socioeconomic status in danish women with polycystic ovary
TRANSCRIPT
University of Southern Denmark
Socioeconomic status in Danish women with polycystic ovary syndrome. A register-basedcohort study
Rubin, Katrine H; Andersen, Marianne skovsager; Abrahamsen, Bo; Glintborg, Dorte
Published in:Acta Obstetricia et Gynecologica Scandinavica
DOI:10.1111/aogs.13514
Publication date:2019
Document version:Accepted manuscript
Citation for pulished version (APA):Rubin, K. H., Andersen, M. S., Abrahamsen, B., & Glintborg, D. (2019). Socioeconomic status in Danish womenwith polycystic ovary syndrome. A register-based cohort study. Acta Obstetricia et Gynecologica Scandinavica,98(4), 440-450. https://doi.org/10.1111/aogs.13514
Go to publication entry in University of Southern Denmark's Research Portal
Terms of useThis work is brought to you by the University of Southern Denmark.Unless otherwise specified it has been shared according to the terms for self-archiving.If no other license is stated, these terms apply:
• You may download this work for personal use only. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying this open access versionIf you believe that this document breaches copyright please contact us providing details and we will investigate your claim.Please direct all enquiries to [email protected]
Download date: 10. Dec. 2021
This article has been accepted for publication and undergone full peer review but has not
been through the copyediting, typesetting, pagination and proofreading process, which may
lead to differences between this version and the Version of Record. Please cite this article as
doi: 10.1111/aogs.13514
This article is protected by copyright. All rights reserved.
DR DORTE GLINTBORG (Orcid ID : 0000-0002-8338-8025) PROFESSOR MARIANNE SKOVSAGER ANDERSEN (Orcid ID : 0000-0002-4603-9504)
Article type : Original Research Article
Socioeconomic status in Danish women with polycystic ovary syndrome. A
register-based cohort study
Katrine H Rubin1, Marianne Andersen
3, Bo Abrahamsen
1,2, Dorte Glintborg
3
1Odense Patient data Explorative Network-OPEN, Department of Clinical Research, University of
Southern Denmark, and Odense University Hospital, Odense, Denmark
2Department of Internal Medicine, Holbaek Hospital, Denmark
3Department of Endocrinology, Odense University Hospital, Odense, Denmark
Corresponding author:
Dorte Glintborg
Odense University Hospital, Kløvervænget 6, 3rd floor, 5000 Odense C, Denmark
Email: [email protected]
Conflict of interest:
The authors have nothing to disclose.

This article is protected by copyright. All rights reserved.
ABSTRACT
Introduction: Low socioeconomic status (SES) could be associated with increased risk of
polycystic ovary syndrome (PCOS) and vice versa. Possible associations between SES,
obesity, and ethnicity in PCOS are undetermined. Material and methods: National register-
based study including women with PCOS aged 25 years or above (PCOS Denmark and an
embedded cohort; PCOS Odense University Hospital (OUH)) and one control population.
PCOS Denmark (N=13,891) included women with PCOS in the Danish National Patient
Register. Women in PCOS OUH underwent clinical examination (N=814). Three age
matched controls were included per patient (N=41,584). The main outcome measure was SES
(Personal income, occupational status, and education). Results: The median (Q1; Q3) age of
women in PCOS Denmark and controls was 33 (29; 39) years. Women with personal income
in the lower tertile had higher probability of a PCOS diagnosis than women in the high-
income tertile (adj. odds ratio OR 1.5 (95% CI; 1.4 to 1.6)). Women being unemployed or on
welfare payment (adj. OR 1.5 (95% CI; 1.4 to1.6)), or being early retired (OR 1.8 (95% CI;
1.7 to 2.0)) had higher probability of a PCOS diagnosis than women affiliated to the labour
market. Women originating from the Middle East more often had PCOS (adj. OR 3.2 (95%
CI 2.8 to 3.7)) compared to women originating from Europe. In PCOS OUH, SES was lower
in obese vs. normal weight women. Conclusions: A diagnosis of PCOS was associated with
lower SES. In PCOS, women of foreign origin and women with obesity, more often had low
SES.
Keywords:
polycystic ovary syndrome, register-based, socioeconomic status, ethnicity, nationwide
Key message
A diagnosis of PCOS was associated with lower socioeconomic status in a Danish register based study
population. Furthermore, in women with PCOS, socioeconomic status was inversely associated with
obesity.
This article is protected by copyright. All rights reserved.
Abbreviations
FG-score: Ferriman Gallwey score
OUH: Odense University Hospital
PCOS: polycystic ovary syndrome
SES: socioeconomic status
OR odds ratio
INTRODUCTION
Polycystic ovary syndrome (PCOS) can be diagnosed in around 10% of premenopausal women (1,2).
PCOS is characterized by irregular menses, polycystic ovaries, and hyperandrogenism (1). Quality of
life may be impaired in PCOS and the risk of depression and development of medical and psychiatric
diseases is increased (3,4).
More than 50% women with PCOS are obese (5). Obesity is associated with a more severe PCOS
phenotype including more irregular menses, infertility, and hirsutism (6,7) and obesity is associated
with impaired quality of life and depression in PCOS (8,9). In the general population, Newton et al
reported a consistent association between lower life course socioeconomic status (SES) and obesity
among women in developed countries (10). Accordingly, obesity was associated with lower income
(11,12) and shorter education (13) in wealthy societies. Apart from obesity, other factors known to
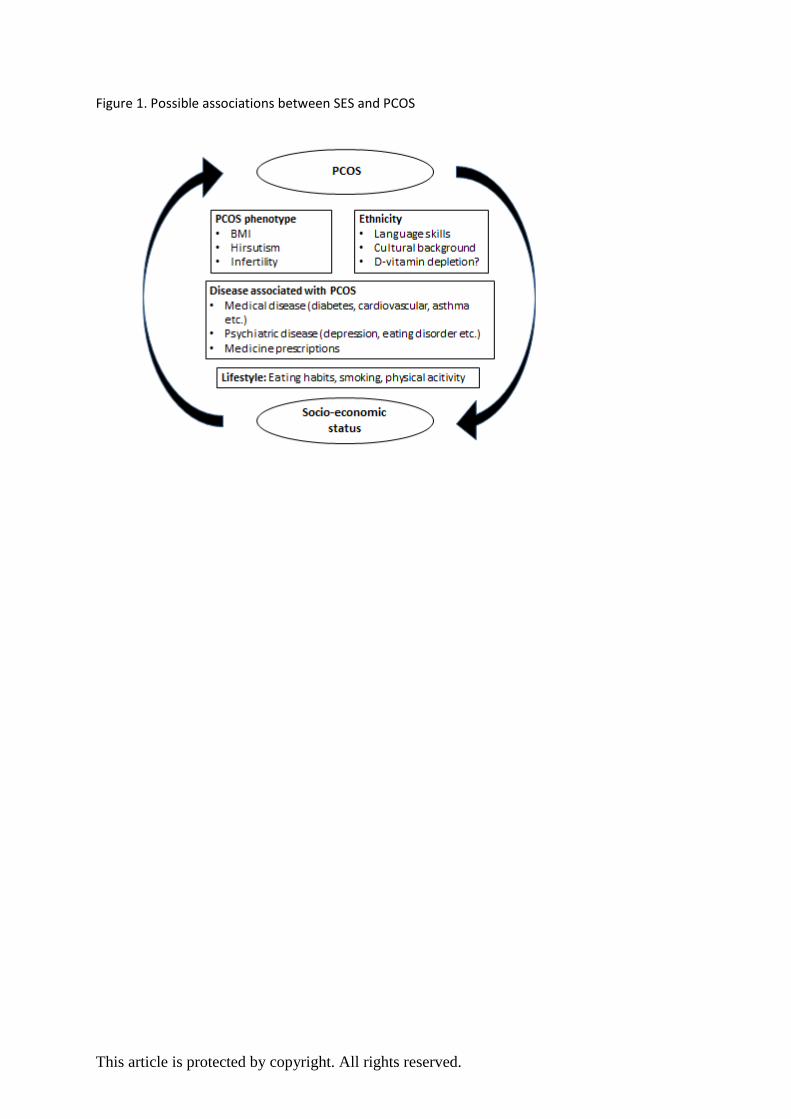
be associated with lower SES (14) are clustered in women with PCOS (figure 1). Women with PCOS
have increased risk of type 2 diabetes (15), hypertension (16) and dyslipidemia (17). Importantly,
obesity increases the risk of type 2 diabetes, cardiovascular disease, and several cancer types in
PCOS (18). Presence of obesity may therefore be associated with lower SES in PCOS. Furthermore,
PCOS is associated with increased risk of medical diseases such as asthma and thyroid disease and
psychiatric diseases including depression, anxiety and eating disorders (19). In accordance, women
with PCOS have more medicine prescriptions than controls (19). Higher morbidity also in young
women with PCOS (9,19) could be associated with low SES.
