sleep-disordered breathing in pregnancy conference/obrien... · pamidi 2014. recent multicenter ......
TRANSCRIPT

Sleep-Disordered Breathing in Pregnancy
Louise M. O’Brien, Ph.D., M.S.
Associate Professor
Sleep Disorders Center & Department of Obstetrics & Gynecology
Michigan Medicine

Conflict of Interest Disclosures for Speakers
1. I do not have any relationships with any entities producing, marketing, re-selling, or
distributing health care goods or services consumed by, or used on, patients, OR
2. I have the following relationships with entities producing, marketing, re-selling, or
distributing health care goods or services consumed by, or used on, patients:
Type of Potential Conflict Details of Potential Conflict
Grant/Research Support Phillips Respironics Inc., ResMed
Consultant
Speakers’ Bureaus
Financial support
Other
3. The material presented in this lecture has no relationship with any of these potential conflicts, OR
4. This talk presents material that is related to one or more of these potential conflicts, and the following
objective references are provided as support for this lecture:
1. Poyares et al. Pre-eclampsia and nasal CPAP: part 2. Hypertension during pregnancy, chronic snoring, and
early nasal CPAP intervention. Sleep Med. 2007 Dec;9(1):15-21. Epub 2007 Jul 20
2. Blyton DM, Sullivan CE, Edwards N. Reduced nocturnal cardiac output associated with preeclampsia is
minimized with the use of nocturnal nasal CPAP.Sleep. 2004 Feb 1;27(1):79-84
3. Blyton DM, Skilton MR, Edwards N, Hennessy A, Celermajer DS, Sullivan CE. Treatment of sleep disordered
breathing reverses low fetal activity levels in preeclampsia. Sleep 2013 Jan 1;36(1):15-2
X
X

Sleep-Disordered Breathing
What do we know about SDB in pregnancy?
• Habitual snoring affects 5-10% of non-pregnant women but up to 35% of
pregnant women (Redline et al 1994, Bixler et al 2001, Bourjeily 2010, O’Brien 2012)
• In women with pre-eclampsia, up to 85% have habitual snoring
(Izci 2005, Izci2006,Reid 2011, O’Brien 2014)
• OSA affects 3% of nullips in early pregnancy and 8% by mid-pregnancy
(Facco et al 2017)
• OSA present in about 15% of obese women in early pregnancy
(Louis et al 2013)
• OSA present in about 50% of women with pre-eclampsia
(Reid 2011, O’Brien 2014)

Evidence suggests strong link between SDB and hypertension in pregnancy
• 1st case description of SDB and pre-eclampsia in 1996 (Lefcourt & Rodis 1996)
• 1st study suggesting link between SDB and hypertension during pregnancy in 2000 (Franklin et al 2000)
Pamidi 2014

Recent multicenter trial of approx n=3000 nulliparous women found aOR of 1.94 (95% CI 1.07–3.51) for pre-eclampsia in women with OSA
(Facco et al 2017)

Timing of Snoring and Maternal Hypertension
O’Brien 2012
BUT
New pregnancy-onsetsnoring was independently associated with gestational hypertension AND pre-eclampsia:OR 2.4[1.5-3.8] GHTNOR 1.6 [1.1-2.6] preE
0
5
10
15
20
25**
**p<0.001 vs. controls
Compared to non snoring controls, chronic habitual snoring was not independently associated with gestational hypertension or pre-eclampsia

• N=51 pregnant women with hypertension unselected for sleep problems
• Mean gestation 27±7 weeks
• 41% African American
• 78% obese
• 61% reported habitual snoring (snoring ≥3 nights/wk)
OSA in Hypertensive Pregnancies
O’Brien 2014
Baseline PSG results:
- Mean AHI=13.5 (range 0.1-117.2)
- 80% of women had AHI≥1
- 41% had AHI≥5
- 16% had AHI≥15
- 12% had AHI≥30
Pooled relative risk for OSA in hypertensive women who
snored, vs. non-snoring hypertensives, was 2.0 (1.4-2.8)
OSA

