sexual addiction, sexual compulsivity, sexual …faculty.buffalostate.edu/macleamg/440/bancroft 2004...
TRANSCRIPT

Sexual Addiction, Sexual Compulsivity, Sexual Impulsivity, or What?Toward a Theoretical Model
John Bancroft and Zoran VukadinovicThe Kinsey Institute, Indiana University
We critically review the concepts of sexual addiction, sexual compulsivity, and sexual impulsivity and discuss their theo-retical bases. A sample of 31 self-defined sex addicts was assessed by means of interview and questionnaires and comparedwith a large age-matched control group. A tendency to experience increased sexual interest in states of depression or anxi-ety was strongly characteristic of the sex addict group. Dissociative experiences were described by 45% of sex addicts andmay have some explanatory relevance. Obsessive-compulsive mechanisms may be relevant in some cases, and the addictionconcept may prove to be relevant with further research. Overall, results suggested that out of control sexual behavior resultsfrom a variety of mechanisms. We propose an alternative theoretical approach to investigating these mechanisms based onthe dual control model and recent research on the relation between mood and sexuality.
Increasing attention is being paid to the concept of sex-ual behavior that is, in some way, out of control. Much ofthe recent literature has employed two currently fashion-able concepts: compulsive sexual behavior and sexualaddiction. At this time, both concepts are of uncertain sci-entific value. Barth and Kinder (1987) argued for the use ofimpulse control disorder as a description, which in contrastwith the compulsivity and addiction labels is consistentwith DSM criteria but which has little explanatory valuebeyond inferring a problem of self-control. In the past,other labels such as nymphomania, satyriasis, and hyper-sexuality have been used (Rinehart & McCabe, 1997)
A crucial issue that has received little attention is theextent to which out of control sexual behavior can beunderstood as a behavioral pattern at the extreme of thenormal range, or rather a behavioral pattern that is qualita-tively different from the norm in ways that are problemat-ic (see Orford, 1978, for earlier discussion of this issue).
The literature on sexual compulsivity and sexual addic-tion has been preoccupied with issues of definition, par-ticularly pertaining to DSM-IV, and has paid very littleattention to possible causal explanations for why, in suchcases, sexual behavior becomes problematic. Researchersoften make statements about likely mechanisms (e.g.,anxiety reduction or mood regulation), but these are moreoften based on clinical impression than on reported data.This discrepancy led Gold and Heffner (1998) to title theirreview paper "Sexual Addictions: Many Conceptions,Minimal Data."
Of the few data-based studies to date, three have exam-ined potentially relevant comorbidity. Quadland (1985) com-pared 30 gay men presenting for treatment for compulsive
This study was made possible, in part, by NIMH Grant R0I-MH60519-02.Address correspondence to John Bancroft, M.D., Director, The Kinsey
Institute for Research in Sex, Gender, and Reproduction, Morrison Hall 313,Indiana University, Bloomington, IN 47405-3700; e-mail: [email protected].
sexual behavior with an age-matched group of 24 gay menwho were presenting for treatment for nonsexual problems.While he found differences in their patterns of sexual behav-ior (e.g., number of sexual partners and duration of sexualrelationships), he found no group differences in mood or per-sonahty disorder. Raviv (1993) found that 32 self-identifiedsex addicts had higher mean scores than 38 controls onSymptom Checklist-90-R (SCL-90-R) scales for anxiety,depression, obsessive-compulsiveness, and interpersonalsensitivity. In an uncontrolled study of 37 subjects with self-defined "out-of-control" sexual behavior. Black, Kehrberg,Flumerfelt, and Schlosser (1997) found a high prevalence ofcomorbidity with psychiatric conditions, most notably life-time histories of substance use disorders (64%), anxiety dis-orders (50%), and mood disorders (39%).
Researchers are paying more attention to the fact thatout of control sexual behavior can be reduced with moodelevating drugs such as the SSRIs (Fedoroff, 1993; Kafka,2000; Stein et al., 1992). As yet, we do not know the extentto which such pharmacological benefits, when they occur,result from improvement in mood or specific inhibition ofsexual response or both.
The best review of the literature in terms of theoreticalmodels is by Goodman (1997); we consider some of hisconclusions further in the discussion. However, few of thesetheoretical ideas have been formulated in ways suitable fortesting. In this project we explored the relevance of a newtheoretical model to out of control sexual behavior, testingsome preliminary hypotheses with a small study of self-defined sex addicts. We followed this with a more detaileddiscussion of the theoretical possibilities and some furtherdevelopment of our own eminently testable theoreticalideas, particularly relating to the impact of negative mood.
If we assume that anxiety reduction or mood improve-ment is a key factor in many cases of out of control sexualbehavior, we need to reconcile this with the conventionalwisdom that most people experience a decline in sexual
The Journal of Sex Research Volume 41, Number 3, August 2004: pp. 225-234 225
226 Sexual Addiction, Compulsivity, Impulsivity
interest and/or responsiveness in negative mood states(Araujo, Mohr, & McKinlay, 2003; Beck, 1967; Cassidy,Flanagan, Spellman, & Cohen, 1957; Kennedy, Dickens,Eisfeld, & Bagby, 1999). In addition, we must ask whysuch behavioral patterns persist and even worsen if themood-enhancing effects are not only transient but havesuch negative consequences.
Some evidence exists that the relationship between nega-tive mood and sexuality is paradoxical in some individuals,with increased sexual interest occurring in association withnegative mood (Angst, 1998; Mathew & Weinman, 1982;Nofzinger et al., 1993). We have been studying this rela-tionship at The Kinsey Institute using a simple trait measure,the Mood and Sexuality Questionnaire (MSQ, see below),which asks respondents to rate on a bipolar scale what typi-cally happens to (a) their sexual interest and (b) their sexu-al responsiveness when they are depressed or experiencinganxiety. We have reported our initial findings for 919 het-erosexual men (Bancroft, Janssen, Strong, Cames, et al.,2003a) and 662 gay men (Bancroft, Janssen, Strong, &Vukadinovic, 2003). Whereas the majority in both samplesreported a decrease in sexual interest when depressed oranxious, a minority (15-25%) reported an increase, some-what higher with anxiety than with depression. Qualitativedata from these two studies indicate a more complex rela-tionship between depression and sexuality than betweenanxiety and sexuality. Thus, increased sexual interest whendepressed can indicate increased desire for sex or the needfor personal contact or validation by another person.Conversely, those with a negative association betweendepression and sexual interest may experience a simplereduction in sexual interest, or a mood-related need to avoidpersonal contact because of low self-esteem. With anxiety,the typical patterns are either a preoccupation with the causeof the anxiety or stress, so sex goes "out of mind," or sexemerges as a means for achieving at least transient reductionof anxiety following orgasm. The idea that some individualsmay be more likely to pursue sexual interaction or stimula-tion or to become sexually aroused when in a negative moodstate is of considerable potential relevance to understandingout of control patterns of sexual behavior.
