simposio problematiche psicogeriatriche nel paziente ... · asmn-irccs reggio emilia. demenza come...
TRANSCRIPT

SIMPOSIO
Problematiche
psicogeriatriche nel paziente
fratturato
Giulio Pioli
ASMN-IRCCS
Reggio Emilia

Demenza come fattore di rischio di frattura
AD case (N = 56,186, mean age 79.9 (SD 6.8) years, range 42–101 years)
Tolppanen et al. • Incident Hip Fractures among Community Dwelling Persons with Alzheimer’sDisease in a Finnish Nationwide Register-Based Cohort. PLoS ONE 2013
Hazard ratios for hip fractures according to age at AD diagnosis
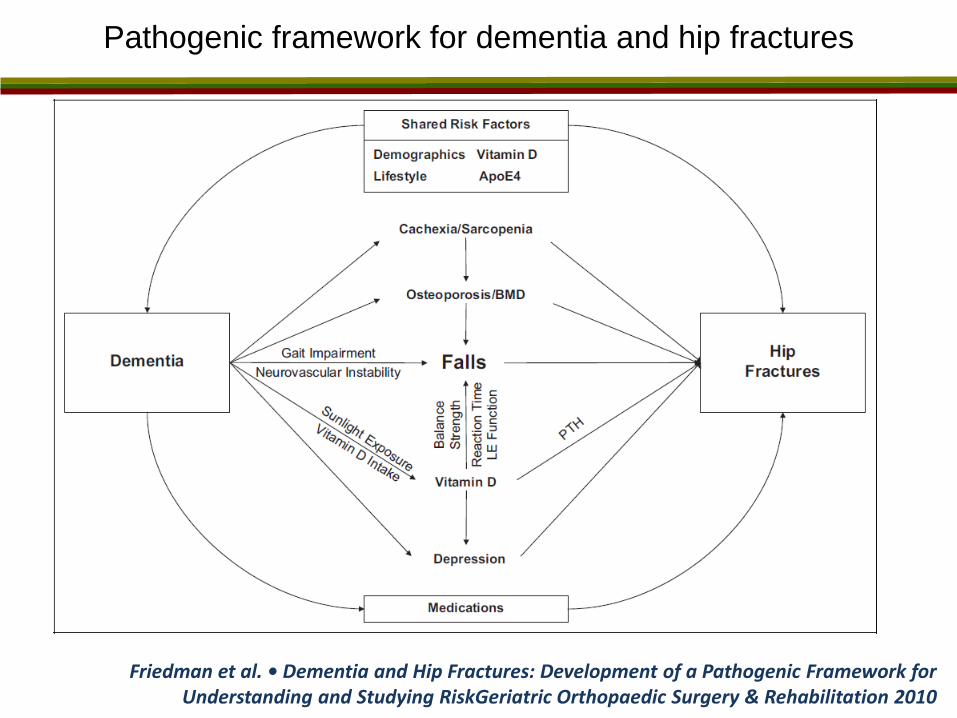
Pathogenic framework for dementia and hip fractures
Friedman et al. • Dementia and Hip Fractures: Development of a Pathogenic Framework for Understanding and Studying RiskGeriatric Orthopaedic Surgery & Rehabilitation 2010
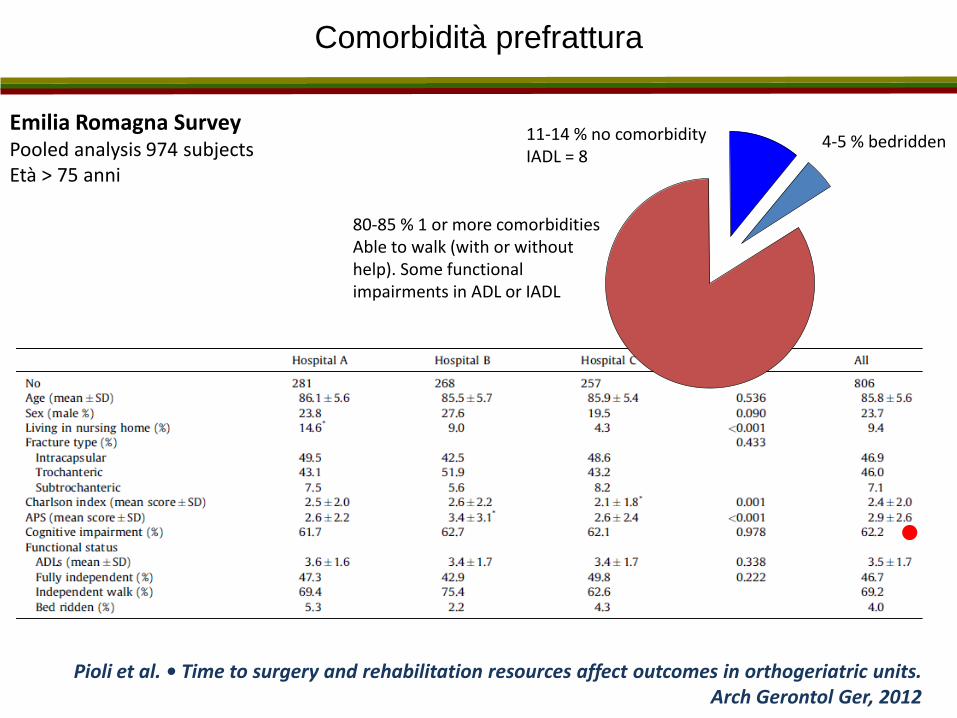
Comorbidità prefrattura
Emilia Romagna Survey Pooled analysis 974 subjects Età > 75 anni
4-5 % bedridden 11-14 % no comorbidity IADL = 8
80-85 % 1 or more comorbidities Able to walk (with or without help). Some functional impairments in ADL or IADL
Pioli et al. • Time to surgery and rehabilitation resources affect outcomes in orthogeriatric units. Arch Gerontol Ger, 2012

Demenza come fattore di rischio dopo la frattura
Population-based, retrospective cohort study. Ontario, Canada. 45,602 older adults had hip fractures
Seitz et al. • Effects of Dementia on Postoperative Outcomes of Older Adults With Hip Fractures. JAMDA 2014
community long term care
Mortality

Il paziente con frattura di femore e demenza
Gestione delle fase acuta
• Controllo del dolore
• Tipo di anestesia
• Complicanze (delirium)
• Postoperative Cognitive Dysfunction
Gestione della fase postacuta
• Il recupero funzionale nel paziente con demenza
• Tipo di riabilitazione
• Accesso ai servizi riabilitativi
• Rischio di istituzionalizzazione