Is snoring a good marker for OSA?
O’Brien et al unpublished

Pamidi 2016
Is snoring a good marker for OSA?
O’Brien et al unpublished
There are no validated screening tools for OSA in pregnant women: however we currently have an on-
going study that will develop one…..watch this space
Can we use a screening tool to identify OSA risk?
Berlin Questionnaire
STOP-BANG

Data from n=21 women with BMI≥40:
- BMI≥40, 67% have OSA. Odds ratio for OSA is 5.3 (1.9-14.8)
- BMI≥40 AND habitual snoring, 81% have OSA. Odds ratio for
OSA is 8.7 (2.6-29.2)
- BMI≥40 AND hypertension, 81% have OSA.
Odds ratio for OSA is 3.1 (1.1-9.0) regardless of whether
snoring present or notO’Brien unpublished
What about obesity?
15%-25% of pregnant women with a BMI ≥30 have OSA
(Louis 2013, Facco 2017)
Obesity is complicated:
E.g. when looking at SDB and hypertension, maybe we should not
just “adjust” for BMI in a regression model
Take a step back and review the bigger picture because SDB may
be only part of pathway to HTN and obesity is playing a big role.
We hypothesized that frequent snoring mediates the association of pre-pregnancy BMI and GHTN
New methods in mediation analysis allow us to look at the total
effect of obesity on HTN which has two components;
1) direct effect
2) indirect effect via SDB
Important to only include incident SDB and
incident HTN as this analysis is causal mediation
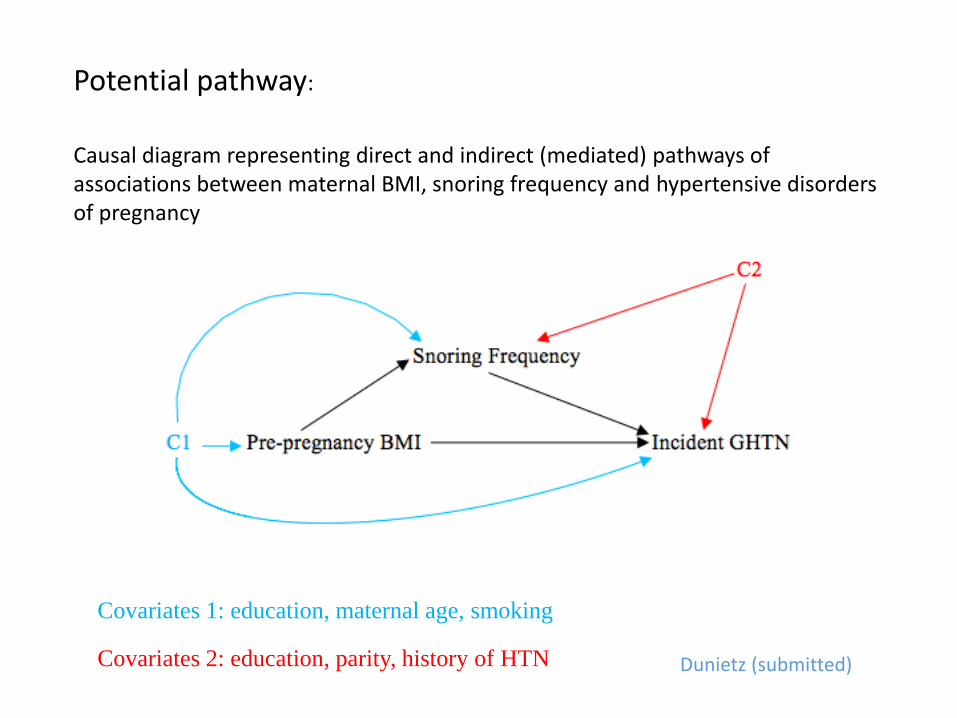
Covariates 1: education, maternal age, smoking
Covariates 2: education, parity, history of HTN
Potential pathway:
Causal diagram representing direct and indirect (mediated) pathways of associations between maternal BMI, snoring frequency and hypertensive disorders of pregnancy
Dunietz (submitted)
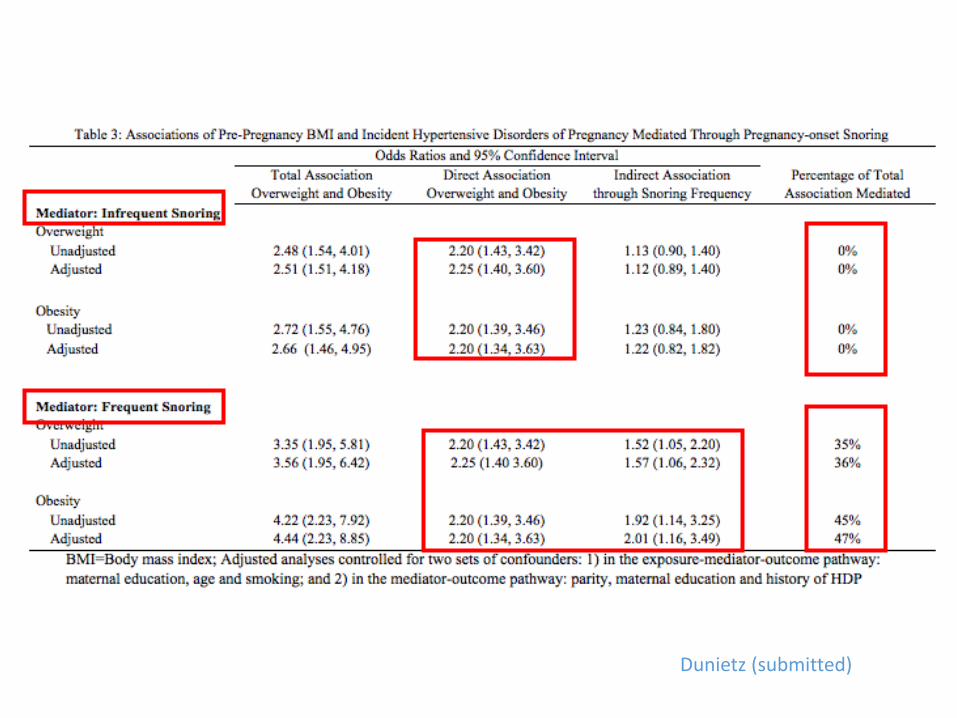
Dunietz (submitted)

