social autopsies of maternal deaths in selected areas of ... · pdf filesocial autopsies of...
TRANSCRIPT

Social Autopsies of Maternal Deaths in Select Areas of Gujarat A Report by Jan Swasthya Abhiyan, Gujarat and CommonHealth
August 21, 2014

ACKNOWLEDGEMENTS
Our salutations to the women who lost their lives in child birth – may we all learn from their
sacrifice. Thanks to the families who spoke to us about their trials, despite their loss and grief.
Inputs provided by:
ANANDI, Dahod, Panchmahals – Pradeepa Dube, Rita Parmar, Urmila Baria
Tribhuvandas Foundation, Anand – Neha
SEWA Rural, Jhagadiya – Shobha Shah, Ranjanben
CHETNA RRC, Ahmedabad – Smita Bajpai, Arpita Suthar
Report compiled by:
Sunanda Ganju, Renu Khanna, Mahima Taparia, Pallavi Saha (SAHAJ), Vadodara
Case stories translated by – Mansi Shah, Parul Mistry and Seema Purohit
Report reviewed by:
Neeta Hardikar - ANANDI
Smita Bajpai - CHETNA RRC
Pankaj Shah, Shobha Shah - SEWA Rural
Gayatri Giri - CommonHealth
Alka Barua - CommonHealth
Dr. Lata Shah
Guidance from Subha Sri B and Sundari Ravindran (CommonHealth) are warmly acknowledged.
This report is a subset of a larger report cited as follows:
Subha Sri, B., & Khanna, R. (2014). Dead Women Talking - Learning from women’s experiences: A civil society report
on maternal deaths in India. CommonHealth and Jan Swasthya Abhiyan, 2014.

Contents ACKNOWLEDGEMENTS ....................................................................................................................... 2
1. Introduction ................................................................................................................................ 4
2. Objectives.................................................................................................................................... 7
3. Methodology ............................................................................................................................... 7
Limitations....................................................................................................................................... 9
4. Findings ..................................................................................................................................... 10
4.1 Profile of the women who died .............................................................................................. 11
4.2 Details of Deaths ............................................................................................................... 12
5. Issues emerging ............................................................................................................................. 15
5.1 Vulnerability of women – high risk assessment? .................................................................... 15
5.2 Poor quality of care in community based services - Absent or inadequate antenatal care ... 16
5.3. Poor quality of care – Absence of Post Partum Care ............................................................. 19
5.4 Referrals and Transport .......................................................................................................... 22
5.5 Out of Pocket Expenses........................................................................................................... 25
5.6 Lack of support/ facilities for arranging Blood ........................................................................ 27
5.7 Role of Public Health Facilities ................................................................................................ 28
6. Conclusion and Recommendations........................................................................................... 30
Annexure 1 Compilation of 46 Maternal Deaths in Gujarat
Annexure 2 Profile Tables of Women who died
Annexure 3 Stories of some women who died – English and Gujarati

1. Introduction
India has been reporting a steady decline in the country's maternal mortality ratio (MMR)
over the last few years. According to the latest reports, the MMR has fallen from 254 per 1,
00,000 live births in 2004-06 to 212 in 2007-09 to the latest figures of 178 per 1, 00,000 live
births in 2010-12 (1). However, this is far behind the Millennium Development Goal (MDG) 5
target of 109 per 1, 00,000 live births by 2015. It is now fairly certain that India will fail to
meet MDG 5.
Since the last decade, and especially since the launch of the National Rural Health Mission
(NRHM) in 2005, the Government of India has put in significant efforts to improve the
maternal health situation in the country. The primary focus of these initiatives has been to
promote institutional deliveries. The Janani Suraksha Yojana that provides conditional cash
entitlement to women to deliver in health facilities, and the more recent Janani Shishu
Suraksha Karyakram, are programmes to this end. In addition, the NRHM has also put in
significant efforts to strengthen health systems. However, civil society networks like
CommonHealth and Jan Swasthya Abhiyan have been expressing concern over this exclusive
push for institutional births and have suggested that the maternal health policy should
move away from the paradigm of institutional deliveries to that of safe deliveries.
While maternal health is much more than maternal deaths, maternal mortality ratio (MMR)
is well accepted as an indicator of a country’s maternal health status. In addition to
calculating aggregated MMR figures, several efforts have been made in the last few years to
analyse causes and contributors behind individual maternal deaths and use learning from
this exercise to improve health systems. The World Health Organization has published
guidelines for verbal autopsy of maternal deaths and this has been used in several countries
across the globe.
1 Registrar General of India, Ministry of Home Affairs (SRS Estimates 2013)

The GOI efforts on institutionalizing Maternal Death Reviews (MDR) have faced significant
challenges. By the government’s own admission (2) , as of March 2012, only 18% of all
expected maternal deaths were being reported and of these, only 2/3rd were being
reviewed by the district level committee for MDR. Also, this exercise was largely restricted
to finding a medical cause for death rather than identifying gaps in the health system and
instituting corrective action, the original objective of the whole process.
In additional to the above, one of the major shortcomings of the GOI instituted MDR review
process is of non availability of information in public domain. This lack of transparency in the
process precludes any engagement from other stakeholders like civil society, academics,
and professional associations in the process and signals a major lack of accountability.
Gujarat is among the four states in India which are close to achieving the Millennium
Development Goal 5. The Maternal Mortality Ratio is estimated at 122 per 100,000 live
births (SRS 2013) which has decreased by 26 points from 148 in 2007-09. However,
improvement in the nutritional status of women continues to be a challenge with every
second adolescent and more than half of the women in reproductive age group suffering
from anaemia. Pregnancy anaemia is almost universal (3).
Besides implementation of national programmes such as the National Rural Health Mission
and schemes such as the Janani Shishu Suraksha Yojana and Janani Suraksha Yojana,
others like Chiranjeevi Yojna, Kasturba Poshan Sahay Yojana, Indira Gandhi Matrutva Sahay
Jojana, Balsakha Yojana, 108 Free Ambulance, etc are some key interventions to bring
about an improvement in the health status of women and children in the state. These
efforts are welcome and indicative of the state’s attention for maternal and infant mortality
reduction. However, translating these efforts in to action has given rise to several concerns.
Studies point out that coordination among different maternal health interventions at
different levels is a weakness in Gujarat and point to a need for an improvement in capacity
to implement maternal health policy (4). Inequities persist in utilisation of maternal health
2 Maternal Death Review – Country Perspective, presentation by Dr Manisha Malhotra, Dy Commissioner,
Maternal Health, MoHFW, WHO multi-country workshop, Bangkok, Sep 2012 3 District Level Household Survey on Reproductive and Child Health, 2002- 2004
4 Sanneving, Linda, Asli Kulane, Aditi Iyer and Bengt Ahgren. Health system capacity: maternal health policy
implementation in the state of Gujarat, India. Global Health Action 2013, 6: 19629 http://dx.doi.org/10.3402/gha.v6i0.19629

care services – Saxena et al analysed DLHS data and found that three ANC visits, institutional
deliveries and use of modern contraceptives were significantly associated with caste group,
education and wealth. Being poor irrespective of caste group and place of residence is a
single most important factor in lower utilisation of maternal health care services (5).
As per April 2011-March 2012 data (6), maternal death reviews have been done and used for
strengthening the system. Out of 14,14,000 pregnancies per year, 12,86,000 deliveries occur
and an estimated 1900 maternal deaths per year (5-6 maternal deaths per day) and 38,500
Neonatal deaths (106 neonatal deaths every day) take place every year. According to the
same report, all 26 District Collectors and CDHOs are reviewing all the maternal deaths. This
has resulted in series of corrective actions to avert maternal deaths. The presentation states
that the following are being done:
Special 4 wheel drive vehicles launched to reach out to geographically difficult
terrains (12 vehicles in five districts).
Inter-Facility Transfer (IFT) services launched to address referral services from one
hospital to another further reducing transportation delays.
Essential drugs required for delivery and management of its complications made
available in facilities conducting delivery
Districts were sensitized and directed to implement use of partograph.
Technical Series for capacity building initiated on Acute Management of Third Stage
of Labor (AMTSL), Use of Partograph and Use of Magnesium Sulphate.
Pool of 30 MDR resource persons created at State level.
Newer approaches to help to understand why women die: Confidential Enquiries into
Maternal Deaths to be piloted
In spite of these efforts by the government, these interventions are not being widely
publicized and in many districts, community leaders are unaware of these. Further, the
detailed plan for each district to reduce referrals and upgrade health facilities does not
appear to have been shared with civil society organizations till date.
5 Saxena, Deepak, Ruchi Vangani, Dileep V. Mavalankar, and Sarah Thomsen. Inequity in maternal health care
service utilisation in Gujarat: analysis of district-level health survey data. Global Health Action 2013, 6:19652, http://dx.doi.org/10.3402/gha.v6i0.19652 6 Power Point Presentation titled Maternal Death Review – As a tool for System Strengthening-source
www.gujhealth.gov.by Dr N.B Dholakia, Additional Director (FW), Department of Health and Family Welfare

