shock in children
TRANSCRIPT

Dr.rajesh .k

Shock is a state of impaired tissue perfusion resulting in an imbalance between oxygen demand and supply.
This widespread reduction in effective tissue perfusion causes insufficient or improper delivery and distribution of
oxygen and nutrients, the end result of which is an altered
cellular and subcellular function leading to anaerobic
metabolism, accumulation of lactic acid and consequently
cellular damage, multiple organ dysfunction and finally
cardiovascular collapse.
Clinically shock is characterized by signs of hemodynamic instability, tachycardia,
hypotension and evidence of organ hypoperfusion.

Etiologic Classification of Shock
The patient with shock has abnormalities of either:
• The heart
• The blood volume
• The blood flow distribution.
Accordingly shock can be classified into three groups:
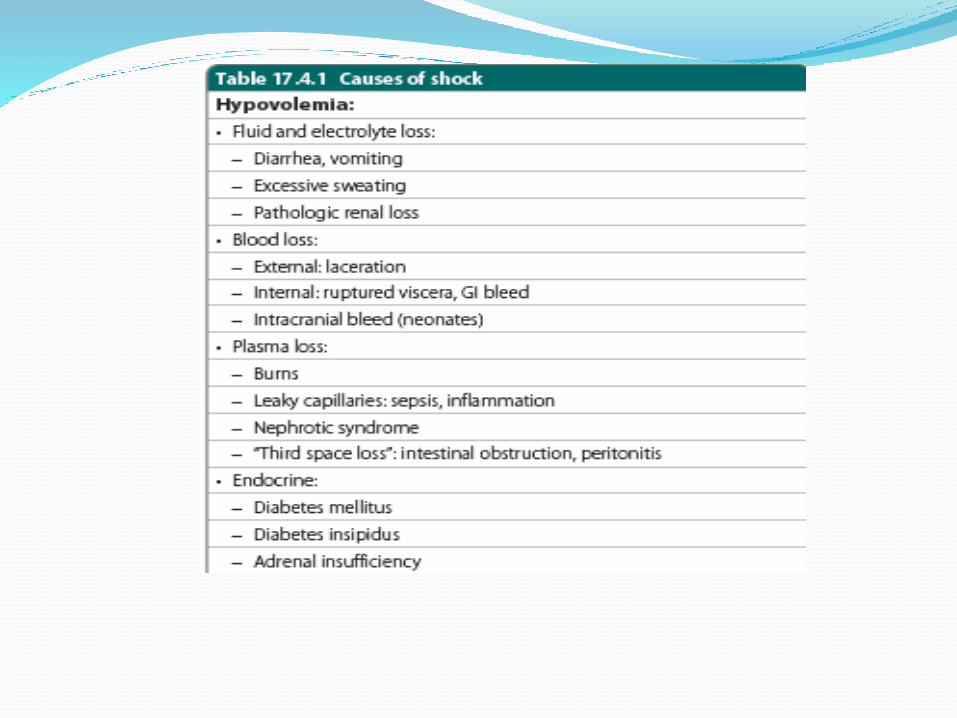
1. Hypovolemic (decreased circulating blood volume)
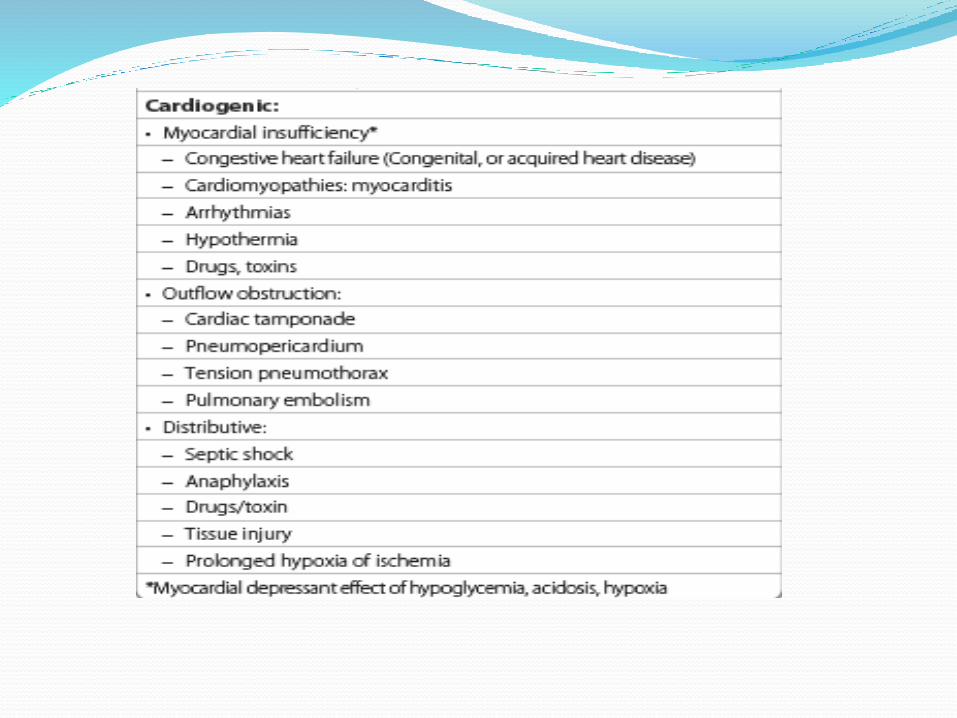
2. Cardiogenic (impaired cardiac function)
3. Distributive (inappropriate distribution of blood flow).

