sensing an improvement: an experimental study to evaluate the use of aromatherapy, massage and...
TRANSCRIPT

Joumal of Advanced Nursing, 1995, ?1, 34-40
Sensing an improvement: an experimental studyto evaluate the use of aromatherapy, massageand periods of rest in an intensive care unitChnstine Dunn RN DPSN BSc(Hons)Senior Nurse Practice Development, Royal Berkshire ond Battle Hospitals NHS Trust,Reading
Jennifer Sleep RN RM MTD BAResearch Co-ordmator, Berkshire College of Nursing and Midwifery, Reading
and David CoUett PhDLecturer in Statistics, Department of Applied Statistics, University of Reading,Reading, England
Accepted for publication 28 March 1994
DUNN c , SLEEP J & COLLETT D (1995) Journal of Advanced Nursing 21,34-40Sensing an improvement: an experimental study to evaluate the use ofaromatherapy, massage and penods of rest m an mtensive care unitThere is widespread belief that the use of aromatherapy and massage m anintensive care environment offers a means of increasing the quality of sensorymput that patients receive, as well as reducing levels of stress and anxietyDespite a wealth of anecdotal eA^dence m support of these claims, there haveheen few objective studies to evaluate the effects of these therapies In thisexperimental study 122 patients admitted to a general intensive care unit wererandomly allocated to receive either massage, aromatherapy using essential oilof lavender, or a period of rest Both pre- and post-therapy assessmentsincluded physiological stress indicators and patients' evaluation oftheiranxiety levels, mood and ahihty to cope with their intensive care experienceNinety-three patients [77%) were ahle to complete subjective assessmentsThere were no statistically significant differences in the physiological stressindicators or observed or reported behaviour of patients' ability to copefollowing any ofthe three mterventions However, those patients who receivedaromatherapy reported significantly greater improvement m their mood andperceived levels of anxiety They also felt less anxious and more positiveimmediately foUovinng the therapy, although this effect was not sustained orcumulative
INTRODUCTION ^®° have to cope not only with a physical emergencyrequiring urgent action but also severe emotional and
Patients requinng admission to an mtensive care unit sire psychological trauma There is also evidence to suggestin the throes of an acute physiced cnsis Moreover, they that receiving treatment m an mtensive care unit (ICU) can
be a depersoncdizmg and dehumanizmg expenenceConespondence ChnsbneDunn Semor Nurse Pwctice Development, ^^^^ ^ ^ j ^ ^ ^ ^^ mcreasmg demotivation, apathy andRoyal Berkstiire and Battle Hospitals, NHS Trust, Battle Hospital, Oxford , , , , , , , , ' r- JRoad,Headingm3iAG,Ensland Withdrawal (Meyer ef a/ 1961)
34

Sensing an improvement
Despite receiving constant attention, cntically illpatients may suffer intense loneliness as a result of theirphysical and emotional seclusion frtim both family andcarers This feeling of isolation may be heightened andtheir perception of touch distorted if they are unable tosee or hear clearly as a consequence of fluctuating con-scious levels, drugs or enforced immobility They may alsobe unable to interpret mconung stimuh because of sensorydepnvation or, alternatively, overload
Patients' feelmgs of solitude may be mtensified whenvisitors refram from touching the patient for fear of causingharm There is evidence to suggest that the more senouslyill the patient, the less physical contact he/she receivesfrom the nurses responsible for providing care (Bamett1972) Nurses may avoid spontaneous, comfortmg touchm order to avoid disturbing sensitive momtonng equip-ment Storlie (cited by Clement 1983) descnbes this as'professional autism', that is when technological demandsalmost exclusively focus the nurse's attention on technicalaspects rather than on a holistic approach to care Worrell(1977) also considers that professionals may deliberatelydistance themselves from senously ill patients as a defencemechamsm against personal distress and to protect them-selves from the need to confront their own mortality
TOUCH IN INTENSIVE CARE UNITS
