sila thonglai md. bangkok eye center bangkok … sila, ocular... · acute hordeolum preseptal...
TRANSCRIPT
SILA THONGLAI MD.
Bangkok Eye center Bangkok Hospital
Thailand
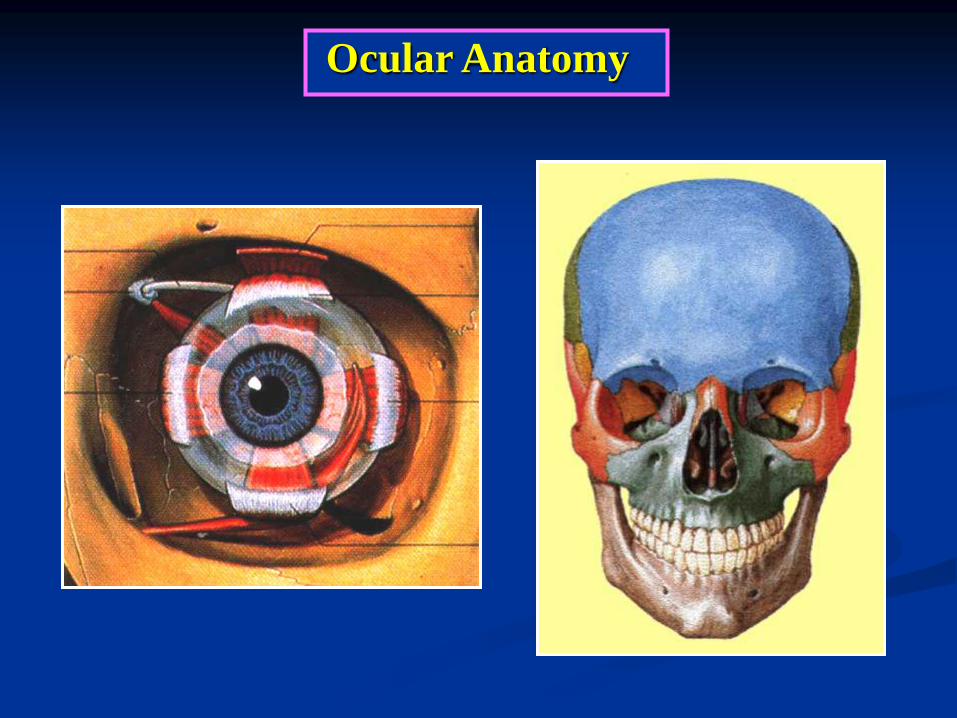
Ocular Anatomy

