share a patient provider agreement (ppa) … · 2018-06-21 · differential diagnostic...
TRANSCRIPT

SHAREAPATIENTPROVIDERAGREEMENT(PPA)WITHCLEARLYESTABLISHEDBOUNDARIESANDPATIENTEXPECTATIONSPRIORTOINITIATINGATRIALOFOPIOIDSFORCHRONICNON-CANCERPAINAPPAsignedbybothpatientandprescriberandgiventothepatientisanimportant,convenientcommunicationtoolthatcanalsodocumentpatientcounselingandeducation.OfferingaPPAtoallpatientsregardlessofapatient’sidentifiedriskofopioidmisuseandabusereducesstigmaandprovidesaminimallevelofprecaution/protectiontoprescriberandpatient.Thereisnostandard,validatedorlegallybindingformofaPPA;considerinclusionofinformedconsent(e.g.,potentialrisksandbenefitsofanopioidtrial,continuationanddiscontinuation)andplanofcare(e.g.,goalsofcareandexpectations,rightsandresponsibilitiesofprescriberandpatient).OPTIMIZEPATIENTTREATMENT(DRUG/NON-DRUG)USINGAMULTI-DIMENSIONALRATINGSCALETOASSESSCHRONICPAIN,QUALITYOFLIFEANDPROGRESSTOWARDFUNCTIONALGOALSThePEGisabriefmulti-dimensionalmeasureofPain,EnjoymentoflifeandGeneralactivityusefulatbaselineandatregularintervalstoassessanddocumentpatientresponsetotreatment.SetrealisticexpectationsthatfullpainreliefisunlikelyandsetindividualizedgoalsthatareAchievable,Recovery-related,andMeasurable(A.R.M.);e.g.,15minutedailywalk.Continueormodifyopioidtreatmentwithdemonstratedbenefit.Discontinuewhentherisksofsideeffects,misuse,addiction,and/oroverdoseoutweighthebenefit.Engagefamilyandotherkeyindividualswhenpossibletosupportpatient-obtainedinformation.SCREENFORAPPROPRIATEOPIOIDUSEANDTHECONTINUEDNEEDFOROPIOIDTHERAPY,INCLUDINGPRESCRIPTIONDRUGMONITORINGREPORTS(I.E.,SCRIPTSREPORTS)AssessanddocumentriskofopioidmisusewithsubjectiveandobjectivemeasuresPRIORtoprescribing,andindividualizelevelofmonitoringandpossibleco-managementtomatchtheidentifiedrisk.ReviewSCRIPTSreportsatbaselineandperiodicallytohelpidentifypotentialopioidmisuse/abuseandsupportsafeprescribinganddispensing.Continuetoassess,monitoranddocumentriskofopioidmisuse/abuse(includinginputfromfamilymembersandkeycontacts)sincerisklevelcanchangeforanypatientatanypoint.Adjustongoingmonitoringplan(e.g.,SCRIPTSreportreview,frequencyofvisits,urinedrugtests,pillcounts)tomatchrisklevel,andco-manageorreferforaddictiontreatmentasneeded.
Guidelinerecommendationsarelargelybasedonexpertconsensus,observationalorepidemiologicstudies,and/orfromguidelines.Fewstudiesdirectlyaddressquestionsofwhetherchangingpracticedecreasesrisk.Giventhepressingneedtoaddressopioid-relatedadverseoutcomes,guidelinedevelopersgenerallyagreeonforgingrecommendationsbasedonrelativelyweakorindirectevidencenowratherthanwaitingformorerigorousstudies.
DIFFERENTIALDIAGNOSTICCONSIDERATIONSFORABERRANTBEHAVIORS
ADDICTION:oftencharacterizedbybehaviorsthatmayincludelossofcontrolregardingdruguse,craving,compulsiveuseandcontinuedusedespiteharmtohealthorrelationships*Physicaldependenceandtolerancearenormalphysiologicadaptationstoextendedopioidtherapyandarenotthesameasaddiction.
