simulator training: the future? mike larvin rcs director of education professor of surgery...
TRANSCRIPT

Simulator Training: The Future?
Mike Larvin
RCS Director of Education
Professor of Surgery
University of Nottingham at Derby

Imitation of reality for research, testing,
training or education
Requires:
• valid source information
• simplifying approximations and assumptions
• validity, reliability, fidelity
Simulation

Technological triggers: Cold war
“Tennis for Two” (1957) Higinbotham (Brookhaven)
used missile trajectories
Sputnik 1 (1957)Launched atop a modified
ballistic missile
• UG: less practical surgery
• PG1-2: foundation years
• PGY3-4: core MRCS
• PGY5-8+: specialty FRCS
• Less experience, WTD
• New technologies to learn
• Patients and trainees have changed
Surgical training has changed

• medical errors kill 98,000 people annually
• $37 to $50 billion for adverse events
• resident 80h week, less direct interaction
• bioterrorism threats and crisis management
Public drivers US IOM 2004

Generation ‘X’ = most of you
• Followed ‘baby boomer’ generation
• Born 1961 to 1981, ‘13th US generation’ - premarital sex, atheistic, republican, less respect for parents and authority - greater formal education
Generation X: Tales for an Accelerated CultureDouglas Coupland, 1991

• Followed ‘Generation X’
• Born early 1980s to mid-1990s - rapid communication, peer orientation, instant gratification, stimulating work - family breakdown, tech-savvy, ‘open’
Hunter-Gatherers of the Knowledge EconomyDavid Berreby, 1999
Generation ‘Y’ = junior trainees

• Followed ‘Generation Y’
• Born early mid-1990s to 2000s - baby boomlet - highly connected, lifelong use of comms and media technologies such as WWW - “digital natives”: instant messaging, texting, MP3, mobile phones, YouTube
Grown Up Digital: How the Net Generation is Changing Your WorldDon Tapscott 2009
Generation ‘Z’ = coming soon
Trainees still require:
• Knowledge
they prefer e-learning• Skills
technical, decisions, comms: like simulation• Structure
curriculum and assessment: online is fine