Children with sepsis are more likely to have
cardiac failure than vascular failure as seen in adults.
When cardiac output is unable to meet the demands of the tissues, compensatory sympathetic activity produces selective vasoconstriction of the skin and splanchnic vessels to divert blood flow to vital organs, namely brain, heart and kidney.
Three pathophysiological concepts that need understandingespecially in septic shock are as follows:
Myocardial dysfunction: It develops in nearly all patients with septic shock. This dysfunction peaks soon after the onset of sepsis and resolves within 7–10 days in survivors. Sepsis stimulates the release of inflammatory mediators that can compromise cardiac function.
Diminished responsiveness of the myocardium to β1 agonists is secondary to downregulation of β1 receptors, uncoupling of receptors from adenylate cyclase or depressed generation of cAMP.
The myocardium is dysfunctional despite an increase
in cardiac output during the hyperdynamic phase of
sepsis.

Mean arterial pressure (MAP): It is important to recognize that oxygen is not distributed uniformly to the body. Modulation of systemic vascular resistance in different vascular beds is one of the body’s primary compensatory mechanisms to shunt blood preferentially to vital organs such as the heart and brain.When meanarterial pressure falls below the autoregulatoryrange of an organ, blood flow decreases, resulting in tissue ischemia and organ failure. Because the kidney receives the second highest blood flow of any organ in the body,measurement of urine output (with the exception of patients with hyperosmolar states leading to osmotic diuresis) and creatinine clearance can be used as an indicator of adequate perfusion pressure.
Oxygen delivery versus consumption: Oxygen delivery is primarily dependent on cardiac output.Enhancing cardiac output by increasing preload and contractility or by decreasing afterload will thus increase oxygen delivery.
Contrary to adults, oxygen delivery, not oxygen extraction, is the major determinant of oxygenconsumption in children.
In patients with septic shock the concept of pathologicaloxygen utilization is forwarded to explain dependence of oxygen consumption on oxygen delivery even atsupernormal oxygen delivery.
The goal in such patients is therefore to increase oxygen delivery and consumption until consumption is independent of delivery.

Hypovolemic Shock
Hypovolemic shock is the leading form of shock in children worldwide. It is usually caused by hemorrhage or dehydration. Relative hypovolemia may occur secondary to “third spacing” of fluids (extravascular fluid shifts) as it may be observed in children with burns or with sepsis. Depending on the severity and rate of development of hypovolemia, the shock may appear abruptly or evolve gradually over several stages.
Regardless of etiology the final common pathway to circulatory insufficiency is diminished intravascular volume.
Children with hypovolemia due to fluid and electrolyte losses have both intravascular and interstitial depletion. Clinical findings include sunken eyes, depressed anterior fontanel, dry mucous membrane,
poor skin turgor, delayed capillary refill, and cool extremities.

The classical signs of dehydration based on interstitial fluid depletion are absent. Once again,
hypotension is a late finding and may not occur until intravascular volume has decreased by about 25%. This is the time when the compensatory mechanisms fail, and profound
reduction of cardiac output and fall of blood pressure occur.

Cardiogenic Shock
Cardiogenic shock is commonly described as “pump
failure”. The common causes are myocarditis, dysrhythmias,
and drugs with a myocardial depressant action, acidosis,
congenital heart lesions and sepsis. It can also result from
obstruction to the outflow tract, e.g. coarctation of aorta
or aortic stenosis or in states of increased afterload like
hypertension. Cardiogenic shock will have low cardiac
output, hypotension and clinical signs of inadequate tissue
perfusion. Typically intravascular volume is adequate or even
increased, but cardiac dysfunction limits cardiac output.