PHYSICALDEPENDENCE:biologicadaptationtoadrugthatresultsinabstinencesyndrome(signsandsymptomsofwithdrawal)uponcessation,rapiddosereductionand/oradministrationofantagonistTOLERANCE:aphysiologicstateofreducedeffectovertimefromregulardrugexposureinwhichincreaseddosageisneededtoproducespecificeffect(increaseindoseandnoincreaseineffectmaymeanopioidisineffective)HYPERALGESIA:increaseinpainsensitivitythatcanbeseenwithrapidopioiddoseescalationorhighopioiddose(considerifincreaseinpainwithincreaseindose)PSEUDO-ADDICTION:aberrantdrug-relatedbehaviorsdrivenbyuncontrolledpain(reliefseekingvsdrugseeking)thatarereducedbyimprovedpaincontrolOTHERPSYCHIATRICILLNESSES:anxiety,depression,PTSD,“chemicalcoping”(knowinglyorunknowinglytakingmedicationstodecreaseornumbnegativeemotions)DIVERSION:movingmedicationsfromlegal/medicallyindicateduserstoillegal/unauthorizedusers
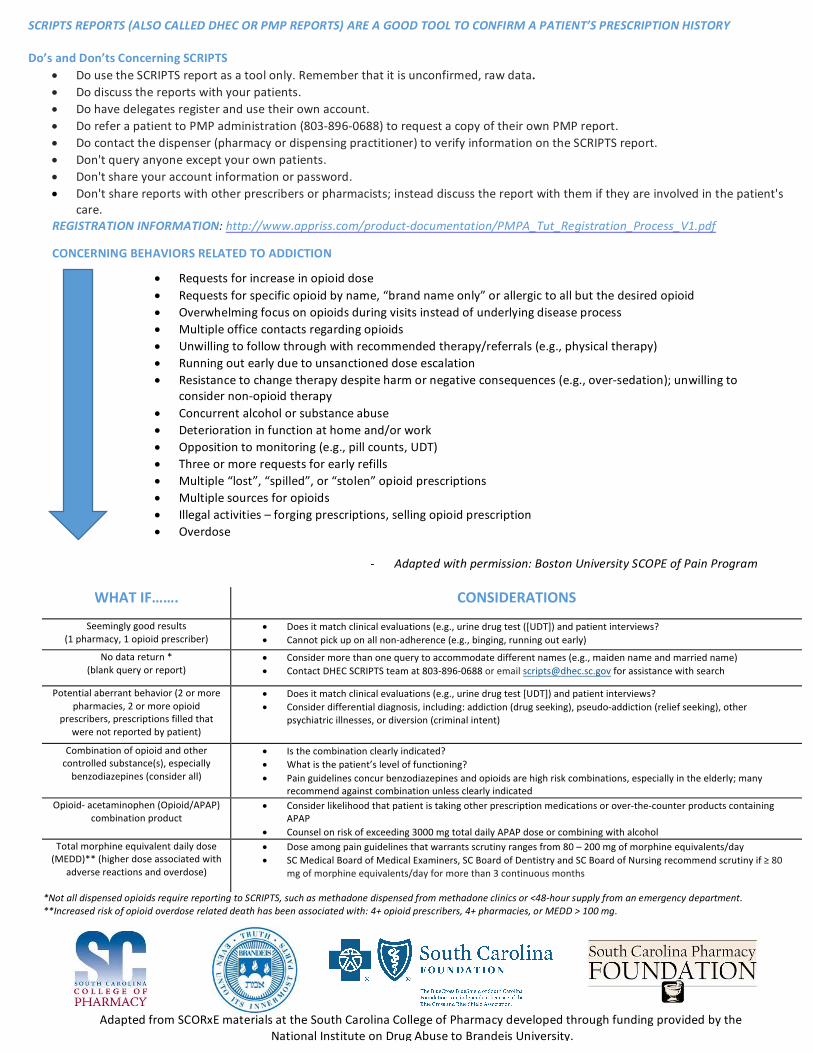
WHATIF……. CONSIDERATIONS
Seeminglygoodresults(1pharmacy,1opioidprescriber)
• Doesitmatchclinicalevaluations(e.g.,urinedrugtest([UDT])andpatientinterviews?• Cannotpickuponallnon-adherence(e.g.,binging,runningoutearly)
Nodatareturn*(blankqueryorreport)
• Considermorethanonequerytoaccommodatedifferentnames(e.g.,maidennameandmarriedname)• ContactDHECSCRIPTSteamat803-896-0688oremailscripts@dhec.sc.govforassistancewithsearch
Potentialaberrantbehavior(2ormorepharmacies,2ormoreopioid
prescribers,prescriptionsfilledthatwerenotreportedbypatient)
• Doesitmatchclinicalevaluations(e.g.,urinedrugtest[UDT])andpatientinterviews?• Considerdifferentialdiagnosis,including:addiction(drugseeking),pseudo-addiction(reliefseeking),other
psychiatricillnesses,ordiversion(criminalintent)
Combinationofopioidandothercontrolledsubstance(s),especiallybenzodiazepines(considerall)
• Isthecombinationclearlyindicated?• Whatisthepatient’sleveloffunctioning?• Painguidelinesconcurbenzodiazepinesandopioidsarehighriskcombinations,especiallyintheelderly;many
recommendagainstcombinationunlessclearlyindicatedOpioid-acetaminophen(Opioid/APAP)
combinationproduct• Considerlikelihoodthatpatientistakingotherprescriptionmedicationsorover-the-counterproductscontaining
APAP• Counselonriskofexceeding3000mgtotaldailyAPAPdoseorcombiningwithalcohol
Totalmorphineequivalentdailydose(MEDD)**(higherdoseassociatedwith
adversereactionsandoverdose)