Message:
• Frequent pregnancy-onset snoring plays an indirect role in the association of pre-pregnancy BMI and hypertensive disorders of pregnancy
• It explains about;• one third of the total association between maternal BMI and hypertensive
disorders of pregnancy in women who were overweight at the start of their pregnancy, and
• almost half of the total association between maternal BMI and hypertensive disorders of pregnancy in women who were obese.
This approach accounts for the temporal aspect of these associations
Dunietz (submitted)

SDB is associated with metabolic dysregulation
What about Gestational Diabetes?
Shaw et al 2008

Luque-Fernandez, 2013
Meta-analysis of 9,795 participants enrolled in epidemiological
observational studies for SDB and GDM
Recent multicenter trial of approx n=3000 nulliparous women found aOR of 3.5 (95% CI 1.95–6.19) for gestational diabetes in women with OSA
(Facco et al 2017)

Does Maternal SDB Impact the Fetus?

SDB
Fetal growth restriction
Vasoconstriction O2
desats
Hypertension
Reduced placental delivery Maternal hypoxia assoc. to fetus with fetal movements
and bradycardia
Maternal SDB and IUGR…..logical?

Brief exposures to hypoxia in late pregnancy associated with reduced birth weight in rats
(Schwartz et al 1998)
In animal models exposure to hypoxia during gestation associated with stunted fetal growth
(Gozal et al 2003)
Maternal SDB and IUGR…..logical?