Our dual control model of sexual response (Bancroft,1999; Bancroft & Janssen, 2000) postulates that the occur-rence of sexual arousal depends on a balance between sex-ual excitation and inhibition of sexual response and thatindividuals vary in their propensity for both excitation andinhibition, with typical inhibition proneness being adap-tive across species. That is, in threatening situations whereattention needs to be focused on nonsexual coping, inhibi-tion of sexual arousal reduces the likelihood of being sex-ually distracted. Janssen, Vorst, Finn, and Bancroft (2002a,b) developed a questionnaire to measure these propensities(SIS/SES). It contains three scales, one measuring excita-tion proneness (SES) and the other two inhibition prone-ness. Based on the items making up each scale, Janssen etal. labeled the first inhibition factor (SISl) "inhibition inresponse to threat of performance failure" and the second
(SIS2) "inhibition in response to threat of performanceconsequences." Scores on these three scales show close tonormal distributions in nonclinical samples of both menand women. This is consistent with the idea that middlerange scores in each case reflect adaptive response patternswhile more extreme scores reflect maladaptive responsepatterns. Thus, high SISl scores have been shown to bestrongly related to vulnerability to erectile dysfunction inmen (Bancroft & Janssen, 2000), and low SIS2 scores tocertain aspects of sexual risk-taking in both gay (Bancroft,Janssen, Strong, Cames, et al., 2003b) and heterosexual(Bancroft et al., 2004) men.
We have used our theoretical model to explain paradoxi-cal increase of sexual interest in negative mood states. Onthe assumption that situations that induce negative moodnormally inhibit sexual interest and arousal to allow maxi-mum focus on the coping process, we postulated that para-doxical increase in sexual interest in negative mood statesrequires unusually low levels of inhibition of sexualresponse (as measured by SIS2) and relatively high levels ofsexual arousability (as measured by SES). In our study ofheterosexual men (Bancroft, Janssen, Strong, Cames, et al.,2003a), we obtained some support for this hypothesis withour SIS/SES measures, together with a trait measure ofdepression proneness (ZDPR) and anxiety proneness(STAI), accounting for 19% of the variance in MSQ scores.In our parallel study of gay men (Bancroft, Janssen, Strong,& Vukadinovic, 2003), we were only able to account for 4%of the variance in this way. We have also postulated(Bancroft, Janssen, Strong, Cames, et al., 2003b) that theparadoxical effect of anxiety on sexuality could be an exam-ple of excitation transfer (Zillman, 1983), which occurswhen arousal induced in association with anxiety becomesincorporated into response to sexual stimuli in those withlow inhibition of sexual response.
In our studies of high risk sexual behavior, we foundsome interesting contrasts between the predictive value ofSIS2 (sexual inhibition due to the threat of performance con-sequences) and of MSQ (relation between negative moodand sexuality). In both straight and gay men, low SIS2 waspredictive of non-use of condoms; that is, the persistence ofsexual arousal in potentially risky sexual interactions reducesthe likelihood of using a condom. Our measure of sexualinterest when depressed (MS-1) was predictive of the num-ber of casual partners but not of condom use (Bancroft et al.,2004; Bancroft, Janssen, Strong, Cames, et al., 2003a). Ingay men, our measure of sexual interest in states of anxiety(MS-3) was more strongly predictive of masturbation fre-quency than of frequency of sexual activity with a partner(Bancroft, Janssen, Strong, & Vukadinovic, 2003).
High risk sexual behavior overlaps with but is not thesame as out of control sexual behavior. However, on thebasis of these findings, we formulated the followinghypotheses as relevant to out of control sexual behavior:
1. A tendency to increased sexual interest and responsivenessduring negative mood states will be more common in menwith out of control sexual behavior.
Bancroft and Vukadinovic 227
2. Increased sexual interest associated with anxiety will be prin-cipally associated with out of control masturbation.
3. Increased sexual interest associated with depression will beassociated with out of control interaction with sexual partners(e.g., increased number of sexual partners).
4. In general, out of control sexual behavior will be more likelyin men with a combination of high SES and low SIS2, partlybecause of the paradoxical association between negative moodand sexuality and partly because of a more direct impact ofhigh arousal and low inhibition on self-regulation.
In this project, we used a combination of interviews andquestionnaires with a small sample of self-designated sexaddicts to explore these theoretical possibilities, as well asother qualitative descriptions of the out of control sexualexperience. We have also used an age-matched controlgroup for evaluation of the questionnaire data.
METHODS
Participants
Following distribution of leafiets describing the researchproject to local Sex Addicts Anonymous (SAA) groups, 22SAA members volunteered to be interviewed and completequestionnaires (20 male and 2 female). Interviews wererecorded and transcribed. Each volunteer signed aninformed consent sheet and was paid $35 for his or her par-ticipation. In addition, 11 self-defined sexual addictionpatients (all male) attending The Kinsey Institute SexualHealth Clinic were assessed in a similar fashion. Thesepatients were asked to sign an informed consent sheet andwere charged only half of the usual clinic fee as compensa-tion. We obtained approval for the study from the IndianaUniversity Bloomington Human Subjects Committee.
To allow testing of our specific hypotheses with the ques-tionnaire data from the male sample, we derived an age-matched sample from our two studies of mood and sexuality(Bancroft, Janssen, Strong, Cames, et al., 2003a; Bancroft,Janssen, Strong, & Vukadinovic, 2003). First, we excludedthose outside the age range of the sex addicts group Q2-66).We then randomly selected a 50% sample from each orien-tation group. This produced the same mean age for the het-erosexual men. The gay men were, however, younger, so werandomly deleted individual cases from the lower part of theage range until the same mean age was achieved. These twosubsamples—heterosexual, n = 196, 57.8%, and homosexu-al, n = 143, 42.2%—were then combined (« = 339).'
Interviews
Issues covered in the research interviews included the type ofbehavior involved, the importance of novelty or specificity.
' A comparison of the heterosexual and gay subgroups showed that there weresome significant differences in our trait measures. The homosexual group scoredhigher on SISl (30.2 vs. 27.9, p < .001), ZDPR (58.3 vs. 50.1,/)< .001), MS-1(4.1 vs. 3.6, p = .04), and MS-3 (4.6 vs. 4.1,p = .03).
the steps in a typical sequence, whether participants usuallyattempt to resist the urge to "act out," their state of mindwhile acting out, the extent to which the participants canexercise control over their behavior, how various mood statesaffect the acting out behavior, and the extent to which theyuse acting out to improve mood. We also asked questionsabout whether the individual had been sexually abused as achild, whether religion was important, whether there wasevidence of other types of addictive behavior, and whetherthere was a family history of addictive disorders. Similarquestions were asked of the clinic patients. Volunteer inter-views were audiorecorded and transcribed. We then analyzedthe content of the transcripts along with the case notes fromthe clinic patients to identify presence or absence of the keyvariables reported in this paper.
Materials
All male participants completed the following two ques-tionnaires.
The Mood and Sexuality Questionnaire (MSQ;Bancroft, Janssen, Strong, Cames, et al., 2003a; Bancroft,Janssen, Strong, Vukadinovic, 2003). This instmment is atrait measure that asks respondents to indicate what typi-cally happens to (a) sexual interest and (b) erectile respon-siveness when they are depressed (MS-1 and MS-2) andwhen they are anxious or stressed (MS-3 and MS-4; e.g.,"When you have felt depressed what typically happens toyour sexual interest/response?"). Each item is answered ona bipolar scale with 5 indicating no change, 1 markedreduction, and 9 marked increase. The range for each indi-vidual item is, therefore, 1 to 9, and for the sum score (MS-total) of the four scales, 4 to 36 (Cronbach's a = .85). Foreach mood state, there is a box to check if the subject hasnever been depressed (or anxious) enough to find out.Subjects checking this box are excluded from analysesinvolving this variable. We reported only MS-1 and MS-3in this paper.
