short bowel syndrome anne aspin 2010. definition rickham (1967) – an extensive resection to...
TRANSCRIPT

Short Bowel SyndromeShort Bowel Syndrome
Anne Aspin 2010Anne Aspin 2010

DefinitionDefinition
• Rickham (1967) – an extensive resection Rickham (1967) – an extensive resection to maximum of 75cmto maximum of 75cm
• Kuffer (1972) – 15cm with ileocaecal valveKuffer (1972) – 15cm with ileocaecal valve
- 38cm without ileocaecal valve- 38cm without ileocaecal valve
• Dorney (1985) – 11cm with I/C valve or Dorney (1985) – 11cm with I/C valve or 25cm without I/C valve 25cm without I/C valve

IntroductionIntroduction
• Most common cause of intestinal failure.Most common cause of intestinal failure.
• NEC, Congenital atresia, Gastroschisis NEC, Congenital atresia, Gastroschisis and volvulus.and volvulus.
• Promote adaptive response through Promote adaptive response through enteral feeding and careful enteral feeding and careful management of TPN.management of TPN.

The Digestive SystemThe Digestive System
• Digestion starts in the mouthDigestion starts in the mouth
• Moisten by saliva (contains Pytalin), Moisten by saliva (contains Pytalin), begins to turn starch to sugar.begins to turn starch to sugar.
• In stomach food churned mixes with In stomach food churned mixes with gastric juices.gastric juices.

Gastric juicesGastric juices
• Acid reactionAcid reaction
• Kills bacteriaKills bacteria
• Controls pylorusControls pylorus

• Gastric juices:Gastric juices:
- Rennin coagulates milk- Rennin coagulates milk
- Hydrochloric Acid – Converts Pepsinogen to - Hydrochloric Acid – Converts Pepsinogen to Pepsin.Pepsin.
- Pepsin turns protein to peptone- Pepsin turns protein to peptone

• Food is released in small amounts by Food is released in small amounts by relaxation of the sphincter passing onto relaxation of the sphincter passing onto Duodenum.Duodenum.
• Food further digested by Trypsin, Food further digested by Trypsin, Amylase and Lipase.Amylase and Lipase.
• Digestion completed in small intestine.Digestion completed in small intestine.

Intestinal juices.Intestinal juices.
• Enterokinase – pancreatic trypsinogenEnterokinase – pancreatic trypsinogen
• Peptidase – polypeptide to amino acidPeptidase – polypeptide to amino acid
• Maltase - maltose}Maltase - maltose}
• Sucrase – sucrose} to glucoseSucrase – sucrose} to glucose
• Lactase – Lactose}Lactase – Lactose}
• Lipase – Fats to fatty acids and glycerolLipase – Fats to fatty acids and glycerol

• Onto large intestine where fluids and Onto large intestine where fluids and nutrients are re absorbed. nutrients are re absorbed.
• Waste fluids taken by blood stream Waste fluids taken by blood stream to kidneys to be filteredto kidneys to be filtered
Small intestineSmall intestine
• Convoluted tube from pyloric sphincter Convoluted tube from pyloric sphincter to the junction of ileo – caecal valveto the junction of ileo – caecal valve
• Mucus membrane –has circular folds to Mucus membrane –has circular folds to increase surface area for absorption.increase surface area for absorption.
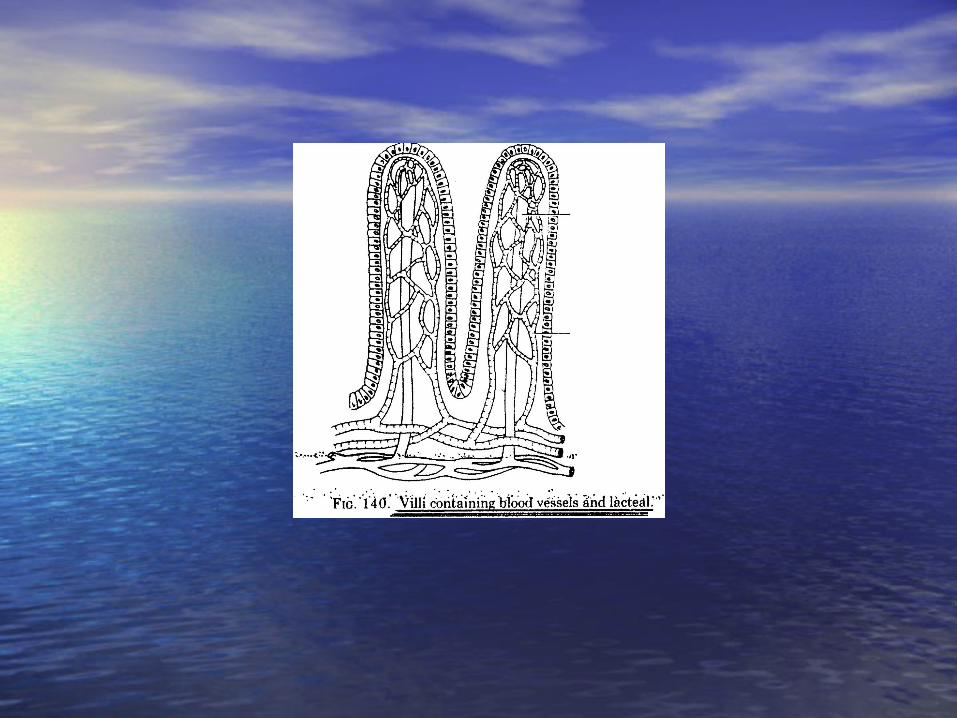
• Villi which contain blood and lymph Villi which contain blood and lymph vessel.vessel.
• Supplied with tubular glands secreting Supplied with tubular glands secreting intestinal juice.intestinal juice.
AbsorptionAbsorption
• Proteins, Carbohydrates and Fats Proteins, Carbohydrates and Fats through villi in small intestine.through villi in small intestine.
• Fats in the form of fatty acids and Fats in the form of fatty acids and glycerol are absorbed by cells glycerol are absorbed by cells covering villi. Pass into lymph within covering villi. Pass into lymph within villi drained by lymphatic capillaries.villi drained by lymphatic capillaries.

