skin tear prevention - wound care today · skin (e.g. to prevent maceration if the wound has a high...
TRANSCRIPT


Skin tear prevention and management
Dr. Karen OuseyProfessor and Director for the Institute of Skin Integrity &
Infection PreventionUniversity of Huddersfield
Learning points
1. What is a skin tear2. Risk factors for skin tear development3. Prevention of skin tears4. Classifying skin tears and assessment5. Management and treatment of skin tears

What are skin tears?

What is a skin tear?
The International Skin Tear Advisory Panel (ISTAP) defines a skin tear as:
‘A traumatic wound caused by mechanical forces, including removal of adhesives.
Severity may vary by depth (not extending through the subcutaneous layer).’1

Skin tears2
• Skin tears occur across varied patient groups; patients with aged and fragile skin are at an increased risk of skin tears — ageing of the worldwide population means that incidence is increasing.
• They can be painful wounds, affecting quality of life and causing distress to the patient.
• Skin tears may increase the likelihood of hospitalisation, and prolong hospitalisation stay.
• Skin tears result in increased community visits.

What causes skin tears?
• Equipment injuries (wheelchair/bed-rails)
• Blunt trauma• Patient transfers• Falls• Dressing/tape removal• Activities of daily living (ADLs)
Image Property of Smith+Nephew following case study generation from Sue Johnson(Wound Care Lead Nurse) & Kathy Leak (Wound Care sister) both of Doncaster &Bassetlaw Hospitals NHSF Trust 2011.
Injury from safety sides in hospital

How big a problem are skin tears?
• ‘Skin tears are common acute wounds that are misdiagnosed and under-reported too often’1
• Most research is centred around USA and Australia:➢An estimated 1.5 million skin tears occur in elderly
residents of institutions in the USA annually3
➢0.92% incidence rate reported in an elderly care facility in the USA

How big a problem are skin tears?
• 16% of the population sustained skin tears each month in a 120-bed facility in Australia
• 41.5% of known wounds were found to be skin tears in elderly care residents (mean age 80 years) in a 347-bed long-term care facility in Western Australia
• 8–11% skin tear prevalence reported in surveys in all WA public hospitals in 2007, 2008 and 2009

Incidence and prevalence1
‘Incidence and prevalence rates vary incredibly across countries, healthcare settings and populations.
Studies report the prevalence of skin tears being between 3% and 26% in long-term care facilities and the incidence rates being as high as 92%.’1

How big a problem are skin tears in the current environment?
• Variation in incidence may be due to different practices and a lack of a uniform method for assessment and documentation
• During the COVID-19 crisis, consider:• Are skin tears being prioritised?
• In care/nursing homes?
• At home?
• Visits to ED or GP?