(Franklin et al 2000)
SDB and Fetal Growth
Joel-Cohen & Schoenfeld 1978

O’Brien 2013
Chronic habitual snoring: smaller babies
Witnessed apnea: bigger babies
Reported Symptoms

Pamidi 2016
Polysomnography

Bin 2016
Epidemiological studies of OSA Dx


Uterine environment: Metabolic dysregulation
High blood pressure: Vasoconstriction

Subjective Measures of SDBStudy Predictor Design
Odds Ratio
OR (95%CI)
Study
OR (95%CI)
Fig2
Warland (under review)
Objective Measures of SDB

SDB and Fetal Growth
(Fung et al 2013)
OSA (n=14) Control (n=27)
Serial measures of fetal growth in n=54 controls, n=34 untreated OSA, n=14 treated OSA: - Fetal growth problems defined as birth weight <10th centile, or a slowing of fetal
growth by >30% during the last trimester. - In a logistic regression model, after accounting for co-morbid hypertension, diabetes,
anti-hypertensive and anti-diabetic medications, maternal age, and smoking, untreated OSA was associated with a 3-fold increased odds of fetal growth problems (OR 3.0, 95%CI 1.1-8.3, p=0.03).
- There were no differences in fetal growth trajectories between non-OSA and treated OSA (Kneitel, Treadwell & O’Brien under review)

What about preterm birth?

Subjective Measures of SDBStudy Predictor Design
Odds Ratio
OR (95%CI)
OR (95%CI)
Fig1
Objective Measures of SDB
Warland (under review)

SDB and Time to Delivery
Some studies suggest a relationship between sleep disturbance and preterm birth although many studies do not.
Delivery is typically measured as either preterm vs. full term OR mean gestational age. No study has yet used survival analysis to investigate this despite delivery being a “time to event”.
Recall: timing of snoring: chronic vs. pregnancy-onset
Now also consider intensity:- Non snoring controls
- Infrequent-quiet snorers- Frequent-quiet snorers- Frequent-loud snorers
Included non-hypertensive, non-diabetic women in order to estimate the impact of habitual snoring without these key confounders

SDB and Time to Delivery
In n=954 non-hypertensive, non-diabetic women, there was an increased hazard ratio for earlier delivery in chronic loud frequent snorers vs. controls: HR 1.60, (95% CI 1.04, 2.45)
These women delivered approximately 6 days earlier; 25% were considered “early term” (37+0 – 38+6 weeks) Dunietz (under review)
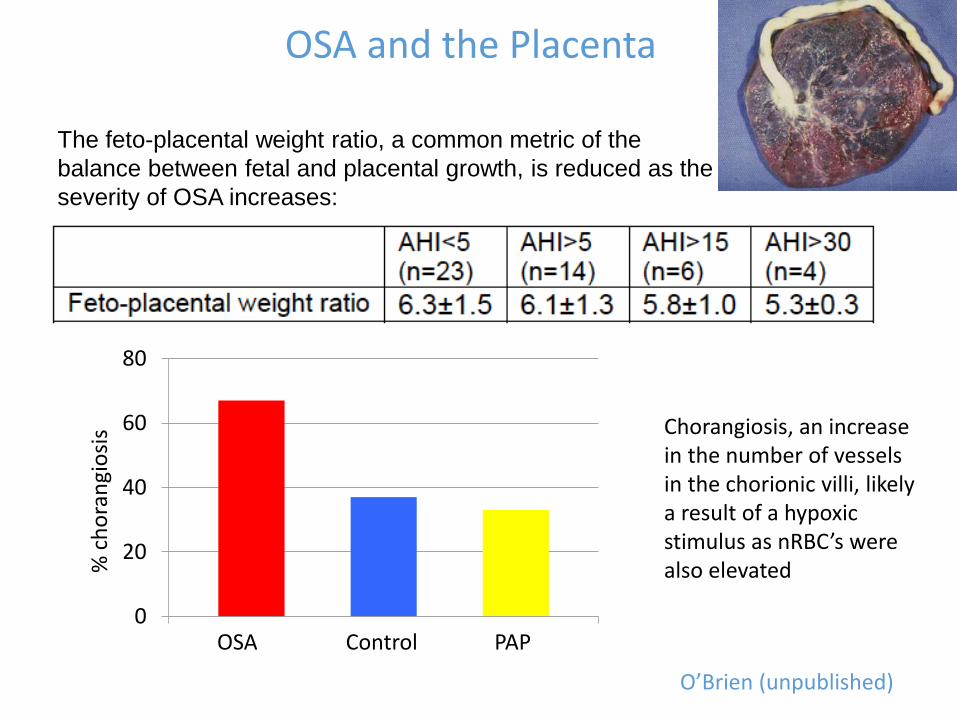
OSA and the Placenta
The feto-placental weight ratio, a common metric of the
balance between fetal and placental growth, is reduced as the
severity of OSA increases:
0
20
40
60
80
OSA Control PAP
% c
ho
ran
gio
sis Chorangiosis, an increase
in the number of vessels in the chorionic villi, likely a result of a hypoxic stimulus as nRBC’s were also elevated
O’Brien (unpublished)