Sexual Inhibition/Sexual Excitation Scales (SIS/SES;Janssen et al., 2002a, b). This questionnaire, with 45 items,measures three factors: (a) propensity for sexual excitation(SES; range = 20-80); (b) propensity for sexual inhibitiondue to the threat of performance failure (SISl; range = 14-56); and (c) propensity for sexual inhibition due to thethreat of performance consequences (SIS2; range = 1 1 -44). The response for each item ranges from 1 = stronglyagree to 4 = strongly disagree. Cronbach alphas for thethree scales are .88, .83, and .66, respectively. Scores oneach of these scales are close to normally distributed in theapproximately 2,500 men we have so far tested. The scaleshave good discriminant validity with only modest overlapwith measures of global traits of behavioral inhibition,harm avoidance, and reward responsivity.
The following questionnaire was completed by the SAAvolunteers and all the age-matched controls, but not theclinic sex addicts.
Zemore Depression Proneness Ratings (ZDPR; Zemore,Fischer, Garratt, & Miller, 1990). This is a trait measure of
228 Sexual Addiction, Compulsivity, Impulsivity
propensity for depression in terms of frequency and sever-ity. We used the 13-item version. All questions begin,"Compared to most people you know...." Three of thequestions conclude, (a) "...how often do you getdepressed?"; (b) "...how long do your depressions last?";and (c) "...how deeply depressed do you become?" Tenfurther questions ask how often the participant experiencesa variety of depressive symptoms (e.g., feeling discouragedabout the future, feeling guilty or unworthy). Each questionis answered on a Likert-type scale from 1 (e.g., much less)to 9 (e.g., much more), with 5 indicating the same "as oth-ers you know." The range of scores on this measure is there-fore 13 to 117. Zemore et al. (1990) reported on the relia-bility and validity of the ZDPR. Factor analysis showed asingle factor structure accounting for 44% of the variancewith a Cronbach alpha coefficient of .90.
RESULTS
Two SAA volunteers described behavioral patterns (onepedophilic, aged 47, the other exhibitionist, aged 38) thatwere not described as out of control but rather as behaviorsthey would want to do if they could "get away with it."Both of these men obtained some benefit from regardingthemselves as sex addicts, but as they did not report out ofcontrol sexual behavior they were not included in furtheranalyses. This left 29 men, mean age 40.1 years, and 2women, ages 38 and 41 years.
Behavioral Patterns
Twenty-two men were heterosexual, 1 bisexual, and 6homosexual in orientation; both women were heterosexu-al. Ten men reported paraphilic behaviors (6 involvingchildren, 5 voyeurism, and 3 exhibitionism). Five of thegay men were "compulsive cruisers." Nineteen men andboth women described "compulsive masturbation" as theirprincipal form of acting out. One of the women told a storyreminiscent of persistent sexual arousal disorder (Leiblum& Nathan, 2001), describing herself masturbating as "likea gerbil on a wheel."
The relevance of mood. Of the 31 subjects, only 4 menstated that their sexual acting out was not predictablyaffected by their mood. Seventeen subjects reported beingmore likely to sexually act out when depressed, and 19reported this in relation to anxiety or stress. Eleven sub-jects (9 men and both women) reported an increase in act-ing out in states of both depression and anxiety. Two mensaid that they were less likely to act out when depressed;no one said this in relation to anxiety. There was no appar-ent difference between those reporting increased acting outwhen depressed and those reporting it when anxious interms of the types of behaviors involved.
Resistance to acting out. Subjects were asked whetherthey found themselves trying to resist the urge to act out orwhether at the time it was something they genuinely want-ed to do. Eleven men and one of the women indicated thatthey tried to resist, but most of them did not give a con-vincing description of resistance. One man, for example.
said "sometimes I've wanted to, sometimes I've fought it,and sometimes I've done it without thinking." Another gayman with compulsive cruising said, "I tell myself not to doit, but I do it anyway." He went on to say that he devisestactics to avoid cruising and then forgets them. Anotherman, when asked to explain how he resisted, said, "I wantto do it, yet I know it's unhealthy for me."
The two most convincing accounts of resistance werefrom men with obsessive-compulsive personalities. In bothcases the sexual acting out was masturbation. In one case,the participant had intrusive thoughts about teenage boysor a compulsion to look at pictures of them. This lead toconsiderable guilt and resistance, and he obtained a verytransient calming effect by masturbating, followed quicklyby renewed guilt and depression. It should be noted herethat the resistance was to the intrusive thoughts about boysrather than the masturbation. The other man described pre-occupation with sexual thoughts, which would lead tomasturbation followed by a need to take a shower becauseof the "dirtiness" of the act.
State of mind during sexual acting out. Thirteen menand one woman described a typical state of mind sugges-tive of some degree of dissociation. The following areillustrative descriptions, each from a different subject:".. .just find myself doing it... another voice in my head";"...an overpowering drive...nothing else is under consid-eration"; ".. .numb, completely zoning out, not present, notconscious of reality"; "trancelike...there seems to be achemical or hormonal difference in me"; "...eyes glazed,numbing...unfeeling...focusing on the pleasure";"...trancelike state...kills time and pain...numb like adream"; "I'm not aware of anything else...I block every-thing out...my preoccupation"; "When I'm sexuallyaroused, I click out"; "...suspension of reality—nothingelse enters your mind"; "...like being taken over—a dif-ferent person—trancelike, peaceful"; "...feel detachedfrom what is happening"; "...like euphoria—likecocaine"; "I shut myself off to everything and I am oblivi-ous of what I am doing"; ".. .like a drug to numb out."
Other addictive patterns. Ten subjects reported otheraddictive patterns either currently or in their past: 3 withdrugs, 4 with alcohol, and 3 with both drugs and alcohol.One man described overeating, another addiction to com-puter games, and one of the women described shoppingsprees. Fifteen subjects, 4 of them with their own addictionhistories, reported addiction problems in other familymembers.
Questionnaire Data in Male Subjects
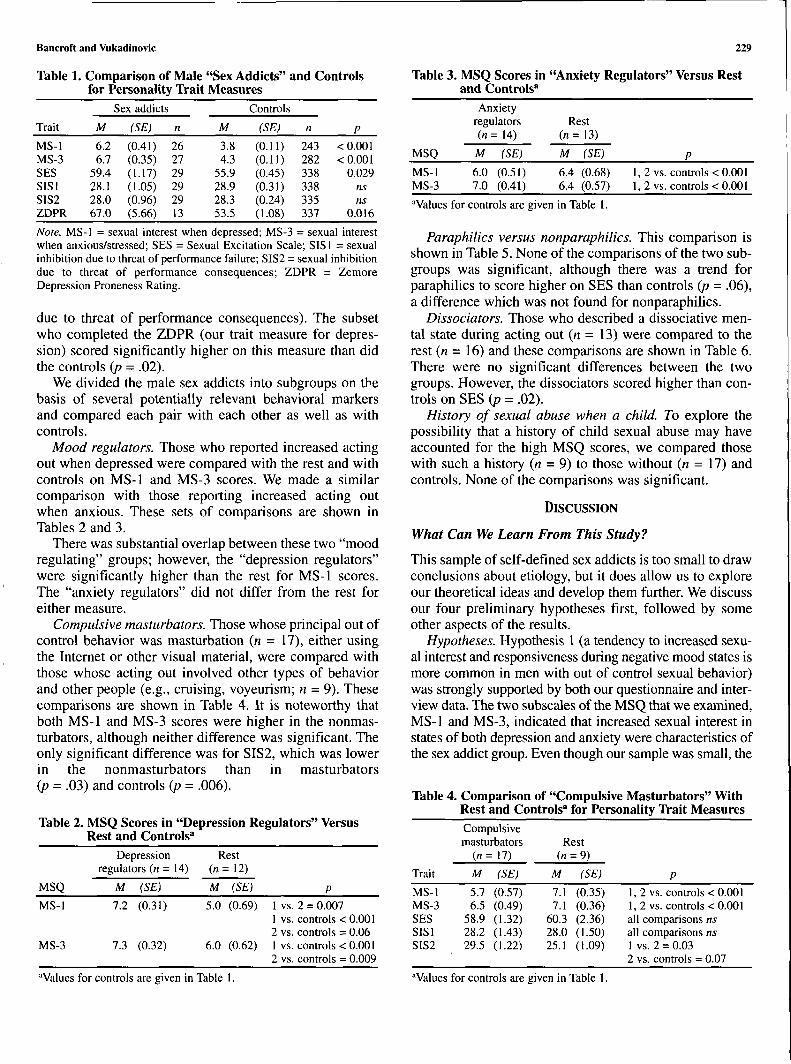
Comparison of our measures for the male sex addicts andfor the controls is shown in Table 1. The sex addicts report-ed significantly higher MS-1 (sexual interest whendepressed) and MS-3 (sexual interest when anxious)scores than did the controls {p < .001 in each case). Theyalso had higher SES (sexual excitation) scores (p - .029),but did not differ from controls in either SISl (inhibitiondue to threat of performance failure) or SIS2 (inhibition
Bancroft and Vukadinovic 229
Table 1. Comparison of Male "Sex Addicts" and Controlsfor Personality Trait Measures
Table 3. MSQ Scores in "Anxiety Regulators" Versus Restand Controls"
Sex addicts Controls
Trait
MS-1MS-3SESSISlSIS2ZDPR
M
6.26.7
59.428.128.067.0
(SE)
(0.41)(0.35)(1.17)(1.05)(0.96)(5.66)
n
262729292913
M
3.84.3
55.928.928.353.5
(SE)
(0.11)(0.11)(0.45)(0.31)(0.24)(1.08)
n
lA-i282338338335337
P
< 0.001< 0 001
0.029nsns
0.016
Note. MS-1 = sexual interest when depressed; MS-3 = sexual interestwhen anxious/stressed; SES = Sexual Excitation Scale; SISl = sexualinhibition due to threat of performance failure; SIS2 = sexual inhibitiondue to threat of performance consequences; ZDPR = ZemoreDepression Proneness Rating.