Women with PCOS could have a more unfavorable lifestyle compared to healthy women. Appetite
regulation may be impaired in PCOS (20) and women with PCOS more often had unhealthy dietary
This article is protected by copyright. All rights reserved.
intake compared to controls (21). We previously reported a higher prevalence of smoking in PCOS
vs. controls (22) and smoking was associated with a more adverse lipid profile (22) and insulin re-
sistance (23) in PCOS. Unhealthy lifestyle including low physical activity (24) could be associated with
low SES in PCOS (25).
Only two previous studies investigated SES in PCOS (26,27). Both studies reported an inverse associa-
tion between SES and BMI in PCOS (26,27), but the studies were of limited size (n<250) and one
study did not include healthy controls (26). The hypothesis that SES is lower in women with PCOS
compared to controls therefore remains to be tested.
Ethnic background affects PCOS phenotype and metabolic risk profile (28,29). Danish women with
PCOS originating from the Middle East had higher Ferriman Gallwey (FG)-score and lower insulin
sensitivity than ethnic Northern European Danish women with PCOS (29). A more adverse metabolic
risk profile and a more severe PCOS phenotype in women with PCOS originating from the Middle
East could be associated with lower SES. Furthermore, low vitamin D levels are common in women
with PCOS originating from the Middle East (30). The possible effect of low vitamin D levels on men-
tal health is debated (31). Previous studies regarding SES in PCOS (26,27) included women from Italy
(26) (ethnic homogeneous) and USA (27) (50% white, 50% black). The hypothesis that ethnic back-
ground could be associated with SES in PCOS was not tested in these studies.
The aim of the present register-based study was to compare SES in women with a diagnosis
of PCOS and controls based on data from Danish national registers. We also investigated
possible associations between SES, obesity, and ethnic background in women with PCOS.
MATERIAL AND METHODS
Design and population
The study design and baseline data for this study cohort have been reported in detail earlier
(19). Data regarding development of type 2 diabetes, cardiovascular disease and incident
fractures (15,32,33) in the study cohort has been published recently. We included two patient
populations with PCOS and one control population (Figure 1). In women with hirsutism, the
prevalence of PCOS is more than 75% (34,35), and women with a diagnosis of hirsutism
were included in the patient cohort. PCOS Denmark included all women in Denmark aged
12-60 years, who were diagnosed through a hospital contact with PCOS (E282) and/or

This article is protected by copyright. All rights reserved.
hirsutism (L680) between January 1st, 1995 and the end of 2012. PCOS Odense University
Hospital (OUH) included an embedded cohort of women with PCOS and/or hirsutism treated
at OUH with available clinical and biochemical information. For each patient in PCOS
Denmark (and PCOS OUH), three control women born in the same year as the patient were
randomly drawn from the Civil Population Register. Controls were assigned the index date
(date of first PCOS diagnosis) of their matched PCOS case and should be alive at the index
date of their PCOS case.
Exclusion criteria were women with the diagnoses E221 (hyperprolactinemia), E220
(acromegaly), E24 (Cushing’s syndrome), E25 (adrenogenital syndrome), and Q96 (Turner
syndrome). Furthermore, women aged <25 years at the index date were excluded.
Variables
Danish National Registries
All Danish individuals are assigned a unique personal identification number. The
identification number can be used to link data from all public registers at an individual level
(36,37). Denmark has a large array of high-quality national registers that cover the entire
population and include consistently coded long-term data (37). Register based data provide a
unique opportunity to perform population-based studies linking information about hospital
diagnoses, socioeconomic data, medicine prescriptions at the individual level with a very
high validity (37,38).We retrieved information from registers about SES, ethnicity and area of
origin, and hospital contacts in the study population.
The Danish Patient Register (NPR) holds data on all inpatient hospital contacts in Denmark
since 1977 and since 1995, outpatient contacts are included in Danish Patient Register. The
diagnostic codes used in the patient register are classified according to the Danish version of
the International Classification of Diseases, version 8 (ICD8: 1977-1993) and, since 1994,
version 10 (ICD10). As previously described (19), Danish Patient Register was used to
identify the PCOS Denmark cohort and to obtain information regarding comorbidity in the
study population.
Socioeconomic status (SES)
Variables on SES included information on personal income, occupational status, and education. Data
were retrieved from Danish registers at Statistics Denmark as described below on the index year for
each woman.
This article is protected by copyright. All rights reserved.
Personal income: Personal income was extracted from the Income Statistics Register (39) and includ-
ed information on the available average income after tax and interest (included salary, retirement
benefits, welfare payment, remuneration, company profits etc.). The income was categorized into
tertiles (high, middle, low).
Occupational status (affiliation to the labour market): Occupational status was also extracted from
the Income Statistics Register (39) and divided into five categories: Affiliated to labour market (em-
ployed or self-employed), education, unemployed or welfare payment, early retirement, and un-
known or missing.
Education: Education was extracted from the Population Education Register and included infor-
mation on the highest completed education based on the International Standard Classification of
Education (40). Population Education Register covers education and training completed in Denmark.
Information on education acquired outside Denmark and information for immigrants is based on
self-reported information on completed education (if available).
Education level was divided into: Master´s or doctoral education, short tertiary education (incl.
bachelor), vocational education, upper secondary school, basic school (primary), and unknown or
missing.
Covariates
We gathered information on ethnicity and area of origin from the Danish Civil Registration System
(36).
Ethnicity: Ethnicity was extracted from the Civil Registration System (36) and divided into Danish,
immigrants, descendants, and unknown or missing.
Area of origin: Area of origin was extracted from Civil Registration System (36) and divided into
women from Europe, Middle East, and other (America, Africa, Oceania, and unknown or missing)
(Countries shown in Supporting Information Table S1).
This article is protected by copyright. All rights reserved.
Comorbidity: The Charlson comorbidity index is based on 19 comorbid conditions (41) and was calcu-
lated from the ICD-10 operationalization by Quan et al.(42). The Charlson comorbidity index was
used to classify comorbid conditions among the respondents from 1995 to index date. To calculate
the Charlson score, we used information from the Danish Patient Register and the score was catego-
rized into no comorbidity (0), and plus one comorbidity (≥1).
Statistical analyses
Descriptive analyses for categorical variables were presented as frequencies and difference
between PCOS and controls was evaluated by Chi-square test. Continuous variables were
tabulated as medians (with quartiles, Q1 and Q3) and nonparametric test on the equality of
medians was used to test for differences between groups.
Conditional logistic regression analyses were used to calculate odds ratios (OR) with 95%
confidence intervals and corresponding p-values, to examine the association between PCOS
and SES, ethnicity, area of origin and comorbidity separately for PCOS Denmark and PCOS
OUH vs. matched controls. The OR was reported unadjusted and mutually adjusted for
education, occupational status, personal income, ethnicity and area of origin.
