solid-phase radioimmunoassay humanimmunoglobulin ...iai.asm.org/content/15/3/883.full.pdf ·...
TRANSCRIPT

INFECTION AND IMMUNITY, Mar. 1977, p. 883-889Copyright X 1977 American Society for Microbiology
Vol. 15, No. 3Printed in U.S.A.
Solid-Phase Radioimmunoassay of Human ImmunoglobulinM and Immunoglobulin G Antibodies Against HerpesSimplex Virus Type 1 Capsid, Envelope, and Excreted
AntigensKIRSTI 0. K. KALIMO,* REIJO J. MARTTILA, KAISA GRANFORS, AND MATTI K. VILJANEN
Departments of Virology, Dermatology and Medical Microbiology, University of Turku,SF-20520 Turku 52, Finland
Received for publication 26 August 1976
A solid-phase radioimmunoassay developed in our laboratory for detection ofhuman viral immunoglobulin M (IgM) and IgG antibodies was applied todemonstrate human class-specific antibody response against capsid, envelope,and excreted antigens of herpes simplex virus type 1. In primary infections, aclear IgM and IgG antibody response was found predominantly against theenvelope components, whereas the IgM and IgG antibodies to the capsid antigenappeared more slowly. Increasing IgG antibody titers to the excreted antigenwere also found in primary infections, though appearing more slowly thanantibodies to the other subunit antigens. The antibody response against capsidand envelope antigens was not type specific, whereas in primary infections IgGclass antibodies against the excreted antigen showed distinct type specificity. Inrecurrent infections, no significant level of IgM class antibodies was demon-strated, but in the patients with a severe secondary herpes simplex virusinfection a definite IgM class antibody response was found against the envelopeantigen. In addition, during severe secondary infections the antibody responseagainst the excreted antigen was enhanced. The host IgG antibody response inrecurrent infections was directed against the envelope and excreted antigens,whereas the level of the capsid antibodies was relatively stable.
Antibody response to subunit antigens ofherpes simplex virus (HSV) types 1 and 2, i.e.,the envelope, capsid, and soluble antigens, hasbeen studied by the complement fixation tech-nique (6) and by an indirect hemagglutinationtest (la). The findings hitherto can be summa-rized as follows: (i) in primary herpetic infec-tions, antibody response against the envelopeantigen is predominant compared to thatagainst the capsid antigen; (ii) in patients withrecurrent herpetic infections, antibodiesagainst the capsid antigen seem to increase;(iii) recurrent HSV infections seem to broadenheterotypic reactivity between type 1 and type2 immune sera with the capsid and envelopeantigens; (iv) antibodies against the solubleantigen can be readily detected in animal im-mune sera, but only rarely in human serumspecimens; and (v) none of these antigensshows significant type specificity, though inantibody response against proteins excretedfrom HSV-infected cells, on the other hand,considerable type specificity was observed inanimal sera (5).
Recently, a sensitive radioimmunoassay
(RIA) technique was developed in our labora-tory to detect antibodies to rubella virus (4).The same methodology was further applied tothe detection ofHSV antibodies (Kalimo et al.,J. Immunol. Methods, in press) and measlesvirus antibodies (1) in human serum speci-mens. The advantages of the technique devel-oped are high sensitivity and the possibility todemonstrate both immunoglobulin G (IgG) andIgM class antibodies.In the present study class-specific antibody
responses detected by RIA in human seraagainst the crude and subunit antigens of HSVtype 1 are described, and a possible diagnosticvalue of the antibody changes during primaryand secondary HSV infections is discussed.
MATERIALS AND METHODSVirus. For preparing all antigens the VR strains
of HSV type 1 grown in Vero cells in 950-ml Rouxbottles was used.
Culture media. To prepare the crude, capsid, orenvelope antigens, Eagle basal medium was supple-mented with 0.2% bovine albumin, fraction V. Eaglebasal medium without any supplements was used toproduce the excreted antigen.