Civil society organizations like SEWA Rural, CHETNA Regional Resource Centre and SAHAJ in
collaboration with ANANDI and Tribhuvandas Foundation (TF) have been doing maternal
death reviews in their own work areas. This report presents a composite picture of maternal
deaths in Gujarat through the civil society lens. Through the present report, Jan Swasthya
Abhiyan seeks to understand the pattern of maternal deaths in different parts of the State
and analyse the gaps in the health system as well as the social determinants that cause
women to die during ante natal period, at the time of delivery and in the post natal period.
It is hoped that this report will complement the initiatives of the health system and lead to
corrective action – by different stakeholders - to prevent such deaths from occurring in the
future. While we hope that the health system will fill the gaps and strengthen maternal
health and emergency obstetric care services, members of Jan Swasthya Abhiyan will also
intensify efforts to enable community action for maternal health.
2. Objectives
1. To determine the pathways leading to maternal death and identifying the health
system and social factors contributing to these deaths.
2. To suggest ways to prevent such maternal deaths in the future.
3. Methodology
This report draws from an analysis of 46 maternal deaths identified and documented over a
period of two years (from January 2012 to December 2013). The deaths are from a
purposive and non representative sample from 11 districts across Gujarat.
Different methodologies were adopted by the three organizations (SAHAJ, CHETNA Regional
Resource Centre and SEWA Rural) involved in documenting the maternal deaths.
ANANDI team has been recording maternal deaths in the field area in a structured manner
since year 2007 with a view to create awareness in community and prevent maternal deaths
in the area. In 2012, SAHAJ in collaboration with ANANDI and Tribhuvandas Foundation (TF)
used the social autopsy tool developed by a group of maternal health activists and
academicians following a national meeting in June 2012 where a framework was developed

to look at maternal mortality in the Indian context (For a more detailed report on the Dead
Women Talking Meeting 2012, refer to www.commonhealth.in). The social autopsy tool was
designed to capture health system gaps, social determinants and human rights violations
that contributed to the maternal death, in addition to identifying a probable medical cause
of death. The tool development process was iterative and the tool was modified based on
feedback from civil society groups' experience of documenting maternal deaths and use of
the tool on the ground.
All deaths of women in the 15-49 years age group were reported by dairy cooperative
volunteers /field level workers in TF and Devgadh Mahila Sangathan women in the field area
of ANANDI. These were then verified by the trained staff of the two organizations to
establish whether they were maternal deaths or not. Following this, the families of the
deceased women – those established as maternal deaths - were contacted by members of
these organizations to do a social autopsy. Information was collected from multiple sources
like ASHA, ANM and Medical officer at PHC, private hospital doctors, and interviews with
the family (both the marital and natal family) were done by a team of two trained
investigators. At least two to three visits were made to complete the social autopsy
interview. Efforts were also made to contact other community members to understand
issues regarding health and other public services and social issues in the community.
The training of these investigators from ANANDI and TF who were staff of the organizations
working on maternal health was conducted by medical doctors (obstetricians), maternal
health activists and academicians. The training included sessions on epidemiology of
maternal deaths, technical inputs on common obstetric complications and their
management, rights based perspectives on looking at maternal deaths and skill based
training on actual use of the tool. Guidelines were adopted to ensure that the information is
captured as a story and does not get lost in the tool format which merely served as a guide
for the investigation.
During the interviews with the family, following a verbal, informed consent, details of the
death were collected using the social autopsy tool.
Similarly, SEWA Rural has been doing maternal death reviews since 2003-04 through a
surveillance system where arogya sakhi (ASHA) or link workers report a death and later

trained supervisory staff and social worker conducts the verbal autopsy making a minimum
of two visits. At present, the organization is using the tool developed by National Alliance
for Maternal Health and Human Rights (NAMHHR) after training by faculty from
CommonHealth. At SEWA Rural, gynaecologists also do facility level enquiries and all
maternal death cases are discussed with the team comprising of clinicians, public health
experts, ASHA, Dai and Anganwadi worker to arrive at possible causes and underlying
factors of a maternal death.
CHETNA as a Regional Resource Centre (RRC) initiated tracking of Maternal Health Services
in underserved areas in 2008 through partners in MNGO scheme. (Please refer
www.chetnaindia.org) In 2012, CHETNA RRC, inspired by a national initiative by
CommonHealth and NAMHHR and ARROW-Malaysia, initiated a process to review maternal
deaths. Action Plans were developed to track all deaths of women in the age group of 15-49
in their area, list their causes and identify maternal deaths. Ten NGOs tracked 229 villages
of 20 blocks in 9 districts of the state for deaths of women in the reproductive age group.
The total population of these villages is 391173. Details of about nine maternal deaths were
collected. These deaths were recorded from a total of 19069 live births, in seven of the
fourteen intervention districts.
For the purpose of producing a state report, available narratives of 46 deaths were compiled
district wise and analysed based on a pre developed framework to identify health system
gaps, social determinants and rights violations leading to the death (see Annexure 1 for a
compilation of the 46 Maternal deaths). During analysis, validation checks were carried out
on the data in the form of checks for internal consistency. The narratives were scrutinised by
two independent teams of Obstetricians to arrive at the probable medical cause of death.
Limitations
1. The purpose of the data analysed here is of advocacy for policy and programmes for
improvement in maternal health care services - it has not been designed as a research
study but as a working document for peer learning.
2. The health activists collected data to understand, analyse and advocate for health sector
accountability in recording, improving and preventing maternal deaths. Efforts have been
made to ensure that the rigour and ethical standards are maintained in the study such as

detailing of case stories and triangulating information from as many sources as possible,
on each case analysed here. The stories, compilation of tables and the report have been
subjected to a thorough scrutiny by four obstetricians and two public health doctors.
3. This documentation has been seen as a qualitative exercise to identify factors that
contribute to maternal deaths and understand those causes. The document captures
some of the maternal deaths in a given area; therefore this is not a report with statistical
information or maternal mortality ratios.
4. The details of these maternal deaths have been collected through interviews with
families who had maternal death in their family. In some cases, interviews with front line
health providers like the ANM and ASHA have contributed to the narrative. However, we
did not have access to the medical records of the women except where the family could
provide copies of some of these records. Thus the analysis draws largely from the
narrative of events provided by the family. Nevertheless this document provides
sufficient material to draw significant conclusions regarding contributors to these
women’s deaths.
4. Findings
Over a period of two years ( January 2012 to Dec 2013), a total of 46 maternal deaths were
documented in 15 blocks of 11 districts of Gujarat, The district wise distribution of these
deaths is depicted in Table 1. Four blocks are in the High Priority Blocks list of Government
of Gujarat.
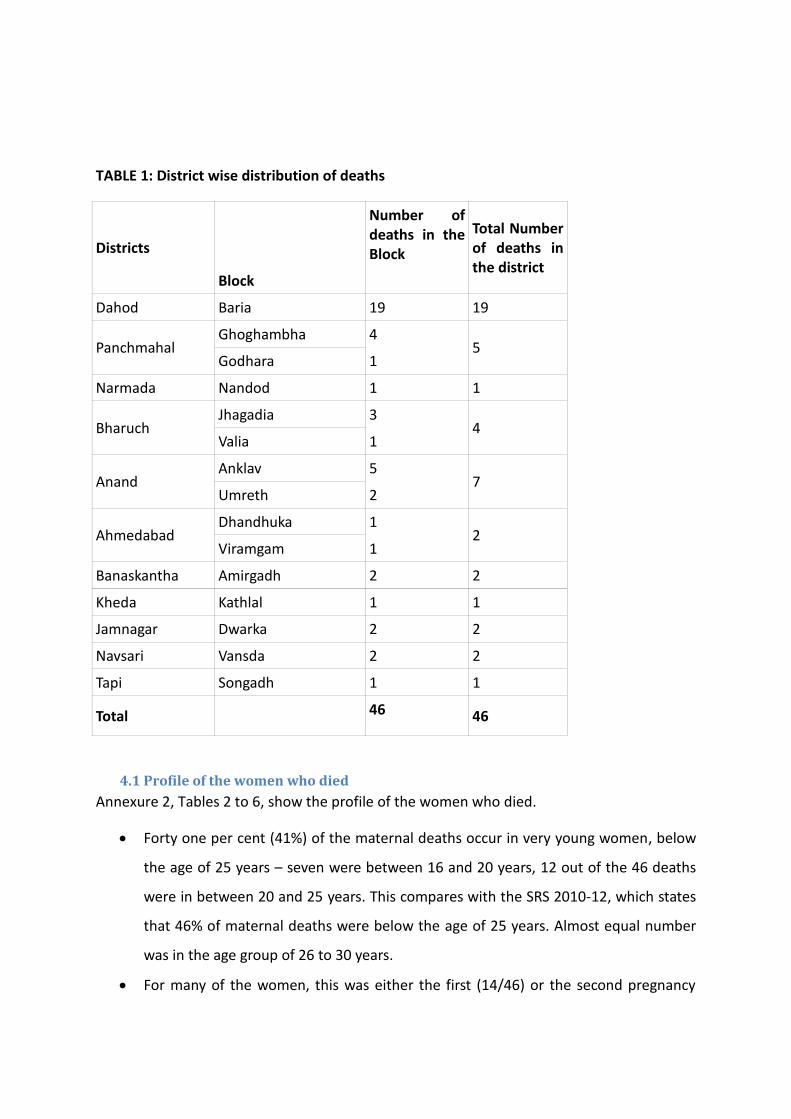
TABLE 1: District wise distribution of deaths
Districts
Block
Number of deaths in the Block
Total Number of deaths in the district
Dahod Baria 19 19
Panchmahal Ghoghambha 4
5 Godhara 1
Narmada Nandod 1 1
Bharuch Jhagadia 3
4 Valia 1
Anand Anklav 5
7 Umreth 2
Ahmedabad Dhandhuka 1
2 Viramgam 1
Banaskantha Amirgadh 2 2
Kheda Kathlal 1 1
Jamnagar Dwarka 2 2
Navsari Vansda 2 2
Tapi Songadh 1 1
Total 46 46
4.1 Profile of the women who died
Annexure 2, Tables 2 to 6, show the profile of the women who died.
Forty one per cent (41%) of the maternal deaths occur in very young women, below
the age of 25 years – seven were between 16 and 20 years, 12 out of the 46 deaths
were in between 20 and 25 years. This compares with the SRS 2010-12, which states
that 46% of maternal deaths were below the age of 25 years. Almost equal number
was in the age group of 26 to 30 years.
For many of the women, this was either the first (14/46) or the second pregnancy