Logistic regression analyses were performed to analyse the association between 1) BMI
(divided into BMI≥25 kg/m2 and BMI<25 kg/m
2 as reference) and SES and 2) FG-score
(divided into FG-score ≥5 and FG-score<5 as reference) and SES in the PCOS OUH cohort.
The logistic regression analyses were carried out unadjusted and mutually adjusted for age,
education, occupational status, personal income, ethnicity and area of origin.P-values <0.05
were considered statistically significant. Analyses were conducted using STATA 14
(StataCorp 2015).
Sensitivity analyses were performed to explore the possible effect of area of origin. Included
women were divided according to origin from Europe or the Middle East. In these
conditional logistics regressions analyses, analyses were mutually adjusted for education,
occupational status, and personal income.
Sensitivity analyses were repeated in women above age 30 years. The Rotterdam criteria
were introduced in 2003 and include more mild PCOS phenotypes. Therefore, two sensitivity
analyses were performed in women with index date before and after 2003, respectively.
This article is protected by copyright. All rights reserved.
Furthermore, women with idiopathic hirsutism could be included in the diagnosis L680.
Therefore, we performed a sensitivity analysis including only women with the diagnosis
E282 (excluding women with L680).
Ethical approval
The core study was an open register-based cohort study. The study did not need approval
from the local Ethics committee or Institutional Review Board by Danish law. The study was
approved by the Data Protection Agency and by Statistics Denmark, project no 704175.
RESULTS
The flow chart of included women is summarized in Figure 1. A total of 55,475 women
fulfilled the inclusion criteria, 13,891 women with PCOS (PCOS Denmark and the embedded
cohort PCOS OUH, N=814) and 41,584 controls.
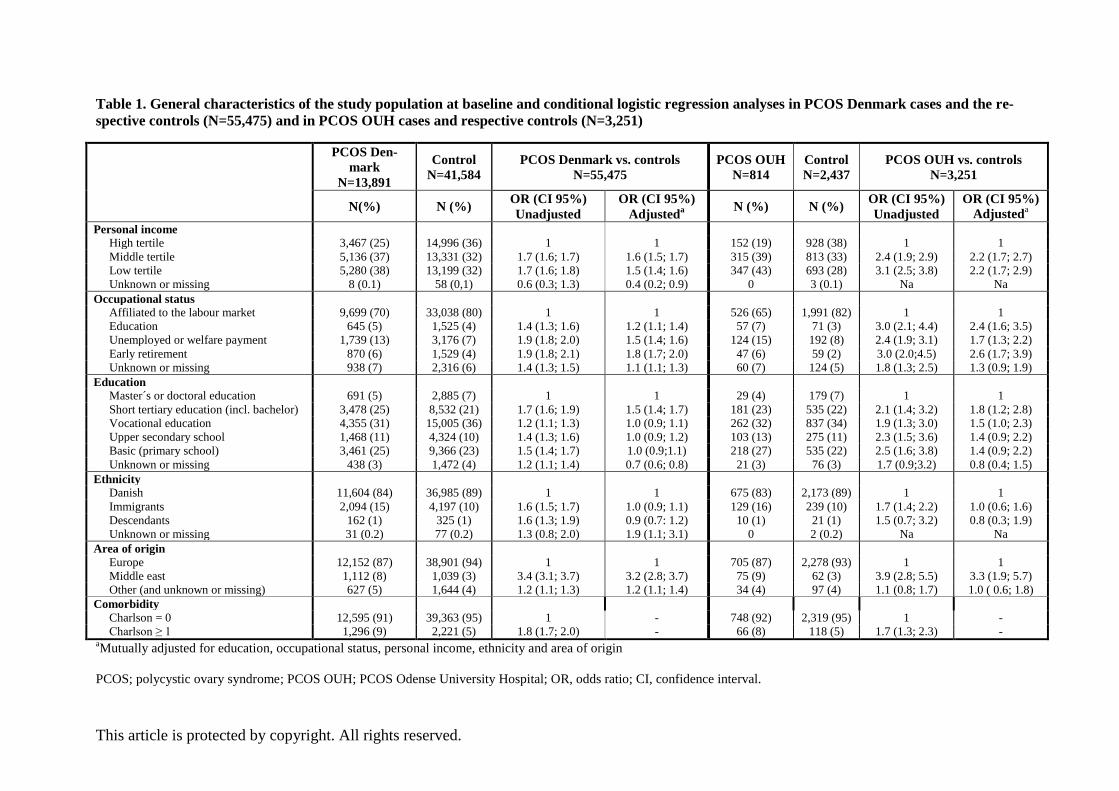
Baseline characteristics of the study population are shown in Table 1. The median age was 33
years in all study cohorts (range 25-60 years). Women in PCOS Denmark were more often in
the middle tertile (37 vs. 32%) and low tertile (38 vs. 32%) of personal income than controls.
Women in PCOS Denmark had lower frequency of affiliation to the labour market (70 vs.
80%) and the occupational status was more often unemployed or on welfare payment (13 vs.
7 %) than controls. Women with PCOS more often had basic school (25 vs. 23%) and short
tertiary education (incl. bachelor) (25 vs. 21%) as highest education compared to controls.
Women in PCOS Denmark more often originated from the Middle East (8 vs. 3%) compared
to controls and more women in PCOS Denmark vs. controls were immigrants (15 vs. 10%).
Comorbidity according to Carlson index ≥1 was more often present in women with PCOS vs.
controls (9 vs. 5%).
Women in PCOS OUH differed from the remaining women in PCOS Denmark regarding
personal income, occupational status and education (Supporting Information Table S2).
The conditional logistics regressions analyses (Table 1) showed significant associations
between PCOS diagnosis and SES (personal income, occupational status, and education).
Women with personal income in the low (OR 1.7) and middle tertile (OR=1.7) had a higher
probability of PCOS than women in the high-income tertile in the unadjusted analysis.
This article is protected by copyright. All rights reserved.
Associations between personal income and PCOS remained significant in the analysis
adjusted for education, occupational status, ethnicity and area of origin.
Women under education (OR=1.4), being unemployed or on welfare payment (OR=1.9), or
being early retired (OR=1.9) had higher probability of PCOS than women affiliated to the
labour market. Significant associations between occupational status and PCOS remained
significant in the adjusted analysis with slightly lower OR.
Women with short tertiary education (incl. bachelor) (OR= 1.7), vocational education
(OR=1.2), upper secondary school (OR= 1.4), and basic school (OR= 1.5) as the highest
educational levels more often had PCOS compared to women with master´s or doctoral
education. In adjusted analyses, only the significant association between short tertiary
education (incl. bachelor) and PCOS remained significant.
Immigrants and descendants more often had PCOS compared to women of European
ethnicity (unadjusted OR= 1.6, OR adjusted for SES not significant). Women originating
from the Middle East more often had PCOS (unadjusted OR=3.4 and adjusted OR= 3.2)
compared to women originating from Europe. Similar significant associations were seen in
the conditional logistic regressions analyses in women in PCOS OUH compared to their
controls, but with higher OR.
