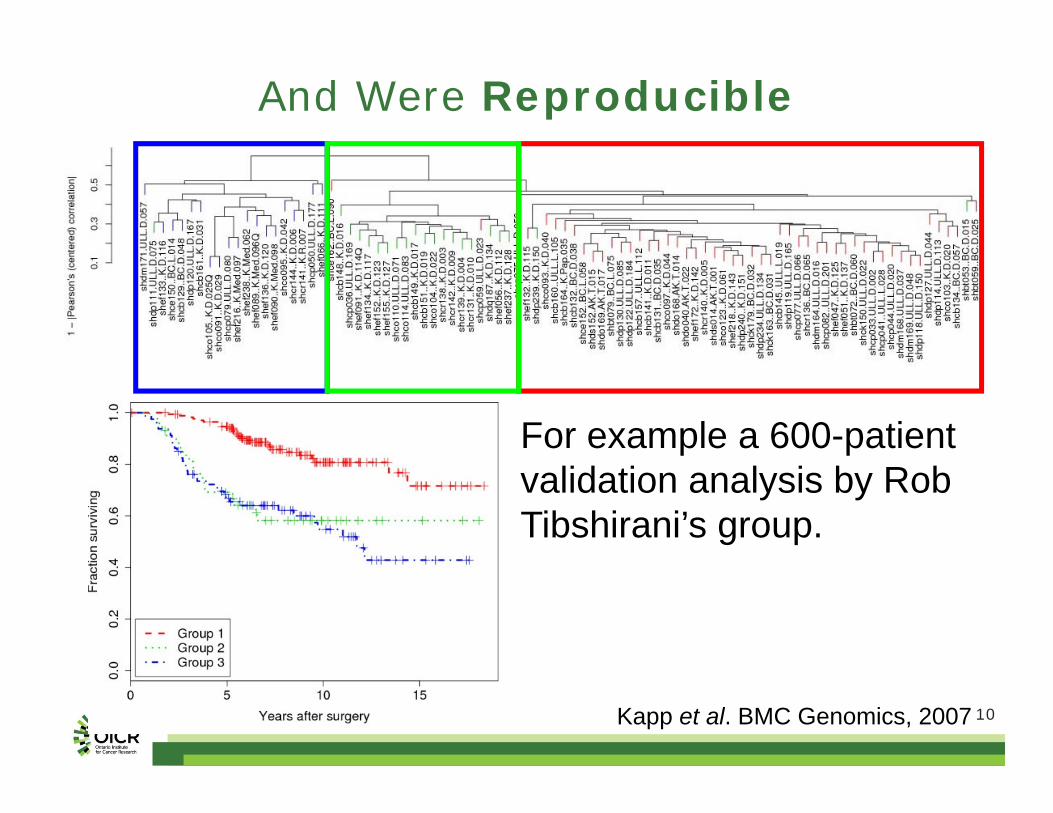
And Were Reproducible
Kapp et al. BMC Genomics, 2007
For example a 600-patient validation analysis by Rob Tibshirani’s group.
11
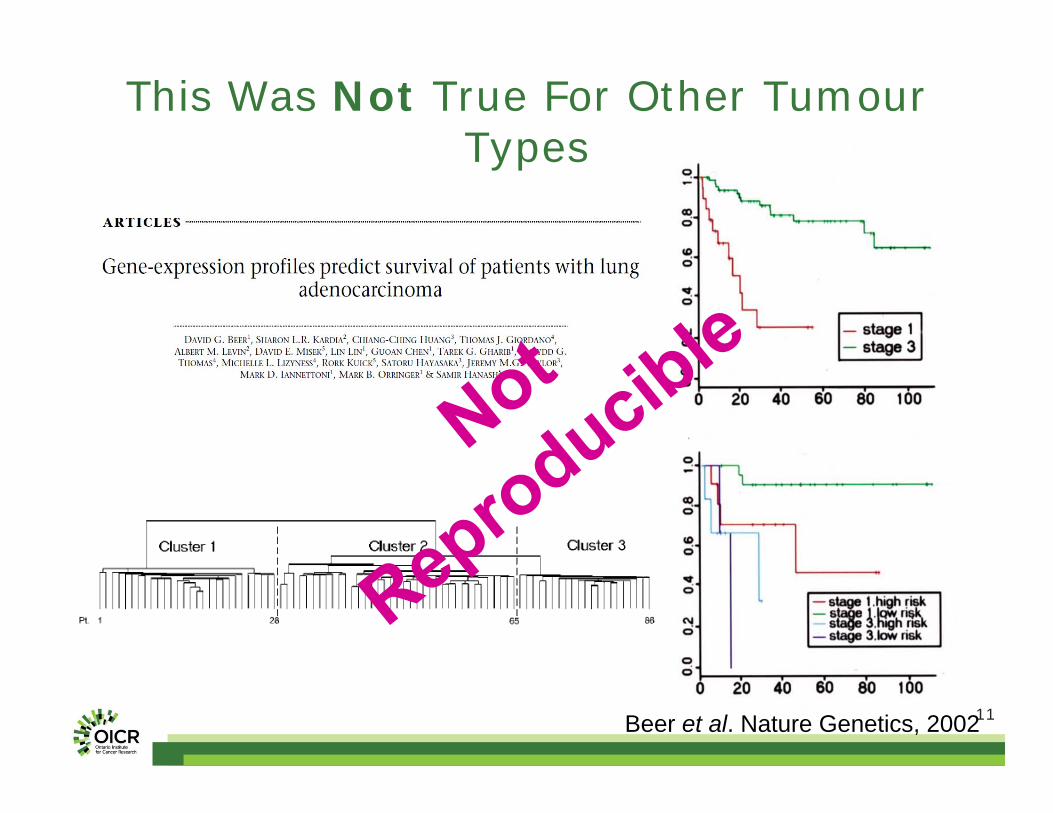
This Was Not True For Other Tumour Types
Beer et al. Nature Genetics, 2002
12
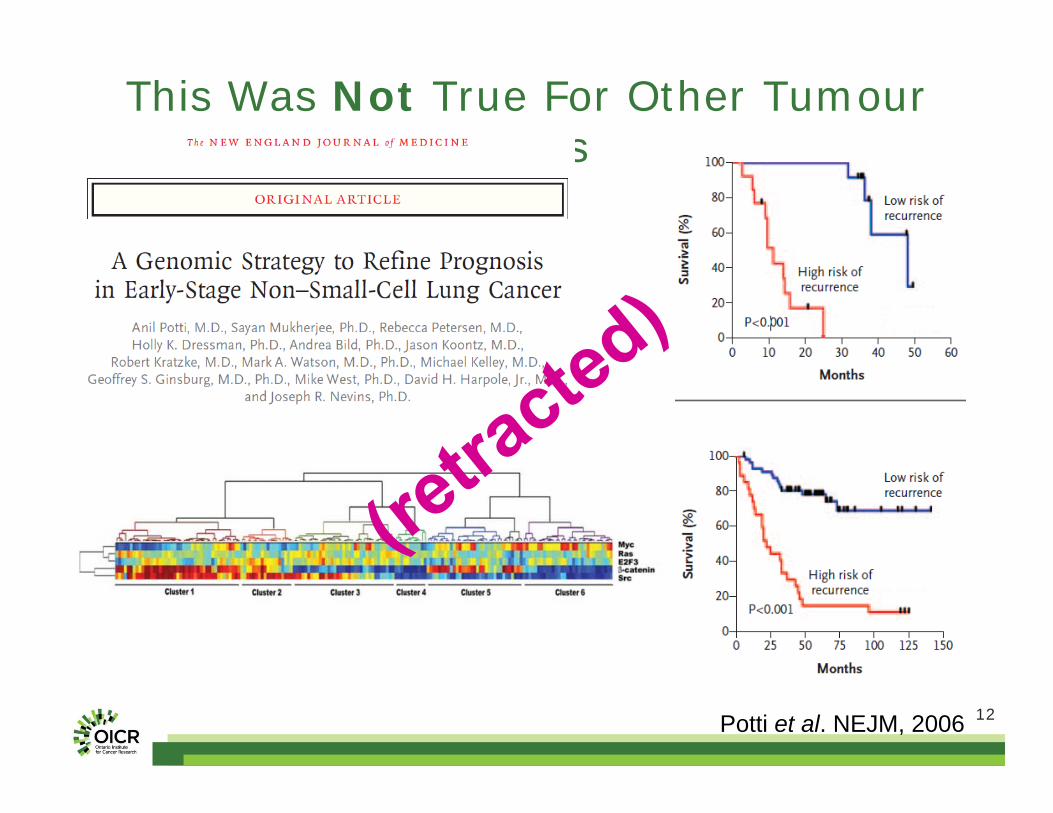
This Was Not True For Other Tumour Types
Potti et al. NEJM, 2006
13
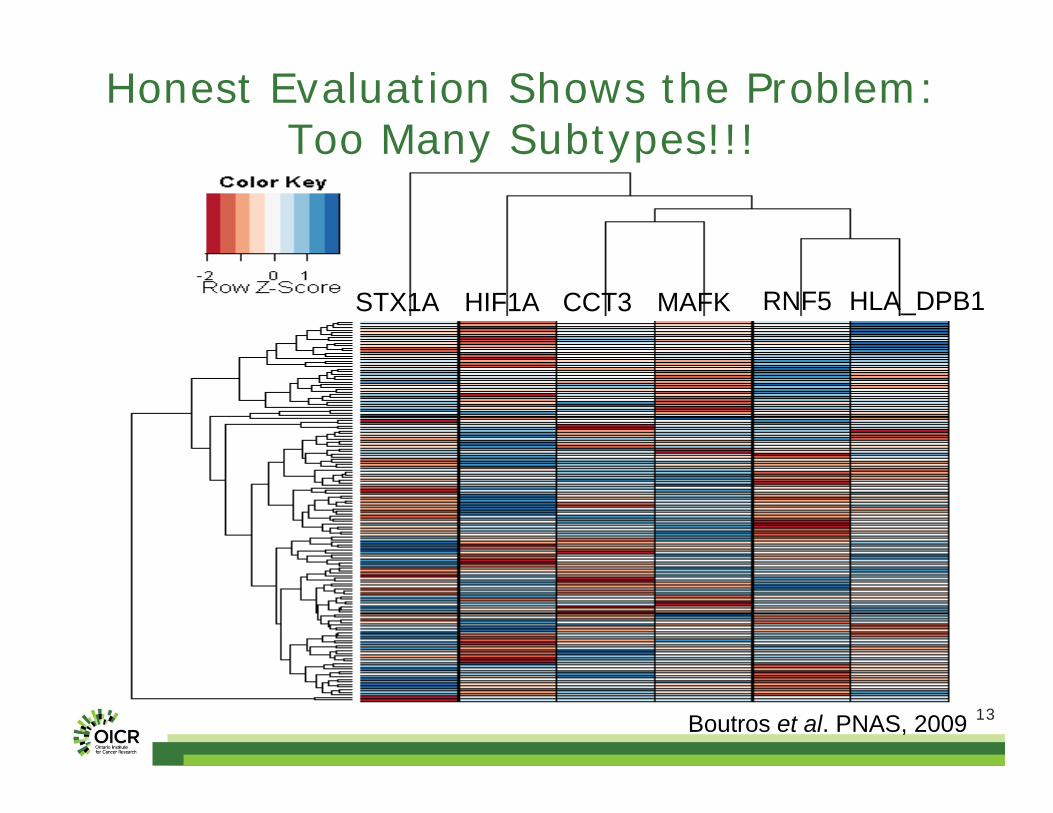
Honest Evaluation Shows the Problem:Too Many Subtypes!!!
STX1A HIF1A CCT3 HLA_DPB1RNF5MAFK
Boutros et al. PNAS, 2009
14
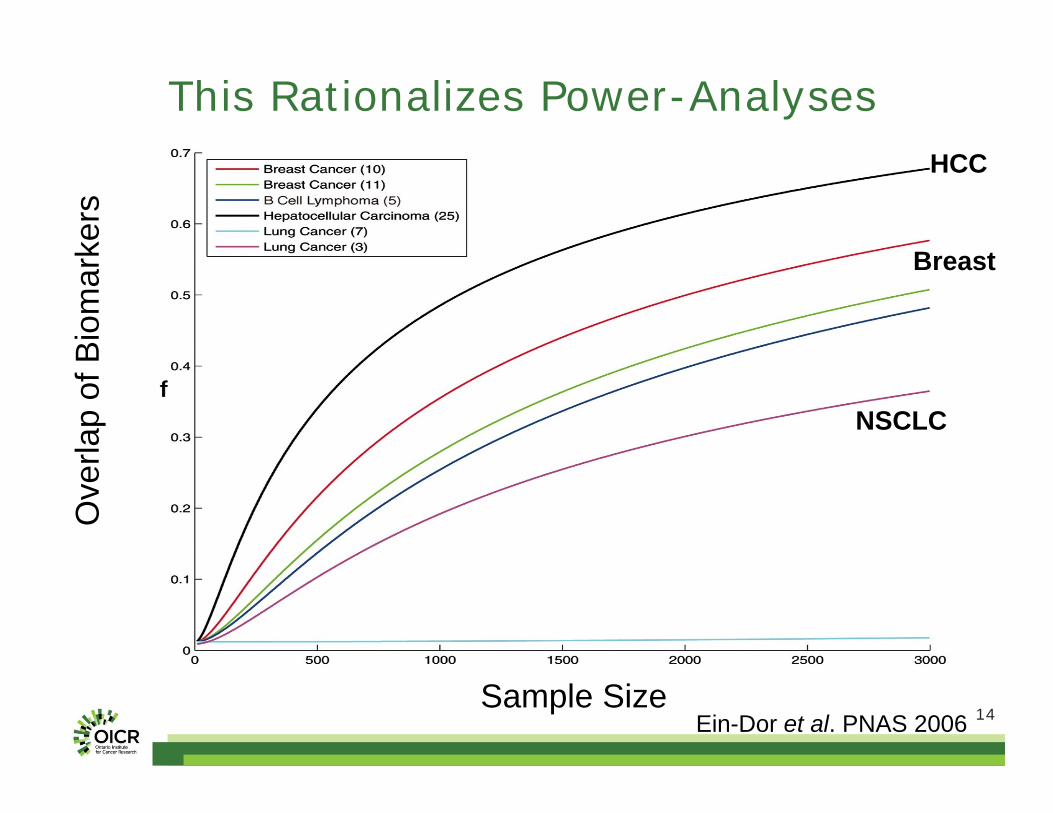
This Rationalizes Power-Analyses
Sample Size
Ove
rlap
of B
iom
arke
rs
Ein-Dor et al. PNAS 2006
NSCLC
HCC
Breast
15
The (New) Hypothesis
There are a large number of distinct tumour subtypes.
Which have overlapping molecular profiles.
And distinct prognoses.
Machine Learning Techniques

