sleep disorders are common sleep disorders are serious sleep disorders are treatable
DESCRIPTION
Important facts ___________________________. Sleep disorders are common Sleep disorders are serious Sleep disorders are treatable Sleep disorders are under diagnosed. Important facts ___________________________. - PowerPoint PPT PresentationTRANSCRIPT

1

2
• Sleep disorders are common
• Sleep disorders are serious
• Sleep disorders are treatable
• Sleep disorders are under diagnosed
Important facts___________________________

• Sleep complaints are usually not due to
psychiatric conditions or character flaws
• Most sleep disorders are readily
diagnosable and treatable
• The studies include– Polysomnography (PSG)
– Multiple sleep latency test (MSLT)
– Actigraphy
3
Important facts___________________________
4
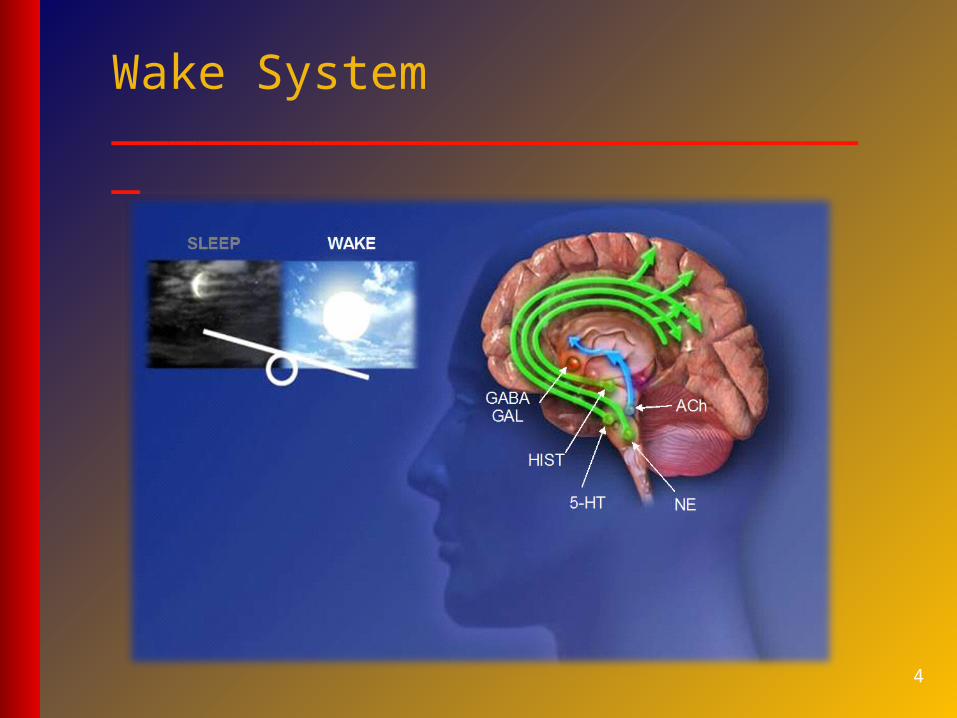
Wake System___________________________

