slide 1
TRANSCRIPT

Khalid Swenia MBBCH, FRCSC
Cardiac Surgeon
Libyan Cardiac Society
Heart Failure Scientific day
July 1 st 2010
TMC

Cardiac Dysfunction Post-Pump: ddx
Ischemia: graft dysfunction or spasm
Valve thrombosis or dehiscence
Uncorrected valvular pathology
Pneumothorax/hemothorax
Pericardial tamponade
Malposition of endotracheal tube (low PO2 and/or pH)
Inadequate volume resuscitation
Intracardiac shunt
Aortic dissection
Most important cause of post-op LV failure is inadequate myocardial protection
If Unable to Separate From CPB…Check:Ventilator O2 sat’n, Exhaled CO2
ABGLytes, CBCSGCO, PAP, Wedge (ie. Adequate filling pressures)
EchoCardiac contractilityValvular functionShunt
ECG
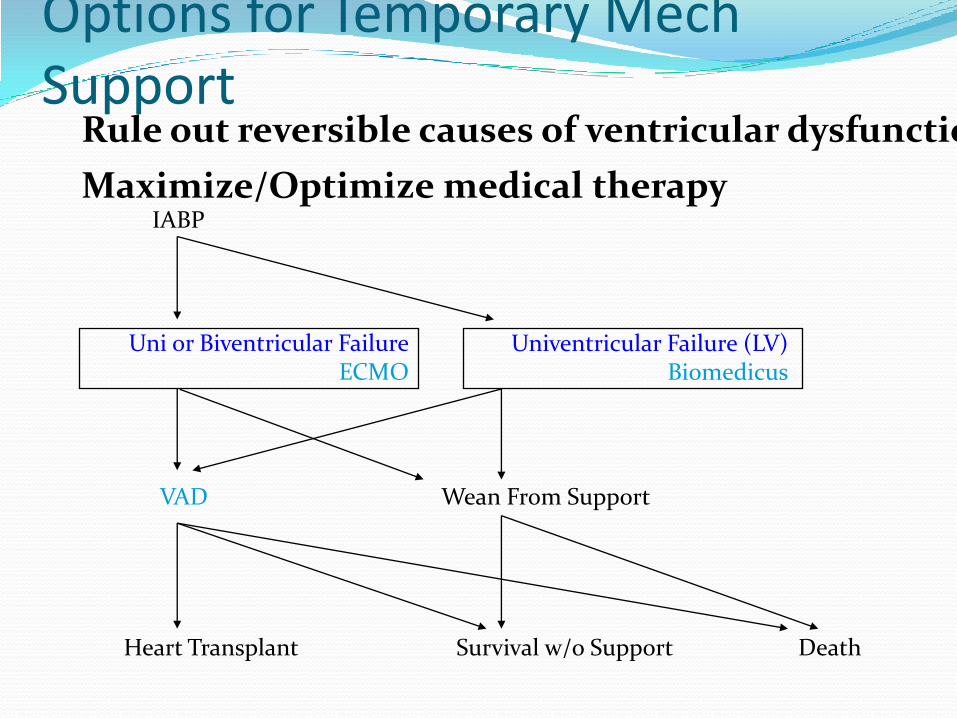
Options for Temporary MechSupport
IABP
Uni or Biventricular FailureECMO
Univentricular Failure (LV)Biomedicus
VAD
Heart Transplant
Wean From Support
DeathSurvival w/o Support
Rule out reversible causes of ventricular dysfunction
Maximize/Optimize medical therapy
IndicationsNote that there is no absolute indication for temporary mechanical support
Rather, based on a clinical assessmentCI < 2.0
SBP < 90
PCWP > 20 (ie. Low CO despite adequate fill)
Evidence of poor tissue perfusion
Oliguria
Acidosis
Low SVO2 (< 50)Refractory ventricular arrhythmias
Note that patients may have low C.O. due to excessive peripheral vasoconstriction (for a weakened heart)
Thus making a peripheral vasodilator very useful in this situation
Eg. Milrinone
Establish a rhythm – sinus, otherwise A/A-V paced if possible, or VVI (last)
%25–10 by C.O.Loss of sinus rhythm can
Especially in LVH or diastolic dysfx
Aim for rate 90 - 100
Finally, ensure sufficient medical support:
Epi ≥ 10 g/min
Dobutamine and Dopamine ≥ 10 g/kg/min
Milrinone ≥ 0.5 g/kg/min
After a 50 g/kg bolus
Inhaled NO if pulmonary hypertension
IABP: IndicationsPre-operative uncontrolled ischemic pain
Pre-operative uncontrolled ischemia
Pre-operative critical left main + RCA disease Especially if ongoing ischemia and/or poor LV function
Or ventricular arrhythmias
Pre-operative severe MR or VSR with CHF
Post-operative failure to wean or low CO syndrome
IABPEffects:
Reduction of afterload
Increased C.O. by up to 25%
Reduces wall stress (which is directly related to peak systolic wall stress) and therefore reduces oxygen consumption
Augmentation of diastolic pressure, with augmented coronary perfusion