Il controllo del dolore nei pazienti con frattura di femore e demenza
Sieber et al. • Postoperative Opioid Consumption and Its Relationship to Cognitive Function in Elderly Hip Fracture Patients. J Am Geriatr Soc. 2011
Pain management
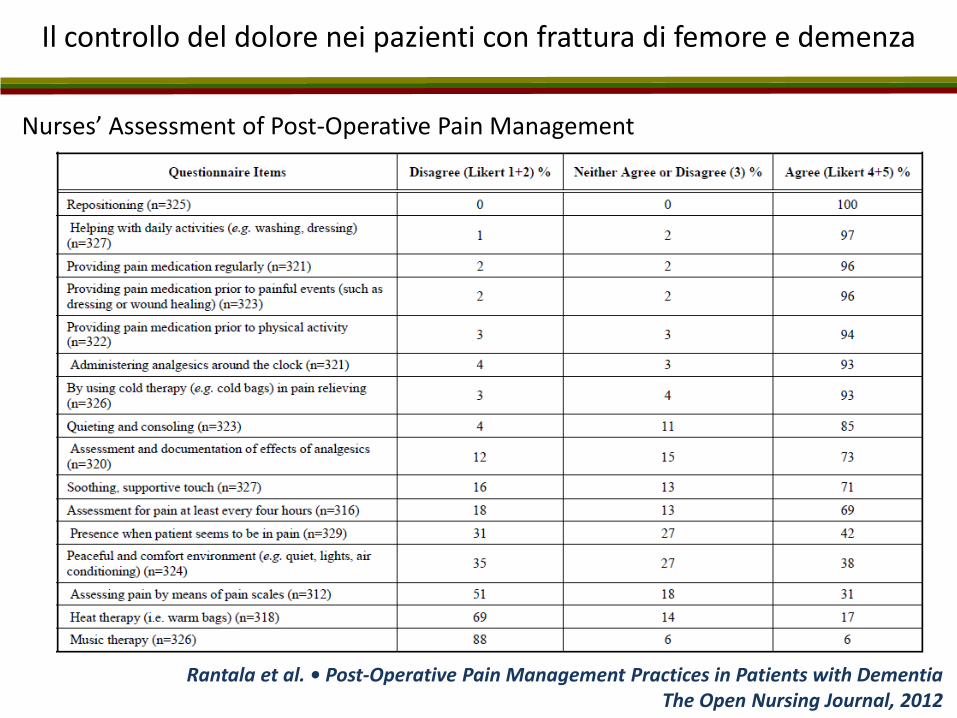
Il controllo del dolore nei pazienti con frattura di femore e demenza
Rantala et al. • Post-Operative Pain Management Practices in Patients with Dementia The Open Nursing Journal, 2012
Nurses’ Assessment of Post-Operative Pain Management
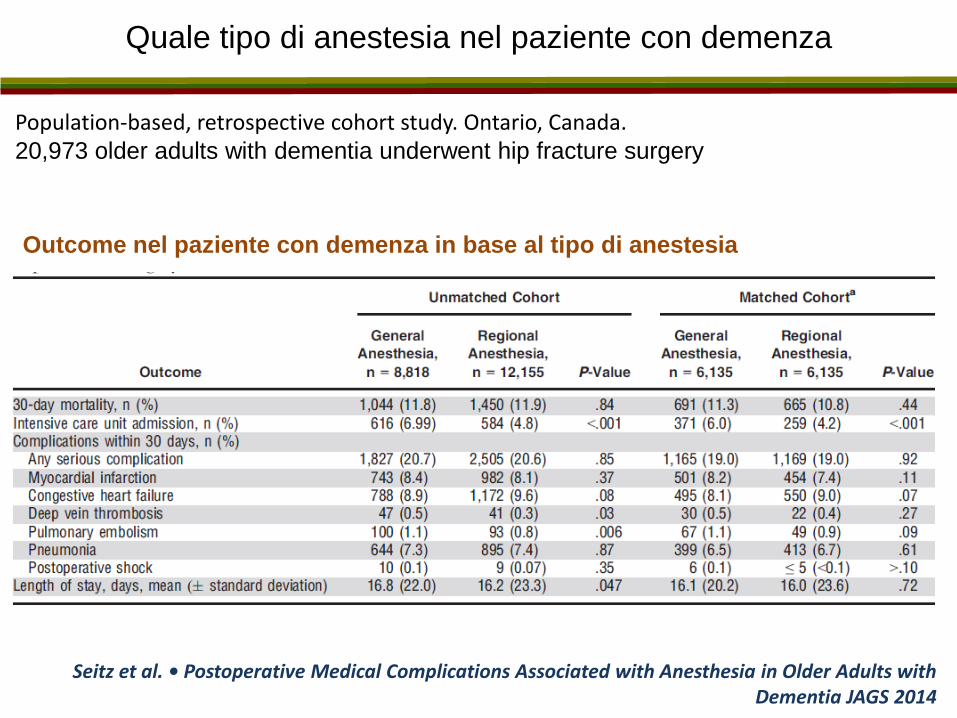
Quale tipo di anestesia nel paziente con demenza
Population-based, retrospective cohort study. Ontario, Canada. 20,973 older adults with dementia underwent hip fracture surgery
Seitz et al. • Postoperative Medical Complications Associated with Anesthesia in Older Adults with Dementia JAGS 2014
Outcome nel paziente con demenza in base al tipo di anestesia

Quale tipo di anestesia nel paziente con demenza
Retrospective review. 500 patients undergoing vascular surgical procedures.
Ellard,et al. • Type of Anesthesia and Postoperative Delirium After Vascular Surgery Dementia JournalofCardiothoracicandVascularAnesthesia,2014
Rischio di delirium in base al tipo di anestesia

Aumento del rischio di demenza dopo anestesia generale ?
Seitz et al. • A review of epidemiological evidence for general anesthesia as a risk factor for Alzheimer's disease. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2013
Fifteen case–control studies
… at the present time
there is limited
information to support
the hypothesis
of AD developing as a
consequence of GA,
although there are few
high quality studies in
this area.
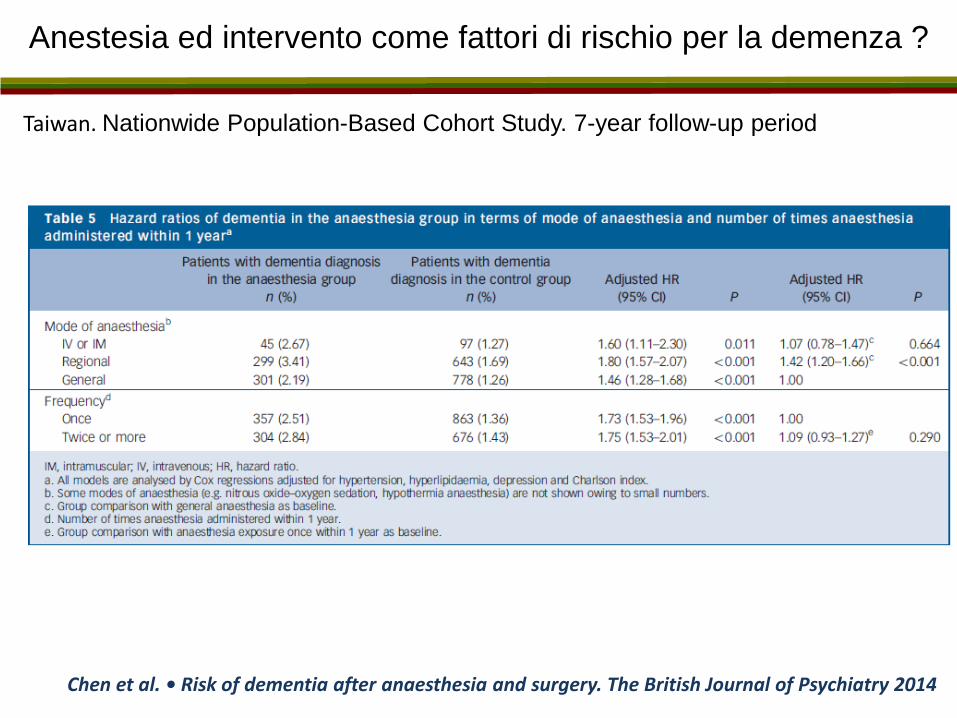
Anestesia ed intervento come fattori di rischio per la demenza ?
Taiwan. Nationwide Population-Based Cohort Study. 7-year follow-up period
Chen et al. • Risk of dementia after anaesthesia and surgery. The British Journal of Psychiatry 2014