883
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
884 KALIMO ET AL.
Crude antigen. Harvesting and purification ofthecrude antigen was done as previously described(Kalimo et al., in press). In brief, infected cells wereharvested when a cytopathic effect (CPE) was evi-dent in 75 to 100% of the cells and separated by low-speed centrifugation. The cells were made 2% (vol/vol) in Dulbecco phosphate-buffered saline and dis-rupted by freezing and thawing, followed by sonica-tion. After low-speed centrifugation, the superna-
tant was collected and further centrifuged at 100,000x g for 2 h. The pellet was run through a 10 to 60%(wt/vol) linear sucrose gradient at 100,000 x g for 2h. The resulting band contained the viral material;the band was collected and sucrose was removed byan additional centrifugation.
Capsid antigen. The preparation of the capsidantigen was carried out as described by Martin et al.(6). HSV-infected cells were harvested at 75% CPEinto 2.5% Nonidet P-40 solution and sonicated. Thesuspension was filtered through 0.45- and 0.22-,um membrane filters (Millex, Millipore S.A. 67120,Molsheim-France). The filtrate was layered onto a
30% (wt/vol) sucrose cushion and centrifuged at100,000 x g for 1 h. The pellet contained the capsidantigen.
Envelope antigen. The method of Martin et al. (6)was used. Infected cells were scraped into the main-tenance medium at 75 to 100% CPE. After disrup-tion by sonication, the suspension was centrifugedat 100,000 x g for 1 h. The pellet was treated with50% diethyl ether for 30 min and then dialyzedagainst 0.85% NaCl buffered at pH 10.4 with 0.05 Mglycine NaOH. The dialysate was layered onto a35% (wt/vol) sucrose cushion and centrifuged for 1 hat 100,000 x g. The supernatant fluid containing theenvelope antigen was collected and dialyzed againstphosphate-buffered saline.
Excreted antigen. The preparation of this antigenwas carried out according to Kaplan et al. (5). Theculture medium was decanted when the infectedcells showed 75% CPE, usually 50 to 55 h postinfec-tion. After low-speed centrifugation to remove thecellular debris, the supernatant was further centri-fuged at 100,000 x g for 1 h to sediment the viralparticles. The supernatant fluid was extensively di-alyzed and considered as the excreted antigen.
Electron microscopy. Specimens from the crude,capsid, and envelope antigens were prepared on car-bon-coated Formvar grids and negatively stainedwith 2% phosphotungstic acid, pH 6.5, and exam-ined with a JEM 100C electron microscope (Fig. la-c).
RIA. The RIA used to detect class-specific HSVantibodies has been described previously in detail(Kalimo et al., in press). Briefly, fourfold serialserum dilutions were incubated in plastic tubes withthe antigen-coated polystyrene balls. After incuba-tion for 1 h at 37°C, the serum was aspirated off andthe balls were washed twice with 5 ml of tap water.An aliquot of '25I-labeled anti-human IgG or IgMcontaining 30,000 cpm was added to each tube. Theanti-human immunoglobulins were prepared insheep. For immunization, pure IgG and IgM frac-tions were used. They were tested to be monospecificby immunodiffusion and immunoelectrophoresis
INFECT. IMMUN.
(12). After incubation for 1 h at 370C for IgG deter-mination and for 16 h at room temperature for IgMdetermination, the radioactive solution was aspir-ated off and the balls were washed as above. Theballs were removed into clean plastic tubes and thebound radioactivity was counted in a LKB Wallac1280 gamma counter.A positive and negative control serum and a
buffer blank, where serum was omitted, were in-cluded in each test.