Treatment of SDB in Pregnancy
Population Attributable Risk: If there is a causal relationship
between SDB and hypertensive disorders of pregnancy,
treating SDB could reduce hypertension in pregnancy by up
to 20%O’Brien 2012
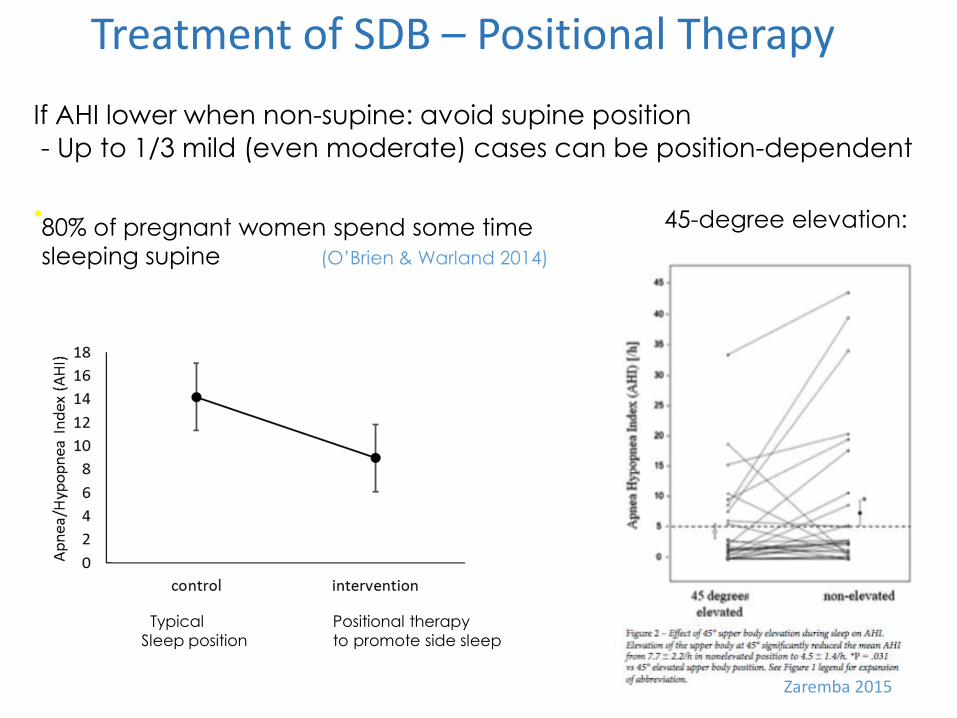
If AHI lower when non-supine: avoid supine position
- Up to 1/3 mild (even moderate) cases can be position-dependent
•
Treatment of SDB – Positional Therapy
Zaremba 2015
45-degree elevation:80% of pregnant women spend some time
sleeping supine (O’Brien & Warland 2014)
Typical Positional therapy
Sleep position to promote side sleep
Why is sleep position important in pregnancy?
Posture in late pregnancy can have a profound effect on maternal cardiovascular control