5
Sleep System___________________________
6
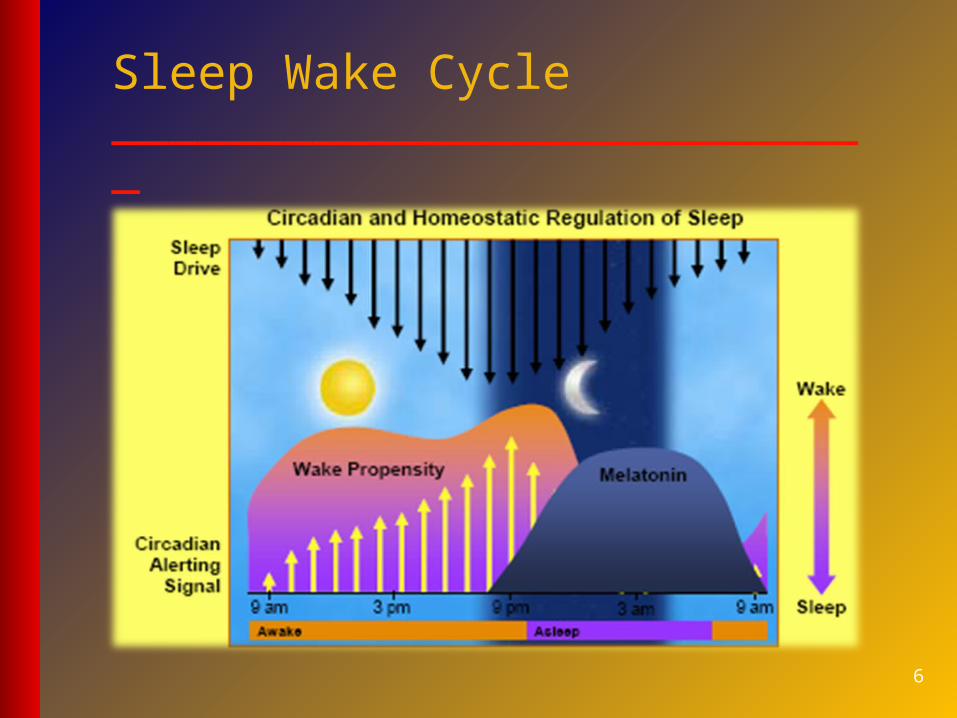
Sleep Wake Cycle___________________________
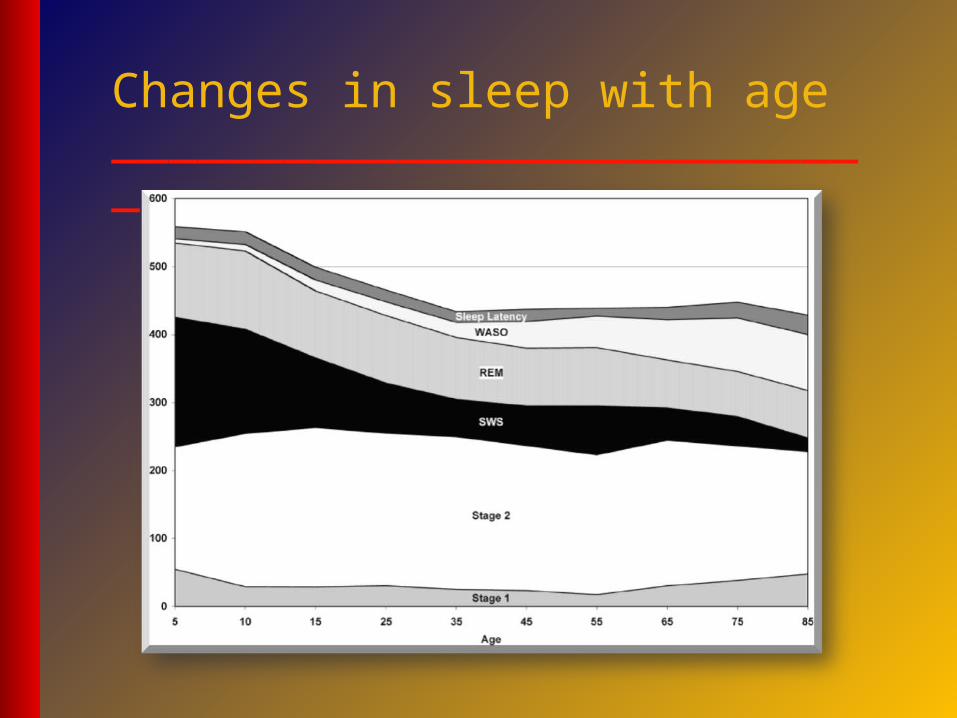
Changes in sleep with age___________________________
8
Stages of sleep___________________________
1. NREM Sleep
A. Stage 1
B. Stage 2
C. Stage 3
D. Stage 4
2. REM Sleep
9
REM Sleep~20% of night
NREM Sleep~80% of night
Wake2/3 of life
Sleep Stages ___________________________