End-point titer values were obtained from thecpm (log,,,) versus dilution (log2) curve of each speci-men. The end-point titer was taken to mean thatserum dilution where the cpm values obtained werethree times those of the negative serum in the IgGassay and two times the negative in the IgM assay.Titers were expressed as log2 values of reciprocals ofthe serum dilutions.Serum specimens. The serum specimens con-
sisted of 64 specimens from 39 patients obtainedfrom the Department of Dermatology and Depart-ment of Infectious Diseases at Turku UniversityHospital and from the routine material in our diag-nostic laboratory.The specimens comprised the following. (i)
Twenty-three specimens were from 10 patients witha primary HSV infection: 6 patients with clinicallyestablished diagnosis ofHSV type 1 infection, and 4patients with type 2 infection. (ii) Twenty specimenswere from 15 patients with a history of several re-current herpetic infections during the past year: 11patients with a history of orofacial lesions, and 4 pa-tients with genital lesions. (iii) Fifteen specimenswere from 10 patients with a past history of herpeticinfections, with the proviso that the last infectionhave been more than 1 year previously. In thisgroup no patient gave a definite history of genitallesions. (iv) Six specimens were from 4 patients witha previous history of HSV infections and currentsevere secondary HSV infection: 1 patient with aserious recurrent stomatitis, 1 with meningitis, and2 with a generalized eczema herpeticum.The pooled, positive control serum for the crude,
capsid, and envelope antigen assays consisted offour convalescent phase specimens, and for the as-say of the excreted antigen a large serum pool of onepatient with several recurrent HSV infections wasused. The negative control serum was pooled fromone donor who did not have a history of HSV infec-tions and did not show antibodies to any of theantigens tested in the HSV RIA. The specimenswere stored at -200C until used.
RESULTSRIA reactivity of different antigens. To es-
tablish the reactivity ofthe subunit antigens inthe RIA, tests with positive and negative con-trol sera were performed. The ratio ofthe radio-activity bound by the positive and by the nega-tive serum, i.e., the binding ratio, in the IgGassay with all antigens was high, sometimeseven as high as 30. There was, however, adistinct difference between different antigensregarding the binding ratios. When the balls
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from

FIG. 1. Electron micrographs ofHSV antigens used in the assays stained with phosphotungstic acid. Bar= 100 nm. (a) Crude antigen, (b) capsid antigen, (c) envelope antigen.
Pr '..
Al.--,'
-C
.it
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
886 KALIMO ET AL.
coated with the capsid antigen were used, thecpm values of the negative sample in the dilu-tions from 1:8 to 1:4,096 were three to four timeshigher than the cpm values obtained with theenvelope-antigen-coated balls. At higher dilu-tions the difference reduced to twofold. Withthe excreted antigen the cpm values for thenegative serum were the same as or two timeshigher than those obtained with the envelopeantigen. In the IgM assay the binding ratiosbetween positive and negative samples werelower than in the IgG assay, reaching ratiosfrom 4 to 8. As in the IgG assay, the capsidantigen gave a higher nonspecific backgroundthan the envelope antigen. IgM class antibodiesagainst the excreted antigen were detected nei-ther in the positive control serum nor in any ofthe sera tested.Antibody response in patients with a pri-
mary HSV infection. The development of IgMand IgG class antibodies in the serum speci-
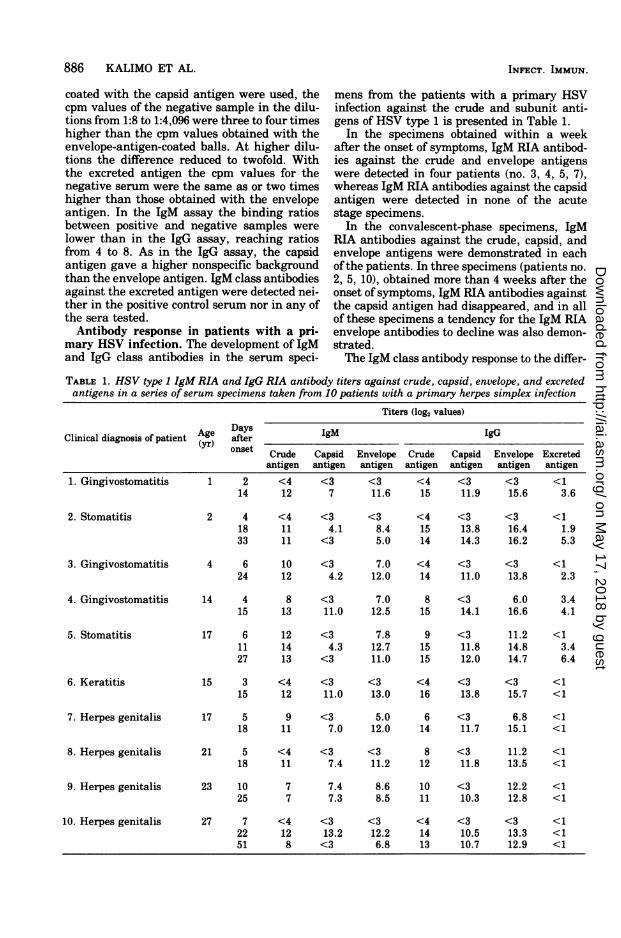
mens from the patients with a primary HSVinfection against the crude and subunit anti-gens of HSV type 1 is presented in Table 1.