due to threat of performance consequences). The subsetwho completed the ZDPR (our trait measure for depres-sion) scored significantly higher on this measure than didthe controls (p - .02).
We divided the male sex addicts into subgroups on thebasis of several potentially relevant behavioral markersand compared each pair with each other as well as withcontrols.
Mood regulators. Those who reported increased actingout when depressed were compared with the rest and withcontrols on MS-1 and MS-3 scores. We made a similarcomparison with those reporting increased acting outwhen anxious. These sets of comparisons are shown inTables 2 and 3.
There was substantial overlap between these two "moodregulating" groups; however, the "depression regulators"were significantly higher than the rest for MS-1 scores.The "anxiety regulators" did not differ from the rest foreither measure.
Compulsive masturbators. Those whose principal out ofcontrol behavior was masturbation (n = 17), either usingthe Internet or other visual material, were compared withthose whose acting out involved other types of behaviorand other people (e.g., cruising, voyeurism; n = 9). Thesecomparisons are shown in Table 4. It is noteworthy thatboth MS-1 and MS-3 scores were higher in the nonmas-turbators, although neither difference was significant. Theonly significant difference was for SIS2, which was lowerin the nonmasturbators than in masturbators(p = .03) and controls (p = .006).
Table 2. MSQ Scores in "Depression Regulators" VersusRest and Controls"
MSQ
MS-1MS-3
Anxietyregulators(n = 14)
M (SE)
6.0 (0.51)7.0 (0.41)
Rest(n=13)
M
6.46.4
(SE)
(0.68)(0.57)
1,1,
2 vs.2 vs.
P
controls < 0.001controls < 0.001
"Values for controls are given in Table 1.
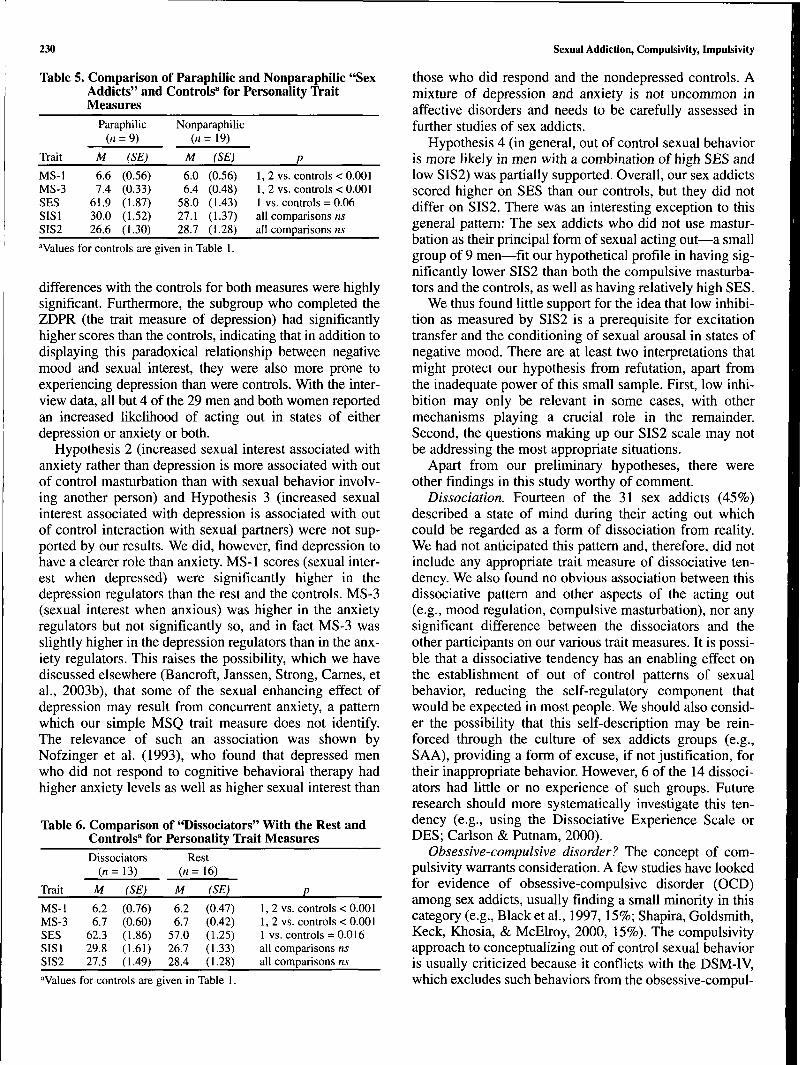
Paraphilics versus nonparaphilics. This comparison isshown in Table 5. None of the comparisons of the two sub-groups was significant, although there was a trend forparaphilics to score higher on SES than controls {p = .06),a difference which was not found for nonparaphilics.
Dissociators. Those who described a dissociative men-tal state during acting out (n = 13) were compared to therest (n = 16) and these comparisons are shown in Table 6.There were no significant differences between the twogroups. However, the dissociators scored higher than con-trols on SES ip = .02).
History of sexual abuse when a child. To explore thepossibility that a history of child sexual abuse may haveaccounted for the high MSQ scores, we compared thosewith such a history (n = 9) to those without (n = 17) andcontrols. None of the comparisons was significant.
DISCUSSION
What Can We Learn From This Study?
This sample of self-defined sex addicts is too small to drawconclusions about etiology, but it does allow us to exploreour theoretical ideas and develop them further. We discussour four preliminary hypotheses first, followed by someother aspects of the results.