1. Frontal bone
2. Zygomatic bone
3. Maxillary bone
4. Sphenoid bone
5. Ethmoid bone
6. Lacrimal bone
7. Palatine bone
1
2 3
4 5
6
7
Bony Components of Orbit
Size 30 x 40 x 45 mm
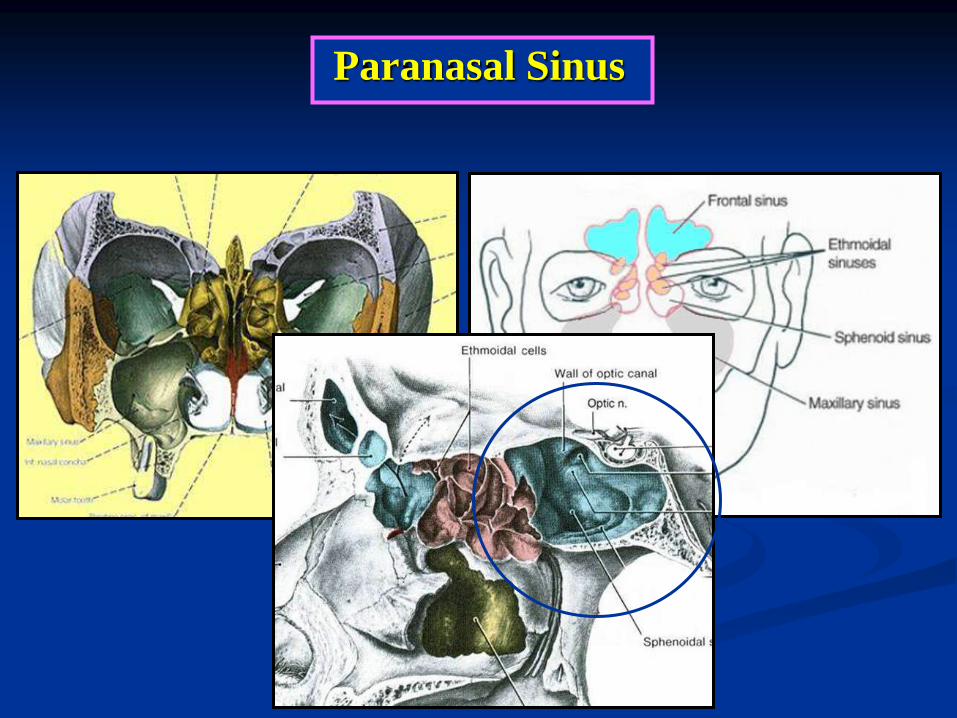
Paranasal Sinus
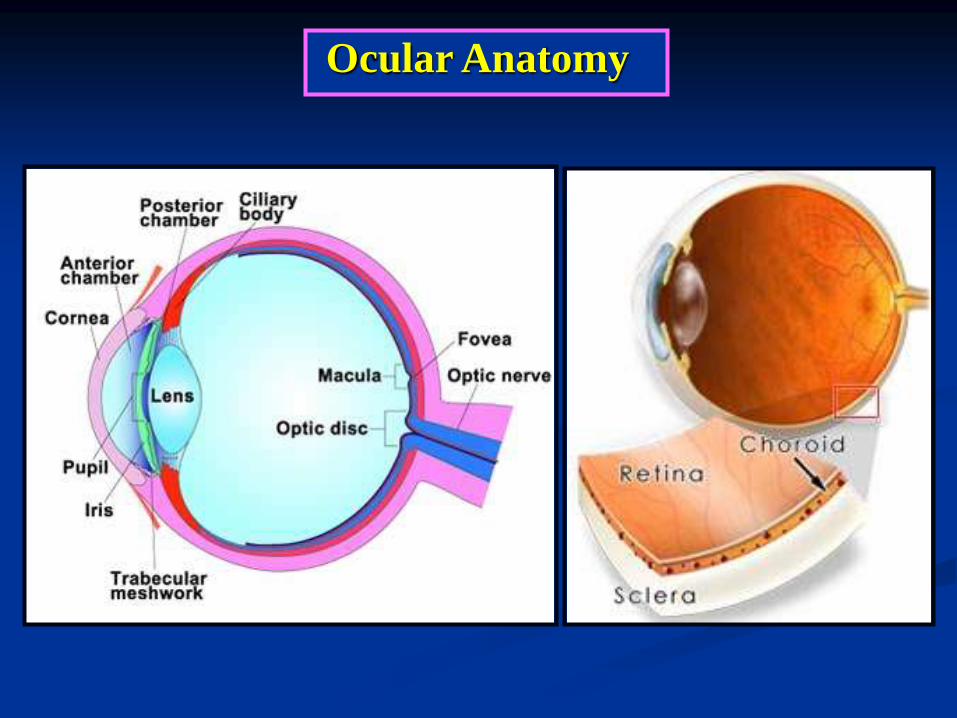
Ocular Anatomy
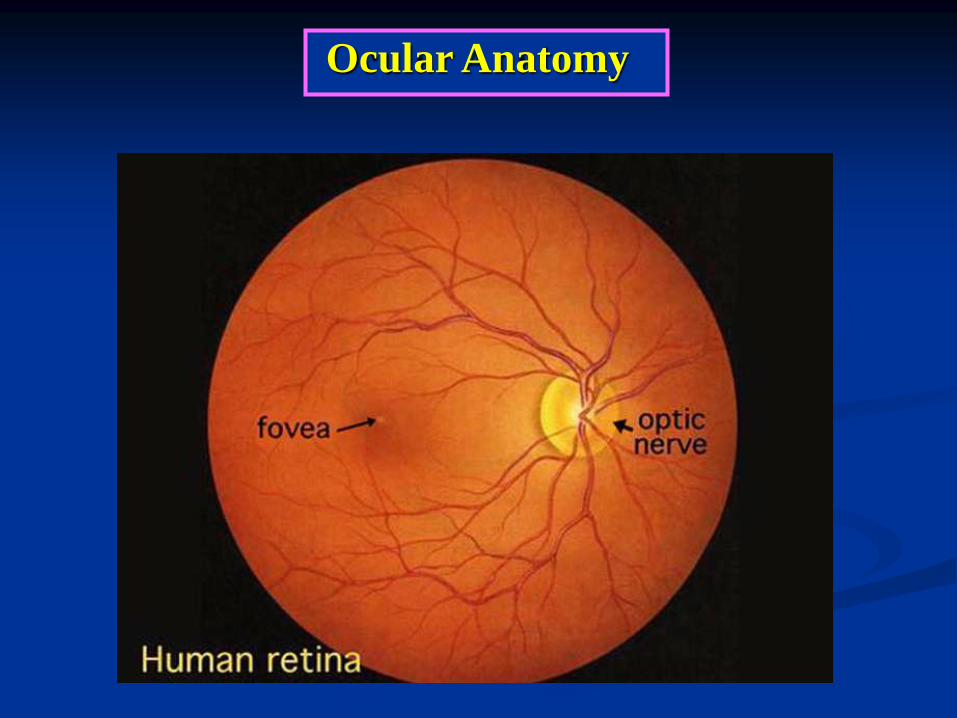
Ocular Anatomy
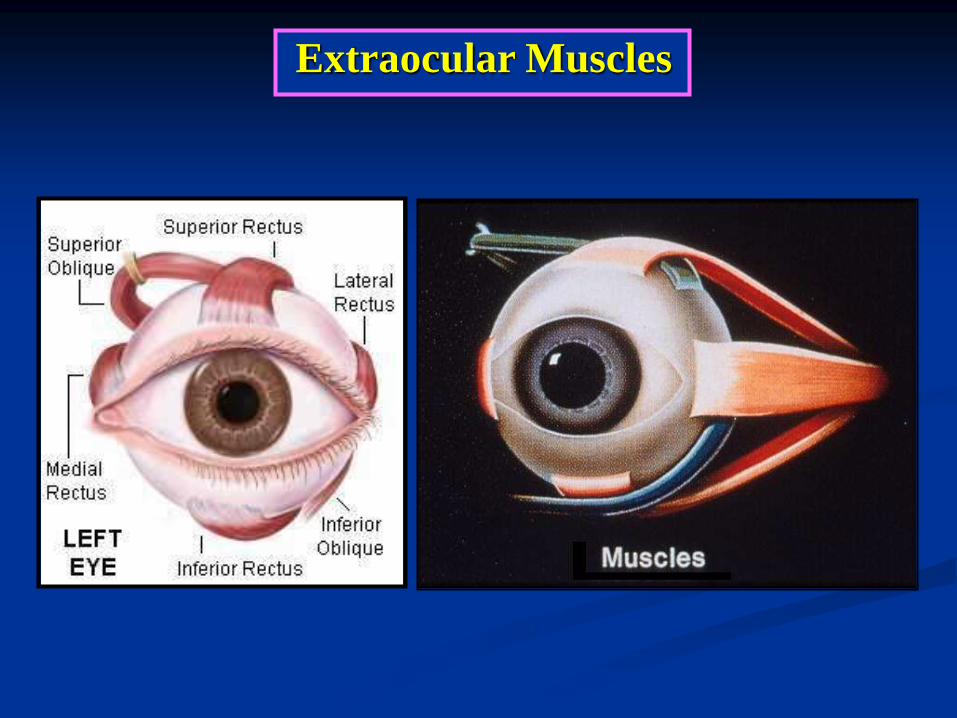
Extraocular Muscles
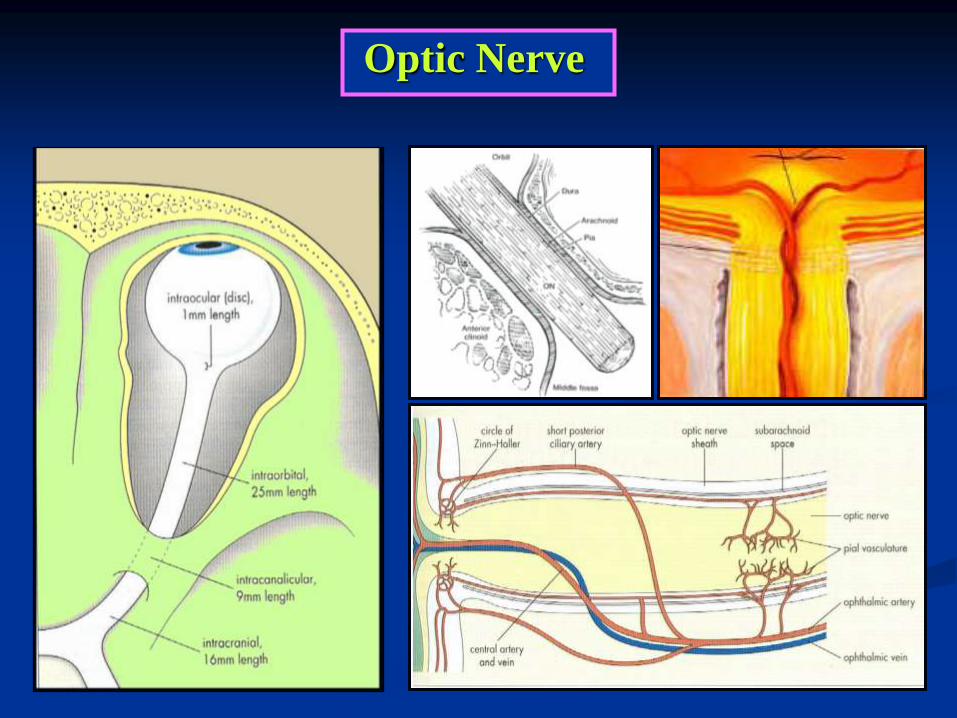
Optic Nerve
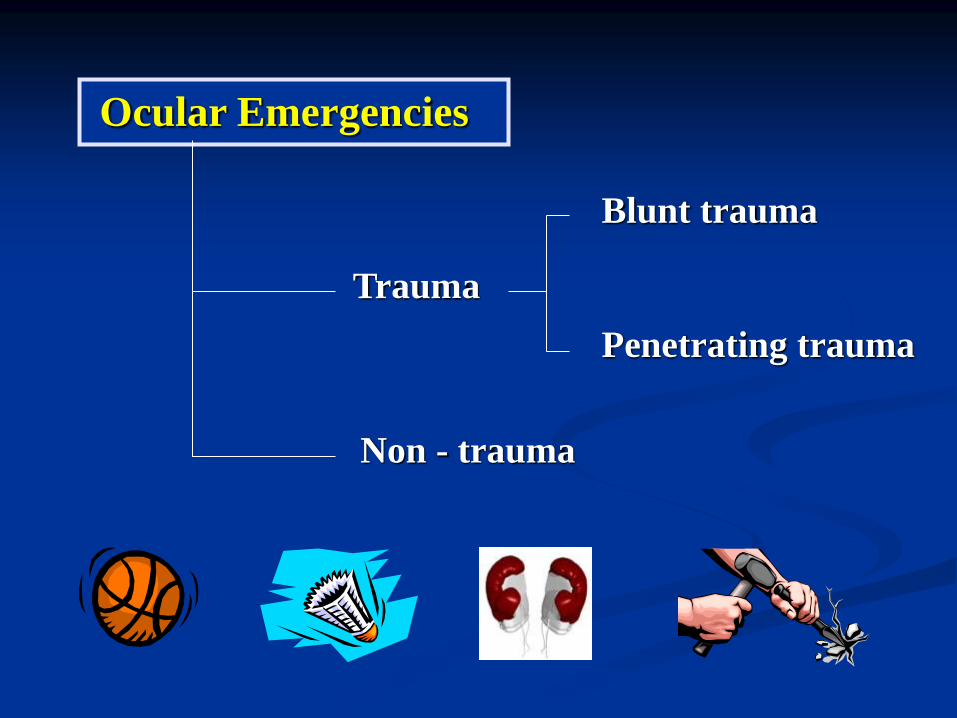
Ocular Emergencies
Trauma
Non - trauma
Blunt trauma
Penetrating trauma
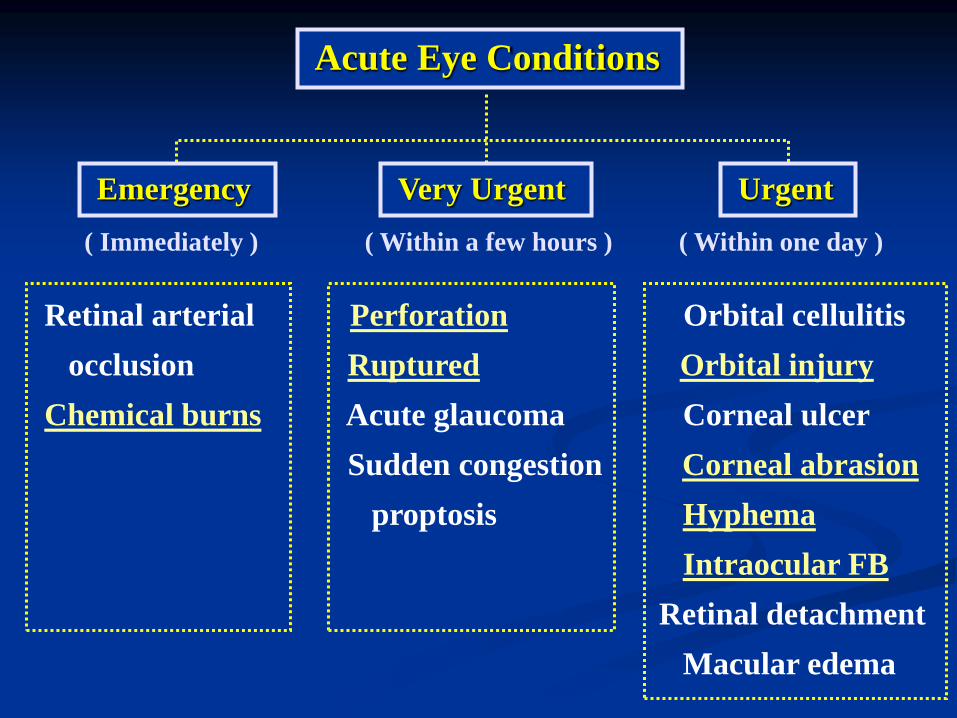
Retinal arterial Perforation Orbital cellulitis
occlusion Ruptured Orbital injury
Chemical burns Acute glaucoma Corneal ulcer
Sudden congestion Corneal abrasion
proptosis Hyphema
Intraocular FB
Retinal detachment
Macular edema
( Immediately ) ( Within a few hours ) ( Within one day )
Acute Eye Conditions
Emergency Very Urgent Urgent
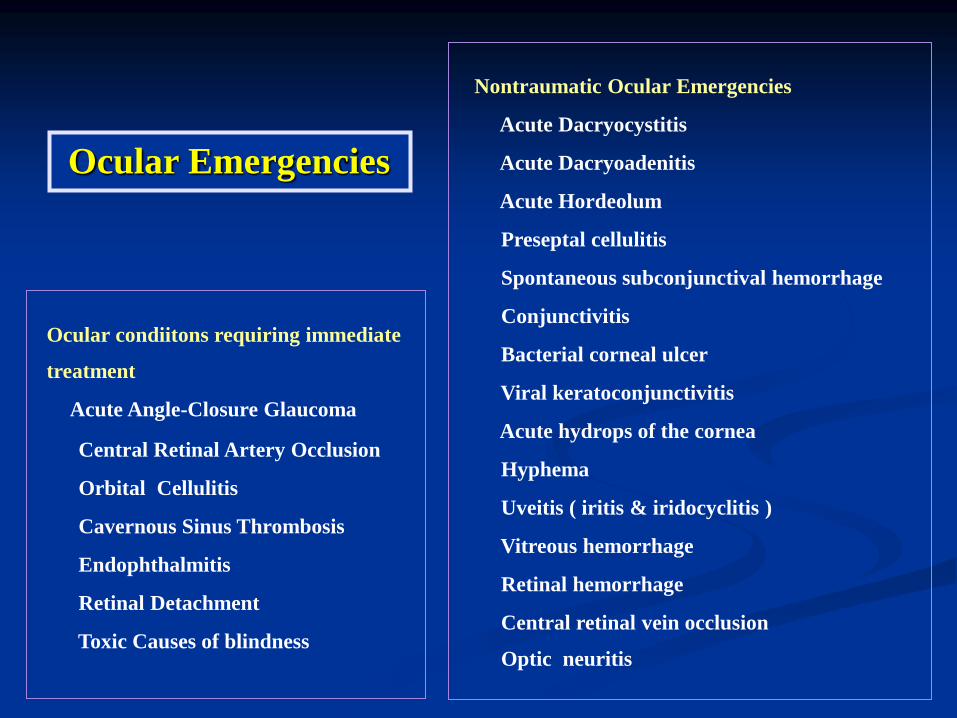
Ocular condiitons requiring immediate
treatment
Acute Angle-Closure Glaucoma
Central Retinal Artery Occlusion
Orbital Cellulitis
Cavernous Sinus Thrombosis
Endophthalmitis
Retinal Detachment
Toxic Causes of blindness
Nontraumatic Ocular Emergencies
Acute Dacryocystitis
Acute Dacryoadenitis
Acute Hordeolum
Preseptal cellulitis
Spontaneous subconjunctival hemorrhage
Conjunctivitis
Bacterial corneal ulcer
Viral keratoconjunctivitis
Acute hydrops of the cornea
Hyphema
Uveitis ( iritis & iridocyclitis )
Vitreous hemorrhage
Retinal hemorrhage
Central retinal vein occlusion
Optic neuritis
Ocular Emergencies