10
Sleep disorders (ICSD 2) ___________________________
1. Insomnia.
2. Sleep Related Breathing Disorders.
3. Hypersomnia.
4. Cicadian Rhythm Sleep Disorder.
5. Parasomnia.
6. Sleep related Movement Disorder.
• Insomnia and excessive daytime sleepiness
are primary complaints regardless of the
stage of the disease
• Insomnia includes difficulty falling asleep,
difficulty staying asleep, and early morning
awakening
Insomnia - definition___________________________
• Insomnia is not defined by the number of
hours of sleep, but rather, by an individual‘s
ability to sleep long enough to feel healthy
and alert during the day.
• The normal requirement for sleep ranges between 4 and 10 hours
• Insomnia is a symptom, not a disorder by itself
Insomnia - definition___________________________
• Determine the pattern of sleep problem (frequency, associated events, how long it takes to go to sleep, and how long the patient can stay asleep)
• Include a full history of alcohol and caffeine intake and other factors that might affect sleep
• Review current medications that patient is taking to eliminate these as possible causes
• Take a history to rule out physical cause and/or psychosocial cause
Insomnia - assessment___________________________
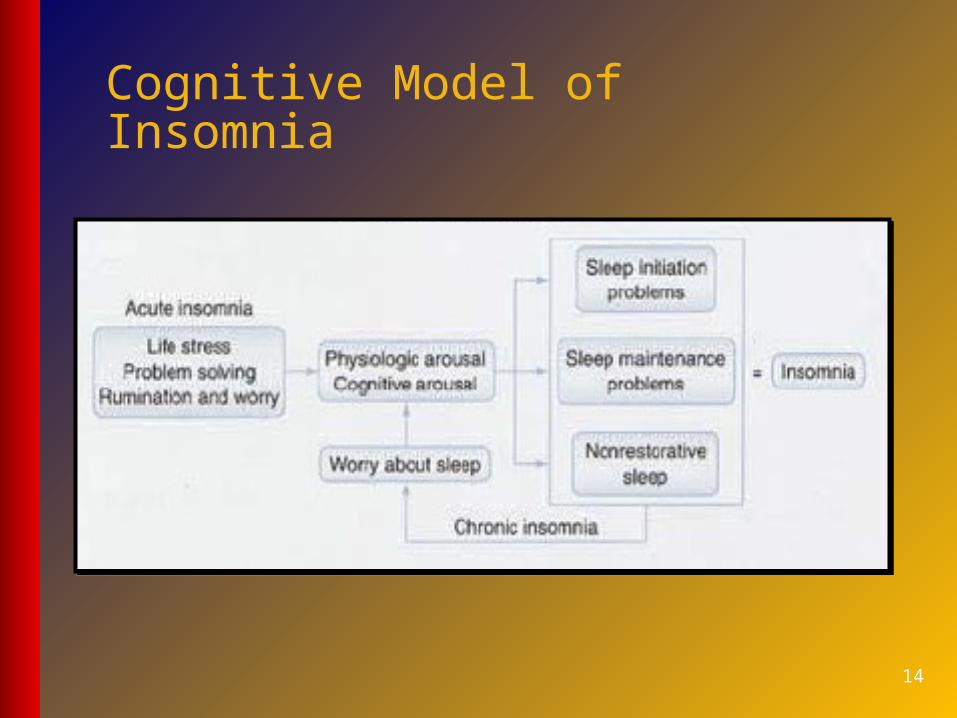
Cognitive Model of Insomnia
14
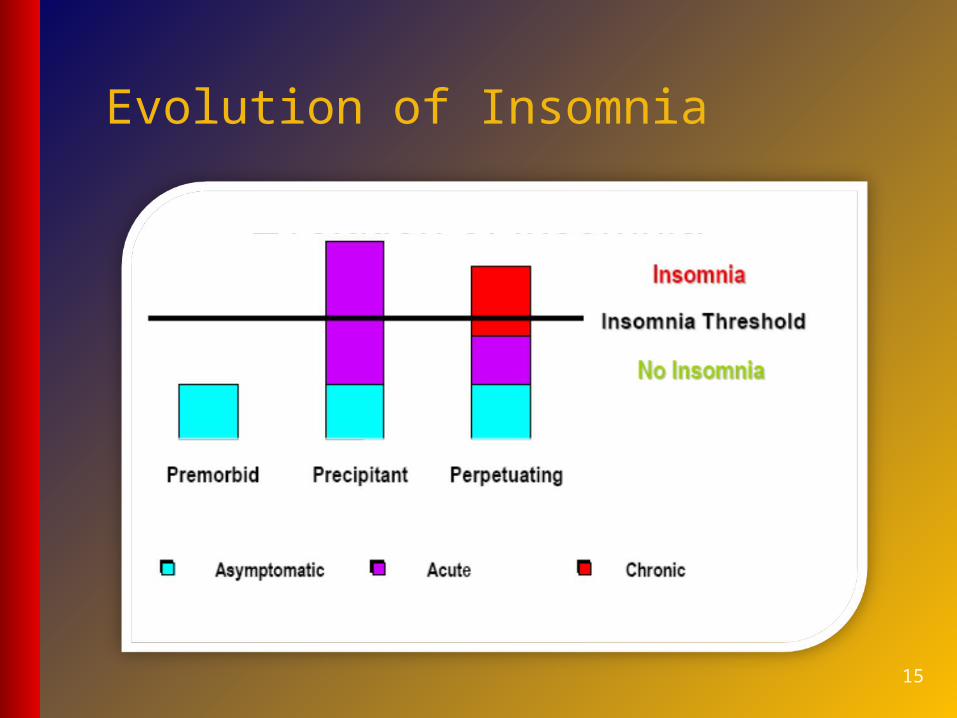
Evolution of Insomnia
15
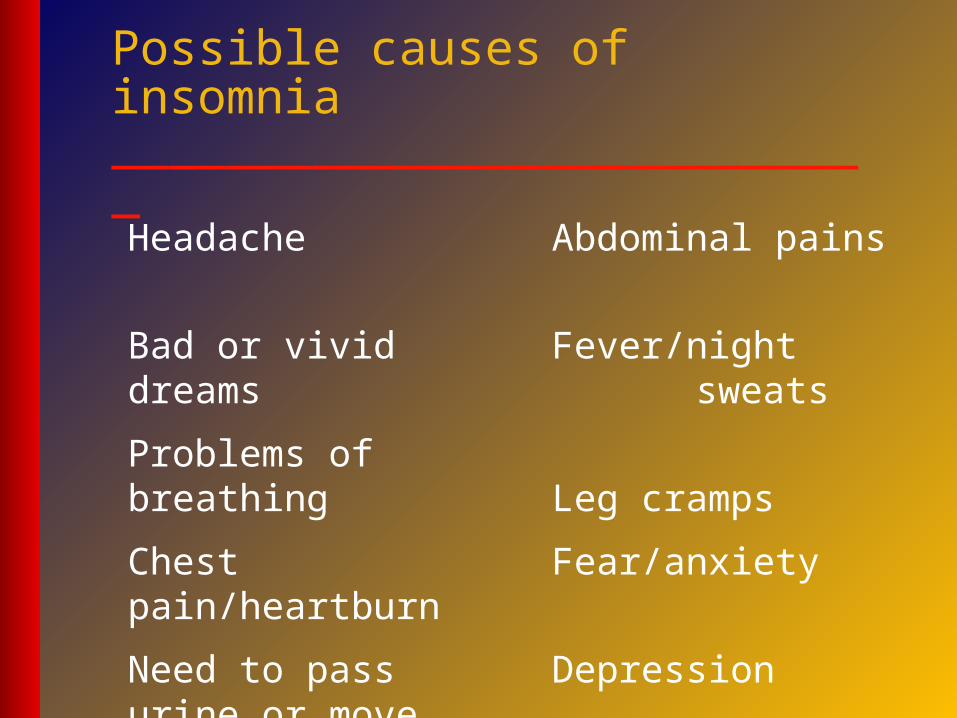
Headache
Bad or vivid dreams
Problems of breathing
Chest pain/heartburn
Need to pass urine or move bowels
Abdominal pains
Fever/night sweats
Leg cramps
Fear/anxiety
Depression
Possible causes of insomnia___________________________
17
Insomnia___________________________
1. A complaint of difficulty in initiating, maintaining or waking up too early or sleep that is non-restorative or poor in quality.
2. The above sleep difficulty occurs despite adequate opportunity and circumstance for sleep.
3. Insomnia is a symptom – not a disease per se