Hypotheses. Hypothesis 1 (a tendency to increased sexu-al interest and responsiveness during negative mood states ismore common in men with out of control sexual behavior)was strongly supported by both our questionnaire and inter-view data. The two subscales of the MSQ that we examined,MS-1 and MS-3, indicated that increased sexual interest instates of both depression and anxiety were characteristics ofthe sex addict group. Even though our sample was small, the
Table 4. Comparison of "Compulsive Maslurbators" WitbRest and Controls" for Personality Trait MeasuresCompulsivemasturbators Rest
Depression Rest
MSQ
MS-1
MS-3
regulators (n - 14)
M
7.2
7.3
(SE)
(0.31)
(0.32)
(n
M
5.0
6.0
= 12)
(SE)
(0.69)
(0.62)
11212
vs.vs.vs.vs.vs.
p
2 = 0.007controls < 0.001controls = 0.06controls < 0.001controls = 0.009
Trait
MS-1MS-3SESSISlSIS2
M
5.76.5
58.928.229.5
(SE)
(0.57)(0.49)(1.32)(1.43)(1.22)
M
7.17.1
60.328.025.1
(SE)
(0.35)(0.36)(2.36)(1.50)(1.09)
P
1, 2 vs. controls < 0.0011, 2 vs. controls < 0.001all comparisons nsall comparisons ns1 vs. 2 = 0.032 vs. controls = 0.07
"Values for controls are given in Table "Values for controls are given in Table 1.
230 Sexual Addiction, Compulslvity, Impulsivity
Table 5. Comparison of Paraphilic and Nonparaphilic "SexAddicts" and Controls" for Personality TraitMeasures
Trait
MS-1MS-3SESSISISIS2
Paraphilic(«
M
6.67.4
61.930.026.6
= 9)
(SE)
(0.56)(0.33)(1.87)(1.52)(1.30)
Nonparaphilic(n
M
6.06.4
58.027.128.7
= 19)
(SE)
(0.56)(0.48)(1.43)(1.37)(1.28)
P1,2 vs. controls < 0.0011,2 vs. controls < 0.0011 vs. controls = 0.06all comparisons nsall comparisons ns
"Values for controls are given in Table 1.
differences with the controls for both measures were highlysignificant. Furthermore, the subgroup who completed theZDPR (the trait measure of depression) had significantlyhigher scores than the controls, indicating that in addition todisplaying this paradoxical relationship between negativemood and sexual interest, they were also more prone toexperiencing depression than were controls. With tiie inter-view data, ail but 4 of the 29 men and both women reportedan increased likelihood of acting out in states of eitherdepression or anxiety or both.
Hypothesis 2 (increased sexual interest associated withanxiety rather than depression is more associated with outof control masturbation than with sexual behavior involv-ing another person) and Hypothesis 3 (increased sexualinterest associated with depression is associated with outof control interaction with sexual partners) were not sup-ported by our results. We did, however, find depression tohave a clearer role than anxiety. MS-1 scores (sexual inter-est when depressed) were significantly higher in thedepression regulators than the rest and the controls. MS-3(sexual interest when anxious) was higher in the anxietyregulators but not significantly so, and in fact MS-3 wasslightly higher in the depression regulators than in the anx-iety regulators. This raises the possibility, which we havediscussed elsewhere (Bancroft, Janssen, Strong, Cames, etal., 2003b), that some of the sexual enhancing effect ofdepression may result from concurrent anxiety, a patternwhich our simple MSQ trait measure does not identify.The relevance of such an association was shown byNofzinger et al. (1993), who found that depressed menwho did not respond to cognitive behavioral therapy hadhigher anxiety levels as well as higher sexual interest than
Table 6. Comparison of "Dissociators" With tbe Rest andControls" for Personality Trait Measures
Trait
MS-1MS-3SESSISISIS2
Dissociators(n =
M
6.26.7
62.329.827.5
= 13)
(SE)
(0.76)(0.60)(1.86)(1.61)(1.49)
Rest(n =
M
6.26.7
57.026.728.4
:16)
(SE)
(0.47)(0.42)(1.25)(1.33)(1.28)
P
1,2 vs. controls < 0.0011, 2 vs. controls < 0.0011 vs. controls = 0.016all comparisons nsall comparisons ns
"Values for controls are given in Table 1.
those who did respond and the nondepressed controls. Amixture of depression and anxiety is not uncommon inaffective disorders and needs to be carefully assessed infurther studies of sex addicts.
Hypothesis 4 (in general, out of control sexual behavioris more likely in men with a combination of high SES andlow SIS2) was partially supported. Overall, our sex addictsscored higher on SES than our controls, but they did notdiffer on SIS2. There was an interesting exception to thisgeneral pattern: The sex addicts who did not use mastur-bation as their principal form of sexual acting out—a smallgroup of 9 men—fit our hypothetical profile in having sig-nificantly lower SIS2 than both the compulsive masturba-tors and the controls, as well as having relatively high SES.
We thus found little support for the idea that low inhibi-tion as measured by SIS2 is a prerequisite for excitationtransfer and the conditioning of sexual arousal in states ofnegative mood. There are at least two interpretations thatmight protect our hypothesis from refutation, apart fromthe inadequate power of this small sample. First, low inhi-bition may only be relevant in some cases, with othermechanisms playing a crucial role in the remainder.Second, the questions making up our SIS2 scale may notbe addressing the most appropriate situations.
Apart from our preliminary hypotheses, there wereother findings in this study worthy of comment.
Dissociation. Fourteen of the 31 sex addicts (45%)described a state of mind during their acting out whichcould be regarded as a form of dissociation from reality.We had not anticipated this pattern and, therefore, did notinclude any appropriate trait measure of dissociative ten-dency. We also found no obvious association between thisdissociative pattern and other aspects of the acting out(e.g., mood regulation, compulsive masturbation), nor anysignificant difference between the dissociators and theother participants on our various trait measures. It is possi-ble that a dissociative tendency has an enabling effect onthe establishment of out of control patterns of sexualbehavior, reducing the self-regulatory component thatwould be expected in most people. We should also consid-er the possibility that this self-description may be rein-forced through the culture of sex addicts groups (e.g.,SAA), providing a form of excuse, if not justification, fortheir inappropriate behavior. However, 6 of the 14 dissoci-ators had little or no experience of such groups. Futureresearch should more systematically investigate this ten-dency (e.g., using the Dissociative Experience Scale orDES; Carlson & Putnam, 2000).
Obsessive-compulsive disorder? The concept of com-pulsivity warrants consideration. A few studies have lookedfor evidence of obsessive-compulsive disorder (OCD)among sex addicts, usually finding a small minority in thiscategory (e.g.. Black et al., 1997, 15%; Shapira, Goldsmith,Keck, Khosia, & McElroy, 2000, 15%). The compulsivityapproach to conceptualizing out of control sexual behavioris usually criticized because it conflicts with the DSM-IV,which excludes such behaviors from the obsessive-compul-

Bancroft and Vukadinovic 231
sive category on the grounds that "the person usuallyderives pleasure from the activity and may wish to resist itonly because of its deleterious consequences" (AmericanPsychiatric Association, 2000, p. 422). Compulsivethoughts of the OCD type often do have sexual content, butthey are typically accompanied by negative mood and nosexual arousal. We would anticipate that most people withobsessive-compulsive personalities and a propensity formood disorders would experience a decline in sexual arous-ability during negative mood states, as is the case for mostpeople. Warwick and Salkovskis (1990) described two menwhose obsessive-compulsive symptoms included intrusivesexual thoughts accompanied by penile erection. Theawareness of the erection intensified the anxiety and,hence, reinforced the process. Is it possible that occasional-ly there is a combination of obsessive-compulsive tenden-cies and a low propensity for inhibition and/or high propen-sity for excitation of sexual response, with an atypical, sex-ualized type of compulsive behavioral pattern resulting? Ifso, one would expect to find evidence of other obsessive-compulsive phenomena in such individuals. In this study,we found two men with such personalities combined withwhat could be described as compulsive and sexually arous-ing behavior patterns. Both had high SES scores (69 and63J, but one SIS2 score was elevated (35) and the other nor-mal (28). This pattern is clearly not relevant to the majori-ty of individuals with out of control sexual behavior, butmay be relevant to a minority. Future research should aimto assess this pattern more systematically, both in terms ofthe specific acting out sequence and in other aspects ofobsessive-compulsive personality.