Risk factors for skin tear development
Who is at risk of skin tears?
• Individuals suffering from skin tears often suffer from a long history of skin tears.4
• As with any wound, once closed the area of injury will have reduced tensile strength, and with each subsequent skin tear, the individual will be at greater risk of skin tears. 4
‘Skin tears are reported across all healthcare settings and are predominantly found in:• The elderly• Neonates• Critically ill populations• Chronically ill populations.1
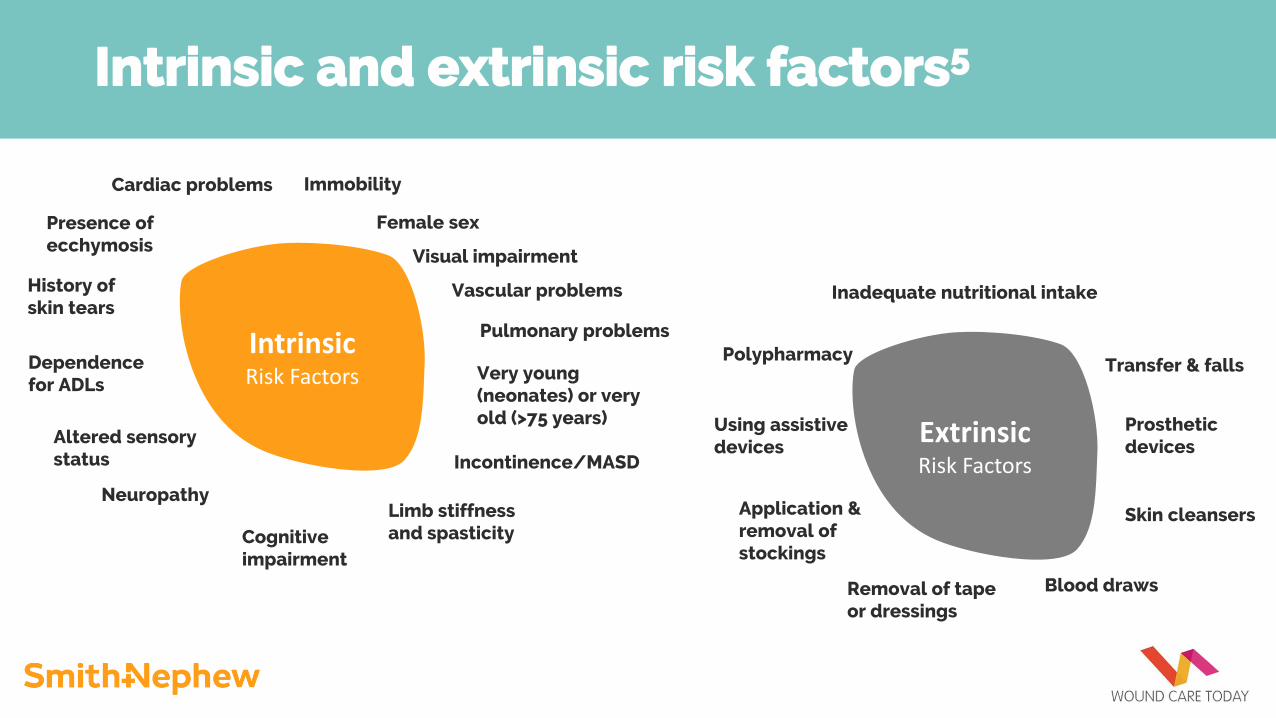
Intrinsic and extrinsic risk factors5
IntrinsicRisk Factors
ExtrinsicRisk Factors
Female sex
Immobility
Presence of ecchymosis
History of skin tears
Dependence for ADLs
Altered sensory status
Cognitive impairment
Limb stiffness and spasticity
Neuropathy
Very young (neonates) or very old (>75 years)
Vascular problems
Cardiac problems
Pulmonary problems
Visual impairment
Incontinence/MASD
Inadequate nutritional intake
Polypharmacy
Using assistive devices
Application & removal of stockings
Removal of tape or dressings
Blood draws
Transfer & falls
Prosthetic devices
Skin cleansers

Prevention of skin tears

Prevention of skin tears2
• Wherever possible, prevention should be the aim when assessing, planning and implementing care for skin tears.
• By controlling modifiable risk factors, skin health can be maintained and injury avoided.
• Prevention is based around the same principles as risk factor identification:
1. General health2. Mobility3. Skin.

Quick reference guide for the ISTAP risk reduction programme2
Risk factor Individual Caregiver/provider
General health Educate patient (if cognitivefunction not impaired)Optimise nutrition andhydration
Safe patient environmentEducate client and caregiversProtect from self-harmDietary consultantNB extreme body mass index (BMI) (under/overweight)Review polypharmacy
Mobility Encourage activeinvolvement (if physicalfunction not impaired)Appropriate selection anduse of assistive devices
Daily skin assessment and monitor for skin tearsSafe patient handling/equipment, including propertransferring and repositioningFall prevention programme (remove clutter, proper lighting)Pad equipmentAvoid sharp fingernails/jewellery
Skin Encourage awareness of medication-induced skin fragilityWear protective clothingMoisturise skinKeep fingernails short
Skin hygiene — warm/tepid water, soapless pH-neutralcleansers, moisturise skinAvoid strong adhesives, dressings, tapesAvoid sharp fingernails/jewellery