18
Insomnia – associated features___________________________
At least one (or more) of the following
• Fatigue or malaise
• Attention, concentration impairment
• Social/ vocational dysfunction/ poor work
• Mood disturbance or irritability
• Daytime sleepiness
19
Insomnia – resultant problems___________________________
• Reduction in motivation, energy or initiative
• Proneness for errors or accidents at work or while driving
• Tension, headaches or gastrointestinal symptoms in response to sleep loss
• Concerns or worries about sleep
• Secondary psychiatric problems

• Sleep onset insomnia
• Sleep maintenance insomnia
• Sleep offset insomnia
• Non restorative sleep
21
Insomnia - subdivisions___________________________
Types of insomnia________________________
• Transient insomnia– < 4 weeks triggered by excitement or stress,
occurs when away from home
• Short-term– 4 wks to 6 mons , ongoing stress at home or
work, medical problems, psychiatric illness
• Chronic– Poor sleep every night or most nights for > 6
months, psychological factors (prevalence 9%)

23
Medical problems__________________________• Depression
• Hyperthyroidism
• Arthritis, chronic pain
• Benign prostatic hypertrophy
• Headaches; Sleep apnoea
• Periodic leg movement,
• Restless leg syndrome (RLS)
24
Other problems__________________________
• Caffeine
• Nicotine
• Alcohol
• Exercise
• Noise
• Light
• Hunger
25
Management of insomnia____________________________
• Good Sleep History
• Rule out primary psychiatric disorders
• Rule out adverse effects of medications
• Sleep Diary
• Good Sleep Hygiene Measures
• Interventions – CB therapy, medications
• Treat underlying causes whenever possible
• Advise patient to avoid exercise, heavy meals, alcohol, or conflict situations just before bed
• Plain aspirin or paracetamol in low doses may be helpful; or give short-acting hypnotics or a sedative
• Treat underlying depression
Management of insomnia___________________________
• Treat underlying Medical Condition
• Treat underlying Psychiatric Condition
• Improve sleep hygiene
• Change environment
• CBT: ‘primary insomnias’, transient insomnia
• Pharmacological
• Light, melatonin, or ‘chronotherapy’ for circadian disorders
Management of insomnia___________________________

Type of medication Example
CNS stimulants D-amphetamine, Methyphenindrate
Blood pressure drugs - blockers, - blockers
Respiratory medicines Albuterol, Theophylline
Decongestants Phenylephine, Pseudoephedrine
Hormones Thyroxin, Corticosteroids
Other substances Alcohol, Nocotine, Caffeine28
Medications and insomnia___________________________

29
Cognitive Behaviour Therapy (CBT)____________________________
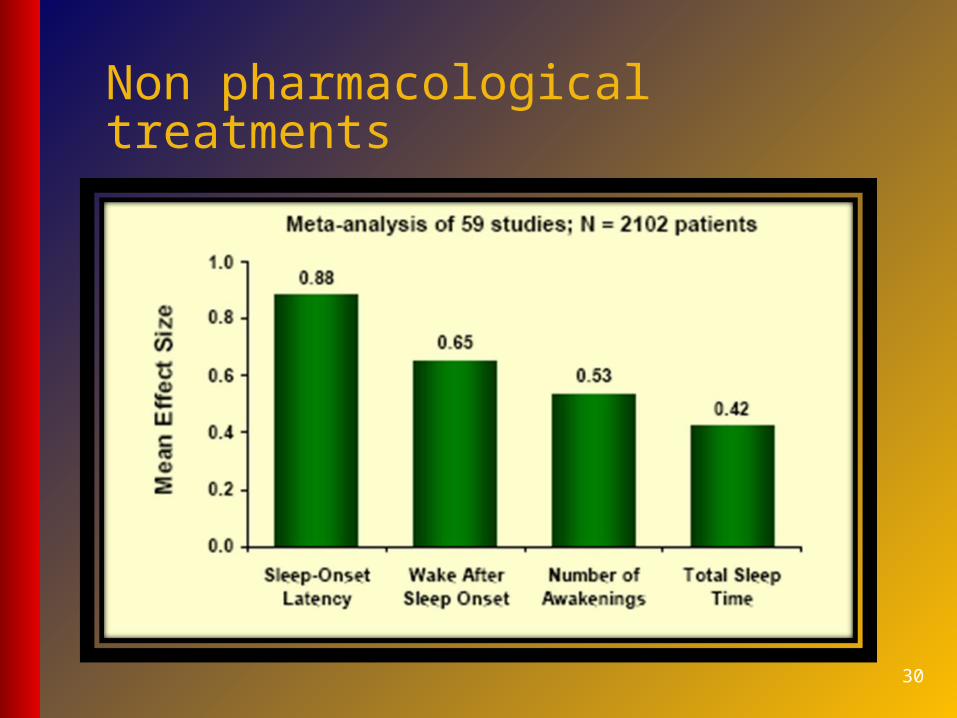
Non pharmacological treatments
30
31
Bed room__________________________• Temperature
• Fresh air
• S&S
• Comfortable bed
32
Stimulus control__________________________• Go to bed when sleepy
• Only S & S in bedroom
• Get up the same time every morning
• Get up when sleep onset does not occur in 20 min, and go to another room
• No daytime napping