Non-verbal communication has been shown to be essentialfor normal physical and mental development (Frank 1957,Montagu 1971) Touch, as a modality on non-verbal com-munication, IS often referred to as being expressive orinstrumental Expressive touch is spontaneous, affectiveand not directed towards achieving a physical procedure,whereas mstrumental touch is a deliberate action intendedto achieve a physical task Rubm (1963) suggests thatexpressive touch is an effective means of communicatingcaring and comfort to patients experiencing isolation andvulnerability This view is endorsed by McCorkle (1974)who mvestigated the effects of touch as a means of non-verbal commumcation with seriously ill patients andfound that nurses effectively used this medium to establishrapport with patients withm a relatively short penod oftime
Weiss (1979) proposes that issues such as duration,location, action, sensation, mtensity and frequency oftouch act as symbols to the receiver by canying impliedmessages She suggests that touch is more likely to stimu-late an increase in nervous activity when it is strong mintensity and applied to highly innervated areas of thebody, for example over the vital organs of the body andthe artenes Alternatively, touch which is infrequent, ofweak intensity and soothmgly applied to diffusely innerv-ated areas such as the outside of the limbs, back and scalphas the potential to reduce nervous activity Other factorssuch as cultural background, previous expenence of touch
and the attitudes of fanuly and friends also influence howmdividuals interpret these messages
Planning
Planmng the use of purposeful touch such as massage forintensive care patients thus requires consideration of thecultural and social meanings that individuals may attachto such a means of expression It should also be recognizedthat senously ill patients may be inhibited in expressmgtheir unwiUmgness to receive this tjrpe of touch becauseof low ene i^ levels, feelmgs of vulnerability or commum-cation difficulties It IS important that attention is paid tothe mdividual patient's preferences and responsiveness inorder to ensure that the therapy is not perceived as yetanother intervention rather than a welcome and sensitivemeans of comfort and commumcation
These considerations have important implications fornurses who may be planning to introduce touch therapieswithm intensive care units, in addition nurses may expen-ence increased stress m developing closer relationshipswith patients
MASSAGE AND AROMATHERAPY ASMODALITIES FOR TOUCH
Massage may be described as the application of vanoussystematic and usually rh)rthmic hand movements per-formed on the soft tissues of the body These movementsproduce different effects depending on a number of factorssuch as the type and speed of movements, the pressureexerted by the hands, fingers or thumbs and the area ofbody treated Massage is considered by many to be atherapy m its own nght, offenng the potential to relievetension, reduce fatigue and to enhance the body's abilityto heal itself (Hamson 1986, Eyerman 1987) Anecdotalclaims by nurse practitioners suggest that mass^eimproves the nurse-patient relationship, provides comfortand relieves anxiety and tension (Hollinger 1980, Byass1988) Others view massage as a natural extension to thenurse's role (Pearson 1988) to this end, m many nursingdevelopment units, staff are currently being trained tomclude massage in their daily nursmg care as a treatmentwhich IS complementary to conventional nursmg
Massage can also provide a medium for the use of aro-matic oils, which may be added to the lubncating agentor inhaled by evaporation This techmque is known asaromatherapy A range of over 200 essential oils may beused to achieve differing effects Their precise mode ofaction IS unclear but they are believed to influence theemotional status of the recipient by a combination ofabsorption, when applied to the skm, and inhalation, fol-lowing evaporation from the skm dunng massage or whenheated m burners or m steam (Valnet 1986)
One of the oils most widely used is lavender, which is
35

C Dunn et al
claimed to have a relaxing and calmuig effect and is alsoone of the least toxic and allei^enic of all the essential oils(Tisserand 1989) Recent laboratory tests suggest that theodour of lavender may have a sedative effect on brain wavepattems {Birchall 1990) and so is likely to be parbcularlyuseful m stressful cm:umstances such as m intensivecare settings
Paucity of research