Ocular burns and trauma
Ocular Burn
Alkali Burns
Acid Burns
Thermal Burns
Burns Due to Ultraviolet Radiation
Mechanical Trauma to the Eye
Penetrating or Perforating injuries
Blunt Trauma to the Eye, Adnexa,& Orbit
1. Ecchymosis of the Eyelids
2. Lacerations of the Eyelids
3. Orbital hemorrhage
4. Fracture of the Ethmoid bone
5. Blowout Fractures of the Floor of the Orbit
6. Corneal Abrasions
7. Corneal & Conjunctival Foreign Bodies
Ocular Emergencies
Eye Examination
Visual acuity
External Eye : orbit, periorbital skin, eyelids
Confrontation visual fields
Ocular motility

Anterior Segment
Conjunctiva
Cornea
Anterior chamber
Iris
Lens
Pupils : RAPD
Eye Examination
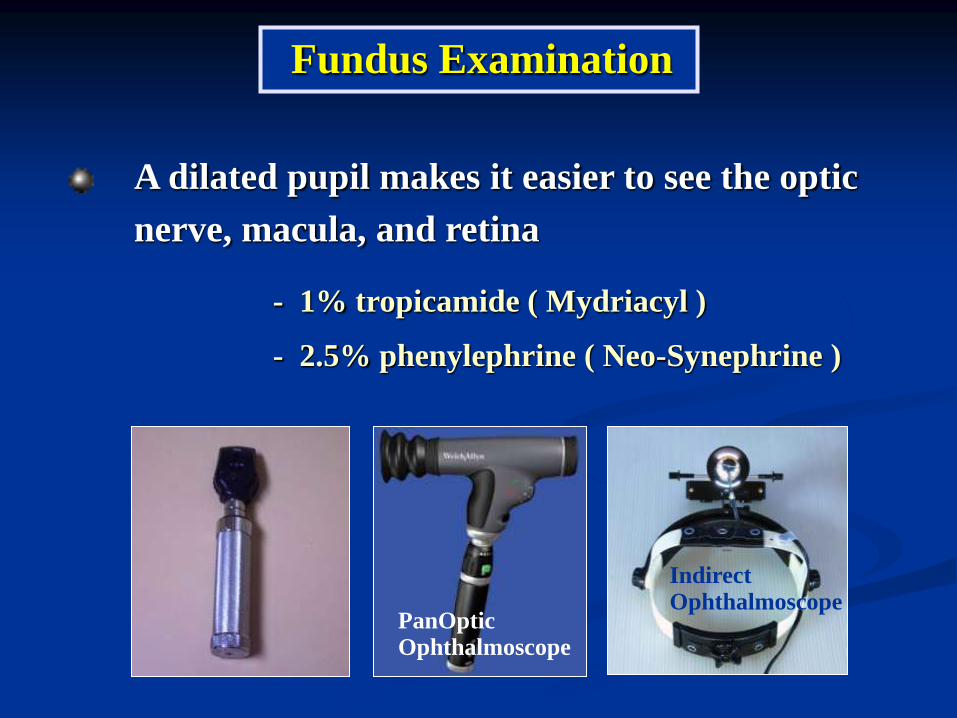
A dilated pupil makes it easier to see the optic
nerve, macula, and retina
- 1% tropicamide ( Mydriacyl )
- 2.5% phenylephrine ( Neo-Synephrine )
PanOptic Ophthalmoscope
Indirect Ophthalmoscope
Fundus Examination
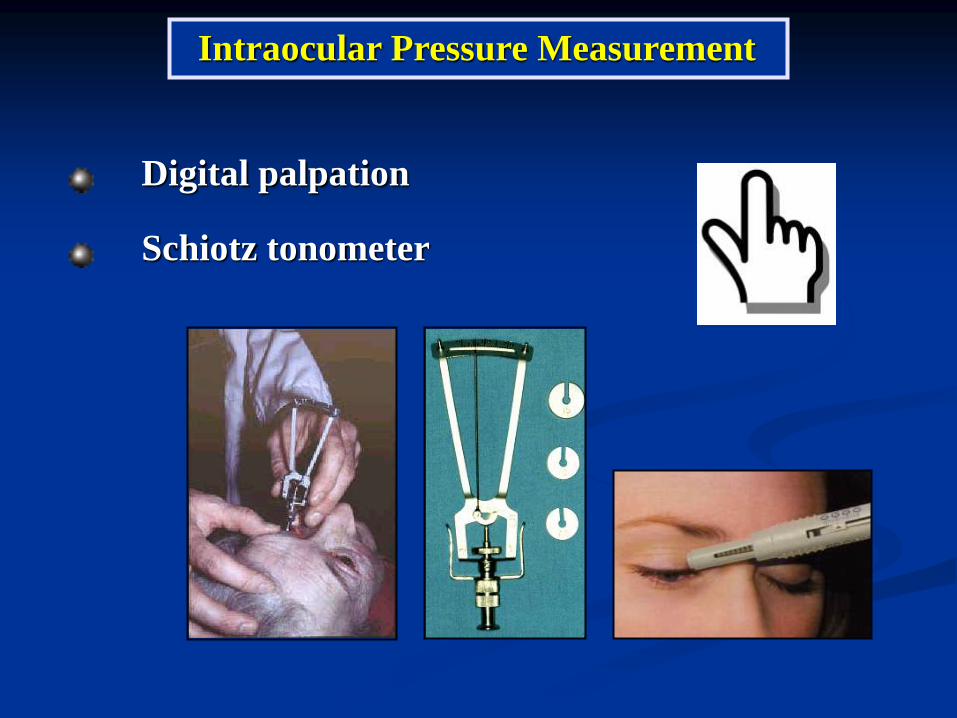
Digital palpation
Schiotz tonometer
Intraocular Pressure Measurement
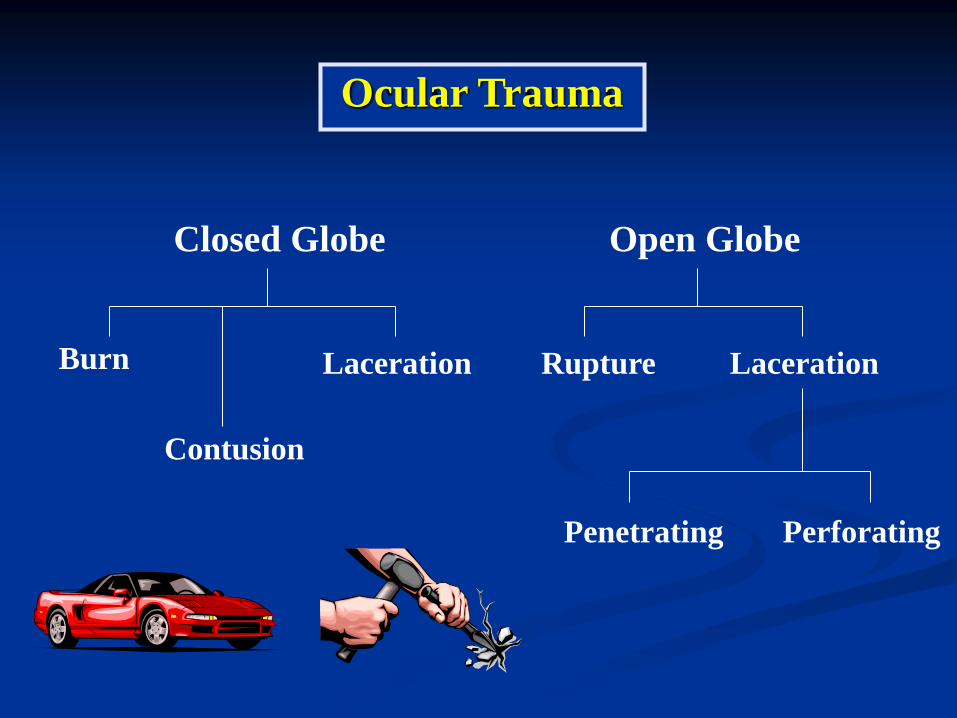
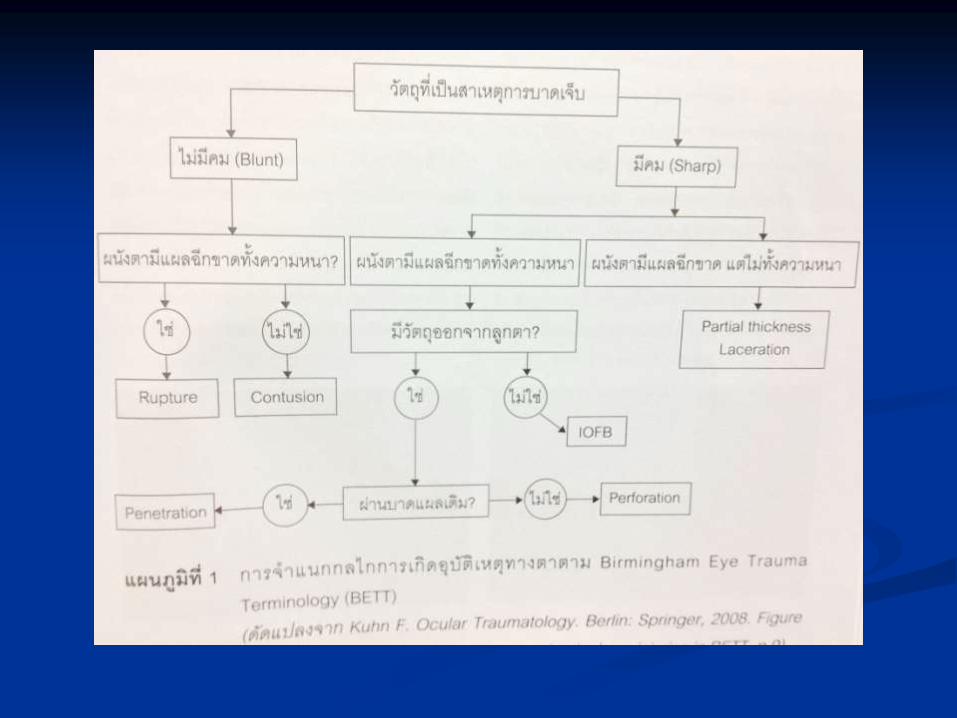
Ocular Trauma
Closed Globe Open Globe
Burn
Contusion
Laceration Laceration
Penetrating Perforating
Rupture
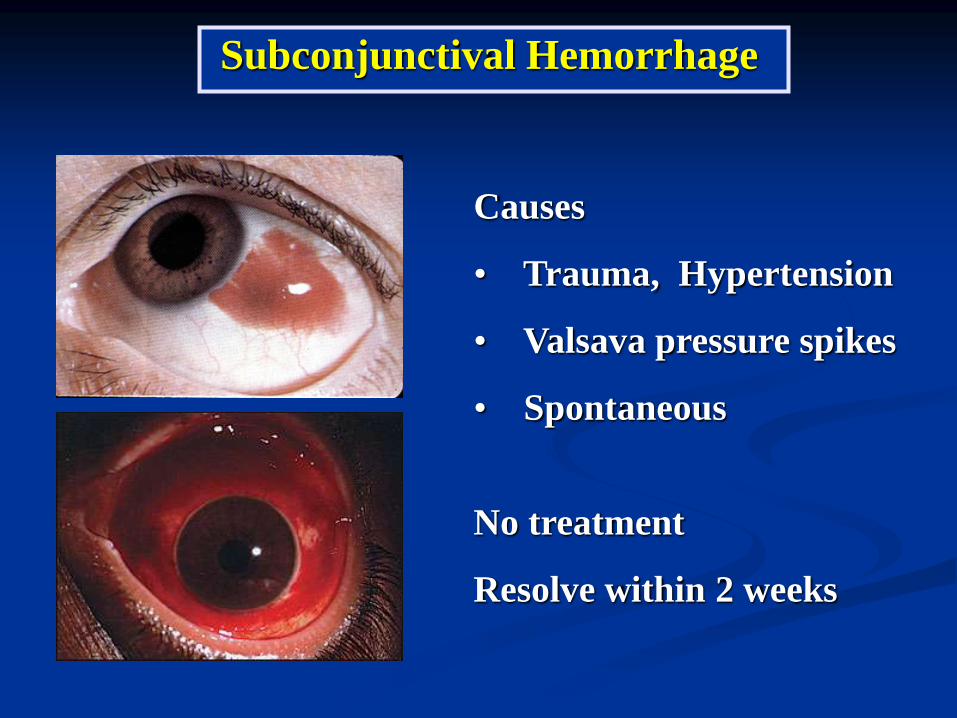
Causes
• Trauma, Hypertension
• Valsava pressure spikes
• Spontaneous
No treatment
Resolve within 2 weeks
Subconjunctival Hemorrhage
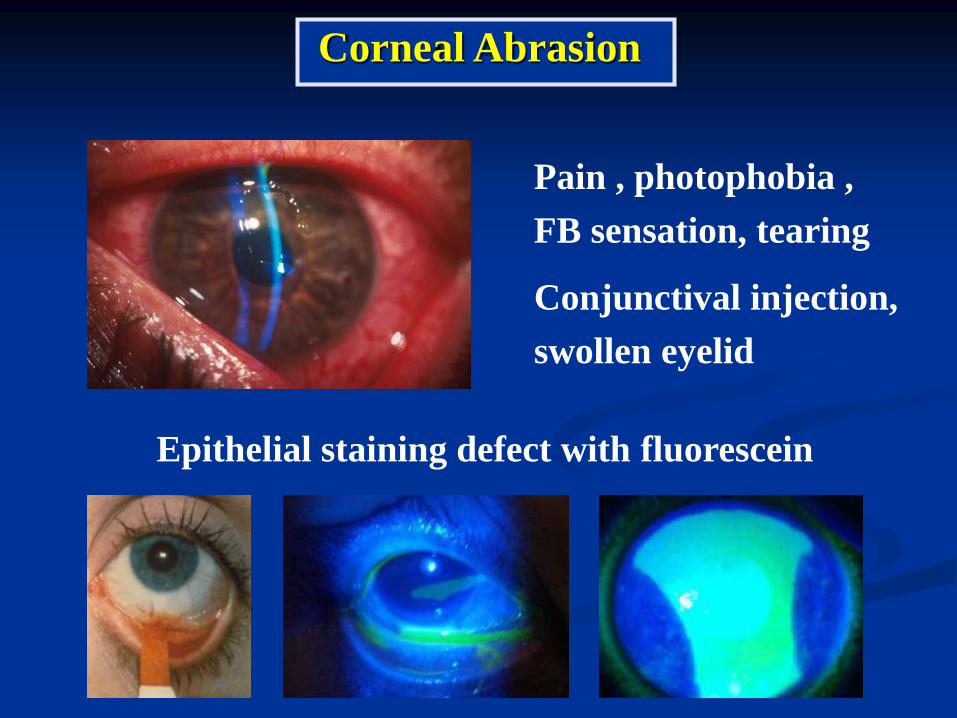
Pain , photophobia ,
FB sensation, tearing
Conjunctival injection,
swollen eyelid
Epithelial staining defect with fluorescein
Corneal Abrasion