Distributive shock The most common cause of distributive shock is sepsis. The common denominator in this shock is leakage of intravascular fluid
through capillary bed into interstitial space known as “third spacing” of fluids because of
endothelial damage. The majority of cases of septic shock are caused by Gram-negative bacilli
but it may be caused by Gram-positive, rickettsial, fungal and viral infections. Early septic shock is known as “warmshock” or hyperdynamic phase as it is
characterized by warm extremities, low SVR, high or normal cardiac outputnormal BP and increased pulse pressure.
Low systemic vascular resistance increases skin blood flow and causesbounding peripheral pulses.
Therefore despite high cardiac output, shock and metabolic acidosis develop because blood flow is inappropriately distributed.

Adequate and early treatment at this stage may prevent progression.
The latter phase of “cold shock” or hypodynamic phase is characterized by cold extremities,high systemic vascular resistance, low cardiac output,narrow pulse pressure and hypotension leading to hypoxia,acidosisand death.

Clinical Features and Stages of Shock Shock refers to dynamic state ranging from
early,compensated shock to irreversible, terminal shock.
Shock can progress over a span of few hours or occur over minutes, e.g. in hemorrhagic shock. The progression can be arbitrarily divided into three stages:
• Early compensated shock
• Decompensated shock
• Irreversible shock.

Early shock Early shock refers to preserved vital organ functions secondary to
effective compensatory mechanisms. Blood pressure is maintained although signs of inadequate tissue and
organ perfusion are observed. The early physical signs are that of an exaggerated sympathetic response to stress.
Tachycardia and signs of decreased peripheral perfusion namely cold-clammy skin, capillary refill time more than 2 seconds and difference between core and surfacetemperature of ≥ 2°C are the most important clinical pointers to early
shock. Tachypnea may be seen without evidence of an underlying pulmonary disease. Blood pressure is maintained within normal range during the early stages.
Septic shock in the early stages presents with fever,warm well-perfusedextremities, bounding pulses and wide pulse pressure.
A capillary refill time of 3 seconds or more denotes impaired skin perfusion. It is a valuable sign during assessment and monitoring

Decompensated Shock In this stage, the blood pressure and cardiac output fall as
they cannot be sustained by the intense peripheral vasoconstriction.
A cascade of anaerobic tissue metabolism and multiorgandysfunction sets in.
Patient presents with poor pulses, peripheral cyanosis, cold extremities,hypotension and acidosis.
Vital organ perfusion gets progressively compromised. Oliguria or anuria results from diminished renal perfusion. Diminished cerebral perfusion manifests in the form of lethargy, confusion and disorientation.
Rapid aggressive intervention is required to halt the progression to irreversible stage.

Irreversible Stage Irreversible stage of shock is a progressive reduction in
cardiac output, fall in blood pressure and worsening metabolic acidosis, and multiorgan failure.
Delayed recognition or inadequate treatment can lead to terminal shock


Presence of hypotension is not a must for diagnosis of shock in children.
children maintain adequate cardiac output by mounting tachycardic response
Children maximize systemic vascular resistance to maintain a normal blood pressure, in the face of significant decrease in the CO.
This increase due to peripheral vasoconstriction mediated by the sympathetic nervous system results in diversion or redistribution of blood flow from less vital organs such as skin, skeletal muscles, kidneys, and splanchnic organs, to more vital organs like the brain,heart, lungs, and adrenal glands.
Therefore, blood pressure will remain maintained till very late stages of shock and hence is a poor indicator of cardiovascular homeostasis in children.
The evaluation of other hemodynamic variables like heart rate and end-organ perfusion, including capillary refill, the quality of the peripheral pulses, mentation, urine output, and acid-base status, is more reliable than blood pressure in determining the adequacy of hemodynamicstatus in a child.

Complications of Shock Myocardial depression, ARDS, acute renal failure, and
disseminated intravascular coagulation (DIC) are the most dreaded and life-threatening complications of shock.

Shock is a clinical diagnosis.and other lab invetigations advised are follows

Management of Shock Two major priorities in treatment of septic shock are
1.rapid assessment of patient’s disease process
2.achievement of cardiopulmonary stability.
Irrespective of the etiology the initial resuscitation and stabilization of all forms of shock should be guided by the ABC’s.
Stabilization of airway, provision of oxygen and establishment of vascular access are immediate goals followed by fluid resuscitation

An immediate intravenous (IV) access has to be established.
In children where IV access is difficult due to collapsedveins an intraosseous (IO) line must be established instead.
Obtaining rapid vascular access with at least two wide bore peripheral venous lines is extremely crucial. Vascularaccess may be extremely difficult in children with shockas they have collapsed veins. Since time is extremely crucial, Pediatric Advanced Life Support (PALS) guidelines recommend placement of an intraosseous needle in infants and children for pushing fluids.

