snq exam
DESCRIPTION
SNQTRANSCRIPT
REGUBREGUB 1st Sitting MAY 2009.
1. In a patient who has suffered a major loss of blood following a stab wound systemic pressure drops below 80 mmHg. Describe the two main theories to explain autoregulation of renal blood flow. What response within the kidney would you expect from the sympathetic nervous system?
2. Describe how the kidney compensates for respiratory acidosis.
3. Describe the countercurrent multiplier mechanism in the renal medulla and explain the role of the distal tubule and collecting ducts in excreting concentrated urine.
4. Contrast the mechanisms of action of the Type II diabetes treatments, sulphonylureas and thiazolidinediones.
5. A young male subject is brought to the hospital emergency department in a deep coma. Documentation on his person inform that he is a Type I diabetic subject and a rapid blood glucose measurement indicates severe hypoglycaemia. Injection of glucagon i.m. is indicated.
a) Explain briefly the necessity of administering a hyperglycaemic.b) Describe why glucagon and not cortisol is administered in this
situation and discuss the contrasting modes of action of glucagon and cortisol at the molecular / biochemical level.
6. The hypothalamus has different kinds of connections with the anterior and posterior pituitary gland. Write a short note discussing these two types of connections. Include in your answer specific examples of how the hypothalamus influences secretions of the pituitary gland.
7. A patient that is urinating excessively is diagnosed with diabetes
insipidus. What are the two major effects that vasopressin normally has in the body. Discuss (i) the role played by vasopressin in diabetes insipidus and (ii) the causes of the two types of this disease.
SNQ REGUB 3 SEP 2009
HIS SNQ Paper I –SEPTEMBER 2009

REGUB SNQ Paper I – 30 AUGUST 2010
HIS SNQ Paper I – 30 AUGUST 2010
HIS SNQ Paper I – 01 SEPTEMBER 2010
REGUB SNQ Paper I – JANUARY 2010

REGUB SNQ Paper I – 01 JUNE 2011
REGUB SNQ Paper I – 23 AUGUST 2011
Short Note Paper September 2007 REGUB
1. A 52 year old man was diagnosed as having Addison’s disease or primary hypoaldosteronism having collapsed at work; he was found to have a low blood pressure. Briefly outline some of the mechanisms involved in the reabsorption of sodium from the renal tubules and describe how the lack of aldosterone, which acts on the distal renal tubules, is implicated in the clinical presentation of primary hypoaldosteronism as described above.
2. A 66 year old woman is prescribed hydrochlorothiazide, a thiazide diuretic, for the treatment of hypertension. Explain how this diuretic produces its effects. What side-effects may she encounter with the use of this diuretic?
3. What is the range of mean arterial blood pressures over which renal blood flow is autoregulated? Describe the tubuloglomerular feedback mechanism for autoregulating renal blood flow.
4. An elderly female patient has been admitted to hospital following two days of severe vomiting. The data on the acid-base status of the patient is as follows:
Blood pH = 7.5 (reference range = 7.35-7.45) Plasma PaCO2 = 50 mmHg (reference range = 35-45 mmHg) Plasma [HCO3
-] = 38 mmol/l (reference range = 22-26 mmol/l)(a) Identify, giving your reasons, the acid-base disturbance from which the patient is suffering.(b) Explain why the plasma [HCO3
-] has risen above the normal value following the severe vomiting.
5. A young man involved in a car accident sustained severe crush injuries to his lower limbs and lost a considerable volume of blood. Following admission to hospital, he developed acute renal failure due to acute tubular necrosis. Some of the results of the initial laboratory investigations indicated that he was severely hyperkalaemic (high plasma [K+]).(a) Describe the mechanism in the distal nephron for secreting K+ into the filtrate.(b) Explain how the patient’s crush injuries could have contributed to the hyperkalaemia.
6. What is the most common molecular defect underlying the condition, congenital adrenal hyperplasia (CAH) in human subjects? Why does hyperplasia of the adrenals result from this defect and why do affected female subjects present very often with physical signs of virilisation?
7. What are the three main hormones involved in the regulation of calcium in the body? Describe the action of PTH and its role in the activation of vitamin D.
8. Methimazole is used in the treatment of hyperthyroidism. Describe how methimazole produces its desired effect. Why is propylthiouracil used in pregnant women? What are the major side-effects associated with anti-thyroid therapy?
9. Synthetic growth hormone is used illegally by some athletes and body builders. What actions of growth hormone are enticing athletes to take supplemental doses of growth hormone? What are the potential side effects of these supplements?
10. 35 year old woman was recently diagnosed with hyperthyroidism. She initially presented to her GP complaining of weight loss. She also complained of heat intolerance and sweating.(a) Describe the sequence of events which leads to sweating in hyperthyroid patients.(b) Explain why hyperthyroid patients usually have warm extremities.