16
Four years of research into machine-learning methods later…
Our mRNA-based markers reached theoretical maximums. Major
improvements are unlikely.
99.98%
Boutros et al. PNAS, 2009
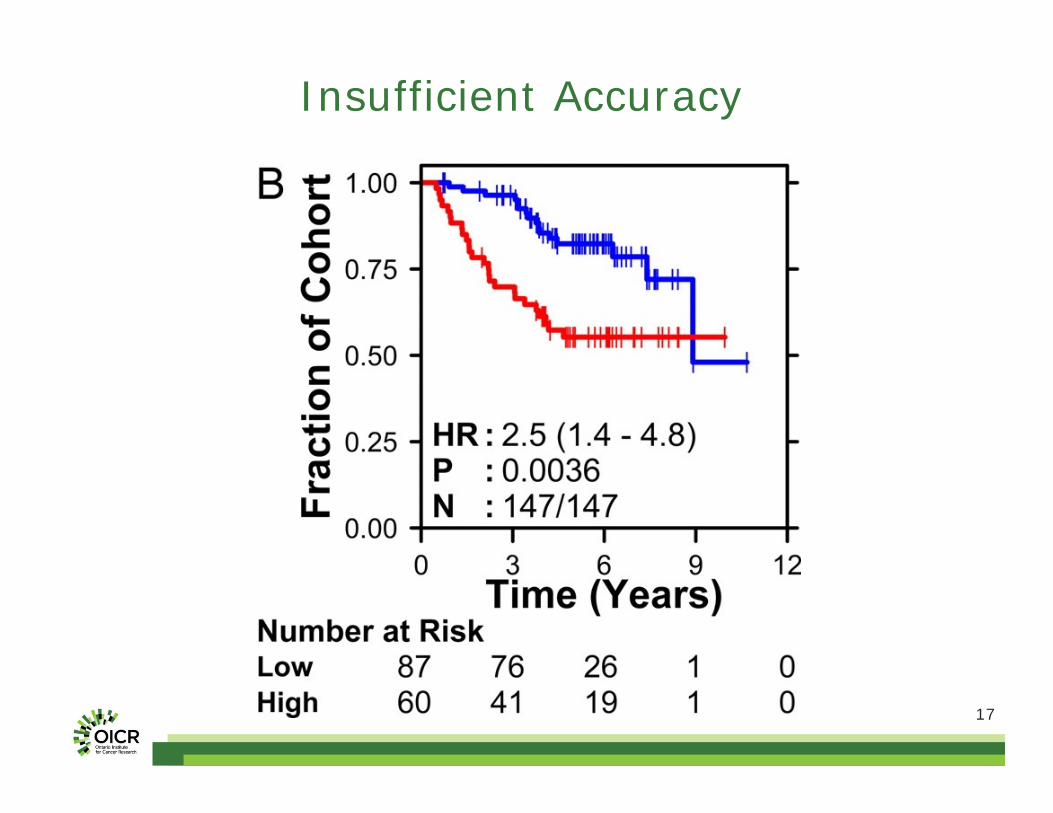
17
Insufficient Accuracy
18
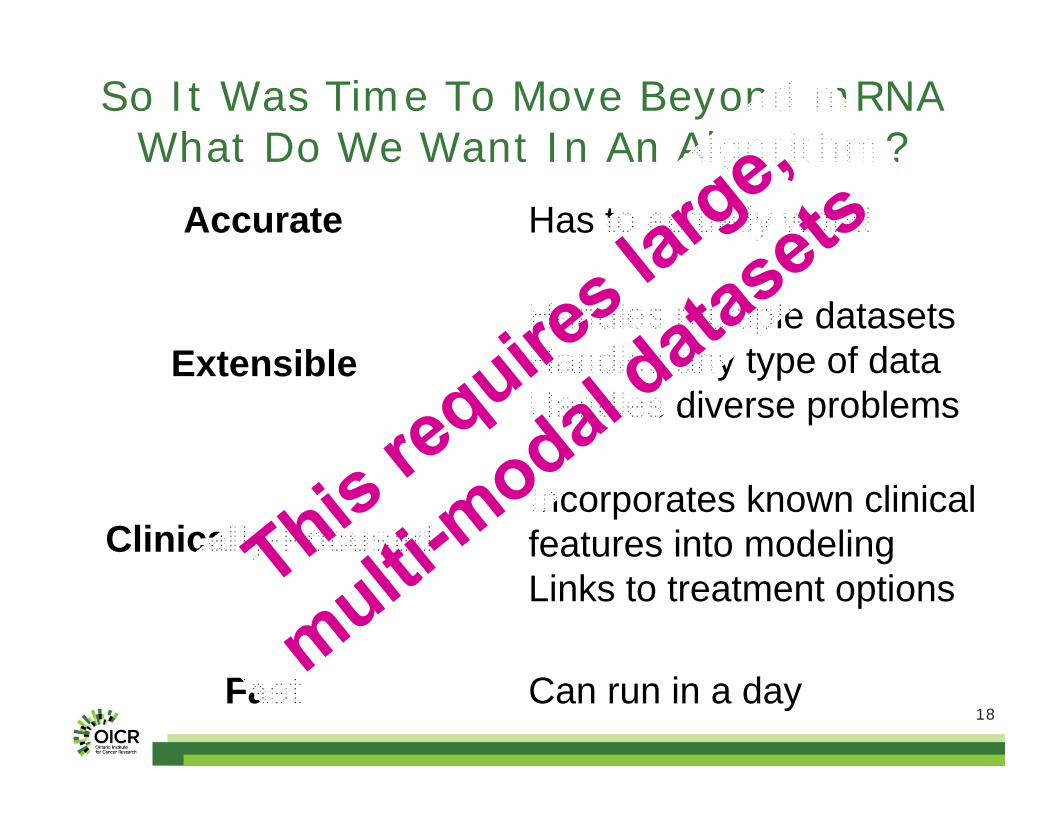
So It Was Time To Move Beyond mRNAWhat Do We Want In An Algorithm?
Accurate
Extensible
Fast
Clinically-Focused
Has to actually work!
Handles multiple datasetsHandles any type of dataHandles diverse problems
Incorporates known clinical features into modelingLinks to treatment options
Can run in a day
19
Problem Formulation
CPC-GENE: A Prostate Cancer ICGC Intra-tumoural Heterogeneity Inter-tumoural Heterogeneity
Pathway
2020
Dr. Robert Bristow Dr. John McPherson
Dr. Theodore van der Kwast
CPC-GENE: The People Involved
21
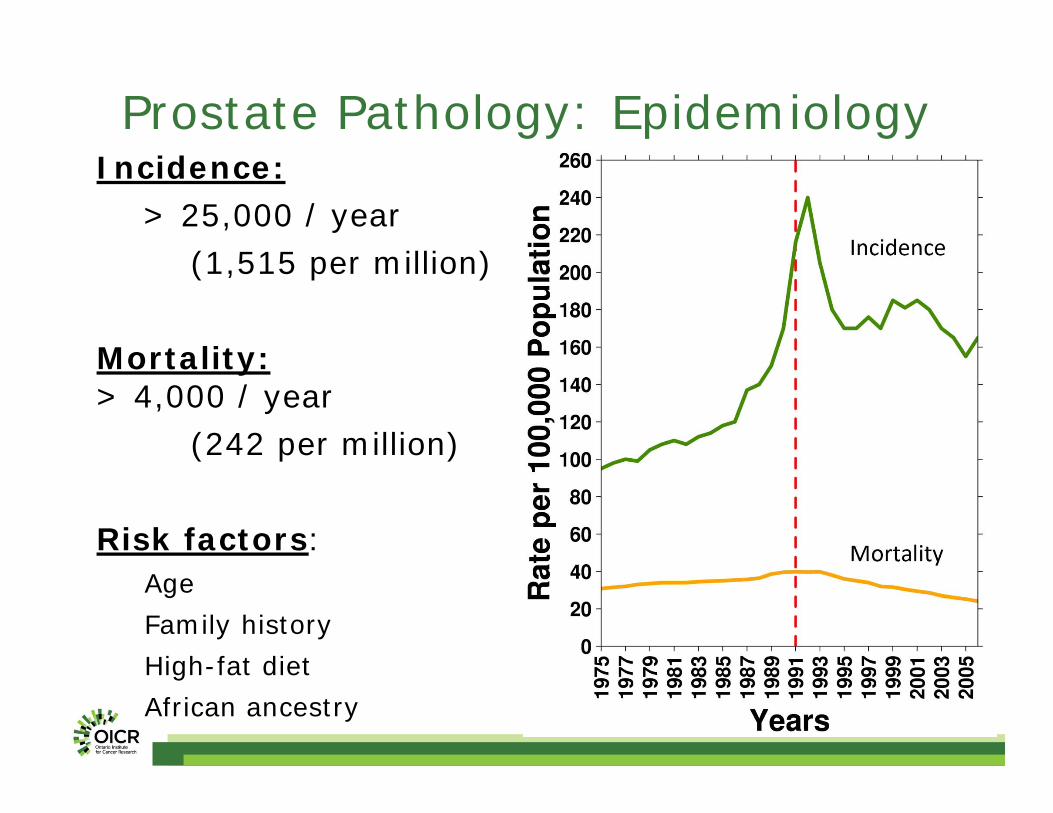
Incidence:> 25,000 / year
(1,515 per million)
Mortality:> 4,000 / year
(242 per million)
Risk factors: AgeFamily historyHigh-fat dietAfrican ancestry
Prostate Pathology: Epidemiology
2222
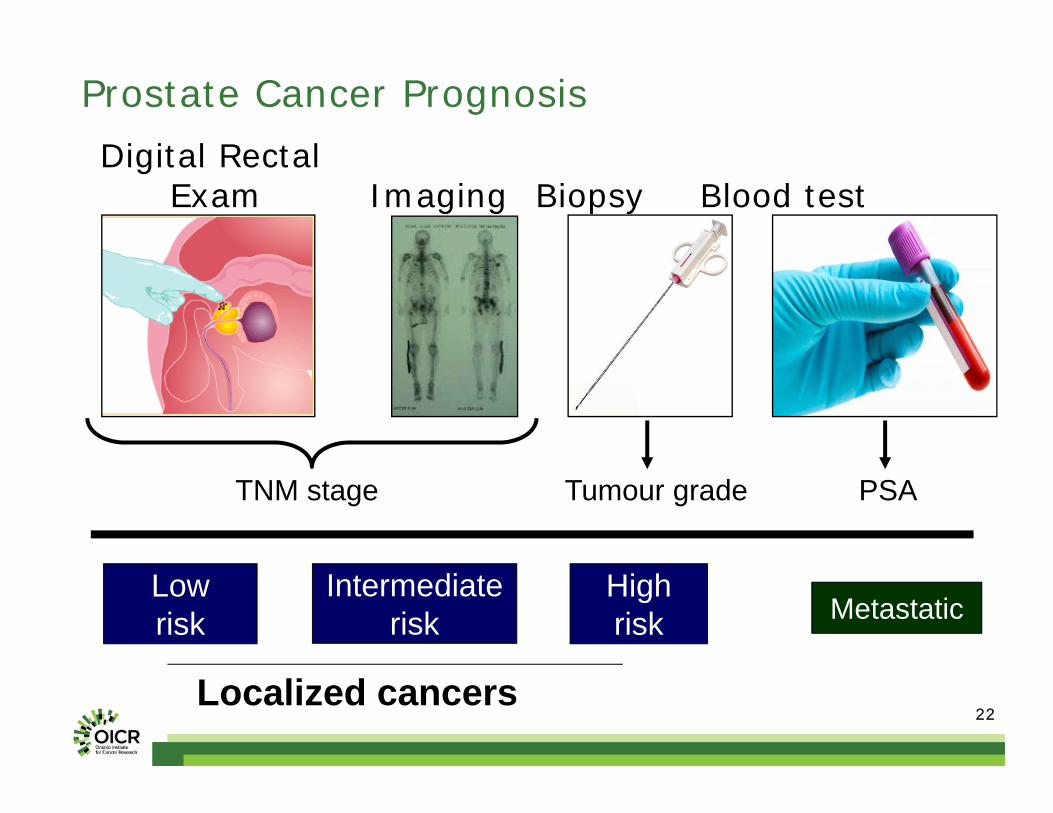
Prostate Cancer PrognosisDigital Rectal
Exam Imaging Biopsy Blood test
TNM stage Tumour grade PSA
Lowrisk
Intermediaterisk
Highrisk Metastatic
Localized cancers

23
Prostate Pathology: Gleason Scores
24
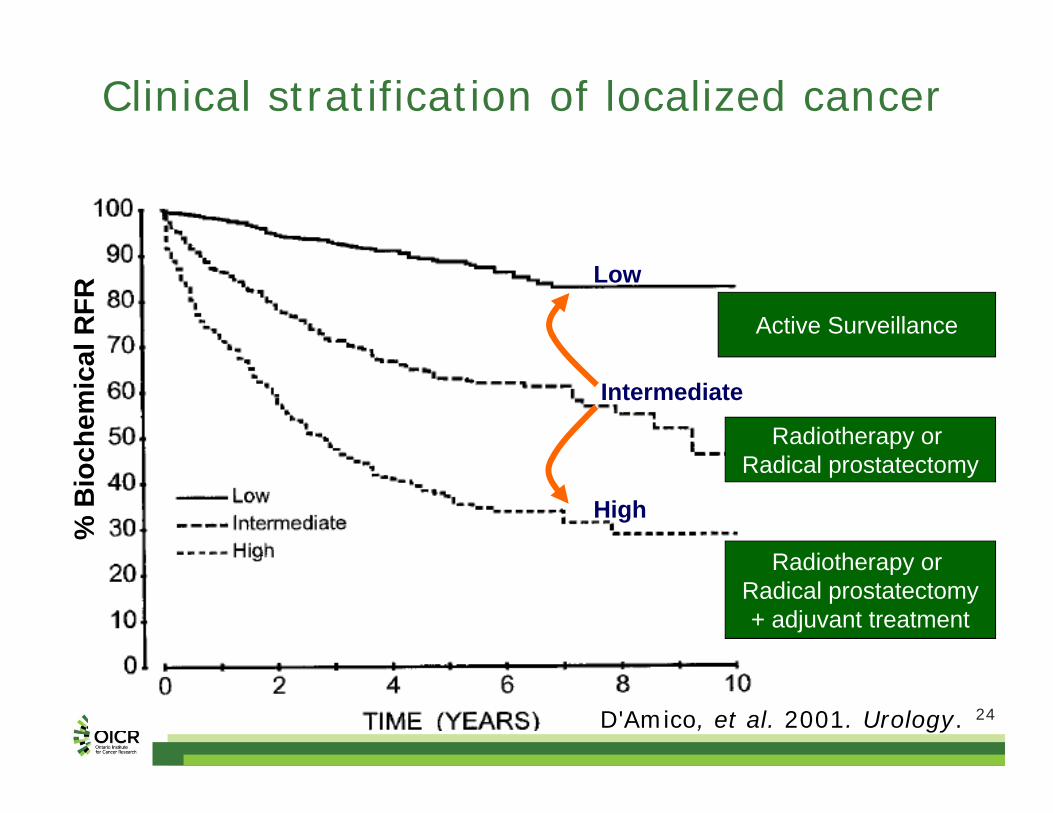
High
Low
% B
ioch
emic
al R
FR
Intermediate
Clinical stratification of localized cancer
D'Amico, et al. 2001. Urology.
Active Surveillance
Radiotherapy or Radical prostatectomy
Radiotherapy or Radical prostatectomy+ adjuvant treatment
25
Problem Formulation
CPC-GENE: A Prostate Cancer ICGC Intra-tumoural Heterogeneity Inter-tumoural Heterogeneity
Pathway
2626
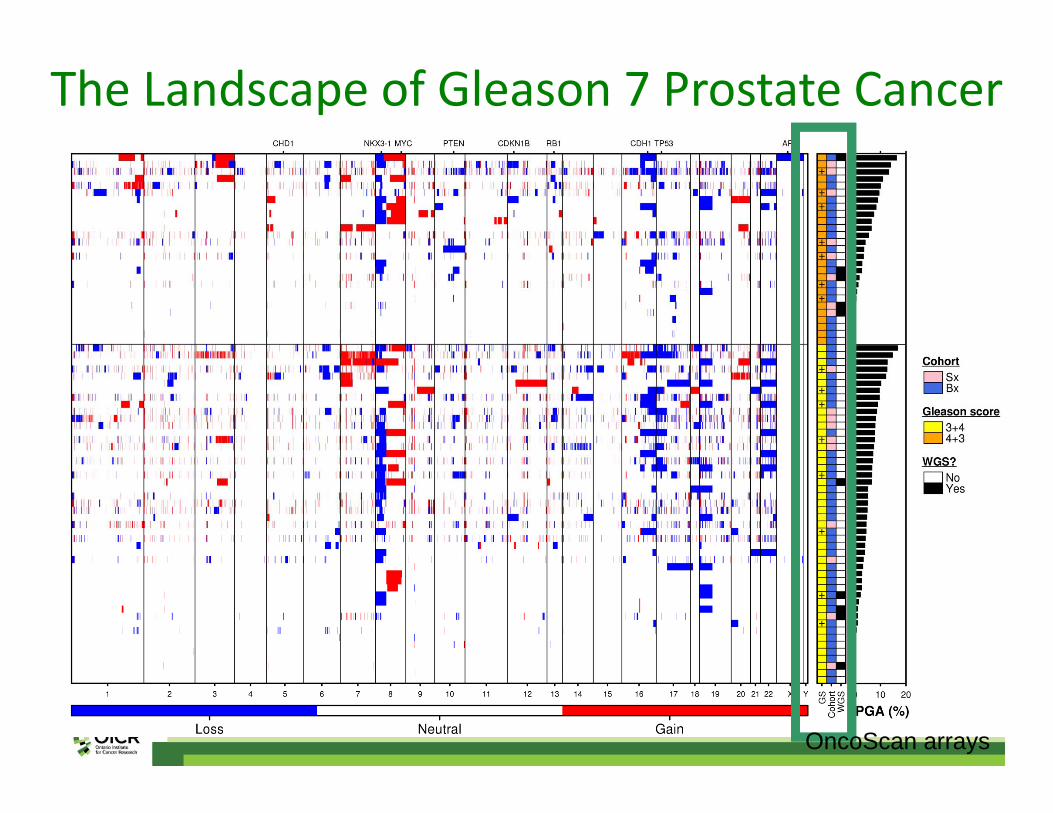
The Landscape of Gleason 7 Prostate Cancer
OncoScan arrays
2727
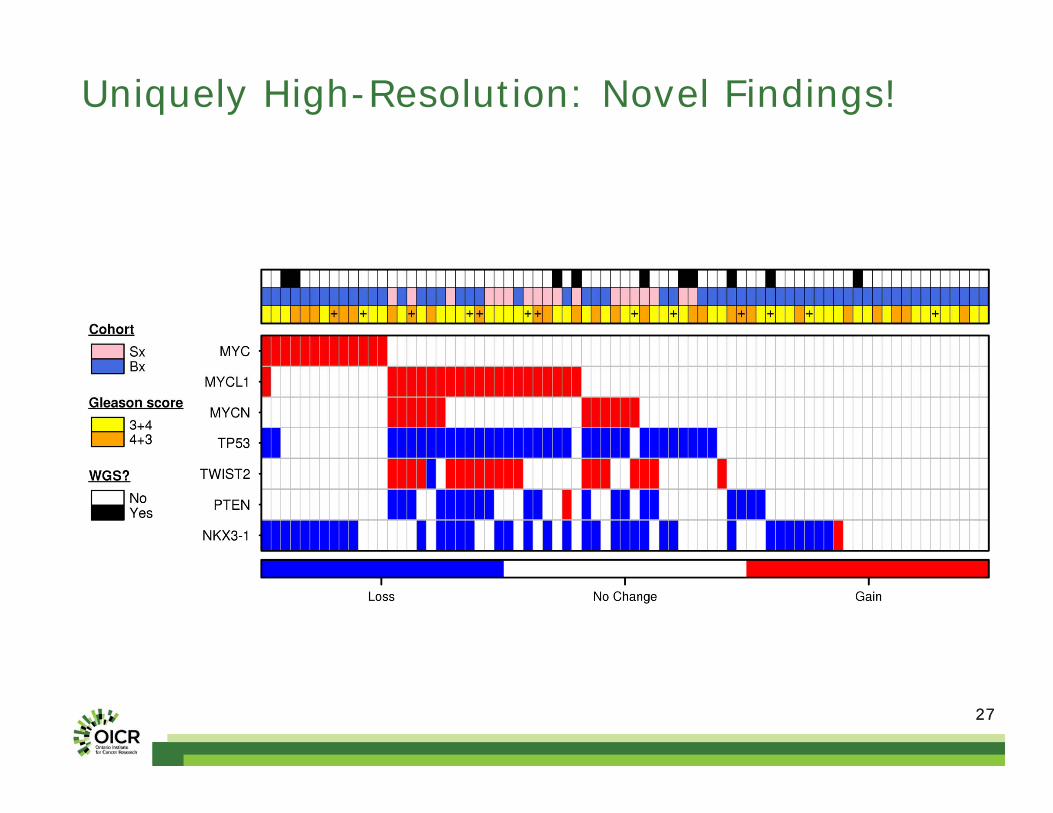
Uniquely High-Resolution: Novel Findings!

