severe asthma management
TRANSCRIPT

S E V E R E A S T H M A
M A N A G E M E N T A N D V E N T I L AT I O N S T R AT E G I E S
ASTHMA
Characteristics
– Episodic reversible bronchoconstriction
– Airway inflammation
– Increased mucus production
Consequences
– Increased WOB
• Increased airway resistance/Reduced Compliance
– Type 2 Resp failure – Hypercapnia & Hypoxia
• Impaired gas exchange
• V/Q mismatches

CASE MB
• 28/M
• Hx Asthma – Dx 2011 1 Prior hospital admission 1 yr ago – overnight
• Flixotide preventer, takes PRN Ventolin prior to exercise
• Office job, smoker
• BIBA:
• Unwell 1 week – cough/sputum /SOB/wheezy Has been self treating with Ventolin
• Spoke in words, accessory muscle use, diaphoretic, not confused
• RR 30, Sats 88RA, widespread wheeze
ASTHMA SEVERITY
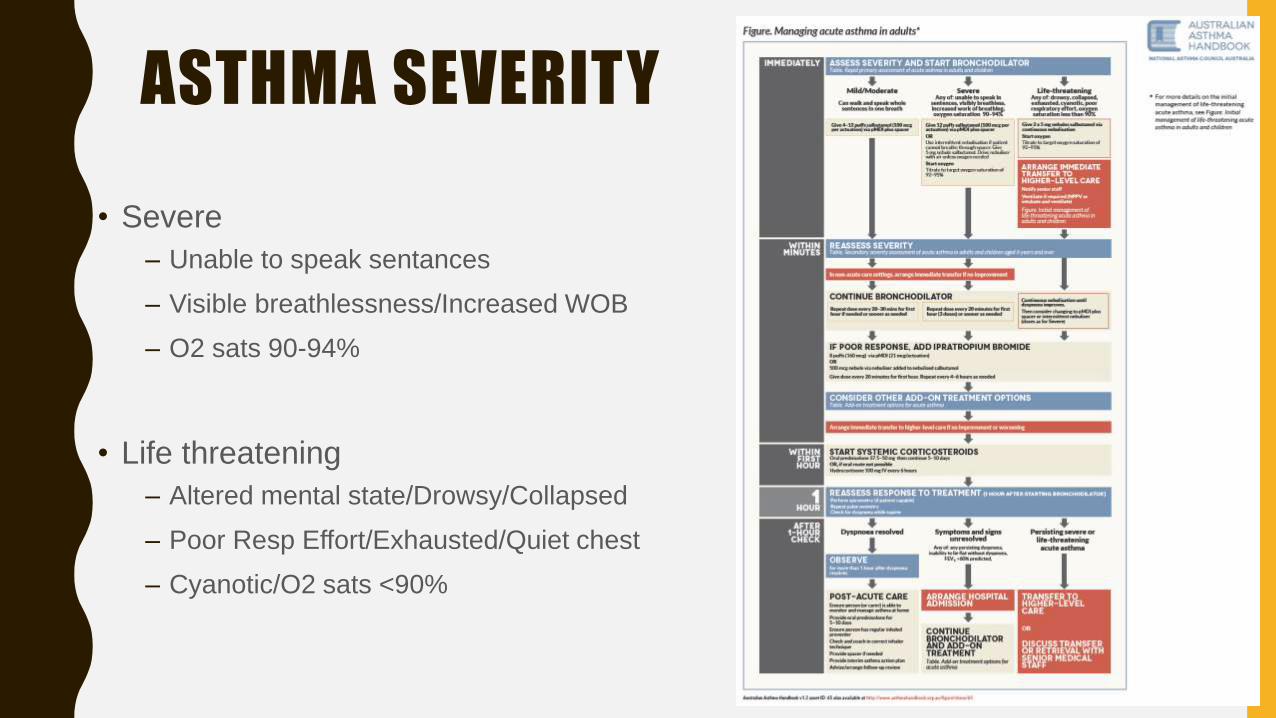
• Severe
– Unable to speak sentances
– Visible breathlessness/Increased WOB
– O2 sats 90-94%
• Life threatening
– Altered mental state/Drowsy/Collapsed
– Poor Resp Effort/Exhausted/Quiet chest
– Cyanotic/O2 sats <90%

RISK FACTORS
• Previous poor control of asthma
– Frequent ED/hospital presentations
– Previous severe exacerbations / ICU & Intubation etc.