Aumento del rischio di demenza dopo frattura ?
Taiwan. Nationwide Population-Based Cohort Study. 12-year follow-up period
Tsai et al. • Fracture as an Independent Risk Factor of Dementia. Medicine 2014
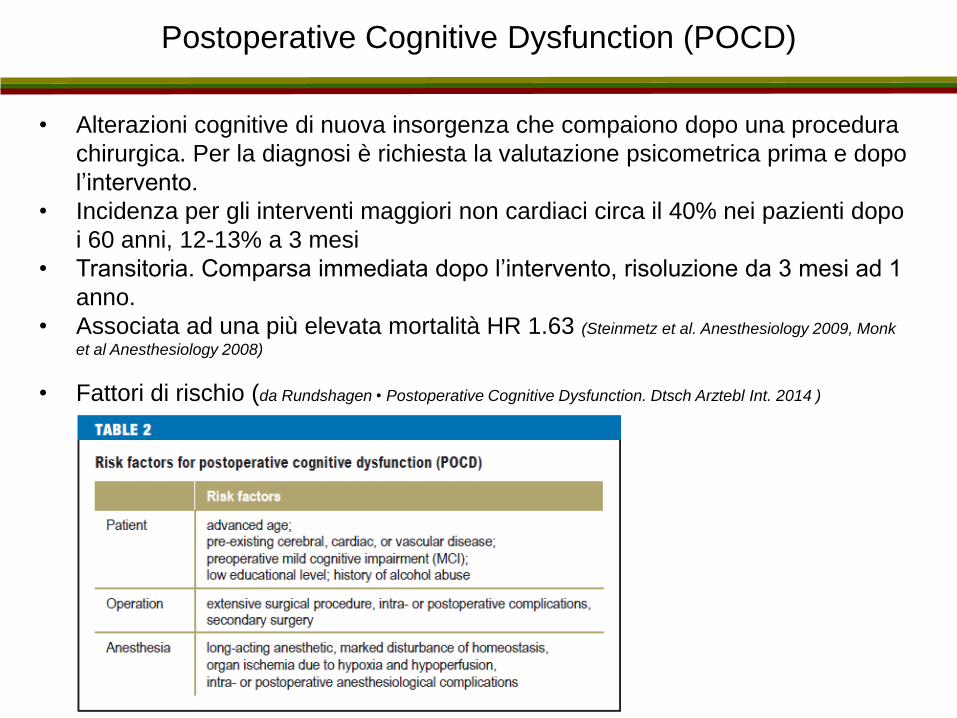
Postoperative Cognitive Dysfunction (POCD)
• Alterazioni cognitive di nuova insorgenza che compaiono dopo una procedura
chirurgica. Per la diagnosi è richiesta la valutazione psicometrica prima e dopo
l’intervento.
• Incidenza per gli interventi maggiori non cardiaci circa il 40% nei pazienti dopo
i 60 anni, 12-13% a 3 mesi
• Transitoria. Comparsa immediata dopo l’intervento, risoluzione da 3 mesi ad 1
anno.
• Associata ad una più elevata mortalità HR 1.63 (Steinmetz et al. Anesthesiology 2009, Monk
et al Anesthesiology 2008)
• Fattori di rischio (da Rundshagen • Postoperative Cognitive Dysfunction. Dtsch Arztebl Int. 2014 )
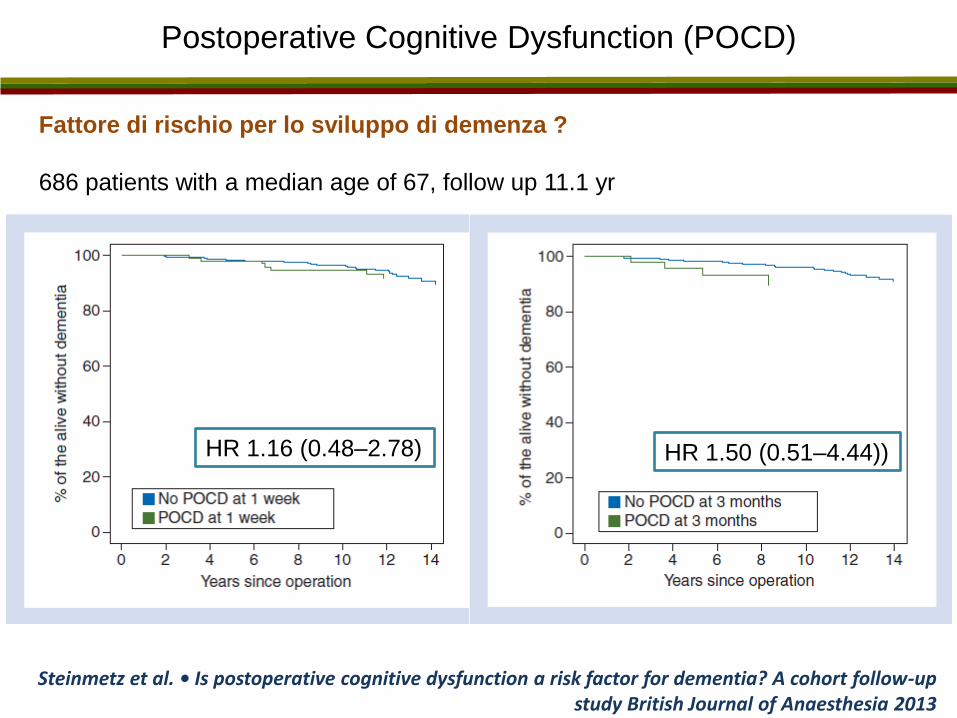
Postoperative Cognitive Dysfunction (POCD)
Fattore di rischio per lo sviluppo di demenza ?
686 patients with a median age of 67, follow up 11.1 yr
Steinmetz et al. • Is postoperative cognitive dysfunction a risk factor for dementia? A cohort follow-up study British Journal of Anaesthesia 2013
HR 1.50 (0.51–4.44)) HR 1.16 (0.48–2.78)