2828
We Didn’t Believe, So We RT-PCR Validated

2929
L-Myc: Associated With Genomic Instability
3030
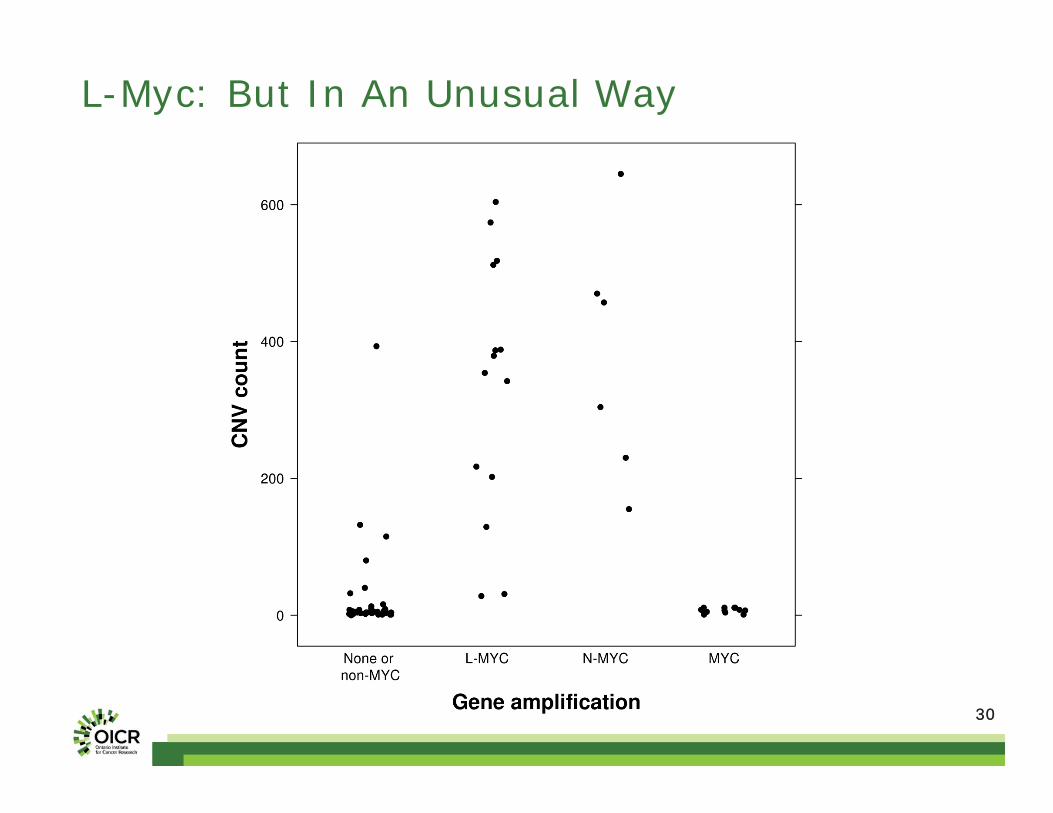
L-Myc: But In An Unusual Way
3131
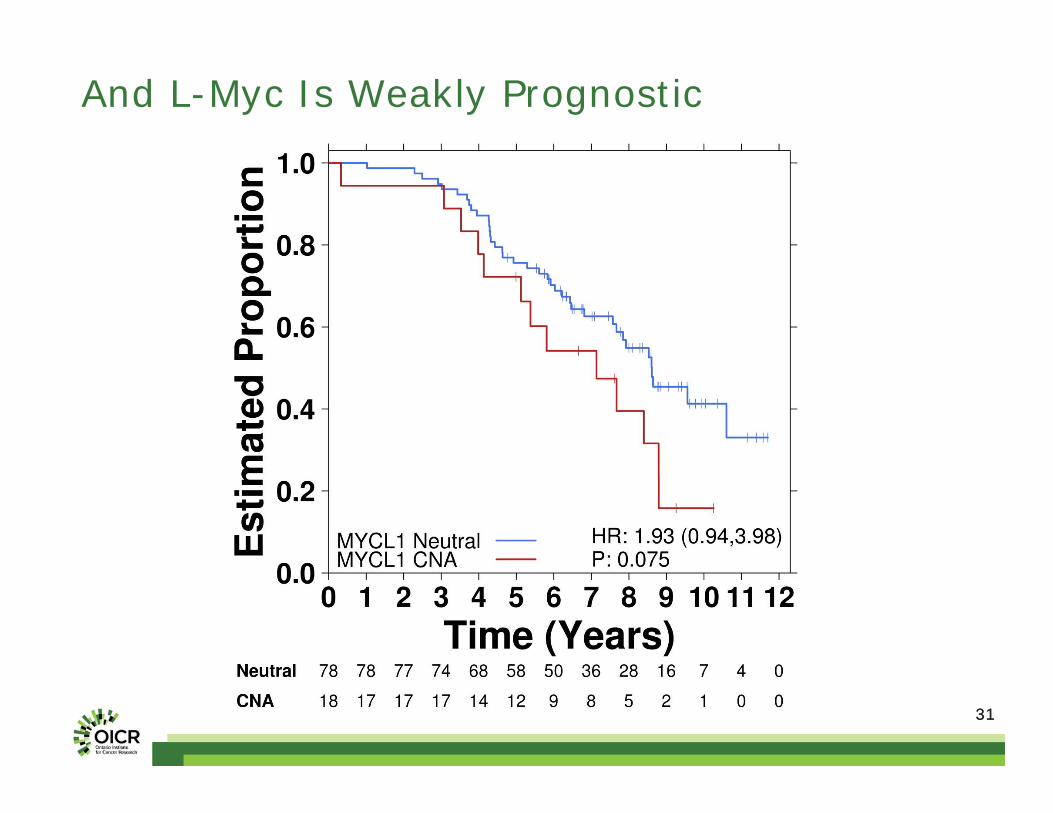
And L-Myc Is Weakly Prognostic
32
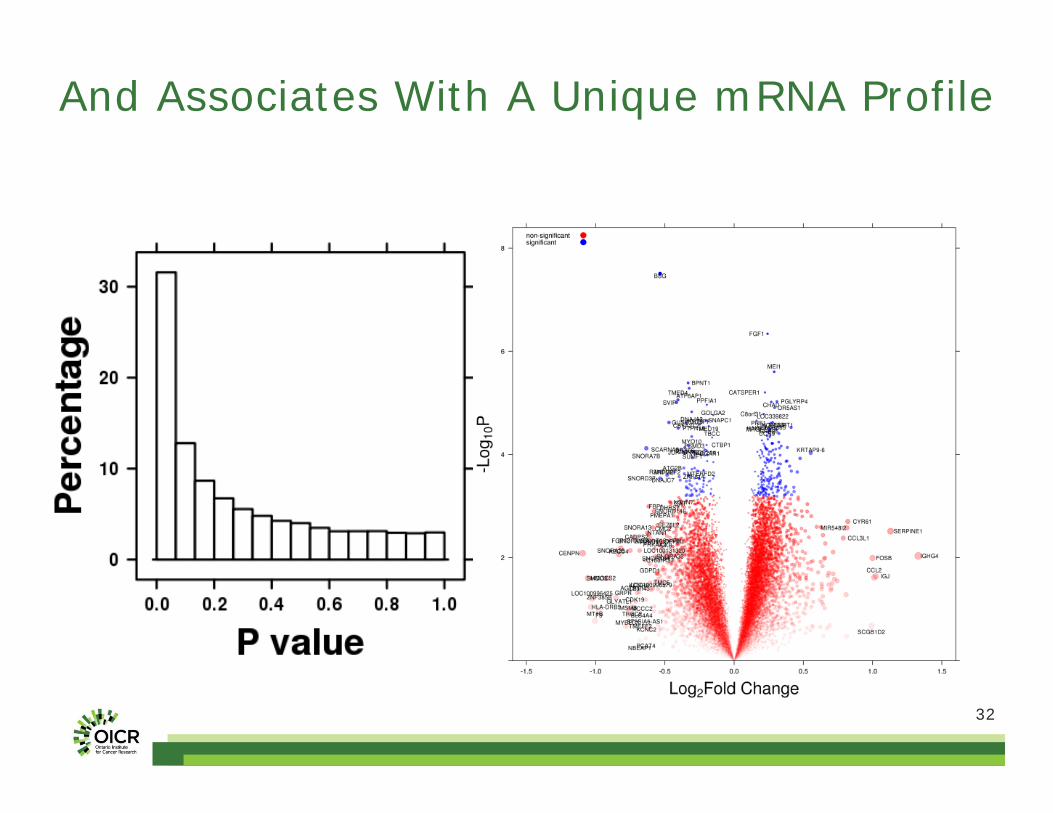
And Associates With A Unique mRNA Profile
3333
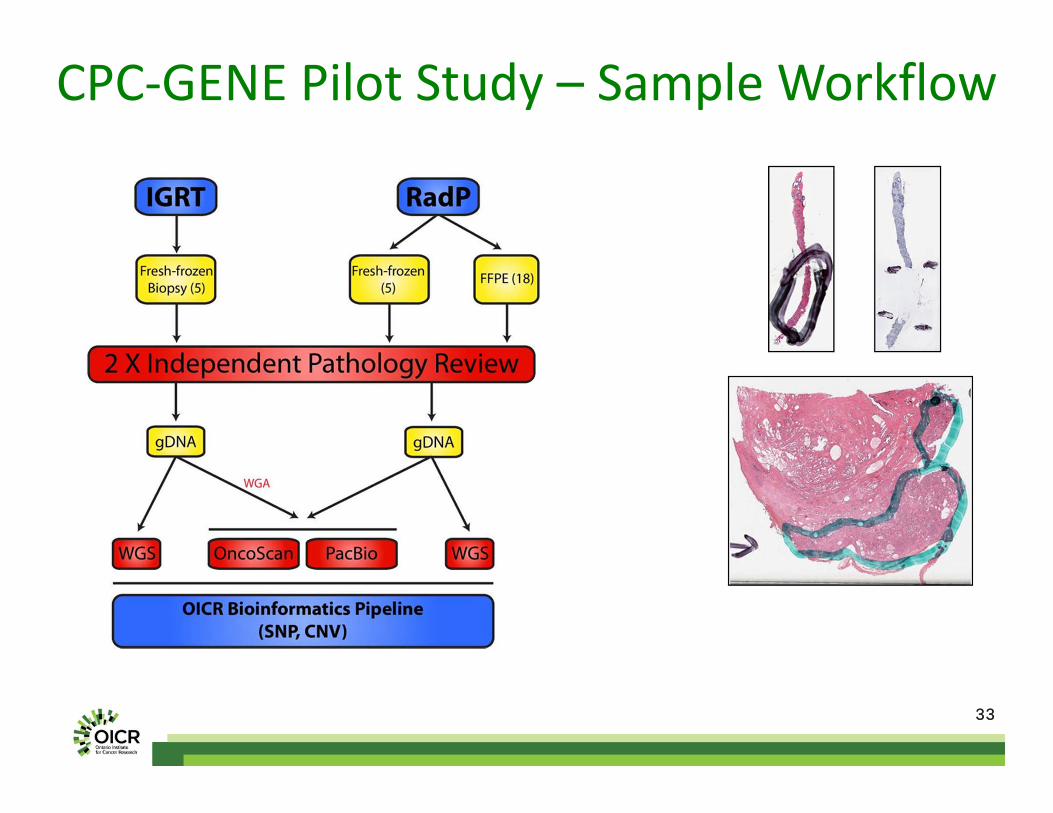
CPC‐GENE Pilot Study – Sample Workflow
3434
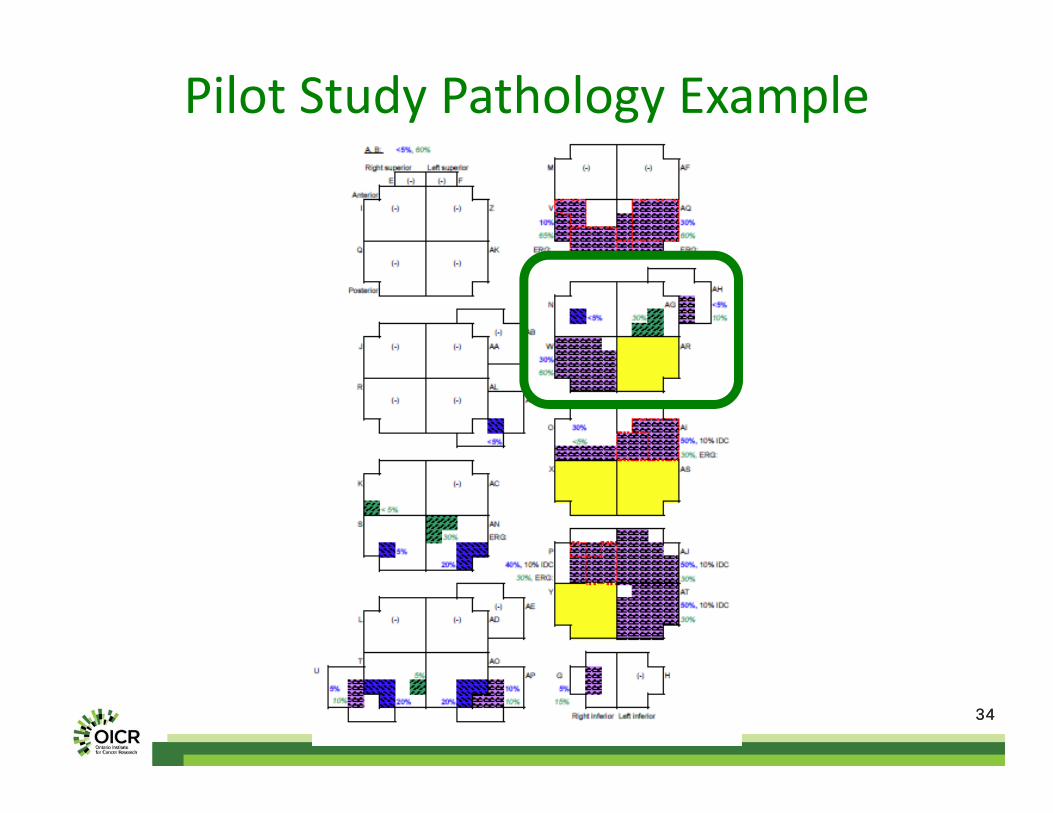
Pilot Study Pathology Example
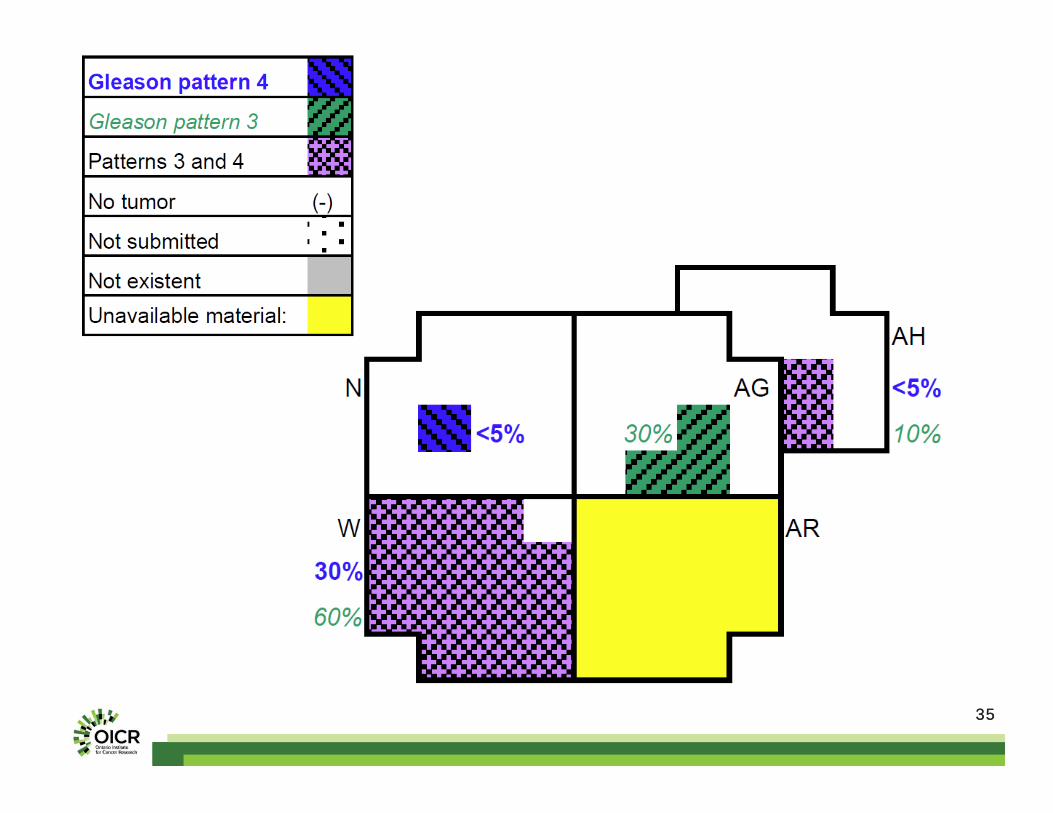
3535
3636
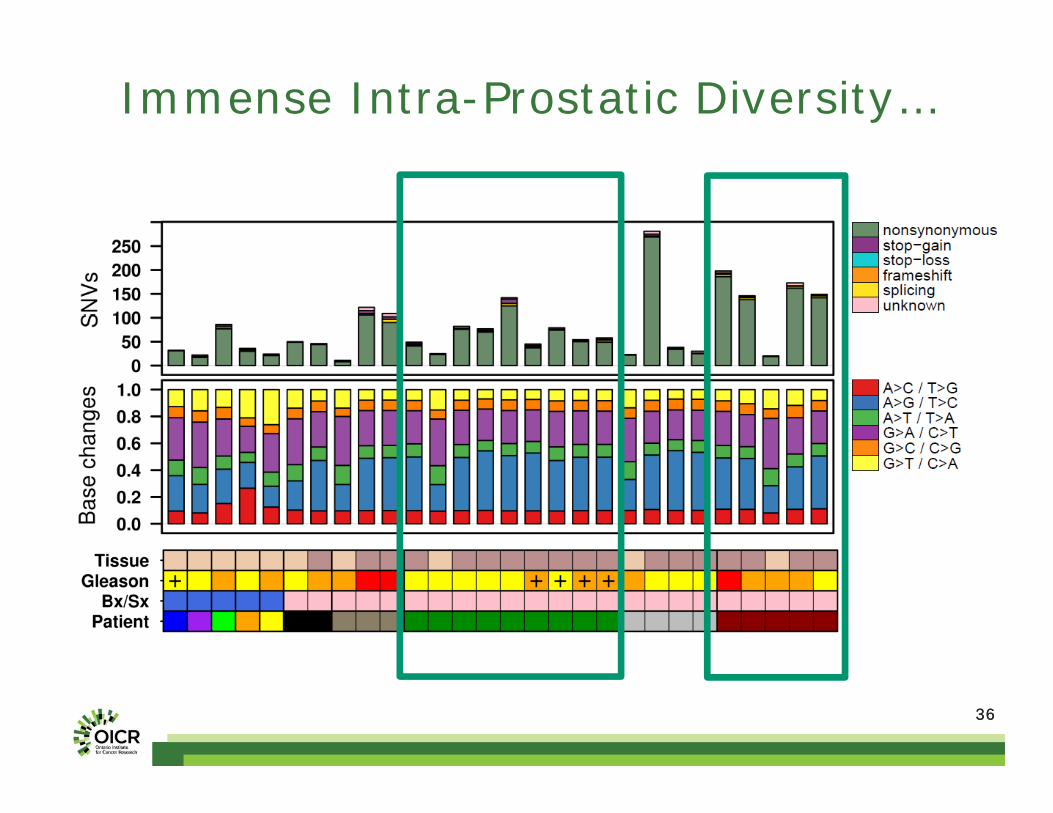
Immense Intra-Prostatic Diversity…
3737
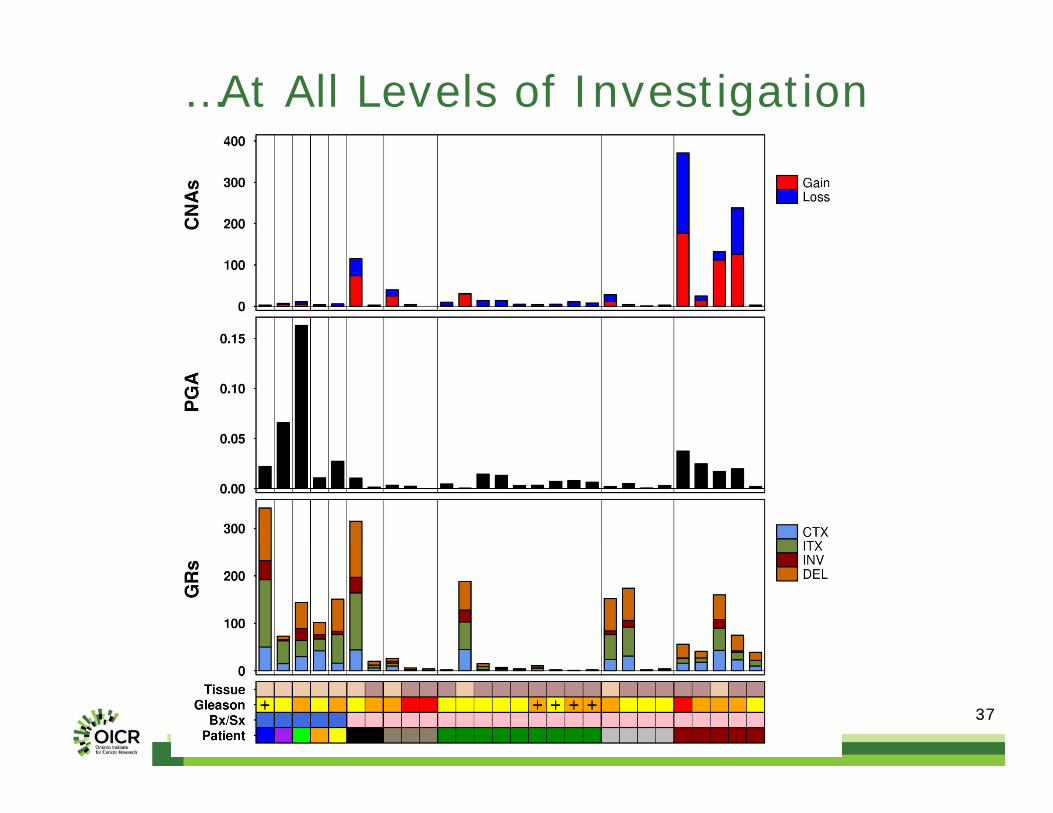
…At All Levels of Investigation

