serum betamethasone therapy to prevent respiratory distress syndrome
TRANSCRIPT

Glucocorticoid Levels in Maternal and Cord
Serum after Prenatal Betamethasone Therapy to
Prevent Respiratory Distress Syndrome
PHiLIp L. BALLARD, PATRICIA GRANBERG,and ROBERTAA. BALLARD
From the Cardiovasctular Research Institute and Department of Pediatrics,University of California, San Francisco, California 94143, and the Departmentof Pediatrics, Mlount Zion Hospital, San Francicso, California 94120
A B S T R A C T Serumii glucocorticoid levels were (le-termined in 20 inothers andI 43 premature infalnts wh-lior-eceived prenatal betamnetlhasonie therapy for preventionlof respiratory distress syndrome (RDS). 'Maternal beta-methasone peaked at 75 ,ug cortisol equivalents per 100ml 1 h after injection of 12 mg steroid and declinedto half by 6 h. Betamethasone in cord blood w-as 14.3 tigcortisol equivalents per 100 ml at 1 h, decreased to alevel of 4.7 at 20 h, aand was not detected 2 days aftera second dose at 24 h. After the second dose, the meanlevel of cortisol in cord blood was 5.9 yg per 100 mlcompared witlh 13.05 y- per 100 ml (P < 0.001) in un-treated premature infanits. The unbound glucocorticoidactivity in treated infants delivered 1-10 h after thesecond dose (mean, 8.4 Ag per 100 nil) is simlilar tothe unbound cortisol level after birth in untreated pre-mature infants who develop RDS.
These findings indicate that (a) serlum glucocorticoidlevels in the physiologic stress range can induce lungmnaturationi in the human aind (b) antenatal treatmentwith this dose of betaimietlhasoine does not expose thelhuman fetuis to potentially hiarm iftil pharmacologic levelsof steroid.
INTRODUCTIONAdmiiinistration of glucocorticoids to fetal animilals ofseveral species accelerates lung development and causesprecocious appearance of alveolar surfactaint (3-5).
Portions of this work were submitted for the meetingsof the Western Society for Pediatric Researclh, Carmel,Calif., February 1975 (1), and the Society for PediatricResearclh, Denver, Colo., April 1975 (2).
Rccived for puZblicationi 10 Juniie 19/75 anid in rvi.sed form20 Autgust 1915.
Since a deficiency of surfactant is the major causse of
resl)iratory distress svnldrome ( S) ' ill premlltluehuman illfatn,ts, these tifi(lilln s SUg'gested that -lticocorti-coids imliglht benefit the human infanit at risk for this(lisease. Recently, Liggins and Hox-ie (6, 7) reporteda significantly lower incideince of RDS in preimlatureii fanits wh-lose mothers were treated w-itlh betamiiethasoniefor at least 24 h before deliverv. In a simiillar studv,Fargier et al. (8) also noted a beneficial effect of pre-natal betamiietlhasoine therapy. These stuclies have indi-cated the effectiveness of prenatal glucocorticoidl treat-ment for prevention of RDS, aild it seellms likely thatsuclh therapy ws1ill comiie into general use in the future.
At present, however, little is knownNIl regai-dinlg thelevel of glucocorticoidl require(l to ilndtuce lun-g imiatura-tionl in lhlumanc infantcs. Also, tlher-e is little iinformiiationlconicerninig the safety of prenat,al corticosteroid ad-ministration. It does appear that the lunlg is a gluco-corticoid target tissue sinice both animal (9, 10) andlhumiani ('11) fetal luIg contain specific receptors forglucocorticoids. These bindin- proteins are saturated byphysiolog,ic levels of corticosteroidls, suggesting that the(lesire(d nmaturational effects slhould he accomplishedwithout the use of pharmacologic doses of steroid. Thisis anlnil)ortant conlsi(leratioln silnce it is knlowII thatlarge (loses of corticosteroids inhibit growvth in manyorgans of fetal ancd neoinatal aninlds (12-18).
In the presenlt studlv, we have (letermiiniedl serumii levelsof glucocorticoid activity in the hulmialn mother and fetusat various timles after prelnatal treatmiielnt itlh beta-methasonie to prevent RDS. The findings are discussedin relationislhip to tlle safety of this therapy anid in r e-
'Abbreviations utsed in this papcr: CBG, corticosteroid-binding globulin (transcortin); PROM, prolonged ruptureof mzemiibranles; RDS, respiratory (listress syndrome.