• Treatment received prior to presentation
– Frequency of Ventolin use
– Poor compliance with asthma medications /action plans
• Other factors:
– Smoking/Illicit drug use, psychosocial problems
– Comorbidities - cardiovascular or chronic lung disease
INITIAL TREATMENT
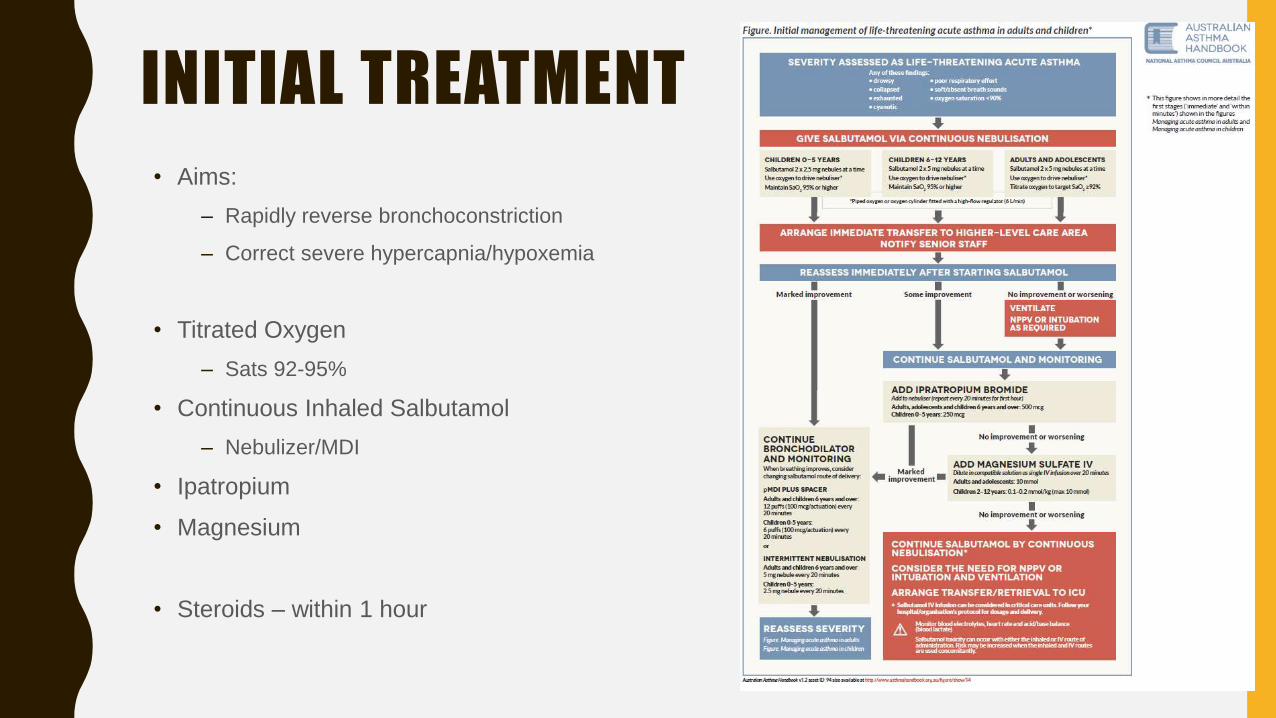
• Aims:
– Rapidly reverse bronchoconstriction
– Correct severe hypercapnia/hypoxemia
• Titrated Oxygen
– Sats 92-95%
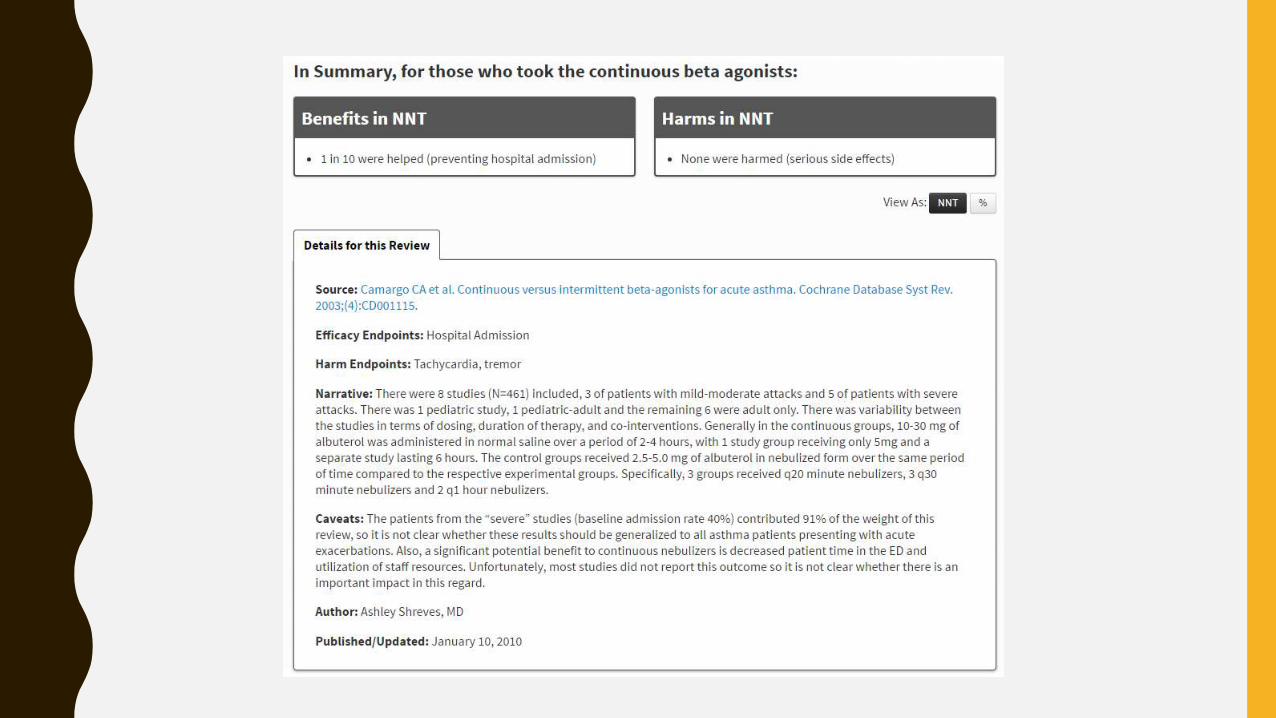
• Continuous Inhaled Salbutamol
– Nebulizer/MDI
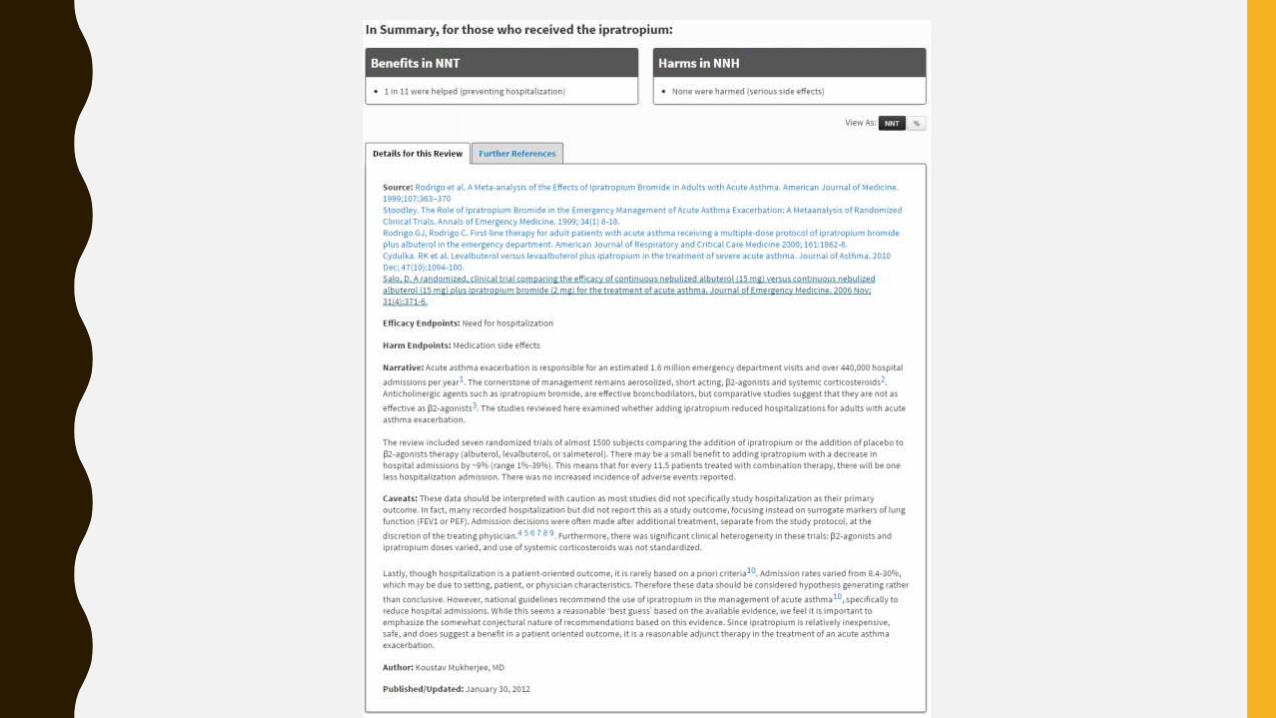
• Ipatropium
• Magnesium
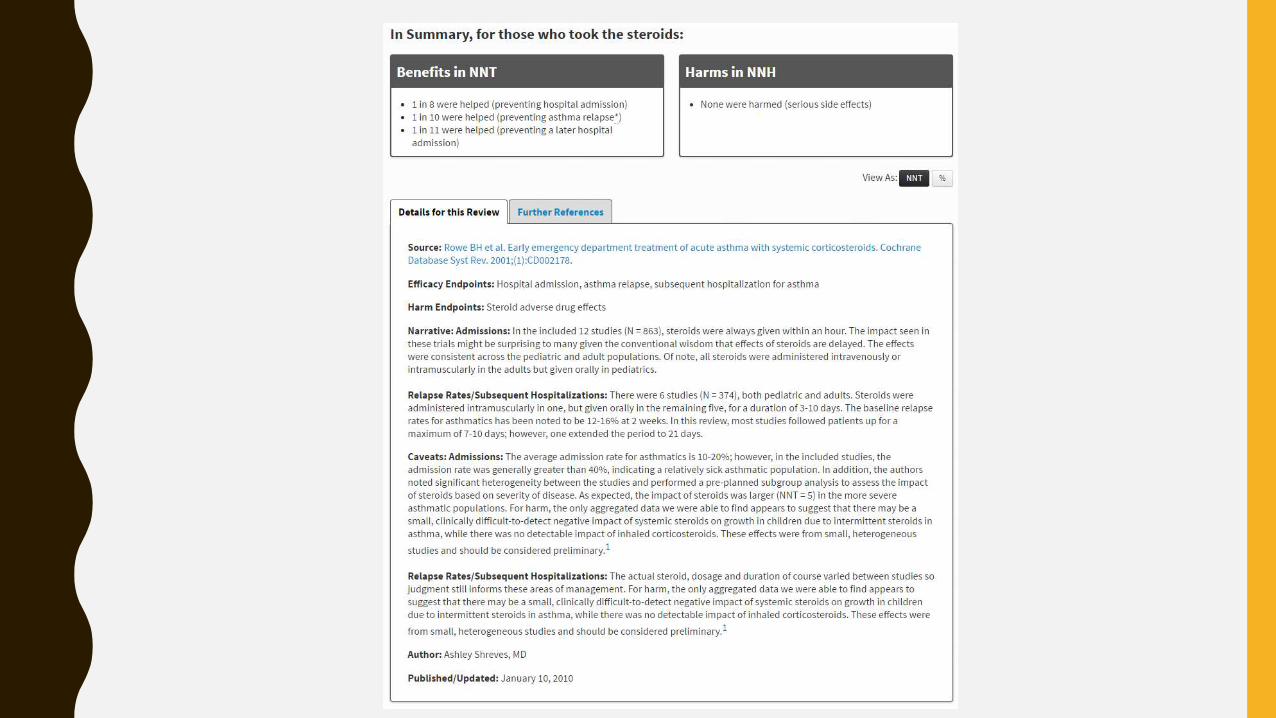
• Steroids – within 1 hour
CASE MB
• Treated with 3 Ventolin nebs/ipratropium/hydrocort/magnesium
• Initial gases pH 7.15, Normal CO2, bicarb 20, Lac 2.4
• CXR clear
• Initial concerns may require ICU admission
• However clinically improved with treatment
• Reviewed by ICU – planned for HDU


CASE MB
Through the night:
– Drowsy/Tiring
– Increased WOB
– Gases relatively unchanged.