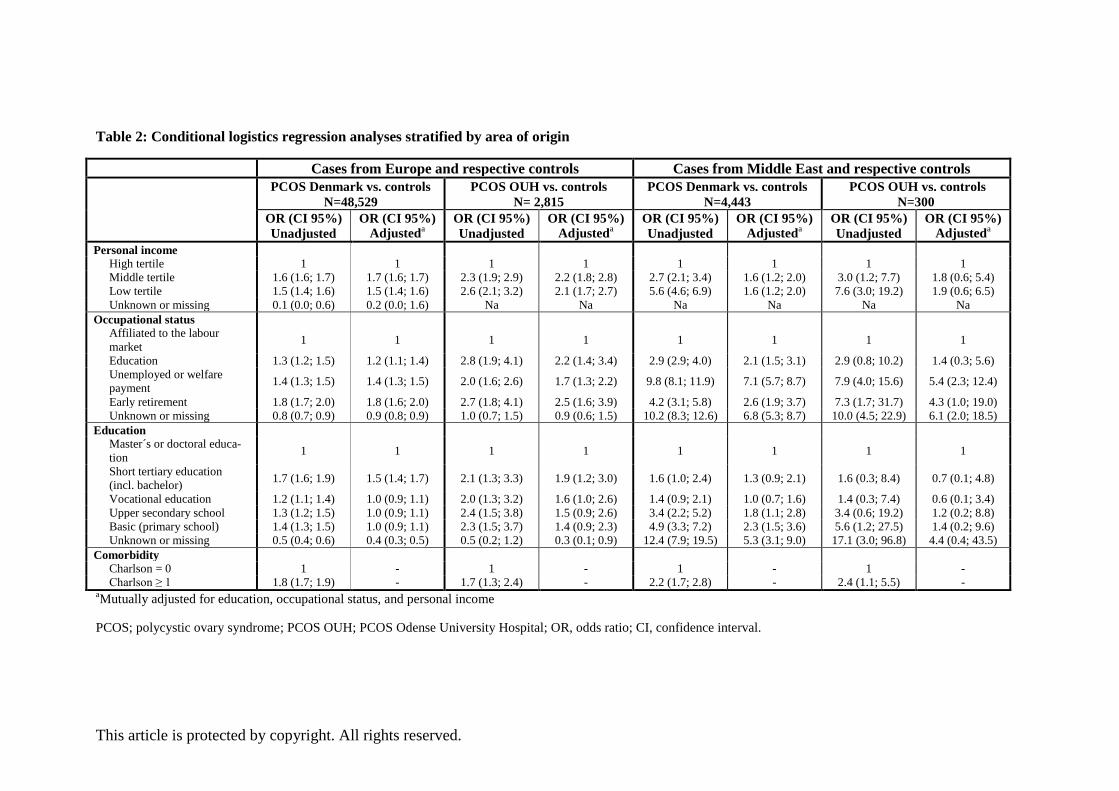
Sensitivity analyses:
Conditional logistic regressions analyses were repeated in women with PCOS originating
from Europe (N=12,152) and in women with PCOS originating from the Middle East
(N=1,112) compared to their age matched controls (Table 2). The association between SES
and PCOS remained significant when women were divided according to area of origin, but
with higher OR in women with PCOS originating from the Middle East compared to analyses
in the whole study cohort. In women with PCOS originating from the Middle East vs.
controls, women under education had adjusted OR=2.1, unemployed women or women on
welfare payment had adjusted OR=7.1 and women on early retirement had an adjusted
OR=2.6 for PCOS compared to women affiliated to the labour market. In women with PCOS
of European origin and their respective controls, results of logistic regression analyses
resembled analyses in the whole study cohort.
This article is protected by copyright. All rights reserved.
Analyses were repeated in the following sensitivity analyses 1: Women aged above 30 years
(N=38,064), 2: Women with index date before (N=23,417) and after (N=32.058) 2003, and 3:
Women with the diagnosis E282 (excluding the diagnosis L680) (N=28,912). This did not
change the findings, nor did analyses excluding all women with unknown or missing
information on personal income, occupational status and/or education (N=50,464). Results
for the five sensitivity analyses are shown in Supporting Information Table S3.
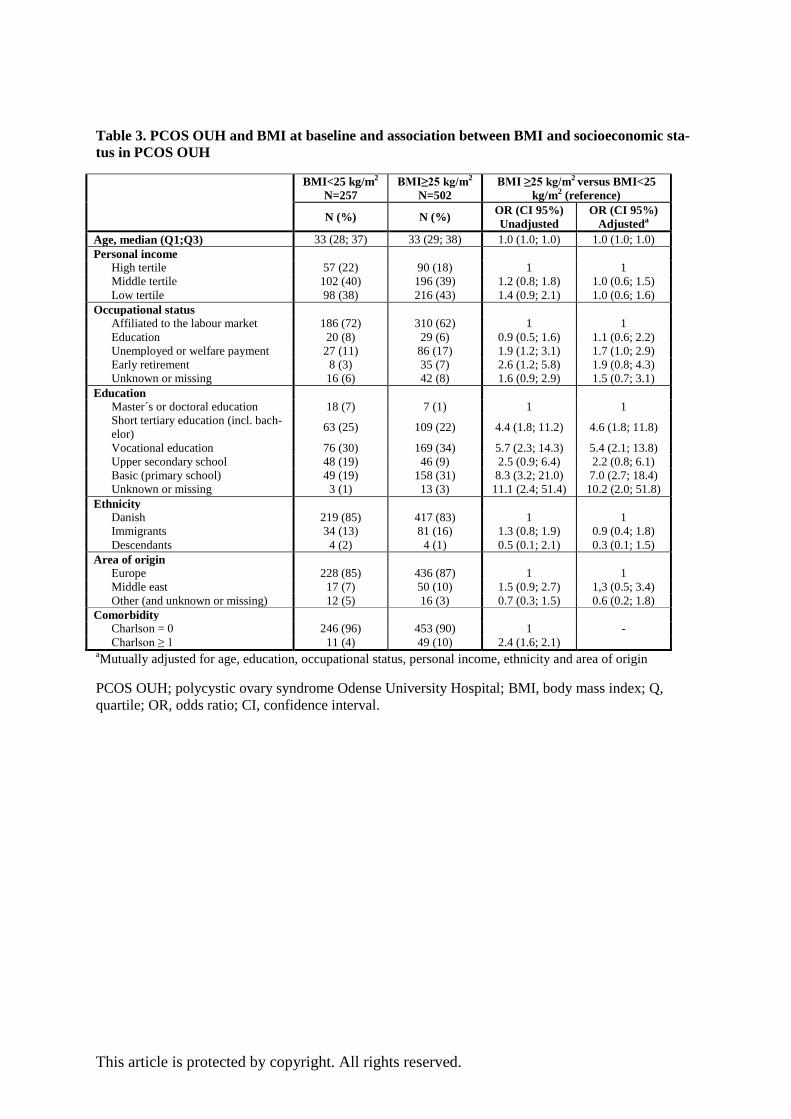
Table 3 shows associations between SES and obesity in PCOS. Women in PCOS OUH
(N=759) were categorized into BMI< 25 kg/m2
(N=257) and BMI≥25 kg/m2
(N=502).
Women with PCOS and BMI< 25 kg/m2
more often had high personal income (22 vs. 18%),
were affiliated to the labour market (72 vs. 62%) and had master´s or doctoral education (7 vs.
1%) or short tertiary education (incl. bachelor) (25 vs. 22%) compared to women with PCOS
and BMI≥25 kg/m2. In logistic regression analyses, women with PCOS, who were
unemployed or on welfare payment (OR=1.9) and early retirement (OR=2.6) had higher
probability of BMI≥25 kg/m2 than women affiliated to the labour market. Further, women
with PCOS and BMI≥25 kg/m2 more often had basic school as highest completed education
compared to women with PCOS and BMI< 25 kg/m2 (OR=8.3 in the unadjusted and OR=7.0
in the mutually adjusted analyses).
Analyses were repeated in PCOS OUH with women stratified according to FG-score
(Supporting Information Table S4). Women with FG-score ≥5 more often had vocational
education (34 vs. 24%) and basic school (28 vs. 24%) as the highest education level
compared to women with FG-score < 5, they were more often immigrants (19 vs. 8%) and
more often originated from the Middle East (12 vs. 2%). FG-score was not associated with
SES in logistic regression analyses.