3838
Is This Heterogeneity Clinically Relevant?
3+4 3+4 3+4 3+43+4 3+44+3 4+3 4+3
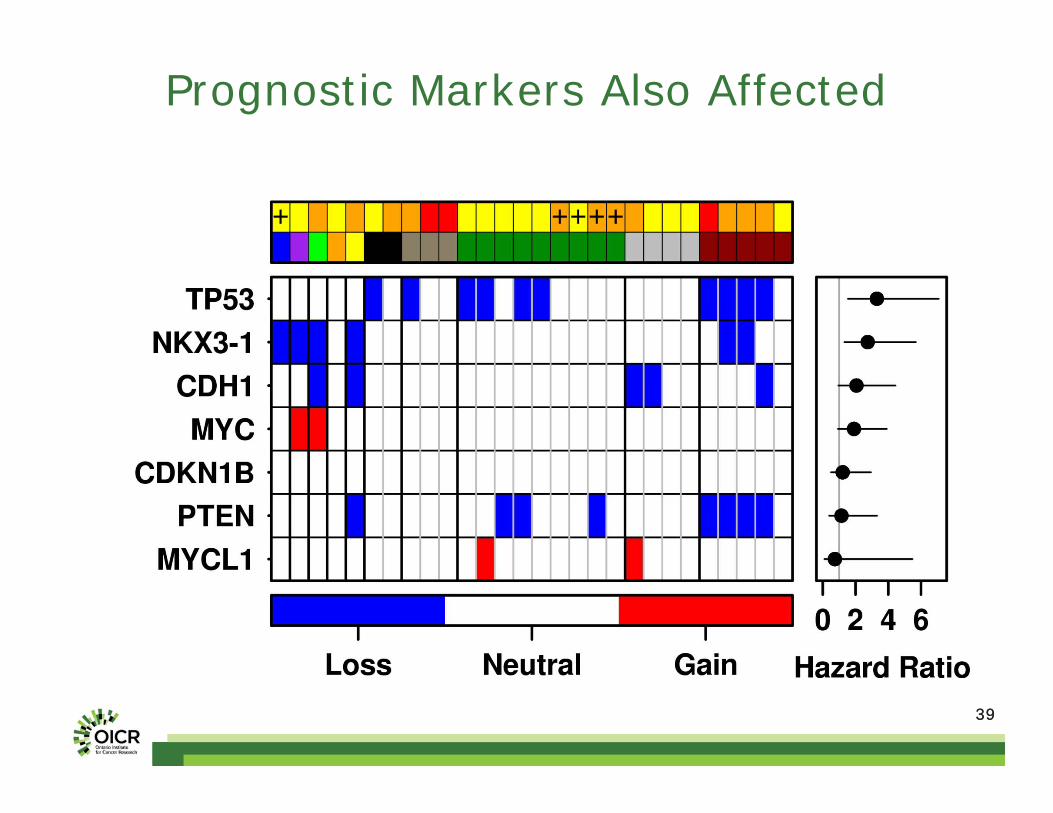
3939
Prognostic Markers Also Affected

