should hypertensive disorders of pregnancy be considered ...€¦ · pregnancy-induced hypertension...
TRANSCRIPT
Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
Pr. Jacques Blacher
Paris-Descartes University ; AP-HP ; Unité HTA, prévention et
thérapeutique cardio-vasculaires, Centre de diagnostic et de thérapeutique,
Hôtel-Dieu, Paris, France
February 2018

Disclosures of Jacques Blacher:
- No financial interest in the capital of a drug
company.
- No lasting connection with a business related to
drugs (employment contract, regular pay...).
- Off interventions related businesses related to
drugs (clinical trials, scientific research, scientific
committees, expert reports, conferences,
seminars, training, participation in various
symposia, writing brochures ...) and, if applicable,
fee billing; and this with the majority of
companies selling cardiovascular medicines and
other products related to my areas of specialty
(Amgen, Astra-Zeneca, Bayer, Boehringer
Ingelheim, Bouchara, Daiichi Sankyo, Egis,
Ferring, Ipsen, Lilly, Le Quotidien du Médecin,
Medtronic, Menarini, MSD, Novartis,
Pharmalliance, Pierre Fabre, Pileje, Quantum
genomics, Sanofi Aventis, Saint Jude, Servier,
Takeda).
- HAS, ANSM, CNAM, MGEN
Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
• Prehypertension : – Stroke risk factor ?
– CHD risk factor ?
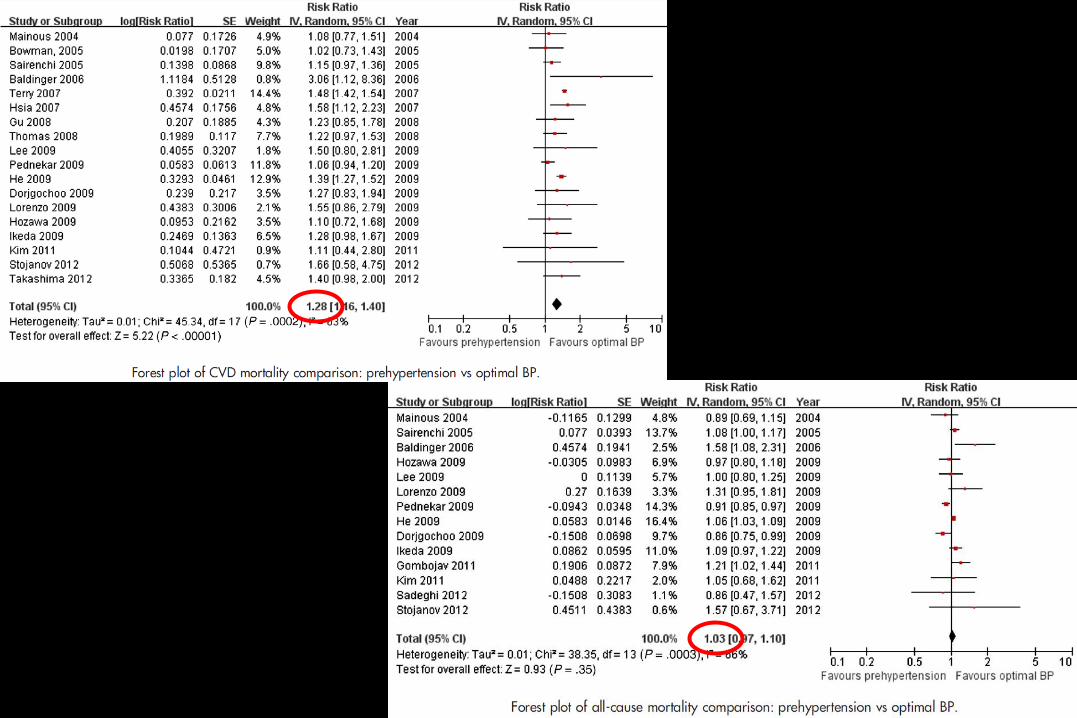
– CV mortality risk factor - all-cause mortality risk factor ?
– Which patients ?
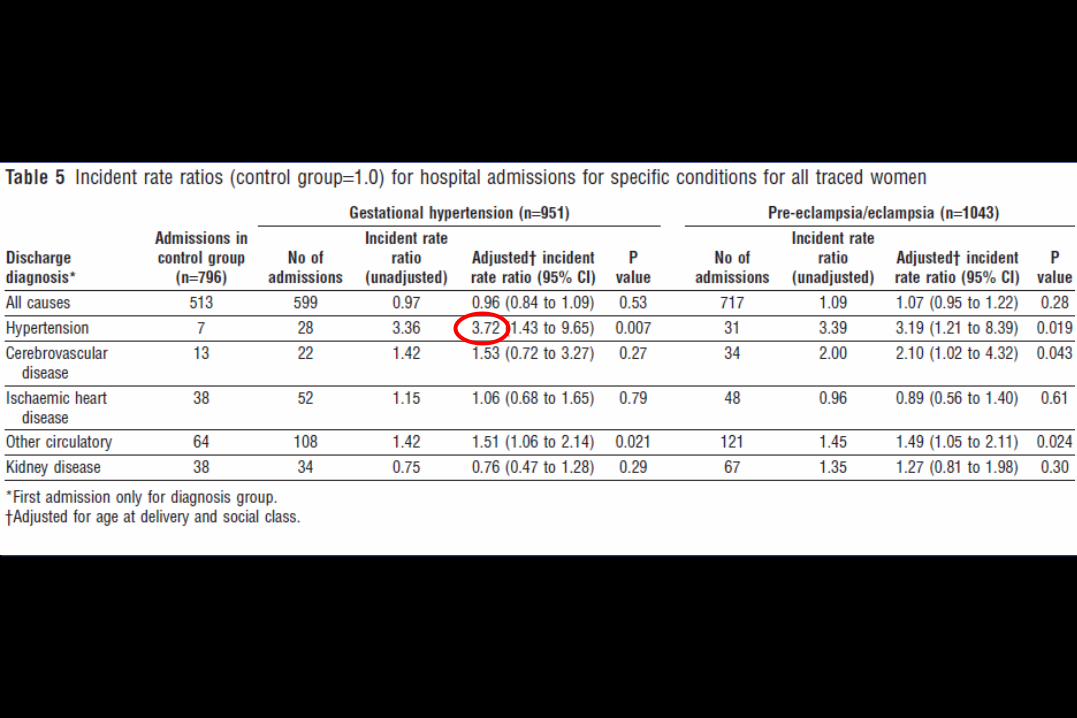
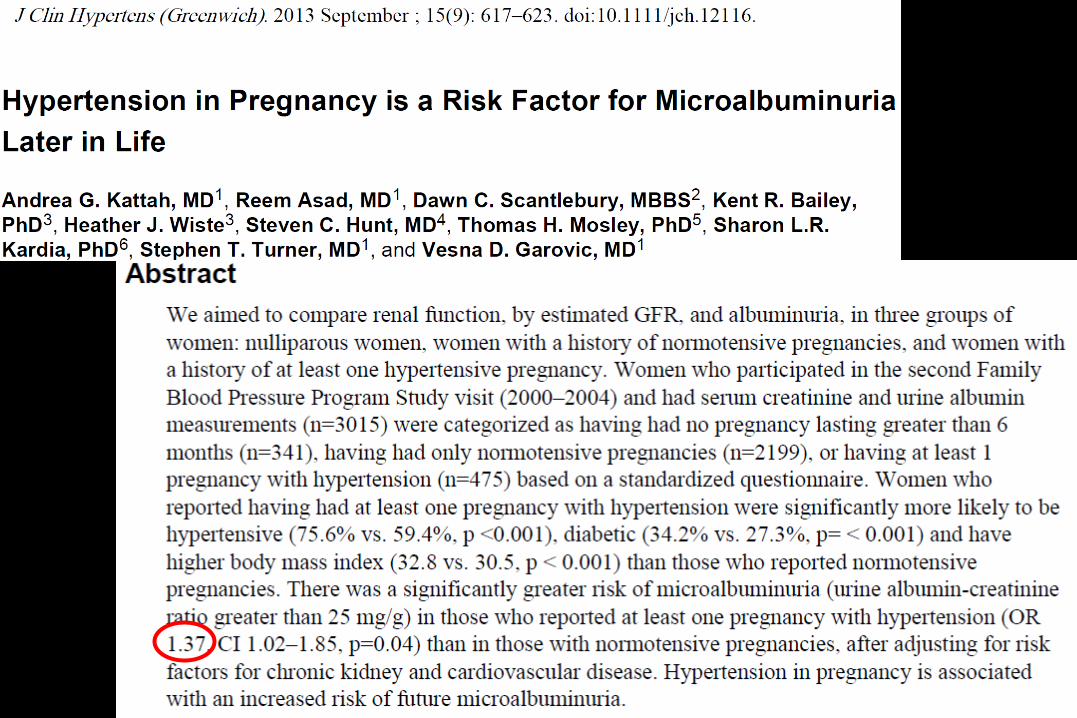
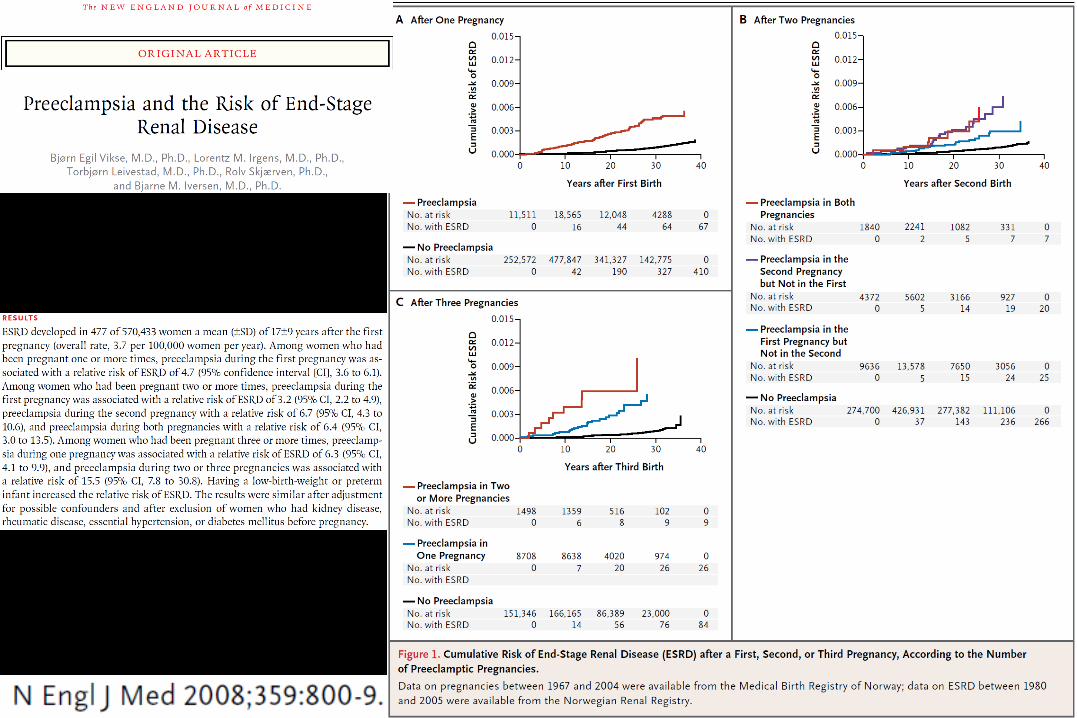
• Hypertensive disorders of pregnancy (pre-eclampsia) :– Hypertension and renal risk factor ?
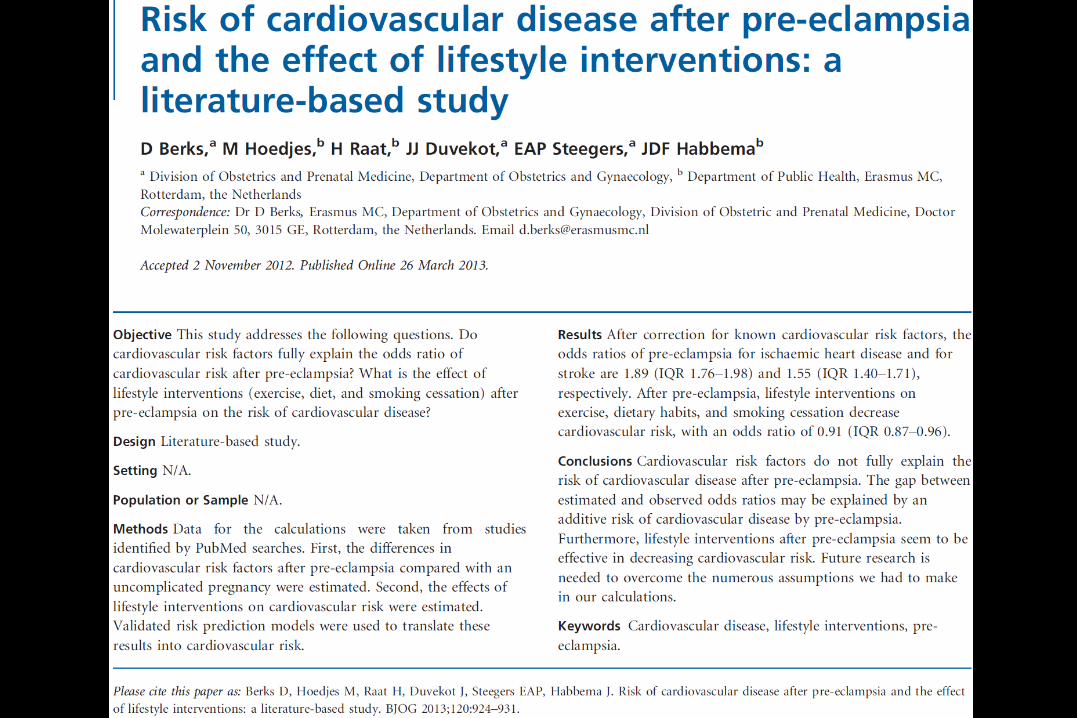
– Stroke and CHD risk factor ?
• One more guideline : why ?
• Conclusion

Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
• Prehypertension : – Stroke risk factor ?
– CHD risk factor ?
– CV mortality risk factor - all-cause mortality risk factor ?
– Which patients ?
• Hypertensive disorders of pregnancy (pre-eclampsia) :– Hypertension and renal risk factor ?
– Stroke and CHD risk factor ?
• One more guideline : why ?
• Conclusion
Prehypertension and risk of stroke
• Huang Y et al. Prehypertension and the risk of
stroke. Neurology 2014 ; 82 : 1153-61.
• Pooled data included the results of 762,393 participants from 19
prospective cohort studies. Prehypertension increased the risk of stroke
(RR 1.66; 95% CI 1.51–1.81) compared with optimal blood pressure
(<120/80 mm Hg).
• After adjusting for multiple cardiovascular risk factors, prehypertension
is associated with stroke morbidity. Although the increased risk is
largely driven by high-range prehypertension, the risk is also increased
in people with low-range prehypertension.




Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
• Prehypertension : – Stroke risk factor ?
– CHD risk factor ?
– CV mortality risk factor - all-cause mortality risk factor ?
– Which patients ?
• Hypertensive disorders of pregnancy (pre-eclampsia) :– Hypertension and renal risk factor ?
– Stroke and CHD risk factor ?
• One more guideline : why ?
• Conclusion






Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
• Prehypertension : – Stroke risk factor ?
– CHD risk factor ?
– CV mortality risk factor - all-cause mortality risk factor ?
– Which patients ?
• Hypertensive disorders of pregnancy (pre-eclampsia) :– Hypertension and renal risk factor ?
– Stroke and CHD risk factor ?
• One more guideline : why ?
• Conclusion