IABPTip of balloon should be just distal to L subclavian ACan check position with TEE
Balloons usually in 2 sizes30 – 40 cc is optimal in most adults
Timing is criticalBy ECGDeflation on the R wave (just before aortic valve opens)
By arterial pressure tracingInflate at the dicrotic notch (ie. With closure of aortic valve
Early inflation causes…
Decreased C.O. (stroke volume)
Increased afterload
VERY important to have a regular rhythm, therefore pacing may be necessary
Heparinize if in longer than 24 hours
Wean by turning down from 1:1 to 3:1 augmentation (then off)
Pressure on femoral A x 30-45 minutes
To OR if puncture above inguinal ligament



IABP: ContraindicationsSevere Aortic regurgitation
Calcification or significant atheroma or aneurysm of descending thoracic aorta
Dissection of descending aorta
Severe peripheral vascular disease
AAA

Complications (~ 20% incidence)
Related to insertion
Lower limb ischemia (Most common, up to 25%)
BleedingDon’t forget possible iliac injury/retroperitoneal bleed
Arterial dissection
Thromboembolism if diseased aorta
Infection (1%)
Occlusion of major branches (renal, mesenteric)
Related to removalFalse aneurysm (1-2%)
Thromboembolism to lower limb
Related to deviceBalloon rupture (< 2%)
See blood in the catheter, ± lack of augmentation
Deflate balloon immediately and remove (b/c of thrombus risk)
A guidewire should be placed through the existing balloon to allow placement of a new one over it!
Disadvantages
Can only expect up to 25% increase in C.O.
Patient is immobilized
No improvement in RV function
ECMO
ECMO Extra-corporeal Membrane Oxygenation
ECLS (Extra-corporeal life support)
Initially developed for treatment of respiratory failure (veno-venous)
Useful also for uni or biventricular failure
Is the most commonly used form of ventricular support in neonates and infants
Is the first-line for ventricular support after IABP

Typically used for 48 – 72 hours, then either try to wean or move on to more permanent solution (LVAD, Transplant)Can perform hemofiltration at the same timeThermodilution C.O. is inaccurate on ECMO but SVO2 can be used insteadAim for 75 – 80%
ECMO for Respiratory FailureIndications
PaO2:FiO2 < 100
A-a gradient > 500
pH < 7.0 due to high pCO2
Eg. Status asthmaticus, airway obstruction
For lung transplant:
Usually only effective for early (ie. Within 1st week of transplant) graft failure

ECMO: ApplicationsAcute cardiogenic shock (either RV or LV)
Cath lab emergencies and support during complex catheter-based procedures
PE with RV failure and shock
Bridge to recovery/LVAD/transplant in acute myocarditis
In RV or Biventricular failure, ECMO is beneficial because of elimination of hypoxia, which then causes a decrease in PVR (also unloads RV)
ECMO: componentsPumpUsually rotary or roller
OxygenatorCan be membrane
Hollow-fibre has advantage of being quick to prime, and can be heparin-coated
Heater/cooler
Cannulas and tubing (± percutaneous)Arterial 16 – 20Fr
Venous 18 – 28Fr
Entire system can be heparin-coated
ECMO: anticoagulationOverall risk of intracardiac thrombus formation withoutheparinization is ~20%
Risk of pumphead thrombus formation is 5 - 10%
For arterio-venous ECMO, aim for ACT of 180 – 200
-venois not as important for heparinizationSystemic ECMOvenous
ACT 160 – 200 if prolonged support
ECMO: Arterio-venousCannulation options:
RAA to Asc Ao
Femoral vein (catheter to RA) to Asc Ao
Femoral vein to Femoral artery
Can be done percutaneously
If intra-thoracic cannulation, tunnel catheters through skin like chest tubes
Unloads RV, and decreases preload to LV
ECMO: Veno-venousCannulation options:Outflow from R int jug, inflow to a common femoral vein (classic, “atriofemoral”)
Femoro-atrial recently shown to be better
Bilateral common femoral veins
May need ASD to allow decompression of right side (to bypass lungs if excessively high PAP or RV dysfunction initially – should improve with reversal of hypoxia, acidosis) – eg. PECan be done with percutaneous balloon septostomy if necessary

ECMO: ComplicationsArterial and venous tears, dissections, hemotomas, false aneurysms
Bleeding
Re-op for bleeding in up to 60%!
Higher incidence if thoracic (central) cannulation
Thrombosis of lines, oxygenator, pump
Emboli
Cerebral emboli in up to 10%
Renal dysfunction in up to 1/3rd !
Can add CVVHD to the circuit if needed
Lower limb ischemia
Infection (mediastinitis)
ECMO: WeaningReadiness for weaning may be indicated by:
Increasing wave-form on arterial line
Improved function on echo
Weaning should be echo-guided
Decrease flows, increase inotropes, and increase ventilation as necessary
Keep ACT > 300 while pump flows are less than 2L/min
ECMO: Results~75% are successfully weaned from ECMO
However, survival to hospital discharge is usually about 30 – 50%
Higher if pt eventually gets a VAD or Tx
Much lower if emergency surgery
ECMO allows screening of pts for VAD and Tx candidacy

ECMO: ContraindicationsIncurable malignancy
Advanced MOF
Severe CNS injury
Relative c/i is pt who is not VAD or Tx candidate

Biomedicus

Biomedicus = ECMO w/o oxygenatorThis is one example of rotary pump used to provide unior biventricular support for a period of hours to days
One pump for either L or R ventricular support, two pumps for both
Cannulation for L heart
R sup pulm vein to asc Ao
Cannulation for R heart
RA to PA (either direct, or via RV puncture and threading of catheter into main PA)
Thank You