4040
Multi-Clonality
41
Problem Formulation
CPC-GENE: A Prostate Cancer ICGC Intra-tumoural Heterogeneity Inter-tumoural Heterogeneity
Pathway
42
Emilie Lalonde
Dr. Robert Bristow
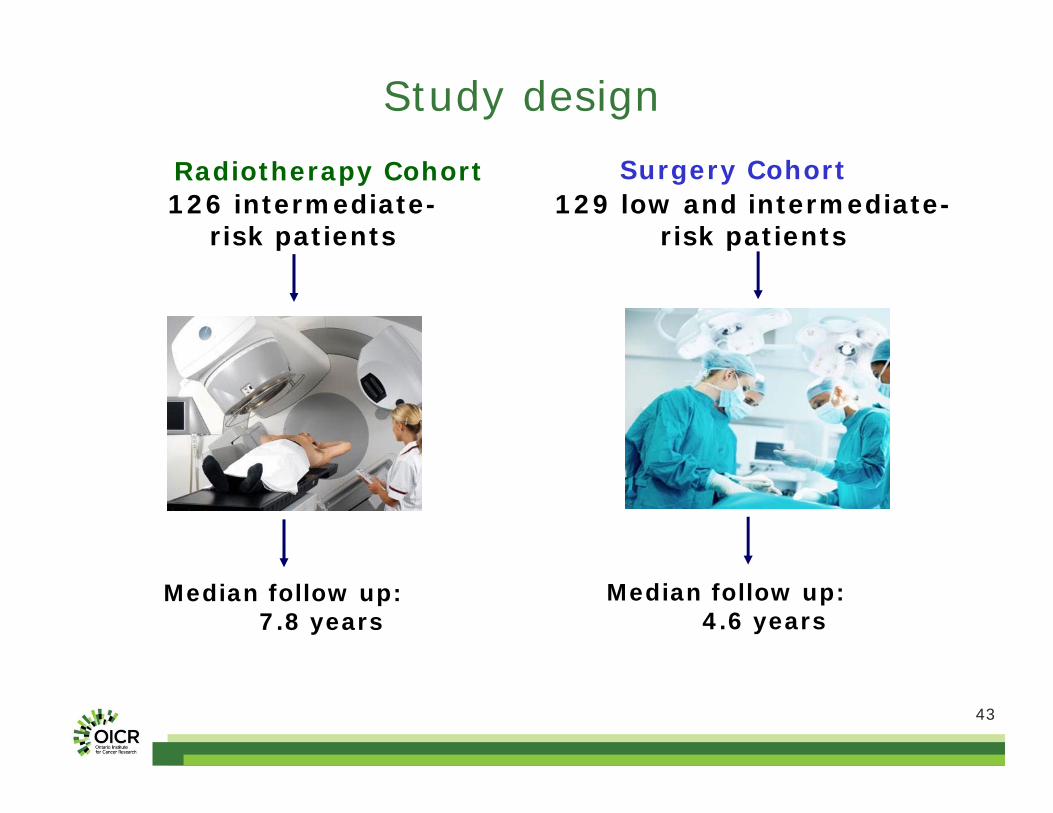
43
Study design
126 intermediate-risk patients
129 low and intermediate-risk patients
Median follow up: 7.8 years
Median follow up: 4.6 years
Radiotherapy Cohort Surgery Cohort
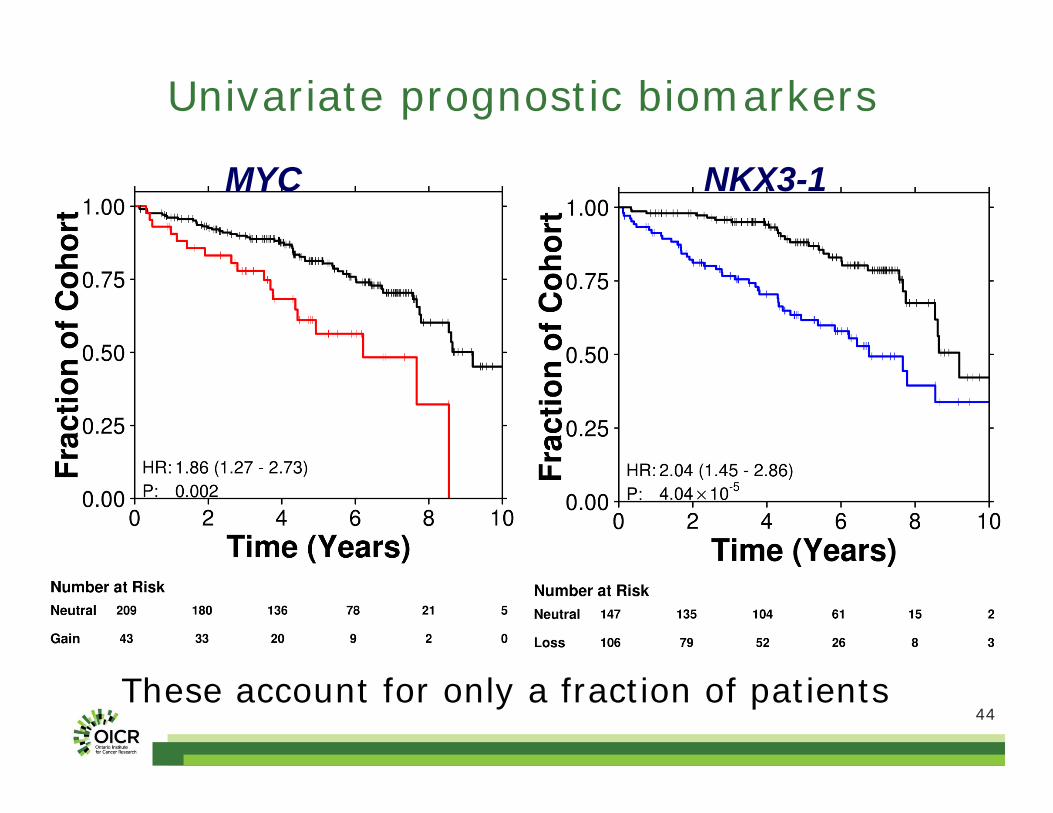
44
Univariate prognostic biomarkers
These account for only a fraction of patients
MYC NKX3-1
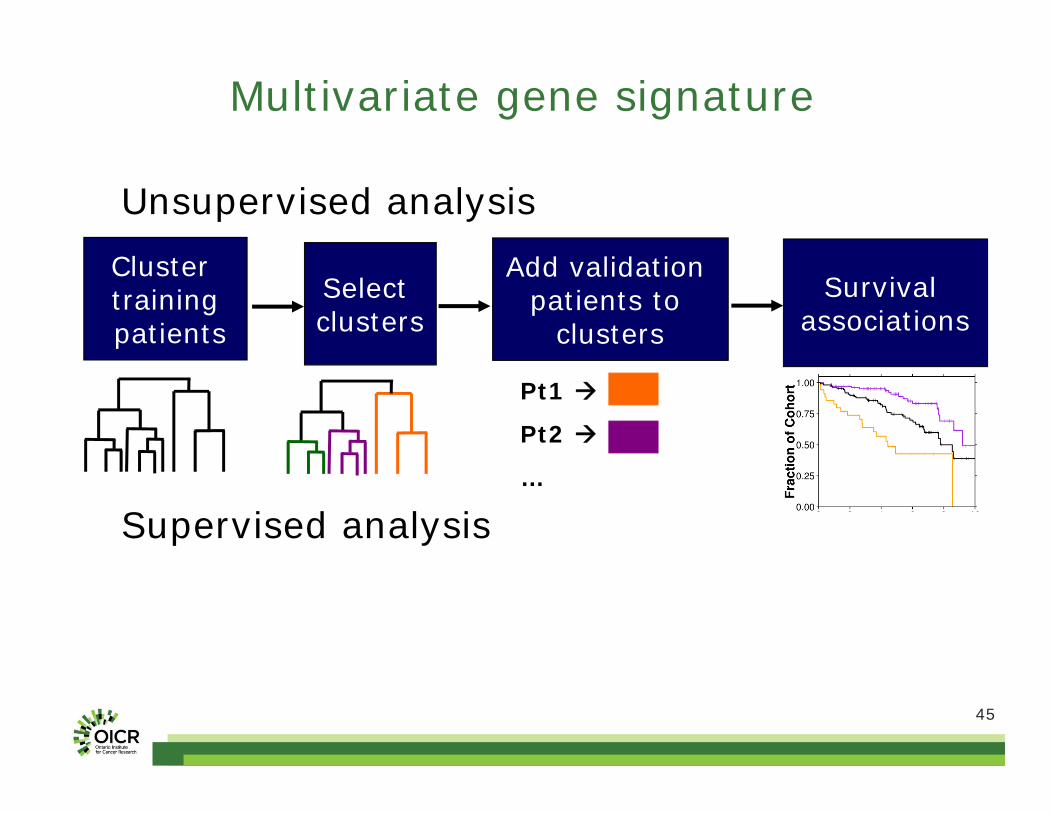
45
Unsupervised analysis
Supervised analysis
Multivariate gene signature
Cluster trainingpatients
Select clusters
Add validation patients to
clustersSurvival
associations
Pt1
Pt2
…
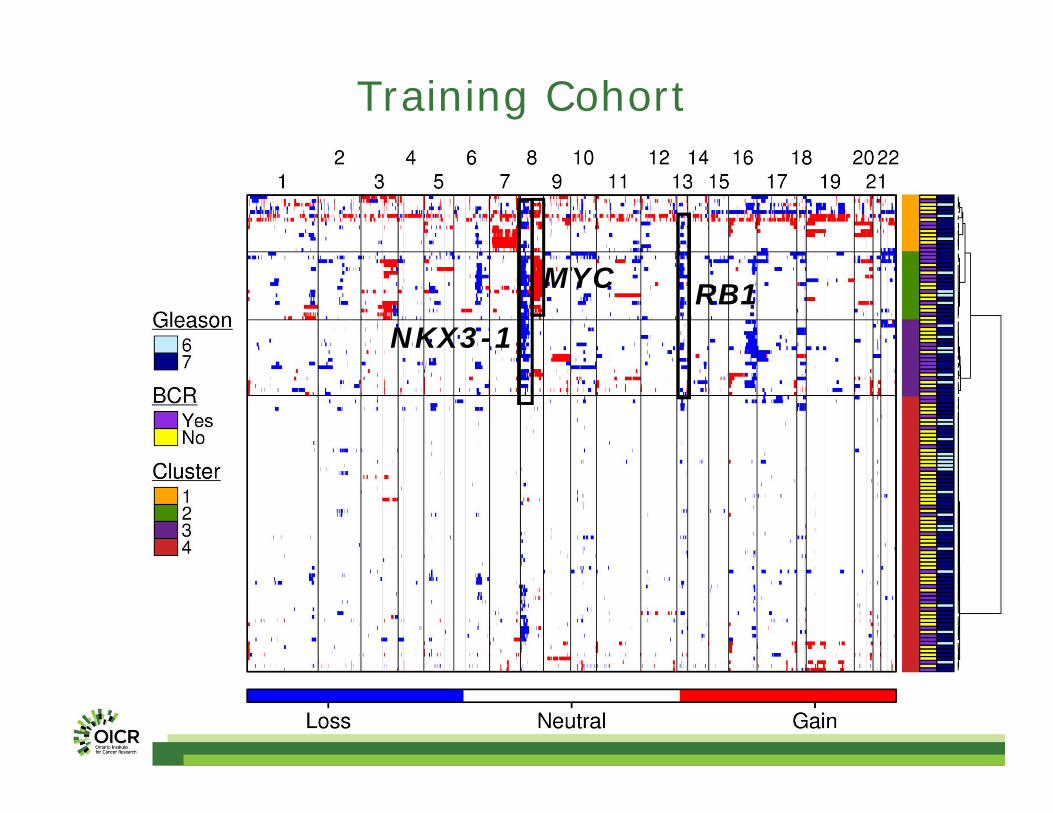
46
MYC
NKX3-1RB1
Training Cohort
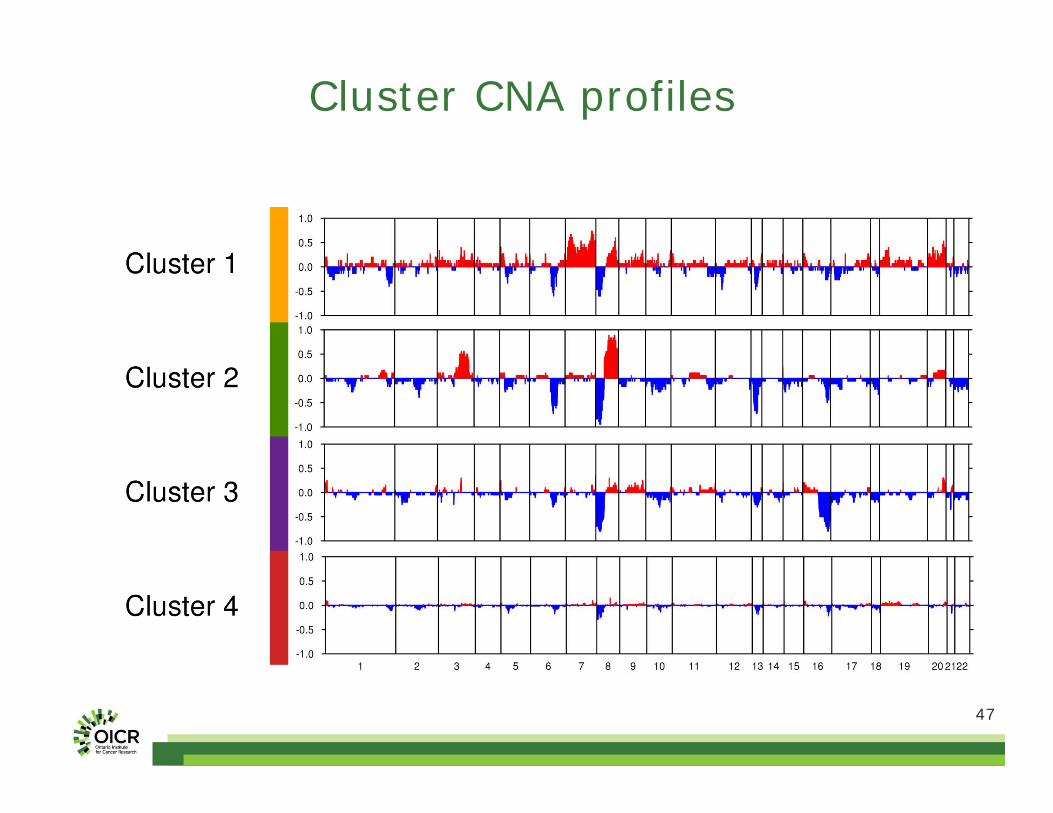
47
Cluster CNA profiles
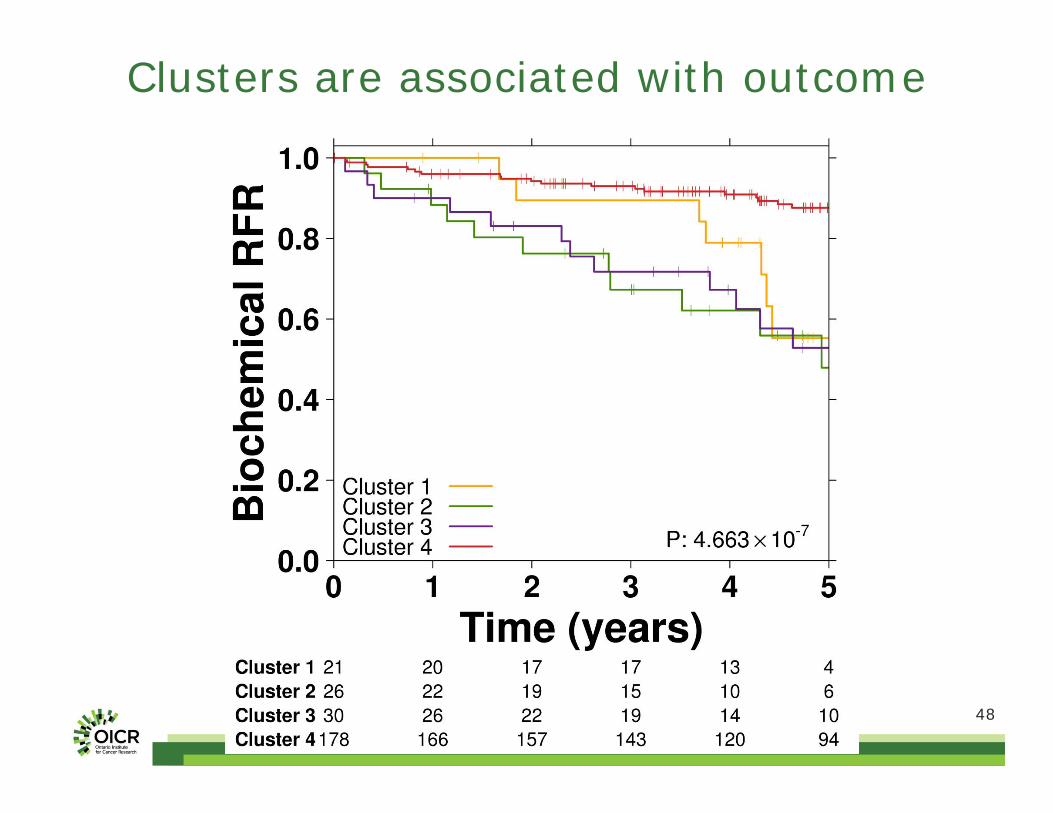
48
Clusters are associated with outcome
49
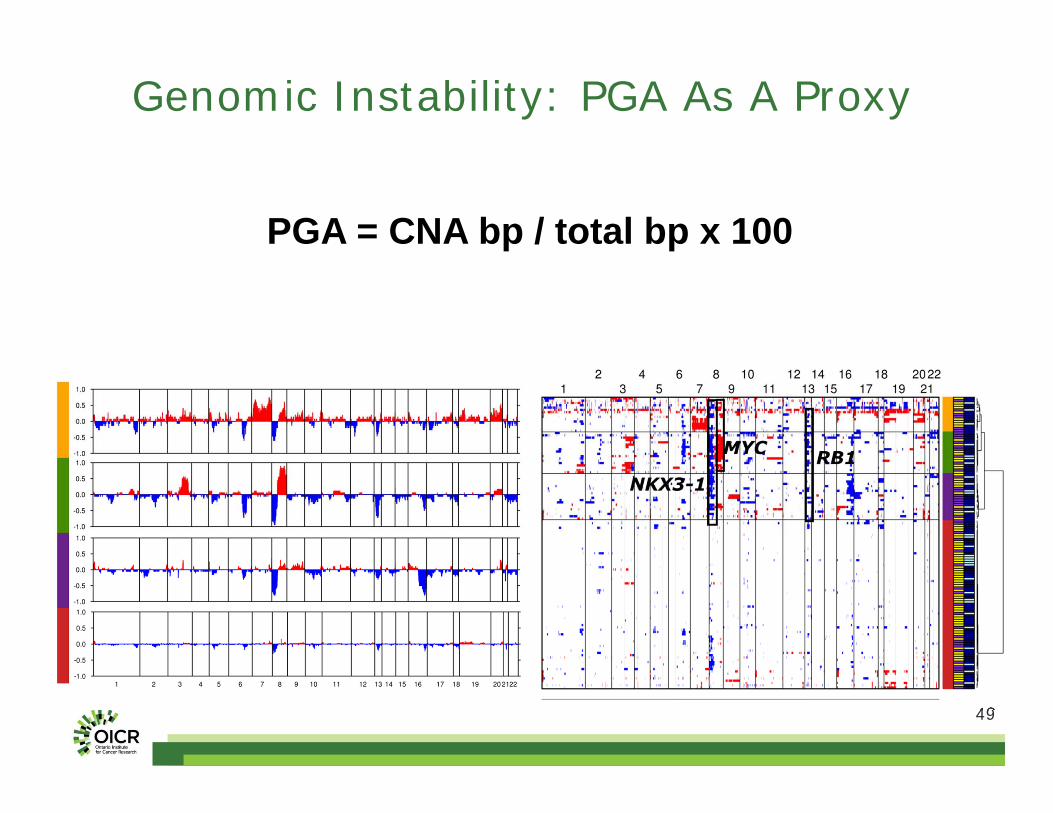
Genomic Instability: PGA As A Proxy
PGA = CNA bp / total bp x 100

50
PGA as a biomarker
51
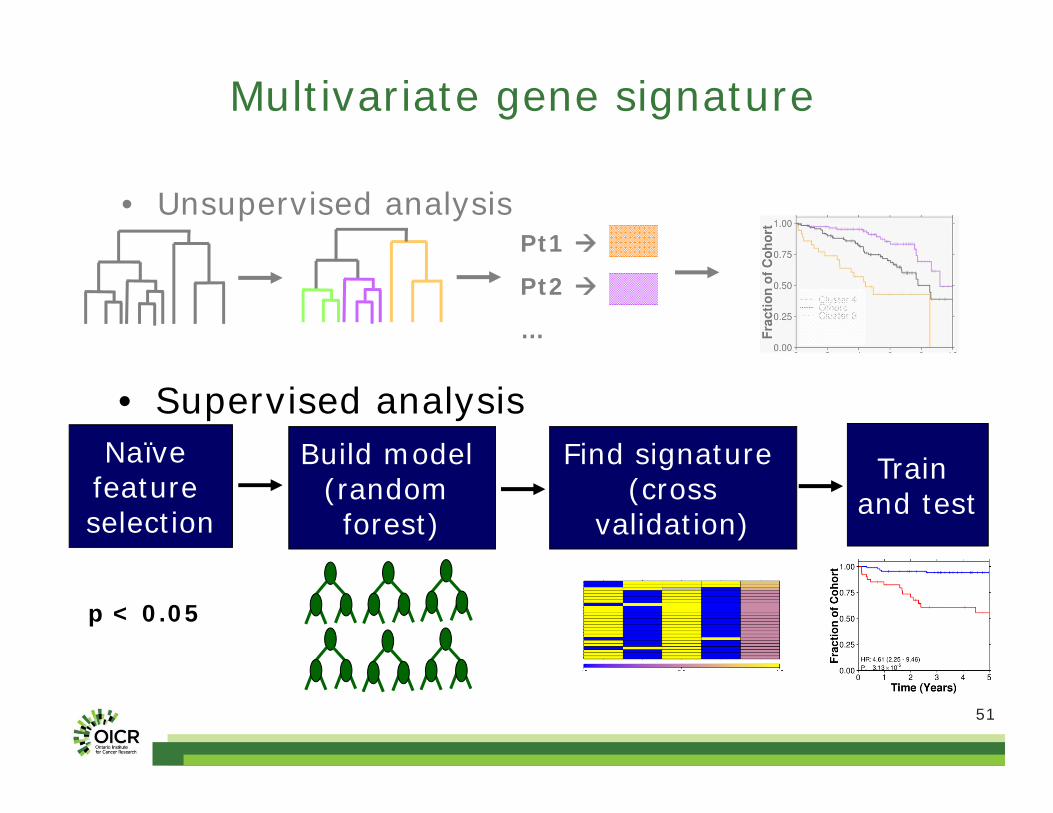
Multivariate gene signature
Naïve feature selection
Find signature (cross
validation)
Build model (random forest)
Train and test
p < 0.05
Pt1
Pt2
…
• Unsupervised analysis
• Supervised analysis

52
Classifier evaluation
PredictionsAccuracy 77.5%
Sensitivity 50.0%Specificity
AUC83.8%0.658
100 genomic regions
or 245 genes
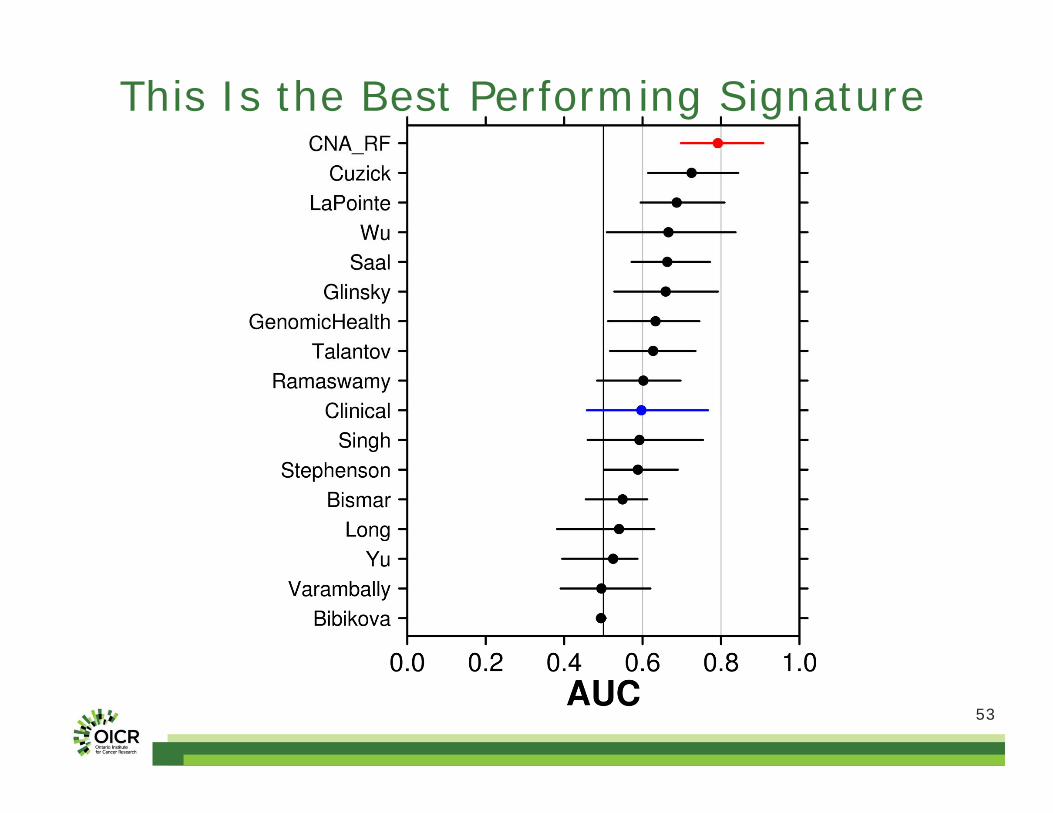
53
This Is the Best Performing Signature
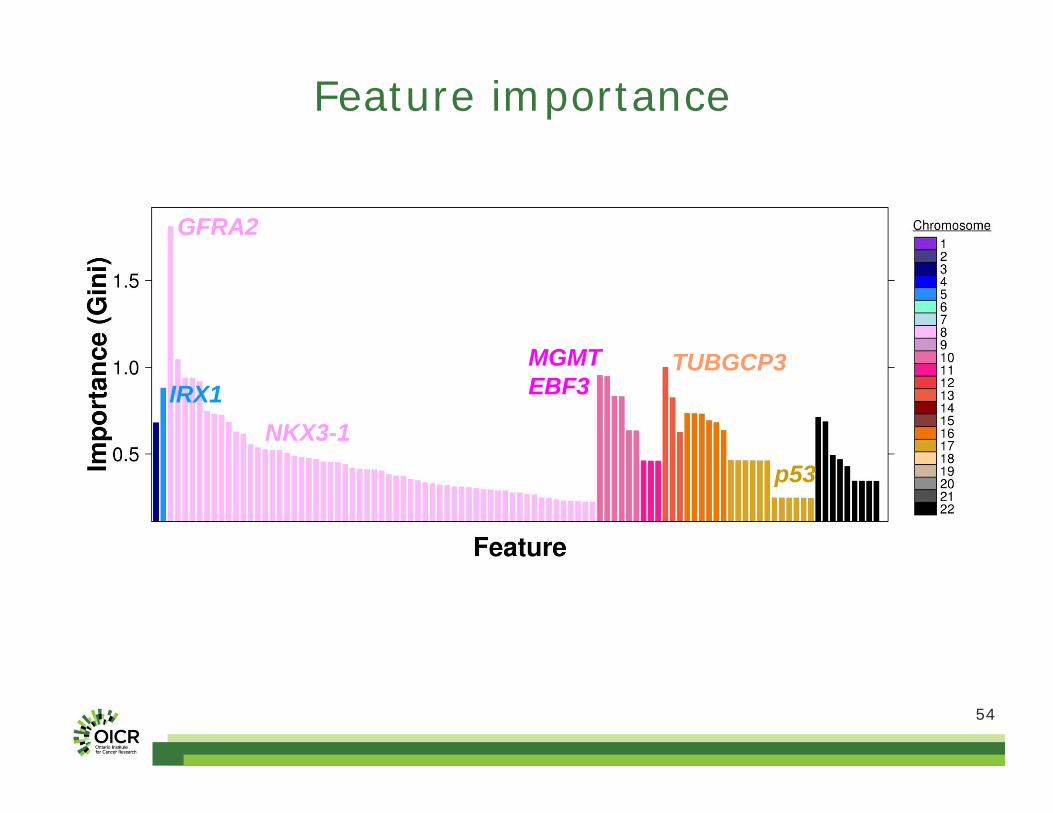
54
Feature importance
GFRA2
MGMTEBF3
TUBGCP3IRX1
NKX3-1p53

