session title: postgraduate course: foregut – beyond gerd
TRANSCRIPT

Session Title: POSTGRADUATE COURSE: Foregut – Beyond GERD & Hiatal Hernia
Date/Time: 4/17/2013; 7:30am-12pm
Session Chair: C. Daniel Smith, MD
Session Co-Chair: Bernard Dallemagne, MD
SESSION DESCRIPTION
This session will cover complex topics in foregut surgery increasingly encountered by surgeons caring for
patient with foregut conditions. World experts will discuss presentation, diagnosis and management
strategies for these conditions that go well beyond basic GERD and hiatal hernia. This session’s objectives are
a classical application of educational principles to adult learning. The problem is the increasing complexity in
managing foregut disease as new therapies become available and the diseases themselves are increasingly
advanced presentations. Participants will learn the varied presentations of these more complex conditions
and management strategies that go beyond managing basic foregut conditions. On returning to their practice,
they will be equipped to change how they operate by applying this knowledge in caring for foregut patients.
This improved understanding will allow for better patient selection and use of advanced interventions.
SESSION OBJECTIVES:
At the conclusion of this session, participants will be able to:
1. Understand and describe complex conditions and circumstances effecting surgical foregut diseases
2. Recognize some of the innovations and new technologies used in managing foregut disease
3. Be aware of the impact that advanced presentations of foregut disease can have on selecting management
strategies for these patients
4. Approach complex foregut conditions with greater confidence
SESSION OUTLINE
Time Presentation Title Faculty Name
7:30am
Introduction C. Daniel Smith, MD
Bernard Dallemagne, MD
GERD & Hiatal Hernia
7:35am
Management strategies for complex GERD
(stricture and Barretts)
Jeffrey Peters, MD
7:55am
Redo Operations – When, How and Who? Bernard Dallemagne, MD
8:15am Hiatal Hernia C. Daniel Smith, MD
8:35am What to Do in the Obese Samer Mattar, MD
8:55am Emerging Technologies and Techniques Reginald Bell, MD
9:15am Panel Discussion – Audience Questions and Cases
10:00am Break
Gastric Neoplasms
10:15am GIST and Submucosal Tumors David Rattner, MD
10:30am Early Gastric Cancer Han-Kwang Yang, MD
Other Esophageal Conditions
10:45am Submucosal Tumors Sricharan Chalikonda, MD
11:00am Esophageal Diverticulae and Achalasia Christy Dunst, MD
11:15am
MIS in Esophageal Neoplasms Giovanni Dapri, MD/ Guy B.
Cadière, MD
11:35am Panel Discussion – Audience Questions and Cases

1
MANAGEMENT OF COMPLEX GERD; STRICUTRES AND BARRETT’S
Jeffrey H. Peters, MD
University of Rochester, Rochester NY
The complications of gastroesophageal reflux result from the damage inflicted by gastric
juice on the esophageal mucosa, laryngeal or respiratory epithelium. These can be conceptually
divided into 1) mucosal complications such as esophagitis and stricture, 2) extra-esophageal or
respiratory complications such as chronic cough, asthma and pulmonary fibrosis and 3)
metaplastic (Barrett’s esophagus) and neoplastic (adenocarcinoma). The prevalence and severity
of complications is related to the degree of loss of the gastroesophageal barrier, defects in
esophageal clearance and the content of refluxed gastric juice.
Stricture and Esophageal Shortening
Esophageal strictures are among the most challenging complications of esophageal
disease. An esophageal stricture can be associated with severe esophagitis or Barrett's esophagus.
In the latter situation, it occurs at the site of maximal inflammatory injury (i.e., the columnar-
squamous epithelial interface). As the columnar epithelium advances into the area of
inflammation, the inflammation extends higher into the proximal esophagus, and the site of the
stricture moves progressively up the esophagus. Patients who have a stricture in the absence of
Barrett's esophagus should have the presence of gastroesophageal reflux documented before the
presence of the stricture is ascribed to reflux esophagitis. In patients with normal acid exposure,
the stricture may be due to cancer or a drug-induced chemical injury, the latter resulting from the
lodgment of a capsule or tablet in the distal esophagus. In such patients, dilation usually corrects
the problem of dysphagia. It is also possible for drug-induced injuries to occur in patients who
have underlying esophagitis and a distal esophageal stricture secondary to gastroesophageal
reflux. In this situation, a long string-like stricture progressively develops as a result of repetitive
caustic injury from capsule or tablet lodgment on top of an initial reflux stricture. These
strictures are often resistant to dilation.
Esophageal shortening is a consequence of scarring and fibrosis associated with repetitive
esophageal injury. The presence of a stricture is among the most reliable indicators of the
possibility of a short esophagus. Anatomic shortening of the esophagus can compromise the
ability to perform an adequate tension-free fundoplication and may result in an increased
incidence of breakdown or thoracic displacement of the repair. Esophageal length is best
assessed preoperatively using video roentgenographic contrast studies and endoscopic findings.
Endoscopically, hernia size is measured as the difference between the diaphragmatic crura,
identified by having the patient sniff, and the GE junction, identified as the loss of gastric rugal
folds. We consider the possibility of a short esophagus in patients with strictures or those with
large hiatal hernias (greater than 5 cm), particularly when the latter fail to reduce in the upright
position on a video barium esophagram.
The definitive determination of esophageal shortening is made intraoperatively when,
after thorough mobilization of the esophagus, the GE junction cannot be reduced below the
diaphragmatic hiatus without undue tension on the esophageal body. Surgeons performing
fundoplication have reported varying incidences of esophageal shortening, attesting to the

2
judgment inherent in defining and recognizing “undue tension.” An advantage of transthoracic
fundoplication is the ability to mobilize the esophagus extensively from the diaphragmatic hiatus
to the aortic arch. With the GE junction marked with a suture, esophageal shortening is defined
by an inability to position the repair beneath the diaphragm without tension. In this situation, a
Collis gastroplasty coupled with either a partial or complete fundoplication may be performed.
Barrett’s Esophagus
The relief of symptoms remains the primary force driving antireflux surgery in patients
with Barrett’s esophagus. Healing of esophageal mucosal injury and the prevention of disease
progression are important secondary goals. In this regard, patients with Barrett’s esophagus are
no different than the broader population of patients with gastroesophageal reflux. Antireflux
surgery should be considered when patient factors suggest severe disease or predict the need for
long term medical management, both of which are almost always true in patients with Barrett’s
esophagus.
An important consideration is that patients with Barrett’s esophagus generally have
severe GERD, with its attendant sequelae such as large hiatal hernia, stricture, shortened
esophagus and poor motility. Compared to mild and nonerosive reflux disease, severe erosive
disease and Barrett’s esophagus are associated with significantly greater loss of the mechanical
antireflux barrier because of associated hiatal hernias and a hypotensive lower esophageal
sphincter. Surgical treatment with a laparoscopic Nissen fundoplication reduces the hiatal hernia,
improves the antireflux barrier and consequently provides similarly excellent symptom control.
Large studies in patients with typical acid reflux symptoms have been published from the U.S.
and Europe. In patients having laparoscopic Nissen at Emory University, relief of heartburn and
regurgitation occurred in 90%, and 70% were off all reflux medications at a mean follow-up of
11 years. These results emphasize the durability of the procedure as well as the persistent relief
of typical symptoms. Risk factors for persistent use of antacids post antireflux surgery include a
partial fundoplication, older age and female gender.
Studies focusing on the symptomatic outcome following antireflux surgery in patients
with Barrett’s esophagus document excellent to good results in 72-95% of patients at 5 years
following surgery. The outcome of laparoscopic Nissen fundoplication in patients with Barrett’s
esophagus has been assessed at 1-3 years after surgery. Hofstetter et al. reported the experience
at the University of Southern California (USC) in 85 patients with Barrett’s esophagus at a
median of 5 years after surgery. Fifty-nine had long and 26 short segment Barrett’s and fifty
underwent a laparoscopic antireflux procedure. Reflux symptoms were absent postoperatively in
79% of the patients. Postoperative 24-hour pH was normal in 17/21 (81%). Ninety-nine percent
of the patients considered themselves cured or improved and 97% were satisfied with the
surgery. In addition to symptomatic improvement in reflux after surgery, there is evidence that
mediators of esophageal inflammation implicated in carcinogenesis are decreased as well. Cox-2
gene expression is elevated in the distal esophagus of reflux patients, but the expression of Cox-2
and another inflammatory mediator Interleukin 8 can be decreased in the distal esophageal
mucosa after a fundoplication.
Dysplasia in Barrett’s Esophagus: The prevalence of dysplasia at diagnosis in patients
presenting with Barrett’s esophagus ranges from 15-25%, and approximately 5% of patients will

3
develop dysplasia each year. The identification of dysplasia in Barrett’s epithelium rests upon
histologic examination of biopsy specimens. The cytologic and tissue architectural changes are
similar to those described in ulcerative colitis. By convention, Barrett’s metaplasia is currently
classified into four broad categories:
1. No dysplasia
2. Indefinite for dysplasia
3. Low grade dysplasia
4. High grade dysplasia
There are few prospective studies documenting the progression of non-dysplastic
Barrett’s epithelium to low or high grade dysplasia. Those that are available suggest that 5-6%/yr
will progress to dysplasia and 0.5-1%/yr to adenocarcinoma. Once identified, Barrett’s
esophagus complicated by dysplasia should undergo aggressive therapy. Patients whose biopsies
are interpreted as indefinite for dysplasia should be treated with a medical regimen consisting of
60-80 mg of PPI therapy for 3 months and re-biopsied. Importantly, esophagitis should be
healed prior to interpretation of the presence or absence of dysplasia. The presence of severe
inflammation makes the microscopic interpretation of dysplasia difficult. The purpose of acid
suppression therapy is to resolve inflammation that may complicate the interpretation of the
biopsy specimen. If the diagnosis remains indefinite, the patient should be treated as if low grade
dysplasia were present with continued medical therapy or antireflux surgery and repeat biopsy
every 6 months.
High grade dysplasia (HGD) should be confirmed by two pathologists knowledgeable in
GI pathology. Once HGD is confirmed, observation is less than optimal as > 50% of patients will
progress to multifocal HGD or cancer. Until recently esophagectomy was considered the
standard of care for patients with high grade dysplasia. With the Western acceptance of an
Eastern modality, endoscopic mucosal resection (EMR) coupled with radiofrequency ablastin, is
now the most common treatment for patients with high grade dysplasia and intramucosal
cancers. The aim of EMR is to excise the area of interest including the mucosal and submucosal
layers down to the lamina muscularis propria allowing optimal histologic interpretation. Reports
from specialized centers combining EMR with mucosal ablation using either photodynamic or
radiofrequency energy, are encouraging with a high prevalence of eradication of
dysplasia/neoplasia. Ell and others initially showed that EMR is feasible and safe; however, in
one of their earlier reports, recurrent or metachronous carcinomas were found in 14% of 64
patients during one year follow-up.
Longer success rates with EMR for early Barrett’s cancer have been reported from the
experienced centers. The largest study comes from Wiesbaden, Germany, involving over 300
patients with high grade dysplasia or intramucosal cancers and a mean follow-up of over 5 years.
A complete response was achieved in 97% of patients, and surgery was necessary in 3.7% after
endoscopic therapy failed. Metachronous lesions developed during the follow-up in 21% of the
patients. The risk factors most frequently associated with recurrence were piecemeal resection,
long-segment Barrett's esophagus and multifocal lesions.

NOTES

1
Redo Operations – When, How and Who?
Bernard Dallemagne, M.D
Department of Digestive & Endocrine Surgery NHC - Les Hôpitaux Universitaires de Strasbourg Scientific Co-Director Digestive Cancer Research Institute (IRCAD) European Institute of Telesurgery (EITS)
1 place de l'Hopital - Hopitaux Universitaires 67091 STRASBOURG Cedex FRANCE

2
Since its introduction in 1991, laparoscopic antireflux surgery (LARS) has rapidly been
incorporated into the management algorithm of gastroesophageal reflux disease (GERD)
by both physicians and surgeons[1]. Given the lower morbidity rate of the laparoscopic
approach versus conventional open procedures for antireflux surgery, patients and
physicians have become more willing to consider surgery as an alternative to lifelong
medical therapy of GERD.
The results of most of the published clinical series have been excellent, with good
symptomatic outcomes in 85% to 90% of patients up to 10 years after surgery[2-4].
However, fundoplication has a published failure rate ranging from 3 to 30%[5].
Revisional surgery is necessary in 3% to 6% of these patients[6, 7].
Reoperative procedures are more technically demanding than primary fundoplications.
Moreover, anatomic defects that precipitated the failure may add to the technical
difficulty. A recent review found the average success rate after laparoscopic redo
operations to range between 65 to 100%. The broad range of values within this review,
65 to 100%[5], is at least partially due to the lack of a standard method for defining
success. Most studies have been directed toward the feasibility of and the subjective
outcome, whereas objective data on postoperative results are rarely available. Follow up
is rather short, not over 50 months.
Furnée et al.[8] reported symptomatic and objective success rate of 70% after 144 re-
operation regardless of the surgical approach laparotomy (34.7%), laparoscopy (11%) or
thoracotomy(54.2%). Mean follow-up was 60.1 months (37.2). They use a selective
approach, abdomen versus thorax, depending on the location of the wrap.
The pattern of anatomical failure of the fundoplication is similar after open and
laparoscopic procedures. Recurrent herniation, which includes migration of the wrap,
paraesophageal hernia or recurrent hiatal hernia with wrap disruption, and mis-
placement or displacement of the wrap on the stomach (slippage) are the leading
indications for redo (70-75%). Dysphagia and recurrent GERD are the most common
symptoms[5, 8, 9].