Thle Jouarnlal of Clitnica(l nveastigation Vohiiiie 56 Decemiiber 1975 1548-17551];-)-Is

gard to the mechanismii of actioIn of glucocorticoids in]Iliug (levelol)ment.
METHODSTrt atmedt of patienits. XVotnen admitted in premature
labor to Motiunt Zion Ilospital, San Franicisco, anid to theU!iiiversity of Califorinia, San Franicisco, weire treated ac-cordinig to the protocol of Ligginis anid Howie (6) with ani.m. administration of a mixture of 6 mg betamethasonephosphate and 6 mg betametlhasone acetate (Celestone Solus-pan, Schering Corporation, Kenilworth, N. J.). An in-formed consent wvas obtained before treatment. Labor wasdelayed in most cases by intravenous alcohol and, whleneverpossible, a second dose of betamethasone was administered24 h after the first. Samples of maternal venous blood wereobtained before and at various times after treatment, andmixed cord bloods were collected when delivery occurredwithin 4 days after the first dose. Additional cord bloodspecimens were obtained from premature infants deliveredat the National Women's Hospital, Auckland, New Zea-land, to women who had received either the same beta-methasone therapy or a placebo (6).2 Serum was separatedby centrifugation within 48 h from both maternal and cordsamples and stored at - 700C.
Infant gestational age was assessed by obstetrical dataand by physical and neurologic development. Statisticalsignificance was evaluated by Student's unpaired t test andby the method of least squares.
Steroid assays. The glucocorticoid radioreceptor assaywas performed as previously described (19). In brief, dupli-cate aliquots of 0.05-0.1 ml of scra were extracted twicewvith 10 vol of absolute ethanol. The extract was broughtto dryness under a gentle stream of air, and the residuewas dissolved in 0.1 ml of buiffer. Before ethanol extrac-tion cord serum samples were washed twice with 10 volof petroleum ether (20), which removes 90-93% of theprogesterone. The *extracted steroids were incubated at 2°Cfor 18 h with [3H]dexamethasone and cytosol (which con-tains glucocorticoid receptor activity) of cultured hepatomacells. Unbound [3H] dexamethasone and receptor-boundsteroid were separated by the charcoal absorption technique.The amount of glucocorticoid activity in the sample wasdetermined by comparison with plasma standards containingknown amounts of cortisol.
In order to determine the amount of glucocorticoid ac-tivity that was due to betamethasone, serum corticoids werealso assayed in the ethanol extracts of each sample by thecorticosteroid-binding globulin (CBG)-isotope method ofMurphy (20) and the charcoal absorption technique (19).This assay does not detect betamethasone. Appropriate con-trol sera (vithout synthetic corticosteroids) were includedin each experiment to establish the correlation between re-sults in the two assays. The level of betamethasone wasthen determined by the amount of excess activity found byradioreceptor assay as compared with the CBG-isotope as-say. Serum concentrations are expressed as cortisol equiva-lents and reflect the relative affinity of betamethasone forglucocorticoid receptors. Values may be converted to micro-grams betamethasone per 100 ml by dividing by 7.1 (19).The assay under these conditions is sensitive to a level of2 ,ug cortisol equivalents per 100 ml.
The percentage of serum cortisol bound to transcortinwas determined in undiluted sera by a modification of the
2We thank G. C. Liggins and R. N. Howie for providingthese samples.
it BtAME IIASOtJI(±neon± SEM)
X CORTISOLf imean t SFM)
E00
0.
A
z4uc
aLLA
0-T1
Z:0
(1)
Hours After First Dose of Betamethasone
io (4)
J-4J
45-52 HoursAfter Second Dose
FIGURE 1 Betamethasone and cortisol levels in maternalserum. The number of samples at each time point is shownin parentheses.
absorption method of Trapp and West (21) with a traceramount of [3H]cortisol and absorption by activated char-coal as previously described (19). This method measuresbinding to transcortin (but not to albumin) and providesresults similar to those found by ultrafiltration and equilib-rium dialysis at 37 C.3 Transcortin binding was assessedin pooled cord serum samples from premature infants afteraddition of various amounts of unlabeled cortisol. Trans-cortin capacity in these and other samples was calculatedfrom the amount of binding at a cortisol level of 50 ,Ag per100 ml (21). The amount of unbound cortisol and cortisolbound to albumin was estimated (22) from these data byusing published values for cord blood albumin levels inpremature infants with and without RDS (23).