There is currently a paucity of sound research evidencewhich can help guide practice m relation to the appro-pnate use of both massage and aromatherapy Perhaps thisIS not altogether surpnsmg given the complex nature oftouch and the lack of valid and reliable tools to measureabstract and affective concepts such as copmg, mood andloneliness Attempts have been made to measure auto-nomic arousal following massage by using physiologicalresponses such as systolic and diastohc blood pressure,heart rate and galvanic skm response In one of the earliestpublished studies to use these indicators, Kaufinan (1964)measured the responses of 36 patients both before and afterreceiving a back rub, but failed to demonstrate a significantdifference in physiological outcomes
In a study using a similar design, Longworth (1982) alsofailed to demonstrate an improvement m physiologicalindicators following back massage m a healthy volunteersample, although a significant improvement was noted mthe reported state of anxiety foUowmg the therapy Sunms(1986) also used a withm-subjects design to evaluate thepsychological effects of slow stroke back massage givento SIX women receiving treatment for cancer A Likert-type symptom distress scale was used to record thewomen's perceptions of the therapy An improvement wasreported m five out of sue mood variables including tir-edness, tension and tranquillity However, the smallsample size and lack of formal controls severely limits theextent to which such findings can be generalized toother settings
There is also a lack of sound evidence regarding theappropriate use of aromatherapy in health care settingsSeveral anecdotal accounts have been reported recently mthe nursing press, each of which has claimed benefits forpatients (Wise 1989, Passant 1990, Tattum 1992) However,whilst offering interesting insights onto the range of appli-cations of this intervention, such uncontrolled obser-vations do not provide a means of systematicallyevaluating a relatively new nursmg therapy which mayhave the potential to do harm as well as good
THE STUDY
In an attempt to evaluate the effectiveness of aromatherapyand massage used m the nursing care of patients in anICU, a randonuzed controlled tnal was designed using
physiological, psychological and behavioural measures ofoutcome
The study took place m the ICU of a busy distnct generalhospital durmg a 14-month penod between May 1989 andJuly 1990 Patients who had sustamed head mjury, wereknown to be hypersensitive to perfume or had skmalleigies such as dermatitis or eczema or who were unableto read or wnte English were not eligible for inclusion inthe trial Recruitment took place withm 24 hours ofadmission to the unit
The participant's consent (or that of the patient's nearestrelative) was sought pnor to recruitment and randomiz-ation Following consent each patient was randomized toreceive one of three treatment schedules
1 body massage,2 aromatherapy,3 undisturbed rest
As the mean length of stay of patients in the ICU was 5days, patients received a mmimum of one and a maximumof three sessions of the allocated therapy withm this 5-daypenod Each therapy was separated by a penod of 24hours
Prior to commencement of the tnal, six members of thenursing team undertook training in massage and aroma-therapy techniques by a qualified aromatherapist who wasalso a qualified nurse The therapist was also responsiblefor assessing the skill levels and proficiency of the nursesThis was achieved by each nurse performing the stan-dardized massage technique on the therapist Details of thethree therapies are given below
Massage
A penod of massage was conducted using a standardizedtechnique of light effleurage strokes performed on diffuselyinnervated areas of the body as available to the therapist,e g back, outside of limbs, scalp The penod of massagecontinued for minimum of 15 minutes to a maximum of30 minutes Grapeseed oil was used as a lubncatmgmedium
Aromatherapy massage
The massage was performed as above, but the lubncatingmedium was aromatic essential oil of lavender (Lavendulavera) diluted to 1% concentration The same supply of oilwas used throughout the tnal
In both aromatherapy and massage groups, verbalizationwas minimized to a level that enabled the therapy to beconducted safely conversation was therefore limited torespondmg rather than mitiatmg contact
36

Sensing an improvement
Undisturbed rest
The bed was scareened to allow the patient undisturbed restfor a minimal penod of 30 minutes The patient wasinformed before the rest penod that although they wouldbe undisturbed, they would contmue to be observed by theallocated nurse Intervention and disturbance by medicalstaff, nurses and visitors was minimized dunng this time