3
In a recent study of long term results (mean follow-up of 75 months) we observed rather
disappointing, both on an anatomical and subjective point of view[10]. Anatomical failure
is demonstrated in 46% of patients after redo for herniation and in 27% after slippage.
Resolution of the symptoms that justified redo surgery was achieved in 72 % of patients
operated for recurrence, and 68.7 % of patients operated for dysphagia. The global score
of GIQLI is significantly lower when compared to healthy patients and patients with a
successful primary repair GIQLI is significantly lower in patients with anatomical failure
(p=0.04). The probability of being free of failure at 5 years after the operation is 83%
after redo for herniation, 93% after redo for slippage. After 10 years the probability is
37% and 50% respectively. A third operation was needed in 7 patients (7.3%) in these
groups of failures.
Our 5 years results compare favourably with the 75 to 81% objective success rate
reported in the literature at a mean follow-up of 34.2 months[8]. Longest follow-up is
more disappointing and this highlights the need for long-term study in the evaluation of a
surgical procedure for functional disease.
Hypotheses that might explain failure rate may be the surgeon’s experience, the surgical
approach or the surgical reoperative procedure.
Surgeons involved in our study had a large experience in open and laparoscopic
antireflux surgery. Long term results obtained after primary repair were comparable to
those reported in the literature.
In a recent review of the literature, success rate after laparoscopic reoperation seemed
higher than after conventional approach, respectively 85.8 ± 5.6% and 78±10.1%[8].
This review highlighted the paucity of consistent reports and only 17 studies reported
objective outcomes. In the largest series of open redo, Deschamps reported 60.2% good
to excellent functional results at a median follow-up of 31 months in 156 patients[11].
Ten percents of patients required an additional operation. Complications occurred in
25.4% of these patients and length of stay was 9 days. At this point, we can consider
that the laparoscopic approach for redo is safer than open surgery, and yields similar
results at short or median follow-up[8, 12].

4
Therefore, surgical strategy may be questionable.
Herniation, in its different forms of presentation, can be caused by an inadequate crural
repair or an excessive traction applied on the esophagus when the GE junction is
repositioned below the diaphragm. Slippage or mis-placement of the antireflux wrap, can
be caused by an inadequate anchoring of the valve on the GE junction or by an excessive
traction on the esophagus. Crural repair is a point of controversy, some advocating wide
use of prosthetic reinforcement[13]. Yet, Koch et al.[14] recently reported a 50%
recurrence rate after reoperation for herniation with a mesh reinforced crural repair.
Similarly, in our experience, mesh does not prevent recurrence and achieves similar
results as sutures reinforced with Teflon pledegts. The risks associated with the latter are
nil, compared to some disastrous complications of mesh[15].
The common denominator for herniation and slippage recurrence, which is excessive
traction on the esophagus, addresses the question of short esophagus, which existence is
recognized by experienced centres[16-18]. In our technique, we perform systematically
an extensive mediastinal dissection, up to the level of the pulmonary veins. It’s obviously
insufficient and we probably missed some shortened esophagus. We performed only 5
Collis Nissen, and 3 of these patients are still free of symptoms and anatomical
recurrence more than 6 years after the operation. More liberal use of lengthening
procedure is probably the condition of success. In the Mayo series of open reoperations
described above, a Collis gastroplasty was performed in 62.7% of patients[11]. The
Pittsburgh group performed laparoscopic gastroplasty in 52.5% of patients in whom less
than 3 cm of tension-free intraabdominal esophagus is present[17].
Our experience and review of literature suggest that typical failure patterns after primary
antireflux repair should be initially approached laparoscopically, with a liberal use of
esophageal lengthening procedure for suspected esophageal shortening. Thoracotomy
does not provide clear and substantial advantages[19]. Failure to re-establish the normal
anatomy, which is more likely in patients with multiple failed antireflux surgeries, should
lead to consideration of other options such as near esophagojejunostomy or
esophagectomy[20].

5
References
1. Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R: Laparoscopic
Nissen fundoplication: preliminary report. Surg Laparosc Endosc 1991, 1(3):138-
143.
2. Dallemagne B, Weerts J, Markiewicz S, Dewandre JM, Wahlen C, Monami B, Jehaes
C: Clinical results of laparoscopic fundoplication at ten years after surgery. Surg
Endosc 2006, 20(1):159-165.
3. Lundell L, Miettinen P, Myrvold HE, Hatlebakk JG, Wallin L, Malm A, Sutherland I,
Walan A: Seven-year follow-up of a randomized clinical trial comparing proton-
pump inhibition with surgical therapy for reflux oesophagitis. British Journal of
Surgery 2007, 94(2):198-203.
4. Lafullarde T, Watson DI, Jamieson GG, Myers JC, Game PA, Devitt PG:
Laparoscopic Nissen fundoplication: five-year results and beyond. Arch Surg
2001, 136(2):180-184.
5. van Beek D, Auyang E, Soper N: A comprehensive review of laparoscopic redo
fundoplication. In: Surgical Endoscopy. Springer New York; 2010: 1-7.
6. Catarci M, Gentileschi P, Papi C, Carrara A, Marrese R, Gaspari AL, Grassi GB:
Evidence-based appraisal of antireflux fundoplication. Ann Surg 2004, 239(3):325-
337.
7. Carlson MA, Frantzides CT: Complications and results of primary minimally
invasive antireflux procedures: a review of 10,735 reported cases. Journal of the
American College of Surgeons 2001, 193(4):428-439.
8. Furnee EJ, Draaisma WA, Broeders IA, Gooszen HG: Surgical reintervention after
failed antireflux surgery: a systematic review of the literature. J Gastrointest Surg
2009, 13(8):1539-1549.
9. Siewert JR, Isolauri J, Feussner H: Reoperation following failed fundoplication.
World J Surg 1989, 13(6):791-796; discussion 796-797.
10. Dallemagne B, Sanchez MA, Francart D, Perretta S, Weerts J, Markiewicz S, Jehaes
C: Long-term results after laparoscopic reoperation for failed antireflux
procedures. Brit J Surg 2011, 98(11):1581-1587.
11. Deschamps C, Trastek VF, Allen MS, Pairolero PC, Johnson JO, Larson DR: Long-
term results after reoperation for failed antireflux procedures. J Thorac
Cardiovasc Surg 1997, 113(3):545-550; discussion 550-541.
12. Hunter JG, Smith CD, Branum GD, Waring JP, Trus TL, Cornwell M, Galloway K:
Laparoscopic fundoplication failures: patterns of failure and response to
fundoplication revision. Ann Surg 1999, 230(4):595-604; discussion 604-596.
13. Granderath FA, Kamolz T, Schweiger UM, Pointner R: Laparoscopic
refundoplication with prosthetic hiatal closure for recurrent hiatal hernia after primary failed antireflux surgery. Arch Surg 2003, 138(8):902-907.
14. Koch O, Asche K, Berger J, Weber E, Granderath F, Pointner R: Influence of the size
of the hiatus on the rate of reherniation after laparoscopic fundoplication and refundopilication with mesh hiatoplasty. In: Surgical Endoscopy. Springer New
York; 2010: 1-7.
15. Zugel N, Lang R, Kox M, Huttl T: Severe complication of laparoscopic mesh
hiatoplasty for paraesophageal hernia. Surgical Endoscopy 2009, 23(11):2563-
2567.
16. Horgan S, Pohl D, Bogetti D, Eubanks T, Pellegrini C: Failed antireflux surgery:
what have we learned from reoperations? Arch Surg 1999, 134(8):809-815;
discussion 815-807.

6
17. Luketich JD, Fernando HC, Christie NA, Buenaventura PO, Ikramuddin S, Schauer
PR: Outcomes after minimally invasive reoperation for gastroesophageal reflux
disease. The Annals of Thoracic Surgery 2002, 74(2):328-332.
18. Khajanchee YS, O'Rourke R, Cassera MA, Gatta P, Hansen PD, Swanstrom LL:
Laparoscopic reintervention for failed antireflux surgery: subjective and objective outcomes in 176 consecutive patients. Arch Surg 2007, 142(8):785-901;
discussion 791-782.
19. Furnee EJB, Draaisma WA, Broeders IAMJ, Smout AJPM, Gooszen HG: Surgical
Reintervention After Antireflux Surgery for Gastroesophageal Reflux Disease: A Prospective Cohort Study in 130 Patients Arch Surg 2008, 143(3):267-274.
20. Pennathur A, Awais O, Luketich JD: Minimally Invasive Redo Antireflux Surgery:
Lessons Learned. The Annals of Thoracic Surgery 2010, 89(6):S2174-S2179.

NOTES

HIATAL HERNIA
C. Daniel Smith, M.D., F.A.C.S.
Professor and Chair
Department of Surgery
Mayo Clinic
Jacksonville, Florida
Phone: 904-953-1491
Fax: 904-953-7368
e-mail: [email protected]

Paraesophageal Hiatal Hernia, CD Smith, Page 2
INTRODUCTION
The terms paraesophageal hernia and hiatal hernia are often intermixed and used
synonymously to describe enlargement of the esophageal hiatus and the subsequent
transdiaphragmatic migration of intraabdominal content, most commonly the gastric cardia and
fundus. While this exchange of terms is reasonable for healthcare providers who primarily
diagnose the anatomically enlarged esophageal hiatus, the distinction between paraesophageal
and hiatal hernia becomes important when considering how patients with this defect should be
managed. Hiatal hernia describes all types of defects involving the esophageal hiatus, of which a
subset are known as paraesophageal hernias. The anatomic differences help predict the natural
history and guide decisions about management.
PATHOPHYSIOLOGY AND CLASSIFICATION
While the exact etiology of a hiatal hernia is unknown, what is clear is that attenuation of
the phrenoesophageal membrane allows the gastroesophageal junction (GEJ) to migrate through
a patulous hiatus into the chest or the gastric fundus to herniate along side the GEJ and into the
chest. While the nature of these defects remains unknown, all types of hiatal hernias are more
common in older individuals, and recent studies suggest hiatal hernia is more common among
the obese and those with delayed gastric emptying. All of this suggests an acquired weakness of
tissue as a result of aging or excess strain on the diaphragm.
There is a well-described familial occurrence of hiatal hernias believed to represent an
autosomal-dominant link with variable clinical expression. Younger siblings of children who
have a hiatal hernia are twenty times more likely to have a hiatal hernia themselves. Some have
suggested that any hiatal hernia in a young patient indicates an underlying congenital problem.
Clearly, confounding data is available from which to guess about etiology.