DISCUSSION
To our knowledge this is the first nationwide, population-based study that reports lower SES in PCOS
compared to controls. We found that Danish women with PCOS more often had low personal in-
come, they were more often unemployed or on welfare payment and were more often early retired
compared to age matched controls. Furthermore, SES was inversely associated with obesity.
This article is protected by copyright. All rights reserved.
As previously reported (19), participants in our study population were relatively lean (median
BMI in PCOS OUH, 27 kg/m2). Our findings therefore supported that low SES should be
considered even in a relatively lean study population of women with PCOS. Furthermore,
area of origin and ethnicity were closely associated with SES. We found that immigrants and
women with PCOS originating from the Middle East had even higher risk of low SES
compared to women of Danish ethnicity and women of European origin.
The data from the present study expand findings from two previous studies regarding SES in
PCOS (26,27). Merkin et al included 938 American women and investigated childhood and
adult SES and risk of development of PCOS (27). The authors found that low childhood SES
(low education in parents) increased the risk of development of PCOS (27). However, this
association was only significant in women of high education. Furthermore, women with high
education had elevated risk of PCOS compared to women with lower education, which could
support increased attention of PCOS diagnosis in women of higher education (27). In
accordance with findings of the present study, significant associations between SES and risk
of PCOS development became stronger in obese compared to lean women (27). However,
study limitations may apply to the study by Merkin et al; the study was of limited size and
included a population of mixed ethnicity, and the diagnosis of PCOS was based on primarily
self-reported data (27). The use of self-reported data could explain some of the findings by
Merkin as women with higher education could be more likely to recall and report past and
current health conditions (27). Women of higher education could be more likely to use the
healthcare system and be diagnosed with PCOS (27). Furthermore, the authors suggested that
upward socioeconomic mobility; ie women with PCOS of high education having parents with
low education, could suffer from more peripubertal stress, greater incidence of obesity, and
thus early disruption of menstrual cycles (27). In the present study we did not include SES of
the parents, but clearly, more studies are needed regarding possible implications of upward
and downward socioeconomic mobility in women with PCOS.
Di Fede et al investigated possible associations between SES and PCOS phenotype in 244
Italian women with PCOS (26). No controls were included in the study. In accordance with
the present study, low family income and low education was associated with higher BMI
(26). Furthermore, low SES was associated with a more severe PCOS phenotype with higher
degree of anovulation, higher waist circumference, and higher insulin levels compared to
women with PCOS and high SES. These findings support the importance of high BMI for
This article is protected by copyright. All rights reserved.
low SES in PCOS. Obesity is closely associated with PCOS phenotype and infertility and
BMI is inversely associated with quality of life in PCOS (18). Furthermore, obesity is an
important risk factor for development of type 2 diabetes and cardiovascular disease in PCOS
(18). In accordance, we found that high FG-score was associated with lower SES, however
this association did not remain significant in logistic regression analyses. It is possible that
lean women with PCOS represent a separate PCOS phenotype (43,44) and metabolic risk in
lean women with PCOS could be determined primarily by hyperandrogenism (45). The
present study design did not allow us to compare SES in lean women with PCOS compared
to lean controls. The study by Merkin et al (27) supported that low parental education
predicted PCOS development, which could be due to poor nutritional habits (27), but genetic
and environmental factors should also be taken into consideration (46). The present study did
not include data regarding physical activity and smoking habits and therefore, we could not
test hypotheses regarding possible associations between BMI, physical activity, smoking, and
SES in PCOS.
In the present study, we investigated the importance of ethnic background for SES in PCOS.
We found that women of foreign origin had lower SES than women of Danish origin, and the
OR for low SES was higher in women with PCOS originating from the Middle East
compared to analyses in the whole study cohort. Several factors could have an adverse effect
on SES in foreign women. We previously reported that women originating from the Middle
East had higher FG-score and were more insulin resistant than women with PCOS originating
from Northern Europe (29). A more severe PCOS phenotype could have a negative impact
on SES in PCOS. In agreement with this hypothesis, we found that a high FG-score was more
prevalent in foreign women with PCOS compared to women with PCOS of Danish origin.
Furthermore, De Fede et al (26) found an inverse association between PCOS phenotype and
SES. Poor language skills and moving to a country of other culture and/or religion could also
have a negative effect on SES in foreign women with PCOS. The present study design did not
allow us to test this hypothesis. D-vitamin is important for brain development and function
(31). Low D-vitamin levels are associated with obesity, foreign origin, low sun exposure and
dietary intake without fatty fish and dairy products. We did not have data on D-vitamin levels
in the present study, and therefore we could not test possible associations between D-vitamin
levels, mental health and SES in the present study. Future studies are needed in foreign
women with PCOS to determine predictors for low SES and to improve possibilities for
structured intervention.

This article is protected by copyright. All rights reserved.
Strengths and limitations may apply in the present study. The study included a large and well-
characterized group of patients with PCOS, we embedded a clinical cohort into a national register-
based study, and we had access to well-validated register-based data. SES will be dependent on age.
Included women in the present study therefore should be aged at least 25 years. Some women could
finish their education at an older age, and we performed a sensitivity analyses in women aged 30
years or more. Inclusion of women aged 30 years or more did not change significant results. Some
limitations may apply to the present study design (15,32,33). Education level in immigrants could be
underestimated as their education must be individually reported to Statistics Denmark while educa-
tion completed in Denmark is already in the registers. Furthermore, the present matched case-
control design did not allow us to investigate the risk of low SES between foreign women with and
without PCOS. Many patients with PCOS are not seen at the hospital, but are treated by their gen-
eral practitioner or a private gynaecologist. Furthermore, some women in the control group could
have undiagnosed PCOS, which could lead to underestimation of differences in SES between women
with PCOS and controls. We included women from 1995 and onwards, whereas the Rotterdam crite-
ria were introduced in 2003 (1). Therefore, different criteria for PCOS would be applied in the earli-
est entries into the PCOS cohort. We included women with hirsutism in the PCOS population as the
majority of patients with clinical and/or biochemical hyperandrogenism are diagnosed with PCOS
(47-49). However, some women could have idiopathic hirsutism, and the inclusion of these women
in the PCOS cohort could lead to a type 2 error. The results from two sensitivity analyses where we
included only women with index date before 2003 and where we included only women with the
diagnosis E282 (PCOS) and excluded women with L680 (hirsutism) did not change significant results.
Our included study cohort was relatively lean and the ethnic background was relatively homogene-
ous. The findings of the present study therefore need to be confirmed in more obese study popula-
tions of other ethnic background. Our cohort (PCOS OUH) differed from PCOS Denmark in terms of
age, comorbidity and prescription history. However, the differences were small and therefore unlike-
ly to be a major source of bias in our findings.
CONCLUSION
SES was lower in women with PCOS compared to controls and SES was associated with
obesity and ethnic background. More studies are needed regarding the effect of medical and
lifestyle intervention on SES in PCOS.
This article is protected by copyright. All rights reserved.
Reference List
1. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consen-
sus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome.
Fertil Steril 2004;81:19-25.
2. Conway G, Dewailly D, Diamanti-Kandarakis E, et al. The polycystic ovary syndrome: a position
statement from the European Society of Endocrinology. Eur J Endocrinol 2014;171:1-29.
3. Cinar N, Kizilarslanoglu MC, Harmanci A, et al. Depression, anxiety and cardiometabolic risk in
polycystic ovary syndrome. Hum Reprod 2011;26:3339-3345.
4. Jones GL, Hall JM, Balen AH, Ledger WL. Health-related quality of life measurement in women
with polycystic ovary syndrome: a systematic review. Hum Reprod Update 2008;14:15-25.
5. Lim SS, Davies MJ, Norman RJ, Moran LJ. Overweight, obesity and central obesity in women
with polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update
2012;18:618-637.
6. Lim SS, Norman RJ, Davies MJ, Moran LJ. The effect of obesity on polycystic ovary syndrome: a
systematic review and meta-analysis. Obes Rev 2013;14:95-109.