(13/46). Eleven of the 46 women had between 4 and 8 pregnancies.
More than half – 59 %, i.e. 27 of the 46 deaths were of SC and ST women. This is a
higher proportion than the state’s SC-ST population of around 22 % (2011 Census).
Almost half of the women, who died – 46 % - were illiterate in comparison to 37%
female illiteracy in Gujarat, and majority of the rest – almost one third of the total
were educated only up to primary level. Only 8 of the 46 women who died had
secondary, graduate and vocational education.
Most of the women who died had multiple occupations/responsibilities – in addition
to domestic work, 25 of them were involved in either agricultural work or/and wage
labour. Nine of the women who died migrated for longer than 2-3 months without
safety of home and other basic amenities or any social security.
Three of the women who died were extension workers of the government – a
teacher, a Mid Day Meal in charge and an ASHA worker. One was an LIC agent.
4.2 Details of Deaths
Tables 7 to 11, give details of the Maternal Deaths.
Out of 46 women who died about one third had complications in previous pregnancy
and more than three fourths – 35 women- had complications in the current delivery.
Out of the 46 women, fourteen women (30%) died in the ante natal period, four
(8.7%) during the childbirth and 28 (60.8%) after delivery. Amongst the Post Natal
Deaths, 8 occurred within 24 hours, 3 within a week of the delivery and the rest (17)
between 8 to 42 days of delivery.
Fourteen maternal deaths – (30 %) - took place at home, 24 (52%) in institutions (10
in private and 14 in public institutions); eight deaths (17%) took place in transit. For
details of Place of Birth and Place of Death refer tables 9 and 10.
Table 11 in Annexure 2 shows that out of 46 maternal deaths, direct causes of
maternal deaths were seen in 28 cases (60.86) %) and indirect causes were
responsible for 15 (32.6 %) deaths. Cause could not be determined in 3 cases
(6.52%).
The most common cause of death was PPH (including Ante partum haemorrhage) in
12 (nearly 26 %), followed by Pre-eclampsia in 7 (15.2%), and Pulmonary embolism in

2 (4.34 %) of the women. There were 2 deaths due to sepsis and one death each due
to blood transfusion reaction and obstructed labour.
Among the indirect causes unrelated to pregnancy, anaemia in 4 (8.6%%) was the
commonest followed by 2 deaths each due to jaundice, sickle cell disease and
cardiovascular disease and one each due to malaria, tuberculosis, rabies, renal failure
and dengue.
The cause of death could not be ascertained in 3 (6.52 %) of the deaths.
The table below indicates that in 16 cases , more than one cause of death was
identified like anaemia was associated with 13/41 cases in both direct and indirect
causes of death followed by Cardiac failure (1/41) and PPH (1/41) and Septicaemia
(1/41) were also some of the additional causes of death.
4.2.1 Deaths in Transit
ANANDI
Sr. No. 5- Veena (name changed) died on the way to the referred hospital. She had a
caesarean during her previous delivery and this was her second pregnancy. She
received regular ANC at the Mamta Divas, however received no calcium tablets and
her Hb was not checked. During the 5th month, due to vomiting, she got her BP, Hb
checked at Dr. P’s clinic at Baria and her Hb was reported to be 12 grams. During the
7th month, Veena got labour pain, and was rushed to Dr. P’s clinic on a bike. The
doctor there diagnosed Intra Uterine Death from the sonography reports, and then
informed the family of the urgent need for arranging blood and performed a
Caesarean Section which lasted 6 hours. There was intra op bleeding and she needed
a hysterectomy. She was given two units of blood, which was arranged by the
woman’s husband from Dahod, however there was too much blood loss and post
operation she was referred to another private hospital at Godhara. An ambulance
was called by the doctor, however no referral papers were provided. Doctor informed
the family to arrange for 2 more bottles of blood and 2 bottles of plasma, for which
the husband’s elder brother rushed to Godhara around 5.30 pm. Around 7.30 pm,
on the way to Godhara, near Mendra Chaukdi, the elder brother reached the
ambulance with 2 bottles of blood, which was administered by the nurse to the

woman in the ambulance, however the woman had stopped breathing. She died in
transit, on the way from Dr. P’s clinic at Baria to a private hospital at Godhara.
Sr. No.6- She was married at 16, and this was her first pregnancy. She had only one
ANC and did not have a Mamta Card. Her height, weight, Hb, BP, abdomen was
checked at Dabhva PHC and Hb was reported to be 8 grams. She went into labour at
nine months and was at her natal home for the delivery. The family first called the
Dai and when the pain increased, they took her to a private hospital at Baria, where
she delivered a baby boy. She continued having pain in the legs and stomach post
delivery, and from there she was referred to the District Hospital as she needed
blood. However, the family did not take her to the referred hospital and she died on
the way back from the private hospital to her home. She was diagnosed to have died
due to anaemia in CCF (Congestive Cardiac Failure).
Sr. No. 9- Died on the way from Public Taluka Hospital to Medical College. There was
a delay in diagnosing and managing PPH. She was referred in a very critical condition,
had seizures in the ambulance and died.
Sr.No18- Died on the way from Dr. M’s clinic at Baria to Godhra, which is around 41
km. She was referred in a very critical condition. Lack of care during pregnancy also
worsened her situation; she was working till the ninth month.
SEWA RURAL
Sr. No 1- Died on the way from a Private Hospital to the referred hospital, there
seems to have been unnecessary blood transfusion at the first hospital, which led to
a reaction, and she died on the way to another hospital.
Sr.No.2- Died on the way from home to a local practitioner. She was initially
admitted in the NGO hospital and referred to Medical College, admitted there and
asked to buy medicines, however, the family came back home due to lack of money.
Reason of death was negligence and lack of PN care, and over reliance on local
practitioners.
Sr. No. 5- Died on the way. There was delay in seeking treatment and too many
referrals contributed to the delay, the 108 was late.

Thus we see, that in the 8 transit deaths, it is factors such as lack of Ante Natal care, lack of
Post Natal Care, delay in diagnosis, delay in treatment and referrals and gaps in the health
system that result in death of the woman. Only in two women’s stories it is evident that the
decisions of the family aggravated/ caused woman's death. (ANANDI-Case 6, SEWA Rural-
Case 2).
5. Issues emerging
5.1 Vulnerability of women – high risk assessment?
From the section on the Profile of the Women who died, it is seen that these were highly
vulnerable women on several counts. Many were primis at young age, with very low levels
of education. About 11 women had 4-9 pregnancies.
In addition to their domestic responsibilities, more than 70% of the women were engaged in
farming, as daily wagers and labourers. Some of them worked till the last month of their
pregnancy and this indicates that these women were extremely poor. Majority of them
belonged to scheduled tribes, scheduled caste or other socio economically backward castes,
social groups that have been historically deprived from the development process.
Majority (30 out of 46) of the women who died were very young, in the age group of 21-30
years. Early marriage is a major problem affecting the health of women. DLHS 3 Gujarat
showed that 22.4% of young women were married before they were 18 years, the legal age
of marriage. It is also known that women who have a pregnancy at an age less than 18 face
a high risk of morbidity and mortality. Despite this the narratives reveal that several young
women in the sample had not received any antenatal care at all during their pregnancy. For
example, Maina, a 20 year old adivasi woman was married at the age of 16 and was
pregnant with her first child – she had had only one antenatal visit at the PHC when her
haemoglobin was detected to be low (8 gms/dl), but she was given no iron tablets, no
antenatal card was made either. She later died after delivery, probably because of cardiac
failure due to anaemia (S No.6).
Yet another group of vulnerable women that were not covered by the health system were
migrant workers. At least nine out of 46 women of the sample who died were migrants.
Portability of services was an issue for these women. They were not covered by antenatal

services or ICDS services and when they died their deaths were not recorded as they did not
belong to anyone's “area”. Similarly, the cultural practice of women moving between their
marital and parental homes is not recognised. Portability of maternity services and
entitlements and universal access is an issue.
Vulnerability and resultant high risk pregnancy was also due to socio-cultural factors
perpetuated in the patriarchal society. In Babiben, Amirgarh, Banaskantha district’s case,
son preference was an overarching determinant of maternal death. Babiben was diagnosed
with heart ailment in her earlier pregnancy. She had three children - one boy and two
daughters earlier but had a desire to have two sons and so she went for fourth pregnancy
despite her family being aware of the risk. (Case 3, CHETNA - RRC)
Older women with history of multiple pregnancies (11 out of 46 women had 4 to 8
pregnancies) are a high risk group for complications both because of their age and
multiparity. This group too seemed to be getting left out of care. Urmila is one such woman
– a 32 year old migrant worker in cotton mills, she had a past history of tuberculosis that
had been treated. Of her three previous deliveries, the first one was at a construction site
where she worked and the next two were at home. In her fourth pregnancy, she had had
only one antenatal care visit at a PHC where only a tetanus toxoid injection was given and
she was handed ten tablets of iron folate. No haemoglobin or BP check up had been done.
Urmila subsequently developed severe breathlessness and after desperately seeking care at
seven different facilities over 5 days, her family gave up and took her back home where she
died (Case 4, ANANDI).
These vulnerability factors indicate that ‘high risk’ assessment on purely biomedical terms is
quite inadequate. The peripheral health workers – ASHAs, FHWs, and AWWs – need to be
systematically trained to do early identification of both biomedical high risk and social
vulnerability factors. The multiple dimensions of vulnerability – including the social
dimensions - need to be recognised by the peripheral health workers and need to be
factored into their birth preparedness plan, health care delivery and follow up plans.
5.2 Poor quality of care in community based services - Absent or inadequate antenatal
care