Paraesophageal Hiatal Hernia, CD Smith, Page 3
Hiatal hernias are classified according to the anatomic position of the GEJ and the extent
of stomach herniated (Table 1). Type I hiatal hernia, also known as a sliding hiatal hernia,
consists of a simple herniation of the gastroesophageal junction into the chest. The
phrenoesophageal ligament is attenuated and there is no true hernia sac. This is the most
common type of hiatal hernia, is more common in women and in the fifth and sixth decades of
life. Type II hiatal hernia, commonly referred to as a true paraesophageal hernia, denotes when
the GEJ remains at the esophageal hiatus while the gastric fundus herniates alongside the
esophagus into the chest. The type III hiatal hernia is a combination of type I and type II hernia,
with the GEJ being displaced into the chest along with the gastric fundus and body.
Paraesophageal hernias (types II and III) have a true hernia sac accompanying the herniated
stomach. This becomes important when surgical repair is undertaken as the sac must be excised.
Finally, some have characterized a type IV hernia as an advanced stage of hiatal hernia where the
entire stomach and other intraabdominal content (e.g., colon, spleen, etc.) are herniated into the
chest. Use of this fourth classification is not widely accepted.
INCIDENCE
While the exact prevalence of hiatal hernia remains unknown, it is clear that it is a
relatively common abnormality and is the most common finding reported on barium studies of
the upper gastrointestinal tract. The difficulty in establishing the incidence of hiatal hernia lies in
the fact that a large number of patients with hiatal hernia are asymptomatic, and the diagnosis is
often made incidentally during investigation of other gastrointestinal problems.
In contrast to all hiatal hernias, paraesophageal hernia is a very rare type of hiatal hernia.
In a series of 46,236 Mayo Clinic patients with hiatal hernias, only 147 (0.32%) were type II or

Paraesophageal Hiatal Hernia, CD Smith, Page 4
true paraesophageal hernias, with women twice as likely to have this type of hernia as men. The
frequency of paraesophageal hernia increases with advancing age.
SYMPTOMS AND PRESENTATION
Most Type I and III hiatal hernias are diagnosed incidentally during a contrast upper GI or
during upper endoscopy performed for other reasons. Type II hernias can be similarly diagnosed,
but are also frequently found on a radiograph of the chest showing an air-fluid-level in the
mediastinum or the left chest. Occasionally, the inability to pass a nasogastric tube followed by a
contrast study reveals a twisted intrathoracic stomach, or a contrast study of the colon reveals
colon in the chest leading to the diagnosis of a type IV hernia.
When symptoms are present, sliding hernias have a different presentation than
paraesophageal hernias. Type I hernias are frequently accompanied by symptoms of
gastroesophageal reflux (GERD), most commonly heartburn or regurgitation. Type II and III
hernias tend to produce symptoms that are more mechanical in nature due to the anatomic
consequence of the hiatal outflow restriction. Typical symptoms include epigastric pain,
postprandial fullness or discomfort in the chest, dysphagia, abdominal bloating, and respiratory
problems. Again, these symptoms are caused by hiatal outflow restriction, altered gastric
anatomy, and distension of the intrathoracic portion of the stomach with esophageal or
pulmonary compression. Interestingly, patients often report a remote history of GERD type
symptoms that abruptly abate and are replaced by obstructive symptoms; this thought to occur as
the hernia enlarges and the esophageal outlet becomes obstructed.
Acute symptoms may develop as a consequence of complete obstruction or strangulation
of the stomach within the chest mimicking myocardial infarction. Type II hernias are at
particular risk for incarceration with obstruction, strangulation and perforation of the herniated

Paraesophageal Hiatal Hernia, CD Smith, Page 5
stomach. Borchardt’s triad comprised of chest pain, retching with inability to vomit, and
inability to pass a nasogastric tube is indicative of an incarcerated hernia and is a surgical
emergency.
An often-overlooked presentation is anemia from chronic GI blood loss. This occurs in
1/3 of patients with type II hernias and prompts an often-exhaustive evaluation for cause. This
anemia is caused by linear ulcerations of the gastric cardia resulting from the proximal stomach’s
repetitive movement across the diaphragm. Ninety two percent of patients will have their anemia
resolve after surgical correction of the hernia.
MANAGEMENT
While most hiatal hernias are asymptomatic, the diagnosis is rarely in question when
patients present with symptoms as outlined above and a chest x-ray or contrast esophogram
confirming the defect. An EGD should be attempted in all patients to assess the distal esophagus
and stomach for concomitant pathology, with caution not to over inflate the stomach that may be
incarcerated in the chest. While motility studies may help identify the patient with esophageal
motor abnormality and direct the type of fundoplication used in repair, the distortion of the GEJ
and distal esophagus makes motility studies difficult to acquire and interpret. For this reason,
motility studies are not useful for most type II and III hernias. The same is true of 24-hour pH or
gastric emptying studies. These studies can be difficult to interpret and rarely change the
decisions regarding management. A CT scan of the chest and abdomen may help confirm the
extent of the hernia, but are not necessary for straightforward cases.
Since hiatal hernia is a purely mechanical abnormality, there is no non-operative
treatment. Currently there is controversy about which patients should undergo repair.
Traditionally it has been held that all patients with type II or III hernias should undergo surgical

Paraesophageal Hiatal Hernia, CD Smith, Page 6
repair regardless of symptoms. This has been based on a report in 1967 documenting a 30%
mortality in patients with paraesophageal hernia (6 of 21 patients died secondary to
complications of their hernia). More recently, a series of 23 patients with a paraesophageal
hernia were followed for a median of 78 months and no life threatening complications developed
in this group and symptoms remained unchanged in 83% of these patients. This has lead many to
recommend repair in only select asymptomatic patients. In contrast, those with symptoms,
esophageal mucosal damage (esophagitis or Barretts), or anemia should undergo elective repair.
Similarly, a significant number of patients with type I hiatal hernias are asymptomatic and
remain so throughout the remainder of their life. Therefore, the presence of a sliding hiatal
hernia alone does not mandate intervention. However, those patients with a Type I hernia and
gastroesophageal reflux, chest pain, dysphagia, regurgitation or other symptoms referable to their
hernia, should undergo symptom specific workup, and may be best served with an operative
repair.
OPERATIVE TECHNIQUE
Operative correction of esophageal hiatal hernia regardless of technique should 1) return
the herniated content to its anatomically correct position below the diaphragm, 2) resect the
hernia sac, 3) establish adequate esophageal length and return the GEJ to an intraabdominal
position, 4) repair the hernia defect, and 5) prevent recurrence while minimizing associated
morbidity. There are a number of proven operations that can be performed through the chest or
abdomen to accomplish these goals.
Currently, the most common approach to hiatal hernia repair is transabdominal using
laparoscopy, although many advocate the open transabdominal approach. Debate continues over
whether a laparoscopic approach compromises the long-term outcome of the repair (see

Paraesophageal Hiatal Hernia, CD Smith, Page 7
Controversies below). While most would agree that the laparoscopic approach is preferred due
to the enhanced recovery associated with laparoscopy, especially in this typically more elderly
patient population, it is clear that the laparoscopic approach is more technically challenging and
if performed by inexperienced surgeons may lead to a higher incidence of peri-operative
complications or long-term failure. On the other hand, when performed by an experienced
laparoscopist and foregut surgeon, the technique of the operation should not differ from that
performed open and thereby lead to no differential outcome.
Historically the thoracic approach has been preferred for larger hernias and those with
suspected esophageal shortening. The relative ease of dissecting the hernia sac and mobilizing
the esophagus makes this approach appealing in select settings. However, the morbidity
associated with a thoracotomy, both immediately postoperatively and long-term with chronic
incisional problems makes this approach appealing in only a small subset of patients.
OUTCOMES
The outcomes of hiatal hernia repair can be broken into symptomatic outcomes and
anatomic outcomes. When considering symptomatic response to operative repair, 88% of
patients after hiatal hernia repair report a significant improvement or resolution of their
preoperative symptoms. This response appears durable with sustained symptom improvement
for up to 4 years after surgery. Ninety-two percent of those with anemia have resolution after
hernia repair. On the other hand, anatomic failure after hernia repair remains very high, with up
to 41% of patients demonstrating recurrent hernia an average of 4 years after repair. Some have
suggested that this rate of anatomic failure is lower when the repair is performed open (see
Controversies below). Regardless, the significance of these anatomic failures remains debated.
A small transdiaphragmatic migration of the wrap or GEJ, essentially an asymptomatic type I

Paraesophageal Hiatal Hernia, CD Smith, Page 8
hernia, is clinically inconsequential. To aspire to a higher rate of anatomic success risks over
treatment and potentially profound complications, especially when mesh is used in the repair.
CONTROVERSIES
Should an antireflux procedure accompany all hiatal hernia repairs?
Whether or not to include an antireflux procedure with all hiatal hernia repairs remains
controversial, especially when dealing with a type II paraesophageal hernia. Since most sliding
type hernias are repaired based on symptoms, adding an antireflux procedure seems more
straightforward due to the prevalence of reflux symptoms in type I and III hernias. In contrast,
most patients who have type II hernias do not have reflux symptoms, and adding an antireflux
operation in these patients may add little to the outcome. However, with careful questioning,
many patients with type II hernias give a history of GERD symptoms that spontaneously abated,
suggesting an anatomic change (perhaps hernia development) leading to this resolution of
symptoms. Recent data from small series are suggesting that GERD may be more prevalent in
type II hernia than earlier recognized, and up to 30% of patients without GERD preoperatively
will have GERD unmasked after hiatal hernia repair.
The role of fundoplication in patients with type II paraesophageal hernia remains
controversial. Conventional thinking suggests that because the lower esophageal sphincter is
located within the abdomen, it is competent and fundoplication is unnecessary. On the other
hand, a key principle in repairing a hiatal hernia is to anchor the stomach within the abdomen to
help prevent recurrence, and some surgeons are now using a fundoplication to serve as this
anchor (the wrap buttresses against the hernia repair and holds the distal esophagus and stomach
intra-abdominally). In up to one third of patients, adding fundoplication may avert the
unmasking of GERD following repair. This rationale is leading many surgeons to use

Paraesophageal Hiatal Hernia, CD Smith, Page 9
fundoplication routinely for all hiatal hernia repairs. Early data suggests that this is a safe and
effective means of managing paraesophageal hernias. However, few studies have objectively
evaluated addition of an antireflux procedure to hiatal hernia repair, and there is limited data
available to definitively answer this question.
Should hiatal hernias be repaired laparoscopically?
The role of laparoscopy in repairing hiatal hernias has recently been challenged.
Anecdotal data suggests that the risk of esophageal or gastric perforation and hernia recurrence is
higher following laparoscopic repair than after traditional open hiatal hernia repair. The
proposed basis for this is increased technical demands with a laparoscopic approach, the
difficulty closing the attenuated esophageal hiatus laparoscopically, and the relative absence of
intraabdominal adhesions that accompanies laparoscopic hernia repair as compared to open
operations. The absence of these adhesions to anchor the stomach and distal esophagus allows
the stomach to more readily “slip” back through the esophageal hiatus and into the chest than
would be the case with the adhesions associated with open repairs. These anecdotal experiences
need further investigation before any conclusions regarding route of abdominal access for repair
of hiatal hernia can be made, and most would agree that a laparoscopic repair performed by a
skilled laparoscopic foregut surgeon should not have any higher rate of complications or failure.
Should mesh be used to repair all hiatal hernias?
The high rate of anatomic failure of hiatal hernia repairs has lead many to suggest that
some sort of prosthetic should be used to reduce these failures. Many argue that the principle of
“tension-free” repair embraced for abdominal wall hernias is generalizable to hiatal hernias as
well. Over the past several years many types of prosthetic material has been used empirically for
reinforcement of the crural repair or hiatal reconstruction for the crura which cannot be

Paraesophageal Hiatal Hernia, CD Smith, Page 10
approximated. A non-randomized prospective study suggested a lower recurrence rate without
any increase in dysphagia in a series of patients where permanent mesh (polypropylene) was used
in all patients undergoing laparoscopic Nissen fundoplication. A more recent collection of
experience from several experienced foregut surgeons identified over 20 patients in whom mesh
was used to reconstruct the esophageal hiatus and subsequently eroded into the esophagus
leading to significant complications including progression to esophagectomy is several patients.
These findings have led many to advocatebioprosthetic mesh that can be used to decrease
the hiatal hernia recurrence rate without such complications. A multicenter, prospective
randomized trial compared the use of a crural buttress using a mesh constructed from porcine
small intestinal submucosa compared to primary repair.51 This study utilized barium swallow X-
rays performed at 6 months postoperatively that demonstrated anatomic hiatal hernia recurrence
in 24% of patients undergoing primary repair compared to only 9% of patients receiving the
bioprosthetic buttress. However, in an update at 5 years postoperatively, the recurrence rate was
nearly identical between the two groups, and in excess of 50%.52 It should be noted that the
majority of recurrent hiatal hernias were small type I hernias resulting in few symptoms. Thus, at
the current time, although the rationale for the use of mesh at the esophageal hiatus to decrease
tension and thus minimize hernia recurrence is cogent, it is unclear if mesh should be used, and if
so, what type.
These findings have led many to look to a bio-mesh that can be used to decrease the hiatal
hernia recurrence rate without such complications. A multicenter, prospective randomized trial
compared the use of a crural buttress using a mesh constructed from porcine small intestinal
submucosa compared to primary repair. Barium swallow performed at 6 months postoperatively

Paraesophageal Hiatal Hernia, CD Smith, Page 11
revealed anatomic hiatal hernia recurrence in 24% of patients undergoing primary repair
compared to only 9% of patients receiving the bioprosthetic buttress. However, at 5 years
postoperatively, the recurrence rate was nearly identical between the two groups and in excess of
50%. As had already been demonstrated in other studies, the majority of recurrent hiatal hernias
were small type I hernias with few symptoms. Thus, at the current time, although the rationale for
the use of mesh at the esophageal hiatus to decrease tension and thus minimize hernia recurrence
is appealing, it is unclear if mesh use provides any real benefit and is it should be used at all, and
if so, what type.