RESULTSMatcrnal steroid levels. Determiiinations of betameth-
asone and cortisol levels were carried out on 37 samplesof blood from 20 women 0-12 h after the first dose ofsteroid. Four additional samples were obtained 45-52 hafter a second dose (Fig. 1). The level of betamethasoneis maximal (755 j.g cortisol equivalents per 100 ml) at1 h and then declines to half of this value at about 6 h;little activity remained in the maternal circulation 2 daysafter the second injection. Cortisol levels begin to de-crease within 2 h of the administration of exogenouscorticosteroid and reach a level of 5 ug per 100 mg mlat 12 h. During the 2nd day of treatment, cortisol wasbelow 5 Ag per 100 ml in four of five patients (data notshown). 2 days after the second injection, the meanlevel of cortisol in five women at delivery was withinthe normal range.
Betamiiethasone levels in cord blood. Steroid levelswere measured in samples of cord blood from 43 pre-mature infants exposed to betamethasone in utero. Cordbloods from another group of 22 infants who weredelivered at comparable times after treatment with a
3 P. Ballard. Data to be published.
Glucocorticoid Levels after Prenatal Betamethasone 1549

placebo (6) served as conassay and for comparison ofin both groups were delivercous labor except for one trlivered by cesarean section.and birth weight, sex distprolonged rupture of membrein the two groups (Table I).
Individual cord blood betaon a time scale in Fig. 2.as 1 h after the first dose.meani level of betamethasonelents per 100 ml at 1 h an- 0.50±0.16 (SD) (P < 0.at 20 h. Somewhat higher1 and 10 h after the seconthese samples was 15.0 sAgml compared with 12.0 msgtime period after the firstthat the three samples withmethasone (29.6, 32.8, andper 100 ml) were from the twith moderate or severe antmethasone was not detecte(cord blood obtained from fiand 72 h after the first dose.
Cortisol levels in cord blctreated and control infantsValues are significantly supfants born after betamethasfor treated infants were 7.after the first and secondspectively. Both values arc
0.001) than the means for13.05 ug per 100 ml). Cortis'4.95 /eg per 100 ml) in the fthe 3rd day after treatment.
istDOSE
E 30
0
o A
_-200 0
o A-
E v-aID
co
)-0
u
re
0
See-S t
C
0 0 -
8 16
Hours After F
FIGURE 2 Betamethasone levture infants. Individual data
trols in the betamethasonef cortisol levels. All infantsed vaginally after spontane--eated infant, who was de-The mean gestational age
;ribution, and incidence ofanes (PROM) were similar
methasone results are shownSteroid is detected as earlyBy regression analysis the
is 14.3 Ag cortisol equiva-id declines with a slope of.01) to 4.7 Ag per 100 nlvalues were found betweenrA r]nQ, - thi. mi-ntn 1P\xP,l fnr
TABLE ICharacteristics of Premature Infant Groups Treated with
Betamethasone or Placebo*
Betamethasone Placebo
Number 43 22Gestational age,: wk 32.7 40.40 32.74±0.60
(27-36.5) (26.5-36)Birth wt,$ g 1,8404-82 1,9874±115
(500-2,680) (800-2,880)Male:female 26:17 11:11PROM(>24 h) 12,'43 (28%) 4 /22 (18%/)
* Includes data provided by G. C. Liggins and R. N. Howie.t Values are mean4SEMand range.
U UU;zV L11t lllCali 1Vt: IVt ILI ' .~ Comptparison of maternal and fetal steroid levels. Acortisol equivalents per 100 comparison of the data in Figs. 1 and 2 suggests that
per 100 ml for the samefetal levels of betamethasone are lower than maternal
injection. It is of interestlevels during at least the first 12 h of treatment. Higher
the highest levels of beta-maternal levels were found in each of six matched
23.6 ug cortisol equivalents maternal and cord blood samples which were obtainedthree infants born to womenBenwet at various intervals (1-61 h) after the first dose of(epartum hemorrhage. betamethasone (Table II). The mean gradient was 3: 1
1 (< 2 Ag per 100 ml) in with a range from 1.6: 1 to 4.1: 1.ye infants born between 62 w
Maternal: fetal gradients also were present for corti-sol (mean, 5.8: 1), and in most cases these were some-
,od. Cortisol levels for the what greater than for betamethasone (Table II). In
aprespresedinmostated inF. one instance (case 7), the fetal sample was collected
pressedainemostAtreatedlin- from the umbilical artery 2 h after birth, when the in-45 ad 5t9 un Mean100vl fant had already developed mild RDS. Cortisol was
4do 5.