1. Describe the process for production of angiotensin II, including reference to the organs and enzymes involved. What are the major effects of angiotensin II in the body? Briefly comment on the activity of aldosterone.
2. In the accident & emergency room a patient is treated with a loop diuretic to reduce the acute pulmonary edema of congestive heart failure:[a] name a specific example of this class of diuretics;[b] describe how this drug acts as a diuretic;[c] list the possible adverse effects.
3. List the criteria which a substance must fulfil so that its clearance is a measure of the glomerular filtration rate (GFR). Explain why creatinine clearance is a measure of the GFR in spite of the fact that it does not fulfil all of the criteria you have listed.
4. A 40 year old man, who had been been admitted to hospital 3 days previously with pneumonia, has now been diagnosed with the syndrome of inappropriate ADH secretion (SIADH).[a] Describe the role of ADH in water reabsorption in the collecting ducts of the kidneys and explain how SIADH is likely to affect plasma and urine osmolarity in the patient.[b] If you were provided with a value for the patient’s plasma sodium concentration, indicate, giving your reasons, how you would calculate an approximate value for plasma osmolarity.
5. A 22 year old known diabetic man presents with severe polyuria and polydipsia. He is dehydrated and hypotensive. Urinalysis is strongly positive for glucose and ketones. The data on his acid-base status is as follows:Blood pH = 7.31 (reference range = 7.35-7.45)Plasma Pa CO2 = 27 mmHg (reference range = 35-45 mmHg)Plasma [HCO3
-] = 13 mmol/l (reference range = 22-26 mmol/l)[a] Identify, giving your reasons, the acid-base disturbance from which the man is suffering.[b] Indicate the type of compensation which is occurring and describe the mechanism which underlies it.
7. What is parathyroid hormone? Describe its actions in health.
8. A 19 year old woman presents to her GP with palpitations and sweats. On examination she appears to be agitated, tremulous and is tachycardic at 130 beats per minute in atrial fibrillation. She is admitted to hospital and improves

with beta blockers and carbimazole. Discuss the likely cause of this woman’s condition and how the drugs may act to relieve her symptoms.
9. A woman in substantial pain called her doctor. She was crying and was worried that she was about to have her baby “right now”. The doctor calmed her down and asked her how she knew this. She explained that her water had broken and that her husband could see the baby’s head.[a] Was she going to deliver her baby ? If so, what stage of labor was she in?[b] Explain whether or not she would have time to get to a hospital that was 1.5 hours away to deliver the baby ?[c] Describe the role of physical and hormonal factors in parturition.
10. A 26 year old woman has had insulin-dependent diabetes mellitus for the past fifteen years. Diabetic nephropathy has now been diagnosed. Describe the symptoms and consequences of diabetic nephropathy. What are advanced glycation end products and how may these contribute to this diabetic complication?
GIHEP
January 2009
Q1. A 64 year old lady undergoes surgical repair of her pelvic diaphragm to help treat her urinary incontinence. Draw or describe the pelvic diaphragm, including its parts, attachments and innervation. What other problems may this lady experience with a lax (loose) pelvic diaphragm?
Q2. A 45 year old male presents to Accident and Emergency, stating that he has started vomiting blood earlier that day (haematemesis). He undergoes endoscopy and an ulcer is found in the first part of his duodenum. Draw or describe the duodenum, including its parts, relations and blood supply. Why was this patient vomiting blood?
Q3. A young man is stabbed in the abdomen resulting in a tear through the greater omentum. Omentum is a form of peritoneum.
(a) What are the attachments of the greater and lesser omenta?(b) What is the Foramen of Winslow (epiploic foramen) and what are its
boundaries?(c) What is Pringle’s Manoevre and why is it performed?(d) What are the greater and lesser omenta derived from?
Q4. A patient with cholera is given oral rehydration therapy with a solution of glucose and salt. Describe, using a diagram, how the sodium, chloride, glucose and water will be absorbed.
Q6. A patient with Type I Diabetes who is non-compliant with their insulin therapy will typically present with hyperglycaemia, ketosis and

hypertriglyceridaemia. Describe briefly the mechanisms underlying these three phenomena in such a patient.
Q10. Both in family practice and in the hospital setting, nausea and vomiting are commony encountered. Classify potential causes of nausea and vomiting and distinguish how they are treated with drugs having differing mechanisms of action.GIHEP SNQ Paper I – JANUARY 2010
1. A rural GP (doctor) sees an 18 year old male patient in his clinic with a 2 month history of a right groin lump. The GP identifies this as an inguinal hernia. Draw or describe the inguinal canal. What are the surface markings of the deep and superficial rings? What is the difference between a direct and an indirect inguinal hernia?
2. A 2-year-old child was brought to the outpatient clinic because he has had constipation and poor weight gain for approximately one year. Examination revealed anemia and abdominal distension. A barium enema X ray was requested and the diagnosis of Hirschsprung’s disease was suspected. This was confirmed by rectal biopsy.