Paraesophageal Hiatal Hernia, CD Smith, Page 12
SUGGESTED READINGS
Skinner DB, Belsey RH: Surgical management of esophageal reflux and hiatus hernia. Long-
term results with 1,030 patients. J Thorac Cardiovasc Surg 1967; 53: 33.
Terry M, Smith CD, Branum GD, Galloway K, Waring JP, Hunter JG. Outcomes of laparoscopic
fundoplication for gastroesophageal reflux disease and paraesophageal hernia. Surgical
Endoscopy 2001;15(7): 691-699.
Mattar SG, Bowers SP, Galloway KD, Hunter JG, Smith CD. Long-term outcome of
laparoscopic repair of paraesophageal hernia. Surgical Endoscopy 2002;16(5): 745-749.
Lin E, Swafford V, Chadalavada R, Ramshaw BJ, Smith CD. Disparity between symptomatic
and physiologic outcomes following esophageal lengthening procedures for antireflux surgery.
Journal of Gastrointestinal Surgery 2004;8(1): 31-39; discussion 38-39.
Smith CD, McClusky DA, Rajad MA, Lederman AB, Hunter JG. When fundoplication fails:
redo? Annals of Surgery 2005;241(6): 861-869; discussion 869-871.
El Sherif A. Yano F. Mittal S. Filipi CJ. Collagen metabolism and recurrent hiatal hernia:
cause and effect? Hernia 2006; 10:511-20.
Oelschlager BK. Pellegrini CA. Hunter J. Soper N. Brunt M. Sheppard B. Jobe B. Polissar N.
Mitsumori L. Nelson J. Swanstrom L. Biologic prosthesis reduces recurrence after laparoscopic

Paraesophageal Hiatal Hernia, CD Smith, Page 13
paraesophageal hernia repair: a multicenter, prospective, randomized trial. Annals of Surgery
2006; 244:481-90.
Oelschlager BK, Pellegrini CA, Hunter JG, et al. Biologic prosthesis to prevent recurrence after
laparoscopic paraesophageal hernia repair: long-term follow-up from a multicenter, prospective,
randomized trial. Journal of the american college of surgeons. 2011;213(4):461-8.

Paraesophageal Hiatal Hernia, CD Smith, Page 14
TABLE
Table 1. Classification of Hiatal Hernias.
Hernia Type Location of Gastroesophageal Junction Hernia Contents
I (Sliding) Intrathoracic Gastric Cardia ± Fundus
II (True Paraesophageal) Intraabdominal Gastric Fundus ± Body
III (Combination I & II) Intrathoracic Gastric Fundus and Body
IV Intrathoracic Gastric Fundus, Body and other
abdominal organs (e.g., colon)

NOTES

Beyond GERD and Hiatal
Hernia:
What To Do in the Obese?
Samer G. Mattar, MD, FACS, FASMBS
Associate Professor of Surgery
Indiana University School of Medicine
Epidemiology
• The prevalence of obesity has increased dramatically from 13% to 34% in US population.
• The prevalence of GERD has increased • The prevalence of GERD has increased significantly over past 40 years (20%-30% of
population).
• There appears to be a dose-response relationship between BMI and GERD (gain
BMI 3.5 units = 3 fold increase in GERD symptoms.)Friedenberg et al; Am Coll Gastroenterol:2008Serag; Dig Dis Sci:2008

Epidemiology
• Nearly all epidemiological studies have found an association between obesity and GERD.
• There is a linear relationship between BMI • There is a linear relationship between BMI and GERD symptoms.
• Central adiposity may be the most important risk factor.

Epidemiology
• Waist circumference, rather than BMI, appears
to be has a stronger link (OR 4.3) with long-
segment BE.
• In another study, patients obese > 20 years had • In another study, patients obese > 20 years had
an OR 16.2 for developing esophageal
adenocarcinoma.
• The incidence of esophageal cancer has
increased >650% over past 35 years.
Edelstein et al; Gastroenterol: 2007
Lagergren J et al; Gut 2000
Brown et al. J Natl Cancer Inst 2008; 100:1184-87
Epidemiology
• In a pooled analysis of 12 epidemiological international
studies (BEACON), there were 1997 OA cases, 1990
OGJA cases, and 11,160 control subjects.
• By logistic regression and random-effects meta-analysis, • By logistic regression and random-effects meta-analysis,
BMI ≥40 was associated with both OA (OR 4.76, 95% CI
2.96-7.66) and OGJA (OR 3.07, 95% CI 1.89-4.99).
• There was synergistic interaction between BMI and
GERD symptoms in relation to OA/OGJA risk.
Hoyo C et al. Int. J. Epidemiol. 2012;ije.dys176

Restricted cubic spline models of the relationship between body mass index and adenocarcinomas of the oesophagus and oesophagogastric junction.
OA
MalesFemales
Hoyo C et al. Int. J. Epidemiol. 2012;ije.dys176
OGJA
Males Females

Epidemiology
• There was no evidence of effect modification when
stratified by GERD symptoms, suggesting an indirect
proinflammatory route of association between BMI and
OA/OGJA exists.
• The higher prevalence in men may be due to the typical
android fat patterning, with highly metabolic visceral
adipose.
• Obesity-related hormones may induce esophageal
inflammatory damage, promoting proliferation and
malignant transformation.Hoyo C et al. Int. J. Epidemiol. 2012;ije.dys176

Esophageal Acid Exposure in the
Obese (48h)
8
10
12
Normal Weight
157 patients
0
2
4
6
Total Upright Supine
Normal Weight
Overweight
Obese
Percent pH<4
Crowell et al; Am J Gastroenterol:2009

Causes of GERD
• Reduced LES sphincter pressure.
• Increased frequency of transient LES
relaxations.
• Increased prevalence of hiatal hernias.• Increased prevalence of hiatal hernias.
• Increased prevalence of esophageal motor
disorders.
• Increased prevalence of gastric motor disorders.
• Pro-inflammatory agents?

Causes of GERD
Do these factors apply in the morbidly obese?in the morbidly obese?

Unidentified cause of GERD in the
Morbidly Obese?
15
20
25
599 patientsMO was independently associated with GERD severity
0
5
10
15
Normal Wt MO
HTN LES
HTN DE Amp
%
Herbella et al; J of Gastrointest Surg: 2007

Nissen Fundoplication in the
Morbidly Obese
20
25
30
35
187 patients
0
5
10
15
20
NW OW OB
Recurrence (%)
Perez et al; Surg Endosc:2001

Surgical Options
• Gastric bypass
• Adjustable gastric band
• Sleeve gastrectomy
• Duodenal switch• Duodenal switch
• NOTES
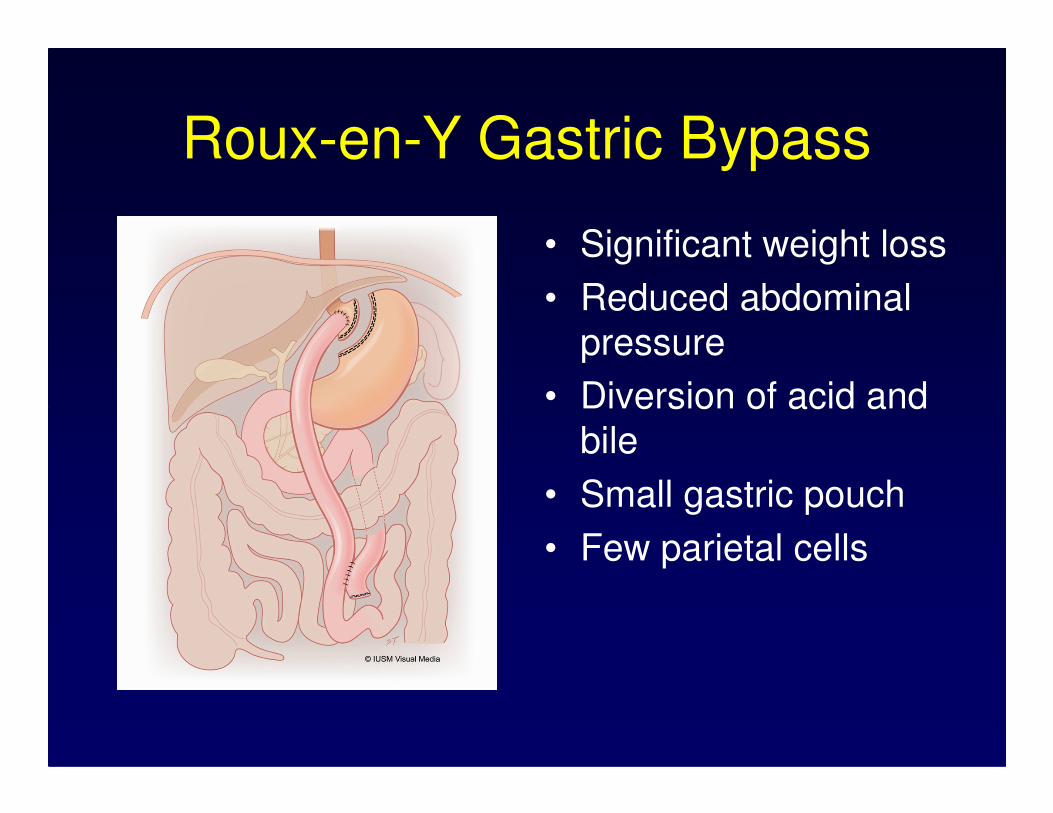
Roux-en-Y Gastric Bypass
• Significant weight loss
• Reduced abdominal
pressure
• Diversion of acid and • Diversion of acid and
bile
• Small gastric pouch
• Few parietal cells

Roux-en-Y Gastric Bypass
8
10
12
20 patients
0
2
4
6
Preop Postop
pH<4 (%)
Mejia-Rivas et al; Obes Surg: 2008

Adjustable Gastric Band
• Controversial
• Conflicting outcome
reportsreports
• MUST repair crural
defect if hiatus hernia
present.

Adjustable Gastric Band
• Initial improvement of GERD in band patients.
• Gastric band may act to reinforce anti-reflux mechanism.reflux mechanism.
• However, there is an increased incidence of 20.5 % of developing late GERD
Dixon and O,Brien; Obes Surg; 1999Himpens et al; Obes Surg: 2006

Adjustable Gastric Band
• Retrospective study
• 1298 LAGB only vs. 520 LABG + HHR
• Mean FU = 25 months vs. 20 months
• Reoperation rate = 5.6% vs. 1.7%• Reoperation rate = 5.6% vs. 1.7%
• Reoperations were for HH, band slip, or pouch dilatation.
• Conclusion: Adding HHR to LAGB reduced the reoperation rate.
Gulkarov et al. Surg Endosc 2008;22(4):1035-45

Sleeve Gastrectomy
SG may exacerbate GERD due to:
- generation of high
intragastric pressuresintragastric pressures
- division of sling fibers
- disruption of angle of
His
- narrowing at incisura

Sleeve Gastrectomy
Prerequisites in GERD patients:
- repair hiatal hernia- repair hiatal hernia
- do not use a very
small bougie

• 176 patients with Sleeve Gastrectomy
• 34.6% Pre-op GERD
• Post-op(<30d) GERD = 49%.
• Persistent(>30d) GERD = 47.2%.
• Medication for GERD 33.8%
Prevalent Thinking
• Medication for GERD 33.8%
Carter PR, Leblanc KA et al. SOARD 7 2011(569-574)
*Anterior repair of Hiatus Hernias

Prevalent Thinking
Himpens 2006: Band vs Sleeve:
Pre-existing GERD: 75% resolution after SG
butbut
22% denovo GERD cases developed at 1 year
but
GERD improved from year 1(22%) to 3(3%)
Himpens J, Dapri G, Cadiere GB. Obes Surg 2006;16:1450-6

Systematic review:
• 15 reports
• 4 showed increase in GERD
• 7 found reduced GERD
Prevalent Thinking
• 7 found reduced GERD
• 3 reported on only postoperative GERD prevalence.
• Conclusion: No consensus
Chiu, Birch et al. SOARD 7 (2011) 510-515

• 706 patients underwent sleeve gastrectomy
• 8 (1.1%) developed severe reflux symptoms and
proximal sleeve dilation.
Technical Factors: Effect on GERD
Keidar A, Baltasar A. Obes Surg. 2010 Feb; 20(2): 140-7.
proximal sleeve dilation.
• 1 required reoperation, 7 managed medically.

�20 patients had manometry pre and post SG
�BMI decrease: 38kg/m2 to 28.2kg/m2 at 6
months
Motility Factors: Effect on GERD
�Mean LESP preop 14.2 mmHg
�6 months postop 11.2 mmHg
�Ten with <6 mmHg.
�Explanation: resection of the sling fibers?.
Braghetto, I Obes Surg(2010) 20:357-362

Reasons why sleeve may REDUCE GERD
• Reduces acid production
• Removes the fundus which
is the source of relaxation
waves to the LES
• Reduces tension on gastric • Reduces tension on gastric
wall below the cardia
• Accelerates gastric
emptying
• Correct repair of HH
• Weight loss

Reasons why sleeve may
WORSEN or CAUSE GERD�� Aggressive encroachment at angle of His Aggressive encroachment at angle of His
may may resectresect sling fibers and reduce LESsling fibers and reduce LES
�� Narrowing at Narrowing at angularisangularis may create may create obstructionobstruction
�� Initial architecture may not remain static: Initial architecture may not remain static: �� Initial architecture may not remain static: Initial architecture may not remain static: pouch malformations leading to pouch malformations leading to obstruction and reflux can occur over obstruction and reflux can occur over time. time. IntrathoracicIntrathoracic migration, retained migration, retained fundusfundus..
�� Patent HH > 3cmPatent HH > 3cm
�� It may be “pseudoIt may be “pseudo--reflux” due to reflux” due to improper alimentation.improper alimentation.