Postoperative Cognitive Dysfunction nel paziente ortopedico
Shoair et al• Incidence and risk factors for postoperative cognitive dysfunction in older adults undergoing major noncardiac surgery: A prospective study. J Anaesthesiol Clin Pharmacol. 2015
69 patients aged 65 years or older undergoing major noncardiac surgery
(88% elective orthopedic surgery) MMSE 28 ± 1.4
Multivariate logistic regression
Incidenza a 3 mesi, 15.9%
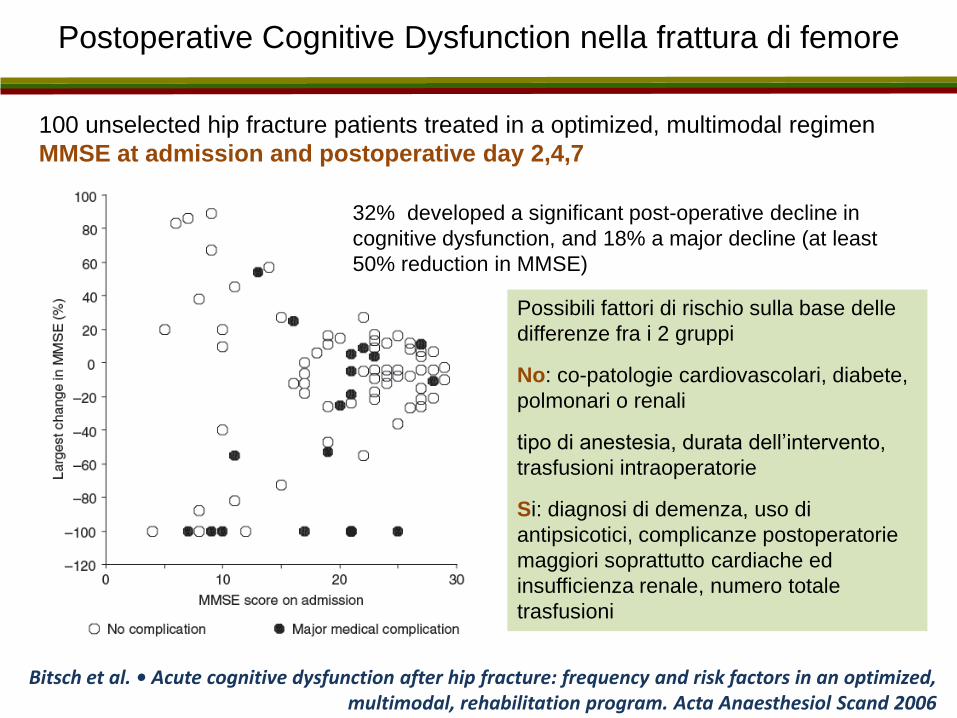
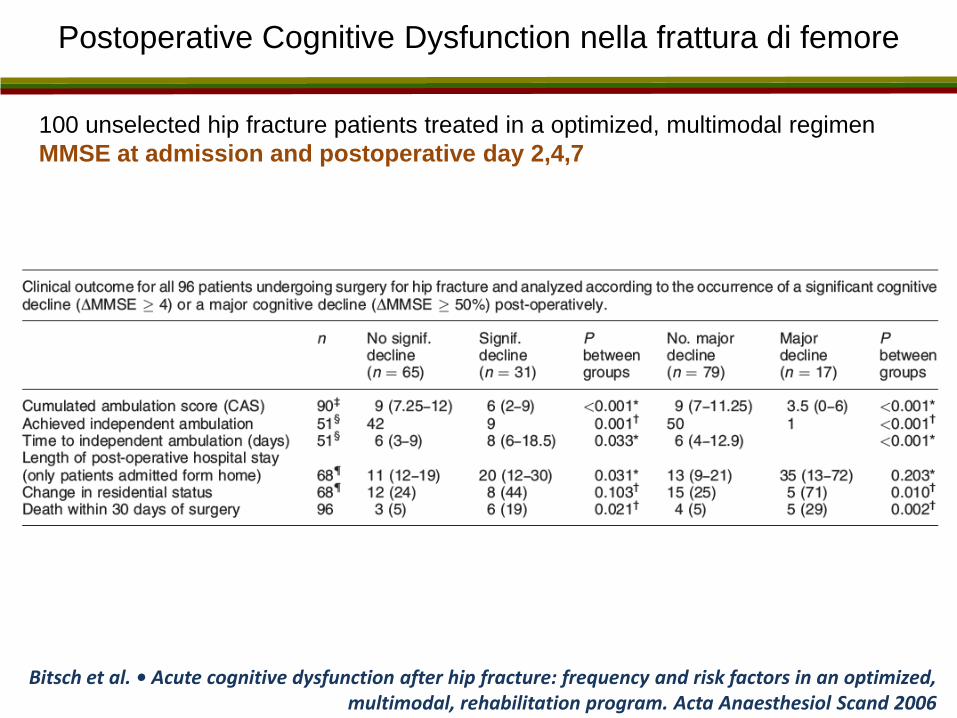
Postoperative Cognitive Dysfunction nella frattura di femore
Bitsch et al. • Acute cognitive dysfunction after hip fracture: frequency and risk factors in an optimized, multimodal, rehabilitation program. Acta Anaesthesiol Scand 2006
100 unselected hip fracture patients treated in a optimized, multimodal regimen
MMSE at admission and postoperative day 2,4,7
32% developed a significant post-operative decline in
cognitive dysfunction, and 18% a major decline (at least
50% reduction in MMSE)
Possibili fattori di rischio sulla base delle
differenze fra i 2 gruppi
No: co-patologie cardiovascolari, diabete,
polmonari o renali
tipo di anestesia, durata dell’intervento,
trasfusioni intraoperatorie
Si: diagnosi di demenza, uso di
antipsicotici, complicanze postoperatorie
maggiori soprattutto cardiache ed
insufficienza renale, numero totale
trasfusioni
Postoperative Cognitive Dysfunction nella frattura di femore
Bitsch et al. • Acute cognitive dysfunction after hip fracture: frequency and risk factors in an optimized, multimodal, rehabilitation program. Acta Anaesthesiol Scand 2006
100 unselected hip fracture patients treated in a optimized, multimodal regimen
MMSE at admission and postoperative day 2,4,7
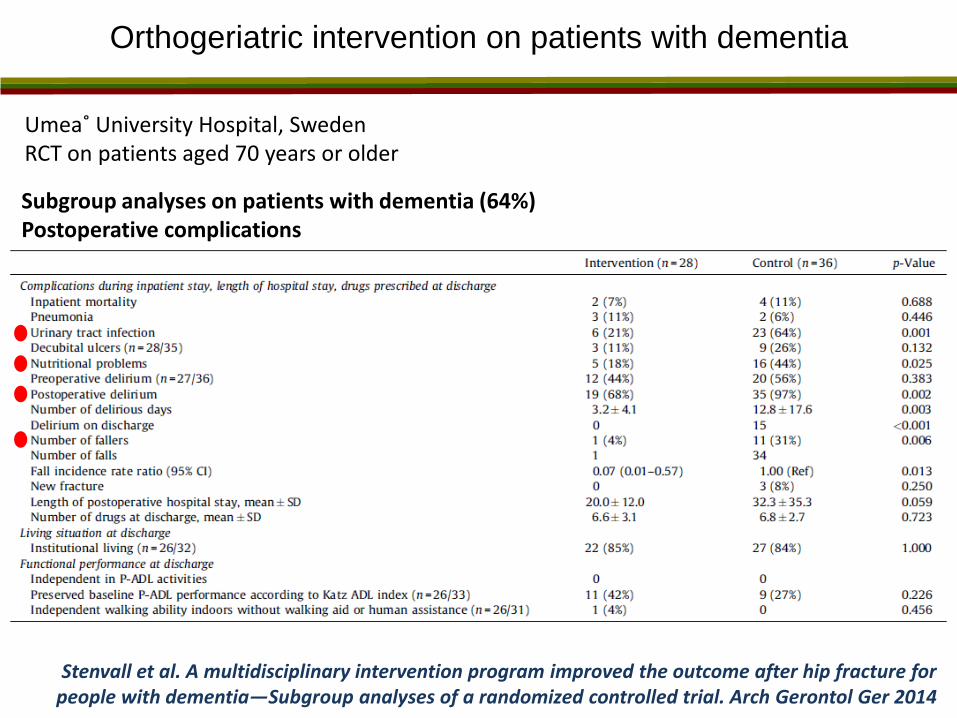
Orthogeriatric intervention on patients with dementia
Umea˚ University Hospital, Sweden RCT on patients aged 70 years or older
Stenvall et al. A multidisciplinary intervention program improved the outcome after hip fracture for people with dementia—Subgroup analyses of a randomized controlled trial. Arch Gerontol Ger 2014
Subgroup analyses on patients with dementia (64%) Postoperative complications