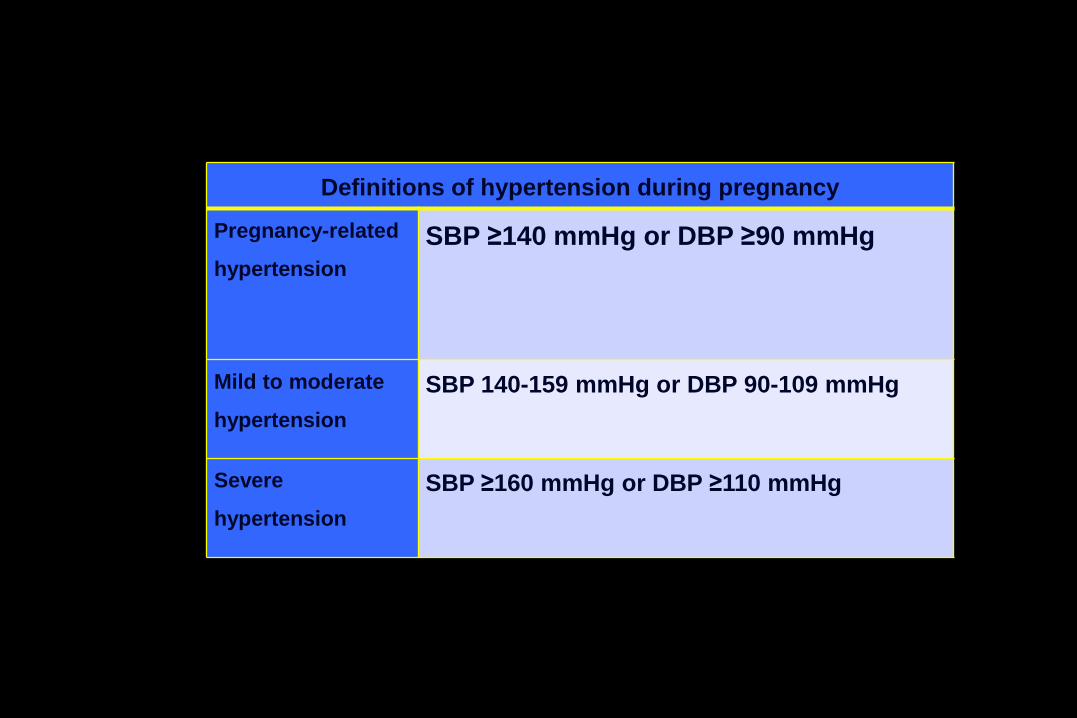
Definitions of hypertension during pregnancy
Pregnancy-related
hypertension
SBP ≥140 mmHg or DBP ≥90 mmHg
Mild to moderate
hypertension
SBP 140-159 mmHg or DBP 90-109 mmHg
Severe
hypertension
SBP ≥160 mmHg or DBP ≥110 mmHg

Pregnancy-induced hypertension can present as
one of the following:
• Chronic hypertension (preexisting or diagnosed
before 20 weeks gestation)
• Gestational hypertension (onset after 20 weeks
gestation) with no proteinuria
• Preeclampsia defined as onset of hypertension
(controlled or not) associated with significant
proteinuria after 20 weeks gestation.

Severe preeclampsia is associated with at
least one of the following:
• severe hypertension,
• target organ damage defined by one or more of the
following:
– oliguria <500 mL per 24 hours, or creatininemia >135
µmol/L, or proteinuria >3 g per 24 hours,
– pulmonary edema,
– persistent epigastric or right upper quadrant abdominal
pain,
– HELLP syndrome (intravascular hemolysis, hepatic
cytolysis and thrombocytopenia),
– Persistent neurological symptoms (visual disturbances,
headache, hyperactive deep-tendon reflexes, seizures),
– Retro-placental hematoma.