Pouch Deformities may occur over time
and lead to reflux symptoms
• Coiling or Spiraling
• Dilated upper sleeve
• Others: angulation, volvulus, gastric atony, fundic regeneration, diverticulum.
• Options for Prevention:
– Avoid excess cardia
– Omental fixation to the new greater curve
– Create a slightly larger pouch at the angularis
Fixation

HH repair: Effect on GERD
• 378 SG pts
• All had preop manometry and 24h pH
• Preop GERD in 41pts.
• HH > 3cm was considered abnormal
• 97pts had concomitant posterior crural repair• 97pts had concomitant posterior crural repair
• GERD remission in 80% and reduction in 20%
• Denovo GERD in 23% of pts who had SG alone
• No denovo GERD in any pt with SG + HHR
• Is HHR protective against denovo GERD?
Soricelli E, Basso N, et al. SOARD 2012 in press

HHR and LRYGB
Controversial
• LRYGB is a very effective anti-reflux operation.

Herniated Gastric Pouch
Flanagin BA et al. Obes Surg 2010; 20(3):386

Herniated Gastric Pouch
Flanagin BA et al. Obes Surg 2010; 20(3):386

Impact of HHR and LRYGB
• Retrospective review of UHC data
• 1589 patients with HH had LRYGB only
• 644 patients had LRYGB + HHR
• There was no difference in mortality, • There was no difference in mortality, morbidity, 30 day readmission, LOS, and cost.
• Conclusion: LRYGB + HHR is safe
Kuthari et al Obes Surg 2012;22(10):1607-10

Summary
• Hiatus hernias are common in patients
undergoing bariatric surgery.
• It is recommended to repair HH in patients
having gastric band surgery.having gastric band surgery.
• In Sleeve Gastrectomy patients, there is
conflicting data, but trend is to offer it to patients
with HH and/or GERD.
• It is recommended that HH be repaired in
patients undergoing SG.

Summary
• In patients undergoing LRYGB, there is no additional M&M for concomitant repair of HH.
• Concomitant HHR and LRYGB may • Concomitant HHR and LRYGB may prevent gastric pouch herniation if HH are very large.

NOTES

Emerging Technologies and Techniques in GERD
Reginald C.W. Bell M.D.
SurgOne Foregut Institute
401 W Hampden Place Suite 230
Englewood CO 80110
303-788-8989
Emerging Diagnostic Technologies
ENRD:
Current ambulatory imp/pH testing lacks sensitivity in diagnosis of endoscopy-negative GERD
(ENRD, no longer NERD), ranging from 0%-71%, and does not delineate injury to esophagus. The
finding of dilated intercellular spaces is considered a fairly specific finding of NERD, but is currently
not a practical test (where to biopsy, need for EM of biopsies).
Evaluation of mucosal impedance using a catheter at time of endoscopy may have a role in the
diagnosis of ENRD. [1] (Figures 1 and 2).
LPR:
Finding more specific methods of diagnosis LPR remains problematic, especially for surgeons
referred patients for antireflux procedures. Pepsin has been a topic of interest; recent report of no
Difference in pepsin or bile acids in induced sputum between patients with chronic cough and
controls[2].
Therapeutic Innovations The potential role of therapies other than laparoscopic fundoplication is significant.
Probably 30 million patients in the US have GERD. Thirty to 50% of patients treated with daily
PPIs are dissatisfied with the results of their therapy. Doubling PPI dose provides relief in 25% of this
subgroup.[3] Surgical treatment is often omitted from articles reviewing treatment of medically
refractory GERD (MRG) – indicating a failure of the surgical community to provide adequate treatment
options.
Laparoscopic fundoplication is performed approximately 25,000 cases per year in the US [4], or in
less than 1% of the 5-10 million patients with medically refractory GERD.
Antireflux surgery is invasive, creates a permanent change in gastro- esophageal anatomy and
long-term outcomes are variable and highly dependent on the skill of the surgeon. Furthermore, the
efficacy of antireflux surgery deteriorates over time with substantial number of patients requiring
treatment with acid suppression medication for control of symptoms and revisional (re-do) surgery.
Antireflux surgery is associated with side effects such as dysphagia, bloating, inability to vomit, and
diarrhea, which, though infrequent, are genuine. These side effects and the need for reoperation are the
main drawbacks of antireflux surgery.
What should be the therapeutic goal of surgical treatment of GERD? A minority of patients with
refractory GERD do require near complete control of reflux to facilitate healing of esophagitis,
eliminate potential for aspiration, and so forth. However the majority of patients with refractory GERD
are looking for improved symptom control. 25-50% of patients rendered asymptomatic on PPIs have
excess esophageal acid exposure.
Radiofrequency Energy Delivery to the Lower Esophageal Sphincter
RF energy can be delivered to the LES using the Stretta Device. The device is currently available
commercially (Mederi Therapeutics Inc.,Greenwich, CT 06830).
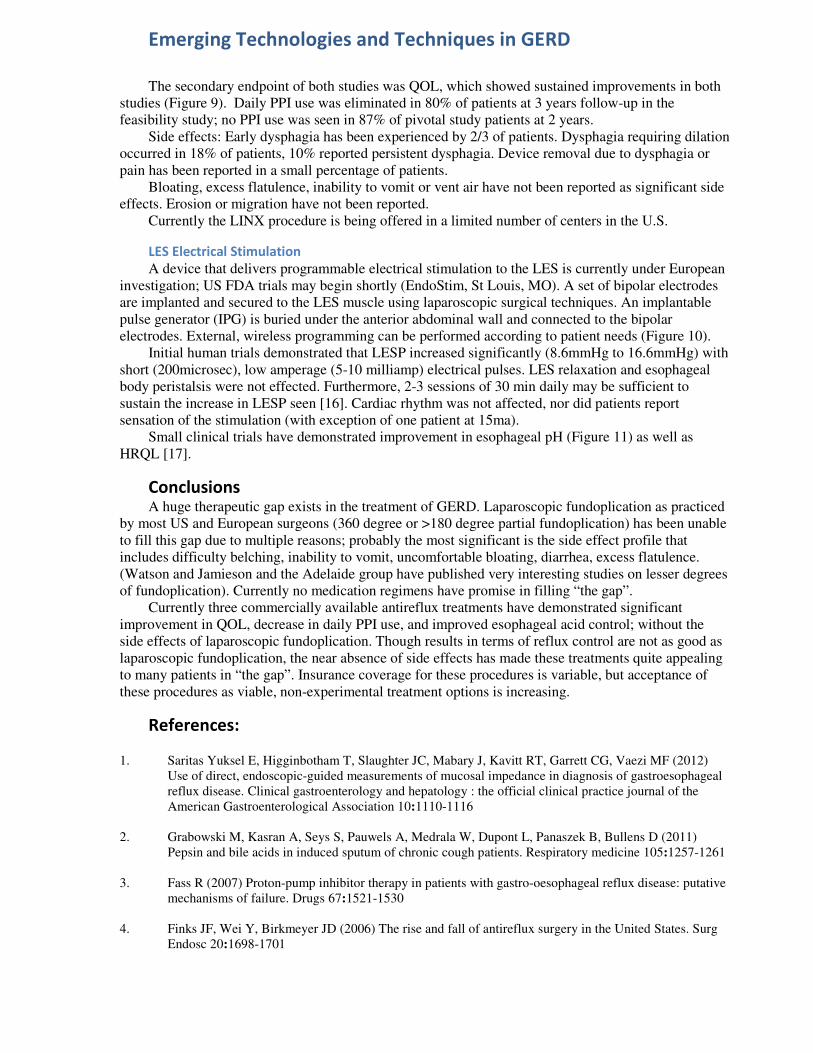
A recently published metaanalysis of a total of 1441 patients from 18 studies were included.
Radiofrequency treatment improved heartburn scores (P=0.001), and produced improvements in quality
of life as measured by GERD–health-related quality-of-life scale (P=0.001) and quality of life in reflux
and dyspepsia score (P=0.001). Esophageal acid exposure decreased from a preprocedure Johnson-
DeMeester score of 44.4 to 28.5 (P=0.007) (Figure 3)[5].