• Contacted HDU&ICU – Busy with another code
• Given cont Ventolin nebs with limited effect
• Started on NIV
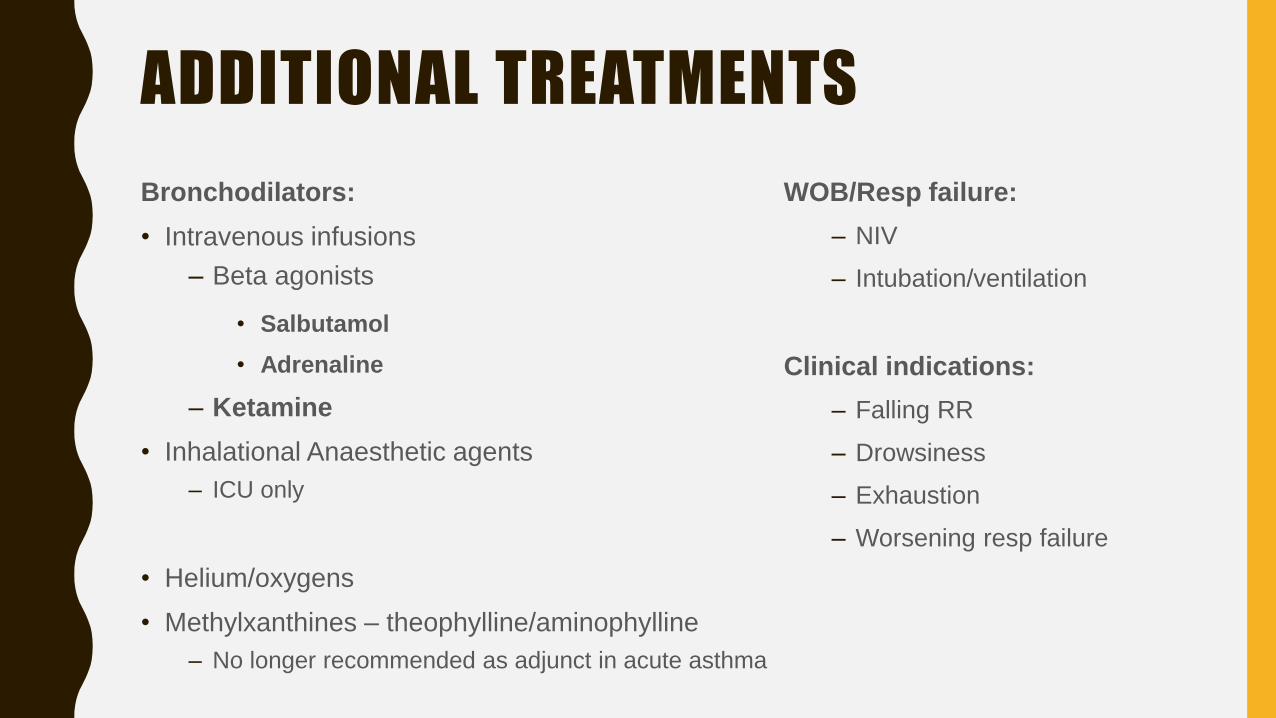
ADDITIONAL TREATMENTS
Bronchodilators:
• Intravenous infusions
– Beta agonists
• Salbutamol
• Adrenaline
– Ketamine
• Inhalational Anaesthetic agents
– ICU only
• Helium/oxygens
• Methylxanthines – theophylline/aminophylline
– No longer recommended as adjunct in acute asthma
WOB/Resp failure:
– NIV
– Intubation/ventilation
Clinical indications:
– Falling RR
– Drowsiness
– Exhaustion
– Worsening resp failure

MECH VENTILATION• Mech ventilation in asthma is difficult
– Relatively normal alveolar compliance
– High airway resistance high airway pressures
– Prolonged expiration Risk gas trapping
– Gas trapping increases intrinsic PEEP
– Very high peak airway pressures
– Plateau/insp pause pressures
Flow X Resistance
Vol/Complianc
e
+ PEEP
Alveoli
Bronchioles
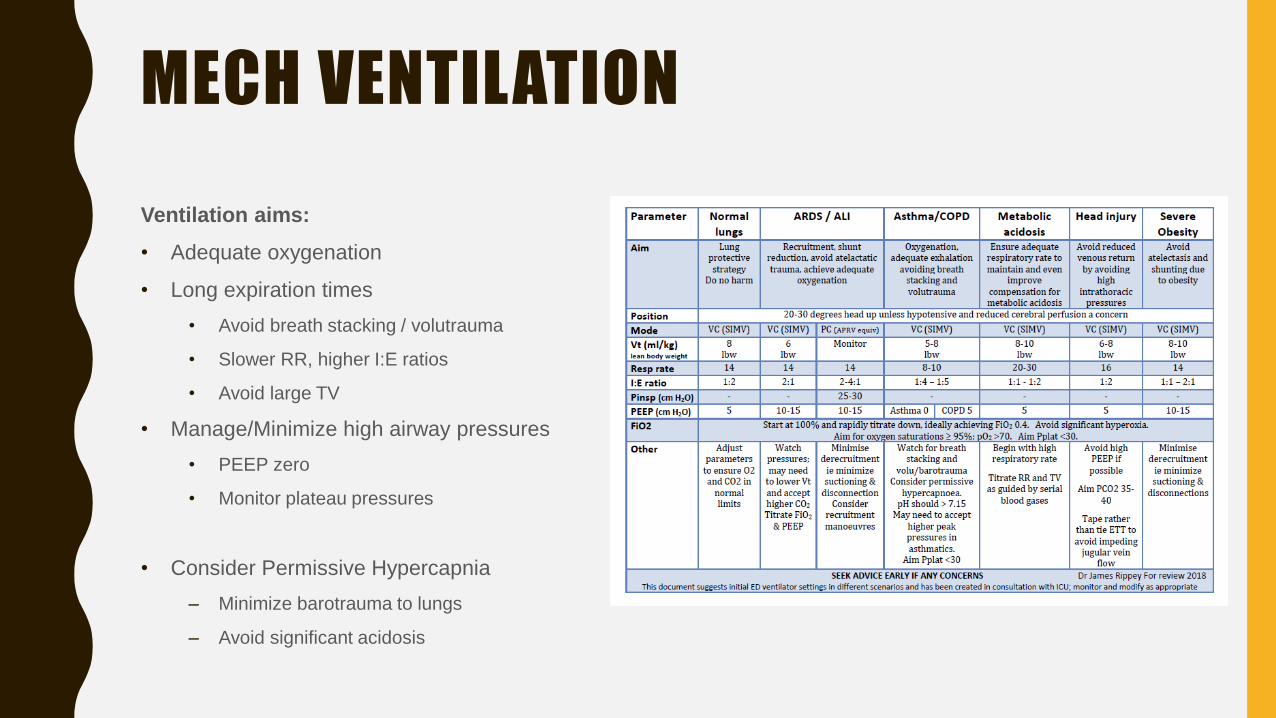
MECH VENTILATION
Ventilation aims:
• Adequate oxygenation
• Long expiration times
• Avoid breath stacking / volutrauma
• Slower RR, higher I:E ratios
• Avoid large TV
• Manage/Minimize high airway pressures
• PEEP zero
• Monitor plateau pressures
• Consider Permissive Hypercapnia
– Minimize barotrauma to lungs
– Avoid significant acidosis
NIVADV:
• Reduce Fatigue/work of breathing
• Improve oxygenation/ventilation
– V/Q mismatch