In the specimens obtained within a weekafter the onset of symptoms, IgM RIA antibod-ies against the crude and envelope antigenswere detected in four patients (no. 3, 4, 5, 7),whereas IgM RIA antibodies against the capsidantigen were detected in none of the acutestage specimens.
In the convalescent-phase specimens, IgMRIA antibodies against the crude, capsid, andenvelope antigens were demonstrated in eachofthe patients. In three specimens (patients no.
2, 5, 10), obtained more than 4 weeks after theonset of symptoms, IgM RIA antibodies againstthe capsid antigen had disappeared, and in allof these specimens a tendency for the IgM RIAenvelope antibodies to decline was also demon-strated.The IgM class antibody response to the differ-
TABLE 1. HSV type 1 IgM RIA and IgG RIA antibody titers against crude, capsid, envelope, and excretedantigens in a series ofserum specimens taken from 10 patients with a primary herpes simplex infection
Titers (log2 values)
Clinical diagnosis of patient (AYge) gM IgGonset Crude Capsid Envelope Crude Capsid Envelope Excreted
antigen antigen antigen antigen antigen antigen antigen
1. Gingivostomatitis 1 2 <4 <3 <3 <4 <3 <3 <114 12 7 11.6 15 11.9 15.6 3.6
2. Stomatitis 2 4 <4 <3 <3 <4 <3 <3 <118 11 4.1 8.4 15 13.8 16.4 1.933 11 <3 5.0 14 14.3 16.2 5.3
3. Gingivostomatitis 4 6 10 <3 7.0 <4 <3 <3 <124 12 4.2 12.0 14 11.0 13.8 2.3
4. Gingivostomatitis 14 4 8 <3 7.0 8 <3 6.0 3.415 13 11.0 12.5 15 14.1 16.6 4.1
5. Stomatitis 17 6 12 <3 7.8 9 <3 11.2 <111 14 4.3 12.7 15 11.8 14.8 3.427 13 <3 11.0 15 12.0 14.7 6.4
6. Keratitis 15 3 <4 <3 <3 <4 <3 <3 <115 12 11.0 13.0 16 13.8 15.7 <1
7. Herpes genitalis 17 5 9 <3 5.0 6 <3 6.8 <118 11 7.0 12.0 14 11.7 15.1 <1
8. Herpes genitalis 21 5 <4 <3 <3 8 <3 11.2 <118 11 7.4 11.2 12 11.8 13.5 <1
9. Herpes genitalis 23 10 7 7.4 8.6 10 <3 12.2 <125 7 7.3 8.5 11 10.3 12.8 <1
10. Herpes genitalis 27 7 <4 <3 <3 <4 <3 <3 <122 12 13.2 12.2 14 10.5 13.3 <151 8 <3 6.8 13 10.7 12.9 <1
INFECT. IMMUN.
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from
RIA ANTIBODIES TO HSV SUBUNIT ANTIGENS 887
ent HSV 1 antigens appeared to be similar inall patients, although six patients had a clini-cally established type 1 infection and four pa-tients had type 2 infection.IgG RIA antibodies against the crude and
envelope antigens were detected in four pa-
tients (no. 4, 5, 7, 8) in the specimens obtainedwithin a week after the onset of symptoms.None of those specimens showed IgG RIA anti-bodies against the capsid antigen. In only one
case (no. 4) were IgG RIA antibodies againstthe excreted antigen detected in the acute-phase specimens.