Emerging Technologies and Techniques in GERD
A sham-controlled study indicated that decreased GEJ compliance after the Stretta procedure was
reversed by sildenafil, questioning the theory that the Stretta device produces fibrosis of the GE
junction[6].
Transoral Fundoplication
Currently the only commercially available device enabling transoral reconstruction of the GE
junction is the EsophyX device (EndoGastric Solutions, Redmond, WA). The technique of transoral
incisionless fundoplication (TF or TIF) using this device has evolved from a gastro-gastric plication to
an esophago-gastric fundoplication (Figure 4)[7].
Most reports of transoral fundoplication with the EsophyX device have been limited by small
numbers, frequently representing the learning curve, and with short follow-up. Results have been, not
surprisingly, quite variable (Figure 5)
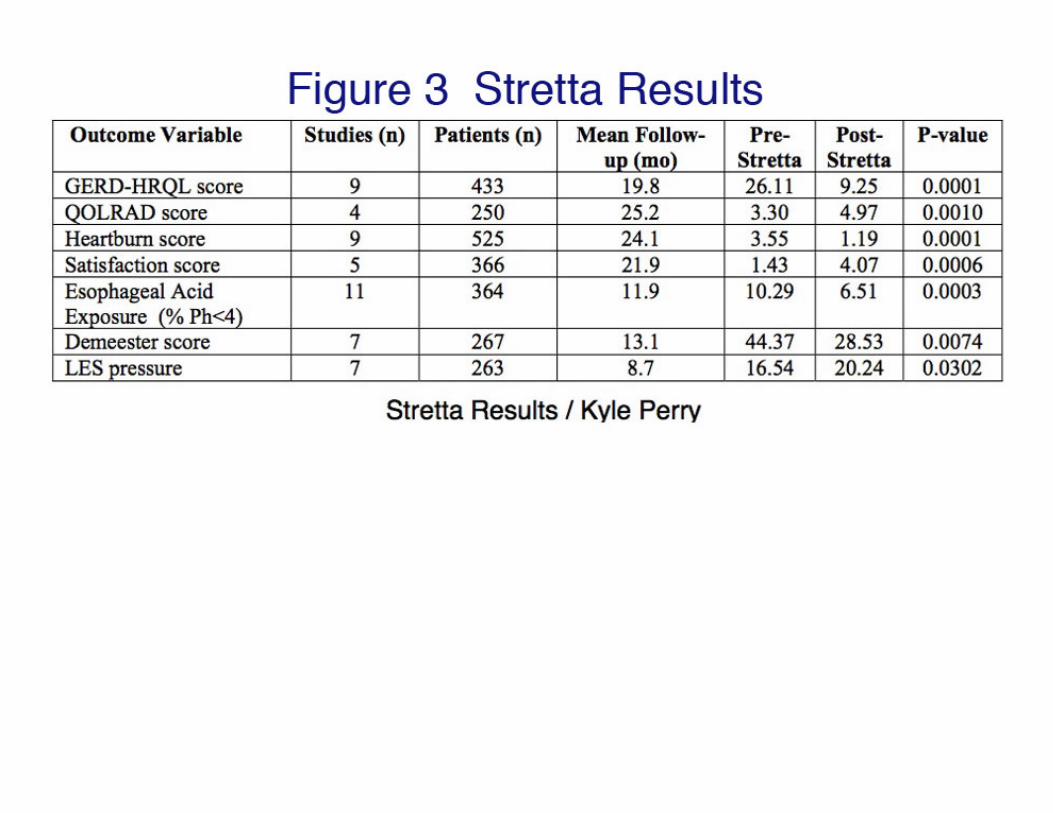
Prospective 6 month and 1 year follow-up reports of a cohort of 100 patients undergoing TIF have
demonstrated a small decrease in clinical success between the two time periods (Figure 6). 24-month
and 36-month clinical follow-up is underway (24-month to be reported at SAGES 2013). Muls et al
reported long-term (3+ year) data on patients treated with an early TIF technique (ELF, TIF 1). Of 79
patients followed at 1 year, 13 were lost to f/u. Of remaining 66, 12 had undergone revisional
procedures. Sustained discontinuation of daily PPI use at median of 3.1 years was 61% (mITT) and
74%(PerProtocol) [8].
An important finding across multiple studies of the TIF procedure has been that the side-effect
profile (dysphagia, bloating, increased flatus) has been minimal (< 1%) and when reported have not
been severe.
Patients requiring laparoscopic revision to traditional fundoplication after TIF have been reported
to have a higher risk of infection[9] or postoperative dysphagia[10].
One limitation of all transoral antireflux procedures is the inability to repair hiatal hernias of any
significant size (generally 2cm axial height). Some surgeons have performed laparoscopic hiatal hernia
repair in combination with transoral fundoplication (with the premise that transoral fundoplication will
have a lower side-effect profile than laparoscopic fundoplication). However, prospective data is lacking,
with one retrospective study suggesting at least that the procedure was safe [11].
Patients who have a failed 360-degree fundoplication without an obvious hernia may benefit from
transoral revision of the fundoplication [12].
Magnetic Augmentation of the Lower Esophageal Sphincter (LINX system)
This system consists of a series of interlinked titanium beads with magnetic cores that is implanted
laparoscopically around the lower esophagus. The beads for a non-compressive Roman arch gently
resting around the lower esophagus. The lower esophagus, at rest, is typically closed. The beads will
separate when the intraluminal pressure at the beads reaches 15-20mmHg, and so will allow swallowed
food and liquids to pass through (as long as reasonable motility is present). Most gastroesophageal
reflux occurs with a pressure gradient of 9-11mmHg, and so will not occur with the LINX device in
place. However higher G-E pressure gradients (such as occur with vomiting) will open up the
augmented LES and allow retrograde bolus movement (Figure 7).
The LINX system gained FDA approval in May 2012 on the basis of two clinical trials (a
feasibility study conducted primarily in Europe, [13] [14] and a pivotal study conducted primarily in the
U.S. [15]) Patients entered into the study were partially but incompletely responsive to PPI therapy,
possessed early stage disease (HH < 3cm axial, no LA C or D, stricture, LSBE), and good esophageal
body motility (DEA >35 or DCI >400) without troublesome dysphagia.
The primary endpoint of both studies was objective – esophageal acid exposure. Eighty percent of
20 patients followed to 3 years in the feasibility trial normalized total esophageal acid exposure time. In
the FDA pivotal trial, the mean total acid exposure time was reduced from 11.6% at baseline to 5.1% at
12 months. 90% of treated subjects (86/96) had some reduction in their total acid exposure time.
Normalization of total acid exposure occurred in 67% (64/96) of pivotal trial subjects who completed
pH testing at 12 months (Figure 8).
Emerging Technologies and Techniques in GERD
The secondary endpoint of both studies was QOL, which showed sustained improvements in both
studies (Figure 9). Daily PPI use was eliminated in 80% of patients at 3 years follow-up in the
feasibility study; no PPI use was seen in 87% of pivotal study patients at 2 years.
Side effects: Early dysphagia has been experienced by 2/3 of patients. Dysphagia requiring dilation
occurred in 18% of patients, 10% reported persistent dysphagia. Device removal due to dysphagia or
pain has been reported in a small percentage of patients.
Bloating, excess flatulence, inability to vomit or vent air have not been reported as significant side
effects. Erosion or migration have not been reported.
Currently the LINX procedure is being offered in a limited number of centers in the U.S.
LES Electrical Stimulation
A device that delivers programmable electrical stimulation to the LES is currently under European
investigation; US FDA trials may begin shortly (EndoStim, St Louis, MO). A set of bipolar electrodes
are implanted and secured to the LES muscle using laparoscopic surgical techniques. An implantable
pulse generator (IPG) is buried under the anterior abdominal wall and connected to the bipolar
electrodes. External, wireless programming can be performed according to patient needs (Figure 10).
Initial human trials demonstrated that LESP increased significantly (8.6mmHg to 16.6mmHg) with
short (200microsec), low amperage (5-10 milliamp) electrical pulses. LES relaxation and esophageal
body peristalsis were not effected. Furthermore, 2-3 sessions of 30 min daily may be sufficient to
sustain the increase in LESP seen [16]. Cardiac rhythm was not affected, nor did patients report
sensation of the stimulation (with exception of one patient at 15ma).
Small clinical trials have demonstrated improvement in esophageal pH (Figure 11) as well as
HRQL [17].
Conclusions A huge therapeutic gap exists in the treatment of GERD. Laparoscopic fundoplication as practiced
by most US and European surgeons (360 degree or >180 degree partial fundoplication) has been unable
to fill this gap due to multiple reasons; probably the most significant is the side effect profile that
includes difficulty belching, inability to vomit, uncomfortable bloating, diarrhea, excess flatulence.
(Watson and Jamieson and the Adelaide group have published very interesting studies on lesser degrees
of fundoplication). Currently no medication regimens have promise in filling “the gap”.
Currently three commercially available antireflux treatments have demonstrated significant
improvement in QOL, decrease in daily PPI use, and improved esophageal acid control; without the
side effects of laparoscopic fundoplication. Though results in terms of reflux control are not as good as
laparoscopic fundoplication, the near absence of side effects has made these treatments quite appealing
to many patients in “the gap”. Insurance coverage for these procedures is variable, but acceptance of
these procedures as viable, non-experimental treatment options is increasing.
References:
1. Saritas Yuksel E, Higginbotham T, Slaughter JC, Mabary J, Kavitt RT, Garrett CG, Vaezi MF (2012)
Use of direct, endoscopic-guided measurements of mucosal impedance in diagnosis of gastroesophageal
reflux disease. Clinical gastroenterology and hepatology : the official clinical practice journal of the
American Gastroenterological Association 10:1110-1116
2. Grabowski M, Kasran A, Seys S, Pauwels A, Medrala W, Dupont L, Panaszek B, Bullens D (2011)
Pepsin and bile acids in induced sputum of chronic cough patients. Respiratory medicine 105:1257-1261
3. Fass R (2007) Proton-pump inhibitor therapy in patients with gastro-oesophageal reflux disease: putative
mechanisms of failure. Drugs 67:1521-1530
4. Finks JF, Wei Y, Birkmeyer JD (2006) The rise and fall of antireflux surgery in the United States. Surg
Endosc 20:1698-1701

Emerging Technologies and Techniques in GERD
5. Perry KA, Banerjee A, Melvin WS (2012) Radiofrequency energy delivery to the lower esophageal
sphincter reduces esophageal acid exposure and improves GERD symptoms: a systematic review and
meta-analysis. Surg Laparosc Endosc Percutan Tech 22:283-288
6. Aziz AM, El-Khayat HR, Sadek A, Mattar SG, McNulty G, Kongkam P, Guda MF, Lehman GA (2010)
A prospective randomized trial of sham, single-dose Stretta, and double-dose Stretta for the treatment of
gastroesophageal reflux disease. Surg Endosc 24:818-825
7. Bell RC, Cadiere GB (2011) Transoral rotational esophagogastric fundoplication: technical, anatomical,
and safety considerations. Surg Endosc 25:2387-2399
8. Muls V, Eckardt AJ, Marchese M, Bastens B, Buset M, Deviere J, Louis H, Rajan A, Daniel MA,
Costamagna G (2012) Three-year Results of a Multicenter Prospective Study of Transoral Incisionless
Fundoplication. Surg Innov
9. Furnee EJ, Broeders JA, Draaisma WA, Schwartz MP, Hazebroek EJ, Smout AJ, van Rijn PJ, Broeders
IA (2010) Laparoscopic Nissen fundoplication after failed EsophyX fundoplication. Br J Surg 97:1051-
1055
10. Witteman BP, Kessing BF, Snijders G, Koek GH, Conchillo JM, Bouvy ND (2013) Revisional
laparoscopic antireflux surgery after unsuccessful endoscopic fundoplication. Surg Endosc
11. Ihde GM, Besancon K, Deljkich E (2011) Short-term safety and symptomatic outcomes of transoral
incisionless fundoplication with or without hiatal hernia repair in patients with chronic gastroesophageal
reflux disease. Am J Surg 202:740-746; discussion 746-747
12. Bell RC, Hufford RJ, Fearon J, Freeman KD (2012) Revision of failed traditional fundoplication using
EsophyX((R)) transoral fundoplication. Surg Endosc
13. Bonavina L, Saino GI, Bona D, Lipham J, Ganz RA, Dunn D, DeMeester T (2008) Magnetic
augmentation of the lower esophageal sphincter: results of a feasibility clinical trial. J Gastrointest Surg
12:2133-2140
14. Lipham JC, DeMeester TR, Ganz RA, Bonavina L, Saino G, Dunn DH, Fockens P, Bemelman W (2012)
The LINX(R) reflux management system: confirmed safety and efficacy now at 4 years. Surg Endosc
26:2944-2949
15. Bonavina L, DeMeester TR, Ganz RA (2012) LINX() Reflux Management System: magnetic sphincter
augmentation in the treatment of gastroesophageal reflux disease. Expert review of gastroenterology &
hepatology 6:667-674
16. Rodriguez L, Rodriguez P, Neto MG, Ayala JC, Saba J, Berel D, Conklin J, Soffer E (2012) Short-term
electrical stimulation of the lower esophageal sphincter increases sphincter pressure in patients with
gastroesophageal reflux disease. Neurogastroenterology and motility : the official journal of the
European Gastrointestinal Motility Society 24:446-450, e213
17. Rodriguez L, Rodriguez P, Gomez B, Ayala JC, Saba J, Perez-Castilla A, Galvao Neto M, Crowell MD
(2012) Electrical stimulation therapy of the lower esophageal sphincter is successful in treating GERD:
final results of open-label prospective trial. Surg Endosc









NOTES
Gastrointestinal Stromal Tumors
David W. Rattner, M.D Chief, Division of General and Gastrointestinal Surgery
Massachusetts General Hospital
The Warshaw Family Professor of Surgery, Harvard Medical School
Gastrointestinal Stromal Tumors (GIST) are one of the most common submucosal
lesions identified in the foregut. These tumors arise from the interstitial cells of
Cajal. Approximately 85% of tumors have c-kit mutations and 5% of tumors
have PDFGRA mutations. Although many of these tumors have a bland behavior,
all must be considered as potentially malignant. Tumors that have the c-kit
mutation respond to tyrosine kinase inhibitors such as Gleevac. Over the past two
decades the incidence of GIST tumors has doubled. This is in part due to the
greater use of diagnostic studies that detect these tumors incidentally. It is also
possible that for unknown reasons there truly is an increased incidence of GISTs
in the general population. 45% of GIST tumors are found incidentally either on
routine endoscopy or CT scans, 25% present with bleeding, about 20% are found
in patients complaining of abdominal pain, and 10% are found in the course of
other investigations.
GISTs can occur at any location in the GI tract. The most common site is
in the stomach. Gastric GIST tumors account for 60% of all GIST tumors. As a
rule of thumb, the more proximal in the GI tract that the GIST tumor occurs, the
better the prognosis. Of the gastric GIST’s, 40% occur in the body of the
stomach, 30% in the antrum, 20% in the fundus and 10% at the GE junction.
Surgical management for tumors in the central portion of the stomach is quite
straightforward, but resection of tumors at the GE junction or near the pyloris can
be technically challenging.
The differential diagnosis of a gastric submucosal mass includes GIST,
leiomyoma, schwannoma, and carcinoid tumors. Carcinoids can generally be
distinguished by their gross appearance. Lesions that are larger than 2 cm or those
that are enlarging on sequential imaging studies should probably be resected. In
borderline situations or in high risk surgical patients a biopsy may be useful and
provide information as to the nature of the tumor. However, an FNA biopsy
cannot always distinguish a GIST from a benign tumor such as a leiomyoma or
Schwannoma. In large tumors or in the setting of potential metastatic disease a
biopsy is very useful because neoadjuvant therapy is likely to be needed. For
GISTs that can be easily resected , no staging workup is necessary prior to
surgery. Once the tumor is resected it is relatively easy to assess the risk for
mestatasis and appropriate staging can be performed at that point in time. GIST
tumors that are exophytic, pendunculated , or are smaller than 5-6 cm are best

handled by a laparoscopic resection. For larger tumors the benefit of laparoscopic
resection is less clear cut. Small GIST’s have been resected successfully
endoscopically but it is important to remember that these are not mucoscal lesions
as they arise in th emuscularis layer and are frequently attached to the serosa.
Therefore one must be prepared to close a full thickness defect in the stomach
when attempting to resect a lesion endoscopically.
Special considerations for GIST resections in difficult locations:
Whereas GISTS in the body and fundus of the stomach can be easily
removed by a wedge resection of the gastric wall, other locations can present
technical challenges. When resecting GISTS arising on the lesser curvature
attention should me paid to preserving the nerves of Laterjet. If both the anterior
and posterior nerves are transected, the pylorus will be denervated and patients
may develop delayed gastric emptying.
GIST’s at the GE junction can be particularly challenging. There are two
good ways to approach these laparoscopically. In both techniques it is important
to protect the anterior vagus nerve. The most straightforward approach is to
sharply dissect out the GIST and then hand sew the defect closed. It is important
to make sure that the closure is air tight and that the esophageal lumen is not
narrowed. Addition of an anterior fundoplication- either a Thal Patch or Dor
Fundoplication may provide additional security. Another good technique for GE
Junction GISTs is a transgastric endoluminal resection. Transgastric laparscopic
trocars allow one to use a stapler for resecting the tumor endoluminally while a
gastroscope can be used for both visualization and retraction of the tumor. With
this technique the tumor can be extracted trans-orally if the tumor is 2 cm or less.
If one encounters a GIST that is 5 cm in size at the GE junction, there is a good
chance that it is malignant and it will be difficult to get adequate margins with a
local resection. In this setting one should consider performing an
esophagogastrectomy. Tumors in the antrum of the stomach often need a bit of
planning before resection. Attempting a simple wedge resection with a stapler can
narrow the pylorus and obstruct the gastric outlet. Therefore for pre-pyloric
lesions and for those in the distal anterim I prefer to excise them sharply in a
longitudinal fashion and then repair the defect with a hand sewn transverse
closure. No matter what approach is chosen one should always respect oncologic
principles and obtain a tissue margin of 1 cm. Lymph node dissection is not
necessary for GIST tumors since these tend to spread hematogenously.
When treating a locally advanced GIST Gleevac therapy can be extremely
helpful. If one can appreciate the tumor as locally advanced prior to surgery
neoadjuvant therapy is indicated. The maximum response is usually obtained
after six to nine months of treatment at this point surgical resection should be
undertaken.