Classifying skin tears and assessment
Classification tools
• Payne-Martin Classification System
• Skin Tear Audit Research (STAR)6,7
• International Skin Tear Advisory Panel (ISTAP) Classification System1,2

Classification tools: Payne-Martin Classification System
‘Grades skin tears based on extent of tissue loss, measured
as a percentage’1
Table taken from: LeBlanc K et al. Best practice recommendations for the prevention and management of skin tears in aged skin. Wounds International 2018. Available to download from www.woundsinternational.com

Classification tools: Skin Tear Audit Research (STAR)6
Figure adapted (with permission) from the Skin Tear Audit Research (STAR) photographic library, Silver Chain Nursing Association and School of Nursing and Midwifery, Curtin University of Technology6, 7

Classification tools: ISTAP1
‘The ISTAP tool classifies skin
tears based on the severity of “skin
flap” loss, but does not provide a
definition of a “skin flap”.’1

Management and treatment

Management and treatment of skin tears2
• Skin tears are acute wounds that have the potential to be closed by primary intention.
• Traditionally, wounds closed by primary intention are secured with sutures, staples or adhesive strips; however, given the fragility of aged skin and that skin tears are generally not deep, these are not viable options.

Management and treatment of skin tears8
•Where possible, treatment of skin tears should aim to:•Preserve the skin flap•Maintain the surrounding tissue•Re-approximate the edges of the wound
(without stretching the skin)•Reduce the risk of infection and further injury
while considering any comorbidities.
Assessment — what do you need to include?
• Anatomical location and duration of skin tear• Dimensions (length, width depth)• Wound bed characteristics and percentage of
viable/non-viable tissue• Type and volume of exudate• Presence of bleeding or haematoma• Degree of flap necrosis• Integrity of surrounding skin• Signs of infection• Associated pain

Management and treatment of skin tears2
ISTAP pathway

Treatment of skin tears2
Control bleeding and cleanse the wound according to protocol
Control bleeding• Apply pressure and elevate the limb if
appropriate.• When controlling bleeding is the main goal,
dressings to assist with haemostasis may be used.

Treatment of skin tears2
Control bleeding and cleanse the wound according to protocol
Cleanse• Cleanse/irrigate the wound as per local protocol and
remove any residual debris or haematoma; gently pat the surrounding skin dry to avoid further injury.
• If viable, re-approximate the skin flap to use as a ‘dressing.’ Ease the flap back into place using a gloved finger, dampened cotton tip, tweezers or a silicone strip.

Treatment of skin tears2
Manage infection/inflammation and consider moisturebalance/exudate control
Manage infection/inflammation• Wound inflammation from trauma should be
distinguished from wound infection.• Wound infection can result in pain and delayed
wound healing; diagnosis of infection should be based on clinical assessment and appropriate infection control measures taken.

Treatment of skin tears2
Manage infection/inflammation and consider moisturebalance/exudate control
Consider moisture balance/exudate control• Skin tears tend to be dry wounds, but there may be some
circumstances in which exudate is an issue.• Moisture balance is essential to promote wound healing
and to protect the peri-wound skin from maceration.• Observe the volume and viscosity of the exudate when
selecting a topical wound dressing.

Treatment of skin tears2
Monitor wound edge/closure
Monitor wound edge/closure• Skin tears are acute wounds that should typically proceed to closure in a
timely fashion and follow an acute wound closure trajectory of 14–21 days.
• Ensure that all potential factors that could delay healing (e.g. diabetes, peripheral oedema, nutritional issues) have been addressed.
• Compression therapy should be considered if the wound is on the lower leg. Before applying compression, a full leg assessment including vascular assessment, e.g. ankle brachial pressure index (ABPI) should be carried out.