In the convalescent-phase specimens, IgGRIA antibodies to the crude, envelope, and cap-
sid antigens could be demonstrated in each pa-tient. In antibody response to the crude, capsid,or envelope antigens used, no difference wasfound between the patients with type 1 or type 2infection. On the other hand, IgG RIA antibod-ies against the excreted antigen could be ob-served in rather low titers in the convalescentsera from five patients (no. 1, 2, 3, 4, and 5), allof them with a clinically established type 1infection. None ofthe four patients with a clini-cal diagnosis of genital herpes infection hadantibodies against the excreted antigen. Also,one patient with a clinical diagnosis of keratitisdid not show antibodies to the excreted antigen.Antibodies in patients with a previous his-
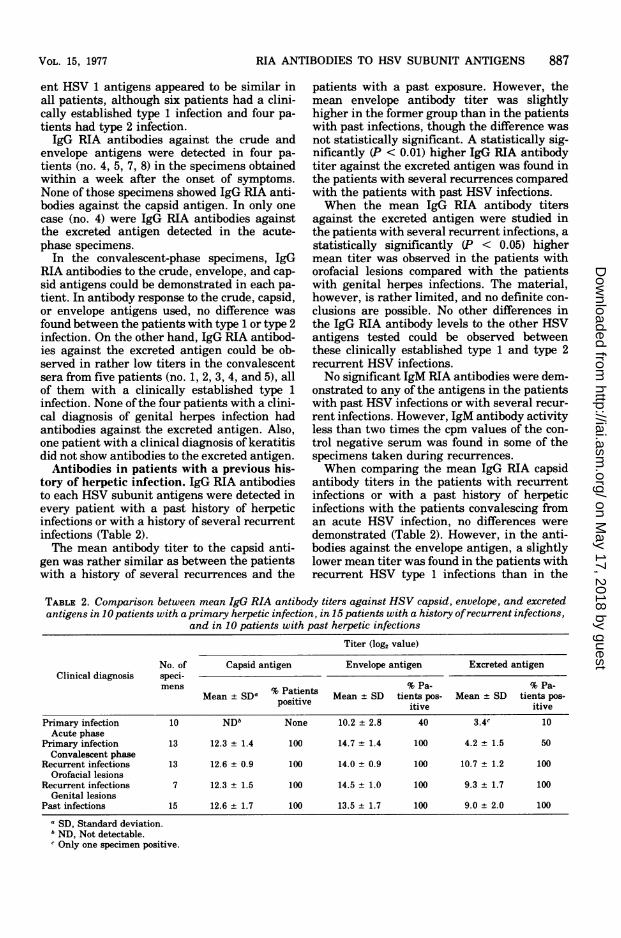
tory of herpetic infection. IgG RIA antibodiesto each HSV subunit antigens were detected inevery patient with a past history of herpeticinfections or with a history of several recurrentinfections (Table 2).The mean antibody titer to the capsid anti-
gen was rather similar as between the patientswith a history of several recurrences and the
patients with a past exposure. However, themean envelope antibody titer was slightlyhigher in the former group than in the patientswith past infections, though the difference wasnot statistically significant. A statistically sig-nificantly (P < 0.01) higher IgG RIA antibodytiter against the excreted antigen was found inthe patients with several recurrences comparedwith the patients with past HSV infections.When the mean IgG RIA antibody titers
against the excreted antigen were studied inthe patients with several recurrent infections, a
statistically significantly (P < 0.05) highermean titer was observed in the patients withorofacial lesions compared with the patientswith genital herpes infections. The material,however, is rather limited, and no definite con-
clusions are possible. No other differences inthe IgG RIA antibody levels to the other HSVantigens tested could be observed betweenthese clinically established type 1 and type 2recurrent HSV infections.No significant IgM RIA antibodies were dem-
onstrated to any of the antigens in the patientswith past HSV infections or with several recur-rent infections. However, IgM antibody activityless than two times the cpm values of the con-
trol negative serum was found in some of thespecimens taken during recurrences.