55
Signature Genes Have Interesting Biology
Homo sapiens SET binding factor 1(SBF1)
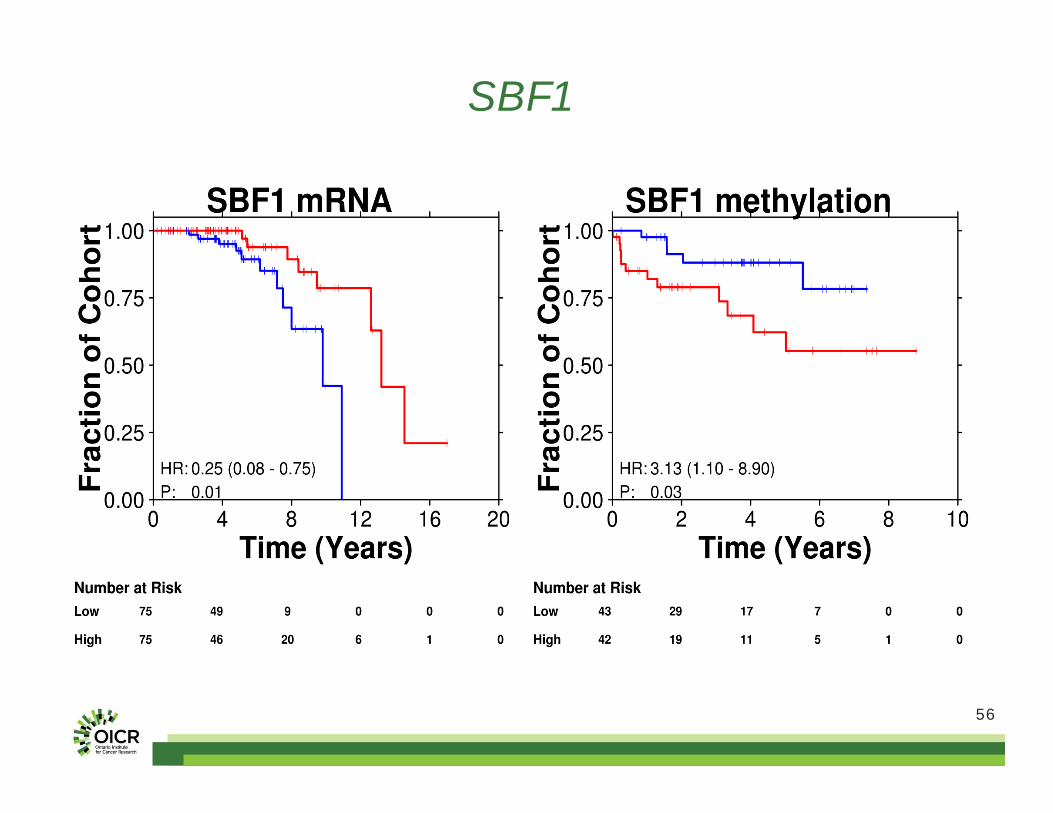
56
SBF1
57
Intra-tumoural Heterogeneity Prostate cancer can be multi-clonal
Inter-tumoural Heterogeneity CNAs alone are a promising biomarker
Summary
5858
Dr. Robert Bristow Dr. John McPhersonDr. Theodore van der Kwast
CPC-GENE: The People Involved
Boutros LabRichard de BorjaNicholas HardingPablo Hennings-YeomansEmilie LalondeAmin ZiaJianxin WangFrancis NguyenNatalie FoxMichelle Chan-Seng-YueMaud StarmansTakafumi YamaguchiVeronica Sabelnykova
InformaticsTimothy BeckFouad YousifRobert DenrocheXuemei Luo
GenomicsTaryne ChongAndrew BrownMichelle SamJeremy JohnsLee TimmsNicholas BuchnerAda Wong
Clinico-MolecularDominique TrudelAlice MengGaetano Zafarana
PIs & PMsMichael FraserMelania PintilieNeil FleshnerLakshmi MuthuswamyColin CollinsThomas HudsonLincoln Stein

Brought to you by the Science/AAAS Custom Publishing Office
Sponsored by:
June 11, 2014
Participating Experts
Solid Tumors Reveal Their SecretsPredictive and Prognostic Evidence from Copy Number Analysis
Webinar Series
Paul C. Boutros, Ph.D.Ontario Institute for Cancer ResearchToronto, Canada
Ajay Pandita, D.V.M., Ph.D.Core DiagnosticsPalo Alto, CA
Copy Number Alterations: From Bench to Bed
Ajay PanditaCore DiagnosticsJune 11, 2014
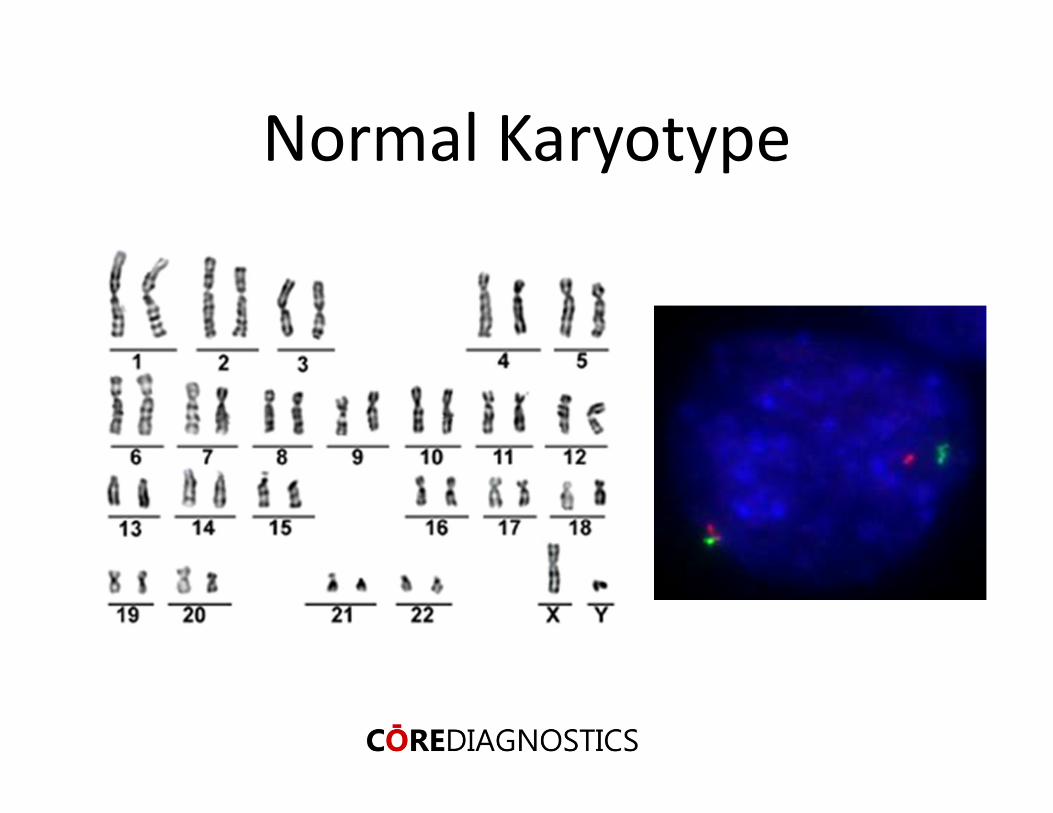
Normal Karyotype
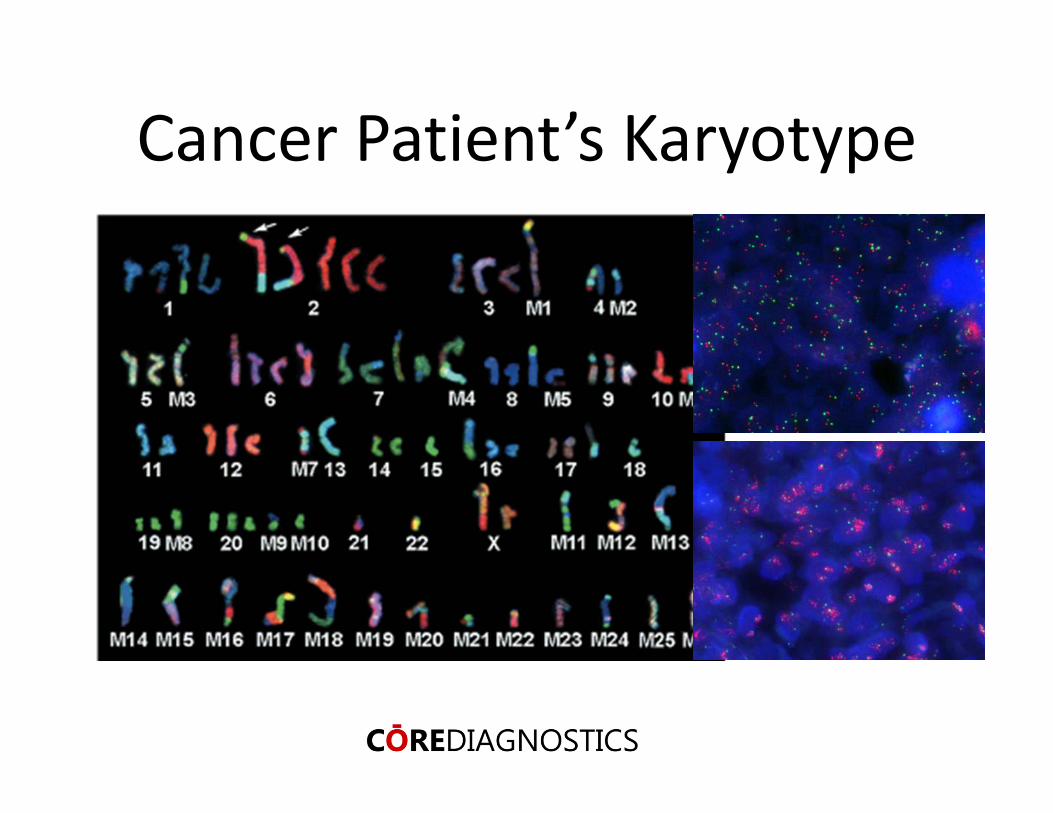
Cancer Patient’s Karyotype

Trisomy 21 (Down’s Syndrome)
Exhibit a number ofdevelopmental disabilities and have a significantly reduced life‐span
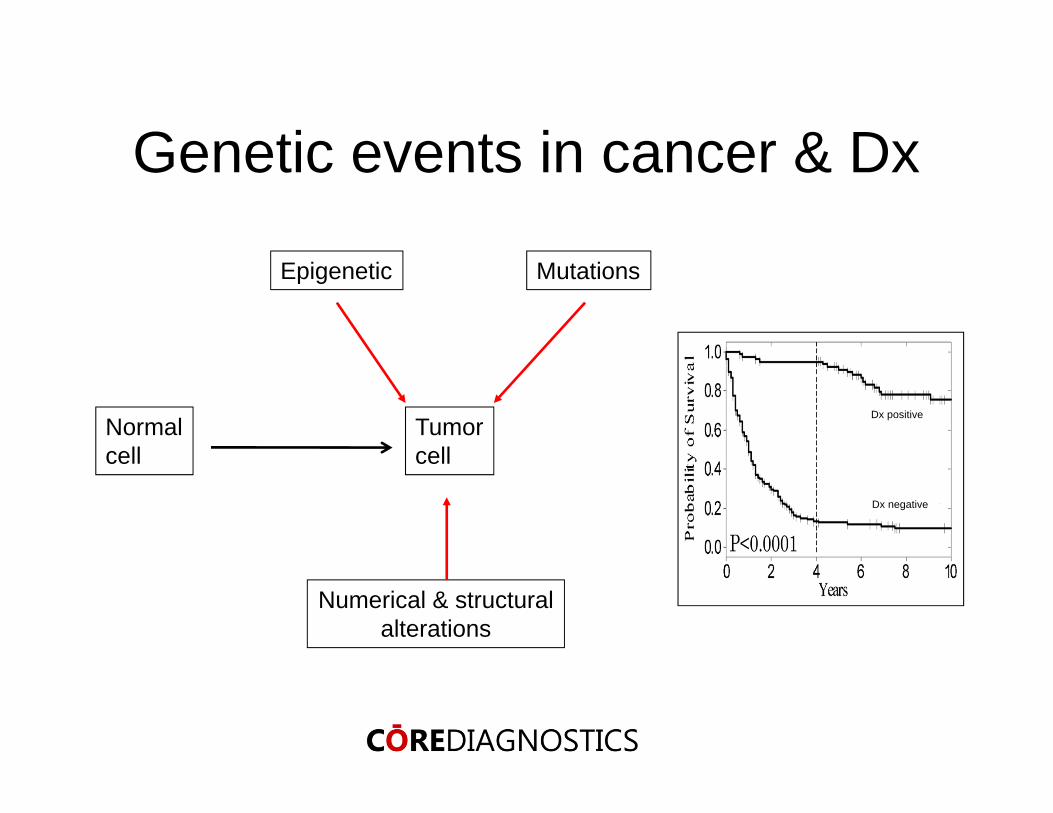
Normalcell
Tumorcell
Epigenetic Mutations
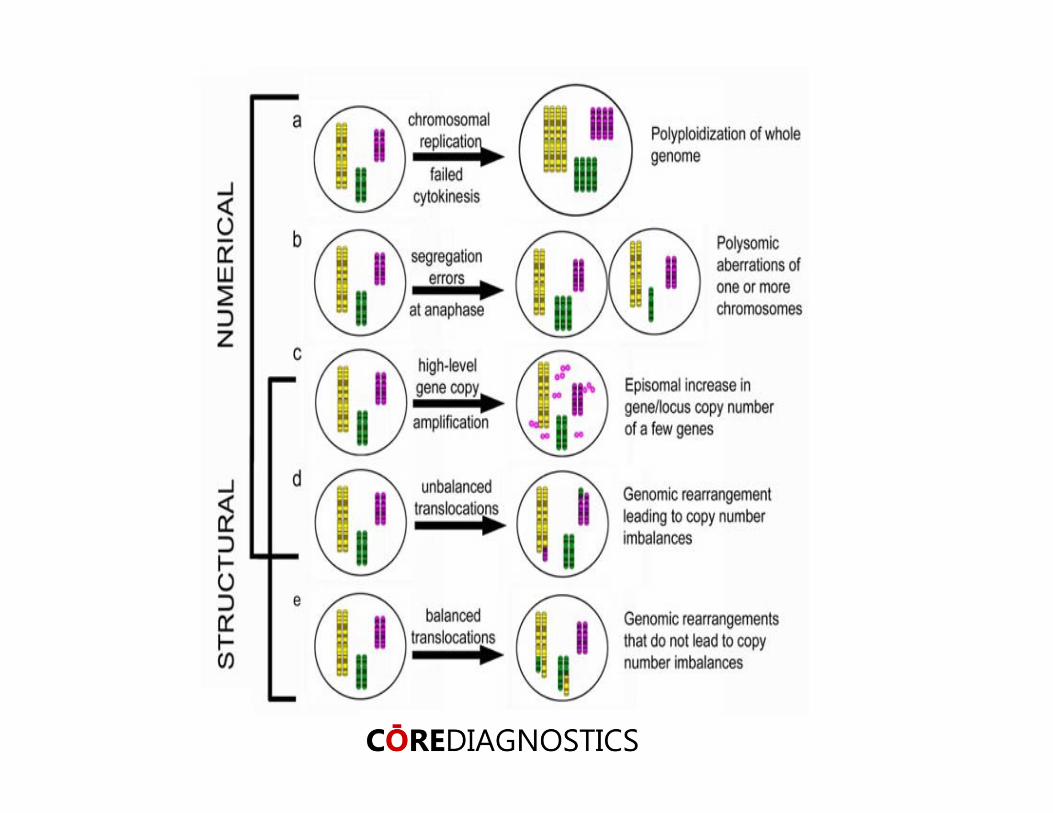
Numerical & structuralalterations
Dx positive
Dx negative
Genetic events in cancer & Dx