Suitable dressings for skin tears
When skin tears occur, it is vital that the wound care products chosen will optimise wound healing and not increase the risk of further skin damage.
The ideal dressing for managing skin tears should2:
If possible, leave the dressing in place for several days to avoid disturbing the skin flap.7
The skin flap should not be disturbed for at least five days to allow for adherence to the cellular structures below.9
• Control bleeding
• Be easy to apply and remove
• Not cause trauma on removal
• Provide a protective anti-shear barrier
• Be flexible and mould to contours
• Provide secure, but not aggressive, retention
• Afford extended wear time
• Be cost-effective
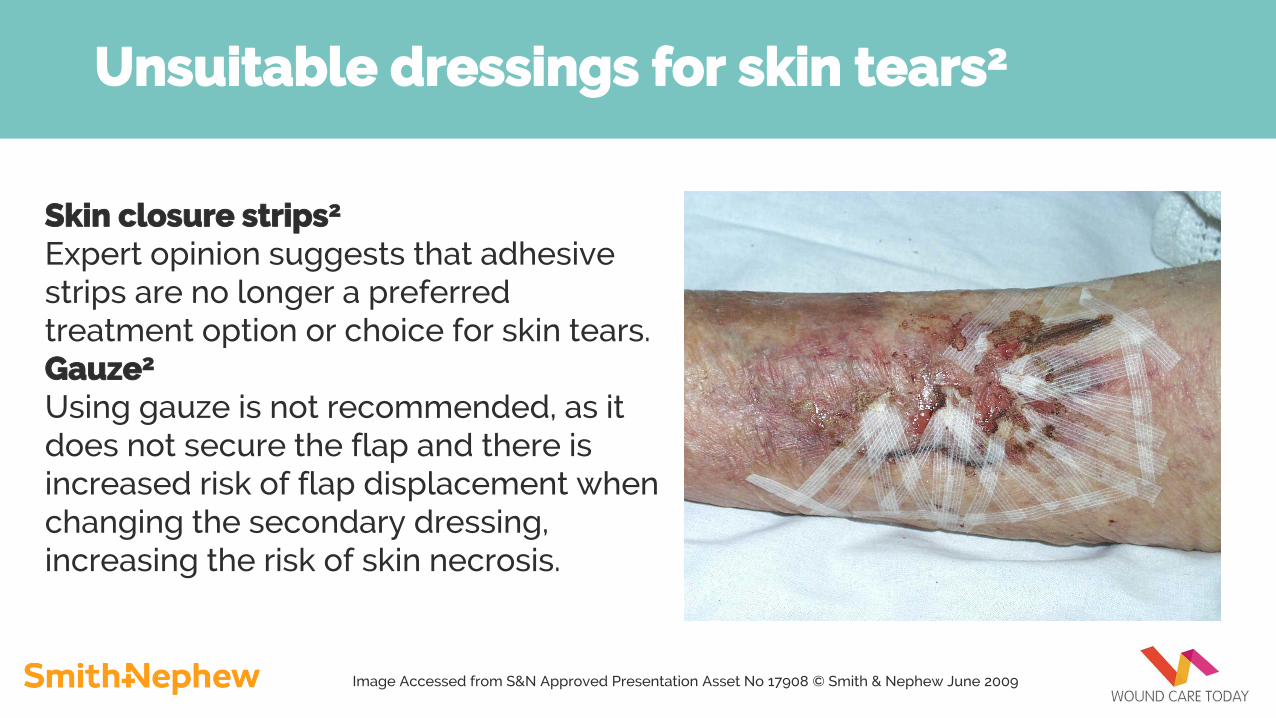
Unsuitable dressings for skin tears2
Skin closure strips2
Expert opinion suggests that adhesive strips are no longer a preferred treatment option or choice for skin tears.Gauze2
Using gauze is not recommended, as it does not secure the flap and there is increased risk of flap displacement when changing the secondary dressing, increasing the risk of skin necrosis.
Image Accessed from S&N Approved Presentation Asset No 17908 © Smith & Nephew June 2009

Unsuitable dressings for skin tears2
Iodine-based dressings2
Iodine causes drying of the wound and peri-wound skin. A major risk factor for skin tear development is listed to be dry skin.
Image Accessed from S&N Approved Presentation Asset No 17908 © Smith & Nephew June 2009