When comparing the mean IgG RIA capsidantibody titers in the patients with recurrentinfections or with a past history of herpeticinfections with the patients convalescing froman acute HSV infection, no differences were
demonstrated (Table 2). However, in the anti-bodies against the envelope antigen, a slightlylower mean titer was found in the patients withrecurrent HSV type 1 infections than in the
TABLE 2. Comparison between mean IgG RIA antibody titers against HSV capsid, envelope, and excretedantigens in 10 patients with aprimary herpetic infection, in 15 patients with a history ofrecurrent infections,
and in 10 patients with past herpetic infectionsTiter (log2 value)
No. of Capsid antigen Envelope antigen Excreted antigenClinical diagnosis speci-
mens %PainsPa- % Pa-Mean + SDa % Patients Mean + SD tients pos- Mean + SD tients pos-
itive itive
Primary infection 10 NDb None 10.2 + 2.8 40 3.4c 10Acute phase
Primary infection 13 12.3 ± 1.4 100 14.7 + 1.4 100 4.2 ± 1.5 50Convalescent phase
Recurrent infections 13 12.6 + 0.9 100 14.0 + 0.9 100 10.7 + 1.2 100Orofacial lesions
Recurrent infections 7 12.3 ± 1.5 100 14.5 ± 1.0 100 9.3 ± 1.7 100Genital lesions
Past infections 15 12.6 + 1.7 100 13.5 ± 1.7 100 9.0 ± 2.0 100
aSD, Standard deviation.bND, Not detectable.¢ Only one specimen positive.
VOL. 15, 1977
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from

888 KALIMO ET AL.
patients in the convalescent phase; but, on theother hand, the patients with several recur-rences showed a somewhat higher mean titerthan the patients with past infections. A statis-tically significantly (P < 0.05) lower mean anti-body titer against the envelope antigen wasobserved in the patients with past infectionswhen compared with the patients convalescingfrom acute infection.
Fifty percent of the convalescent sera showedantibodies with a low mean titer to the excretedantigen, whereas all sera from the patientswith several recurrences or with past infectionscontained antibodies to that antigen in a signif-icantly (P < 0.001) higher mean titer, thusdemonstrating the slow appearance and in-crease of these antibodies.
In four patients with a severe secondary HSVinfection (Table 3), IgM class antibodies to theenvelope antigen were demonstrated, but noneof those patients showed IgM antibodiesagainst the capsid antigen. In two patientsfrom whom paired samples were available, afourfold IgG antibody rise against the excretedantigen was observed, whereas one of the pa-tients also showed a similar antibody riseagainst the envelope antigen and almost four-fold antibody rise against the capsid antigen.
DISCUSSION
In the present study, human antibody re-sponse to subunit antigens of HSV type 1 wasstudied by solid-phase RIA during primary andsecondary herpetic infections. This highly sen-sitive method, which allows both IgM and IgGclass-specific antibody detection, was applied todemonstrate antibodies to the HSV crude, cap-sid, envelope, and excreted antigens.