7. Glintborg D, Petersen MH, Ravn P, Hermann AP, Andersen M. Comparison of regional fat mass
measurement by whole body DXA scans and anthropometric measures to predict insulin re-
sistance in women with polycystic ovary syndrome and controls. Acta Obstet Gynecol Scand
2016;95:1235-1243.
8. Altinok ML, Glintborg D, Depont CR, Hallas J, Andersen M. Prescription of antidepressants is
increased in Danish patients with polycystic ovary syndrome and is associated with
hyperandrogenism. A population-based cohort study. Clin Endocrinol (Oxf) 2013;80:884-889.
9. Glintborg D, Andersen M. MANAGEMENT OF ENDOCRINE DISEASE: Morbidity in polycystic
ovary syndrome. Eur J Endocrinol 2017;176:R53-R65.
10. Newton S, Braithwaite D, Akinyemiju TF. Socio-economic status over the life course and obesi-
ty: Systematic review and meta-analysis. PLoS ONE 2017;12:e0177151.
11. Wamala SP, Wolk A, Orth-Gomer K. Determinants of obesity in relation to socioeconomic sta-
tus among middle-aged Swedish women. Prev Med 1997;26:734-744.
12. Delva J, Johnston LD, O'Malley PM. The epidemiology of overweight and related lifestyle be-
haviors: racial/ethnic and socioeconomic status differences among American youth. Am J Prev
Med 2007;33:S178-S186.
13. Sabanayagam C, Shankar A, Wong TY, Saw SM, Foster PJ. Socioeconomic status and over-
weight/obesity in an adult Chinese population in Singapore. J Epidemiol 2007;17:161-168.
This article is protected by copyright. All rights reserved.
14. Tang KL, Rashid R, Godley J, Ghali WA. Association between subjective social status and cardi-
ovascular disease and cardiovascular risk factors: a systematic review and meta-analysis. BMJ
Open 2016;6:e010137.
15. Rubin KH, Glintborg D, Nybo M, Abrahamsen B, Andersen M. Development and risk factors of
type 2 diabetes in a nationwide population of women with polycystic ovary syndrome. J Clin
Endocrinol Metab 2017;102:3848-3857.
16. Glintborg D, Mumm H, Altinok ML, Richelsen B, Bruun JM, Andersen M. Adiponectin, interleu-
kin-6, monocyte chemoattractant protein-1, and regional fat mass during 12-month random-
ized treatment with metformin and/or oral contraceptives in polycystic ovary syndrome. J
Endocrinol Invest 2014;37(8):757-764.
17. Sundstrom P, I, Mellembakken JR, Papunen LM, et al. Should we individualize lipid profiling in
women with polycystic ovary syndrome? Hum Reprod 2016;32:966.
18. Glintborg D, Andersen M. Medical comorbidity in polycystic ovary syndrome with special focus
on cardiometabolic, autoimmune, hepatic and cancer diseases: an updated review. Curr Opin
Obstet Gynecol 2017;29:390-396.
19. Glintborg D, Hass RK, Nybo M, Abrahamsen B, Andersen M. Morbidity and medicine prescrip-
tions in a nationwide Danish population of patients diagnosed with polycystic ovary syndrome.
Eur J Endocrinol 2015;172:627-638.
20. Mumm H, Altinok ML, Henriksen JE, Ravn P, Glintborg D, Andersen M. Prevalence and possible
mechanisms of reactive hypoglycemia in polycystic ovary syndrome. Hum Reprod
2016;31:1105-1112.
21. Turner-McGrievy G, Davidson CR, Billings DL. Dietary intake, eating behaviors, and quality of
life in women with polycystic ovary syndrome who are trying to conceive. Hum Fertil (Camb )
2015;18:16-21.
22. Glintborg D, Mumm H, Hougaard DM, Ravn P, Andersen M. Smoking is associated with in-
creased adrenal responsiveness, decreased prolactin levels and a more adverse lipid profile in
650 white patients with polycystic ovary syndrome. Gynecol Endocrinol 2012;28:170-174.
23. Legro RS, Chen G, Kunselman AR, et al. Smoking in infertile women with polycystic ovary syn-
drome: baseline validation of self-report and effects on phenotype. Hum Reprod
2014;29:2680-2686.
24. Eleftheriadou M, Michala L, Stefanidis K, Iliadis I, Lykeridou A, Antsaklis A. Exercise and seden-
tary habits among adolescents with PCOS. J Pediatr Adolesc Gynecol 2012;25:172-174.
25. Conte F, Banting L, Teede HJ, Stepto NK. Mental health and physical activity in women with
polycystic ovary syndrome: a brief review. Sports Med 2015;45:497-504.
26. Di FG, Mansueto P, Longo RA, Rini G, Carmina E. Influence of sociocultural factors on the ovu-
latory status of polycystic ovary syndrome. Fertil Steril 2009;91:1853-1856.
This article is protected by copyright. All rights reserved.
27. Merkin SS, Azziz R, Seeman T, et al. Socioeconomic status and polycystic ovary syndrome. J
Womens Health (Larchmt ) 2011;20:413-419.
28. Huddleston HG, Cedars MI, Sohn SH, Giudice LC, Fujimoto VY. Racial and ethnic disparities in
reproductive endocrinology and infertility. Am J Obstet Gynecol 2010;202:413-419.
29. Glintborg D, Mumm H, Hougaard D, Ravn P, Andersen M. Ethnic differences in Rotterdam cri-
teria and metabolic risk factors in a multiethnic group of women with PCOS studied in Den-
mark. Clin Endocrinol (Oxf) 2010;73:732-738.
30. Glintborg D, Hermann A, Andersen M. Bone mineral density and vitamin D in PCOS and
hirsutism. Expert Rev Endocrinol Metabol. 2013;8:449-459.
31. Cui X, Gooch H, Petty A, McGrath JJ, Eyles D. Vitamin D and the brain: Genomic and non-
genomic actions. Mol Cell Endocrinol 2017;453:131-143.
32. Rubin KH, Glintborg D, Nybo M, Andersen M, Abrahamsen B. Fracture risk is decreased in
women with polycystic ovary syndrome: A register- and population-based cohort study. J Bone
Miner Res 2015;31:709-717.
33. Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M. Cardiovascular disease in a na-
tionwide population of Danish women with polycystic ovary syndrome. Cardiovasc Diabetol
2018;17:37.
34. Glintborg D, Andersen M. An update on the pathogenesis, inflammation, and metabolism in
hirsutism and polycystic ovary syndrome. Gynecol Endocrinol 2010;26:281-296.
35. Azziz R. The evaluation and management of hirsutism. Obstet Gynecol 2003;101:995-1007.
36. Pedersen CB. The Danish Civil Registration System. Scand J Public Health 2011;39:22-25.
37. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish
National Patient Registry: a review of content, data quality, and research potential. Clin
Epidemiol 2015;7:449-490.
38. Thygesen LC, Ersboll AK. When the entire population is the sample: strengths and limitations in
register-based epidemiology. Eur J Epidemiol 2014;29:551-558.
39. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J
Public Health 2011;39:103-105.
40. Jensen VM, Rasmussen AW. Danish Education Registers. Scand J Public Health 2011;39:91-94.
41. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic
comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-
383.

This article is protected by copyright. All rights reserved.
42. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-
CM and ICD-10 administrative data. Med Care 2005;43:1130-1139.
43. Goyal M, Dawood AS. Debates Regarding Lean Patients with Polycystic Ovary Syndrome: A
Narrative Review. J Hum Reprod Sci 2017;10:154-161.
44. Pelanis R, Mellembakken JR, Sundstrom-Poromaa I, et al. The prevalence of Type 2 diabetes is
not increased in normal-weight women with PCOS. Hum Reprod 2017;32:2279-2286.