RECOMMENDATION N°20 - (Grade C - Class 2)
• It is suggested that a dedicated consultation
focusing on patient information and announcement
of the diagnosis of hypertension should be
programed some time after the birth for all patients
who experienced hypertension during their
pregnancy. The objectives would be:
– to explain the links between hypertension during
pregnancy and the risk of cardiovascular and renal
disease;
– to underline the importance of a coordinated
multidisciplinary care-plan, and to ensure that preventive
measures are set up, targeting lifestyle measures and the
control of cardiovascular and renal risk factors.
RECOMMENDATION N°21 (Grade B - Class 1)
• It is recommended that women who experienced
hypertension during a pregnancy should be offered:
– BP-, creatininemia- and proteinuria-monitoring;
– An assessment of the etiology of the disease;
– Evaluation and management of other cardiovascular and renal
risk factors;
– Long-term BP monitoring, even for patients whose BP returns to
normal after delivery, because of the persistently elevated risk
of cardiovascular and renal outcomes;
– Adjustment of their antihypertensive treatment if necessary.

RECOMMENDATION N°22 - (Grade C - Class 2)
• It is suggested that women with chronic hypertension or a
history of gestational hypertension in a previous pregnancy
should be offered a preconception checkup with a view to:
– assessing and advising the woman about the risks associated with a
new pregnancy (recurrence of hypertension or preeclampsia or intra-
uterine growth retardation, or premature birth);
– discussing the possibility of researching a possible etiology of the
patient’s hypertension before beginning a new pregnancy;
– postponing a new pregnancy in a women with severe hypertension
until the disease is controlled;
– adjusting the antihypertensive drug therapy to the potential new
pregnancy;
– suggesting a specific coordinated care-plan for a new pregnancy;
– informing the patient whether she needs to take aspirin.

Should hypertensive disorders of pregnancy be
considered as a prehypertension state ?
• Prehypertension : – Stroke risk factor ?
– CHD risk factor ?
– CV mortality risk factor - all-cause mortality risk factor ?
– Which patients ?
• Hypertensive disorders of pregnancy (pre-eclampsia) :– Hypertension and renal risk factor ?
– Stroke and CHD risk factor ?
• One more guideline : why ?
• Conclusion

Conclusion
• Prehypertension : cerebrovascular and coronary risk factor
• Limited to those who will develop hypertension ?
• Hypertensive disorders of pregnancy (pre-eclampsia) :
cerebrovascular, coronary and renal risk factor
• Both situation partly neglected
Eclampsia
• Eclampsia is characterized by the occurrence
of convulsions or generalized tonic-clonic
seizures in a setting of pregnancy-induced
hypertension.

Recommendation N°1
• It is recommended that BP should be measured with the
patient seated, in a medical setting, after at least 5 minutes
rest, using an approved electronic brachial blood pressure
measuring device. (Grade A - Class 1)
• For office-measured mild to moderately high BP, hypertension
should be confirmed by measurements taken outside the
physician’s office (HBPM following the ‘rule of 3’ or daily
average of 24-hour ABPM) to exclude any possible white-coat
effect (Grade B - Class 1) (29). SBP ≥135 mmHg or DBP ≥85
mmHg, outside the physician’s office, is considered
pathological. (Grade C - Class 2)

Recommendation N°2 - (Grade B - Class 1)
• It is recommended that proteinuria should be measured at
least once a month in all pregnant women by urine collection
or by dipstick.
• A dipstick result greater than 1+ proteinuria requires
laboratory confirmation on a morning urine sample or a 24-
hour urine collection.
• Proteinuria >300 mg/24h or a proteinuria/creatininuria ratio
≥30 mg/mmol (or ≥300 mg/g) are reliable indicators of disease.
If onset occurs after the 20th week of gestation, it defines
preeclampsia in a hypertensive patient, regardless of whether
hypertension is controlled.
RECOMMENDATION N°3 - (Grade A - Class 1)
• It is recommended that treatment for severe
hypertension (SBP ≥160 mmHg or DBP ≥110
mmHg) should be initiated without delay.

RECOMMENDATION N°4 - (Grade C - Class 2)
• Office-measured mild to moderate hypertension
(SBP, 140-159 mmHg or DBP, 90-109 mmHg),
confirmed by HBPM or by the daytime average of
ABPM measurements (SBP ≥135 or DBP ≥85 mmHg),
a history of cardiovascular disease, pregestational
diabetes, chronic renal disease or high
cardiovascular risk in primary prevention, are all
situations where initiation of antihypertensive
treatment should be considered.