Il paziente con frattura di femore e demenza
Gestione delle fase acuta
• Controllo del dolore
• Tipo di anestesia
• Complicanze (delirium)
• Postoperative Cognitive Dysfunction
Gestione della fase postacuta
• Il recupero funzionale nel paziente con demenza
• Tipo di riabilitazione
• Accesso ai servizi riabilitativi
• Rischio di istituzionalizzazione
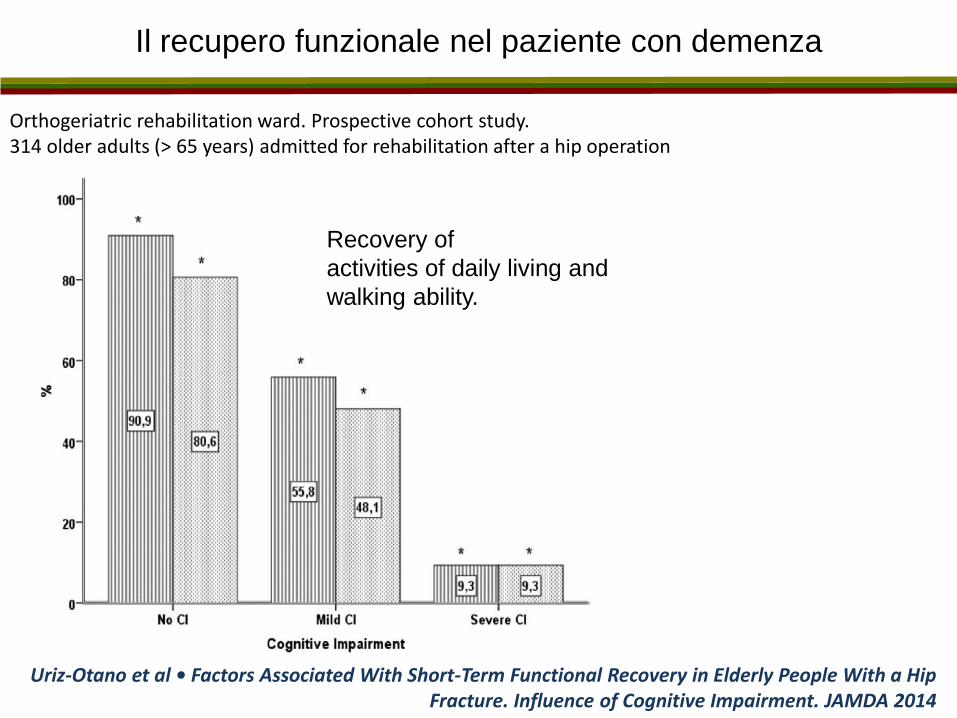
Il recupero funzionale nel paziente con demenza
Uriz-Otano et al • Factors Associated With Short-Term Functional Recovery in Elderly People With a Hip Fracture. Influence of Cognitive Impairment. JAMDA 2014
Orthogeriatric rehabilitation ward. Prospective cohort study. 314 older adults (> 65 years) admitted for rehabilitation after a hip operation
Recovery of
activities of daily living and
walking ability.

Il recupero funzionale nel paziente con demenza
Uriz-Otano et al • Factors Associated With Short-Term Functional Recovery in Elderly People With a Hip Fracture. Influence of Cognitive Impairment. JAMDA 2014
Orthogeriatric rehabilitation ward. Prospective cohort study. 314 older adults (> 65 years) admitted for rehabilitation after a hip operation
Conclusion:
Previous walking ability and
the presence of
complications, such as
pressure ulcers or
delirium, play a greater role
in functional recovery than
cognitive impairment. Not
considering these
aspects could lead to an
overestimation of the impact
of cognitive impairment in
the recovery of these
patients.

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
dead
walking performance lower than prefracture
walking performance similar to prefracture
3 m 12 m 6 m 3 m 12 m 6 m 3 m 12 m 6 m
Perc
ent of
the w
hole
sam
ple
Group 2
Mobile indoors
Group 1
Mobile outdoors
Group 3
Mobile with help
Recupero del cammino dopo la frattura di femore
Pioli et al • (Submitted) 2015
Emilia Romagna Survey Pooled analysis 774 subjects (excluded bed-ridden before fracture) Età > 75 anni