Supine Lateral
Gravid uterus compresses the inferior vena cava resulting in:venous returnejection fraction impaired uterine perfusioncardiac output
“Maternal supine hypotensive syndrome”
http://what-when-how.com/nursing/normal-pregnancy-maternal-and-newborn-nursing-part-4/


Supine sleep independently associated with stillbirth (OR, 8.0; 95% CI, 1.5–43.2).
Supine sleep independently associated with low birth weight (OR, 5.0; 95% CI, 1.2–20.2).
When low birth weight was added to the stillbirth model, the OR for the relationship between supine sleep and stillbirth was almost eliminated (OR, 4.9; 95% CI, 0.80–31.4)
Thus low birth weight appears to mediate the effects of supine sleep on stillbirth.
If supine sleep has a causative role in low birth weight and subsequently stillbirth, up to 17% of low birth weight, and consequently 26% of stillbirths, might be prevented by changing maternal
sleep position.
Risk is higher for term (aOR 10.26, 3.00–35.04) vs. preterm babies (aOR 3.12, 0.97–10.05)( McCowan 2017)

Supine non-supine
Supine sleep position is not good for fetal wellbeing:
In the supine position:
- fetal heart rate variability reduced
- Fetal behavior change from active to quiescence (low oxygen consuming state).
In the presence of a stressor (uteroplacental perfusion or hypoxia), shift to a low
oxygen consuming state would be a protective reaction.
Maternal supine position may be disadvantageous for fetal wellbeing and in
compromised pregnancies may be a sufficient stressor to contribute to fetal demise.
Warland (under review)
Stone 2016
Positional therapy isn’t always
sufficient…..

• First line treatment is PAP
• Meta-analyses of randomized studies representing over 1400 subjects show that PAP improves daytime and nocturnal BP.
(Bazzano et al 2007, Haentjens et al 2007)
Treatment of SDB with PAP
• Small studies suggest that BP may be reduced when PAP is used in pregnant women:
Sydney, Australia: Saskatoon, Canada
- Edwards et al 2000 n=11 - Reid et al 2013 n=13
- Blyton et al 2004 n=12
Stanford, USA:
- Guilleminault et al 2004 n=12
- Poyares et al 2007 n=7
- Guilleminault et al 2007 n=12
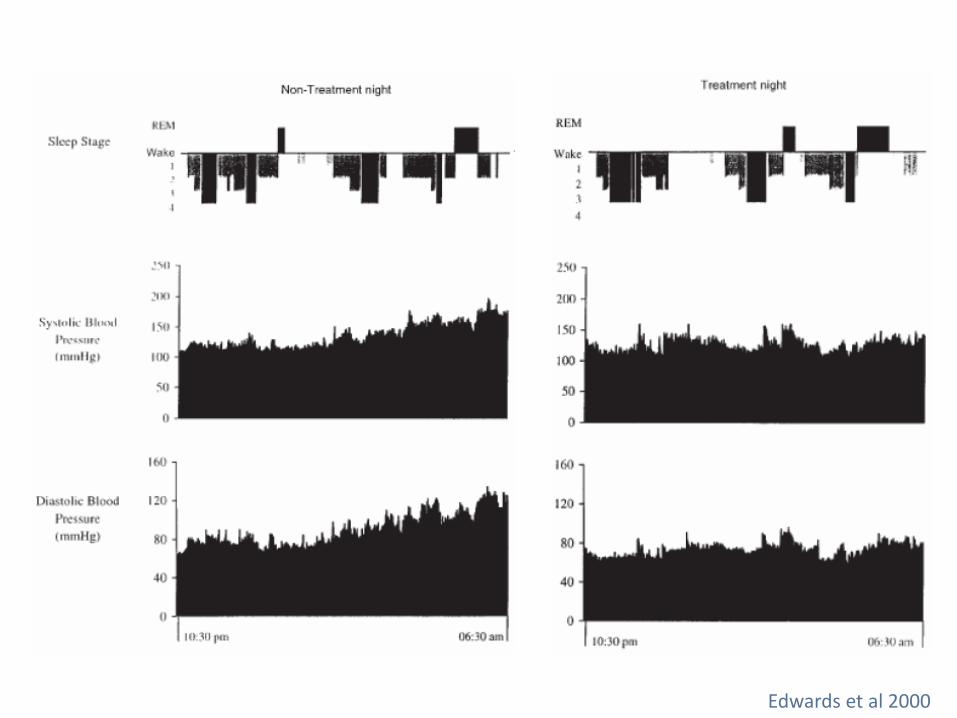
Edwards et al 2000