ofb gta perhas100, rel elevated in this infant (22.4 jug per 100 ml) compareddosegnofibetamethlone, re- with cord values of other infants delivered after a
signtroinfiantly lower5 (P similar treatment interval (cf. Fig. 3). In four othercontrol infants (14.65 and premature newborn infants with mild or moderate RDS
ol remains depressed (mean, delivered 52, 68, 82, and 95 h after the first dose offive samples obtained during betamethasone, cortisol levels at 13-24 h of life were
28.9, 11.4, 19.0, and 29.9 ALg per 100 ml.Unboutnd glucocorticoid levels in cord blood. The
data presented thus far have described the total amountDOSE of plasma glucocorticoid activity. Since it is generally
felt that unbound glucocorticoid and perhaps albumin-bound steroid are the physiologically active fractions,we determined the amounts of transcortin-bound and
v non-transcortin-bound steroid in cord bloods. In agree-* ment with earlier reports (24) we found that the bind-
* * ing capacity is lower in cord than in adult blood. Thev*.* transcortin capacities of pooled control and treated cord
? * U bloods from the premature infants were 8.3 and 9.6 iAgcortisol per 100 ml, respectively, compared with meanvalues of 10.8±1.1 (SEM) iAg per 100 ml (n=7) in
24 32 2 term infant cord bloods and 20.3±+1.7 lAg per 100 ml:irst Dose of Betomethosone (n = 10) in adult samples. At cortisol levels of 5.9, 10.5,
rels in cord bloods of prema- 16.2, and 22.1 iAg per 100 ml in premature infant cordfor 43 infants are shown. serum, the percentage of steroid not bound to trans-
1550 P. L. Ballard, P. Granberg, and R. A. Ballard
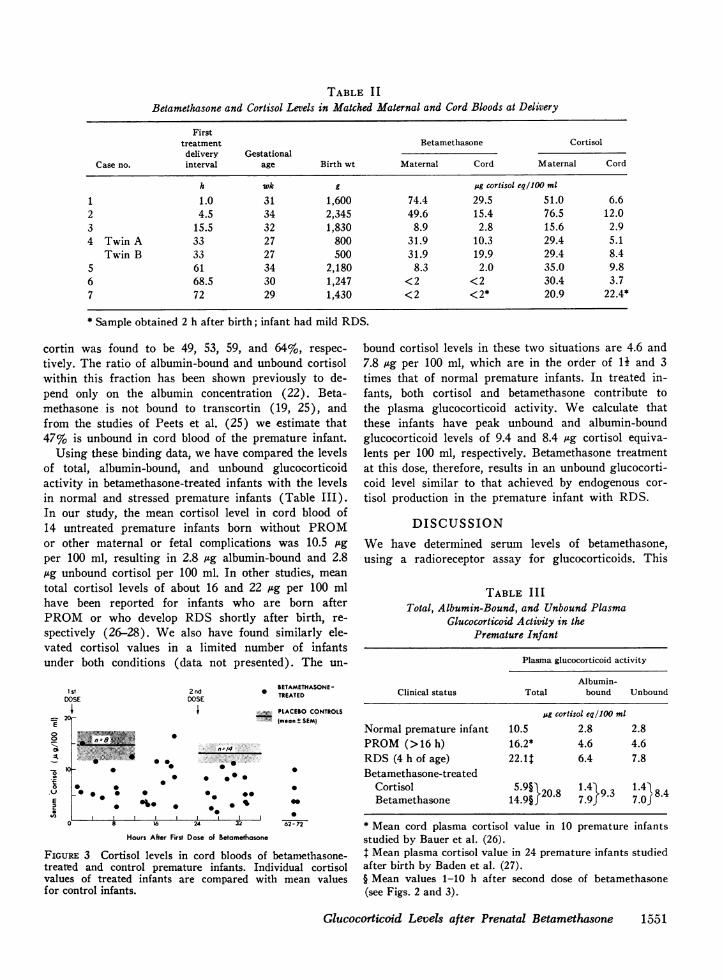
TABLE I IBetamethasone and Cortisol Levels in Matched Maternal and Cord Bloods at Delivery
Firsttreatment Betamethasone Cortisol
delivery GestationalCase no. interval age Birth wt Maternal Cord Maternal Cord
h wk g jg cortisol eq/100 ml
1 1.0 31 1,600 74.4 29.5 51.0 6.62 4.5 34 2,345 49.6 15.4 76.5 12.03 15.5 32 1,830 8.9 2.8 15.6 2.94 Twin A 33 27 800 31.9 10.3 29.4 5.1
Twin B 33 27 500 31.9 19.9 29.4 8.45 61 34 2,180 8.3 2.0 35.0 9.86 68.5 30 1,247 <2 <2 30.4 3.77 72 29 1,430 <2 <2* 20.9 22.4*
* Sample obtained 2 h after birth; infant had mild RDS.
cortin was found to be 49, 53, 59, and 64%, respec-tively. The ratio of albumin-bound and unbound cortisolwithin this fraction has been shown previously to de-pend only on the albumin concentration (22). Beta-methasone is not bound to transcortin (19, 25), andfrom the studies of Peets et al. (25) we estimate that47% is unbound in cord blood of the premature infant.