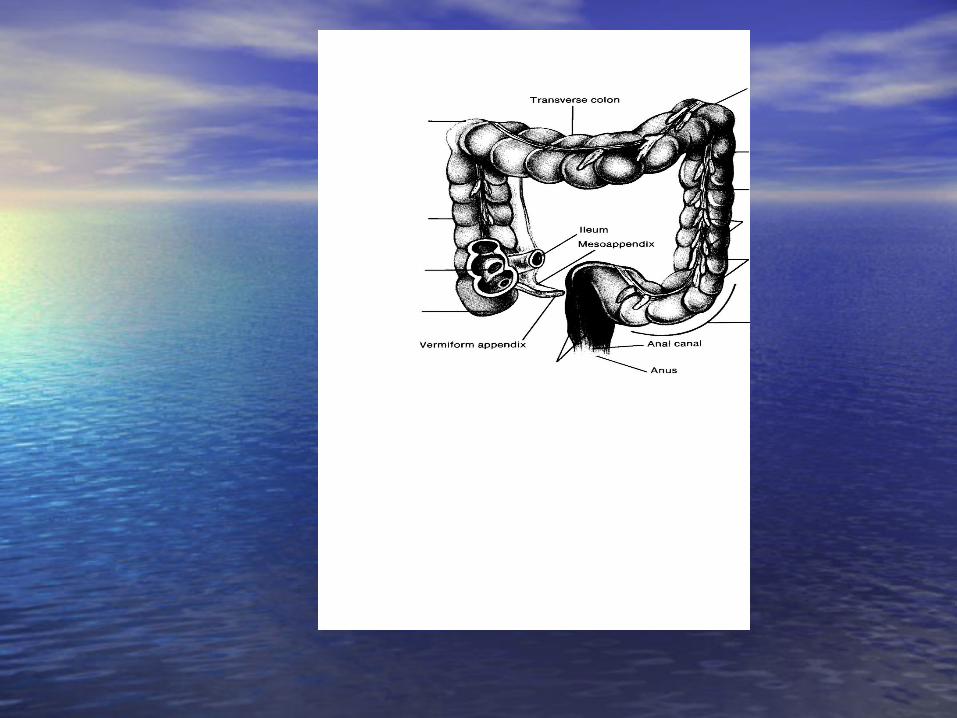
Ileo Caecal valve.Ileo Caecal valve.
• The Caecum lies in the right ileac fossa.The Caecum lies in the right ileac fossa.
• The Ileum opens into the Caecum The Ileum opens into the Caecum through the Ileo-Caecal valve.through the Ileo-Caecal valve.
• This is a sphincter which prevents the IC This is a sphincter which prevents the IC contents passing back into the Ileum.contents passing back into the Ileum.