Toward a Theoretical Model
Our data, together with our understanding of the literature,suggest that in striving to understand out of control sexualbehavior, we should be expecting a range of etiologicalmechanisms associated with different behavioral patternsthat share the two key features of addictive behavior asdescribed by Goodman (1997): a recurrent failure to con-trol the sexual behavior and continuation of the behavior inspite of harmful consequences.
Goodman's (1997) integrated theoretical model hasthree principal components: (a) impaired affect regulation,(b) impaired behavioral inhibition, and (c) aberrant func-tion of the motivational reward system. This provides areasonable framework for our theoretical discussion.
The role of affect. We regard the role of affect to beimportant in most, if not all, cases of out of control sexualbehavior. For most people whose capacity for sexual inter-est and response goes down in states of depression and anx-iety, such mood-related mechanisms are not relevant, andindeed this may explain why their sexual behavior is lesslikely to get out of control. We should be cautious, howev-er, in interpreting the association between negative moodand sexual acting out as a form of mood regulation, or thedeliberate use of acting out to improve mood. In some cir-cumstances, when sexual connection with another person is
motivated by the need to make personal contact or the needfor self-validation or improvement of self-esteem, moodimprovement may be the driving force. However, an alter-native pattern possibly relevant to much of sexual actingout is that the negative mood, particularly if associated withincreased arousal (i.e., anxiety), leads to sexual arousal bymeans of excitation transfer. Once sexual arousal is estab-lished, there will be an intrinsic drive toward sexual releasethrough orgasm, which will have the incentive of transientpleasure and post-orgasm calming. Such a sequence maythen become reinforced and established by conditioning,with the individual learning to think sexual thoughts (orseek out sexual stimuli) when feeling such negative mood.This explanation is consistent with the fact that more oftenthan not the individual knows in advance, as a result ofexperience, that the transient reward will be outweighed bythe longer term negative consequences. We would thereforemove beyond a simple notion of the sexual behavior as amood regulator to define three affect-related patterns, eachof which requires a certain relationship between affect andsexuality. The possibility of such different patterns under-lines the likely variability of etiological determinants in outof control sexual behavior.
Pattern 1 involves the capacity to retain one's sexualinterest or responsiveness in states of depression, whichallows the pursuit of sexual contact with another person tomeet depression-related emotional needs. Such needs mayinclude establishing personal contact through sex, feelingvalidated by another person, or enhancing one's self-esteem by feeling desired by another person. Pattern 2involves the use of sexual stimulation to distract one'sattention from issues that when thought about induce neg-ative mood. This assumes that negative affect is being keptat bay by the distraction. As Baumeister and Heatherton(1996) put it, "the source of emotional distress is not pre-sent in the immediate situation, but is highly available inmemory (e.g., just after a major rejection or failure experi-ence). Under such circumstances, people will seek to dis-tract themselves to prevent themselves from thinking aboutthe upsetting event" (p. 5).
Pattern 3 involves the tendency for sexual interest andarousability to be increased in negative mood states thatare characterized by increased arousal, that is, states ofanxiety or stress. This pattern, we are postulating, is basedon an excitation transfer mechanism made possible by abelow-normal level of inhibition of sexual arousability inthe face of threat or other situations which elicit anxietyor stress. Our nonclinical data indicate that this pattern isfar from rare, but for most people so affected it is notassociated with out of control sexual behavior. Althoughwe found no clear support for this hypothesis in our smallsample of sex addicts, we would still postulate, on thebasis of our much larger nonclinical samples, that this pat-tern is most likely to be manifested in solitary or mastur-batory patterns of" behavior. In this pattern, we do not seethe sexual behavior as primarily determined by moodregulation, but as resulting from sexual arousal, which

232 Sexual Addiction, Compulsivity, Impulsivity
becomes a conditioned response to certain types of higharousal negative mood. Once the arousal has been trans-ferred into sexual arousal, there is a strong intrinsic needto pursue sexual release through orgasm, which, once thisis recognized as a recurring and out of control pattern,induces further negative mood.
An important qualification of these patterns is the possi-bility that in some individuals, depression can be associat-ed with anxiety, allowing for a blending of Patterns 1 and 3.
A key and as yet unanswered question is why someindividuals have the capacity for these atypical and poten-tially problematic interactions between mood and sexuali-ty. In our study of heterosexual men, we found a negativecorrelation between MSQ score and age, indicating thatsuch paradoxical patterns are more common in youngermen and presumably change for most individuals as theyget older. We did not find the association with age in ourgay men. This may be because our gay sample covered adifferent age range or because gay men typically have adifferent developmental history regarding the relationshipbetween mood and sexuality. Nevertheless, the potentialnegative association with age begs the question of whensuch an association becomes established. One obvioushypothesis, which remains to be adequately tested, is thatthe paradoxical mood-sexuality relationship is developedduring childhood or early adolescence as a consequence ofearly experiences which combine sexual response withnegative mood, such as child sexual abuse (CSA) orinduced guilt about masturbation. We found no support forthis in the current study; those with a history of child abusedid not differ in their MSQ scores from those without suchhistories. But because this sample was very small and weperformed only limited assessment of the childhood fac-tors, these results cannot be regarded as definitive. A bet-ter test of this hypothesis would be to identify relativelylarge samples with and without the trait of increased sexu-ality in negative mood states and compare them on variousaspects of their developmental history, including CSA.Coleman (1986) has postulated that the predisposition touse substances or behaviors to alleviate emotional painmay reflect an "intimacy dysfunction" which could resultfrom child sexual abuse or neglect. It would not be sur-prising if an early established pattern of increased sexualarousal and interest in association with negative moodcould become a barrier to the normal incorporation ofone's sexuality into close, intimate sexual relationships. Inour study of sexual risk taking in heterosexual men(Bancroft et al., 2004), we found that men in monogamousrelationships had lower MSQ scores.
Clearly, assessment of the relationship between moodand sexuality should be carried out in future studies of outof control sexual behavior. Our MSQ has the advantage ofbeing brief, with, by now, a substantial amount of norma-tive data from both men and women. However, this is avery simple trait measure which does not pick up the com-plexities of the relationship between depression and sexu-ality, nor the potential admixture of depression and anxi-
ety. We are in the process of developing a more sophisti-cated instrument for these purposes. But in addition, fur-ther research should not rely only on cross-sectional stud-ies such as that reported here but should also use prospec-tive methodology, such as daily diaries.