The World Health Organization recommends a minimum of four antenatal care visits for
women with low risk pregnancies. While antenatal care by itself cannot prevent maternal
deaths, it can help in very specific ways – in situations where anaemia continues to be highly
prevalent in pregnancy and contributes to a significant proportion of maternal deaths,
antenatal care can help in diagnosing and treating anaemia before childbirth. In addition,
antenatal care can help screen women who have certain risk factors and need closer
monitoring and care – like those with sickle cell anaemia, mal presentations, previous
caesarean section or previous obstructed labour. The antenatal care session can also serve
as a space where the woman and her family are provided information and counselling
regarding birth preparedness and emergency readiness. It can also serve to foster the trust
of the woman and her family in the public health system.
Availability and Quality of Ante natal Care
Under the National Rural Health Mission, a community based fixed day antenatal care
model has been implemented in the form of Village Health and Nutrition Day. However,
narratives from the family showed that many women either did not receive antenatal care,
or received care that was of very poor quality. Out of 46 women who died, 4 women (Case
9, 10, 22 ANANDI and one from CHETNA RRC) had not received any form of antenatal care
at all.
In many cases ANC is done as tokenism. As the cases below will illustrate, 23 out of 46
women who died, received very poor ANC. Out of 23 women, five had no Mamta Card and
one had falsified information noted in it while some family members even said that ASHA
never visited them (Case 8, ANANDI).
In one case in Dahod (Case 14, ANANDI), even TT was not given to the woman and in two
cases (Case 4 Urmilaben mentioned above, and Case 7, ANANDI) there was no Hb, BP or
weight measured and the woman was given 10 tablets of IFA when she should have been
given the full count of 100 tablets. In yet another case, there were no iron supplements
given at all (Case 17 ANANDI).
Out of 43 cases whose obstetric history was available, 18 were reported to be anaemic. The
fact that so many women were anaemic indicates that there were lapses in ante natal care
and such women were not given iron supplements/iron sucrose injections and were

subjected to high risk pregnancy, and high risk delivery and post delivery period. One
Meetaben, an adivasi woman from Devgadh Baria, Dahod district was diagnosed with
severe anaemia ( Hb 2 gm) in the 7th month of pregnancy which was not treated during her
early ante natal period. She went to a private hospital complaining of swelling and bleeding
and from there was referred to a Civil Hospital. From Civil Hospital, she was further referred
to a private hospital where she was refused admission and finally referred to another
private hospital where she underwent a caesarean section and 4 units of blood were given
but she died soon after that (Case 2, ANANDI). This clearly indicates how severe and
untreated anaemia can be fatal.
One of the other lacunae in the ante natal care is lack of information or counselling given to
women and their families about high risk symptoms or complications during pregnancy,
delivery and post natal period. Out of 46 women, narratives of 10 families indicate that they
lacked information about basic ante natal care. Even in Anand district which is reportedly
well equipped and developed the narratives revealed lack of information given to the
women and their families about complications during pregnancy and post natal period. In
another case in Anand (Case 2, TF) the woman and her family were not guided about the
treatment for TB that needed to be continued in the post natal period.
In Dahod and Panchmahal, the case stories specifically indicate that the women who died did not
receive any information about JSSK, JSY, Kasturba Poshan Sahay schemes (Case 20, 17 ANANDI).
Further, in two cases they lacked information about 108 or did not know how to call it to the village
(Case 6, 24, ANANDI). While access to ante natal care and birth preparedness are key steps in
managing high risk pregnancies; information, access and realisation of maternity entitlements in
form of financial support through the KPSY and free of cost health care services in form of cash,
food grain and support and assistance, are critical.
Portability of Services to ensure Continuum of Care
Due to cultural practice of moving to natal homes during pregnancy ASHA/ANMs lose track
of the women and their checkups and complications before they move out of the village.
Dahiben, aged 22, an adivasi woman, first time pregnant from Vansda, Navsari district
complained of pain and bleeding during pregnancy. She shifted to her natal place and
delivered a still born baby there. Later, she developed complications of disseminated

intravascular Coagulation preceded by Abruotio Placenta and finally died. (Case 8, CHETNA -
RRC)
The summary of the case stories points to how social determinants interact with the ante
natal conditions, especially for vulnerable women, to accentuate their risks for maternal
deaths and morbidities. The vulnerabilities of these women may be a reflection of multiple
social and systemic factors interplaying – however, by not making special provisions to
ensure that these women receive care, the health system adds to their vulnerability.
Quality of ante natal care needs to be improved. In addition to the standard ANC
parameters - haemoglobin, BP, Odema etc for which the understanding and skills of the
health care providers need to be enhanced - better history taking, assessing of social
vulnerability factors needs to be included. Rigorous monitoring of ANC is required – the
supervisors/medical officers need to ask FHWs and ASHAs about follow-up actions for each
high risk and vulnerable pregnant woman.
5.3. Poor quality of care – Absence of Post Partum Care
There seems to be at least some notional effort at providing antenatal care. But postpartum
care seems completely absent both at the levels of the facility and the community. It is well
known that most maternal deaths occur in the first week of the post partum period. Of our
sample of 46 deaths, 28 deaths took place in the post partum period. However, postpartum
care was found to be highly inadequate. Once the woman was discharged from a facility,
there seemed to be no system of providing any care to her.
Usha (name changed) from Anand district, was pregnant for the third time and was regular
in getting her ante natal checkups done. She also got her sonography done. In her previous
pregnancies, she suffered from hypertension and swelling. In her current pregnancy, she
was anaemic, while her BP was normal and weight was reported to be 31 kilograms. She had
loose motions during the seventh month, and there was presence of albumin in her urine.
During the 8th month, she delivered two twin baby girls at a hospital and was discharged
after two days in spite of a premature delivery. She had swelling post delivery and also had

difficulty in breathing; however she was not taken to the hospital. Ten days post delivery
her swelling persisted and she was breathless so was taken to S Hospital where she was
given blood and next day was referred to Karamsad Medical College, wherein she was kept
on oxygen for a few hours and then referred to SSG Hospital, Vadodara. She was taken to
Vadodara by 108 and reached SSG in about two hours, wherein she was declared dead by
the doctor within a few minutes. (Case 1, Tribhovandas Foundation)
Shanti (name changed) went to a private practitioner in Dahod district with breathlessness
and loss of foetal movements – she was diagnosed to have an intrauterine foetal death and
referred to the Civil Hospital. Since there was no doctor there, her family took her to two
different private hospitals before she was admitted in one and delivered a stillborn baby.
After she was discharged and sent home, she developed bleeding on the fifth day; an
ambulance (108) was called the next morning and she was carried the three fourths of a
kilometre on a bed sheet when she died.
These cases highlight that there is no continuity of care after deliveries in health facilities.
There is an absence of any form of post natal care in the villages after childbirth. The front
line workers are unable to recognize postnatal complications. These stories also reflect the
inefficiency and apathy of the government hospitals to give referrals even in such critical
conditions.
Recording of Maternal Deaths - Natal Homes or Marital Home?
As mentioned earlier, several women received partial ante natal care due to socio-cultural
practice of them moving to their natal home during pregnancy. Such mobility not only
affects the quality of care received during pregnancy but in case of death, it also has
implications on the recording of maternal death. There have been instances where the
officials declined to record death if the registration was done in another village.
Shanti (name changed) had conceived after four years of marriage and had been staying
with her parents during pregnancy as her in laws and husband did not treat her well. Shanti
went to Dr. M during 8th month of pregnancy when she experienced breathing problems
and pain in legs; however he confirmed everything to be normal. After a week, when Shanti