45. Spalkowska M, Mrozinska S, Galuszka-Bednarczyk A, et al. The PCOS Patients differ in Lipid
Profile According to their Phenotypes. Exp Clin Endocrinol Diabetes 2018;126:437-444.
46. Merkin SS, Phy JL, Sites CK, Yang D. Environmental determinants of polycystic ovary syndrome.
Fertil Steril 2016;106:16-24.
47. Azziz R, Sanchez LA, Knochenhauer ES, et al. Androgen excess in women: experience with over
1000 consecutive patients. J Clin Endocrinol Metab 2004;89:453-462.
48. Escobar-Morreale HF, Carmina E, Dewailly D, et al. Epidemiology, diagnosis and management
of hirsutism: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome
Society. Hum Reprod Update 2012;18:146-170.
49. Azziz R, Carmina E, Dewailly D, et al. Positions statement: criteria for defining polycystic ovary
syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guide-
line. J Clin Endocrinol Metab 2006;91:4237-4245.
Supporting Information legends
Table S1: Area of origin and included countries.
Table S2: General characteristics and comparison of the PCOS OUH and PCOS Denmark cohort
Table S3: Conditional logistic regression analyses in PCOS Denmark cases and the respective control
for 5 different sensitivity analyses.
Table S4: PCOS OUH and FG-score at baseline and association between FG-score and socioeconomic
in PCOS OUH.
This article is protected by copyright. All rights reserved.
Legends tables and figures
Table 1. General characteristics of the study population at baseline and conditional logistic regres-
sion analyses in PCOS Denmark cases and the respective controls (N=55,475) and in PCOS OUH cases
and respective controls (N=3,251).
Table 2: Conditional logistics regression analyses stratified by area of origin.
Table 3. PCOS OUH and BMI at baseline and association between BMI and socioeconomic status in
PCOS OUH.
Figure 1. Possible associations between socioeconomic status (SES) and polycystic ovary syndrome
(PCOS).
Figure 2. Flowchart of the study. PCOS, polycystic ovary syndrome; NPR, Danish Patient Register;
OUH, Odense University Hospital. .
This article is protected by copyright. All rights reserved.
Table 1. General characteristics of the study population at baseline and conditional logistic regression analyses in PCOS Denmark cases and the re-
spective controls (N=55,475) and in PCOS OUH cases and respective controls (N=3,251)
PCOS Den-
mark
N=13,891
Control
N=41,584
PCOS Denmark vs. controls
N=55,475
PCOS OUH
N=814
Control
N=2,437
PCOS OUH vs. controls
N=3,251
N(%) N (%) OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
N (%) N (%) OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
Personal income
High tertile 3,467 (25) 14,996 (36) 1 1 152 (19) 928 (38) 1 1
Middle tertile 5,136 (37) 13,331 (32) 1.7 (1.6; 1.7) 1.6 (1.5; 1.7) 315 (39) 813 (33) 2.4 (1.9; 2.9) 2.2 (1.7; 2.7)
Low tertile 5,280 (38) 13,199 (32) 1.7 (1.6; 1.8) 1.5 (1.4; 1.6) 347 (43) 693 (28) 3.1 (2.5; 3.8) 2.2 (1.7; 2.9)
Unknown or missing 8 (0.1) 58 (0,1) 0.6 (0.3; 1.3) 0.4 (0.2; 0.9) 0 3 (0.1) Na Na
Occupational status
Affiliated to the labour market 9,699 (70) 33,038 (80) 1 1 526 (65) 1,991 (82) 1 1
Education 645 (5) 1,525 (4) 1.4 (1.3; 1.6) 1.2 (1.1; 1.4) 57 (7) 71 (3) 3.0 (2.1; 4.4) 2.4 (1.6; 3.5)
Unemployed or welfare payment 1,739 (13) 3,176 (7) 1.9 (1.8; 2.0) 1.5 (1.4; 1.6) 124 (15) 192 (8) 2.4 (1.9; 3.1) 1.7 (1.3; 2.2)
Early retirement 870 (6) 1,529 (4) 1.9 (1.8; 2.1) 1.8 (1.7; 2.0) 47 (6) 59 (2) 3.0 (2.0;4.5) 2.6 (1.7; 3.9)
Unknown or missing 938 (7) 2,316 (6) 1.4 (1.3; 1.5) 1.1 (1.1; 1.3) 60 (7) 124 (5) 1.8 (1.3; 2.5) 1.3 (0.9; 1.9)
Education
Master´s or doctoral education 691 (5) 2,885 (7) 1 1 29 (4) 179 (7) 1 1
Short tertiary education (incl. bachelor) 3,478 (25) 8,532 (21) 1.7 (1.6; 1.9) 1.5 (1.4; 1.7) 181 (23) 535 (22) 2.1 (1.4; 3.2) 1.8 (1.2; 2.8)
Vocational education 4,355 (31) 15,005 (36) 1.2 (1.1; 1.3) 1.0 (0.9; 1.1) 262 (32) 837 (34) 1.9 (1.3; 3.0) 1.5 (1.0; 2.3)
Upper secondary school 1,468 (11) 4,324 (10) 1.4 (1.3; 1.6) 1.0 (0.9; 1.2) 103 (13) 275 (11) 2.3 (1.5; 3.6) 1.4 (0.9; 2.2)
Basic (primary school) 3,461 (25) 9,366 (23) 1.5 (1.4; 1.7) 1.0 (0.9;1.1) 218 (27) 535 (22) 2.5 (1.6; 3.8) 1.4 (0.9; 2.2)
Unknown or missing 438 (3) 1,472 (4) 1.2 (1.1; 1.4) 0.7 (0.6; 0.8) 21 (3) 76 (3) 1.7 (0.9;3.2) 0.8 (0.4; 1.5)
Ethnicity
Danish 11,604 (84) 36,985 (89) 1 1 675 (83) 2,173 (89) 1 1
Immigrants 2,094 (15) 4,197 (10) 1.6 (1.5; 1.7) 1.0 (0.9; 1.1) 129 (16) 239 (10) 1.7 (1.4; 2.2) 1.0 (0.6; 1.6)
Descendants 162 (1) 325 (1) 1.6 (1.3; 1.9) 0.9 (0.7: 1.2) 10 (1) 21 (1) 1.5 (0.7; 3.2) 0.8 (0.3; 1.9)
Unknown or missing 31 (0.2) 77 (0.2) 1.3 (0.8; 2.0) 1.9 (1.1; 3.1) 0 2 (0.2) Na Na
Area of origin
Europe 12,152 (87) 38,901 (94) 1 1 705 (87) 2,278 (93) 1 1
Middle east 1,112 (8) 1,039 (3) 3.4 (3.1; 3.7) 3.2 (2.8; 3.7) 75 (9) 62 (3) 3.9 (2.8; 5.5) 3.3 (1.9; 5.7)
Other (and unknown or missing) 627 (5) 1,644 (4) 1.2 (1.1; 1.3) 1.2 (1.1; 1.4) 34 (4) 97 (4) 1.1 (0.8; 1.7) 1.0 ( 0.6; 1.8)
Comorbidity
Charlson = 0 12,595 (91) 39,363 (95) 1 - 748 (92) 2,319 (95) 1 -
Charlson ≥ 1 1,296 (9) 2,221 (5) 1.8 (1.7; 2.0) - 66 (8) 118 (5) 1.7 (1.3; 2.3) - aMutually adjusted for education, occupational status, personal income, ethnicity and area of origin
PCOS; polycystic ovary syndrome; PCOS OUH; PCOS Odense University Hospital; OR, odds ratio; CI, confidence interval.
This article is protected by copyright. All rights reserved.