Using these binding data, we have compared the levelsof total, albumin-bound, and unbound glucocorticoidactivity in betamethasone-treated infants with the levelsin normal and stressed premature infants (Table III).In our study, the mean cortisol level in cord blood of14 untreated premature infants born without PROMor other maternal or fetal complications was 10.5 Agper 100 ml, resulting in 2.8 Ag albumin-bound and 2.8Ag unbound cortisol per 100 ml. In other studies, meantotal cortisol levels of about 16 and 22 ,ug per 100 mlhave been reported for infants who are born afterPROMor who develop RDS shortly after birth, re-spectively (26-28). We also have found similarly ele-vated cortisol values in a limited number of infantsunder both conditions (data not presented). The un-
I stDOSE
c xCE0
0
r-
0t
2ndDOSE
_ * 00
Ob4
RBETAMETHASONE-TREATED
-;.. PLACEBOCONTROLS(mean t SEM)
* - 22 2.0w* 0 .-0-0
0- 00>>0
0
0
0062- 72
Hours After First Dose of Betamethasone
FIGURE 3 Cortisol levels in cord bloods of betamethasone-treated and control premature infants. Individual cortisolvalues of treated infants are compared with mean valuesfor control infants.
bound cortisol levels in these two situations are 4.6 and7.8 ug per 100 ml, which are in the order of 14 and 3times that of normal premature infants. In treated in-fants, both cortisol and betamethasone contribute tothe plasma glucocorticoid activity. We calculate thatthese infants have peak unbound and albumin-boundglucocorticoid levels of 9.4 and 8.4 ug cortisol equiva-lents per 100 ml, respectively. Betamethasone treatmentat this dose, therefore, results in an unbound glucocorti-coid level similar to that achieved by endogenous cor-tisol production in the premature infant with RDS.
DISCUSSIONWe have determined serum levels of betamethasone,using a radioreceptor assay for glucocorticoids. This
TABLE IIITotal, Albumin-Bound, and Unbound Plasma
Glucocorticoid Activity in thePremature Infant
Plasma glucocorticoid activity
Albumin-Clinical status Total bound Unbound
jig corlisol eq/100 ml
Normal premature infant 10.5 2.8 2.8PROM(>16 h) 16.2* 4.6 4.6RDS (4 h of age) 22.1$ 6.4 7.8Betamethasone-treated
Cortisol 5.9§V20.8 1.4k 9.3 1.41 8.4Betamethasone 14.9§ 7.9} 7.oJ
* Mean cord plasma cortisol value in 10 premature infantsstudied by Bauer et al. (26).1 Mean plasma cortisol value in 24 premature infants studiedafter birth by Baden et al. (27).§ Mean values 1-10 h after second dose of betamethasone(see Figs. 2 and 3).
Glucocorticoid Levels after Prenatal Betamethasone 1551

iiiethod miieasures steroids with gluhcocorticoid activ-ityin proportion to both their concentration and theiraffinity for the cytoplasimic recel)tor. It is felt that thelatter property reflects the intriinsic biologic potency ofcorticosteroids. In this regard we have reported previ-ously that the relative affinities of many natural andsynthetic corticosteroids for receptors of hepatomiia cells(used in the assay) and humain fetal lunig are similar(19). For this reason, we have expressed betamethasoneconicenitrations in terms of cortisol equivalents and halvedirectly comlpared serumii lev els of adminiistered anden(logenious glucocorticoids.