HTN, SDB and Fetal Movements
Edwards & Sullivan 2008
? Due to impaired cardiac output and increased peripheral vascular resistance
Uteroplacental hypoperfusion and fetal hypoxemia

Poyares et al 2008
Alpha-methyl dopadose increased in controls;
constant or decreased in CPAP
Auto-PAP in Pregnant Women with Hypertension
N=48 APAP and n=77 standard of care
• Mean gestation at enrollment: 28.1±7.2 weeks
• Mean PAP use 54 days: (range 5-144 days)
• Mean PAP pressure: 10cmH20 (range 5-18cmH2O)
• Remote monitoring of compliance data using web-based technology
Positive Airway Pressure (PAP) Therapy
O’Brien unpublished
70% of pregnant women were compliant users

Compliant Subject

Non-Compliant Subject

O’Brien unpublished
Auto-PAP and Blood Pressure

Auto-PAP, Blood Pressure, and Medication
Standard of Care comparison group (hypertensive women, no APAP):
- About 55% of women developed worsening BP and ended up with a
diagnosis of pre-eclampsia after enrollment despite antihypertensives
- Other 45% remained CHTN/GHTN although 80% had increased meds
APAP group - Non-compliant users:
- About 65% of women developed worsening BP and ended up with a
diagnosis of pre-eclampsia after enrollment despite antihypertensives
- Other 35% remained CHTN/GHTN although 90% had increased meds
APAP group – Compliant users (≥4 hours/night and ≥4 nights/week):
- About 27% of women developed worsening BP and ended up with a
diagnosis of pre-eclampsia after enrollment despite antihypertensives
- Other 73% remained CHTN/GHTN and only 10% had increased meds
(90% had stable or even decreased meds)
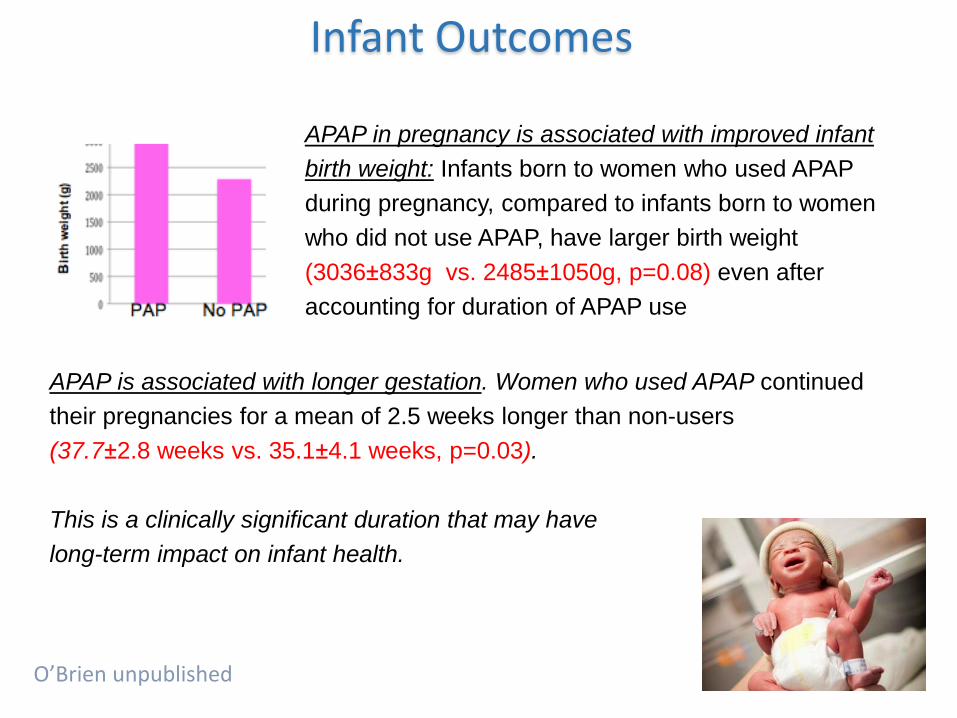
Infant Outcomes
O’Brien unpublished
APAP in pregnancy is associated with improved infant
birth weight: Infants born to women who used APAP
during pregnancy, compared to infants born to women
who did not use APAP, have larger birth weight
(3036±833g vs. 2485±1050g, p=0.08) even after
accounting for duration of APAP use
APAP is associated with longer gestation. Women who used APAP continued
their pregnancies for a mean of 2.5 weeks longer than non-users
(37.7±2.8 weeks vs. 35.1±4.1 weeks, p=0.03).
This is a clinically significant duration that may have
long-term impact on infant health.