RECOMMENDATION N°5 (Grade A - Class 1)
• It is recommended that when antihypertensive
medication is prescribed, target office BP levels
should be DBP between 85 mmHg and 100 mmHg
and SBP <160 mmHg.

RECOMMENDATION N°6 - (Grade B - Class 2)
• During pregnancy, it is suggested that any one of the
following antihypertensive medications should be
used first line (presented in alphabetical order):
alpha-methyldopa, labetalol, nicardipine, or
nifedipine.

RECOMMENDATION N°7 - (Grade A - Class 1)
• Angiotensin converting enzyme (ACE) inhibitors,
angiotensin II receptor blockers (ARB) and aliskiren
must not be used at any time-point of pregnancy and
are contraindicated in the 2nd and 3rd trimesters.

RECOMMENDATION N°8 - (Grade C - Class 2)
• It is suggested that a Personal Pregnancy Care-Plan
notebook should be used in patients with
hypertension to ensure the best possible use is
made of the coordinated healthcare pathway (general
practitioner, hypertension specialist, obstetrics team,
and pharmacist).

RECOMMENDATION N°15
• To prevent the onset of preeclampsia, it is
recommended that low-dose (75-160 mg) aspirin
should only be prescribed to patients with a history
of preeclampsia. This treatment should be initiated
before 20 weeks gestation, ideally at the end of the
first trimester. (Grade A - Class 1)
• It is suggested that treatment with aspirin should be
continued until at least 35 weeks gestation. (Grade C
- Class 2)
RECOMMENDATION N°16 - (Grade B - Class 3)
• Low-dose aspirin is not currently recommended for
the prevention of preeclampsia in other high risk
populations, i.e., patients with chronic hypertension,
obesity, pregestational diabetes, chronic kidney
disease, abnormal uterine artery Doppler scan, or
those having undergone medically assisted
procreation, or screening by different biomarkers
during the first trimester.
RECOMMENDATION N° 17 - (Grade A - Class 3)
• Low molecular weight heparin, nitric oxide
(NO) donors, antioxidants (Vitamins C and E)
or physical exercise are not recommended for
the prevention of preeclampsia.
RECOMMENDATION N°18 - (Grade B - Class 2)
• It is suggested that the following
antihypertensive agents should be selected
for women who are breastfeeding:
– β-blockers: labetalol, propranolol;
– Calcium channel blockers: nicardipine, nifedipine;
– Alpha-methyldopa;
– ACE inhibitors: benazepril, captopril, enalapril or
quinapril, except for mothers of premature infants
or those with renal failure.
RECOMMENDATION N°19
• It is recommended that combined hormonal contraceptives
should not be prescribed prior to six weeks post-partum
because of the elevated risk of venous or arterial
thromboembolic disease. (Grade B - Class 1)
• It is recommended that non-hormonal contraceptive methods
should be prescribed for hypertensive patients with
inadequate BP control despite appropriate treatment. (Grade
B - Class 1)
• For women who rapidly become normotensive after the birth,
progestin-only contraception can be prescribed (pill, implant
or intrauterine device). (Grade B - Class 2)
• For patients who wish to use an intrauterine device, it is
recommended that this should be fitted at the post-natal visit.
(Grade B – Class 2)

RECOMMENDATION N°20 - (Grade C - Class 2)
• It is suggested that a dedicated consultation
focusing on patient information and announcement
of the diagnosis of hypertension should be
programed some time after the birth for all patients
who experienced hypertension during their
pregnancy. The objectives would be:
– to explain the links between hypertension during
pregnancy and the risk of cardiovascular and renal
disease;
– to underline the importance of a coordinated
multidisciplinary care-plan, and to ensure that preventive
measures are set up, targeting lifestyle measures and the
control of cardiovascular and renal risk factors.