The role of inhibition. Goodman's (1997) second theo-retical concept is impaired behavioral inhibition. Inhibitionof sexual response is, according to our theoretical model(Bancroft, 1999; Bancroft & Janssen, 2000), an adaptivemechanism across species, and we have developed a psy-chometrically well validated measure of the propensity forsuch a mechanism (Janssen et al., 2002a). The concept oflow propensity for sexual inhibition has already proveduseful in explaining some aspects of high risk sexualbehavior (Bancroft, Janssen, Strong, Cames, et al., 2003b;Bancroft et al., 2004). It is also central to our theoreticalmodel of out of control sexual behavior, both as mediator inthe paradoxical relationship between negative mood andsexual arousability and as a factor enabling sexual respons-es in risky or problematic situations. However, we onlyfound partial support for our inhibition-based hypothesiswith our small sample of sex addicts, and mainly with thosewho did not use masturbation as their principal form of sex-ual acting out. As discussed above, we may be missingsome of the key aspects of inhibition with our SIS/SESquestionnaire, and should certainly be prepared to exploreother inhibition-related situations with different questions.
The neurobiology and psychopharmacology of sexualinhibition is complex, with an array of mediators and neu-romodulators involved (Bancroft, 1999). However, sero-tonin does appear to play a crucial role. Kafka (1997) hasproposed that a dysregulation of central monoamine func-tion underlies out of control sexual behavior. Goodman(1997) reminds us of the difficulties in locating complexeffects within the central nervous system or particular neu-rotransmitters, and the case has been made for formulating"conceptual systems" in the brain based on function ratherthan specific neurotransmitter mediation or anatomic loca-tion (Bancroft, 1999). There is a clear need for well-designed, controlled studies of selective serotonin reuptakeinhibitor (SSRI) treatment for men and women with out ofcontrol sexual behavior, in which groups are carefullyselected and matched for indicators of impaired inhibitionas well as other behavioral characteristics.
While direct investigation of serotonergic mechanismsin the central nervous system is difficult in humans, devel-opment in the genetics of neurotransmitters offers a newand potentially informative approach for explaining indi-vidual differences. Do individuals who develop out of con-trol patterns of sexual behavior have lower levels of sero-tonin transporter gene markers (Lesch et al., 1996)?Another new approach to the study of central inhibitorymechanisms is the use of brain imaging (e.g., Redoute etal., 2000; Stoleru et al., 1999), by which certain areas ofthe brain are shown to be deactivated during response tosexual stimuli with arousal. Brain imaging, particularly forthe study of complex processes such as sexual arousal, is

Bancroft and Vukadinovic 233
at an early stage of development, but there is considerablepotential here for future research.
The motivational reward system. Goodman's (1997) thirdtheoretical concept is aberrant function of the motivationalreward system. So far, we have little to say about howreward and incentive mechanisms may help to explain out ofcontrol sexual behavior. However, we are open to the possi-bility that some changes in sensitivity of the incentivereward system may occur as part of the establishment of anout of control pattern, changes comparable to those associ-ated with chronic use of addictive drugs (Robinson &Benidge, 1993) and that may be relevant to "behavioraladdictions" of various kinds (Holden, 2001). Once again,such mechanisms are difficult to study in humans, but brainimaging offers possibilities for the future (e.g., Breiter,Aharon, Kahneman, Dale, & Shizgal, 2001). However, untilwe have further understanding of such mechanisms, weshould regard the concept of sexual addiction as no morethan an analogy that may have beneficial effects, at least forsome individuals, in therapeutic programs.
Self-regulatory failure. In addition to Goodman's threecomponents, general issues of behavioral regulation deserveattention. To what extent is out of control or unregulatedsexual behavior similar to other out of control behaviors likebinge eating or overspending? Baumeister and Heatherton(1996) provided a useful theoretical approach to failure ofself-regulation, which they described as a multifacetedprocess that can break down in several different ways. Theypaid little attention to sexual behavior in this article, buttheir theoretical analysis is relevant in several respects. Theydescribed three ingredients of self-regulation: (a) standards,(b) monitoring, and (c) the operative phase of regulation.Standards are of interest for our study, in particular thedilemma of conflicting or incompatible standards, whichcan undermine regulation. For five of our male sex addicts,religion was very important. It is not difficult to see how, insuch cases, the unquestionable moral unacceptability ofmost types of sexual behavior would conflict with one's sex-ual impulses to undermine any sensible pattern of regulatedsexual behavior. Thus, an individual who believes mastur-bation is evil and who has strong impulses to masturbateusing the Internet will be unable to see that a regulated pat-tern of masturbation can be a responsible way of dealingwith one's sexual needs. Coleman (1986) proposed thathighly restrictive attitudes about sexuality result in inabilityto conform, starting off the cycle of guilt, pain, and compul-sivity. We would suggest that such mechanisms might beimportant in some cases.
Monitoring is clearly important to effective self-regula-tion, and Baumeister and Heatherton (1996) suggested thatalcohol as well as fatigue and stress can impair normalmonitoring. Sexual arousal may also have this effect, andwe have examined this closely in heterosexual and gaymen in relation to sexual risk management (Strong,Bancroft, Cames, Davis, & Kennedy, 2003). On the otherhand, our theoretical model discussed above proposes thatinhibition of sexual arousal may be an adaptive mechanism
that could facilitate self-regulation. If correct, this couldset sexual behavior apart from other types of behaviorrequiring self-regulation. Nevertheless, the individual withlow propensity for inhibition of sexual arousal will befaced with the same self-regulatory challenge posed byother behaviors, such as eating.
An important aspect of monitoring, discussed byBaumeister and Heatherton (1996), is transcendence orfocusing one's awareness beyond the immediate situationso that more distal concerns or consequences are kept inmind. The dissociative tendency, discussed earlier, couldbe directly relevant to out of control behavior by under-mining, if not eliminating, this transcendence.
These more general aspects of self-regulation, aboutwhich a substantial literature exists (Baumeister,Heatherton, & Tice; 1994), deserve systematic attention infuture research into out of control sexual behavior.
Conclusions
While acknowledging the importance to both the individ-ual and society of patterns of sexual behavior that are outof control and have problematic consequences, we think itlikely that such patterns are varied in both their etiologicaldeterminants and how they are best treated. For that rea-son, we consider it to be premature to attempt some over-riding definition relevant to clinical management until wehave a better understanding of the various patterns andtheir likely determinants. The concepts of compulsivityand addiction may prove to have explanatory value insome cases, but are not helpful when used as general termsfor this class of behavior problem. Until we have a betterunderstanding of the subtypes, we prefer the generaldescriptive term out of control to describe sexual behaviorthat is unregulated for a variety of possible reasons. In themeantime, we have postulated some testable, clinically rel-evant hypotheses and have developed or identified a num-ber of measures suitable for their testing.
REFERENCES
American Psychiatric Association. (2000). Diagnostic and statistical manu-al of mental disorders (4th ed., text rev.). Washington, DC. Author
Angst, J. (1998). Sexual problems in healthy and depressed persons.International Clinical Psychopharmacology, /i(Suppl. 6), S1-S4.
Araujo, A. B., Mohr, B. A., & McKinlay, J. B. (2003). Changes in sexualfunction in older men: Longitudinal data from the Massachusetts MaleAging Study. Manuscript in preparation.
Bancroft, J. (1999). Central inhibition of sexual response in the male: A the-oretical perspective. Neuroscience and Biobehavioral Reviews, 23,763-784.
Bancroft, J., & Janssen, E. (2000). The dual control model of male sexualresponse: A theoretical approach to centrally mediated erectile dysfunc-tion. Neuroscience and Biobehavioral Reviews, 24, 571—579.
Bancroft, J., Janssen, E., Cames, L., Strong, D. A., Goodrich, D., & Long,J. S. (2004). Sexual activity and risk-taking in young heterosexual men:The relevance of sexual arousability, mood, and sensation seeking. TheJournal of Sex Research, 41, 181-192.