Central venous access should be considered for children in fluid refractory shock as this access helps in infusion of vasoactive drugs and monitoring of central venous pressure.
Fluid therapy Optimization of circulating volume with help of fluids is
most important cornerstone of therapy in shock. Volume replacement should begin as 20 mL/kg IV while
one is trying to assess the etiology. Patients in hypovolemic and septic shock may require up to
60 mL/kg in first 1–1.5hours. Patients with septic shock may require up to 150–200mL/kg
within the first hour itself. Volume resuscitation beyond the first hour should be titrated to signs of improvedperfusion, age, appropriate mean arterial pressure (MAP), a mixed venous oxygen saturation of >70% and cardiac index > 3.3 L/minute/m2 (ACCM practice guidelines, 2008).

Cardiovascular Support Vasoactive drug therapy in the treatment of shock states
aims to increase oxygen delivery or organ perfusion or both.
The vasoactive agents used to support circulatory function may be classified as inotropes, vasopressors,vasodilators, and inodilators.
Increasing mean arterial pressure(MAP) to a level that allows appropriate distribution of cardiac output for adequate organ perfusion and hence oxygen delivery is one of the key functions of vasopressors.
Optimal preload is essential for all patients in shock before vasoactive therapy is contemplated.
How to Choose the Appropriate Drug? Vasodilators are the only class of agents that can increase
cardiac output and simultaneously reduce myocardial oxygen demand, e.g. nitroglycerin,nitroprusside. Inodilators (inotropes + vasodilator) improve cardiac contractility and reduce afterload, e.g. phosphodiesteraseinhibitors like milrinone and amrinone.
Children with severe sepsis can present with low cardiac output and high systemic vascular resistance (SVR) (cold shock) or low cardiac output and low SVR (warm shock).
Accordingly in the cold shock, inotropic support should be started in case of fluid refractory shock while a combination of inotrope together with a vasopressor is warranted in warm shock

Children with catecholamine resistant cold shock requiring inotropy can be treated with phosphodiesterase inhibitors like milrinone.
Children with primary cardiogenic shock can be treated with inotropes at the first go.
When an appropriate fluid challenge fails to restore adequate blood pressure and organ perfusion in patients with high cardiac output and low systemic vascular resistance (warm shock), vasopressor agents should be started.
Since children with septic shock more often have associated myocardial dysfunction as opposed to adults, it is preferable to combine inotropy with a vasopressor.
Prostaglandin E1, a potent vasodilator is indicated in newborns with ductus-dependent lesion presenting in cardiogenic shock due to ductus closure.

Correction of Metabolic Derangements Metabolic acidosis: Metabolic acidosis, poor tissue
perfusion and resultant anaerobic metabolism leads
to significant metabolic acidosis.
Acute renal failure: Adequate fluid replacement is
necessary to prevent development of renal failure. Dialysis
will be indicated in case of hyperkalemia, refractory
acidosis and fluid overload. The current trend is towards
early renal replacement therapy especially in septic shock
as this helps in removal of noxious triggers too.

Hematologic support, Gastrointestinal support,calciumNutritional support, Respiratory support should be given.
Antibiotic therapy: Appropriate empiric antibiotics
should be started in suspected septic shock. It should
provide broad-spectrum coverage depending upon site of
infection and local epidemiologic data regarding sensitivity pattern. An aminoglycoside (gentamicin or amikacin) and
a third-generation cephalosporin (cefotaxime, ceftriaxone) should be used for suspected Gram-negative sepsis.
Combination of cloxacillin and an aminoglycoside should
be used if staphylococcal sepsis is suspected.

Newer and Adjunctive TherapiesCorticosteroids: The 2008 Surviving Sepsis Campaign guidelines recommend
use of stress dose of steroids (hydrocortisone 50 mg/m2 per 24 hours) in children once they are diagnosed to have catecholamine-resistant septic shock and in suspected or proven adrenal insufficiency.
Newer inodilators: Levosimendan and enoximone are two new inodilatorsbeing investigated for use in cardiogenic shock. They possess inotropy as well as coronary and systemic vasodilatory properties. They increase myocytesensitivity to calcium and mediate vasodilatation throughactivation of adenosine triphosphate (ATP)-dependent potassium channels in
vascular smooth muscles.
Vasopressin: Vasopressors are used in the settingof warm shock having low SVR. Vasopressin is used as a second-line vasoconstrictor in patients withcatecholamine-resistant warm shock. However its experience in children is limited.


ref:
IAP textbook of pediatrics
Nelson textbook of pediatrics
thank you