In both large studies reporte(l to date (6-8), pre-natal betamethasoine therapy has significantly reducedthe incidence of RDS in premature infanits. \Ve havedetermined the serum levels of steroid at variGus timesafter injection of the same dose of betaimietlhasone acetateand betamethasone phosphate. In nmaternal serum peaklevels of betamethasone occur witllin 1 h and declinewvith a half-time of about 6 h. In cord blood, beta-methasone is detecte(l wNithiln 1 Ih of treatmiienit andsteroid levels decrease with a hlalf-time of about 14 h.At all times during treatmilenit, tlhere is less betamietha-sone in fetal than maternal serumi vith a miiean gradientof 3: 1 in matclhed comiparisons. A larger gradienit wasfound for endogenous cortisol (mean, 5.8: 1). It isreported that the maternal: fetal gradielnt for predniso-lone is about 10: 1 after infusion of either prednisone orprednisolone (29). Tlhus, betamiethasone seemls prefer-able to cortisol, prednisone, or prednisololne for prenataltherapy since relatively lower (loses need be adnminis-tered to the mother.
It would appear that the miieani le-el of betametlha-sonie in the cord bloods of our series decreases to about3 sig cortisol equivalenits per 100 mil before the secoinddose at 24 h. This produces an unbound glucocorticoidactivity of 3.3 stg per 100 mil, whlich is siimilar to thatfound in untreated infants, suggesting that the level ofbetamethasone in some infants may be less than optimalfor several lhours before the secoind (lose. For thisreason, it would seem appropriate in subsequent clinicaltrials with this preparation of steroid to repeat a 12-mgdose more frequently (e.g., 12 mg at 0 and 18 h). Itslhould also be noted that the plasmiia glucocorticoid ac-tivity in treated infants falls below control levels duringthe 3rd day. It is possible that a longer exposure toelevated steroid levels (e.g., a tlhird dose 24 h after thesecond) would increase the effectiveneis of therapy.
As reported previously (6), therapy with this doseof synthetic corticosteroid rapidly suppresses maternalcortisol levels. Cortisol in cord blood is also decreasedsoon after treatment; values were lower after the secondinjection at a time when betamethasone levels werelighest and maternal cortisol quite loxv. These lower
valuies in cord bloo10 probably reflect decrease(l coItisolp)roduction in the fetus as well as in the mlothler. HowN-ever, in five treated infants with RDS, we foundelevated cortisol levels after birth, suggesting that thenorimial pituitary-adrenal response to stress is not lostwvith treatment.
Another concern regarding the use of prenatal cor-ticosteroids in human infants is the possibility of ad-verse effects on grow-tlh. Administrationi of these steroidsto fetal and neonatal animals cain seriously iml)airOlrgalnl anid somiatic growth and neurologic functioni (12-18). Only somiie of these effects are 1)artially or fullyrev ersed by comlpenisatory catclh-up grows tlh after witlh-drawal of steroid (12, 13, 16, 17, 30). However, thedoses of lhormlone per kilogram body w-eiglht used in theanimal studies are 15-300 times that which the humanfetus receives xvith prenatal betamethlasonie therapy.This is a critical consideration since the extent of theeffects in animals is dose related (12, 13, 18).
Harmiiful effects of hiigh doses of corticosteroids a(l-miiinistered to the humlilan infanit in the neonatal periodare also reported (for reviewv see reference 31) aindinclud(le impaired growtlh anid increase(d inci(lenice ofcentr,al nervous system abnormalities. We estimate thatthe glucocorticoid levels in those infants were at least10 tinmes greater than the maximiial lexvels which wefound in the premiiature infants of this study. Thus, itappears that the dose of prenatal betamiethasone usedin this study slhould not expose the premlatuire infant topotentiallv lharmiiful pharmiiacologic levels of plasmia glu-cocorticoid activity. The apparent safety of betametlha-sone at this dose is supported by preliminary observa-tions on the neonatal clinical course of premiiature in-fanits treated in utero (6, 32).
In addition, w-e find only a tlhreefold mlaximiial increasein the unbounild glucocorticoid level in premlature in-fanits exposed to prenatal betamethasone therapy. Thislevel can be compared to the 1ly- and 3-fold increasesfound in premature infants wlho are delivered afterPRO.M or who develop RDS after birth, respectively.Thus, such treatnment exposes the infant to corticoiddoses no higher, and for nIo longer, than those wlhichoccur by endogenous production in the infant w-itlhRDS. These conmparisons suggest that antenatal beta-metlhasonie treatment at this dose closely approximatesa physiologic stress response. It seems unlikely, thouglhunprovein, that this level of corticoid is hazardous tothe premature infant.