stopped feeling baby’s movement and had breathing problems, she was taken to the same
doctor at Baria, who confirmed the death of the baby in the mother’s womb. He asked the
woman’s family to transfer her to the closest government clinic and refused to deliver the
stillborn at his facility. At the government clinic/hospital, no doctor was present to attend to
her so they went to Godhra. The government hospital staff there refused to take her case.
Finally she got admitted in a private facility named Satyanarayan Hospital where she
delivered the still born. Five days after coming home from the hospital, the woman started
bleeding at night, and also complained about loss of appetite and breathlessness. The next
day her family members called an ambulance (108). To avail the service they had to take her
to the main road which was at a distance of 6 kilometres. They carried her in a bed sheet
but she died on her way to the ambulance. Because she was supposed to be a “married
woman” with her marital home in another area, she was not recognised as a resident of her
natal village, although she was registered in Mamta Diwas at the Aanganwadi Centre, the
health department refused to register this death under their PHC area. (Case 7, ANANDI)
Kantaben Rabari (name changed) from Anand district belonged to a pastoralist family and it
was her fourth pregnancy. She had registered at the Anganwadi at her in laws’ village and
had also been given TT here. During the ninth month of pregnancy she went to her natal
home, where she visited the Anganwadi and was informed by the nurse about ‘paleness in
her blood’. No other check up was done. On the 15/01/2013 at 4.00 am, she experienced
labour pains, and gave birth to a baby boy at home. She was assisted in her delivery by her
relatives. Post delivery there was delay in expulsion of the placenta, and there was profuse
bleeding. Around 9.00 am, 108 ambulance was called and she was taken to S Hospital at
Borsad (15 km away). She was admitted and given injections, but died within an hour. (Case
5, Tribhovandas Foundation)
In such cases, we observe a lack of follow up and care by the health functionaries, probably
because of the idea that ‘this woman does not belong in my area’. Poor quality of ante
natal check-ups, coupled with lack of follow up in cases where the women have migrated,
aggravate her vulnerability and inability to seek timely treatment.
The Medical Officers and the Block Health officers need to impress upon the FHWs and
ASHAs that any woman who is pregnant or post natal in their villages, are their

responsibility – they have to provide them all necessary services, keep the requisite records
and report on these cases, just as they would ‘women of their own areas’.
5.4 Referrals and Transport
Women have visited between two and seven facilities before succumbing to death. Around
40 women visited up to three facilities. Here is a story of an adivasi woman who went to
seven facilities over five days to finally die at her home.
Urmila (name changed) from Goghamba, a 32 year old adivasi woman, a migrant worker in
cotton mills was pregnant with her fourth baby. Her first delivery was on a construction site
and other two at home. She had a history of TB which was cured. She went to the PHC (on a
bike) with complaint of breathlessness and was referred from there to the Taluka Hospital
(went across the river 3 kms to the 108 pickup point and from there in 108) and from there
to the District Hospital by ambulance. The doctor at the District Hospital said that he would
not be present during the night and that she should be taken to a private hospital (we don’t
know his or someone else’s). So Urmila was taken home (by chhakda, bus and rickshaw) as
the family did not have money for treatment in a private hospital. By third day the family
was able to arrange for money so they took her to a private hospital in another town (by
bus) and from there to yet another. Here she was told that she had an intra uterine death
and was told to go to the medical college. The family arranged for a private ambulance and
went to the medical college. The next day the doctor in the medical college referred them
to a private hospital in the city. The family decided to just go back home. They went by bus
and chhakda. Urmila died that night at home after five days of being shunted around for
treatment. (Case 4 ANANDI)
Babbiben (name changed) a 27 year old tribal woman from Banaskantha, had a history of a
chest pain in her third pregnancy which subsided after the delivery. In her fourth pregnancy,
she died in the Civil Hospital after visiting six facilities. From the PHC she went to a Trust
Hospital, then to two private clinics, then to the Civil Hospital, from there to a private
nursing home, again to the Trust Hospital and to the Civil Hospital once again. From here
she was referred to Ahmedabad Civil Hospital. A District level Civil Hospital did not have the
life saving services to deal with non-obstetric causes of maternal mortality. Neither did it
have a system of accompanied transfers. (Case 3, CHETNA RRC).

Shanti a 26 year old adivasi woman from Baria (name changed), in her first pregnancy went
to four facilities. Her ANC was done during the Mamta Diwas, BP was normal, Hb was not
done. She was given 10 IFA tablets. She complained of breathlessness during her pregnancy,
went to a private doctor and was told that all was normal. She continued to feel breathless
and felt absence of foetal movements and went to the private doctor once again. He
diagnosed intra uterine death and referred her to the Civil Hospital where there was no
doctor present. So she was taken to a private hospital in the district headquarter where she
was refused treatment. She went to yet another private doctor who delivered a still born
baby. On day 5 after the delivery, she started bleeding heavily. 108 was called in the
morning. She died while being carried on a bed sheet to the ambulance 6 km away. (Case 7
ANANDI).
These families find negotiating repeated referrals and transfers very difficult and ultimately
decide to take the woman back home. Maina from Dahod district got married at the age of
16 and it was her first pregnancy. When the girl complained of pain at 7.00 pm in the
evening, her mother called the dai who examined her and confirmed everything to be
alright. Since the dai was tired, she went to sleep at the girl’s house. After some time, when
the pain became unbearable, the dai advised the family to take the girl to the hospital. Due
to lack of knowledge about calling/ directing 108 ambulance to their location, they couldn’t
avail the service. They finally left for the facility at 5.00 am in a private rickshaw. She was
taken to Dr. M’s Clinic at Bariya. As per ANANDI field staff the reason for concern was ‘green
water’. When the doctor checked her eyes and tongue, he sent her to the lab first for the
investigation and then she was transferred to the delivery room where she gave birth. Post-
delivery the mother kept complaining about pain in stomach and feet. Doctor referred her
to Godhra district hospital for blood. However, the woman’s family members found the
process of transfer difficult and decided to take her back to the village in the same rickshaw
at 10.00 pm. On her way to the village, the girl had stopped talking and was believed to be
dead before reaching home. (Case 6, ANANDI).
Many of the stories indicate that women and their families prefer to go to the private
doctors rather than to public facilities. From the private, even from Chiranjivi doctors, they
are referred to public and they choose once again to go private facilities or simply to go

home (Case 6 CHETNA RRC, ANANDI). There have been situations when doctors have not
been present in the public hospitals (Case 5 SEWA Rural, Cases 1, 7 and 8 ANANDI).
What is astonishing is how the Medical College doctors as well as the Civil Hospitals in the
districts are sending women away to private hospitals. (Case7 and Case 13, ANANDI).
Another noteworthy issue is the lack of coordination between health care facilities – both
the referring facility and the one where the woman is being referred. (Case 3, Case 12, Case
18 CHETNA RRC). There is absence of any referral protocols, documentation or even
accompanied referrals.
We did find a couple of positive case studies of accompanied referral. Veena (name
changed) BA B.Ed, in her second pregnancy went into pre term labour at 7 months. Intra
Uterine Death was diagnosed in a private hospital. She was taken for a Caesarian Section
which lasted 6 hours. There was intra operative bleeding, and she needed a hysterectomy.
She was given 2 units blood, and referred to another private hospital in District HQ with
ambulance, nurse and blood (2 units more + 2 plasma given in the ambulance). However she
died in transit. (Case 5 ANANDI). Kamla (case study is in the next section) was also
accompanied by a doctor and nurse in 108, but to no avail – the lapses in the 108 service
were too many.
Transport
Analysis of these case studies points also to the fact that although 108 has helped to
increase access to health services for many women; many especially vulnerable women in
remote areas continue to be plagued by lack of physical access and transport facilities.
Denial and availability of transport at affordable rate and full reimbursement of expense
incurred for hospitalisation as well as return journey home remains a common complaint.
Case 2 (ANANDI) had severe anaemia in ante natal period, which was not treated. She went
with swelling to a private hospital from where she was referred to the Civil Hospital. Here
she was induced labour and referred to the District Hospital due to bleeding. Strangely the
family was not provided with ambulance, vehicle or assistance to deal with the emergency. .
She went to a private hospital in a private vehicle where she was refused admission. So she
went to another private hospital in the District Headquarter where a CS was done. She was

given 4 units of blood but died soon after. Case 2 (ANANDI) states that ‘Ambulance not
provided, 108 refused to come.
‘There are many situations where the 108 has come late (Case 5 SEWA Rural, Case 8
ANANDI). ‘A woman who went into labour at term, called 108, had to wait 2 hours for it. She
was carried to it in a bed sheet for 3/4th kilometre till the main road, where it stood. She was
taken to the Taluka Hospital where she was assigned a bed and given an injection by the
nurse. The doctor was not present there, and the woman was kept waiting. She couldn’t
survive that long and died unattended. (Case 8 ANANDI)
Kamla’s case from Narmada District (name changed) is the epitome of how things can go
wrong for a woman due to 108. ‘She was a 24 year old graduate. She had a normal delivery
at home before the dai could arrive. There was profuse bleeding. 108 was busy so another
108 had to come from 70 km away and came after 1 ½ hrs. She was unconscious by then.
108 took her to the CHC, no doctor or nurse was present there. So she was taken to a
private nursing home where she was admitted and given 5 units blood. Feeling
breathlessness on Day 2, she was referred to another private hospital, where she was given
1 more unit of blood. But her condition worsened. So she was referred to the medical
college after 11 hours, in 108, but the vehicle broke down in between. Another 108 was
called and she was taken to the medical college (the doctor and nurse accompanied her),
but she died before reaching there’. (Case 5 SEWA Rural). In the area of Anand where the
maternal deaths were documented, it was observed that 108 have not been used often.
There appears to be lack of adequate information about this facility and pregnant women in
situations of emergency have taken auto rickshaws.
5.5 Out of Pocket Expenses.
Despite the Chiranjivi Yojana and the JSSK, the guarantee of free and cashless service for
childbirth is a hollow promise. Where ever the question on Out of Pocket Expenditure has
been asked, the response from the families has been ‘yes’. Expenditures have ranged from a
low of Rs. 990 to over Rs. 20,000, with a number of families having incurred between Rs.
17,000 and Rs. 19,000. In Anand district, four out of the seven women who died after
seeking services at multiple facilities, incurred Rs. 20,300, 19,000, 7,000, and 17,000 (Cases

