shoulder impingement : the surgeon's approach
TRANSCRIPT

Subacromial Impingement Surgeon’s Approach
Mr Mike WaltonConsultant Shoulder Surgeon


Impingement
• Theory of EXTRINSIC impingement
• Neer (1972) - Anterior acromioplasty for chronic impingement of the shoulder, “a preliminary study” JBJS(Am) 54(1):41-50

Subacromial Decopression
• “Impingement on the tendinous portion of the rotator cuff by the coraco-acromial ligament and the anterior third of the acromion is responsible for a characteristic syndrome of disability of the shoulder. A characteristic proliferative spur and ridge has been noted on the anterior lip and undersurface of the anterior process of the acromion and this area may also show erosion and eburnation. The treatment of the impingement is to remove the anterior edge and undersurface of the anterior part of the acromion with the attached coraco-acromial ligament.”

Subacromial Decopression
• “Fifty shoulders in forty-six patients have been subjected to anterior acromioplasty during the past five years. Nineteen had proliferative bursitis and tendinitis or partial tears of the supraspinatus, without roentgenographic evidence of calcium deposits, and twenty had complete tears of the supraspinatus and the results in these thirty-nine patients from one to five years following surgery were good. Eleven patients with residual impingement following partial lateral acromionectomy were improved but their results were impaired by pre-existent deltoid weakness and scar”
• McShane 1987, Hawkins 1988, Bigliani 1989

Bigliani Classification
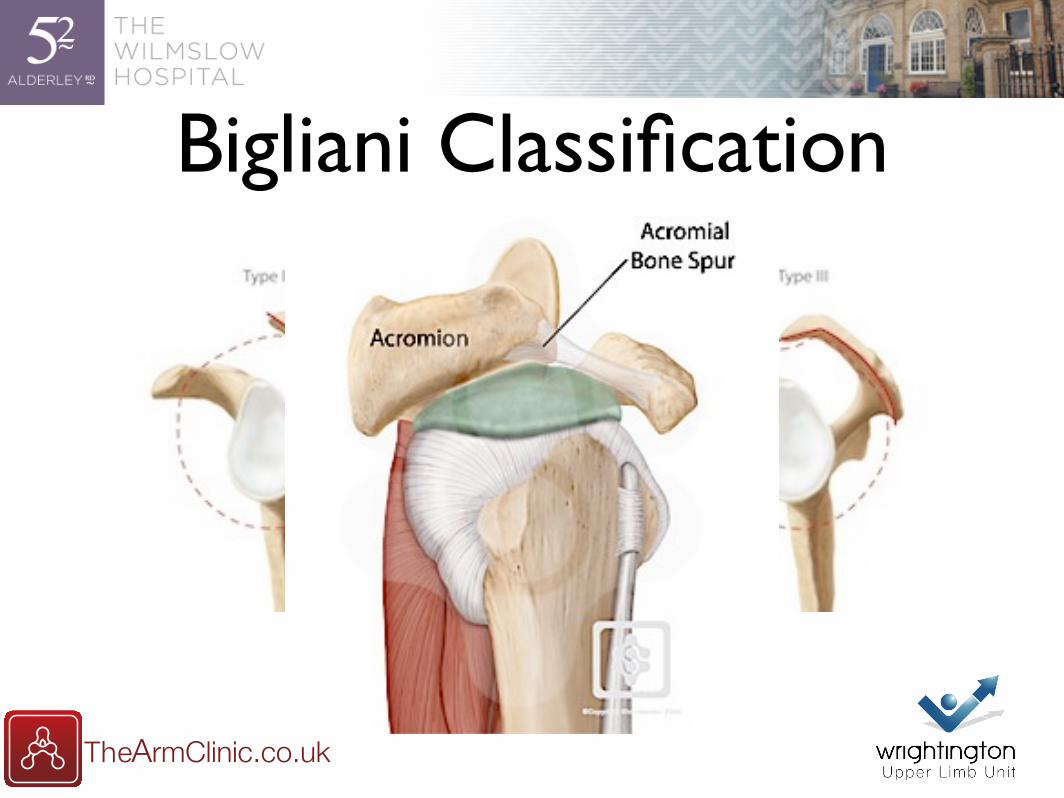
Bigliani Classification

Acromial Spurs
• Type III acromions associated with cuff disease (Bigliani 1991, Balke 2013)
• Anterior and Lateral spurs associated with full thickness cuff tears (Nyffeler 2006, Ames 2012, Fujisawa 2014)

Extrinsic Theory
• Acromionplasty
• reduces extrinsic compression
• improves visualisation during cuff repair
• induces healing response through bleeding