Conjunctival Foreign Bodies
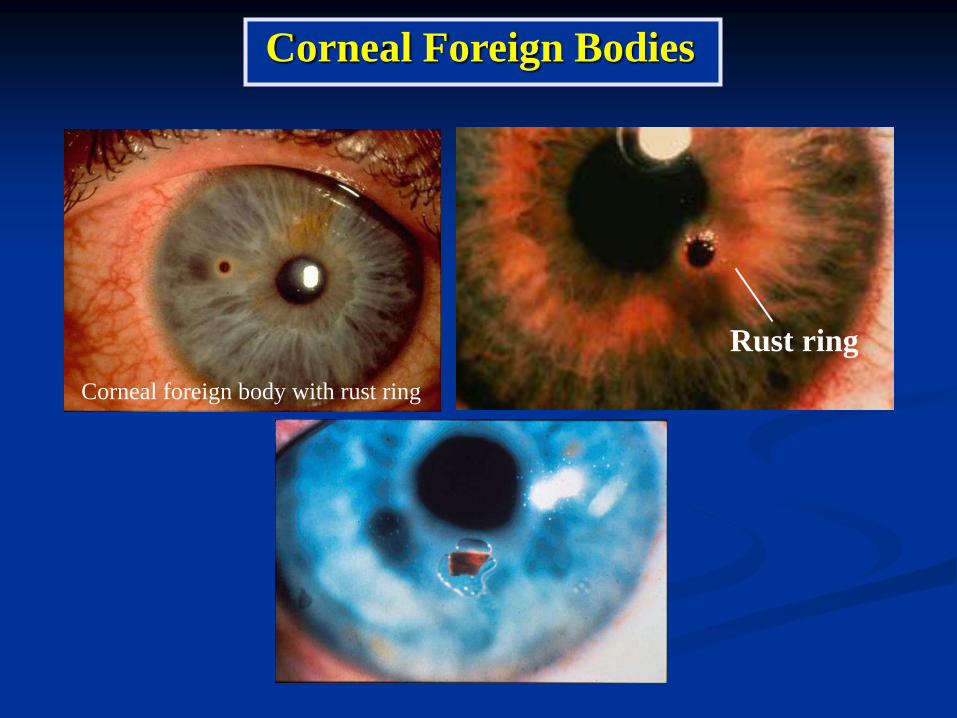
Corneal foreign body with rust ring
Rust ring
Corneal Foreign Bodies
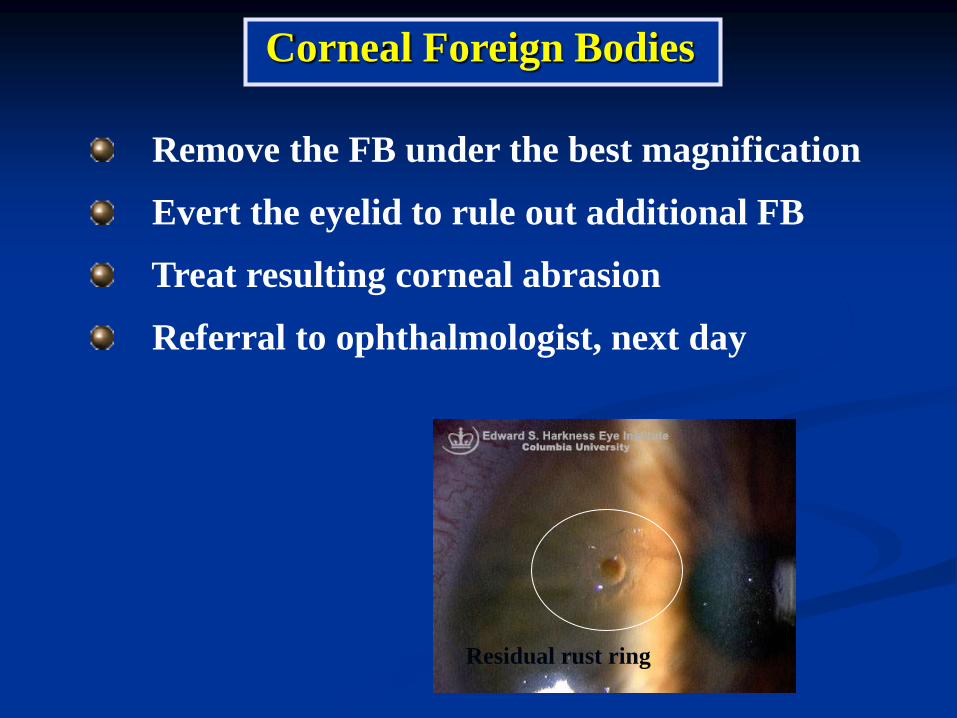
Remove the FB under the best magnification
Evert the eyelid to rule out additional FB
Treat resulting corneal abrasion
Referral to ophthalmologist, next day
Residual rust ring
Corneal Foreign Bodies