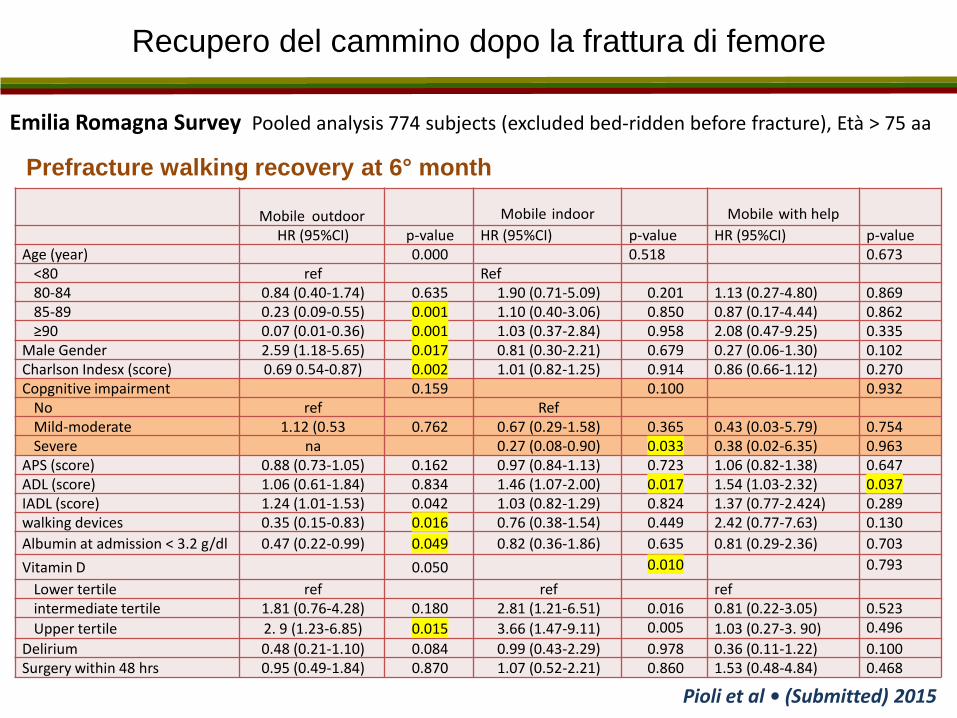
Recupero del cammino dopo la frattura di femore
Pioli et al • (Submitted) 2015
Emilia Romagna Survey Pooled analysis 774 subjects (excluded bed-ridden before fracture), Età > 75 anni
0
10
20
30
40
50
60
70
80
90
100
Mobile outdoors Mobile indoors Mobile with help
cognitively healthy
moderate cognitive impairment
severe cognitive impairment
*
#
Prefracture walking recovery at 6° month
Recupero del cammino dopo la frattura di femore
Pioli et al • (Submitted) 2015
Emilia Romagna Survey Pooled analysis 774 subjects (excluded bed-ridden before fracture), Età > 75 aa
Mobile outdoor Mobile indoor Mobile with help
HR (95%CI) p-value HR (95%CI) p-value HR (95%CI) p-value Age (year) 0.000 0.518 0.673
<80 ref Ref 80-84 0.84 (0.40-1.74) 0.635 1.90 (0.71-5.09) 0.201 1.13 (0.27-4.80) 0.869 85-89 0.23 (0.09-0.55) 0.001 1.10 (0.40-3.06) 0.850 0.87 (0.17-4.44) 0.862 ≥90 0.07 (0.01-0.36) 0.001 1.03 (0.37-2.84) 0.958 2.08 (0.47-9.25) 0.335
Male Gender 2.59 (1.18-5.65) 0.017 0.81 (0.30-2.21) 0.679 0.27 (0.06-1.30) 0.102 Charlson Indesx (score) 0.69 0.54-0.87) 0.002 1.01 (0.82-1.25) 0.914 0.86 (0.66-1.12) 0.270 Copgnitive impairment 0.159 0.100 0.932
No ref Ref Mild-moderate 1.12 (0.53 0.762 0.67 (0.29-1.58) 0.365 0.43 (0.03-5.79) 0.754 Severe na 0.27 (0.08-0.90) 0.033 0.38 (0.02-6.35) 0.963
APS (score) 0.88 (0.73-1.05) 0.162 0.97 (0.84-1.13) 0.723 1.06 (0.82-1.38) 0.647 ADL (score) 1.06 (0.61-1.84) 0.834 1.46 (1.07-2.00) 0.017 1.54 (1.03-2.32) 0.037 IADL (score) 1.24 (1.01-1.53) 0.042 1.03 (0.82-1.29) 0.824 1.37 (0.77-2.424) 0.289 walking devices 0.35 (0.15-0.83) 0.016 0.76 (0.38-1.54) 0.449 2.42 (0.77-7.63) 0.130
Albumin at admission < 3.2 g/dl 0.47 (0.22-0.99) 0.049 0.82 (0.36-1.86) 0.635 0.81 (0.29-2.36) 0.703
Vitamin D 0.050 0.010 0.793
Lower tertile ref ref ref intermediate tertile 1.81 (0.76-4.28) 0.180 2.81 (1.21-6.51) 0.016 0.81 (0.22-3.05) 0.523
Upper tertile 2. 9 (1.23-6.85) 0.015 3.66 (1.47-9.11) 0.005 1.03 (0.27-3. 90) 0.496
Delirium 0.48 (0.21-1.10) 0.084 0.99 (0.43-2.29) 0.978 0.36 (0.11-1.22) 0.100 Surgery within 48 hrs 0.95 (0.49-1.84) 0.870 1.07 (0.52-2.21) 0.860 1.53 (0.48-4.84) 0.468
Prefracture walking recovery at 6° month
Recupero funzionale nella demenza
Muir et al. The impact of cognitive impairment on rehabilitation outcomes in elderly patients admitted with a femoral neck fracture: a systematic review. J Geriatr Phys Ther. 2009
CONCLUSION:
There is some evidence that older adults with cognitive impairment who receive
intensive inpatient rehabilitation after surgical repair of a hip fracture may be able to
gain comparable benefit in physical function as cognitively intact patients. There is
not enough information to guide recommendations of specific physical therapy
interventions to optimize outcomes in this patient population. Further work is
needed.