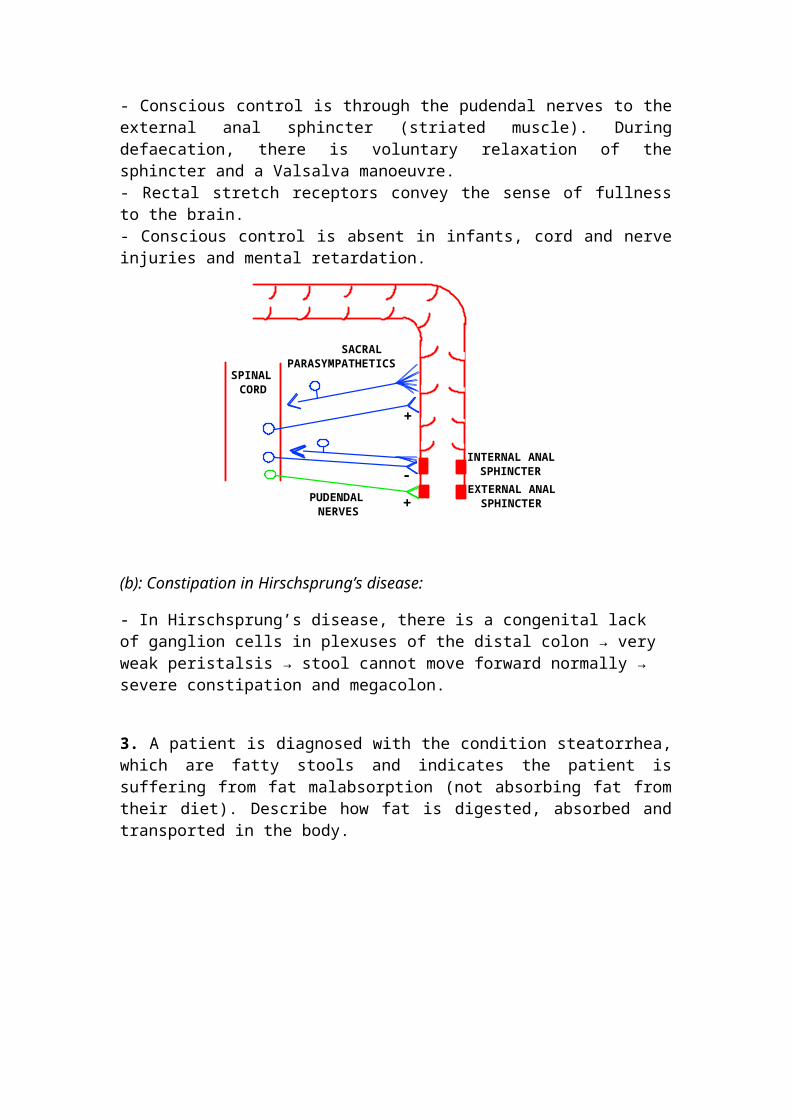
(a) With the aid of a diagram, describe the defecation reflex.
(b) Explain why there is severe constipation in Hirschsprung’s disease.
Model answer:
(a) Defecation reflex:
INTRINSIC REFLEX:- Rectal distension causes peristalsis in the descending and sigmoid colon and in the rectum and relaxation of the internal anal sphincter. - This intrinsic reflex is controlled by intramural plexuses. Therefore, with lesions of the extrinsic nerves or spinal cord, defecation is still possible.EXTRINSIC REFLEX:- Rectal distension activates stretch receptors → sensory information running in the sacral parasympts.- This reflexly activates parasympt. efferents causing reflex peristalsis in the colon and rectum and relaxation of the internal anal sphincter. Sympts do the opposite but are less important.CONSCIOUS CONTROL:- Conscious control is through the pudendal nerves to the external anal sphincter (striated muscle). During defaecation, there is voluntary relaxation of the sphincter and a Valsalva manoeuvre.- Rectal stretch receptors convey the sense of fullness to the brain.- Conscious control is absent in infants, cord and nerve injuries and mental retardation.

SPINAL CORD
INTERNAL ANAL SPHINCTER
EXTERNAL ANAL SPHINCTER
+
-
+
SACRALPARASYMPATHETICS
PUDENDAL NERVES
(b): Constipation in Hirschsprung’s disease:
- In Hirschsprung’s disease, there is a congenital lack of ganglion cells in plexuses of the distal colon → very weak peristalsis → stool cannot move forward normally → severe constipation and megacolon.
3. A patient is diagnosed with the condition steatorrhea, which are fatty stools and indicates the patient is suffering from fat malabsorption (not absorbing fat from their diet). Describe how fat is digested, absorbed and transported in the body.
HIS SNQ Paper I – January 2009


HIS SNQ Paper I 30 AVRIL 2010
GIHEP SNQ Paper I 17 JANUARY 2011
ALIMENTARY SYSTEM
Q1 What is jaundice? Briefly describe the mechanism by which Bilirubin is detoxified and excreted by the liver.