Ethical considerations
Considerable attention was paid to this aspect of the studyas the staff were acutely aware of the distress experiencedby both patients and their relatives As the majority wereadmitted as emergencies it was not always possible to pre-pare patients in advance of admission to the umt Greatcare was taken to explain the precise nature of the trial topotential participants who were conscious and to theirclosest relative when they were unable to respond Theywere assured that refusal to participate would not jeop-ardize their care in any way Wntten mformation describ-ing the nature and conduct of the study weis also madeavailable Nursing staff were freely available to discussaspects of concern related to the tnal Patients and theirrelatives were given 24 hours m which to consider partici-pating in the study pnor to giving formal consent Thestudy protocol was approved by the Research and EthicsCommittee for the West Berkshire Health Distnct
Sample size
- It was estimated that the proportion of patients experienc-T ing anxiety was likely to differ by 30% between the control^ and the treatment groups To achieve 90% power m ldent-"̂ lfying such a difference as being significant at the 5% level,
35 patients were required in each of the treatment groups•' The overall minimal sample size was therefore pre-set at
105 subjects
Randomization
J Consecutively numbered, opaque, sealed envelopes con-tained the random allocation to one of three therapies The
3 opening of the envelope signalled the irrevocable entry ofJ a patient into the trial for the purpose of einedysis, as thisj minimized selection bias Pre- and post-therapy assess--« ments were conducted by a nurse who did not tcike part
m the care of that individual patient Once the obser-vations were completed, the data sheet was filed awayfrom the clinical area so that it was not available for refer-ence following completion of the treatment Thus everyattempt was made to minimize observer bias and to blindassessors to the actual therapy administered
The following pnncipal outcome measures wererecorded both before and after each therapy session
assessment
The physiological vanahles measured were systohc anddiastohc blood pressure, heart rate and rhythm, and respir-atory rates The majonty of patients m an ICU receivefrequent momtonng of their vital signs, these are often con-tinuously recorded via pressure transducers which transimtdirectly onto bedside momtors Patients being ventilatedhave the number of spontaneous breaths and controlledbreaths displayed separately Objective and accuraterecordings were therefore readily available without mcreas-ing the workload of staff or unduly disturbing the patientWhere physiological assessment ublized electromc mom-tors, the equipment was calibrated before the pre-treatmentetssessment recordings and recalibration did not occur untilafter the post-treatment recordmgs were completed
Behavioural assessment
This was scored using a modified assessment tool devel-oped specifically for intensive care patients who areunable to respond verbally (O'Brien & Alexander 1985)This included both positive and negative responses basedon a range of observable behaviours, including motoractivity, somatic changes and facial expressions The rangeof behaviours was categorized into a four-point scale,which the nurse used to assess the response of consciouspatients The validity and lnter-rater reliability of this toolwere tested by askmg eight nurses to independentlyobserve three specific patients and complete the assess-ment score for each There was good agreement m theirscoring This exercise was repeated on three successiveshifts with sirmlar results The neurological status ofunconscious patients was recorded using the Glasgowcoma scale (Teasdale & Jennett 1974)
Patient assessment
Conscious patients, able to respond, used four-point scalesto assess their level of anxiety, their mood and their abilityto cope with their present situation The terms selected forinclusion on the scale attempted to recogmze the limitedattention span likely to be experienced by the majonty ofcritically ill patients Patient responses were completedimmediately before sind following each therapy and othermterventions were kept to a mmimum dunng this periodIn addition patients were mvited to make any other com-ments they wished