What is SBSWhat is SBS
• Reduced bowel surface area for Reduced bowel surface area for absorption of nutrients together with absorption of nutrients together with rapid transit of intestinal contents.rapid transit of intestinal contents.
• TPN reduced as enteral feeds are TPN reduced as enteral feeds are introduced.introduced.
• Need to promote intestinal adaptation.Need to promote intestinal adaptation.
MotilityMotility
• The IC valve and colon is important The IC valve and colon is important to slow intestinal transit.to slow intestinal transit.
• Proteins, Fats and Carbohydrates are Proteins, Fats and Carbohydrates are absorbed almost completely within absorbed almost completely within first 150cm of small bowel.first 150cm of small bowel.

• Jejunum – most of electrolyte Jejunum – most of electrolyte absorptionabsorption
• Ileum is the only site for absorption Ileum is the only site for absorption of Vit B12 and bile salts.of Vit B12 and bile salts.

After resection.After resection.
• Increase gastric emptying.Increase gastric emptying.
• Ileal resection, increased transit timeIleal resection, increased transit time
• An intact IC valve prolongs gut transit, loss An intact IC valve prolongs gut transit, loss of this causes an increase.of this causes an increase.
• If colon resected transit increases.If colon resected transit increases.

• Duodenal resection – malabsorption of Duodenal resection – malabsorption of Iron, Calcium and Folic Acid.Iron, Calcium and Folic Acid.
• Jejunal resection – If extensive resection, Jejunal resection – If extensive resection, lactose intolerencelactose intolerence
• Ileal resection – Some diarrhoea due to Ileal resection – Some diarrhoea due to bile salts being incompletely absorbed.bile salts being incompletely absorbed.

Gastric HypersecretionGastric Hypersecretion
• After abdominal surgery, gastric hyper-After abdominal surgery, gastric hyper-secretion occurs in 50% cases.secretion occurs in 50% cases.
• This impairs digestion of lipids by This impairs digestion of lipids by lowering intraluminal PH and lowering intraluminal PH and inactivating the pancreatic enzymes.inactivating the pancreatic enzymes.
• Also stimulates peristalsis. Also stimulates peristalsis.

How does the bowel adapt?How does the bowel adapt?
• Cellular hyperplasiaCellular hyperplasia
• Villous hypertrophyVillous hypertrophy
• Intestinal lengtheningIntestinal lengthening
• Altered motilityAltered motility
• Hormonal changesHormonal changes
• Takes approx 2 years Takes approx 2 years to reach max effect.to reach max effect.

Management of SBS.Management of SBS.
• Total TPNTotal TPN
• Gradual introduction of enteral Gradual introduction of enteral feeding.feeding.
• Fluid and electrolyte balanceFluid and electrolyte balance
• Fluid replacement if stool, gastric Fluid replacement if stool, gastric aspirate or ostomy losses are highaspirate or ostomy losses are high
• Reducing substances above1% contra Reducing substances above1% contra indicate increasing enteral feeds.indicate increasing enteral feeds.

Weaning off TPNWeaning off TPN
• Cycling – one hour off, line lock with Cycling – one hour off, line lock with Gentamycin. Build up to off all day.Gentamycin. Build up to off all day.

Complications.Complications.
• Bacterial overgrowthBacterial overgrowth
• AnaemiaAnaemia
• Bile salt depletionBile salt depletion
• Bone diseaseBone disease
• CholestasisCholestasis
• DiarrhoeaDiarrhoea
• HypocalcaemiaHypocalcaemia

Complications (cont)Complications (cont)
• HypomagnesaemiaHypomagnesaemia
• Liver fibrosisLiver fibrosis
• Renal stonesRenal stones
• Protein malnutritionProtein malnutrition
• Trace mineral deficiencyTrace mineral deficiency
• Vitamin deficiency, A, D, E, K, B12Vitamin deficiency, A, D, E, K, B12

Central line complicationsCentral line complications
• InfectionInfection
• ThrombosisThrombosis
• Break in catheterBreak in catheter
• Air embolusAir embolus
• Tissue necrosisTissue necrosis
• MalpositionMalposition
• Cardiac tamponadeCardiac tamponade

Bacterial OvergrowthBacterial Overgrowth
• Bloating, cramps, diarrhoea, Bloating, cramps, diarrhoea, gastrointestinal blood loss.gastrointestinal blood loss.
• Treat with sugar free Metronidazole Treat with sugar free Metronidazole and Trimethoprimand Trimethoprim

Watery diarrhoeaWatery diarrhoea
• LoperamideLoperamide
• Malabsorption of bile acids.Malabsorption of bile acids.
• PectinPectin

SurgerySurgery
• Further resection might be avoided Further resection might be avoided by tapering, strictureplasty or serosal by tapering, strictureplasty or serosal patching. patching.
• Patients with dilated segments Patients with dilated segments proximal to tight anastomosis – proximal to tight anastomosis – resect and taper improves bacterial resect and taper improves bacterial overgrowth by improving flow.overgrowth by improving flow.