“Growth inhibiting & growth promoting chromosomes results in unlimited multiplication” and suggested that malignant tumors might be a result of “abnormal conditions of the chromosomes”
Theodor Boveri1902
Venter et al. Science, 2001
Human Genome Project
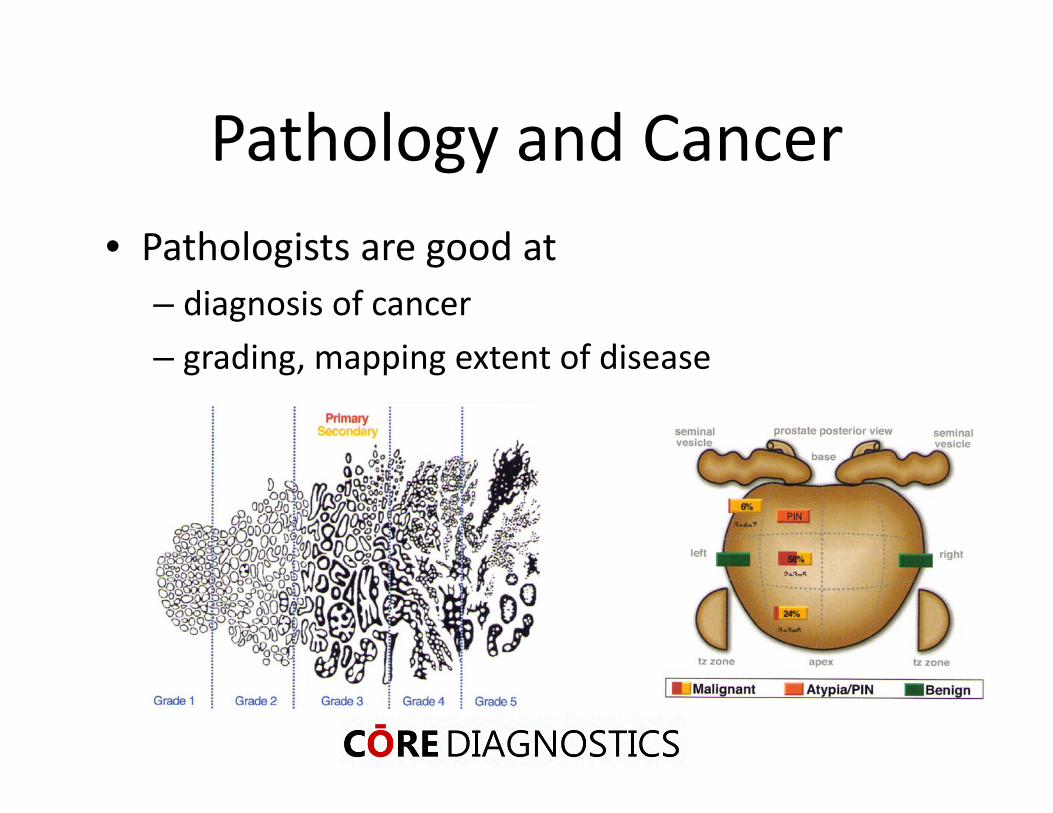
Pathology and Cancer• Pathologists are good at
– diagnosis of cancer– grading, mapping extent of disease

Diagnosis of Typical Cancers
Histology – H&E Immunohistochemistry

However….
• Conventional pathology not good at
–diagnosing rare tumors
–determining which tumors will be the “good” or “bad” players
–predicting which therapy is most effective for early or advanced tumors
BiomarkersA biomarker is anything that can be used to measure any biological process
Biomarkers
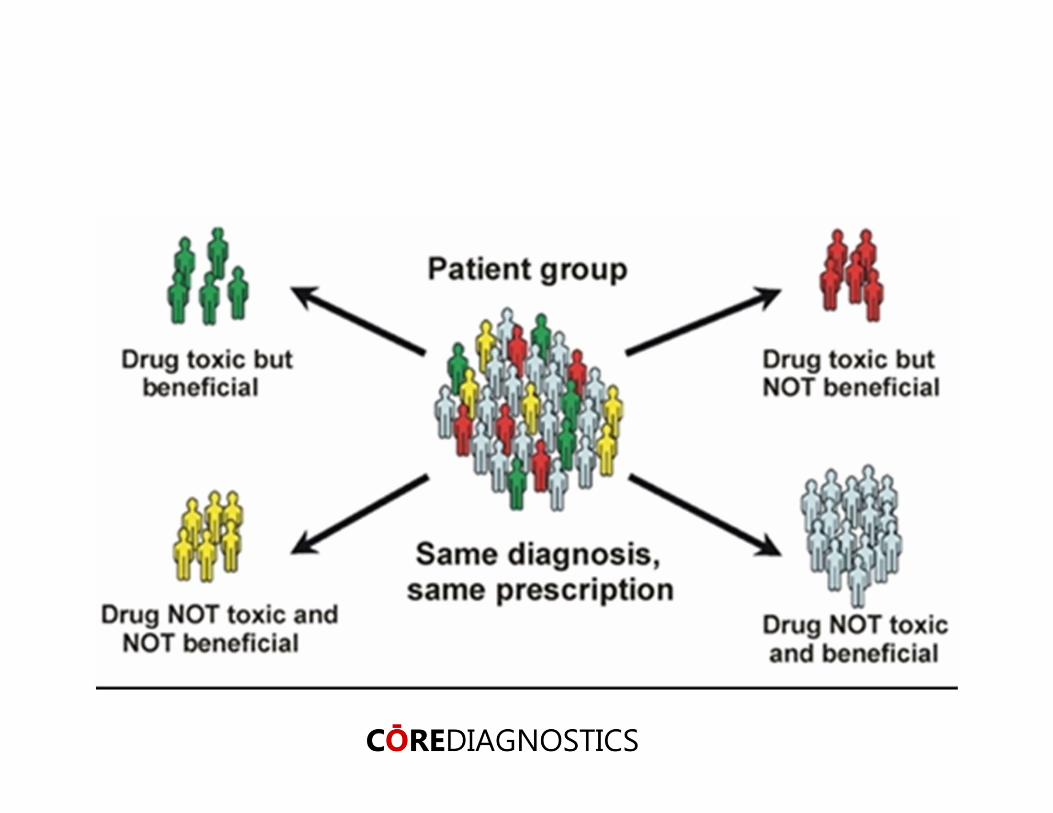
Predictive biomarker: a test that can be done before treatment to predict whether a particular treatment is likely to be beneficial
Prognostic biomarkers correlate with disease outcome. They improve our ability to design informative trials and to interpret them confidently.
Resistance markers correlate with resistance to treatment. They improve our ability to understand resistance mechanisms to treatment.
Diagnostic biomarker: a test that can be done to confirm the diagnosis
Ajay Pandita
Prognostic value of biomarkers• Early detection of cancer• Important to determine
– indolent tumor• “wait and watch” with periodic monitoring
– Progressive tumor• aggressive treatment regimen• surgery• quality of life
Confidential 73
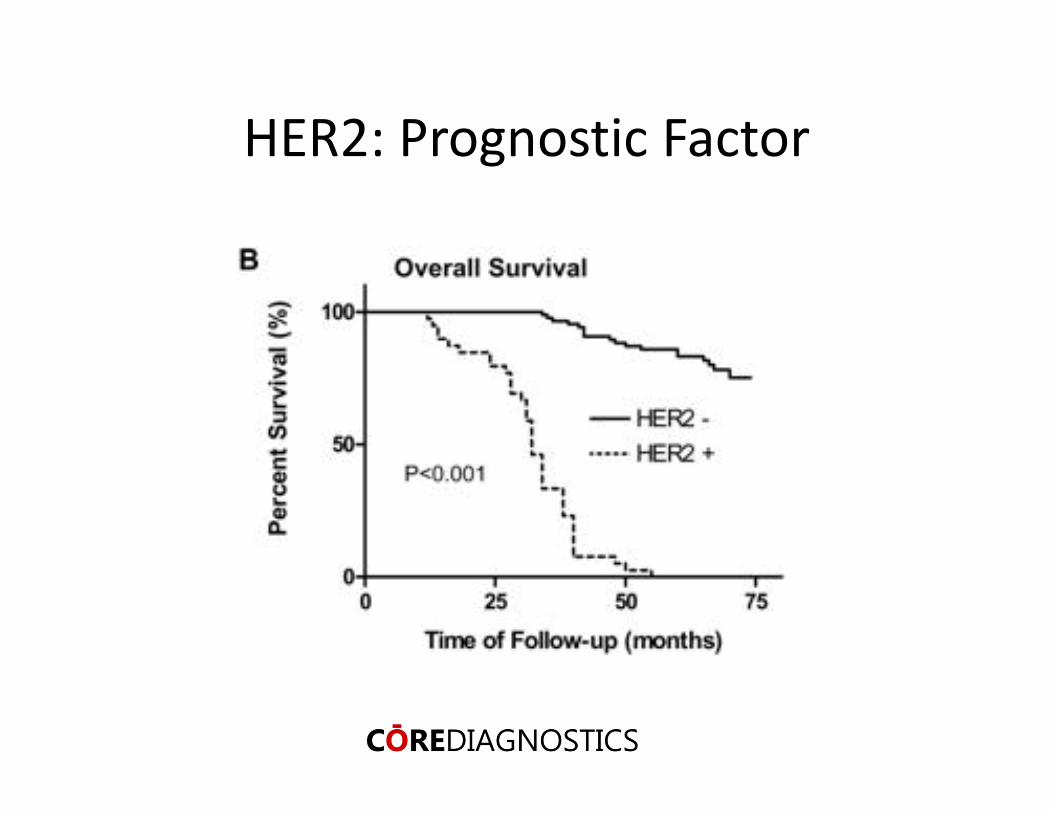
HER2: Prognostic Factor

Predictive biomarkers (Companion Diagnostics)
• A test that can be done before treatment to predict whether a particular treatment is likely to be beneficial
• bcr‐abl for imatinib• hormone receptors for tamoxifen• HER2 for trastuzumab
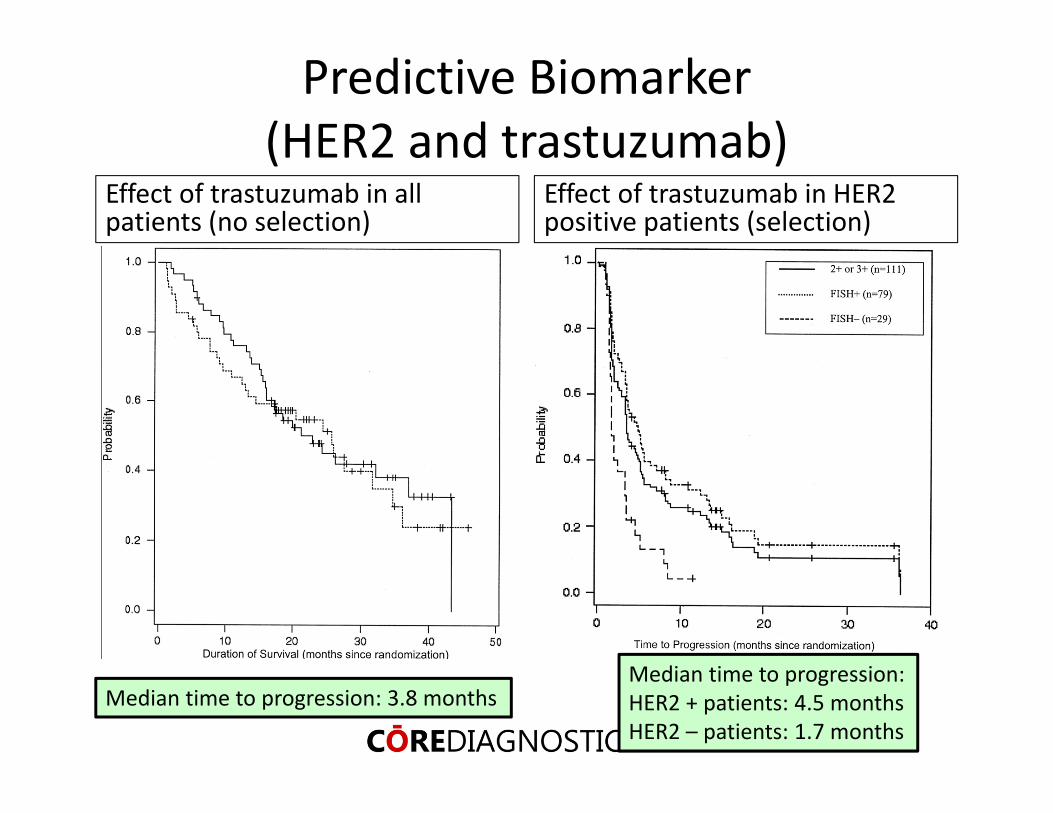
Predictive Biomarker (HER2 and trastuzumab)
Effect of trastuzumab in all patients (no selection)
Effect of trastuzumab in HER2 positive patients (selection)
Median time to progression: 3.8 monthsMedian time to progression: HER2 + patients: 4.5 monthsHER2 – patients: 1.7 months
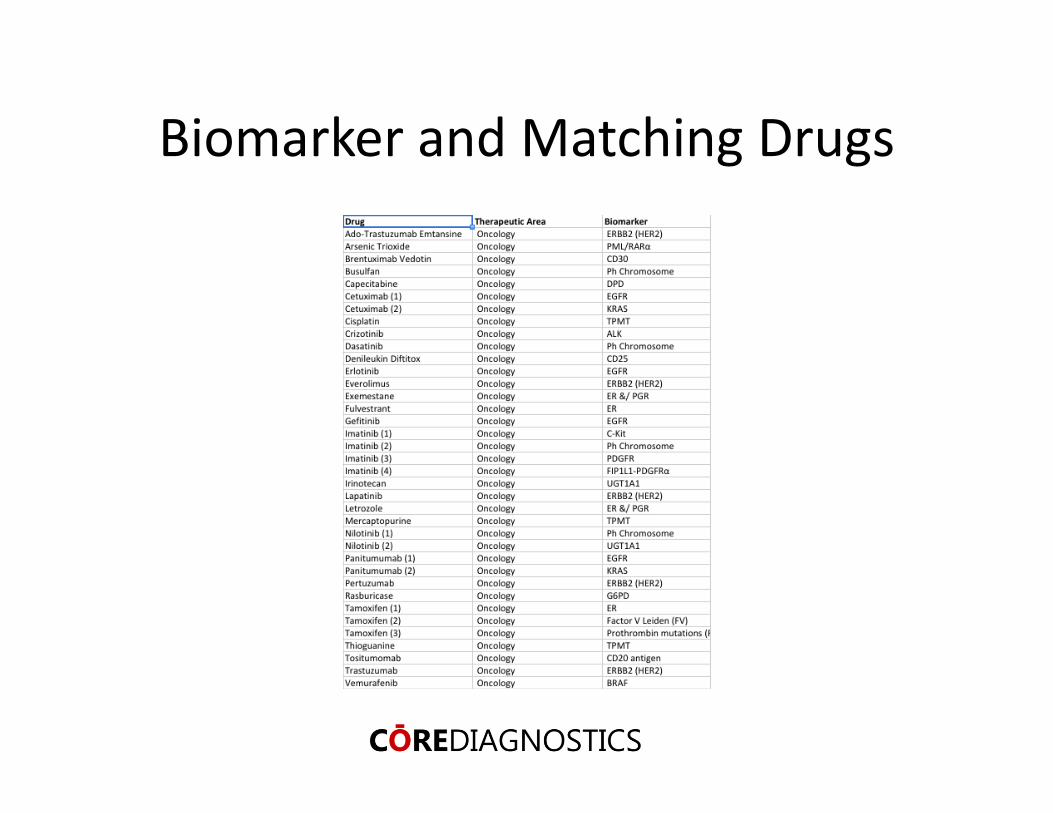
Biomarker and Matching Drugs
Ajay Pandita

Drug discovery: Past, Present & Future…
BasicResearch
Prototype design/Discovery
Preclinicaldevelopment
Phase I Phase II Phase III FDA filing, approval& launch
Label considerations basedon marker status
Label considerations basedon trial results
Marker assayvalidation
Analytical validationdiagnostic kit
Clinical validation diagnostickit; final platform determined
Targetselection
Targetvalidation
Identification of stratificationmarkers
Clinical utility forstratification markers
Clinical validation forstratification markers
Analytical validation
Pre-clinical feasibility
Clinical validation
Clinical utility
TMN Staging
Molecular Biomarkers• PD biomarker• Predictive• Prognostic• Resistance
BasicResearch
Non‐small cell lung cancer (NSCLC)
• ~ 120,000 new patients a year• Molecular stratification
– KRAS mutation– ALK fusion– EGFR (mutation, amplification)
• MET over‐expression
Confidential 80