Our findings also indicate that prevention of RDSoccurs with serum glucocorticoid levels in the physio-logic stress range, suggesting that such levels are suf-ficient to induce lung maturation in the human fetus.This is consistent with a direct glucocorticoid effect inlung mediated by the receptor system since the levels
1552 P. L. Ballard, P. Granberg, and R. A. Ballard

of serum glucocorticoid activity after treatment wouldbe sufficient to fill all receptor sites and thereby evokean optimal response. The elevated corticoid levels asso-ciated with PROMand RDS suggest that endogenouscortisol may act by the same mechanism to acceleratepulmonary development in these situations. It is alsopossible that during normal gestation the appearanceof alveolar surfactant is triggered by an increase inendogenous cortisol levels. In this regard, Murphy (33)has reported that higher levels of cortisol in cordblood are associated with less RDS, and Fencl andTulchinsky (34) have noted an increase in amnioticfluid cortisol after 34 wk gestation in normal pregnan-cies. Thus, the level of endogenous corticosteroid maybe an important regulatory factor in both the patho-genesis and prevention of this disease. In this case,administration of prenatal glucocorticoids in appropriatecircumstances may accelerate developmental events inthe lung through normal physiologic mechanisms.
ACKNOWLEDGMENTSWe thank Ms J. Carter for capable technical assistance andDrs. F. Berman and R. Creasy for their cooperation intreatment of patients and collection of samples.
This work was supported by Pulmonary Specialized Cen-ter of Research HL 14201 from the National Heart andLung Institute.
REFERENCES1. Ballard, P. L., R. A. Ballard, and J. P. Granberg. 1975.
Glucocorticoid levels in maternal and infant serum fol-lowing antenatal betamethasone therapy. Cliii. Res. 23:157A. (Abstr.)
2. Ballard, P. L., R. A. Ballard, and P. Granberg. 1975.Serum glucocorticoid levels following betamethasonetherapy to prevent respiratory distress syndrome(RDS). Pediatr. Res. 9: 393. (Abstr.)
3. deLemos, R. A., J. W. Shermeta, J. H. Knelson, R.Kotas, and M. E. Avery. 1970. Acceleration of appear-ance of pulmonary surfactant in the fetal lamb by ad-ministration of corticosteroids. Aoi. Rev. Respir. Dis.102: 459-461.
4. Motoyama, E. K., M. M. Orzalesi, Y. Kikkawa, M.Kaibara, B. Wu, C. J. Zigas, and C. D. Cook. 1971.Effect of cortisol on the maturation of fetal rabbitlungs. Pediatrics. 48: 547-555.
5. deLemos, R. A., and G. W. 'McLaughlin. 1973. Induc-tion of the pulmonary surfactant in the fetal primate bythe intrauterine administration of corticosteroids. Pedi-atr. Res. 7: 425. (Abstr.)
6. Liggins, G. C., and R. N. Howie. 1972. A controlledtrial of antepartum glucocorticoid treatment for preven-tion of the respiratory distress syndrome in prematureinfants. Pediatrics. 50: 515-525.
7. Howie, R. N., and G. C. Liggins. 1973. Prevention ofrespiratory distress syndrome in premature infants byantepartum glucocorticoid treatment. In RespiratoryDistress Syndrome. C. A. Villee, D. B. Villee, and J.Zuckerman, editors. Academic Press, Inc., New York.369-380.
8. Fargier, P., B. Salle, M. Baud, J. C. Gagnaire, P.Arnaud, and P. Magnin. 1974. Prevention du syndromede detresse respiratoire chez le premature. Interet dutraitement antepartum par les glucocorticoides. Nouv.Presse Med. 3: 1595-1597.
9. Ballard, P. L., and R. A. Ballard. 1972. Glucocorticoidreceptors and the role of glucocorticoids in fetal lungdevelopment. Proc. Natl. Acad. Sci. U. S. A. 69: 2668-2672.
10. Giannopoulos, G. 1974. Variations in the levels of cyto-plasmic glucocorticoid receptors in lungs of variousspecies at different developmental stages. Endocrinology.94: 450-458.
11. Ballard, P. L., and R. A. Ballard. 1974. Cytoplasmicreceptor for glucocorticoids in lung of the human fetusand neonate. J. Clin. Invest. 53: 477-486.
12. De Souza, S. W., and B. P. F. Adlard. 1973. Growthof suckling rats after treatment with dexamethasoneor cortisol. Implications for steroid therapy in humaninfants. Arch. Dis. Child. 48: 519-522.
13. Cotterrell, M., R. Balazs, and A. L. Johnson. 1972.Effects of corticosteroids on the biochemical maturationof rat brain: postnatal cell formation. J. Neurochemii.19: 2151-2167.
14. Weichsel, M. E. Jr. 1974. Glucocorticoid effect uponthymidine kinase in the developing cerebellum. Pediatr.Res. 8: 843-847.