1 to 4 Tribhuvandas Foundation). TF Case 3’s story states that she was a 24 year old woman
with anaemia in previous pregnancy as well as the current one. Lack of information on high
risk symptoms like PPH, no Mamta Card, no blood facility in government hospital due to
which she was referred to a private hospital where they could not pay for the blood (she
was given 4 units of blood). She was discharged early, after 12 hours of delivery from the
hospital, no post natal care given by the system. So they brought her back home. She died
at home.
Stories of denial of services because of lack of money with the family are not uncommon.
Cases 2 and 11 ANANDI are two such stories. Meeta (named changed) an agricultural,
migrant labourer, whose both earlier children had died in their infancy, was severely
malnourished and anaemic (other symptoms included night blindness and Hb 2 gms %). Her
severe anaemia in the ante natal period was not treated. She went with swelling to a
private hospital and from there was referred to a Civil (sub district hospital) Hospital. Labour
was induced in the Civil Hospital. And she was referred to District Hospital due to bleeding,
but was not given any vehicle. They took a private vehicle to a private hospital where she
was refused admission. From there they went to another private hospital in the District
Head quarter where a CS was done – 4 units of blood was given, but she died soon after.
Her family reported that they spent Rs. 19,200 before she died - she was ‘severely anaemic,
yet was not provided blood during initial check up due to lack of money’. (Case 2 ANANDI).
Sheelaben’s (name changed) first three babies died, in the current pregnancy she had fever
in the 5th month, and pain in the 7th month. She visited three facilities – there was an
incorrect diagnosis by the first doctor (breech position was not diagnosed), and then she
was referred in an emergency. Dr. XYZ’s Hospital did not admit her till both money and
blood were arranged. Responsibility of arranging for the blood as always was put on the
family. (Case 11 ANANDI).
It is not only at the private practitioners that families have to incur out of pocket
expenditures. Even at government medical college hospitals, women have to spend on child
birth. The story of Case 2 SEWA Rural goes like this: She was admitted in the NGO hospital
with severe anaemia and dengue. With no improvement even after 10 days, she was
referred to the medical college (ambulance), where she was admitted and asked to buy

medicines for Rs 11000 from outside. The family came back home since they had no money.
She had a pre term delivery the next day. There was fever and swelling after that. She was
shown to a local practitioner on Day 7 after delivery. He gave her IV Fluids and an injection.
Her condition worsened 4 days later and she died while being taken to the local practitioner
on a bike.
Cashless services have to be provided to pregnant women. Otherwise, reimbursement of all
expenses has to be made part of the system. Grievance redressal mechanism need to be
clearly communicated to families so that they have a forum to complain and get their
complaints satisfactorily addressed.
5.6 Lack of support for arranging Blood
One way of reducing maternal mortality is by improving the availability, accessibility, quality
and use of services for the treatment of complications that arise during pregnancy and
childbirth, services such as EmOC (Emergency Obstetric Care). Arranging for blood in
emergency situations was one of the areas that families were held responsible for. Blood
transfusion can be a life saving medical procedure in certain medical emergencies like
haemorrhage and shock. Also, women with severe anaemia in late pregnancy may need
blood transfusion. In the narratives, it was seen that in situations of emergency, blood
transfusion was either delayed or inadequate – this was because the responsibility of
arranging for blood is considered to be that of the family’s. Poor families of the deceased
women often had to pay enormous sums in addition to finding donors at short notice to
arrange blood.
Gayatri (name changed) from Dahod district suffered from swelling in her legs during the
sixth month of her first pregnancy. She was admitted at a private clinic at Godhra, and given
medicines, and then readmitted at S Hospital. A month later she was taken to P Maternity
Home at Godhra, where check up showed 7.9% Hb and sonography showed twins. Doctor
said that blood was needed, which couldn’t be arranged at Godhra so they came back
home. Her husband refused to donate blood. They came back to Godhra, admitted her to P
Maternity Home for 2 days and then took her to Baria Civil Hospital by ambulance (108).
They stayed there the entire day and were assured that she would get well, however no
doctor came to check on her at night. So next day, early morning around 6.00 am they took

her to L’s private clinic where they were informed that her condition was very critical.
Gayatri’s father, brother and uncle went to the Indian Red Cross Society to arrange for blood
but in the meantime she died. (Case 13, ANANDI)
Jyoti (name changed) from Anand district was pregnant for the second time and was
severely anaemic. She was given iron supplements by the ASHA; however she had not been
consuming them as informed by the family. During her ninth month, she was admitted at N
Hospital as she was suffering from cold, cough and very low Hb. She was given four bottles
of blood in two days and then discharged. A few days later, she complained of labour pain.
Due to lack of blood facility in the government hospital, she was re admitted in a private
hospital, where she delivered a baby boy. However, she was severely anaemic, and the
family could not pay for the blood. So her family requested for discharge from the hospital
the next day. Four days later, the woman complained of breathing problems and died at
home due to excessive loss of blood. (Case 3, Tribhovandas Foundation)
In cases recorded above, no observation and follow up during the post natal period, coupled
with insufficient EmOC facilities, and support for blood, led to woman’s death. Non
availability of blood due to lack of arrangements at the facilities- public and private seemed
a common phenomena which has been instrumental in delayed treatment, inadequate
care and issues of quality care are some of the commonly prevalent factors in most cases
of maternal mortality. Availability of blood has to be assured for all pregnant women. This
also has to be part of birth preparedness. Families, communities, college students, youth
groups, need to be mobilised for blood donation regularly.
5.7 Role of Public Health Facilities in Emergency Obstetric Care
The role played by a range of public health facilities – CHCs, Taluka Hospitals, Civil Hospitals,
District Hospitals as well as the Medical College Hospital - in these 46 stories is rather
distressing. The question which comes up is whether there are any protocols, standard
procedures and practices to ensure Comprehensive Emergency Obstetric Care that is
guaranteed in each district. What are the accountability mechanisms to ensure that each
level of the health delivery system discharges its role in provision of Emergency Obstetric
Care in the most responsible manner? Where and what are the checks and balances?

As mentioned earlier, many pregnant women and their families experienced that the
medical and para medical staff was not present at the time of hospitalisation in CHCs, Taluka
Hospitals, Civil Hospitals. This could contribute to the trust deficit that exists vis a vis the
public health system forcing people to find their way to other health facilities, in situations
of emergencies. Even where doctors were available in the hospital, in some cases there was
denial of services to patient. In a District Hospital the doctor present actually told the family
that he would not be there at night and that they had better take the woman to another
facility (a private hospital) Case 22 (ANANDI) states that Rs. 5000 was demanded in the
government hospital for an operation. Case 4 (ANANDI) states that there was denial of
services at various levels of the public health system. Most amazing was referral of a
woman from a medical college hospital to a private hospital!!
Case 3 TF is about lack of availability of blood in a government facility and the family having
to take the woman to a private hospital. Case 3 CHETNA RRC was about lack of life saving
care at the District Hospital for non obstetric care. Case 4 CHETNA RRC was about the
inability to administer the anti rabies vaccine. Case 8 ANANDI – the woman was left to die
unattended at the Taluka Hospital.
Continuum of care through the public health structure has been a problem. Case 2
Tribhuvandas Foundation states that the woman’s TB was not detected early enough in the
pregnancy. Similarly Case 7 Tribhuvandas Foundation was about late diagnosis of high risk
symptoms like the negative blood group, cardiac problems, and high BP. In Case 6
Tribhuvandas Foundation, the PHC nurse does not measure the BP and refers to SSG in
Vadodara and the woman dies on the stretcher. Thus failures to identify areas of concern in
the ANC period and not being able to communicate these to higher levels of care
jeopardises women’s lives. Similarly, when women fail to attend the follow up sessions
after crises, there is no follow up from the health system or any home visit.
Regular monitoring of maternal deaths and near misses, with the perspective of learning
from them and not fixing blame, and periodic meetings with community leaders and CBOs,
will help to build trust and complementary action to prevent maternal deaths.