STEP® Foundation and Core
• MMC and ISCP competences
• MRCS preparation
• 8 A4 printed modules
• e-learning, video, web simulation
• e-community and college days
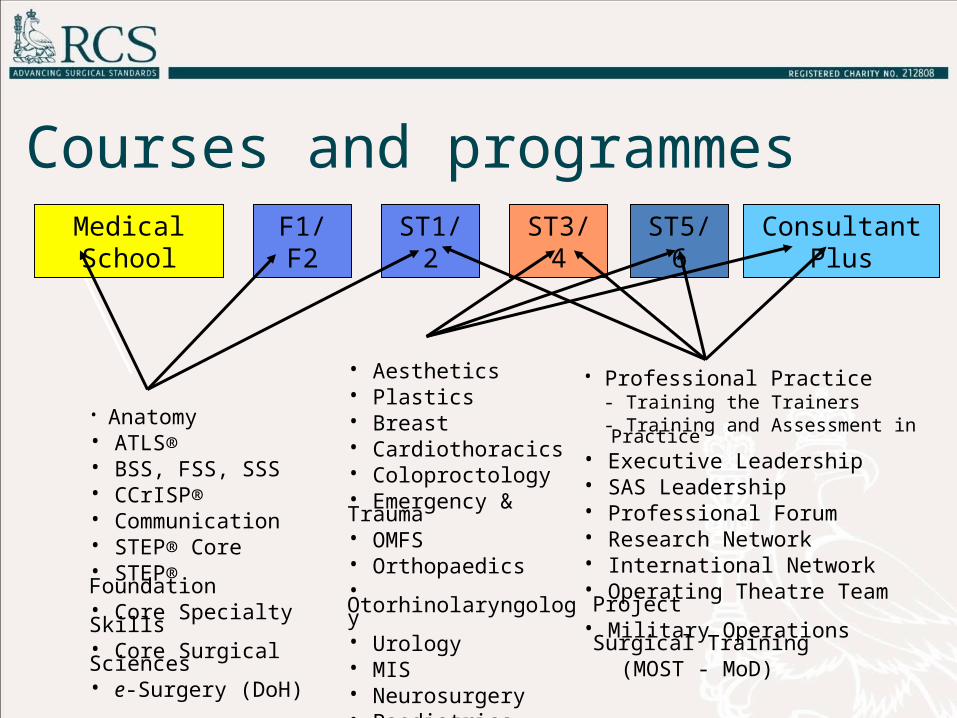
Courses and programmesMedical School F1/F2 ST1/2 ST3/4 ST5/6 Consultant Plus
• Anatomy• ATLS® • BSS, FSS, SSS• CCrISP®• Communication• STEP® Core• STEP® Foundation• Core Specialty Skills• Core Surgical Sciences• e-Surgery (DoH)
• Aesthetics• Plastics • Breast• Cardiothoracics • Coloproctology• Emergency & Trauma• OMFS• Orthopaedics• Otorhinolaryngology• Urology• MIS• Neurosurgery• Paediatrics• Vascular Surgery
• Professional Practice - Training the Trainers - Training and Assessment in Practice
• Executive Leadership • SAS Leadership • Professional Forum • Research Network• International Network• Operating Theatre Team Project• Military Operations Surgical Training (MOST - MoD)