Bancroft, J., Janssen, E., Strong, D., Carnes, L., Vukadinovic, Z., & Long,J. S. (2003a). The relation between mood and sexuality in heterosexualmen. Archives of Sexual Behavior, 32, 217-230.
Bancroft, J., Janssen, E., Strong, D., Cames, L., Vukadinovic, Z., & Long,J. S. (2003b). Sexual risk-taking in gay men: The relevance of sexual
234 Sexual Addiction, Compulsivity, Impulsivity
arousability, mood and sensation seeking. Archives of Sexual Behavior,32, 555-572.
Bancroft, J., Janssen, E., Strong, D., & Vukadinovic, Z. (2003). The relationbetween mood and sexuality in gay men. Archives of Sexual Behavior,32, 231-242.
Barth, R. J., & Kinder, B. N. (1987). The mislabeling of sexual impulsivity.Journal of Sex and Marital Therapy, 13, 15—23.
Baumeister, R. R, & Heatherton, T. F. (1996). Self-regulation failure: Anoverview. Psychological Inquiry, 7(1), 1-15.
Baumeister, R. F , Heatherton, T. F , & Tice, D. M. (1994). Losing control:How and why people fail at self-regulation. San Diego, CA: AcademicPress.
Beck, A. T. (1967). Depression: Clinical, experimental and theoreticalaspects. London: Staples Press.
Black, D. W., Kehrberg, L. L. D., Flumerfelt, D. L., & Schlosser, S. S.(1997). Characteristics of 36 subjects reporting compulsive sexualbehavior. American Journal of Psychiatry, 154(2), 243-249.
Breiter, H. C , Aharon, I., Kahneman, D., Dale, A., & Shizgal, P. (2001).Functional imaging of neural responses to expectancy and experience ofmonetary gains and losses. Neuron, 20, 619-639.
Carlson, E. B., & Putnam, F W. (2000). Dissociative Experiences Scale(DES). In J. Rush (Ed.), Handbook of psychiatric measures (pp.621-624). Washington, DC: American Psychiatric Association.
Cassidy, W. L., Flanagan, N. B., Spellman, M., & Cohen, M. E. (1957).Clinical observations in manic depressive disease. Journal of theAmerican Medical Association, 164, 1535-1546.
Coleman, E. (1986, July). Sexual compulsion vs. sexual addiction: Thedebate continues. SIECUS Report, 14, 7-11.
Fedoroff, J. P. (1993). Serotonergic drug treatment of deviant sexual inter-ests. Annals of Sex Research, 6, 105-121.
Gold, S. N., & Heffner, C. L. (1998). Sexual addiction: Many conceptions,minimal data. Clinical Psychology Review, 18, 367-381.
Goodman, A. (1997). Sexual addiction. In J. H. Lowinson, P. Ruiz, R. B.Millman, & J. G. Langrod (Eds.), Substance abuse: A comprehensivetextbook (pp. 340-354). Philadelphia: Williams & Wilkins.
Holden, C. (2001). "Behavioral addictions": Do they exist? Science, 294,980-982.
Janssen, E., Vbrst, H., Finn, P , & Bancroft, J. (2002a). The SexualInhibition (SIS) and Sexual Excitation (SES) Scales: I. Measuring sex-ual inhibition and excitation proneness in men. The Journal of SexResearch, 39, 114-126.
Janssen, E., Vorst, H., Finn, P., & Bancroft, J. (2002b). The Sexual Inhibition(SIS) and Sexual Excitation (SES) Scales: II. Predicting psychophysio-logical response patterns. The Journal of Sex Research, 39, 127-132.
Kafka, M. P. {\997). A monoamine hypothesis for the pathophysiology ofparaphilic disorders. Archives of Sexual Behavior, 26, 343-357.
Kafka, M. P. (2000). Psychopharmacologic treatments for nonparaphiliccompulsive sexual behaviors. CNS Spectrums, 5, 49-59.
Kennedy, S. H., Dickens, S. E., Eisfeld, B. S., & Bagby, R. M. (1999).Sexual dysfunction before antidepressant therapy in major depression.Journal of Affective Disorders, 56, 201-208.
Leiblum, S. R., & Nathan, S. G. (2001). Persistent sexual arousal syndrome:
A newly discovered pattern of female sexuality. Journal of Sex &Marital Therapy, 27, 365-380.
Lesch, K. P , Bengel, D., Heils, A., Sabol, S. Z., Greenberg, B. D., Petri, S.,et al. (1996). Association of anxiety-related traits with a polymorphismin the serotonin transporter gene regulatory region. Science, 274,1527-1531.
Mathew, R. J., & Weinman, M. L. (1982). Sexual dysfunction in depression.Archives of Sexual Behavior, 11, 323-328.
Nofzinger, E. A., Thase, M. E., Reynolds, C. F , III, Frank, E., Jennings, J.R., Garamoni, G. L., et al. (1993). Sexual function in depressed men:Assessment by self-report, behavioral, and nocturnal penile tumescencemeasures before and after treatment with cognitive behavior therapy.Archives of General Psychiatry, 50, 24—30.
Orford, J. (1978). Hypersexuality: Implications for a theory of dependence.British Journal of Addiction, 73, 299-310.
Quadland, M. C. (1985). Compulsive sexual behavior: Definition of a prob-lem and an approach to treatment. Journal of Sex and Marital Therapy,11, 121-132.
Raviv, M. (1993). Personality characteristics of sexual addicts and patho-logical gamblers. Journal of Gambling Studies, 9, 17-30.
Redout^, J., Stoldru, S., Grdgoire, M. C , Costes, N., Cinotti, L., Lavenne,F , et al. (2000). Brain processing of visual sexual stimuli in humanmales. Human Brain Mapping, 11, 162-177.
Rinehart, N. J., & McCabe, M. P. (1997). Hypersexuality: Psychopathologyor normal variant of sexuality? Sexual and Marital Therapy, 12, 45-60.
Robinson, T. E., & Berridge, K. C. (1993). The neural basis of drug crav-ing: An incentive-sensitization theory of addiction. Brain ResearchReviews, /S, 247-291.
Shapira, N. A., Goldsmith, T D., Keck, P E., Khosia, U. M., & McElroy, S.L. (2000). Psychiatric features of individuals with problematic Internetuse. Journal of Affective Disorders, 57, 267-272.
Stein, D. J., Hollander, E., Anthony, D. T., Schneier, F. R., Fallon, B. A.,Liebowitz, M. R., et al. (1992). Serotonergic medications for sexualobsessions, sexual addictions, and paraphilias. Journal of ClinicalPsychiatry, 53,267-211.
StoMru, S., Grdgoire, M. C , Gerard, D., Decety, J., Lafarge, E., Cinotti, L.,et al. (1999). Neuroanatomical correlates of visually evoked sexualarousal in human males. Archives of Sexual Behavior, 28, 1-21.
Strong, D. A., Bancroft, J., Cames, L. A., Davis, L. A., & Kennedy, J.(2003). The impact of sexual arousal on sexual risk taking: A qualitativestudy. Manuscript submitted for publication.
Warwick, H. M. C , & Salkovskis, P M. (1990). Unwanted erections inobsessive-compulsive disorder. British Journal of Psychiatry, 157,919-921.
Zemore, R., Fischer, D. G., Garratt, L. S., & Miller, C. (1990). The depres-sion proneness rating scale: Reliability, validity, and factor structure.Current Psychology: Research & Reviews, 9, 255-263.
Zillman, D. (1983). Transfer of excitation in emotional behavior. In J. T.Cacioppo & R. E. Petty (Eds.), Social psychophysiology: A sourcebook(pp. 215-240). New York: Guilford Press.
Manuscript accepted November 4, 2003