Q2 You are asked by your consultant surgeon to assist her in a hysterectomy. She discusses the anatomy of the uterus with you prior to the operation.
a) Explain the normal position of the uterus.b) What is the blood supply of the uterus? c) What is the lymphatic drainage of the uterus? Where can lymph
nodes draining the uterus be palpated?d) What are the supports of the uterus?
Q3 A 44-year-old female presented with a 6-month history of fatigue, myalgia (muscle pain), and decreased production of saliva and tears. Antibodies to the SSA antigen were positive and the diagnosis of Sjogren’s syndrome was confirmed.
a) Outline the functions of saliva.
b) Briefly describe normal control of salivation.
HIS SNQ Paper I – 17 AUGUST 2011
Paper I – 16 JANUARY 2011
GIHEP SNQ Paper I –SPTEMBER 2008
1. You have been asked to insert a urinary catheter into a male patient. Describe the anatomy of the male urethra, including its position, parts and relations.
2. An elderly gentleman presents to the accident and emergency department with bowel infarction (loss of blood supply to the bowel). Describe the origin and branches of the superior mesenteric artery (SMA). What does it supply? Where does the venous drainage from the superior mesenteric vein go? Which parts of the gastrointestinal tract are derived from the embryological midgut?
3. A lady attends her GP with severe dull pain in her epigastrium and back, associated with weight loss. A CT scan confirms a pancreatic carcinoma. Describe the pancreas, including its parts, relations and blood supply. What is an annular pancreas?
4. A 45 year old gentleman attends the accident and emergency unit with severe upper abdominal pains, following a night of heavy alcohol consumption. Blood tests reveal an elevated serum amylase level; in addition, his liver transaminases are mildly elevated. A CT scan is performed, which shows evidence of early cirrhosis of the liver and an acutely inflamed pancreas. Describe the different phases of bile secretion from the liver.
5. The folded structure of proteins is crucial to determining their biological activity in the body. Describe briefly the primary, secondary and tertiary structure of proteins, using diagrams as appropriate.
6. Briefly outline some of the mechanism by which the liver can detoxify foreign compounds giving some examples.
7. . The Cori cycle involves the recycling of lactate in the human body. When this cycle is active, what tissues are involved and what is achieved by its operation?
8. Describe the digestion and absorption of fats. Include reference to causes and consequences of fat malabsorption.
9. In a busy family practice, disorders of bowel habit are common, with extremes of function indicated by constipation and diarrhoea. Outline one class of drug used to treat each of these extremes. Describe the mechanism of action and adverse effects for each example.
10. The therapeutic index is an indicator of the safety profile of a drug. Discuss this statement using quantal dose response curves to illustrate your answer.
Short Note Paper January 2009
Q1. A 64 year old lady undergoes surgical repair of her pelvic diaphragm to help treat her urinary incontinence. Draw or describe the pelvic diaphragm, including its parts, attachments and innervation. What other problems may this lady experience with a lax (loose) pelvic diaphragm?
Q2. A 45 year old male presents to Accident and Emergency, stating that he has started vomiting blood earlier that day (haematemesis). He undergoes endoscopy and an ulcer is found in the first part of his duodenum. Draw or describe the duodenum, including its parts, relations and blood supply. Why was this patient vomiting blood?
Q3. A young man is stabbed in the abdomen resulting in a tear through the greater omentum. Omentum is a form of peritoneum.
1. (a) What are the attachments of the greater and lesser omenta? 2. (b) What is the Foramen of Winslow (epiploic foramen) and what are
its
boundaries?
3. (c) What is Pringle’s Manoevre and why is it performed? 4. (d) What are the greater and lesser omenta derived from?
Q4. A patient with cholera is given oral rehydration therapy with a solution of glucose and salt. Describe, using a diagram, how the sodium, chloride, glucose and water will be absorbed.
Q5. Metabolic processes in the body often require utilization of endergonic chemical reactions which require the input of energy in order to proceed. This is achieved by coupling such reactions to the hydrolysis of adenosine triphosphate (ATP). Write a short note on the synthesis of ATP by mitochondria, including comment on the significance of the impermeability of the inner mitochondrial membrane.
Q6. A patient with Type I Diabetes who is non-compliant with their insulin therapy will typically present with hyperglycaemia, ketosis and
hypertriglyceridaemia. Describe briefly the mechanisms underlying these three phenomena in such a patient.
Q7. Epidermal growth factor (EGF) is a growth factor that plays an important role in the regulation of cell growth, proliferation, and differentiation by binding to its receptor EGFR. What type of receptor is the EGFR? Explain how binding of EGF to its receptor produces a response in the target cell.
Q8. Describe the metabolic roles of vitamin A and vitamin D in the body. Outline their dietary sources and the causes and effects of deficiency.
Q9. Write short notes on DNA replication describing how the leading and lagging strands are synthesized. Diagrams may be used to illustrate your answer.