Table 2: Conditional logistics regression analyses stratified by area of origin
Cases from Europe and respective controls Cases from Middle East and respective controls
PCOS Denmark vs. controls
N=48,529
PCOS OUH vs. controls
N= 2,815
PCOS Denmark vs. controls
N=4,443
PCOS OUH vs. controls
N=300
OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
Personal income
High tertile 1 1 1 1 1 1 1 1
Middle tertile 1.6 (1.6; 1.7) 1.7 (1.6; 1.7) 2.3 (1.9; 2.9) 2.2 (1.8; 2.8) 2.7 (2.1; 3.4) 1.6 (1.2; 2.0) 3.0 (1.2; 7.7) 1.8 (0.6; 5.4)
Low tertile 1.5 (1.4; 1.6) 1.5 (1.4; 1.6) 2.6 (2.1; 3.2) 2.1 (1.7; 2.7) 5.6 (4.6; 6.9) 1.6 (1.2; 2.0) 7.6 (3.0; 19.2) 1.9 (0.6; 6.5)
Unknown or missing 0.1 (0.0; 0.6) 0.2 (0.0; 1.6) Na Na Na Na Na Na
Occupational status
Affiliated to the labour
market 1 1 1 1 1 1 1 1
Education 1.3 (1.2; 1.5) 1.2 (1.1; 1.4) 2.8 (1.9; 4.1) 2.2 (1.4; 3.4) 2.9 (2.9; 4.0) 2.1 (1.5; 3.1) 2.9 (0.8; 10.2) 1.4 (0.3; 5.6)
Unemployed or welfare
payment 1.4 (1.3; 1.5) 1.4 (1.3; 1.5) 2.0 (1.6; 2.6) 1.7 (1.3; 2.2) 9.8 (8.1; 11.9) 7.1 (5.7; 8.7) 7.9 (4.0; 15.6) 5.4 (2.3; 12.4)
Early retirement 1.8 (1.7; 2.0) 1.8 (1.6; 2.0) 2.7 (1.8; 4.1) 2.5 (1.6; 3.9) 4.2 (3.1; 5.8) 2.6 (1.9; 3.7) 7.3 (1.7; 31.7) 4.3 (1.0; 19.0)
Unknown or missing 0.8 (0.7; 0.9) 0.9 (0.8; 0.9) 1.0 (0.7; 1.5) 0.9 (0.6; 1.5) 10.2 (8.3; 12.6) 6.8 (5.3; 8.7) 10.0 (4.5; 22.9) 6.1 (2.0; 18.5)
Education
Master´s or doctoral educa-
tion 1 1 1 1 1 1 1 1
Short tertiary education
(incl. bachelor) 1.7 (1.6; 1.9) 1.5 (1.4; 1.7) 2.1 (1.3; 3.3) 1.9 (1.2; 3.0) 1.6 (1.0; 2.4) 1.3 (0.9; 2.1) 1.6 (0.3; 8.4) 0.7 (0.1; 4.8)
Vocational education 1.2 (1.1; 1.4) 1.0 (0.9; 1.1) 2.0 (1.3; 3.2) 1.6 (1.0; 2.6) 1.4 (0.9; 2.1) 1.0 (0.7; 1.6) 1.4 (0.3; 7.4) 0.6 (0.1; 3.4)
Upper secondary school 1.3 (1.2; 1.5) 1.0 (0.9; 1.1) 2.4 (1.5; 3.8) 1.5 (0.9; 2.6) 3.4 (2.2; 5.2) 1.8 (1.1; 2.8) 3.4 (0.6; 19.2) 1.2 (0.2; 8.8)
Basic (primary school) 1.4 (1.3; 1.5) 1.0 (0.9; 1.1) 2.3 (1.5; 3.7) 1.4 (0.9; 2.3) 4.9 (3.3; 7.2) 2.3 (1.5; 3.6) 5.6 (1.2; 27.5) 1.4 (0.2; 9.6)
Unknown or missing 0.5 (0.4; 0.6) 0.4 (0.3; 0.5) 0.5 (0.2; 1.2) 0.3 (0.1; 0.9) 12.4 (7.9; 19.5) 5.3 (3.1; 9.0) 17.1 (3.0; 96.8) 4.4 (0.4; 43.5)
Comorbidity
Charlson = 0 1 - 1 - 1 - 1 -
Charlson ≥ 1 1.8 (1.7; 1.9) - 1.7 (1.3; 2.4) - 2.2 (1.7; 2.8) - 2.4 (1.1; 5.5) - aMutually adjusted for education, occupational status, and personal income
PCOS; polycystic ovary syndrome; PCOS OUH; PCOS Odense University Hospital; OR, odds ratio; CI, confidence interval.
This article is protected by copyright. All rights reserved.
Table 3. PCOS OUH and BMI at baseline and association between BMI and socioeconomic sta-
tus in PCOS OUH
BMI<25 kg/m2
N=257
BMI≥25 kg/m2
N=502
BMI ≥25 kg/m2 versus BMI<25
kg/m2 (reference)
N (%) N (%) OR (CI 95%)
Unadjusted
OR (CI 95%)
Adjusteda
Age, median (Q1;Q3) 33 (28; 37) 33 (29; 38) 1.0 (1.0; 1.0) 1.0 (1.0; 1.0)
Personal income
High tertile 57 (22) 90 (18) 1 1
Middle tertile 102 (40) 196 (39) 1.2 (0.8; 1.8) 1.0 (0.6; 1.5)
Low tertile 98 (38) 216 (43) 1.4 (0.9; 2.1) 1.0 (0.6; 1.6)
Occupational status
Affiliated to the labour market 186 (72) 310 (62) 1 1
Education 20 (8) 29 (6) 0.9 (0.5; 1.6) 1.1 (0.6; 2.2)
Unemployed or welfare payment 27 (11) 86 (17) 1.9 (1.2; 3.1) 1.7 (1.0; 2.9)
Early retirement 8 (3) 35 (7) 2.6 (1.2; 5.8) 1.9 (0.8; 4.3)
Unknown or missing 16 (6) 42 (8) 1.6 (0.9; 2.9) 1.5 (0.7; 3.1)
Education
Master´s or doctoral education 18 (7) 7 (1) 1 1
Short tertiary education (incl. bach-
elor) 63 (25) 109 (22) 4.4 (1.8; 11.2) 4.6 (1.8; 11.8)
Vocational education 76 (30) 169 (34) 5.7 (2.3; 14.3) 5.4 (2.1; 13.8)
Upper secondary school 48 (19) 46 (9) 2.5 (0.9; 6.4) 2.2 (0.8; 6.1)
Basic (primary school) 49 (19) 158 (31) 8.3 (3.2; 21.0) 7.0 (2.7; 18.4)
Unknown or missing 3 (1) 13 (3) 11.1 (2.4; 51.4) 10.2 (2.0; 51.8)
Ethnicity
Danish 219 (85) 417 (83) 1 1
Immigrants 34 (13) 81 (16) 1.3 (0.8; 1.9) 0.9 (0.4; 1.8)
Descendants 4 (2) 4 (1) 0.5 (0.1; 2.1) 0.3 (0.1; 1.5)
Area of origin
Europe 228 (85) 436 (87) 1 1
Middle east 17 (7) 50 (10) 1.5 (0.9; 2.7) 1,3 (0.5; 3.4)
Other (and unknown or missing) 12 (5) 16 (3) 0.7 (0.3; 1.5) 0.6 (0.2; 1.8)
Comorbidity
Charlson = 0 246 (96) 453 (90) 1 -
Charlson ≥ 1 11 (4) 49 (10) 2.4 (1.6; 2.1) aMutually adjusted for age, education, occupational status, personal income, ethnicity and area of origin
PCOS OUH; polycystic ovary syndrome Odense University Hospital; BMI, body mass index; Q,
quartile; OR, odds ratio; CI, confidence interval.
This article is protected by copyright. All rights reserved.
Figure 1. Possible associations between SES and PCOS

This article is protected by copyright. All rights reserved.
Figure 2. Flowchart of the study