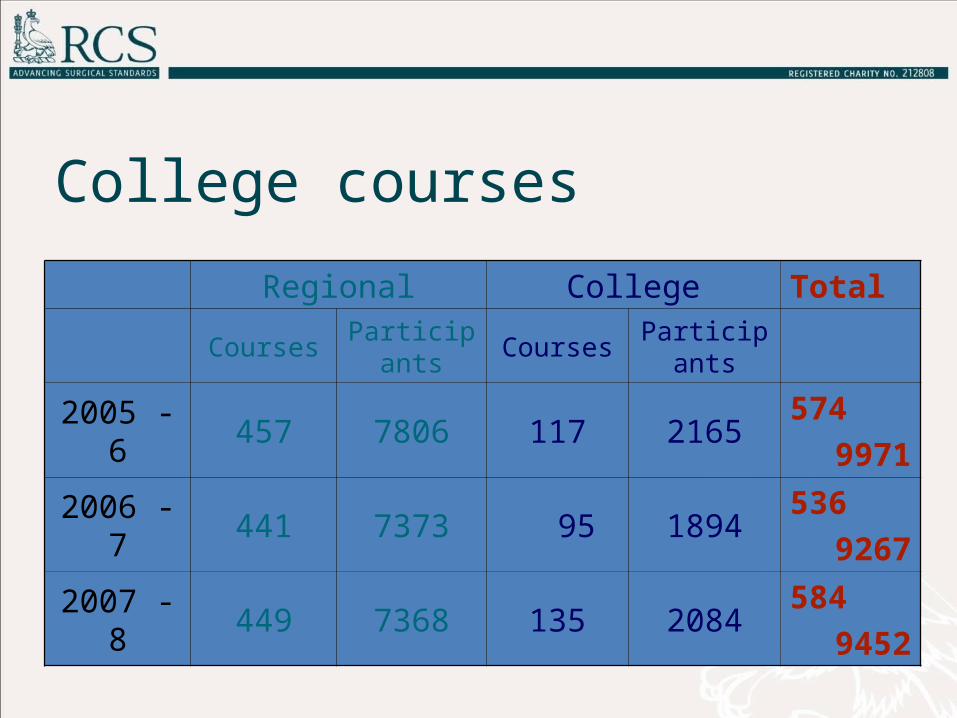
College courses
Regional College Total
Courses Participants Courses Participants
2005 - 6 457 7806 117 2165574
9971
2006 - 7 441 7373 95 1894536
9267
2007 - 8 449 7368 135 2084584
9452
• anatomy, physiology, history, behaviour,
physical findings
• cadavers, prosections, plastinates
• plastics
• animal tissue
Active simulation
‘Human in the loop’ simulation
Ideal when:
• real environment too expensive or risky
• need to learn in "safe" environment
• test mistakes in safety-critical systems
• ‘type change’ after basic pilot training
Interactive simulation
• ‘live’: real people, simulated kit, real world
hi-fidelity, samples likely performance
• ‘virtual’: real people, simulated kit and world
VR training
• ‘constructive’: sim people, kit and world
behavioural training and assessment
Training simulation types