Postoperatively one can assess the risk of recurrence and determine the need for
close follow up using the Sloan Kettering nomogram found at:
http://nomograms.mskcc.org/GastroIntestinal/GastroIntestinalStromalTumor
SELECTED REFERENCES:
Joensuu H. Vehtari A. Riihimaki J. et al. Risk of recurrence of gastrointestinal
stromal tumour after surgery: an analysis of pooled population-based cohorts.
Lancet Oncology. 13(3):265-74, 2012
Frankel TL. Chang AE. Wong SL. Surgical options for localized and advanced
gastrointestinal stromal tumors. Journal of Surgical Oncology. 104(8):882-7, 2011
Pisters PW. Patel SR. Gaastrointestinal Stromal Tumors: Current Management.
Journal of Surgical Oncology. 102(5):530-8, 2010
Gervaz P. Huber O. Morel P. Surgical management of gastrointestinal stromal
tumours. British Journal of Surgery. 96(6):567-78, 2009

NOTES

Laparoscopic Gastrectomy for Early Gastric Cancer
Han-Kwang Yang, MD, PhD, FACS
Department of Surgery and Cancer Research Institute,
Seoul National University College of Medicine, Seoul, Korea
Laparoscopic gastrectomy for gastric cancer (GC) is rapidly popularized, because of the technical
development and the accumulated data of laparoscopic surgery in GC patients. Laparoscopic distal
gastrectomy (LDG) provides better or comparable outcomes, compared to conventional open distal
gastrectomy (ODG) in terms of short-term results. The long-term survival of LDG is expected to be
comparable to that of ODG in early stage GC, and ongoing Korean muticenter RCT (KLASS-01) will
provide more clear evidence. Laparoscopic total gastrectomy is still selectively performed compared to
LDG, and there is still debate on safe laparoscopic esophago-jejunostomy technique. Laparoscopic
pylorus preserving gastrectomy seems to be preferred for EGC in the middle third of stomach, in terms
of functional advantages and comparable oncologic outcome.
Even greater caution is advised when considering the application of a laparoscopic approach for total
gastrectomy as the lymph node (LN) dissection and particularly the reconstruction for a laparoscopic
total gastrectomy (LTG) are technically more demanding compared to a LADG and an anastomotic
leakage more consequential. To address this issue, KLASS group has just commenced KLASS-03 study,
a phase II study, aimed at assessment of technical safety of various reconstructive techniques after total
gastrectomy.
A laparoscopic gastrectomy for cancer is a technically challenging procedure with a steep learning
curve reported to last around 50 cases. Gastrectomy requires a large extent of LN dissection, much of it
in the immediate vicinity of major blood vessels that need to be preserved. As such, many of intra-
operative pitfalls relate to injury to either major blood vessels or bleeding from their branches or
tributaries that impair vision and subsequently lead to other major complications. Other pitfalls relate to
thermal injury to adjacent organs, particularly to the transverse colon, pancreas, duodenum and
esophagus, and steps of reconstruction which is more difficult by the minimally invasive approach.
D2 dissection has long been the standard of care in Japan and Korea and survival advantage of D2
dissection over D1 dissection has only recently been shown using Western data for the first time. The
3rd English version of Japanese Gastric Cancer Treatment Guideline published in 2010 recommends a
D2 dissection for clinical T2-4b tumor or T1 tumor with suspicion of nodal involvement . Most gastric
surgeons in Japan and Korea accept modified D2 (or D1+) dissection as a safe alternative in cT1N0
disease. One should note that the extent of lymphadenectomy is now defined according to the type of
gastrectomy indicated and not the location of the lesion
Laparoscopic sentinel node navigation surgery is yet experimental, and surgical procedure is not
standardized until now. Robotic gastrectomy is feasible to EGC in terms of similar outcome and but
with much higher cost compared to laparoscopic surgery. Its benefit over the conventional laparoscopic
gastrectomy is not proven yet

Figure 1. Recommended treatment algorithm. (From Japanese Gastric Cancer Association.
Japanese gastric cancer treatment guidelines: 3rd
English edition, Gastric Cancer 14:113-123,
2011)

Distal gastrectomy D0 Lymphadenectomy less than D1
D1 Nos. 1, 3, 4sb, 4d, 5, 6, 7
D1+ D1+ Nos. 8a, 9
D2 D1 + Nos. 8a, 9, 11p, 12a.
Total gastrectomy D0 Lymphadenectomy less than D1
D1 Nos. 1-7
D1+ D1+ Nos. 8a, 9, 11p
D2 D1 + Nos. 8a, 9, 10, 11p, 11d, 12a
Figure 2. Extent of lymph node dissection in
distal and total gastrectomies. (From
Gastric Cancer Association. Japanese gastric
cancer treatment guidelines: 3
edition, Gastric Cancer 14:113-123, 2011
Lymphadenectomy less than D1
D1 + Nos. 8a, 9, 11p, 12a.
Lymphadenectomy less than D1
+ Nos. 8a, 9, 10, 11p, 11d, 12a
ymph node dissection in
(From Japanese
Japanese gastric
cancer treatment guidelines: 3rd
English
123, 2011)

Figure 3. Room set-up.
Figure 4. Port positions.
5mm 5mm 12mm 5cm mini- laparotomy 5mm 11mm camera port

References
Kitano S, Yang HK (eds): Laparoscopic gastrectomy for cancer - standard techniques and clinical
evidences. Tokyo, Springer, 2012.
Japanese Gastric Cancer Association: Japanese gastric cancer treatment guidelines 2010 (ver. 3).
Gastric Cancer 2011;14:113-123.
Japanese Gastric Cancer Association: Japanese classification of gastric carcinoma: 3rd English edition.
Gastric Cancer 2011;14:101-112.
Lee HJ, Shiraishi N, Kim HH, Hiki N, Uyama I, Choi SH, Yang HK, Kitano S: Standard of practice on
laparoscopic gastric cancer surgery in Korea and Japan: experts' survey. Asian J Endosc Surg 2012;5:5-
11.
Viñuela EF, Gonen M, Brennan MF, Coit DG, Strong VE: Laparoscopic versus open distal
gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials and high-quality
nonrandomized studies. Ann Surg 2012;255:446-456.
Kim HH, Hyung WJ, Cho GS, Kim MC, Han SU, Kim W, Ryu SW, Lee HJ, Song KY: Morbidity and
mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report-a
phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann Surg 2010;251:417-420.
Nakamura K, Katai H, Mizusawa J, Yoshikawa T, Ando M, Terashima M, Ito S, Takagi M, Takagane A,
Ninomiya M, Fukushima N, Sasako M: A Phase III Study of Laparoscopy-Assisted Versus Open Distal
Gastrectomy with Nodal Dissection for Clinical Stage IA/IB Gastric Cancer (JCOG0912). Jpn J Clin
Oncol DOI: 10.1093/jjco/hys220.
Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N; Japanese Laparoscopic Surgery Study
Group: A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in
Japan. Ann Surg 2007;245:68-72.
Strong VE, Devaud N, Allen PJ, Gonen M, Brennan MF, Coit D: Laparoscopic versus open subtotal
gastrectomy for adenocarcinoma: a case-control study. Ann Surg Oncol 2009;16:1507-1513.
Kodera Y, Fujiwara M, Ohashi N, Nakayama G, Koike M, Morita S, Nakao A: Laparoscopic surgery
for gastric cancer: a collective review with meta-analysis of randomized trials. J Am Coll Surg
2010;211:677-686.
Park DJ, Lee HJ, Jung HC, Kim WH, Lee KU, Yang HK: Clinical outcome of pylorus-preserving
gastrectomy in gastric cancer in comparison with conventional distal gastrectomy with Billroth I
anastomosis. World J Surg 2008;32:1029-1036.
Jiang X, Hiki N, Nunobe S, Fukunaga T, Kumagai K, Nohara K, Sano T, Yamaguchi T: Postoperative
outcomes and complications after laparoscopy-assisted pylorus-preserving gastrectomy for early
gastric cancer. Ann Surg 2011;253:928-933.
Suh YS, Han DS, Kong SH, Kwon S, Shin CI, Kim WH, Kim HH, Lee HJ, Yang HK: Laparoscopy-
assisted pylorus-preserving gastrectomy is better than laparoscopy-assisted distal gastrectomy for
middle-third early gastric cancer. Ann Surg (in press)
Yang HK: Sentinel node biopsy in early gastric cancer: constant exertion for clinical application. Ann
Surg Oncol 2012;19:353-354.
Wall J, Marescaux J: Robotic gastrectomy is safe and feasible, but real benefits remain elusive. Arch
Surg 2011;146:1092.

NOTES

Submucosal Tumors
Presenter: Sricharan Chalikonda, MD
Disclosures:
I have relationships to disclose 1/30/2013 10:44:12 AM intuitive surgical Honoraria Independent Potential Conflict of Interest Contractor
Conflict Management:Does Not Relate

NOTES

Christy M. Dunst, MD
Esophageal Surgeon
The Oregon Clinic
4805 SE Glisan St #6N60
Portland, Oregon 97213
503-281-0561
503-281-0575 (fax)
POSTGRADUATE COURSE: Foregut-Beyond GERD & Hiatal Hernia
4/17/2013 7:30am-12pm
Esophageal Diverticulae and Achalasia
There has been a recent revival in the interest in esophageal motility disorders primarily
due to the popularization of high resolution manometry (HRM) and the emergence of
new endoscopic therapies for esophageal diseases. HRM has beautifully enabled
esophagologists to more easily recognize and precisely characterize a multitude of
esophageal motor disorders including achalasia. Tried and true therapies such as
esophageal myotomy and endoscopic balloon dilation provide successful relief of
dysphagia for ~90% of patients with achalasia.
Per-oral esophageal myotomy (POEM) has emerged as a potential alternative to
esophageal myotomy in the treatment of spastic disorders such as achalasia, diffuse
esophageal spasm and nutcracker esophagus with poorly relaxing lower esophageal
sphincters. In brief, the POEM technique consists of 5 steps: 1) Diagnostic endoscopy
and measurements of landmarks 2) Mucosotomy 3) Creation of sub-mucosal tunnel 4)
Myotomy of the circular muscle fibers 5) Mucosotomy closure. Early results are
encouraging with excellent relief of dysphagia and virtually no postoperative pain.
Although no randomized trials have been done, retrospective comparisons to Heller
myotomy show the two therapies have similar outcomes.
As esophageal motility disorders are becoming easier to characterize and excitement
continues to grow regarding the application of POEM, the diagnosis of associated
problems such as esophageal diverticulae may also increase. Understanding the current
management strategies in this field is imperative. Esophageal diverticulae are defined as
simply outpouchings of the esophageal wall. Epiphrenic diverticulum(ED) is a rare
condition defined as a mucosal outpouching in the mid or distal esophagus as a result of
a weakening in the esophageal wall against an esophageal outflow obstruction. Most
commonly, the obstruction results from an underlying esophageal motor disturbance
but can also be seen with problems such as aggressive hiatal hernioraphy and/or
fundoplication. Esophageal diverticulae can also be the result of external traction due to

adherence of the esophageal wall to other mediastinal structures such as can be seen in
tuberculosis. As the pathogenesis of these two types of esophageal diverticulae are
quite distinct, correct diagnosis is important proper treatment.
Epiphrenic diverticulae can be confused clinically, and even sometimes radiographically,
with paraesophageal hernias. Common symptoms may include dysphagia, chest pain,
regurgitation and aspiration among others. As with paraesophageal hernias, the
presence of attributable symptoms dictates the need for surgical intervention. However
the surgical therapy is, of course, quite different making precise preoperative diagnosis
imperative for appropriate operative planning. Comprehensive esophageal testing
includes esophageal manometry, esophageal contrast radiography and endoscopy with
biopsy. The importance of the contrast study cannot be overemphasized as diverticulae
are frequently missed with endoscopy alone and it will more precisely identify the
location of the diverticulum relative to other mediastinal structures.
Most epiphrenic diverticulae can be resected laparoscopically but a combined
laparoscopic thoracoscopic approach can be helpful for diverticulae located above the
pulmonary hilum. An exception might be those diverticulae associated with a hiatal
hernia in which case the diverticulum becomes approachable after reduction of the
hernia. Although some minor controversy over details exists, the technique can
generally be summarized into the following steps: 1) Mobilization of the esophagus and
dissection of the diverticulum 2) Stapled esophageal diverticulectomy 3) Esophageal
myotomy 4) Partial fundoplication.
Epiphrenic diverticulectomy is associated with a relatively high complication rate (~20%)
most commonly from esophageal leak at the suture line. The most important step to
mitigate suture line failure is correct identification of the mucosal neck of the
diverticulum. Liberal use of intraoperative endoscopy is encouraged as it greatly
enhances visibility of the diverticular borders and can assist stapler positioning to avoid
incomplete resection.
Generally, the presence of an esophageal diverticulum is a contraindication to POEM,
especially early in ones learning curve. It would be unusual to encounter a clinical
scenario in which only the myotomy was indicated. Therefore, since the
diverticulectomy necessitates laparoscopy +/- thoracoscopy, standard myotomy is the
preferred approach. However, we have performed a combination POEM and
laparoscopic diverticulectomy for a specific situation involving extensive diffuse
esophageal spasm. Endoscopic diverticulectomy may one day be a possible adjunct to
POEM.