TaperingTapering

Bowel lengtheningBowel lengthening
• Cutting bowel longitudinally, Cutting bowel longitudinally, preserve blood supply to both sides preserve blood supply to both sides and create a segment of bowel twice and create a segment of bowel twice length, half diameter without loss of length, half diameter without loss of mucosal surface area.mucosal surface area.

Bowel lengtheningBowel lengthening

Antiperistaltic small intestine Antiperistaltic small intestine segmentsegment

Colonic interpositionColonic interposition

Medical managementMedical management
• Pectin (water sol, non cellulose dietary Pectin (water sol, non cellulose dietary fibre which promotes intestinal adaptation)fibre which promotes intestinal adaptation)
• Ranitidine (PH > 4)Ranitidine (PH > 4)
• Loperamide (slow gut transit time)Loperamide (slow gut transit time)
• Cholestyramine (binds bile salts)Cholestyramine (binds bile salts)

It takes approximately two It takes approximately two years to achieve some normal years to achieve some normal dietdiet

Thank youThank you

ReferencesReferences• Bentley D, Lifschitz C, Lawson M (2001). Necrotising Entercolitis Bentley D, Lifschitz C, Lawson M (2001). Necrotising Entercolitis • And Short Bowel Syndrome. And Short Bowel Syndrome.
http://www.naspghan.org/wmspage.cfm?porm1=130http://www.naspghan.org/wmspage.cfm?porm1=130• Koglmeier J, Day C, Puntis J (2008). Clinical outcome in patients from a Koglmeier J, Day C, Puntis J (2008). Clinical outcome in patients from a
single region who were dependent on parenteral nutrition for 28 days or single region who were dependent on parenteral nutrition for 28 days or more. more. Archives of Disease in Childhood. Archives of Disease in Childhood. 93 (4) : 300 - 30293 (4) : 300 - 302
• Martin G, Wallace L and Sigalet D (2004). Glucagon – like Peptide -2 Martin G, Wallace L and Sigalet D (2004). Glucagon – like Peptide -2 Induces Intestinal Adaptation in Parenterally Fed Rats with Short Bowel Induces Intestinal Adaptation in Parenterally Fed Rats with Short Bowel Syndrome. Syndrome. American Journal of Physiology.American Journal of Physiology. Gastro-intestinal and Liver Gastro-intestinal and Liver Physiology. 286: G964-G972Physiology. 286: G964-G972
• McMahon M, Leviller J and Chescheir N (1996). Prenatal Ultrasonographic McMahon M, Leviller J and Chescheir N (1996). Prenatal Ultrasonographic Findings Associated with Short Bowel Syndrome in Two Fetuses with Findings Associated with Short Bowel Syndrome in Two Fetuses with Gastroschisis. Gastroschisis. Obstetrics and Gynaecology.Obstetrics and Gynaecology. 88: 676-678 88: 676-678
• Seidner D and Matarese L (2003). Selected topics in Seidner D and Matarese L (2003). Selected topics in • Gastrotherapy. Case 2: Short Bowel Syndrome : Etiology,Gastrotherapy. Case 2: Short Bowel Syndrome : Etiology,• Pathophysiology and Management. Pathophysiology and Management. The Cleveland Clinic Center for The Cleveland Clinic Center for
Continuing EducationContinuing Education• Sinden A, Sutphen S (2003) Nutritional Management of Paediatric Short Sinden A, Sutphen S (2003) Nutritional Management of Paediatric Short
Bowel Syndrome. Bowel Syndrome. Nutrition Issues in Gastroenterology.Nutrition Issues in Gastroenterology. Series #12 p28-48 Series #12 p28-48• Warner B, Vanderhoof J and Rayes J (2000). What’s New In The Warner B, Vanderhoof J and Rayes J (2000). What’s New In The
Management of Short Gut Syndrome in Children. Management of Short Gut Syndrome in Children. Division of Paediatric Division of Paediatric Surgery. Department of Surgery. American College of Surgeons.Surgery. Department of Surgery. American College of Surgeons. p725-736 p725-736