Arthroscopy
• Developed over the course of the 1980s and early 1990
• Ellman (1987) - Arthroscopic subacromial decompression: analysis of 1-3 year results. Arthroscopy 3(3):173-181

• “Forty (80%) of the cases had advanced stage II impingement without rotator cuff tear. Ten (20%) had full-thickness tears of the rotator cuff. Patients were evaluated pre and postoperatively on the UCLA Shoulder Rating Scale, which includes an assessment of pain, function, range of motion (ROM), strength, and patient satisfaction. Eighty-eight percent of the cases were rated "satisfactory" (excellent or good), and 12% were rated "unsatisfactory" (fair or poor). The procedure is technically demanding, and to achieve a satisfactory result the criteria of open anterior acromioplasty must be met.”
Arthroscopy

Arthroscopic SubAcromial

Bigliani Classification

Extrinsic Problems
• Codman EA (1934) - The Shoulder: Rupture of the suprapsinatus tendon and other lesions in or about the subacromial bursa.
• Rim Rent tear - “deep surface of the cuff is torn at its attachment to the tubersity”

End Result Theory
• “So I am called eccentric for saying in public that hospitals, if they want to be sure of improvement,
• Must find out what there results are
• Must analyse their results, to find their strong and weak points,
• Must compare their results with other hospitals
• Must welcome publicity not only for their successes but also for their errors”
EA Codman

Intrinsic Theory
• Primary tendon degeneration - tendinopathy
• Cuff & acromial pathology “normal variants”
• Address cuff with strengthening and “biological” treatment for tendinopathy

Exercises vs Surgery
• Arthroscopic surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome). Brox JI, Staff PH, Ljunggren AE, Brevik JI. BMJ. 1993 Oct 9;307(6909):899-903
• Exercises versus arthroscopic decompression in patients with subacromial impingement: a randomised, controlled study in 90 cases with a one year follow up. Haahr JP, Østergaard S, Dalsgaard J, Norup K, Frost P, Lausen S, Holm EA, Andersen JH. Ann Rheum Dis. 2005 May;64(5):760-4.

Exercises vs Surgery
• Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: randomised controlled study. Holmgren T, Björnsson Hallgren H, Öberg B, Adolfsson L, Johansson K. BMJ. 2012 Feb 20;344
• Significant improvement with specific exercise programme compared to control
• 80% reduction in patients “needing” surgery

Exercises vs Surgery
• Specific exercise programme is equally effective as subacromial decompression
• But subacromial decompression is as effective as a specific exercise programme with small but significant set of risks

Ketola et al
• No evidence of long-term benefits of arthroscopic acromioplasty in the treatement of shoulder impingement syndrome. 5 year results of a randomised controlled trial. BJR 2013;2:132-9
• Which patients do not recover from shoulder impingement syndrome, either with operative treatment or with non-operative treatment? Acta Orth 2015, 86;6:641-646
• No difference in long-term development of rotator cuff rupture and muscle volumes in impingement patients with or without decompression. Act Orth 2016, 87;4:351-355
Ketola et al
• 140 patient RCT: ASAD vs Home Exercise programme
• No difference at 2 or 5 years between groups
• No long term “protective effect” of SAD on radiological muscle volumes or future rotator cuff tears
Ketola et al
• Poor outcomes observed in
• Longer duration of Sx (over 12 months)
• Marital status (single)
• Long Periods of sick leave
• Lack of professional education

Intrinsic Problems
• The patient has pain and decreased function
• Has usually “tried” rest and physio
• We don't have a biological treatment
• If they fail is it a failure of rehaber or rehabee??

Failure of conservative?
• Education / Expectations / Compliance
• Patient & Physio
• Pain
• The NHS model makes it very hard to coordinate injections with therapy
• Wrong diagnosis

Role of Surgeon
• Establish a diagnosis
• “Impingement” is a symptom
• Age / Activity
• Cuff tear esp traumatic
• Other - calcific tendinitis / frozen / capsulolabral

What Surgery?
• Bursectomy compared with acromioplasty in the management of subacromial impingement syndrome: a prospective randomised study. Henkus HE, de Witte PB, Nelissen RG, Brand R, van Arkel ER. J Bone Joint Surg Br. 2009 Apr;91(4):504-10
• Small numbers
• Bursectomy and ASAD both effective. ASAD slightly more so

What do we achieve?
• No idea!!!
• Removal of extrinsic compression
• Removal of pain generators - bursa, CAL
• Release of blood factors
• Enforced Exercises Post-op
My Conclusions
• Surgery is effective - Evidence and Anecdote
• We operate too frequently but as a result of system failure
• Rehab is often underfunded, under resourced and waiting lists far too long
• Need to focus on why some don't get better rather than ignoring them.