REFERENCES:
1. Hungness ES, Teitelbaum EN, Santos BF, Arafat FO, Pandolfino JE, Kahrilas PJ, Soper NJ.
Comparison of Perioperative Outcomes Between Peroral Esophageal Myotomy (POEM) and
Laparoscopic Heller Myotomy. J Gastrointest Surg. 2013 Feb;17(2):228-35. Epub 2012 Sep 28.
2. Hirano Y, Takeuchi H, Oyama T, Saikawa Y, Niihara M, Sako H, Omagari K, Nishi T, Suzuki H, Hibi T,
Kitagawa Y Minimally invasive surgery for esophageal epiphrenic diverticulum: the results of 133
patients in 25 published series and our experience Surg Today. 2013 Jan;43(1):1-7. Epub 2012
Oct 21.
3. Zaninotto G, Parise P, Salvador R, Costantini M, Zanatta L, Rella A, Ancona E Laparoscopic repair
of epiphrenic diverticulum Semin Thorac Cardiovasc Surg. 2012 Autumn;24(3):218-22.
4. Swanstrom LL, Kurian A, Dunst CM, Sharata A, Bhayani N, Rieder E Long-term outcomes of an
endoscopic myotomy for achalasia: the POEM procedure. Ann Surg. 2012 Oct;256(4):659-67. doi:
10.1097/SLA.0b013e31826b5212.
5. Boeckxstaens GE, Annese V, des Varannes SB, Chaussade S, Costantini M, Cuttitta A, Elizalde JI,
Fumagalli U, Gaudric M, Rohof WO, Smout AJ, Tack J, Zwinderman AH, Zaninotto G, Busch OR;
European Achalasia Trial Investigators Pneumatic dilation versus laparoscopic Heller's myotomy
for idiopathic achalasia. N Engl J Med. 2011 May 12;364(19):1807-16.
6. Inoue H, Minami H, Kobayashi Y, Sato Y, Kaga M, Suzuki M, Satodate H, Odaka N, Itoh H, Kudo S.
Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010 Apr;42(4):265-
71.
7. Zaninotto G, Portale G, Costantini M, Merigliano S, Guirroli E, Rizzetto C, Rampado S, Ancona E.
Long-term outcome of operated and unoperated epiphrenic diverticula. J Gastrointest Surg. 2008
Sep;12(9):1485-90
8. Zaninotto G, Costantini M, Rizzetto C, Zanatta L, Guirroli E, Portale G, Nicoletti L, Cavallin F,
Battaglia G, Ruol A, Ancona E Four hundred laparoscopic myotomies for esophageal achalasia: a
single centre experience. Ann Surg. 2008 Dec;248(6):986-93.
NOTES

MIS IN ESOPHAGEAL NEOPLASMS
GUY-BERNARD CADIERE MD, PhD
PROFESSOR OF SURGERY
CHIEF OF DEPARTMENT OF GASTROINTESTINAL SURGERY
DIRECTOR OF EUROPEAN SCHOOL OF LAPAROSCOPIC SURGERY
DIRECTOR OF BRUSSELS WEIGHT LOSS CENTER
SAINT-PIERRE UNIVERSITY HOSPITAL, BRUSSELS, BELGIUM
GIOVANNI DAPRI MD, FACS
ASS. PROF. DEPARTMENT OF GASTROINTESTINAL SURGERY
EUROPEAN SCHOOL OF LAPAROSCOPIC SURGERY
SAINT-PIERRE UNIVERSITY HOSPITAL, BRUSSELS, BELGIUM

MIS IN ESOPHAGEAL NEOPLASMS Surgical resection is considered standard treatment for patient with resectable esophageal cancer. Surgery for esophageal cancer should be aimed at achieving on Ro resection. Extensive two-field lymphadenetomy should be standard during esophagectomy. Minimal invasive esophagectomy by thoracoscopy, laparoscopy and or without cervicotomy has better outcomes than by open surgery. 2 techniques are described: esophagectomy by laparoscopy, cervicotomy and thoracoscopy and esophagectomy by laparoscopy and thoracoscopy (Ivor Lewis technique).
1. Esophagectomy by thoracoscopy, laparoscopy and cervicotomy
Minimally invasive esophagectomy access for cancer includes three steps: thoracoscopy in prone position for the mobilisation of the thoracic esophagus and mediastinal lymphadenectomy, laparoscopy in supine position for the celiac trunk lymphadenectomy and gastric tube manufacturing and left cervicotomy for the esophago-gastric anastomosis.
1.1. Thoracoscopy in prone position
1.1.1. Position of the patient and disposition of the trocars
The patient is placed in prone position after induction of general anesthesia and insertion of double-lumen endotracheal tube. The surgeon stands at the right side of the patient. Three trocars are required for the procedure. A 10 mm trocar for the 30 degree angled optical system in the 7
th
intercostals space, a second 5 mm trocar in the 9th intercostals space for the grasping forceps, and a third 5 mm
trocar in the 5th intercostals space for the coagulating hook.
1.1.2. Mobilisation of the intrathoracic esophagus and mediastinal lymphadenectomy
Thanks to gravity, the cardio-pulmonary window drops back and the space of dissection is directly opened. The mediastinal pleura overlying the esophagus is incised and the esophagus is circumferentially mobilizes along the trachea, the descending aorta, reaching the right diaphragmatic pillar. All fatty tissue is separated from the pericardium and descending aorta. The arch of the azygos vein is isolated, ligated by 2/0 silk stitches with clips, and divides. Para esophageal, paratracheal, subcarinal, bilateral tracheobronchial, right pulmonary artery, and veins lymph nodes are dissected so as to remain in block with the surgical specimen. A 28 French chest tube is inserted in the 11
th intercostals space on the anterior axillary line at the end of this step.
1.2. Laparoscopy
1.2.1. Position of the patient and disposition of trocars

The patient is placed in supine position with legs separated. The surgeon stands between the patient’s legs.Five trocars are used: a 10 mm trocar 2 cm above the umbilicus, a 5 mm trocar on the midleft costal margin, a 12 mm trocar half-way between the first two trocars, a 12 mm trocar on the right midunder the xyphoid process.
1.2.2. Mobilisation of the greater curvature and celiac trunk lymphadenectomy
The dissection of the lesser omentum starts to the The dissection of the gastrocolic ligament and thus opening of the lesser sac is carried out just lateral to the right gastroepiploic artery and vein. All lymphoglandulartowards the right is sampled, while preserving the left gastric artery and the hepatic pedicule.Dissection of all lymphoglandular tissue is completed along the abdominal aorta until diaphragmatic reached.
1.2.3. Gastric tube and intramediastinal dissection
The initial firing of the stapler begins at the level of the crow’s foot, perpendicular to the lesser curvature. Other firings are placed parallel to the greater curvature. The limits of the mediastinal dissection are the following: anteriorly, the pericardium and the left inferior pulmonary vein; on the left side, the left pleura; on the right side, the right pleura; posteriorly, the aorta.
1.3. Left cervicotomy
1.3.1. Position of patient
An incision is performed lateral to the left sternoLifting the esophagus containing the tumoral mass (protected by a plastic bag) is achieved under laparoscopic control. A totally mechanical side-to-side esophagosame stapler used for the gastric tube.
patient is placed in supine position with legs separated. The surgeon stands between the patient’s legs.Five trocars are used: a 10 mm trocar 2 cm above the umbilicus, a 5 mm trocar on the mid-clavicular line under the
way between the first two trocars, a 12 mm trocar on the right mid
1.2.2. Mobilisation of the greater curvature and celiac trunk lymphadenectomy
The dissection of the lesser omentum starts to the left of the left gastric artery. The dissection of the gastrocolic ligament and thus opening of the lesser sac is carried out just lateral to the right
artery and vein. All lymphoglandular tissue around the celiac trunk is removed from this point is sampled, while preserving the left gastric artery and the hepatic pedicule.
Dissection of all lymphoglandular tissue is completed along the abdominal aorta until diaphragmatic
tube and intramediastinal dissection
The initial firing of the stapler begins at the level of the crow’s foot, perpendicular to the lesser curvature. Other firings are placed parallel to the greater curvature. The limits of the mediastinal dissection are the following:
dium and the left inferior pulmonary vein; on the left side, the left pleura; on the right side, the
An incision is performed lateral to the left sterno-cleido-mastoid muscle. Lifting the esophagus containing the tumoral mass (protected by a plastic bag) is achieved under laparoscopic
side esophago-gastric anastomosis is performed using three firings of the
patient is placed in supine position with legs separated. The surgeon stands between the patient’s legs. clavicular line under the
way between the first two trocars, a 12 mm trocar on the right mid-clavicular
The dissection of the gastrocolic ligament and thus opening of the lesser sac is carried out just lateral to the right tissue around the celiac trunk is removed from this point
Dissection of all lymphoglandular tissue is completed along the abdominal aorta until diaphragmatic pillars are
The initial firing of the stapler begins at the level of the crow’s foot, perpendicular to the lesser curvature. Other firings are placed parallel to the greater curvature. The limits of the mediastinal dissection are the following:
dium and the left inferior pulmonary vein; on the left side, the left pleura; on the right side, the
Lifting the esophagus containing the tumoral mass (protected by a plastic bag) is achieved under laparoscopic gastric anastomosis is performed using three firings of the

2. Esophagectomy by laparoscopy and thoracoscopy (Ivor Lewis technique)
2.1. Laparoscopy (Cf. 1.2.) Comparing the technique by 3 ways, the stomach is introduced in the chest.
2.2. Thoracoscopy in prone position
The esophagus was sectioned approximately 4 cm proximal to the tumor, approximately 1 cm cranial to the azygos. The specimen was placed in a plastic bag and was alldeployed in the pleural cavity until the tip is
2.2.1 Esogastric suture
The anterior side of the gastric tube was sutured manually in two layers siderunning sutures: Maxon 4/0 internally and PDS 2/0 externally. The apex of the gastric tube was sutured to the esophagus and to the parietal pleura by a couple of silk 2/0 A nasogastric tube was left in place across the anastomosis; A 28 French chest tube wacostodiaphragmatic sinus and placed under 20 cm water seal.
sophagectomy by laparoscopy and thoracoscopy (Ivor Lewis technique)
technique by 3 ways, the stomach is entirely sectioned and stapled and the gastric tube is partially
2.2. Thoracoscopy in prone position (Cf. 1.1.)
The esophagus was sectioned approximately 4 cm proximal to the tumor, approximately 1 cm cranial to the azygos. The specimen was placed in a plastic bag and was allowed to drop inside the abdomendeployed in the pleural cavity until the tip is facing the proximal esophagus.
The anterior side of the gastric tube was sutured manually in two layers side-to-end to the esophagus, by two ures: Maxon 4/0 internally and PDS 2/0 externally. The apex of the gastric tube was sutured to the
esophagus and to the parietal pleura by a couple of silk 2/0 stitches. A nasogastric tube was left in place across the anastomosis; A 28 French chest tube was left into the right costodiaphragmatic sinus and placed under 20 cm water seal.
sectioned and stapled and the gastric tube is partially
The esophagus was sectioned approximately 4 cm proximal to the tumor, approximately 1 cm cranial to the owed to drop inside the abdomen. The gastric tube is
end to the esophagus, by two ures: Maxon 4/0 internally and PDS 2/0 externally. The apex of the gastric tube was sutured to the
s left into the right

NOTES