• Sim Man 3g (Laerdel)
• life-sized mannequin
• responds to injected drugs
• programmed for life
threatening emergencies
• can be changed ‘on the fly’
High-fidelity live simulation

• 1985, K Semm’s
‘pelvi-trainer’
for laparoscopy
• Haptics included
ἅπτεσθαι - to “contact” or “touch”
Laparoscopy

• visual components by computer graphics
• touch components by haptic feedback
• input/output: force feedback
could be widely distributed via standard
web browsers with standard game joysticks
Virtual simulators

• 2010: Symbionix
‘Laparotrainer’
for laparoscopy
• Haptics not included
Laparoscopy


• Largest capital project since post-war rebuilding
Eagle project

Wolfson Surgical Skills Centre
anatomy teaching
procedural simulation
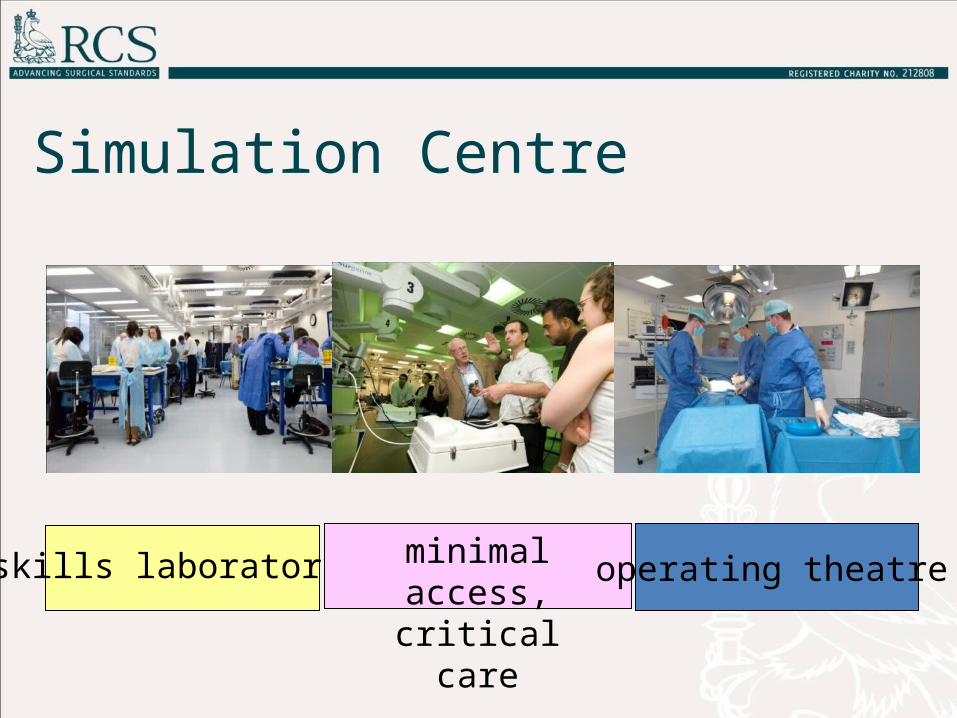
Simulation Centre
skills laboratory minimal access,critical care
operating theatre
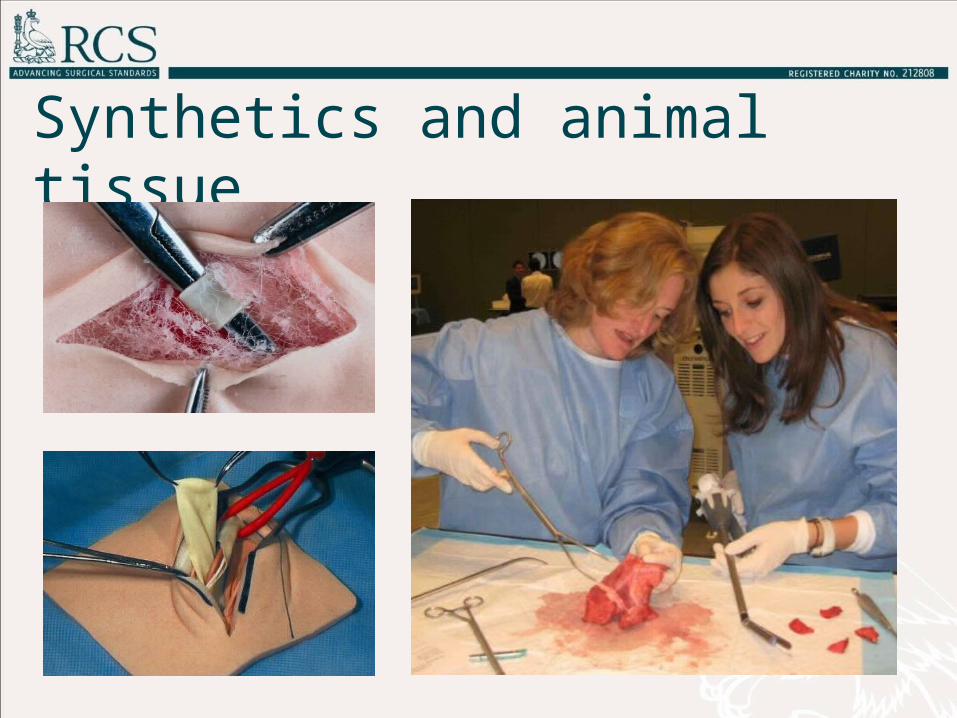
Synthetics and animal tissue
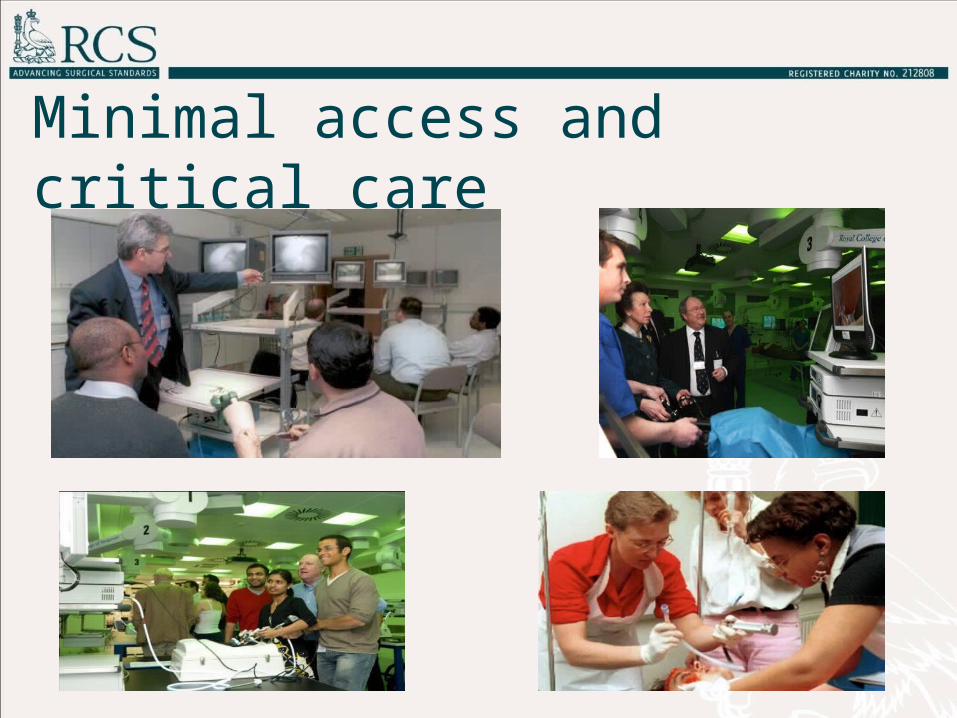
Minimal access and critical care
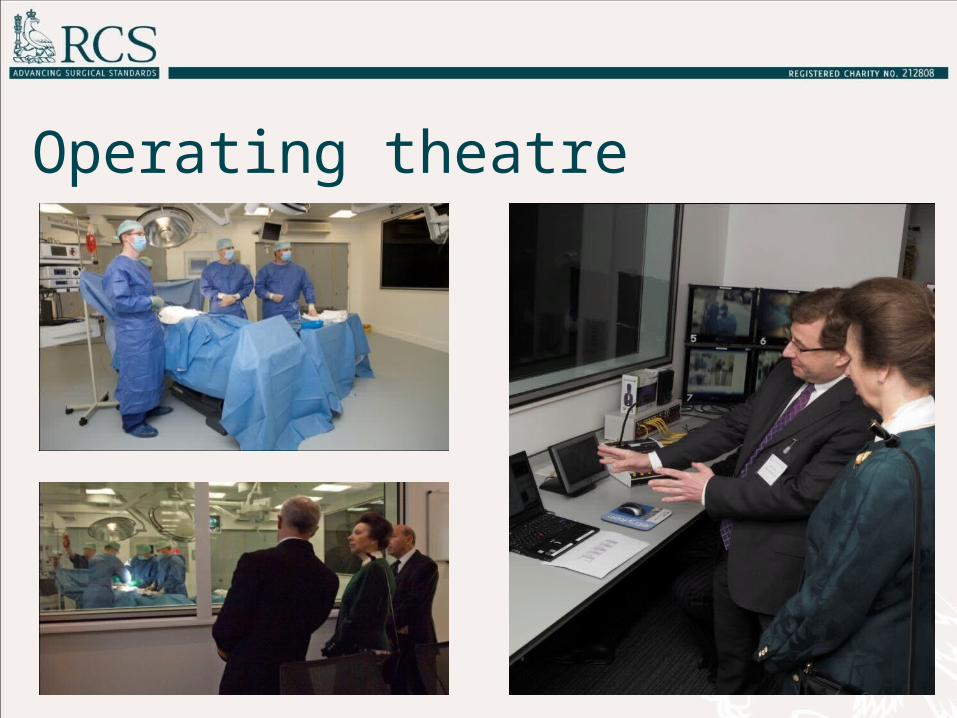
Operating theatre