15. Carson, S. H., H. W. Taeusch, Jr., and M. E. Avery.1973. Inhibition of lung cell division after hydrocorti-sone injection into fetal rabbits. J. Appl. Physiol. 34:660-663.
16. Shapiro, S. 1968. Some physiological, biochemical, andbehavioral consequences of neonatal hormone adminis-tration: cortisol and thyroxine. Gcei. Comp. Endocrinol.10: 214-228.
17. Gumbinas, M., M. Oda, and P. Huttenlocher. 1973. Theeffects of corticosteroids on myelination of the develop-ing rat brain. Biol. Neonate. 22: 355-366.
18. Perey, D. Y. E., R. C. Herdman, and R. A. Good.1967. Polycystic renal disease: a new experimentalmodel. Science (Wash. D. C.). 158: 494-496.
19. Ballard, P. L., J. P. Carter, B. S. Graham, and J. D.Baxter. 1975. A radioreceptor assay for evaluation ofthe plasma glucocorticoid activity of natural and syn-thetic steroids in man. J. Clin. Endocriniol. Metab. 41:290-304.
20. Murphy, B. E. P. 1967. Some studies of the protein-binding of steroids and their application to the routinemicro and ultramicro measurement of various steroidsin body fluids by competitive protein-binding radio-assay. J. Cliii. Endocrinol. .1Metab. 27: 973-990.
21. Trapp, G. A., and C. D. West. 1969. Determination ofcorticosteroid-binding proteins by an absorption method.J. Lab. Cliii. Med. 73: 861-871.
22. Tait, J. F., and S. Burnstein. 1964. In vivo studies ofsteroid dynamics in man. Ini The Hormones. Vol. 5.G. Pincus, K. V. Thimann, and E. B. Astwood, editors.Academic Press, Inc., New York. 441-557.
23. Hardie, G., V. C. Harrison, and J. E. Kench. 1968.Further observations on serum proteins in respiratorydistress syndrome of the new-born. Arch. Dis. Child.43: 471-474.
24. De Moor, P., K. Heirwegh, J. F. Heremans, and M.De Clerck-Raskin. 1962. Protein binding of corticoidsstudied by gel filtration. J. Clin. Iiivest. 41: 816-827.
25. Peets, E. A., -M. Staub, and C. Symchowicz. 1969.
Gltcocorticoid Levels after Prenatal Betamethasone 1 55)3
Plasma binding of betamethasone-3H, dexamethasone-8H, and cortisol-1'C. A comparative study. Biochem.Pharmacol. 18: 1655-1663.
26. Bauer, C. R., L. Stern, and E. Colle. 1974. Prolongedrupture of membranes associated with a decreased in-cidence of respiratory distress syndrome. Pediatrics.53: 7-12.
27. Baden, M., C. R. Bauer, E. Colle, G. Klein, H. W.Taeusch, Jr., and L. Stern. 1972. A controlled trial ofhydrocortisone therapy in infants with respiratory dis-tress syndrome. Pediatrics. 50: 526-534.
28. Reynolds, J. W. 1973. Serum total corticoid and cortisollevels in premature infants with respiratory distresssyndrome. Pediatrics. 51: 884-890.
29. Beitins, I. Z., F. Bayard, I. G. Ances, A. Kowarski,and C. J. Migeon. 1972. The transplacental passage ofprednisone and prednisolone in pregnancy near term.J. Pediatr. 81: 936-945.
30. Kotas, R. V., L. C. Mims, and L. K. Hart. 1974. Re-versible inhibition of lung cell number after glucocorti-coid injection into fetal rabbits to enhance surfactantappearance. Pediatrics. 53: 358-361.
31. Fitzhardinge, P. M., A. Eisen, C. Lejtenyi, K. Met-rakos, and M. Ramsay. 1974. Sequelae of early steroidadministration to the newborn infant. Pediatrics. 53:877-883.
32. Granberg, P., R. A. Ballard, P. L. Ballard, and F.Berman. 1975. Effects of antenatal betamethasone inpreterm infants. Pediatr. Res. 9: 396. (Abstr.)
33. Murphy, B. E. P. 1974. Cortisol and cortisone levelsin the cord blood at delivery of infants with and with-out the respiratory distress syndrome. Am. J. Obstet.Gynecol. 119: 1112-1120.
34. Fencl, M. D., and D. Tulchinsky. 1975. Total cortisolin amniotic fluid and fetal lung maturation. N. Engl. J.Med. 292: 133-136.
155) 4 P. L. Ballard, P. Granberg, anid R. A. Ballard