MET• Evidence of underlying genetic events responsible for oncogene activation
• Expressed in human tumors primarily in epithelial tumors
• Transgenic mice develop tumors
• Prognostic factor
C‐Met expression: poor prognostic marker
Masuya et al, Br J Cancer. 2004 Apr 19;90(8):1555‐62
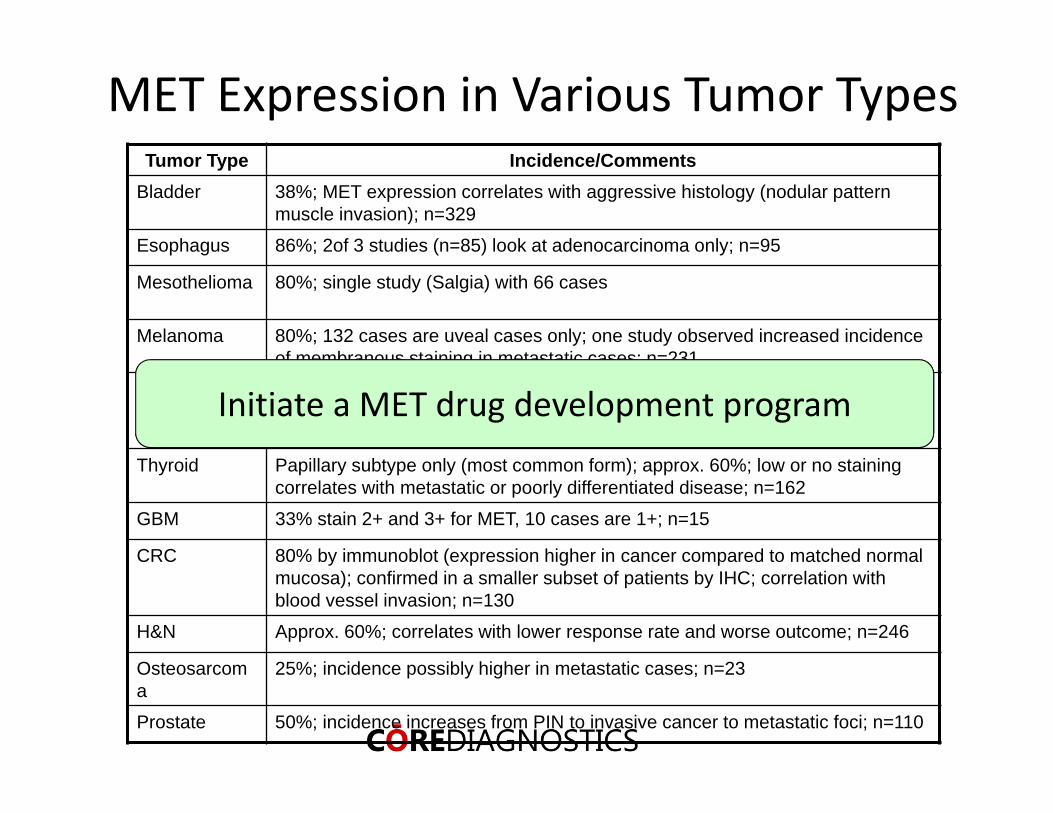
MET Expression in Various Tumor TypesTumor Type Incidence/Comments
Bladder 38%; MET expression correlates with aggressive histology (nodular pattern muscle invasion); n=329
Esophagus 86%; 2of 3 studies (n=85) look at adenocarcinoma only; n=95
Mesothelioma 80%; single study (Salgia) with 66 cases
Melanoma 80%; 132 cases are uveal cases only; one study observed increased incidence of membranous staining in metastatic cases; n=231
Breast The largest study (n=>300 patients) by Rimm (well respected pathologist) shows 28% incidence and correlation with high nuclear grade and poor clinical outcome
Thyroid Papillary subtype only (most common form); approx. 60%; low or no staining correlates with metastatic or poorly differentiated disease; n=162
GBM 33% stain 2+ and 3+ for MET, 10 cases are 1+; n=15
CRC 80% by immunoblot (expression higher in cancer compared to matched normal mucosa); confirmed in a smaller subset of patients by IHC; correlation with blood vessel invasion; n=130
H&N Approx. 60%; correlates with lower response rate and worse outcome; n=246
Osteosarcoma
25%; incidence possibly higher in metastatic cases; n=23
Prostate 50%; incidence increases from PIN to invasive cancer to metastatic foci; n=110
Initiate a MET drug development program
Companion Diagnostic Assays• IHC for over‐expression
– IHC score of 2+, 3+ or H score >200; Dx positive• MET FISH assay for gain/amplification
– >5 copies of MET/cell; Dx positive• MET mRNA expression• HGF expression• MET mutation• Plasma MET levels
Spigel et al. JCO, 2013; Koeppen et al. CCR, 2014
Diagnostic hypothesis & strategyDx Hypothesis
• No clear predictive diagnostic hypothesis from preclinical studies• Target (c‐Met) expression may enrich population likely to benefit
• Elevated c‐Met expression is a poor prognosis factor• Preclinical activity in high c‐Met expressing models
Dx Strategy• A companion Dx test to measure c‐Met protein on tumor cells was developed for potential patient stratification in a pivotal study
• Phase II study sized to evaluate cMet expression and incorporated as primary endpoint
• Exploratory objectives incorporated to evaluate additional markers that may influence clinical benefit to MetMab
• EGFR/KRAS mutation status, MET copy number, MET/EGFR pathway gene expression
Spigel et al. JCO, 2013; Koeppen et al. CCR, 2014
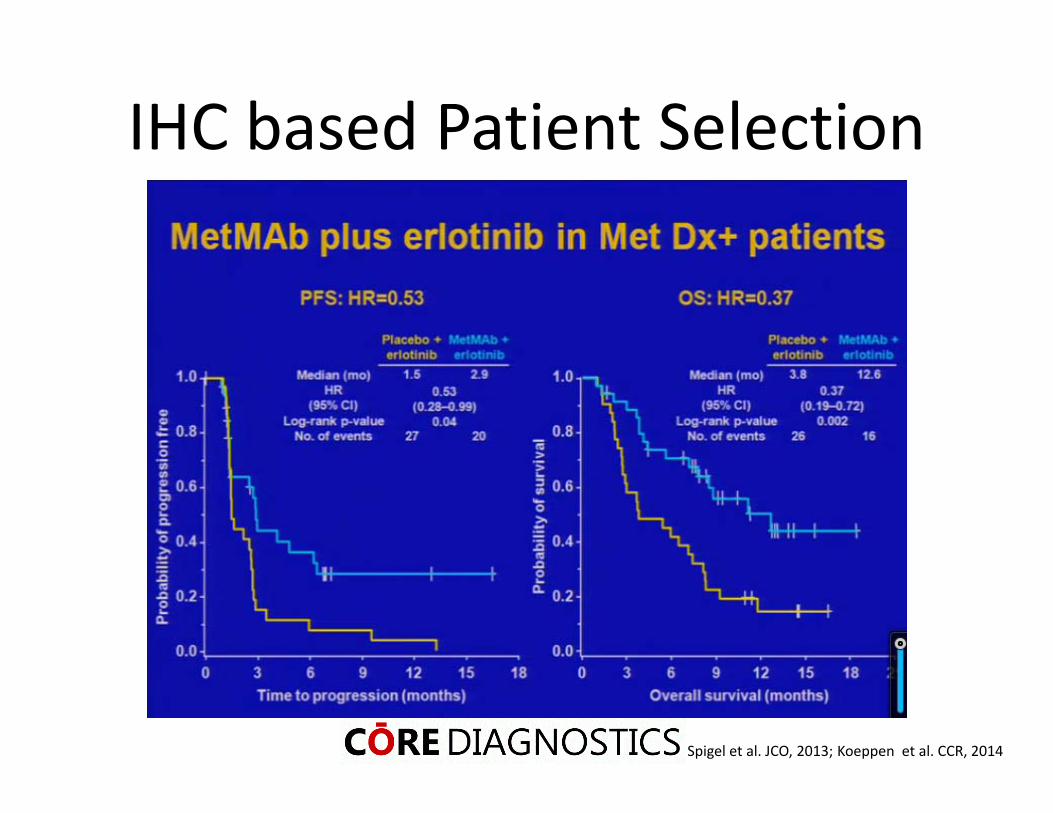
IHC based Patient Selection
Spigel et al. JCO, 2013; Koeppen et al. CCR, 2014
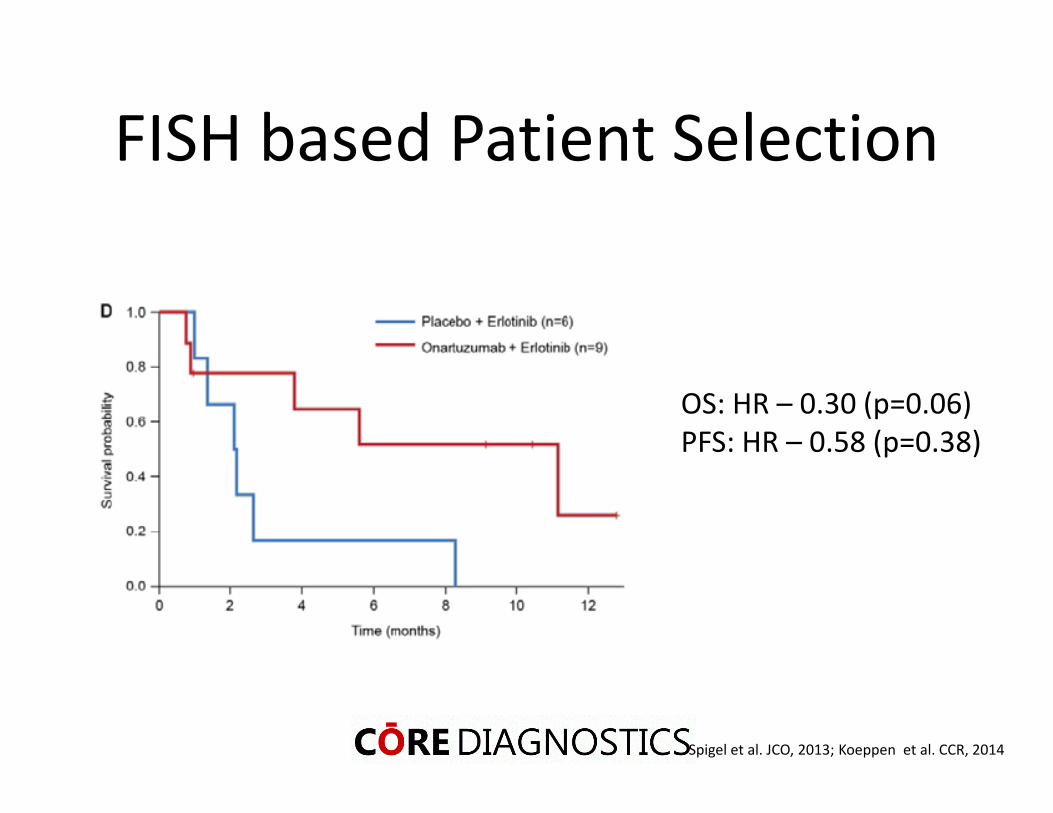
FISH based Patient Selection
OS: HR – 0.30 (p=0.06)PFS: HR – 0.58 (p=0.38)
Spigel et al. JCO, 2013; Koeppen et al. CCR, 2014
Conclusions
• Anti‐met Ab is a potent and selective antibody targeting MET
• MET IHC and FISH are independent predictors for MET based targeted therapy
• MET IHC seems to be a better predictive assay
Confidential 87
Resistance biomarkers
• A test that correlates with resistance to treatment. They improve our ability to understand resistance mechanisms to treatment.
• Mutation in abl for imatinib• T790M for anti‐EGFR therapy• BRAF amplifications for MEK inhibitors
Resistance in Targeted Therapy
• Clinical resistance is likely to reduce the clinical benefit of targeted therapy agents
• Understanding the range of mechanisms contributing to targeted therapy resistance pre‐clinically provides hypothesis for clinical studies
Mechanism of Resistance
• HER2 positive PIK3CA mutant cell line (KPL4)– Resistance to HER2 inhibitors due to PIK3CA mutation
– Sensitive to PI3K inhibitors• Develop KPL4 resistance to PI3K inhibitors• Mechanism of resistance?• OncoScan (Affymetrix) Kit
– Based on molecular inversion probes (MIB)– http://www.affymetrix.com/estore/promotions/mip/index.affx
Huw et al. Oncogenesis, 2013
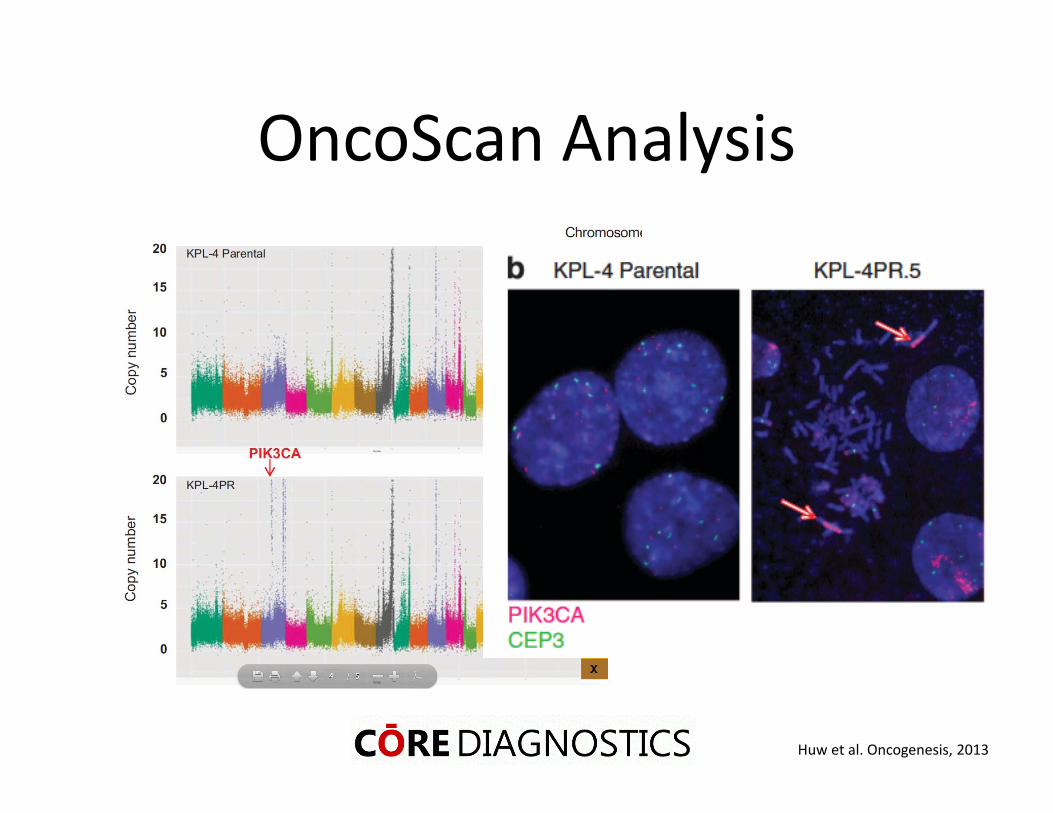
OncoScan Analysis
Huw et al. Oncogenesis, 2013
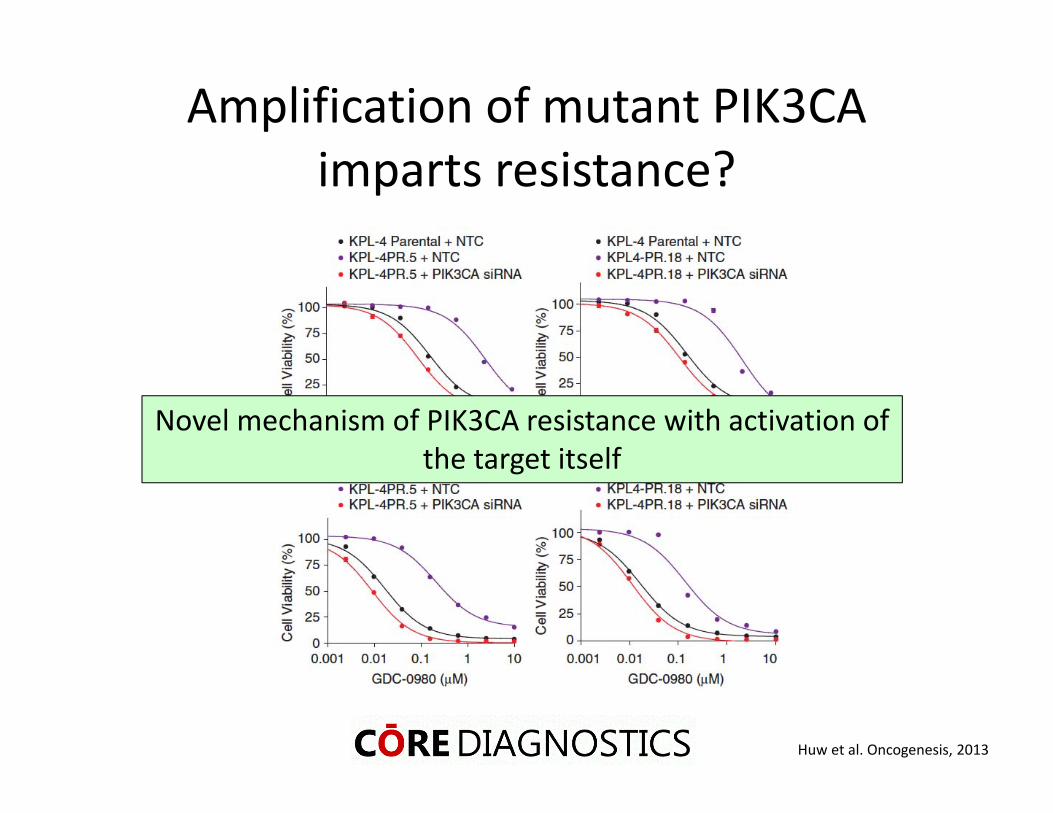
Amplification of mutant PIK3CA imparts resistance?
Novel mechanism of PIK3CA resistance with activation of the target itself
Huw et al. Oncogenesis, 2013
Conclusions
• New technologies aid in discovering novel biomarkers/signatures
• Patient stratification based on these Biomarkers open doors to better clinical management
Confidential 93
Ajay Pandita
Acknowledgements• GNE: Bob Yauch, Sankar Mohan, Jiping Zha, Rajiv Raja, Lukas Amler, Garret Hampton, Wei Yu, Premal Patel, Amy Peterson, Ling Huw, Jill Sproeke, Mark Lackner
• Clinicians: David Spigel, Thomas Ervin, Rodryg Ramlau, Davey Daniel, Jerome Goldschmidt Jr., George Blumenschein Jr., Maciej Krzakowski, Gilles Robinet, Christelle Clement‐Duchene, Fabrice Barlesi, Ramaswamy Govindan, Taral Patel, Sergey Orlov, Michael Wertheim
• Core Diagnostics: Sankar Mohan, Rob Monroe• Patients & families of the patients

To submit yourquestions, type them into the text box and
click
Participating Experts
Sponsored by:
Brought to you by the Science/AAAS Custom Publishing Office
Solid Tumors Reveal Their SecretsPredictive and Prognostic Evidence from Copy Number Analysis
Webinar Series
June 11, 2014
Paul C. Boutros, Ph.D.Ontario Institute for Cancer ResearchToronto, Canada
Ajay Pandita, D.V.M., Ph.D.Core DiagnosticsPalo Alto, CA
For related information on this webinar topic, go to:www.affymetrix.com/oncoscan
Look out for more webinars in the series at:
webinar.sciencemag.org
To provide feedback on this webinar, please e‐mailyour comments to [email protected]
Brought to you by the Science/AAAS Custom Publishing Office
Sponsored by:
Solid Tumors Reveal Their SecretsPredictive and Prognostic Evidence from Copy Number Analysis
Webinar Series
June 11, 2014