Teaching suite
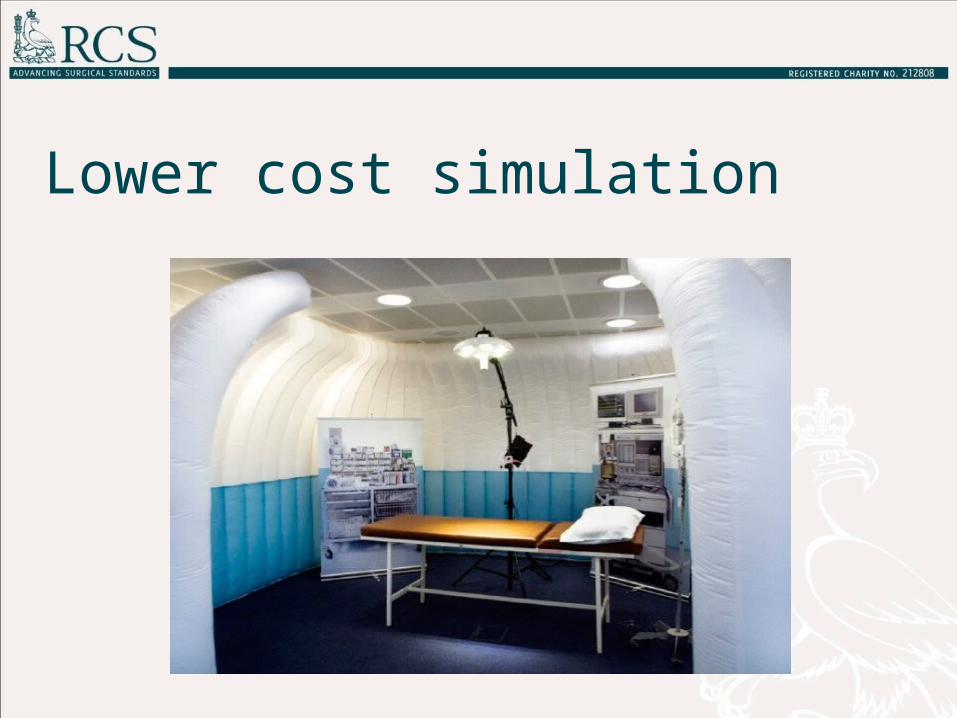
Lower cost simulation

• improved health outcomes, reduced errors
• reduced health care costs, enhanced quality
• better skills, lower malpractice rates
• more flexible training at correct pace
• allows practice and mistakes, improves skills
without consequence to the patient
Benefits
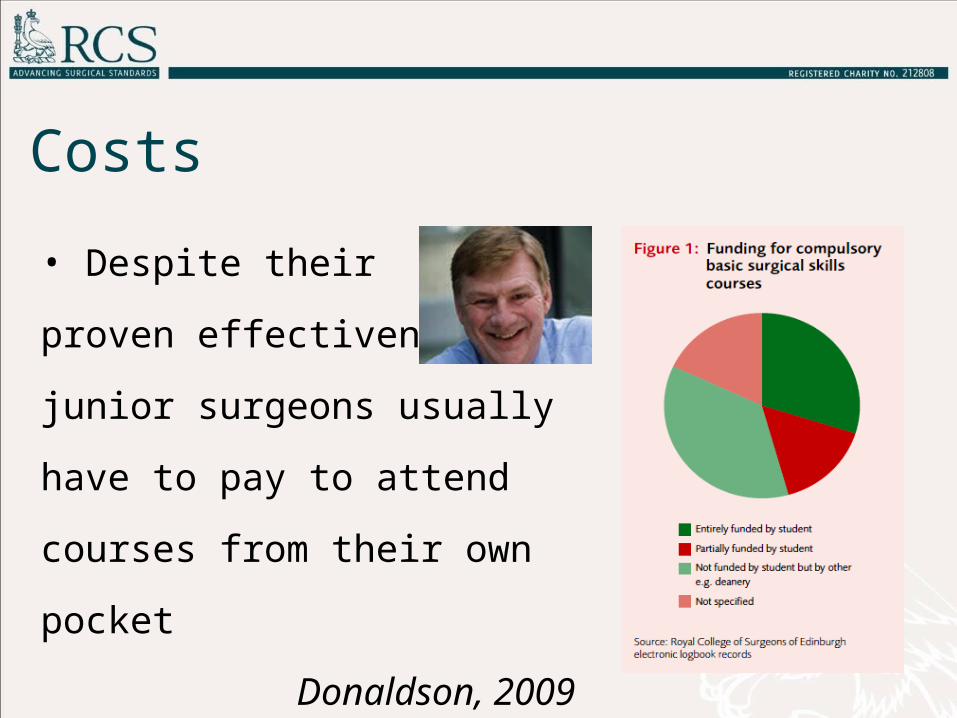
• Despite their
proven effectiveness,
junior surgeons usually
have to pay to attend courses
from their own pocket
Donaldson, 2009
Costs
Simulator training: the future?
• More simulation, improved models
• Expensive, collaboration makes sense
• Preparation for work-based training
• NOT a substitute for the ‘real thing’
• More versatile than patient-based training
• Useful in standardising assessment