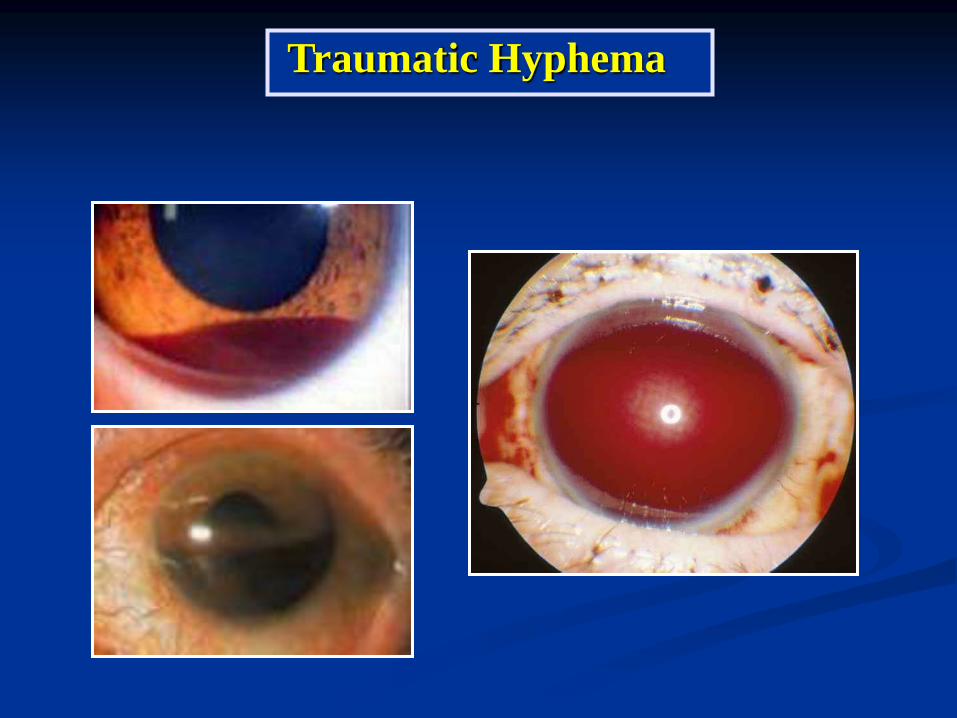
Disruption of blood vessels in the iris or ciliary body
Blood in anterior chamber
Traumatic Hyphema

Grade Size of Hyphema
0 No layered blood circulating red blood cells only
I Less than 1/3
II 1/3 to 1/2
III 1/2 to less than total
IV Total
Traumatic Hyphema : Classification
Traumatic Hyphema
Elevate the patient’s head
Bed rest
1% atropine one drop 3-4 times daily
1% prednisolone acetate one drop 3-4 times daily
If the globe is intact, measure IOP
Reduce IOP
Ophthalmology consult
Traumatic Hyphema : Management
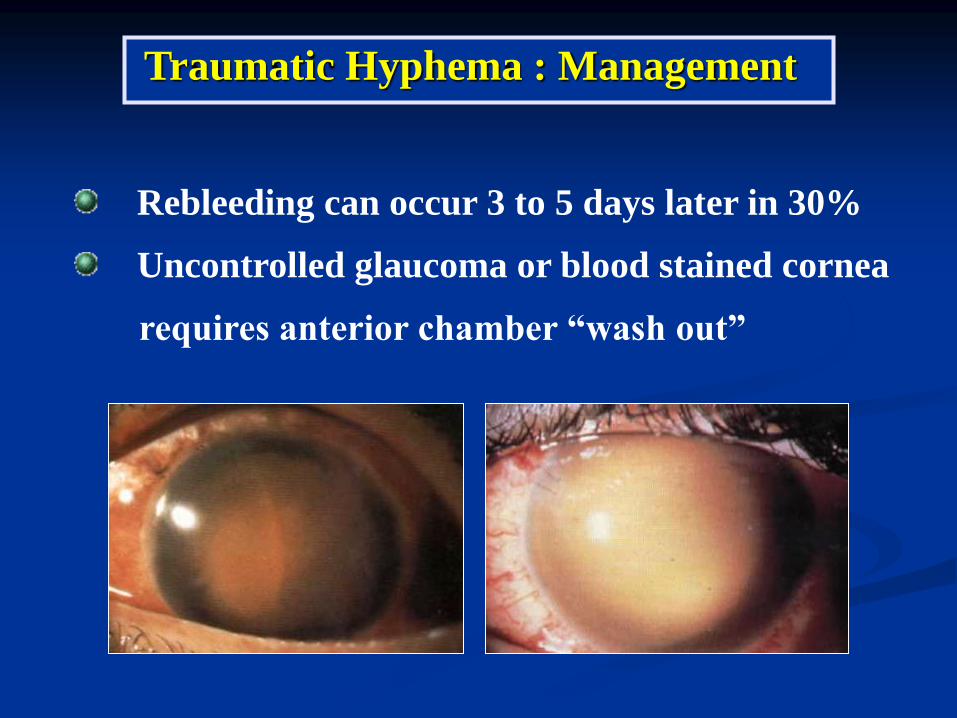
Rebleeding can occur 3 to 5 days later in 30%
Uncontrolled glaucoma or blood stained cornea
requires anterior chamber “wash out”
Traumatic Hyphema : Management
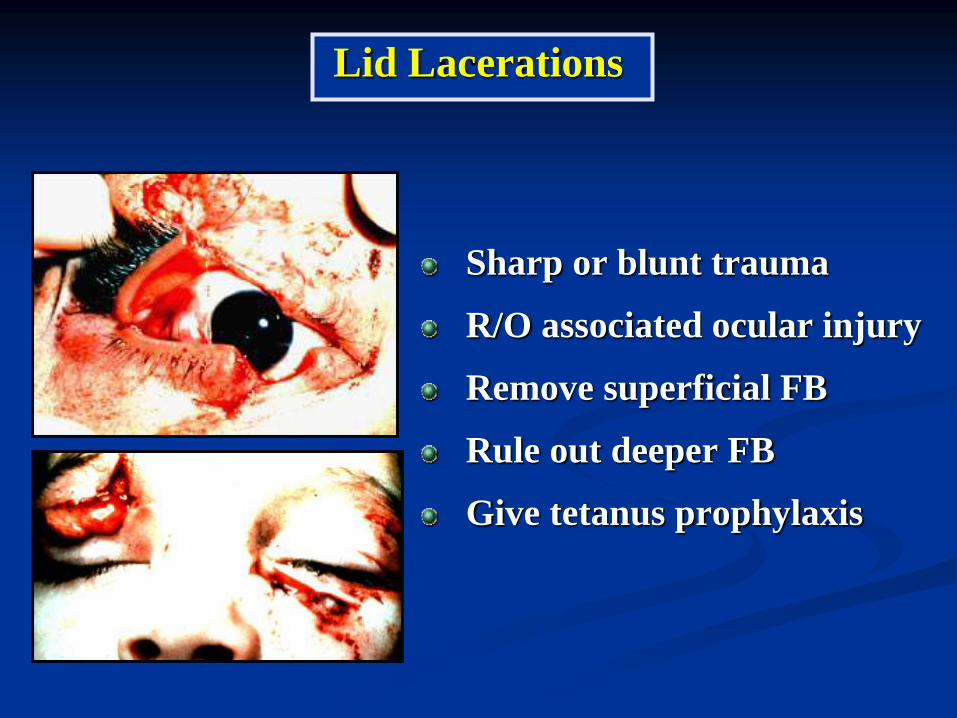
Sharp or blunt trauma
R/O associated ocular injury
Remove superficial FB
Rule out deeper FB
Give tetanus prophylaxis
Lid Lacerations

Tear lid margin
Full Thickness Lid Lacerations
- Gray line
- Lash line
- Mucocutaneous junction

Laceration of lower eyelid margin Post-operative result following a primary repair
Lid Margin Repair
Refer to ophthalmologist if there are
associated ocular injuries
Lid Lacerations
Ruptured globe
Lacrimal drainage system
Levator aponeurosis
Medial canthal tendon
Tissue loss ( > 1/3 )