Corinne DAVID (39 ans)
Tél. : 07 86 12 35 76 [email protected]
31, Boulevard de Valmy 92700 Colombes
√ - Associatif - Gestion d’association - Responsable administrative
Actuellement en poste à la Société Française de Cardiologie, responsable de la gestion de la filiale de la Société Française d’Hypertension Artérielle
√ - Evénementiel - Chef de projet PCO senior
- Gestion d’activités de DM C et réceptives
APTITUDES & COMPÉTENCES PROFESSIONNELLES
√ - Gestion d’association - Coordination et suivi de s activités de l’association en collaboration av ec le Conseil d’Administration, et en ac cord avec les dé cisions co llégialement pr is es - Gestion du secrétariat et de l’administratif, relation avec les membres et adhérents, suivi de la comptabilité (hors analytique = support d’un expert-comptable) √ - Suivi des activités scientifiques et partenariales de l’association et du congrès √ - Conception d’évènements professionnels et associatifs à forte visibilité (congrès, sy mposiums, DM C…) permettant la valorisation de l’institution ou de l’ as sociation - Recherche du concept le mieux adapté aux besoins du client et en adéquation avec le budget et les financements dédiés pour l’ év énement √ - Communication et promotion des ac t i vités de l’ association et des activités événementielles √ - Prise en ch arge d’un pr o jet et des dossiers de A à Z - Coordination en complète autonomie √ - Management d’équipe - Relation clients, partenaires et prestataires √ - Gestion des activités et des étapes des programmes de DPC jusqu’à la clôture des comptes (hospitaliers et libéraux)
ACTIVITÉS PRINCIPALEMENT MENÉES
√ - RELATION CLIENTS, ACTEURS ASSOCIATIFS ET PRESTATAIRES - Rapport d’activité régulier du suivi des dossiers et des activités en cours et à mener auprès du client et des décisionnaires - Pilotage et animation des réunions évènementielles clients et prestataires, organisation des réunions des Conseil d’Administration et des Groupes de Travail, rédaction de compte-rendu et mise en application des décisions prises - Intermédiaire entre tous les acteurs de la vie associative (Président, CA, Groupes de Travail, partenaires, société m
è
r e, so ciétés sœ u rs, membres, ét udi ants, fo r ma t eurs, In stitutions,…) - Interface entre le client ou le Président de l’association et les prestataires jusqu’à la livraison de la commande
√ - COMMUNICATION - Rédaction du cahier des charges et création du site internet institutionnel en accord avec les orientations de communication de l’ associ at ion. Responsable de l’administration du site (gestion du Back Office), création de newsletters, ve ille d’actualités. (Refonte du site Internet de la SFHTA en cours d’ é laboration) - Définition du contenu et élaboration du site in t er net d’ inf or m ation dé di é au x év èn ements, su i vi de s mod i f icat i on s - Création de supports de communication en collaboration avec le pr e stataire PAO / Studio ju s qu’à l’ im pression (Brochures institutionnelles, annonces, newsletters, formulaires programmes scientifiques, livres des résumés, dossier de commercialisation,…) - Action marketing et de promotion de l'événement
√ - ORGANISATION ET PLANIFICATION - Définition des plannings d’activité et respect des délais des actions à mener - Analyse de la faisabilité technique et financière des projets, montage du budget - Rédaction des cahiers des charges / appels d’offre et choix du prestataire le mieux adapté aux besoins - Définition des responsabilités et coordination des équipes et des prestataires, en amont et au cours de l’évènement
√ - SUIVI DES ACTIVITES INSTITUTIONNELLES ET DE CONGRÈS - Coordination de l’évènement annuelle de la SFHTA en collaboration avec l’ a gence PCO mandatée - Suivi de la trésorerie de l’évènement, facturation et reddition des comptes, su i vi co mptable de l’a ssoc iation - Relation et fidélisation des partenaires financiers, recherche de financements pour le congrès, recherche de subventions - Suivi technique et logistique avec les prestataires, définition des besoins, négociations commerciales - Gestion de l’exposition professionnelle (stands) et de s activités parallèles à l’ év ènement (dîner, réunions,..) - Responsable du secrétariat scientifique des congrès, et support des activités scientifique des Groupes de Travail de l’Association - Suivi des programmes de DPC en accord avec la règlementation en vigueur - Gestion des membres et rappel des cotisations