Allen et al. Rehabilitation in Patients with Dementia Following Hip Fracture: A Systematic Review. J Physiotherapy Canada 2012
CONCLUSIONS:
People with mild or moderate dementia may show improved function and
ambulation and decreased fall risk after rehabilitation post hip fracture, similar to
gains achieved by those without dementia. More research is required to ascertain
the effect of rehabilitation in people with moderate to severe dementia, including
those residing in continuing-care settings.
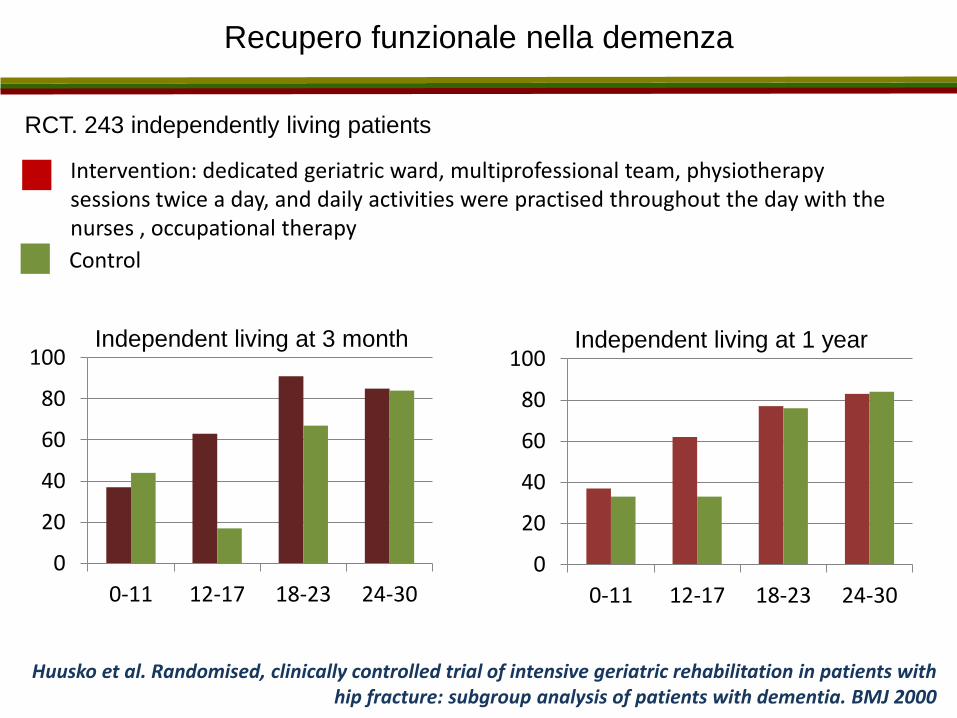
Recupero funzionale nella demenza
RCT. 243 independently living patients
Huusko et al. Randomised, clinically controlled trial of intensive geriatric rehabilitation in patients with hip fracture: subgroup analysis of patients with dementia. BMJ 2000
0
20
40
60
80
100
0-11 12-17 18-23 24-30
0
20
40
60
80
100
0-11 12-17 18-23 24-30
Independent living at 3 month Independent living at 1 year
Intervention: dedicated geriatric ward, multiprofessional team, physiotherapy sessions twice a day, and daily activities were practised throughout the day with the nurses , occupational therapy
Control
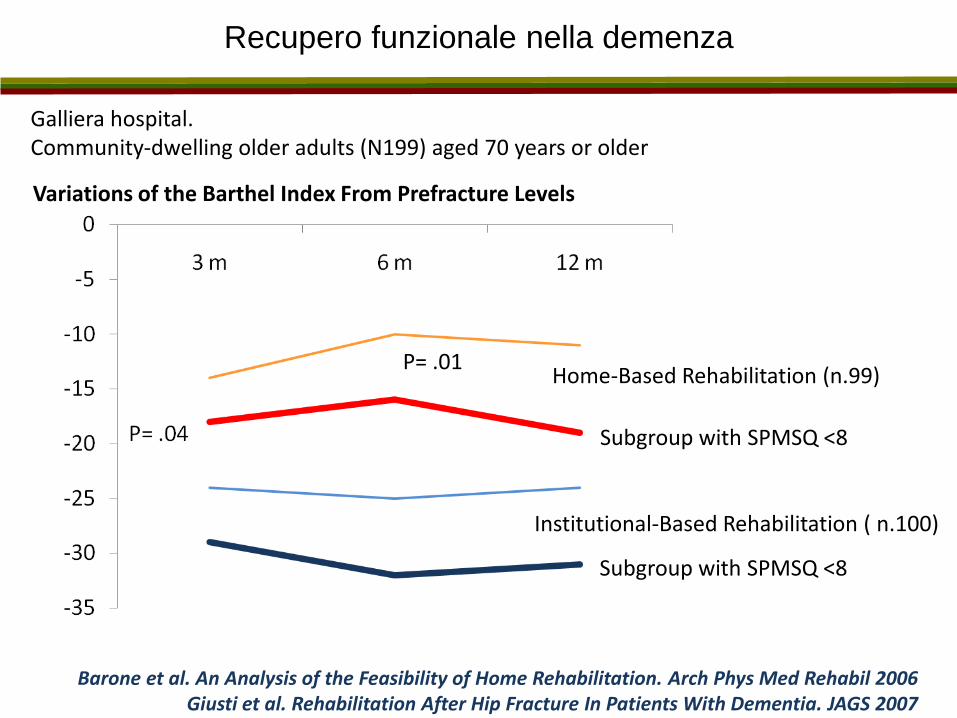
Recupero funzionale nella demenza
Barone et al. An Analysis of the Feasibility of Home Rehabilitation. Arch Phys Med Rehabil 2006
Giusti et al. Rehabilitation After Hip Fracture In Patients With Dementia. JAGS 2007
Galliera hospital. Community-dwelling older adults (N199) aged 70 years or older
Variations of the Barthel Index From Prefracture Levels
Home-Based Rehabilitation (n.99)
Institutional-Based Rehabilitation ( n.100)
P= .01
Subgroup with SPMSQ <8
Subgroup with SPMSQ <8
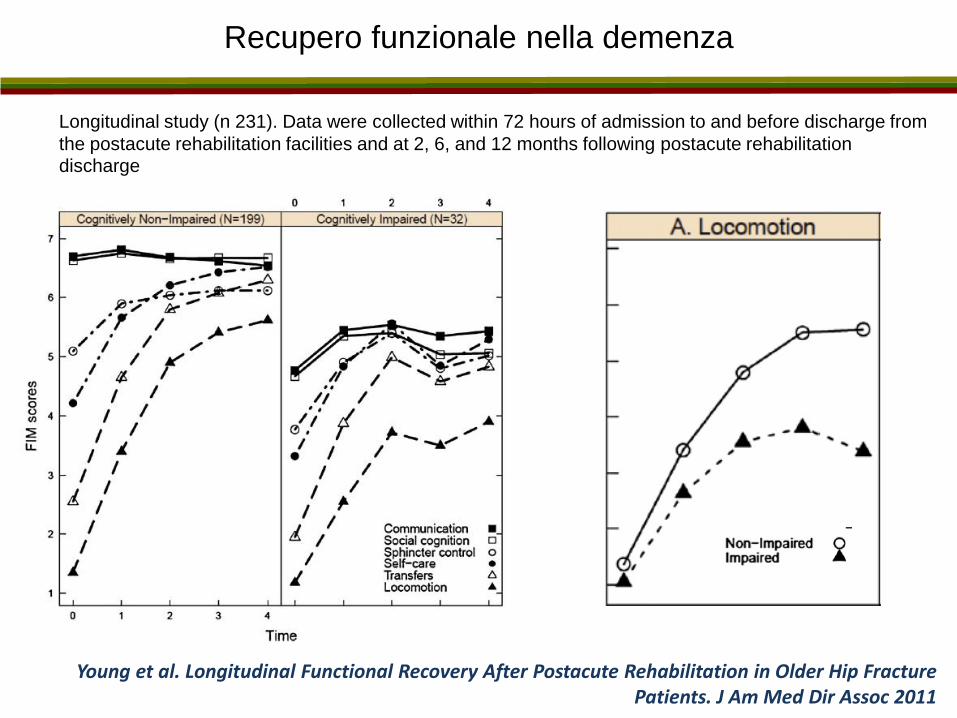
Recupero funzionale nella demenza
Young et al. Longitudinal Functional Recovery After Postacute Rehabilitation in Older Hip Fracture Patients. J Am Med Dir Assoc 2011
Longitudinal study (n 231). Data were collected within 72 hours of admission to and before discharge from
the postacute rehabilitation facilities and at 2, 6, and 12 months following postacute rehabilitation discharge
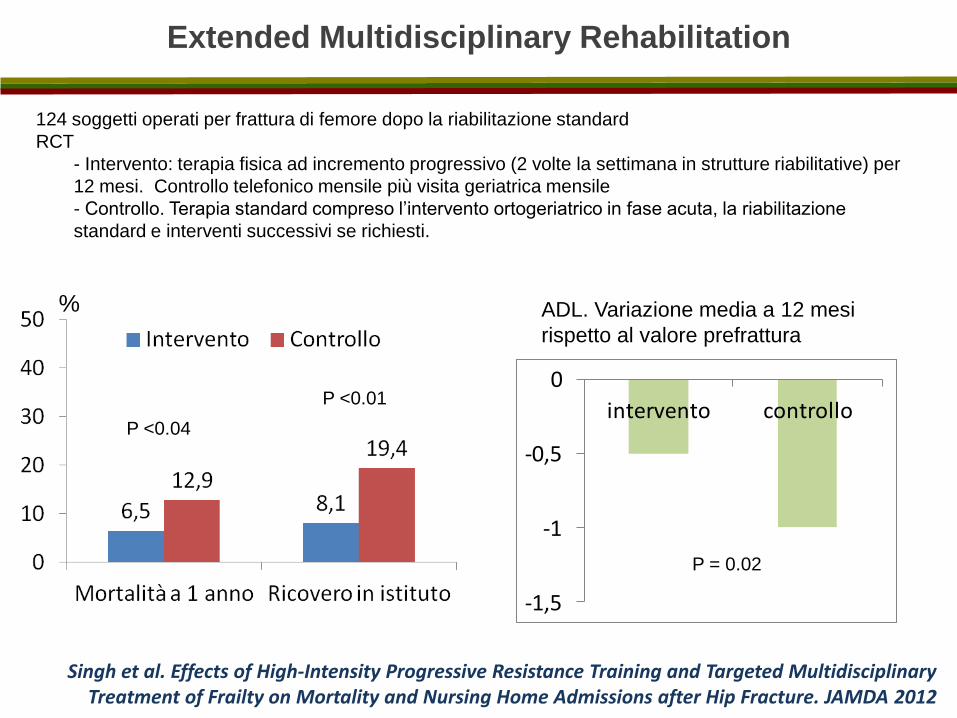
124 soggetti operati per frattura di femore dopo la riabilitazione standard
RCT
- Intervento: terapia fisica ad incremento progressivo (2 volte la settimana in strutture riabilitative) per
12 mesi. Controllo telefonico mensile più visita geriatrica mensile
- Controllo. Terapia standard compreso l’intervento ortogeriatrico in fase acuta, la riabilitazione
standard e interventi successivi se richiesti.
P <0.04
P <0.01
%
-1,5
-1
-0,5
0
intervento controllo
ADL. Variazione media a 12 mesi
rispetto al valore prefrattura
P = 0.02
Extended Multidisciplinary Rehabilitation
Singh et al. Effects of High-Intensity Progressive Resistance Training and Targeted Multidisciplinary Treatment of Frailty on Mortality and Nursing Home Admissions after Hip Fracture. JAMDA 2012