Lid Lacerations with tear canaliculi

Canalicular Repair
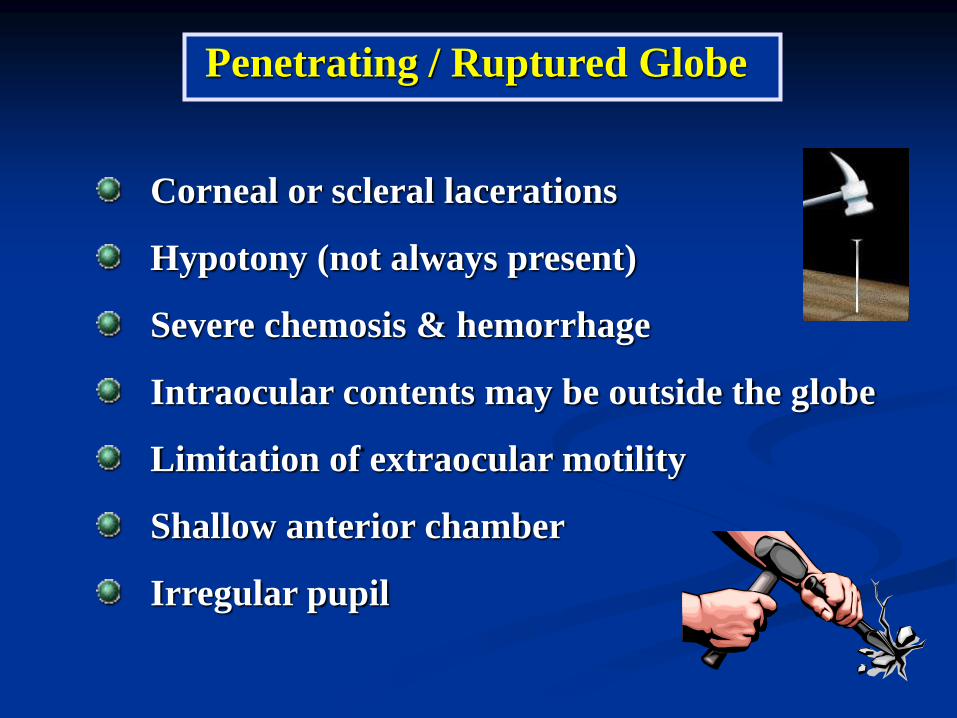
Penetrating / Ruptured Globe
Corneal or scleral lacerations
Hypotony (not always present)
Severe chemosis & hemorrhage
Intraocular contents may be outside the globe
Limitation of extraocular motility
Shallow anterior chamber
Irregular pupil
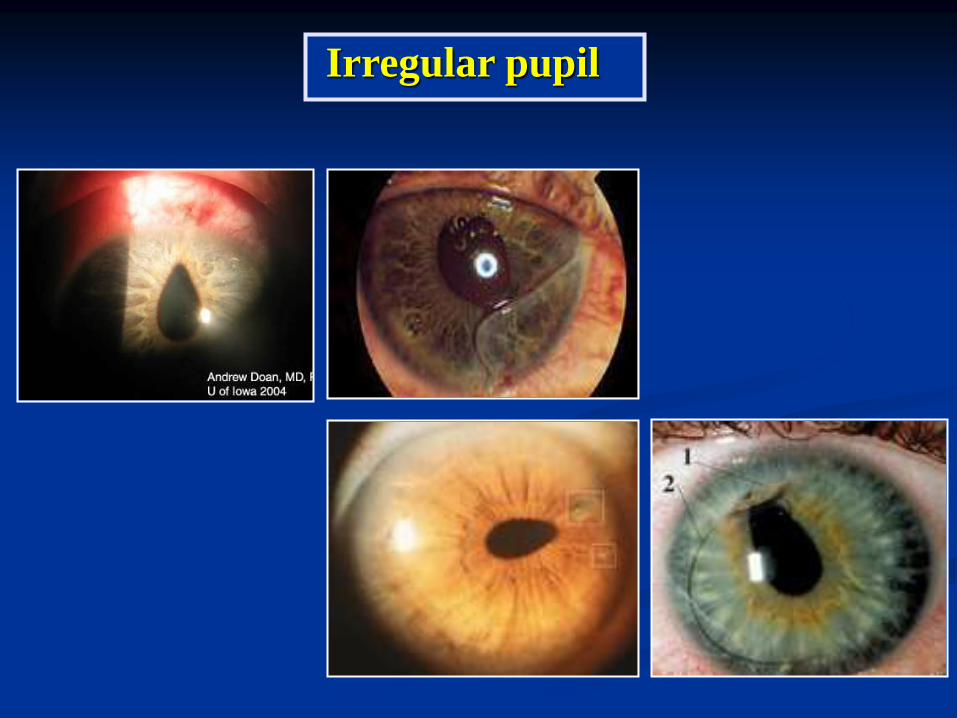
Irregular pupil

Penetrating / Ruptured Globe
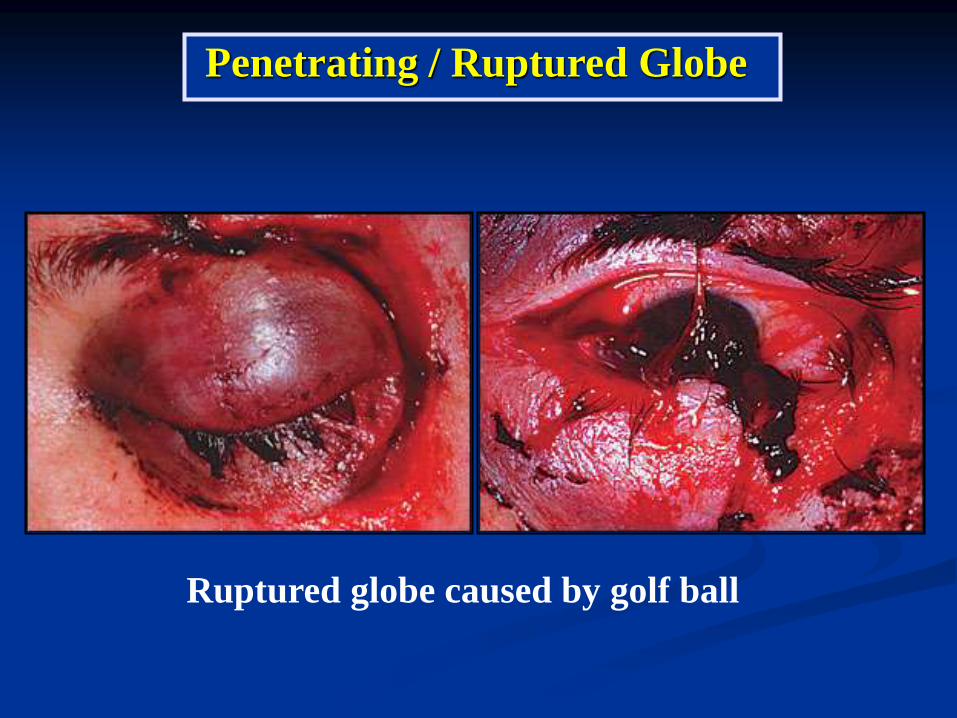
Ruptured globe caused by golf ball
Penetrating / Ruptured Globe

Penetrating / Ruptured Globe : Management
Stop examination
Shield the eye (do not patch)
Give tetanus prophylaxis
NPO and systemic antibiotics
Do not apply eye ointment or eye drop
Film orbit if IOFB can’t be R/O
Refer immediately to ophthalmologist

Intraocular or Intraorbital Foreign Bodies
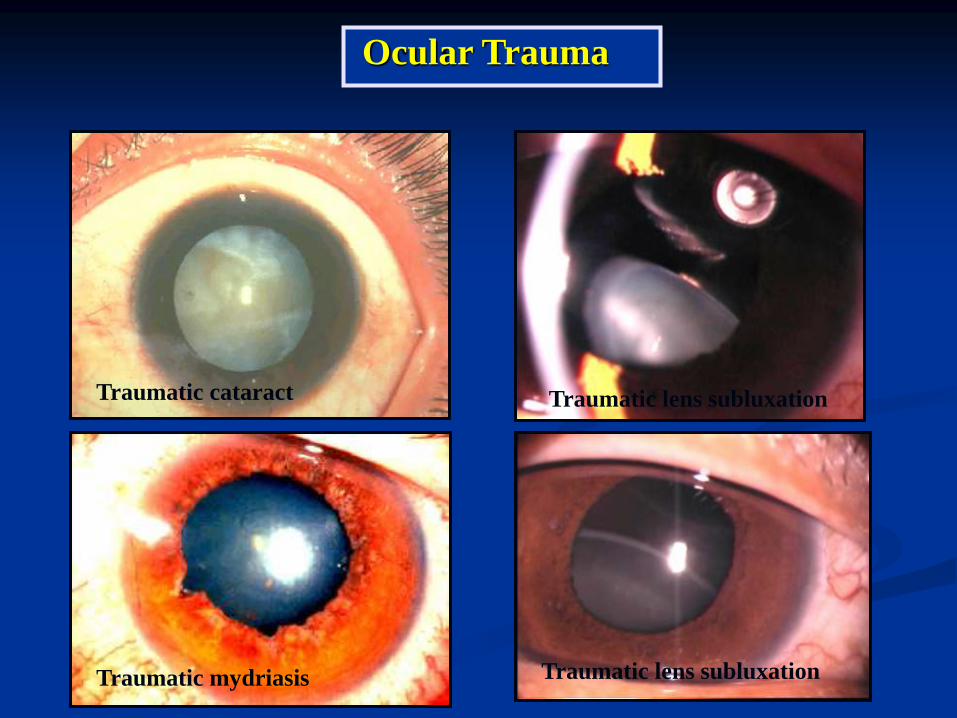
Ocular Trauma
Traumatic cataract
Traumatic mydriasis Traumatic lens subluxation
Traumatic lens subluxation






Traumatic Optic Neuropathy :
Classification and Mechanisms
Direct injury
- Penetrating injury from knife, projectile
- Injury from fractured bone
- Avulsion, transection
Indirect injury
- Contusion with transmission of force through bone
- Compression secondary to orbital hemorrhage or
intrasheath hemorrhage
Clinical Features of Traumatic Optic Neuropathy
Most commonly unilateral
May be overlooked in setting of significant
globe or maxillofacial trauma
Reduced visual acuity ( NLP to 20/20 )
Visual field defect : No pathognomonic defect
Normal optic disc with development of optic
atrophy
Medical Management Options
Steroids : Controversial
- Thought to limit free-radical amplification
of the injury response
- Dosages ( low, high, mega)
- May be harmful
Observation : 57% of untreated patients shown
to have 3 lines or more acuity improvement

Surgical Management Options
Lateral canthotomy and cantholysis for orbital
hemorrhage
Surgical decompression of the optic nerve
within its canal
There is no defined standard protocol of
treatment for indirect optic nerve injury .