Q10. Both in family practice and in the hospital setting, nausea and vomiting are commony encountered. Classify potential causes of nausea and vomiting and distinguish how they are treated with drugs having differing mechanisms of action.
Short Note Paper September 2008 GIHEP
1. In clinical practice, disorders of the upper and lower gastrointestinal tract are common causes of distress. Contrast the roles of histamine H1
antagonists and histamine H2 antagonists in the treatment of such disorders.
3. Paracetamol is a drug that has different clinical indications.[a] Briefly explain the metabolic pathway involved in producing liver necrosis after ingestion of a high dose of this drug.[b] Mention one antidote that can be used to reverse this toxicity. Briefly explain the mechanism of action of that antidote.
4. A 37-year-old woman with a 2-year history of progressive dysphagia (difficulty in swallowing) to both solids and liquids, as well as a 10-lb weight loss, presented for evaluation. Barium studies suggested a diagnosis of achalasia. Esophageal manometry showed absence of peristalsis and a high lower esophageal sphincter pressure. Describe the phases of swallowing. What is the effect of gastrin on the lower esophageal sphincter?
6. The liver is an important organ for the detoxification of both endogenous and exogenous compounds. Briefly describe the detoxification process involved in the excretion of bilirubin. How may known alterations to this process be used to diagnose liver disease?
9. Explain why steatorrhea results from the absence of bile salts or pancreatic juice. Comment briefly on the enterohepatic circulation.
10. Dr. Gaylord prepared for running a 40km marathon by eating a high carbohydrate meal the day before the race. Briefly describe:[a] how and where glucose is stored in a readily mobilizable form in the body[b] how glucose is released from those storesName the process that is used to provide glucose when those stores are depleted and name one reaction unique to that process.
12. You pass a urinary catheter in a male patient. Describe or draw the parts of the urethra through which the catheter passes. What type of epithelium lines most of the urethra?
13. A patient presents to the accident and emergency department with a large abscess, just lateral to his anal canal, which requires surgical drainage. Describe the boundaries and contents of the ischiorectal fossa. What is supplied by the nerve that runs in Alcock’s canal?
14. You are a medical student attending a clinic in the pediatric unit. A 12 year old boy is diagnosed with acute appendicitis. Describe the location / locations and blood supply of the appendix. Explain why the patient has referred pain to the umbilicus. Write a short note on the congenital abnormalities associated with the vitelline duct.
15 On palpating a patient’s abdomen, you feel a large hard mass in the epigastrium. A malignant tumour of the stomach is diagnosed. Describe the position, parts, blood supply and lymphatic drainage of the stomach. To which structures may this malignancy spread?
Short Note Paper SEPTEMBER 2006 GIHEP
Q1. Give the surface markings for the following:
1. a) The transpyloric plane 2. b) The base of the appendix 3. c) The spleen 4. d) The gall bladder
Q2. A 39 year old male presents to the Accident and Emergency Department with ureteric colic. Describe the course of the ureter and structures that are related to it. Outline the places where it is narrowed and why this is important.
Q3. A patient presents to Accident and Emergency Department and is diagnosed with pancreatitis. Describe the anatomy of the pancreas with particular reference to the parts, blood supply and venous drainage. Write a note on the embryological origins of this organ and potential abnormalities that may arise.
Q4. A 55 year old woman has been diagnosed with cancer of the uterus. Describe the anatomy of the uterus. Include details on the structure, relations, blood supply, venous and lymphatic drainage.

Q6. In clinical practice, nausea and vomiting can be a frequent occurrence across all age ranges. Outline the receptors that are involved in the regulation of emesis. Describe briefly how drugs acting at these receptors can be used to control different forms of emesis.
Q8. Hypertriglyceridaemia (plasma triglyceride concentrations > 2.3 mmol/L) is observed in both Type I and Type II diabetes mellitus and results in part from failure of the normal regulation of triglyceride metabolism in adipose tissue. Briefly describe:
1. a) The normal hormonal regulation of triglyceride synthesis and breakdown in adipose tissue
2. b) The factors that contribute to the development of hypertriglyceridaemia in diabetes
Q9. The human body stores energy in the form of glycogen and triglycerides. Regarding glycogen stores, write BRIEF NOTES describing the following:
1. a) The location and relative size of glycogen stores in the human body 2. b) The differences regarding the physiological circumstances and
purposes to which these stores are utilised within the two main sites in the body
3. c) The hormonal influences that determine when and which of these storage sites is to be utilised to supply energy
Q10. Calcium is an essential dietary constituent. Write BRIEF NOTES in response to the following:
1. a) What are good dietary sources of calcium? 2. b) How is it absorbed in the intestine and what kidney-derived
substance controls this process? 3. c) Where is the bulk of calcium found in the body, in what form and to
what extent? 4. d) What is the normal level of calcium in the blood, in what form is it
and name ONE function it is performing there? 5. e) What is the approximate concentration of free calcium within cells
and what ubiquitous protein often binds to it when it exerts its physiological roles?