– Gas exchange
– Recruitment
– Prevention athelectasis
DIS:
• Increased risk of barotrauma
• May lead to delayed
intubation/associated complications
• General NIV issues
Uses:
• To avoid intubation
• For preoxygenation/ventilatory support
prior to Intubation
– Ketamine DSI
INDUCTION
• Ketamine
– Drug of choice – bronchodilator
• Consider DSI
– Optimizing patient with Ketamine/NIV prior to intubation
• Prone to hypotension post intubation – caution with propofol etc.
– Breath stacking
– Hypovolemia
– Induction drugs
– Tension PTX
CASE MB
• Reviewed by ICU – Trial of Ketamine and Adrenaline infusions in ED as temporising
measure
• Taken up to ICU – Intubated - Ketamine/NIV prior
• Spent 2 nights intubated and further 5 days on the ward
• Discharged home with Preventer (increased dose)
• Seen further 5 weeks later on a night shift for another exacerbation of asthma…
RESOURCES/REFERENCES
• LITFL
– Acute Severe Asthma http://lifeinthefastlane.com/ccc/acute-severe-asthma/
– NIV & Asthma http://lifeinthefastlane.com/ccc/non-invasive-ventilation-niv-and-asthma/
• Australian Asthma Handbook https://www.asthmahandbook.org.au/
• EMRAP – C3 Asthma Summary Aug 2016 – S Swadron, M Herbert
• TheNNT: Quick Summaries of Evidence Based Medicine http://www.thennt.com/
• Ventilator settings in asthma – James Rippey http://scghed.com/2015/11/updated-
suggested-initial-ventilator-settings-112015/