6. Conclusion and Recommendations
This report shows the rather unacceptable state of affairs with women dying - in many cases
– needlessly, in the process of child birth in an otherwise progressive state like Gujarat. The
situation for marginalised and vulnerable women is rather grim – social, economic, and
cultural factors interact to compound their vulnerability. Early marriages and childbirths,
poor nutritional status and anaemia, physical work overload, poverty, and gender issues put
these women at grave risk during pregnancy, childbirth and after the child birth. Health
system factors like inadequate and less than satisfactory quality of ante natal care, weak
transport systems (despite the introduction of 108), poorly functioning health care facilities
from the Sub Centre, PHC, CHC, Civil Hospitals, District Hospitals, difficulties in accessing
emergency obstetric care including blood, non- existent Post Natal Care - all contribute in a
compounded way to Maternal Deaths.
Some of our recommendations are:
Ensuring quality ante natal care. In addition to the standard ANC parameters -
haemoglobin, BP, Odema etc for which the understanding and skills of the health
care providers need to be enhanced - better history taking, assessing of social
vulnerability factors, appropriate counselling for family members especially
husbands, needs to be included. Rigorous monitoring of ANC is required – the
supervisors/medical officers need to ask FHWs and ASHAs about follow-up actions
for each high risk and vulnerable pregnant woman. Community monitoring also
needs to be encouraged and institutionalised in a way that the health system feels
supported, and not threatened.
Ensuring sensitivity to social determinants and an understanding of high risk as going
beyond the bio medical factors, to include the various social determinants like young
age, literacy status and gender issues. Ensuring that these high risk women are
carefully followed up and supported through their pregnancies, childbirth and post
natal period. The peripheral health workers – ASHAs, FHWs, and AWWs – need to be
systematically trained to do early identification of both biomedical high risk and
social vulnerability factors. The multiple dimensions of vulnerability – including the
social dimensions - need to be recognised by the peripheral health workers and need

to be factored into their birth preparedness plan, health care delivery and follow up
plans.
Educating families for Ante Natal Care - the importance of each component as well as
the rationale - about high risk symptoms during the ante natal period, at labour and
during post natal period. While access to ante natal care and birth preparedness are
key steps in managing high risk pregnancies; information, access and realisation of
maternity entitlements in the ICDS, financial support through the KPSY, JSSK, JSY,
Chiranjeevi Yojana and free of cost health care services in form of cash, food grain
and support and assistance, are also critical.
Ensuring action to address malnutrition and anaemia in women and girls –
uninterrupted consumption of IFA, iron sucrose, good quality and adequate PDS and
ICDS take-home-rations.
To make Skilled Birth Attendance closer to women, functioning Sub Centres with safe
delivery services with a supportive role for local resources, like the trained traditional
dais that the women trust.
Accountability and governance of the public health institutions is of utmost
importance. As mentioned above, supportive supervision from within the system is
required for problem solving to ensure functioning and responsive Basic Emergency
Obstetric Services at each PHC and Comprehensive Emergency Obstetric Services at
the CHCs, Taluka Hospitals, and District Hospitals.
Ensuring continuum of care through two way communication and referral systems
between health facilities and the community – this will also address post natal care
of women who have delivered in facilities and help reduce the post natal maternal
deaths.
Similarly, ensuring systems of portability of services and entitlements and
disseminating information widely on these.
Assured availability of blood at short notice without making this the families’
responsibility. Organisation and promotion of blood donation camps at community
level.
Cashless services have to be provided to pregnant women. Otherwise,
reimbursement of all expenses has to be made part of the system. Grievance

redressal mechanism need to be clearly communicated to families so that they have
a forum to complain and get their complaints satisfactorily addressed.
Streamlined referral systems that are accountable, based on referral protocols -
written referral slip, phone calls to facilities where the woman is being referred,
accompanied transfers, stabilising the woman with first aid before referring her.
Good quality timely post natal care at facility as well as at household level.
Birth preparedness which includes that referral may be required and a decision
maker should be present. This should also include that blood transfusion may be
required – family and community members should be prepared to donate blood or
arrange for it at short notice. Phone numbers of emergency transport and referral
services should be available with the family. The individual vulnerability factors
should be discussed and birth preparedness should be done to minimise impact of
her vulnerability on her health and pregnancy outcome.
In addition, we would like to recommend that civil society organisations including local
sangathans and peoples’ organisations, panchayats/gram sabhas, VHSNCs should be
involved so as to increase maternal death reporting. NGOs/CSOs should also become part of
the MDR teams so that they can complement the MDRs with a social and community
perspective. NGOs and CSOs should also be part of the MDR Committees at the District
level so that they can take back the lessons from MDR analysis to the communities – this
can increase community consciousness of their responsibility for maternal health.
Discussions on Maternal Health and Maternal Deaths should become a public issue – all
stakeholders must act to promote maternal health! Community leaders and CBOs have an
important role to play locally to prevent maternal deaths and promote maternal health.
NGOs have a role to facilitate dialogue and coordination between community groups/CBOs
and health system at all levels, as well as to support community action for maternal health.

Annexure 1

Annexure 2
TABLE 1: District wise distribution of deaths
Districts
Block
Number of deaths in the Block
Total Number of deaths in the district
Dahod Baria 19 19
Panchmahal Ghoghambha 4
5 Godhara 1
Narmada Nandod 1 1
Bharuch Jhagadia 3
4 Valia 1
Anand Anklav 5
7 Umreth 2
Ahmedabad Dhandhuka 1
2 Viramgam 1
Banaskantha Amirgadh 2 2
Kheda Kathlal 1 1
Jamnagar Dwarka 2 2
Navsari Vansda 2 2
Tapi Songadh 1 1
Total 46 46
These maternal deaths are reported from 15 blocks of 11 Districts. Four of these blocks are
in the High Priority Blocks list of Government of Gujarat.
TABLE 2 - Age distribution of the women
Age (years) Number of women %
16 – 20 7 15.21
21 – 25 12 26.08
26 – 30 18 39.13
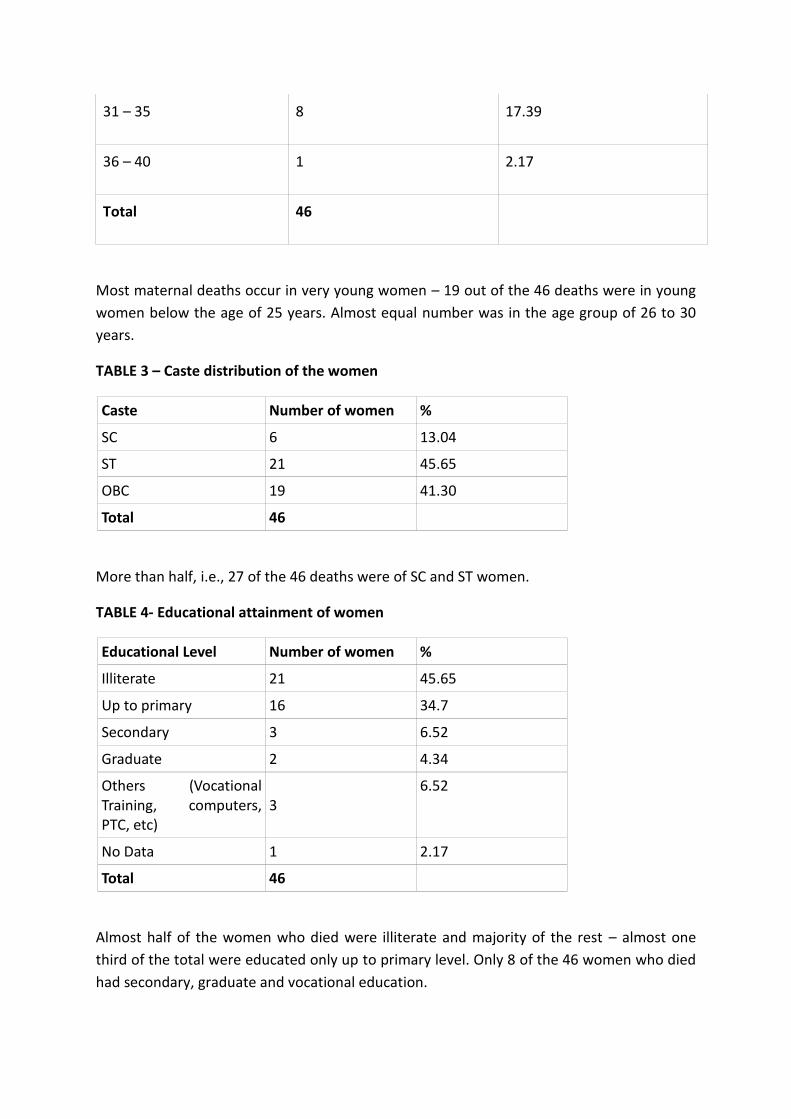
31 – 35 8 17.39
36 – 40 1 2.17
Total 46
Most maternal deaths occur in very young women – 19 out of the 46 deaths were in young
women below the age of 25 years. Almost equal number was in the age group of 26 to 30
years.
TABLE 3 – Caste distribution of the women
Caste Number of women %
SC 6 13.04
ST 21 45.65
OBC 19 41.30
Total 46
More than half, i.e., 27 of the 46 deaths were of SC and ST women.
TABLE 4- Educational attainment of women
Educational Level Number of women %
Illiterate 21 45.65
Up to primary 16 34.7
Secondary 3 6.52
Graduate 2 4.34
Others (Vocational Training, computers, PTC, etc)
3 6.52
No Data 1 2.17
Total 46
Almost half of the women who died were illiterate and majority of the rest – almost one
third of the total were educated only up to primary level. Only 8 of the 46 women who died
had secondary, graduate and vocational education.