In the primary infections, an IgM class anti-body response was clearly detected in all pa-tients. In the acute phase of the infection, theIgM response was detected against the crudeand envelope antigens, but not against the cap-sid antigen. However, during the convalescent
phase, IgM antibodies were also demonstratedagainst the capsid antigen in all patients. Inthree patients from whom the specimens wereobtained more than 4 weeks after onset, theIgM RIA antibodies against the capsid antigenhad disappeared; simultaneously the IgM enve-lope antibody titers also decreased.An IgG class antibody response against the
envelope and crude antigens was mainly dem-onstrated concurrently with the appearance ofthe IgM class antibodies, whereas the IgG cap-sid antibodies were detectable somewhat later.Thus, it is evident that during primary HSVinfection the host IgM and IgG antibody re-sponse is primarily directed towards the enve-lope antigen of HSV and that antibodiesagainst the internal components appear moreslowly. Similar findings have been also previ-ously obtained by less sensitive techniques,namely, the complement fixation test (6) andthe indirect hemagglutination test (la).The predominant host response against the
envelope components of HSV is conceivablyconnected with the early appearance of virus-induced antigens in the external membranes ofHSV-infected cells. In tissue culture conditionsafter a few hours of infection, the cell surfaceacquires virus-specific antigens (3, 8, 10), whichboth antigenically (8) and biochemically (9) cor-respond to the proteins in the viral envelope.Thus, already in an early phase of infection theantigenically altered cell surfaces are availableto the host immune mechanisms. In addition,the antibodies against the envelope componentsseem to be of primary importance to the hostsince they contain the neutralizing activity (7,11).The results of this study also indicate that
HSV type 1 and type 2 share common antigensboth in the envelope and in the capsid; thus adirect typing of antibody response using thesesubunit antigens does not seem to be possible.However, a distinct type specificity in the anti-body response was observed against the ex-creted antigen, since all patients with a genital
TABLE 3. HSV type 1 IgM RIA and IgG RIA antibody titers against capsid, envelope, and excreted antigensin fbur patients with a severe secondary herpetic infection
Titer (log2 value)Days 1gM IgG
Clinical diagnosis Age (yr) after on- _ _ _ _ _ _ _set Capsid an- Envelope Capsid anti- Envelope Excreted
tigen antigen gen antigen antigenEczema herpeticum 20 4 <3 <3 11.9 13.3 9.6
14 <3 11.2 13.7 15.3 14.3Eczema herpeticum 25 5 <3 11.1 13.3 14.7 10.0
11 <3 13.5 13.2 15.0 13.0Stomatitis 46 8 <3 10.9 13.6 15.2 11.5Meningitis 66 10 <3 11.1 13.6 14.7 9.0
INFECT. IMMUN.
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from

RIA ANTIBODIES TO HSV SUBUNIT ANTIGENS 889
primary HSV infection were negative with re-gard to those antibodies, whereas most of thepatients with a clinical diagnosis ofHSV type 1infection showed increasing antibody titers tothe excreted antigen. On the other hand, fourpatients with recurrent genital lesions dis-played antibodies to the excreted antigen ofHSV type 1, but the possibility of the previoustype 1 infection could not be excluded. Thus,the excreted antigen seems to have promisingtype specificity also in human HSV infections,as has previously been observed in animalmodels (5). Further studies, however, are re-quired to establish the final usefulness of thisantigen in serological typing ofHSV infections.
In earlier studies the antibody levels to thecapsid antigen have shown a tendency to in-crease during recurrent HSV infections (la, 6).Our present results indicate that these antibod-ies remain relatively stable on the levelreached in primary infection even in the pa-tients with several recurrences. On the otherhand, the level of antibodies to the envelopeantigen seems to increase in the patients withseveral recurrent HSV infections, suggestingthat the antigenically altered cell surfaces arethe main antigenic stimulus also during recur-rences. However, an increased antibody level tothe excreted antigen was also found in thesepatients and an enhanced antibody responsewas found against the excreted antigen in thepatients with a severe secondary HSV infec-tion, a finding which could be used as a crite-rion in differentiating primary and secondaryinfections. The difference between the slow pri-mary response to the excreted antigen and theenhanced reactivity during the secondary infec-tions compared with the antibody responseagainst the capsid and envelope antigens re-mains obscure at the moment. However, on thebasis of our findings it seems reasonable tosuppose that the excreted antigen differs anti-genically from the capsid and envelope compo-nents of HSV. Consequently, the excreted pro-teins might be nonstructural ones as suggested(5) and as is the case with the proteins excretedfrom pseudorabies virus-infected cells (2, 5).Although IgM class antibodies could not be
detected against any of the subunit or crudeHSV antigens in ordinary recurrent infections,in the patients with a severe secondary infec-tion, an IgM class antibody response againstthe envelope antigen was clearly demonstratedin all patients. In those patients a pronouncedIgG class antibody response against the ex-creted antigen was also observed and, in onepatient, IgG class antibody response againstthe envelope and capsid antigens. Our findingsindicate that an IgM class antibody response is
connected with severe, secondary HSV infec-tions and suggest that also during recurrentinfections of a less severe nature there might bea host IgM antibody response to HSV, thoughto a minor degree and beyond the sensitivity ofthe RIA technique used.