Whitehead 2015
Case Report: Treatment of Early Onset Pre-eclampsia by CPAP:
Biochemical/angiogenic markers of preeclampsia improved after CPAP then worsened around 35/40
Pregnancy progressed an additional 30 days after CPAP allowing the infant to gain about 2lbs

PE024:
32yo Caucasian, BMI 24 G4 P1
Fetal demise #1 at 20/40
Fetal demise #2 at 19/40
Premature delivery at 27/40 - NICU
Case 1
All due to pre-eclampsia
Enrolled on trial at 21/40 AHI=1
Did not develop pre-eclampsia
Delivered healthy male infant at 36+2/40 weighing 6lb 1oz
Interestingly, the placenta was normal except for one small infarct,
unlike her previous placenta which showed typical histological
changes. Was this due to APAP?

PE047:
34yo African American, GHTN, BMI 42 G1 P0
BPs at enrollment >150/80mmHg
Case 2
On PAP:
- FHR became reactive
- Maternal SpO2 normal
- Discharged and continued pregnancy for another week
- Delivered healthy 6lb 3oz female infant
Subsequently found to have severe OSA on study PSG (AHI=117)
- Morning after baseline PSG, subject in triage with non-reactive FHR,
reduced FM, and severe maternal desats
- OBGYN plan to deliver that day (37/40)
- Study team paged by OBGYN; decision made to start PAP immediately

Thank you ! Collaborators:
Alexandra S. Bullough, MBChB, FRCA (Anaesthesiology)
Mark C. Chames, MD (Obstetrics)
Marcie C. Treadwell, MD (Obstetrics)
Timothy R. B. Johnson, MD (Obstetrics)
Galit Dunietz, PhD (Epidemiology/Sleep Medicine)
Ronald D. Chervin, MD, MS (Sleep Medicine)
Anita V. Shelgikar, MD (Sleep Medicine)
Roseanne Armitage, PhD (Psychiatry)
Rob Brook, MD (Cardiovascular Medicine)
Colin Sullivan, MBBS, PhD, FRACP, University of Sydney
Christian Guilleminault, MD, Stanford University
Research Coordinators:Mallory Newsted
Lori Kempf, CCRP
Mary Groll-Brown, PSGT
Jocelynn Owusu, MPH
Support: Gilmore Fund, IRWG, MICHR, NIH NHLBI, Respironics

https://www.coursera.org/learn/sleepdeprivation