33
Sleep hygiene__________________________• Behaviours that interfere with sleep
• Caffeine
• Alcohol
• Nicotine
• Daytime napping
• Exercise < 4hrs before bed
34
Relaxation training__________________________• Progressive muscle relaxation
• Diaphragmatic breathing
• Autogenic training
• Biofeedback
• Meditation, Yoga
• Hypnosis to ↓ anxiety & tension at bedtime
35
Thought stopping__________________________
• Interrupt unwanted pre-sleep cognitive
activity by instructing patient to repeat
sub-vocally ‘the’ every 3 sec
(articulatory suppression)
• To yell sub-vocally “stop”
(thought stopping)

36
Behavioural therapies__________________________
• Explicit instruction to stay awake when they go to bed;
Aim is to reduce anxiety associated with trying to fall
asleep – Paradoxical intention
• Alter irrational beliefs about sleep, provide accurate
information that counteracts false beliefs – Cognitive
restructuring
• Patient imagines 6 common objects (candle, kite, fruit,
hourglass, blackboard, light bulb) emphasis on
imagining shape, colour, texture – Imagery training
• Benzodiazepines– Lorazepam
– Clonezepam
– Temazepam
– Flurazepam
– Quazepam
– Alprazolam
– Triazolam
– Estazolam
• Non Benzodiazepines– Zolpidem
– Zolpidem CR
– Zeleplon
– Eszopiclone
• Both these classes act on the GABAA receptors (BzRA) in PCN
37
Benzodiazepine receptor agonists__________________________
• Antidepressants– Trazadone
– Mirtazapine
– Doxepin
– Amitryptyline
• Antipsychotics– Olanzapine
– Quitiepine
• Melatonin Receptor Agonists– Melatonin
– Ramelteon
• Miscellaneous– Valerian
– Diphenhydramine
– Cyclobenzaprine
– Hydroxyzine
– Alcohol38
Other classes of medications__________________________

• Anterograde amnesia
• Residual sedation – longer acting BzRAs
• Rebound Insomnia?
• Abuse and dependence?
– Mostly used short term (2 weeks)
– When used as a sleeping aid dose escalation rare
– No physical dependence with night time use
– Low psychological dependence with night time use
• Increased fall risk, cognitive effects in the elderly
BzRAs – side effects and safety__________________________

40
• Benzodiazepines (GABA receptor agonist)
• Transient insomnia, (max 2 wks, ideally 2-3/wk)
– Long ½ life - nitrazepam
– Medium ½ life - temazepam
– Short ½ life - diazepam
– Poor functional day time status, cognitive impairment, daytime sleepiness, falls and accidents, depression
– Acute withdrawal, confusion, psychosis, fits - may occur up to 3/52 from stopping
Benzodiazepines____________________________
• Benzodiazepines are the drugs of choice for the
treatment of insomnia.
• Flurazepam can be used for up to one month
with little tolerance.
• Temazepam can be used for up to three months
with little tolerance.
• Intermittent use recommended (every three
days). Use for no longer than 3 – 6 months.
Benzodiazepine use____________________________
• Half-life is an important factor
• Benzodiazepines with long half lives (e.g., flurazepam) produce sustained sleep, but increased risk of daytime somnolence
• Benzodiazepines with short half lives may be best for patients with difficulty falling asleep, but can produce rebound insomnia
• Development of tolerance can produce rebound insomnia in compounds with short half lives
Benzodiazepine use____________________________

• Benzodiazepines have relatively low
abuse potential.
• Prolonged use can lead to withdrawal
symptoms: headache, irritability,
dizziness, abnormal sleep
• Rebound insomnia - triazolam
Benzodiazepine abuse____________________________