ACKNOWLEDGMENTSThis study was supported by grants from The Academy of
Finland, Medical Research Council.The excellent technical assistance of Marita Maaronen
and Soile Niittoaho is gratefully acknowledged.We are grateful to P. Terho for kindly providing some of
the serum specimens, and to H. Kalimo for examining theelectron microscopic specimens.
LITERATURE CITED1. Arstila, P., T. Vuorimag, K. Kalimo, P. Halonen,
M. Viljanen, K. Grenfors, and P. Tolvanen. 1977.Solid-phase radioimmunoassay for IgG and IgM anti-bodies against measles virus. J. Gen. Virol. 34:167-176.
la. Back, A. F., and N. J. Schmidt. 1974. Reactivity ofenvelope, capsid, and soluble antigens of herpesvirushominis types 1 and 2 in the indirect hemagglutina-tion test. Infect. Immun. 10:102-106.
2. Erickson, J. S., and A. S. Kaplan. 1973. Synthesis ofproteins in cells infected with herpesvirus. IX. Sul-fated proteins. Virology 55:94-102.
3. Ito, M., and A. L. Barron. 1972. Surface antigen pro-duced by herpes simplex virus (HSV). J. Immunol.108:711-718.
4. Kalimo, K. 0. K., 0. H. Meurman, P. E. Halonen, B.R. Ziola, M. K. Vilbanen, K. Granfors, and P. Toiva-nen. 1976. Solid-phase radioimmunoassay of rubellavirus immunoglobulin G and immunoglobulin M an-tibodies. J. Clin. Microbiol. 4:117-123.
5. Kaplan, A. S., J. S. Erickson, and T. Ben-Porat. 1975.synthesis of proteins in cells infected with herpesvi-rus. X. Proteins excreted by cells infected with herpessimplex virus types 1 and 2. Virology 64:132-143.
6. Martin, M. L., E. L. Palmer, and R. E. Kissling. 1972.Complement-fixing antigens of herpes simplex virustypes 1 and 2: reactivity of capsid, envelope, andsoluble antigens. Infect. Immun. 5:248-254.
7. Roane, P. R., Jr., and B. Roizman. 1964. Studies of thedeterminant antigens of viable cells. H. Demonstra-tion of altered antigenic reactivity of HEp-2 cellsinfected with herpes simplex virus. Virology 22:1-8.
8. Roizman, B. 1970. Herpesviruses, membranes, and thesocial behavior of infected cells, p. 37-72. In M.Sanders (ed.), Viruses affecting man and animals. W.H. Green, Inc., St. Louis, Mo.
9. Roizman, B. 1971. Biochemical features ofherpesvirus-infected cells, p. 109-138. In W. Nakahara, K. Ni-shioka, T. Hirayma, and Y. Ito (ed.), Recent ad-vances in human tumor virology and immunology(Proc. 1st Int. Symp. Princess Takamatsu CancerRes. Fund). University of Tokyo Press, Tokyo.
10. Schwartz, J., and T. S. Elizan. 1975. Altered immuno-logic specificity of cells infected with herpes simplexvirus: recognition by human antiserum. Z. Immuni-taetsforsch. 148:291-298.
11. Smith, J. W., S. P. Lowry, J. L. Melnick, and W. E.Rawls. 1972. Antibodies to surface antigens ofherpes-virus type 1- and type 2-infected cells among womenwith cervical cancer and control women. Infect. Im-mun. 5:305-310.
12. Viljanen, M. K., K. Granfors, and P. Toivanen, 1975.Radioimmunoassay of class-specific antibodies(RIACA): chicken antibodies to bovine serum albu-min. Immunochemistry 12:699-705.
VOL. 15, 1977
on May 17, 2018 by guest
http://iai.asm.org/
Dow
nloaded from