Q11. Mrs. Smith, a 48 year old publican, is complaining of abdominal pain, with occasional vomiting. Blood tests revealed a low haemoglobin concentration. The possibility of underlying liver disease should be considered in a patient with this history. Briefly describe what biochemical test you would request to exclude a post hepatic liver cause of the abdominal pain and then discuss what biochemical changes you would expect if the diagnosis was impacted gall stones.
Q15. Briefly describe the three major physiological factors causing gastric acid secretion in normal digestion.

Short Note PaperJanuary 2007 GIHEP
3. Peptic ulcer disease is suggested by the symptoms of abdominal pain and occasional vomiting, together with low haemoglobin. What is the most common cause of peptic ulcer? What initial treatment regimen would you recommend and what is the mechanism of action of the acid suppressant used in that regimen?
4. A 67-year-old man with a history of alcohol abuse was admitted with a 4-day history of abdominal pain and vomiting. He was febrile, dehydrated, and hypotensive. Laboratory evaluation showed anemia (hematocrit 29%) and leukocytosis. Occult blood was present in the stool. Endoscopic examination of the upper digestive tract confirmed the diagnosis of peptic ulcer disease.Describe the mechanism of gastric hydrochloric acid secretion.
5. The liver is an important organ for the detoxification of both endogenous and exogenous compounds. Briefly describe the detoxification process involved in the excretion of bilirubin. How may known alterations to this process be used to diagnose liver disease?
6. The human body mobilises its fat stores to provide fuel for the tissues in the fasting state. Describe briefly [a] the process of lipolysis (triglyceride breakdown) and [b] the hormonal stimuli that control the balance between lipolysis and triglyceride synthesis.
7. There is a rare recessively inherited disease, called abetalipoproteinaemia which, in affected subjects, is characterised by an inability to form chylomicrons in the intestine. Affected individuals have only 20-25% of normal plasma cholesterol and triglyceride levels.They have severe fat malabsorption and steathorrhea.BRIEFLY explain:[a]What are chylomicrons.[b]What is your understanding of steathorrhea.[c]Why would a subject with this genetic condition present with delayed blood clotting time, atypical eye lesions and irregularly shaped RBC’s which revert to normal in response to megadoses of vitamin E.
8. Briefly describe the mechanisms for digestion and absorption of proteins.
10. One of the bacterial toxins secreted by Clostridium perefringens, the bacteria that causes gas gangrene, is a lipase that hydrolyses phosphocholine from phosphatidylcholine and sphingomyelin. The resulting lysis of cells provides nutrients for the bacteria’s growth. Discuss the different classes of plasma membrane lipids, commenting on the role of fatty acid chains in maintaining membrane fluidity.
12. A young man is brought to hospital after a road traffic accident with abdominal pain. An abdominal CT scan shows that he has injured his spleen
and needs an operation. Describe the position of the spleen, including its vascular supply and relations. In which direction does it expand if enlarged?
13. A patient presents to the accident and emergency department with a bleeding duodenal ulcer. Describe the parts and relations of the duodenum. Add a note on the embryology and blood supply of the duodenum
14. Mrs. Patel is a 52-year-old canteen supervisor. She presents with a history of recurrent upper right abdominal pain associated with eating fatty meals. The pain has been particularly bad for the past 24 hours and on this occasion she is mildly jaundiced. Radiology confirms the presence of gallstones. Outline the pathway by which bile passes from the cells in the liver to the duodenum. Explain why she has become jaundiced.
15. A patient presents with faecal and urinary incontinence. Describe, briefly, each of the anal and urinary sphincters, including their position and nerve supply. Add a short note on the embryology of the anal canal.
4. Q4. Briefly describe the role of chylomicrons in the post absorption processing of dietary fat.
5. Q5. Describe the post absorption utilization of amino acids with reference to the fates of EITHER the amide or carbon skeleton components.
6. Q6. Describe the metabolic fate of high post-prandial levels of glucose, indicating the tissues involved in its utilization and /or storage.
7. Q7. Briefly outline the mechanism for detoxifying foreign compounds.
8. Q8. A 48 year-old man presents with chronic diarrhoea containing blood and is given a diagnosis of Crohn’s disease. List the treatment options and outline the mechanism of action and side effects of one agent.
9. Q9. A 68 year old man is admitted through A & E with an abdominal aortic aneurysm. Describe the anatomy of the abdominal aorta.Outline the branches and the vertebral levels that they arise from.How does the aorta enter the abdomen and how does it terminate?
10.Q10. A 48 year old male with a history of alcohol abuse is admitted to hospital with haematemesis (vomiting blood). He has a history of oesophageal varices. With the aid of diagrams describe the portal circulation. Give 2 examples where portosystemic anastomoses occur.