Tips in practice
Mark the dressing with an arrow to indicate the correct direction of removal and make sure that this is clearly explained in the notes.2,6
These recommendations are from cited references 2 and 5. All products must be used as per their Instructions for Use (IFU).
Adhesive removers can be used when removing the dressing to minimise trauma. 2,6
Take time to remove dressings slowly.2
Tips in practice
These recommendations are from cited references 2 and 5. All products must be used as per their Instructions for Use (IFU).
Consider using a skin barrier product to protect the surrounding skin (e.g. to prevent maceration if the wound has a high exudate volume).2
Use an emollient to soften and smooth wider skin area and prevent further tears.2
Continue to monitor the wound for changes or signs of infection; if there is no improvement (e.g. after four assessments), or the wound deteriorates, refer to appropriate specialist as per local protocol.2

Resources

Support from Smith+Nephew
• Digital skin tear toolbox• ISTAP & STAR Pathways• Educational presentation• Instructional video

Support from Smith+Nephew
Smith+Nephewcan organise the
rollout for you and your teams
and provide online training where needed.
Facilitate virtual training to implement the pathway:
• Residential care homes can undertake ‘first-aid’ following the pathway. This can ease the pressure on community nurses
• Nursing homes can promote following a standardised process to ensure the best clinical outcome

Support from Smith+Nephew
Skin tear resources and support available from S+N’s extensive team of complex wound specialists and territory managers.
Smith+Nephew website
Wound Care Todaywebsite
Smith+Nephew UKI YouTube
Tissue Viability Societywebsite
Smith+Nephew Wound Care Support Line
References
1. Van Tiggelen H, et al (2019) Standardizing the classification of skin tears: validity and reliability testing of the International Skin Tear Advisory Panel Classification System in 44 countries. Br J Dermatol Oct 12. doi: 10.1111/bjd. 18604 [Epub ahead of print]
2. LeBlanc K, et al (2018) Best practice recommendations for the prevention and management of skin tears in aged skin. Wounds International. Available to download from www.woundsinternational.com
3. Baranoski S (2005) Meeting the challenge of skin tears. Adv Skin Wound Care 18(2): 74–5
4. LeBlanc K, Baronoski S (2011) Skin Tears: state of the Science: consensus statements for the prevention, prediction, assessment, and treatment of skin tears©. Adv Skin Wound Care 24(9 Suppl): 2–15
5. Baronoski S, LeBlanc K, Gloeckner M (2016) Preventing, assessing, and managing skin tears: a clinical review. Am J Nurs 116(11): 24–30
6. Carville K, Lewin G, Newall N, et al (2007) STAR: a consensus for skin tear classification. Primary Intent 15(1): 18-28
7. Stephen-Haynes J, Carville K (2011) Skin tears made easy. Wounds Int 2(4): 1-6
8. Wounds UK (2015) All Wales Guidance for the prevention and management of skin tears. Available online at: http://www.welshwoundnetwork.org/files/8314/4403/4358/content_11623.pdf
9. LeBlanc K, Baranoski S, Christensen D, et al (2016) The Art of Dressing Selection: A Consensus Statement on Skin Tears and Best Practice. Adv Skin Wound Care 29(1): 32–3
The views and opinions expressed in this presentation are those of the presenter and do not reflect the position, opinion, or guidelines for clinical care of any other person, institution,
scientific association, or product manufacturer. Responsibility for obtaining permission to use images contained in this presentation is that of the presenter, not Smith+Nephew.
Smith+Nephew does not provide medical advice and is not responsible for the content or information provided through this presentation. It is the treating health care provider’s responsibility to determine the best course of treatment for their patient based upon his
professional medical judgment.
For detailed product information, including indications for use, contraindications, effects, precautions and warnings, please consult the product’s Instructions for Use (IFU) prior to use. The presentation and the information presented may not be appropriate for all jurisdictions.Products may not be available in all markets because product availability is subject to the
regulatory and/or medical practices in individual markets.
Please contact your Smith+Nephew representative if you have questionsabout the availability of Smith+Nephew products in your area.