True ocular emergency
Both acid and alkali burns can be blinding
- Acid burns tend to coagulate proteins, limiting
the depth of penetration.
- Alkali burns can rapidly penetrate the cornea,
causing damage to intraocular structures.
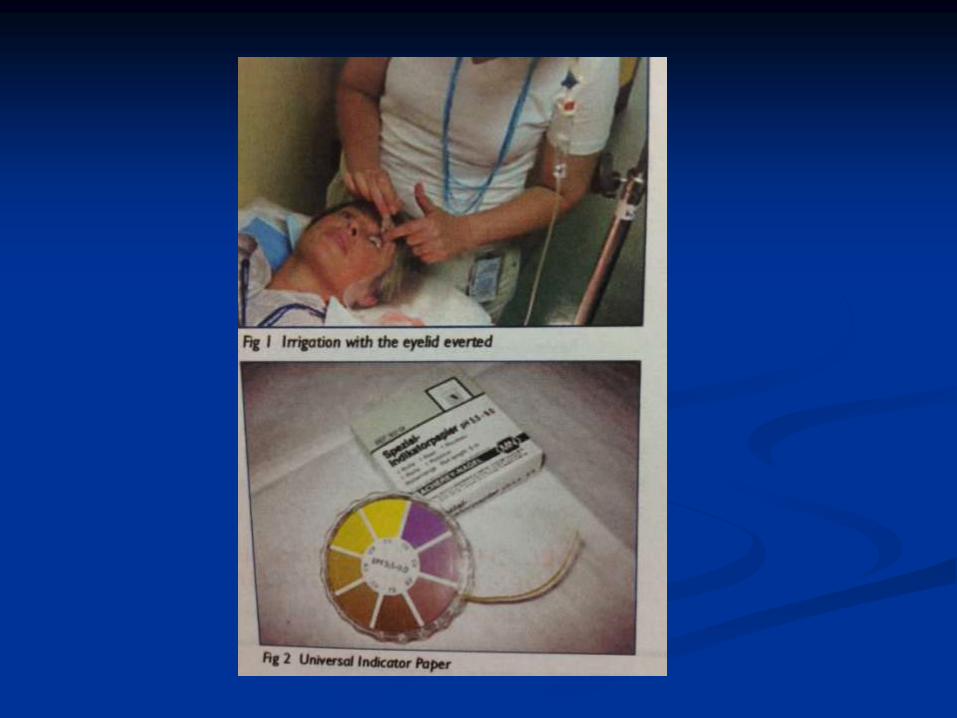
Chemical Ocular Injury

Immediate copious irrigation with a minimum of
1-2 L of saline or until pH is normalized ( 6.8-7.7 )
- Instill a topical anesthetic
- Use eyelid retractor
- Double eversion of the eyelids
Chemical Ocular Injury : Management
Immediate copious irrigation with a minimum of
1-2 L of saline or until pH is normalized ( 7.3-7.7 )
- Instill a topical anesthetic
- Use eyelid retractor
- Double eversion of the eyelids
Chemical Ocular Injury : Management
Ophthalmologists Referral
No corneal involvement
- ATB + steroid eye drop

Chemical Ocular Injury : Classification
Grade I Grade II
Grade III Grade IV

Chemical Ocular Injury : Management
Preservative-free artificial tears
Topical non-preserved steroid
Topical cycloplegic
Topical antibiotics
Oral analgesics
Pressure patch or bandage CL
Antiglaucoma +

Bilateral Alkali Injuries
Chemical Ocular Injury
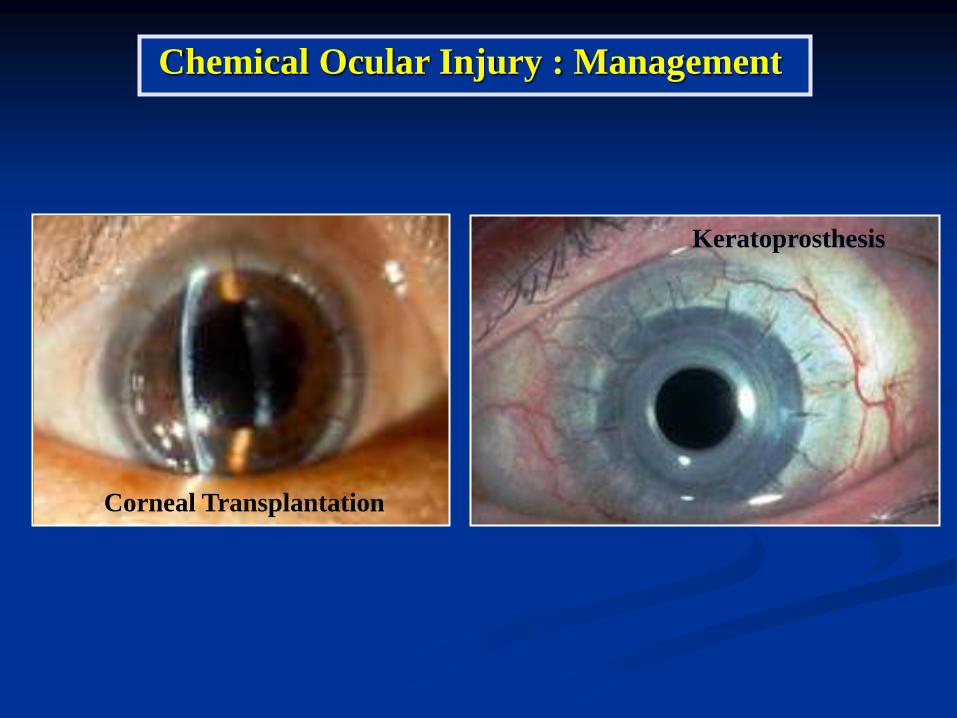
Chemical Ocular Injury : Management
Corneal Transplantation
Keratoprosthesis

Accidental into the eye can cause the lids to
adhere and adhesive clumps to form on the cornea
Not permanently harmful to the eye
Cyanoacrylates are used occasionally directly on the
cornea to seal corneal perforations.
Cyanoacrylate Glue

Moisten the glue with eye ointment, and remove
as much as can be removed easily without causing
damage to underlying tissue
The glue will loosen and become easier to remove
in a few days.
Cyanoacrylate Glue
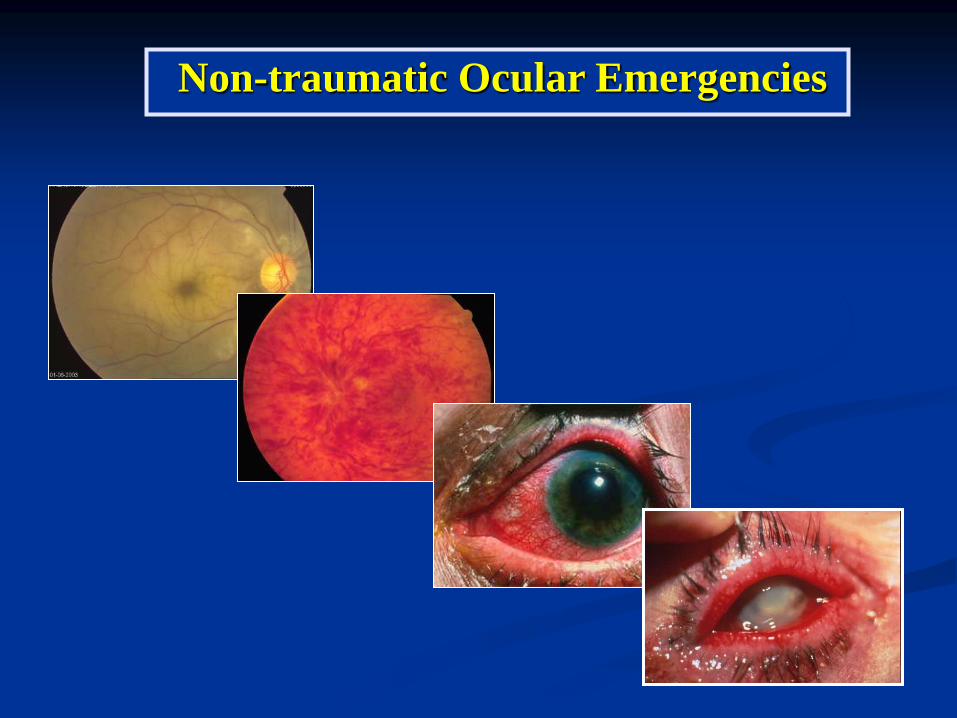
Non-traumatic Ocular Emergencies

Reduce the intraocular pressure
O.5% Timolol 1 drop
2-4 % Pilocarpine 1 drop every 15 minutes
20% Mannitol 250-500 ml IV drip
Acetazolamide 500 mg oral
100% Glycerin 1 cc/kg
Consult ophthalmologist
Acute Angle Closure Glaucoma

A 60-year-old woman with acute, painless loss
of vision in the right eye
Visual acuity CF – LP in 90% of cases
Opaque white retina and attenuated vessels
Central Retinal Artery Occlusion
Treatment must be initiated immediately.
Ocular massage
Inhaled carbogen ( 95% O2 and 5% CO2 )
Reduced intraocular pressure
Central Retinal Artery Occlusion
Consult ophthalmologist immediately
Anterior chamber paracentesis
Direct infusion of t-PA or urokinase in the
ophthalmic artery

Broad spectrum intravenous antibiotics
CT scan orbit
Ophthalmology & ENT consultation
Orbital Cellulitis
Subperiosteal abscess