11.Q11. A patient presents with obstruction of the biliary tree. With the aid of diagrams describe the histology of the liver and biliary tree. Describe the vessels that are compressed during a Pringle’s Manoeuvre and outline the relationship of these structures to each other.
12.Q12. A 54 year old lady presents with bleeding due to haemorrhoids. Describe the upper and lower halves of the anal canal with regard to the anatomy, histology, arterial and venous drainage, lymph drainage and nerve supply. Write a note on the embryological development.
13.Q13. A patient with constipation is given a laxative to increase colon motility. Describe normal colon motility and how it is controlled.
Short Note Paper JANUARY 2006 GIHEP
1. Q2. John, a 52 year-old man, presented to his GP for a general check-up. Blood samples taken for biochemical analysis revealed the following:
Total plasma cholesterol 9.0 mmol/L [reference range 3.5 – 6.5 mmol/L] LDL cholesterol 6.2 mmol/L [reference range 2.0 – 4.5 mmol/L]
To manage John’s hyperlipidaemia, the GP prescribed Lipitor (atorvastatin) and recommended a number of life-style changes. Lipitor is a competitive inhibitor of the enzyme hydroxy-methyl-glutaryl CoA Reductase (HMG-CoA reductase), which plays a key role in cholesterol biosynthesis. Write a short note on enzyme inhibitors, covering mechanisms of inhibition (irreversible, reversible, competitive and noncompetitive) and describing the use of the Lineweaver-Burke plot to identify the mechanism of action of an inhibitor.
2. Q3. Karen, a 25 year-old with a history of poorly controlled Type I diabetes mellitus, presented to the Accident and Emergency Department. During the consultation, Karen said that she had been experiencing polyuria (frequent urination), polydipsia (increased fluid intake), nausea and vomiting. When asked, she admitted that she had neglected to take her Insulin injections over a period of days. Physical examination revealed marked dehydration (dryness of skin and tongue), hyperventilation (Kussmaul respiration) and her breath smelled quite strongly of acetone. Arterial blood gas analysis demonstrated a metabolic acidosis and biochemical testing showed elevated levels of glucose and ketones in her blood and urine.
Briefly describe [a] the normal role of insulin and the biochemical defects observed in Type I diabetes and [b] the mechanism that leads to ketoacidosis in uncontrolled diabetes.
FUN IMMU– January 2009
4. Phagocytes are key to initiating the immune response to infection or injury. Describe the role of these cells in the initiation and resolution of acute infection.
5. The immune system has evolved ways to distinguish between different infections. In the context of viral infection describe how the following two mechanisms help contain the infection.
a. type I interferons (IFNs)b. Cytotoxic T cells
6. Discuss the rationale underlying the use of ‘biologic therapies’ in the management of rheumatoid arthritis.
7. IL-2 is a key regulator of the immune response in auto-immune disease. Describe two mechanisms by which drugs can be used to reduce the actions of IL-2. Give an example of a drug in each class. HIS SNQ Paper I 1 SEPTEMBER 2009
1 A 59 year old man presents to the Emergency Department with central chest pain. He is diagnosed as having had a myocardial infarct (MI) and blood is sent to the laboratory for determination of biomarkers to confirm the diagnosis. He is treated immediately with a cocktail of aspirin, heparin and a thrombolytic drug. Discuss the role of aspirin in this context and comment on its side effects.
Model answer: Aspirin is used in this context as an anti-platelet agent. It inhibits the production of Thromboxane in response to platelet activation. It does this by irreversibly inhibiting the cycloxygenase en zyme. By suppressing thromboxane sysnthesis, aspirin prevents the recruiment of platelets to a growing thembus. It has been shown to inhibit mortality from myocardial infarction by 25%. Its effects are additive with heparin and streptokinase.
Major side effects of aspirin include gastric bleeding-due to inhibition of cyclooxygenase in the endothelial cells of the stomach which affects the

regulation of acid secretion. Other adverse effects include reyes syndrome, allergic reactions and CNS effects.2. Respiratory syncytial virus (RSV) is the major cause of viral pneumonia in infants and young children. It infects bronchial epithelial cells and infection results in lung inflammation and decreased airway function. As a pathogen, RSV is particularly well adapted to evading host immune responses. Write short notes on the role of the following in antiviral immunity1. type I IFNs2. cytotoxic T cellsCJ3. Discuss the rationale underlying the use of ‘biologic therapies’ in the
management of rheumatoid arthritis.
HIS SNQ Paper I –26 AUGUST 2010
HIS SNQ Paper I –SPTEMBER 2008
Q3: The role of innate and adaptive immune responses is ultimately to respond to and eliminate antigen. Briefly describe the effector mechanisms that the following cells use to eliminate pathogens and discuss how they may work together:(a)macrophages(b) B cells.