• Low toxicity when taken alone
• In combination can be fatal
• Flumanzenil is a benzodiazepine antagonist that can be used to block adverse effects of benzodiazepines
• Stomach pump, charcoal, hemodialysis
Benzodiazepine toxicity____________________________
45
• Act at the benzodiazepine receptor
• Less risk of dependence
• Zaleplon short ½ life
• Zolipidem, Zopiclone slightly longer ½ life
• No difference in effectiveness & safety
• More expensive
• Only to be used if adverse effects to BZP
Non benzodiazepines____________________________
• Short half life
• Does not produce rebound insomnia
• Low abuse potential
• Less likely to produce withdrawal symptoms
• Rebound insomnia after first night of withdrawal, but soon resolves
Zolpidem____________________________
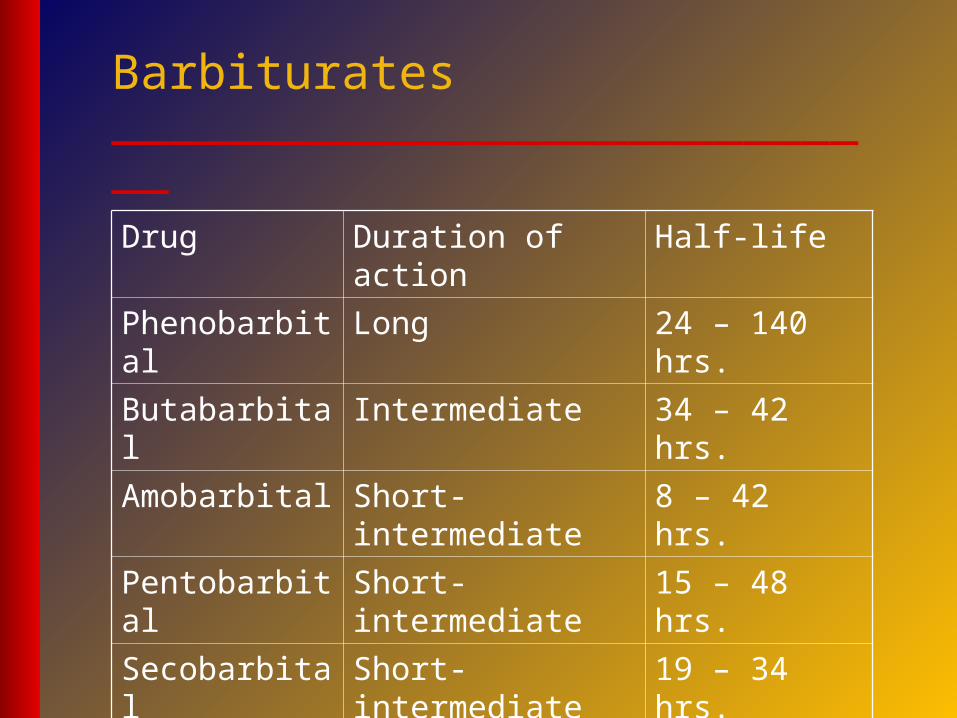
Drug Duration of action Half-life
Phenobarbital Long 24 – 140 hrs.
Butabarbital Intermediate 34 – 42 hrs.
Amobarbital Short-intermediate 8 – 42 hrs.
Pentobarbital Short-intermediate 15 – 48 hrs.
Secobarbital Short-intermediate 19 – 34 hrs.
Barbiturates____________________________
50
• TCA - Amitriptyline, if depression also an issue
• Antihistamines – Promethazine
• Melatonin
– Hormone secreted by pineal gland, effects circadian rhythm, synthesised at night
– Use to counteract jet lag (2-5mg @ bedtime for Four nights after arrival);
– Synthetic analogue of malatonin - Remelteon
– Used in paediatric sleep disorders
Other drugs____________________________
52
Hypersomnia___________________________
1. Narcolepsy with Cataplexy
2. Narcolepsy without Cataplexy
3. Narcolepsy due to Medical Condition
4. Idiopathic Hypersomnia with Long Sleep Time
5. Idiopathic Hypersomnia without Long Sl. Time
6. Behaviorally Induced Insufficient Sleep Syn
7. Hypersomnia due to Medical Condition
8. Hypersomnia due to Drug/ Substance
53
Sleep related movement disorders____________________________
1. Restless Leg Syndrome
2. Periodic Limb Movement Disorder
3. Sleep Related Leg Cramps
4. Sleep Related Bruxism
THANK YOU ALL
HAVE GOOD SLEEP
54