Preseptal Cellulitis
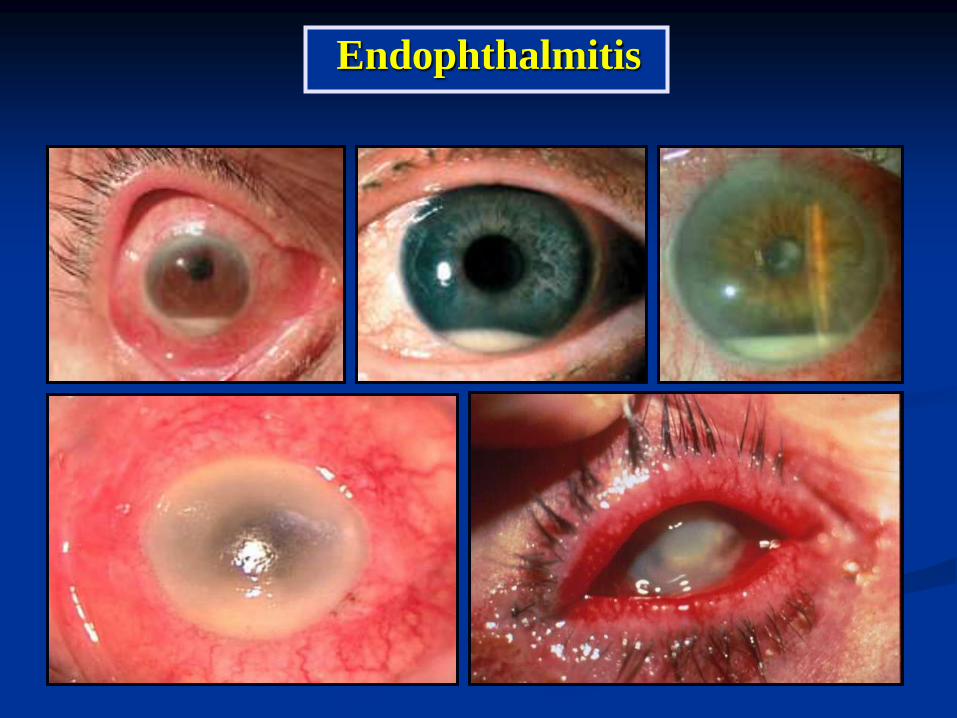
Endophthalmitis

Urgent Neuro-ophthalmology

A 36-year-old-woman with subacute visual loss in
right eye and pain on eye movement
VA 20/200, 20/25 RAPD +ve OD
VF central scotoma OD
Retrobulbar optic neuritis
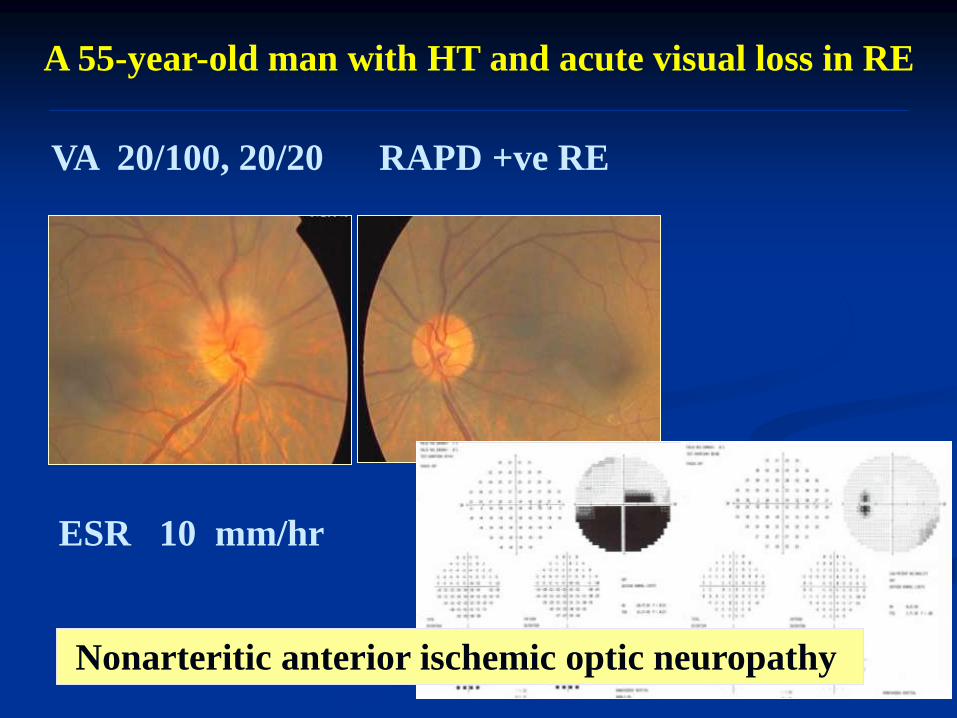
A 55-year-old man with HT and acute visual loss in RE
VA 20/100, 20/20 RAPD +ve RE
Nonarteritic anterior ischemic optic neuropathy
ESR 10 mm/hr

A 73-year-old woman with acute visual loss of right
eye, headache, anorexia and weight loss
VA 10/200, 20/25 RAPD + ve RE
ESR 94 mm/hr, high level of C - reactive protein
Arteritic anterior ischemic optic neuropathy
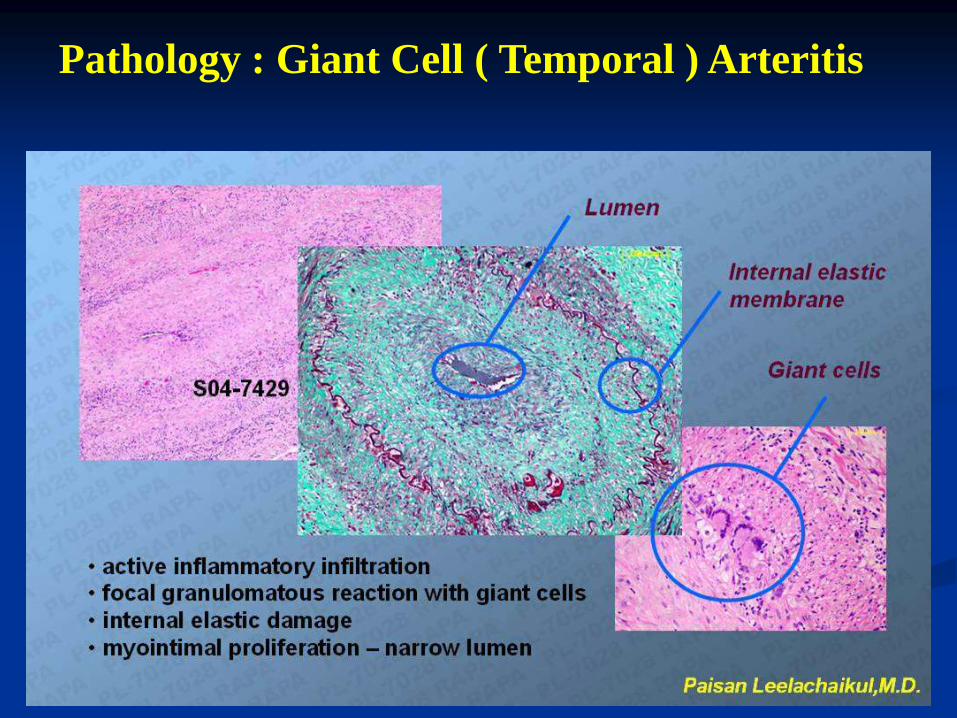
Pathology : Giant Cell ( Temporal ) Arteritis
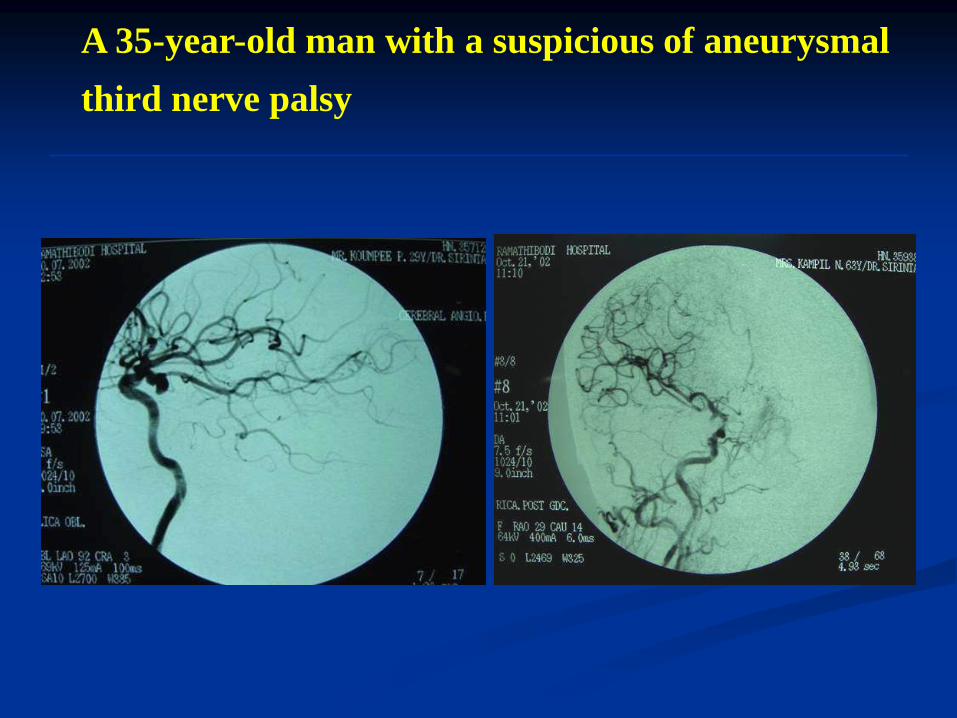
A 35-year-old man with a suspicious of aneurysmal
third nerve palsy

A 40-year-old woman with sudden onset of left
third nerve palsy, visual loss and severe headache
What is the diagnosis?
VA 20/30, LP +ve RAPD LE
References Pisit Preechawat ; Ramathibodi Hospital
Birmingham Eye Trauma Terminology ;
( Kuhn F.Ocular Traumatology Berlin 2008 )
Eye Emergency Manual 2nd Edition ; NSW Deparment of Health
Australin
Manament of Ocular Emergencies 5th Revised Edition ; Raymond
Stein, Harold Stein 2010 Montreal, Quebec Canada
Ocular Emergencies ; American Family Physician Journal Sep 15,2007