Q4: The Major Histocompatibility Complex (MHC) presents antigen to T cells. Describe the role of MHC in an immune response to an extracellular infection focussing on:
a. MHC molecule involvedb. Pathway of antigen presentationc. T cell subtype it presents tod. Downstream consequences of T cell activation
Q5: Haemolytic disease of the newborn is an example of rhesus incompatibility. Describe i) the cause, ii) the consequences for the developing foetus iii) and treatment of this condition.
Short Note Paper September 2007 FUN2 IMMU
1. Describe two ways cells of the immune system communicate with each other giving examples of each. In each example describe the cell types involved, and the functional effects that occur as a result.

2. Activation of T helper cells is a multi-step process. Describe the role of antigen recognition by the T cell receptor and co-stimulatory receptors in this process.
3. Biological DMARDs (Disease modifying anti-rheumatic drugs) are used in the management of rheumatoid arthritis. Name three such drugs and for one, discuss the rationale for its use, and its possible side effects.
4. Medical suppression of the immune system is necessary for the prevention of allograft rejection and autoimmune disease. Write brief notes on the difference in mechanism of action of Cyclosporine A and Sirolimus.
Short Note Paper SEPTEMBER 2006 FUN IMMUNOL
Q3 A 65 year old man has osteoarthritis and is prescribed a non-steroidal anti-inflammatory drug (NSAID). Describe the common side effects associated with NSAID therapy.
Q5 The humoral immune response is important for the clearance of extracellular bacterial infections. Describe briefly how the complement pathway aids in the clearance of a bacterial infection
Q6 Mr Jones, 62 years of age, has developed the syndrome of inappropriate anti-diuretic hormone (SIADH) secretion resulting in excessive water retention.
1. a) How is this excess fluid distributed throughout the body fluid compartments?
2. b) How is body fluid osmolarity affected?
Q7 The main metabolic activities in the human erythrocyte are glycolysis and the hexose monophosphate shunt. In what way is glycolysis in the erythrocyte distinctive and unlike the process in other body tissues?
Q8 Describe, with the aid of a diagram, how cytotoxic T cells recognize and kill virally infected cells. In your answer, indicate the important molecules involved in these processes on T cells and virally infected cells.
9. Q10 A patient is on immunosuppressive therapy following a kidney transplant. Briefly discuss the MOA of ONE immunosuppressive drug.
FUN LL
HIS SNQ Paper I – 11 JANUARY 2010
HIS SNQ Paper I –26 AUGUST 2010
Short Note Paper September 2008 FUN LL
Q1. A patient presents with pain referred along his sciatic nerve. Where is the greater sciatic foramen? Draw or describe the structures that emerge from the greater sciatic foramen. What is the safest injection site in the gluteal region to use, in order to avoid sciatic nerve injury?
Q2. A 38-year-old lady is brought to the Accident & Emergency Department with a bimalleolar ankle fracture following a fall on an icy pavement. Describe the ankle joint, including its articulating surfaces, ligaments and the movements that occur here. Which malleolus is the more commonly fractured?
Q3. You are asked to examine the ligaments of the knee joint. Describe the attachments of each ligament you mention, and state how you would test them.
Q5. Compare and contrast the characteristics and pharmacological properties of muscarinic and nicotinic cholinergic receptors in the autonomic nervous system.
Q6. Malignant hyperthermia, a rare life-threatening condition that is triggered by exposure to drugs used for general anaesthesia, is a condition arising from mutations in components of the excitation-contraction coupling (ECC) mechanism of skeletal muscle. Briefly outline the stages involved in ECC, making reference to the molecular components in each stage. How does relaxation occur?
Q7. A patient is given a calcium channel blocker to reduce heart muscle force. Describe the length-tension relationship for heart muscle. Why can heart muscle not be tetanized?
HIS SNQ Paper I –11 JANUARY 2011
Q4 In October 2010, a cholera epidemic struck the rural Artibonite region of Haiti. The United Nations humanitarian agency reported more than 3500 confirmed

cases and more than 250 deaths. Describe the effects of cholera on body fluid homeostasis, its consequences, and the appropriate treatment strategy.Q6 A 15-year-old schoolgirl was admitted to hospital as an emergency whilst on holiday. Her parents believed her to be allergic to nuts. At the age of 5 years, she developed marked angioedema of her face, lips and tongue, followed by tightness of her throat and vomiting following inadvertent ingestion of peanuts.The emergency admission occurred following a single bite of a health food bar. Within seconds, she developed angioedema of her lips and tongue, difficulty in breathing and felt light-headed. With respect to the above case answer the following:
1. Describe the cells activated during the sensitisation phase of the response (first exposure to antigen).2. What role does IgE specific to the allergen play on subsequent exposure to the allergen?
HIS SNQ Paper I – 16 AUGUST 2011
HIS SNQ Paper I – 30 AUGUST 2011
HIS SNQ
HIS SNQ Paper I – 18 JANUARY 2012
HIS SNQ Paper I –12 JANUARY 2012
HIS SNQ Paper I – 12 JANUARY 2012