TABLE 5- Occupation of the women
Occupation Number of women
Solely Housework 12
Domestic work and wage labour
5
Migrant labourer 9
Domestic work and farming
8
Agriculture, wage labour & domestic work
8
Agriculture, domestic work & migrant labourer
2
Others (Teaching, mid day meal in charge, LIC, ASHA, etc)
4
No data 2
Total 50*
Most of the women who died had multiple responsibilities – in addition to domestic work,
23 of them were involved in either agricultural work or/and wage labour, nine of them as
migrant workers. Three of the women who died were extension workers of the government
– either a teacher, Mid Day Meal in charge or an ASHA worker. One was an LIC agent.
*Multiple responses so the change in N
TABLE 6 – Number of pregnancies
Number of pregnancies Number of women %
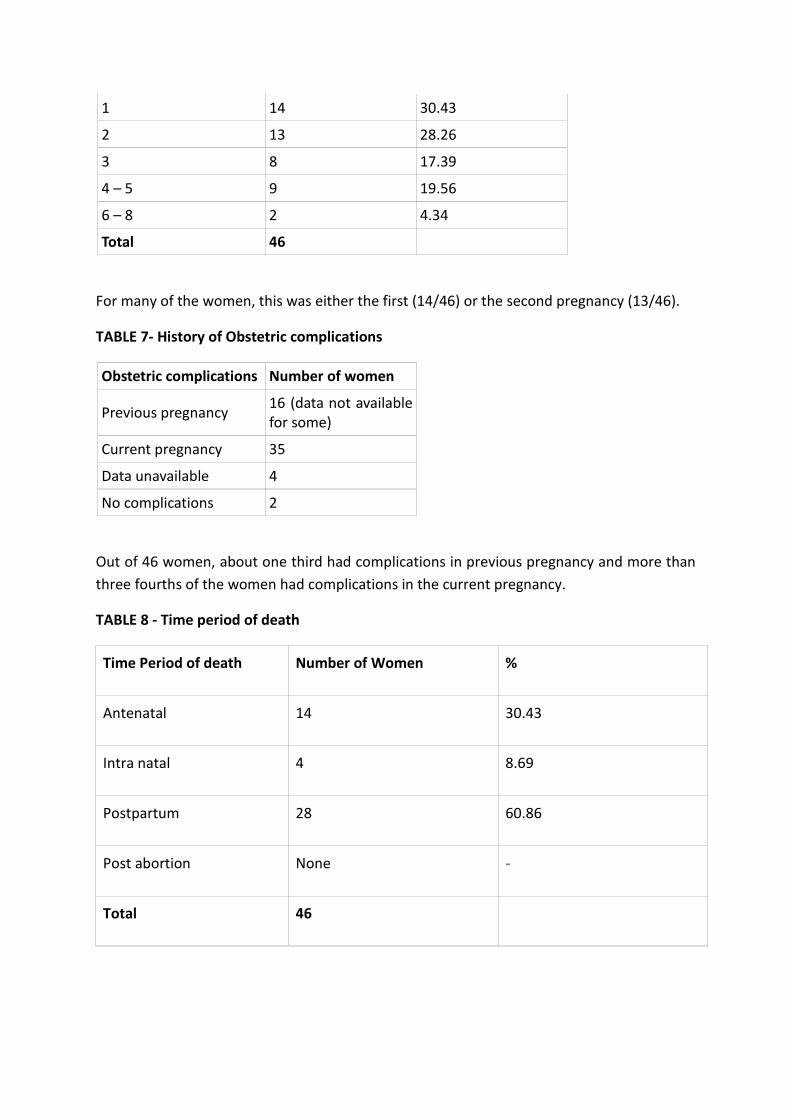
1 14 30.43
2 13 28.26
3 8 17.39
4 – 5 9 19.56
6 – 8 2 4.34
Total 46
For many of the women, this was either the first (14/46) or the second pregnancy (13/46).
TABLE 7- History of Obstetric complications
Obstetric complications Number of women
Previous pregnancy 16 (data not available for some)
Current pregnancy 35
Data unavailable 4
No complications 2
Out of 46 women, about one third had complications in previous pregnancy and more than
three fourths of the women had complications in the current pregnancy.
TABLE 8 - Time period of death
Time Period of death Number of Women %
Antenatal 14 30.43
Intra natal 4 8.69
Postpartum 28 60.86
Post abortion None -
Total 46

Fourteen women died in the ante natal period, four during the childbirth and 28 after
delivery.
TABLE 9 - Place of death
Place of death Number of women Percentage
Home 14 30.43
Health Facility 24 52.17
Public 10 41.6
Private 14 58.3
On the road 8 17.39
Home to first facility 1 12.5
One facility to another 6 75
Facility to home 1 12.5
Total 46 100.0
Fourteen maternal deaths took place at home, 24 in institutions (10 in private and 14 in
public institutions), eight deaths took place in transit.
TABLE 10- Place of Delivery/ Place of Birth
Place of Birth Number of women
Percentage
Home 10 21.7
Hospital 23 50
Public facility 9 19.56
Private facility 14 30.43
Data unavailable 1 2.17
Not applicable 12 26.0
Total 46 100
Out of the 46 cases interviewed for the study, 10 women delivered at home, 23 women
delivered at hospital, with 9 women delivering at a public hospital while 14 women
delivering at a private hospital. The data was not available for 1 case.

TABLE 11 - Probable medical cause of death
Out of forty six deaths that were analyzed and validated by medical experts, ten case stories
were not available for ascertaining the cause of death but probable causes have been
identified and included in the data below.
Table 11 a) Probable medical cause of death
Sr. No Type of cause N (44) %
1 Direct causes 28 60.86 2 Indirect causes 15 32.60
3 No data 3 6.52
Total 46 100
Out of 46 maternal deaths, deaths due to direct causes constituted 28 (60.86%) of deaths and
indirect causes were responsible for 15 (32.6%) deaths.
Table 11 b) - Details of Causes of Deaths
Sr.
No
Type of cause
N(46)
1 DIRECT CAUSES
N %
Haemorrhage (intrapatum, postpartum,Ante Partum) 12 26.08
Eclampsia ,Preeclampsia 7 15.21
Pulmonary Embolism 2 4.34
Sepsis 2 4.34
Blood transfusion reaction 1 2.17
Obstructed labour (Breech baby ) 1 2.17
CCF 3 6.52
Total 28
2 INDIRECT CAUSES
Anemia 4 8.6
Sickle cell Disease 2 4.3

Jaundice 2 4.3
Cardiovascular disease 2 4.3
Dengue/infection
1 2.1
Malaria 1 2.1
Tuberculosis 1 2.1
Renal failure 1 2.1
Rabies 1 2.1
Total 15
3 No data 3 6.52
Total 46 100
The most common cause of death was PPH (including Ante partum haemorrhage) in 12 (nearly 26
%), followed by Pre-eclampsia in 7 (15.2%), and Pulmonary embolism in 2 (4.34 %) of the women.
There were 2 deaths due to sepsis and one death each due to blood transfusion reaction and
obstructed labour.
Among the indirect causes unrelated to pregnancy, anaemia in 4 (8.6%%) was the commonest
followed by 2 deaths each due to jaundice, sickle cell disease and cardiovascular disease and one
each due to malaria, tuberculosis, rabies, renal failure and dengue.
The cause of death could not be ascertained in 3 (6.52 %) of the deaths.
The table below indicates that in 16 cases , more than one cause of death was identified like
anaemia was associated with 13/41 cases in both direct and indirect causes of death followed by
Cardiac failure (1/41) and PPH (1/41) and Septicaemia (1/41) were also some of the additional
causes of death.
Table 11 c) Additional Causes of death
Sr.No Cause Number
1. Anaemia 13
2 PPH 1
3 CCF (Congestive Cardiac failure) 1
4 Septicaemia 1

Total 16

TABLE 12 – Comparative table of probable cause of death and time period of death
Time of death
Probable medical
cause of death
Post
abortion
Antenatal
(14)
Intra-natal
(4)
Postpartum
(28)
Total
DIRECT CAUSE
Haemorrhage
(intrapatum,
postpartum,Ante
Partum)
0 2 1 9 12
Eclampsia
,Preeclampsia
0 2 0 5 7
CCF 0 1 0 2 3
Pulmonary Embolism 0 1 0 1 2
Sepsis 0 0 0 2 2
Blood transfusion
reaction
0 0 0 1 1
Obstructed labour
(Breech baby )
0 1 0 0 1
INDIRECT CAUSES
Anemia 0 1 1 2 4
Sickle cell Disease 0 1 0 1 2
Jaundice 0 1 0 1 2
Cardiovascular
disease
0 1 1 0 2
Dengue/infection
0 0 0 1 1
Malaria 0 1 0 0 1
Tuberculosis 0 0 0 1 1

Renal failure 0 0 0 1 1
Rabies 0 1 0 0 1
No data 0 1 1 1 3
Total - 14 4 28 46
TABLE 13 – Comparative table of probable cause of death and place of death
Place of Death
Probable medical
cause of death
Health
Facility
Home Transit Total
DIRECT CAUSES Public Private Home
to first
facility
One
facility
to
another
Facility
to
home
Haemorrhage
(intrapatum,
postpartum,Ante
Partum)
1 4 2 1 4 12
Eclampsia
,Preeclampsia
3 4 7
CCF 1 1 1 3
Pulmonary Embolism 2 2
Sepsis 2 2
Blood transfusion
reaction
1 1
Obstructed labour
(Breech baby )
1 1
INDIRECT CAUSES
Anemia 1 2 1 4

Sickle cell Disease 1 1 2
Jaundice 1 1 2
Cardiovascular
disease
1 1 2
Dengue/infection
1 1
Malaria 1 1
Tuberculosis 1 1
Renal failure 1 1
Rabies 1 1
No data 3
Total 9 13 13 1 6 1 46
Sr. No 7, TF. 1 death at home, not included in table as cause could not be
ascertained, the cause is mentioned as fever which is incomplete information.
Sr. No 8, ANANDI, death at Public Facility, not included in table as cause of death
could not be ascertained.
Sr. No 17, ANANDI, death at Private facility not included in table as cause of death
could not be ascertained.

Annexure 3