Recupero funzionale nella demenza
Al-Ani et al. Does Rehabilitation Matter in Patients With Femoral Neck fracture and Cognitive Impairment? Arch Phys Med Rehabil 2010
Multicenter study of the Stockholm Hip Fracture Group
with cognitive impairment (known dementia or low [0–2 points] score) in Short Portable Mental Status Questionnaire [0–10 points]) and able to walk before the fracture.
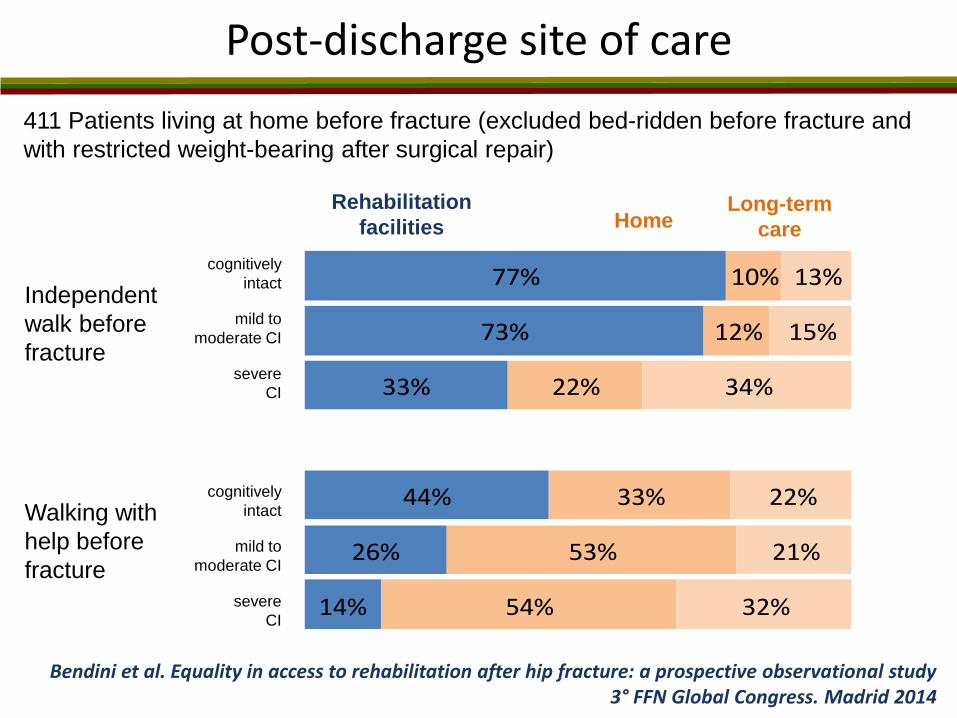
Post-discharge site of care
411 Patients living at home before fracture (excluded bed-ridden before fracture and
with restricted weight-bearing after surgical repair)
77%
73%
33%
44%
26%
14%
10%
12%
22%
33%
53%
54%
13%
15%
34%
22%
21%
32%
Independent
walk before
fracture
Walking with
help before
fracture
cognitively
intact
mild to
moderate CI
severe
CI
cognitively
intact
mild to
moderate CI
severe
CI
Rehabilitation
facilities Home Long-term
care
Bendini et al. Equality in access to rehabilitation after hip fracture: a prospective observational study 3° FFN Global Congress. Madrid 2014

Demenza come fattore di rischio dopo la frattura
Vochteloo et al. • Risk factors for failure to return to the pre-fracture place of residence after hip fracture. Arch Orthop Trauma Surg 2014
Risk factors known at admission for failing to return to their own home
Take home message
Patients with
cognitive impairment
and hip fracture
Long term
outcomes
Il paziente con fratture di femore e deterioramento cognitivo ha maggiori probabilità
di avere risultati negativi rispetto alla popolazione generali con frattura di femore.
L’approccio multidimensionale di tipo ortogeriatrico che include la precocità
dell’intervento chirurgico e della mobilizzazione, l’intervento nutrizionale, la
prevenzione delle complicanze, l’ottimizzare dei livelli di emoglobina e dei fluidi, è in
grado di migliorare gli outcome soprattutto dei pazienti più fragili compresi quelli con
deterioramento cognitivo.
I pazienti con deterioramento cognitivo, almeno lieve-moderato, hanno le stesse
probabilità di recupero funzionale dei pazienti integri dal punto di vista cognitivo e
non dovrebbero essere esclusi dai servizi riabilitativi,