• Doseamongpainguidelinesthatwarrantsscrutinyrangesfrom80–200mgofmorphineequivalents/day• SCMedicalBoardofMedicalExaminers,SCBoardofDentistryandSCBoardofNursingrecommendscrutinyif≥80
mgofmorphineequivalents/dayformorethan3continuousmonths
SCRIPTSREPORTS(ALSOCALLEDDHECORPMPREPORTS)AREAGOODTOOLTOCONFIRMAPATIENT’SPRESCRIPTIONHISTORYDo’sandDon’tsConcerningSCRIPTS
• DousetheSCRIPTSreportasatoolonly.Rememberthatitisunconfirmed,rawdata.• Dodiscussthereportswithyourpatients.• Dohavedelegatesregisterandusetheirownaccount.• DoreferapatienttoPMPadministration(803-896-0688)torequestacopyoftheirownPMPreport.• Docontactthedispenser(pharmacyordispensingpractitioner)toverifyinformationontheSCRIPTSreport.• Don'tqueryanyoneexceptyourownpatients.• Don'tshareyouraccountinformationorpassword.• Don'tsharereportswithotherprescribersorpharmacists;insteaddiscussthereportwiththemiftheyareinvolvedinthepatient's
care.REGISTRATIONINFORMATION:http://www.appriss.com/product-documentation/PMPA_Tut_Registration_Process_V1.pdf
• Requestsforincreaseinopioiddose• Requestsforspecificopioidbyname,“brandnameonly”orallergictoallbutthedesiredopioid• Overwhelmingfocusonopioidsduringvisitsinsteadofunderlyingdiseaseprocess• Multipleofficecontactsregardingopioids• Unwillingtofollowthroughwithrecommendedtherapy/referrals(e.g.,physicaltherapy)• Runningoutearlyduetounsanctioneddoseescalation• Resistancetochangetherapydespiteharmornegativeconsequences(e.g.,over-sedation);unwillingto
considernon-opioidtherapy• Concurrentalcoholorsubstanceabuse• Deteriorationinfunctionathomeand/orwork• Oppositiontomonitoring(e.g.,pillcounts,UDT)• Threeormorerequestsforearlyrefills• Multiple“lost”,“spilled”,or“stolen”opioidprescriptions• Multiplesourcesforopioids• Illegalactivities–forgingprescriptions,sellingopioidprescription• Overdose
- Adaptedwithpermission:BostonUniversitySCOPEofPainProgram
CONCERNINGBEHAVIORSRELATEDTOADDICTION
AdaptedfromSCORxEmaterialsattheSouthCarolinaCollegeofPharmacydevelopedthroughfundingprovidedbytheNationalInstituteonDrugAbusetoBrandeisUniversity.
*NotalldispensedopioidsrequirereportingtoSCRIPTS,suchasmethadonedispensedfrommethadoneclinicsor<48-hoursupplyfromanemergencydepartment.**Increasedriskofopioidoverdoserelateddeathhasbeenassociatedwith:4+opioidprescribers,4+pharmacies,orMEDD>100mg.