A pilot study was conducted on 30 patients to test thereliability and validity of the final assessment tool
RESULTS
A descnption of patients in each of the three groups isgiven m Table 1 The youngest patient weis 2 years and the
37
C Dunn et al
Table 1 Descnptions of groups at tnal entry
MaleFemaleMean age in yearsMean dviration of
therapy dunng 3 days(in minutes)
Massage(n=43)
2518
6417
Aromatherapy(n = 41)
192255
16 5
Rest(n = 38)
251361
35
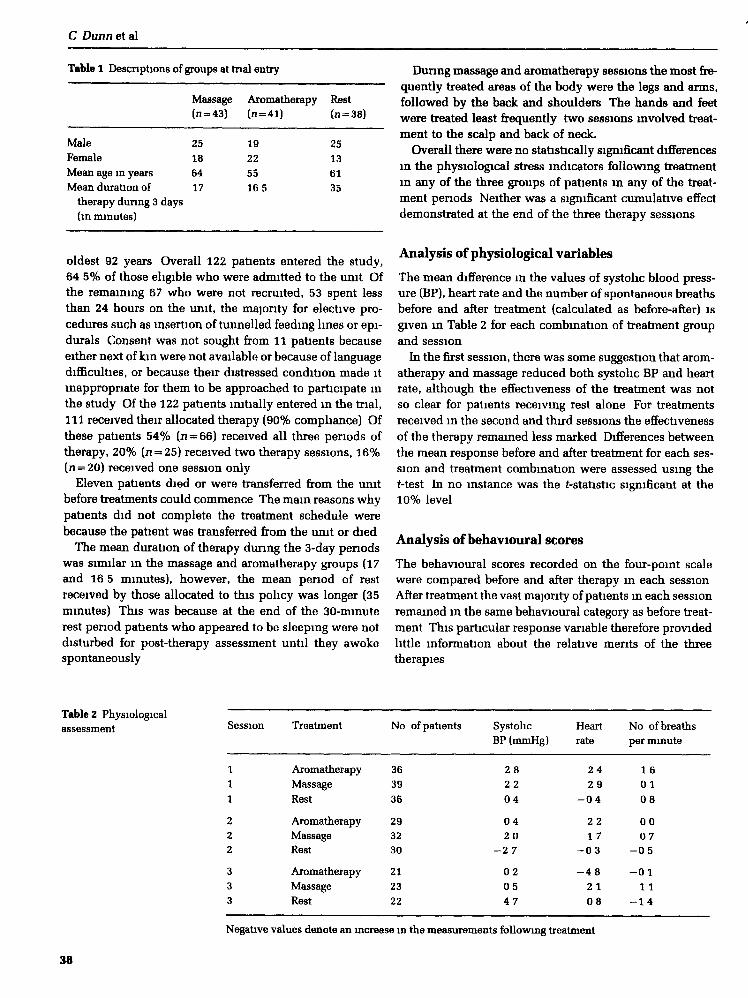
oldest 92 years Overall 122 patients entered the study,64 5% of those eligible who were admitted to the unit Ofthe remaining 67 who were not recaruited, 53 spent lessthan 24 hours on the unit, the majonty for elective pro-cedures such as insertion of tunnelled feeding lines or epi-durals Consent was not sought from 11 patients becauseeither next of kin were not available or because of languagedifficulties, or because their distressed condition made itinappropriate for them to be approached to participate mthe study Of the 122 patients initially entered m the trial,111 received their allocated therapy (90% compliance) Ofthese patients 54% (ii = 66) received all three penods oftherapy, 20% (n = 25) received two therapy sessions, 16%[n = 20) received one session only
Eleven patients died or were transferred from the unitbefore treatments could commence The main reasons whypatients did not complete the treatment schedule werebecause the patient was transferred from the umt or died
The mean duration of therapy dunng the 3-day periodswas similar m the massage and eiromatherapy groups (17and 16 5 minutes), however, the mean penod of restreceived by those allocated to this policy was longer (35minutes) This was because at the end of the 30-minuterest penod patients who appeared to be sleeping were notdisturbed for post-therapy assessment until they awokespontaneously
Dunng massage and aromatherapy sessions the most fre-quently treated areas of the body were the legs and arms,followed by the back and shoulders The hands and feetwere treated least frequently two sessions mvolved treat-ment to the scalp and back of neck.
Overall there were no statistically significant differencesin the physiological stress indicators followmg treatmentin any of the three groups of patients m any of the treat-ment periods Neither was a significant cumulative effectdemonstrated at the end of the three therapy sessions
Analysis of physiological variables
The mean difference m the values of systolic blood press-ure (BP), heart rate and the number of spontaneous breathsbefore and after treatment (calculated as before-after) isgiven m Table 2 for each combination of treatment groupand session
In the first session, there was some suggestion that arom-atherapy and massage reduced both systolic BP and heartrate, although the effectiveness of the treatment was notso clear for patients receiving rest alone For treatmentsreceived m the second and third sessions the effectivenessof the therapy remained less marked Differences betweenthe mean response before and after treatment for each ses-sion and treatment combmation were assessed using thet-test In no instance was the f-statistic significant at the10% level
Analysis of behavioural scores
The behavioural scores recorded on the four-point scalewere compared before and after therapy in each sessionAfter treatment the vast majonty of patients m each sessionremained m the same behavioural category as before treat-ment This particular response vanable therefore providedhttle mformation about the relative ments of the threetherapies
Table 2 Physiologicalassessment Session Treatment No of patients
AromatherapyMassageRest
AromatherapyMassageRest
AromatherapyMassageRest
363936
293230
212322
SystolicBP (mmHg)
Heartrate
28
22
04
04
20
-27
02
05
47
No of breathsper minute
2 42 9
0 4
2 21 70 3
4 82 10 8
1 60 1
0 8
0 00 7
- 0 5
- 0 11 1
- 1 4
Negative values denote an mcrease in the measurements foUowu^ treatment
38

Sensing an improvement
Analysis of psychological assessment
Of the patients who received one or more therapies, 84(76%) were at a cognitive level which enabled them tocomplete this assessment, which included their reportedlevels of anxiety, general mood and their ahihty to copewith being m ICU From these data the proportion ofpatients m each of the three treatment groups and eachsession who showed an improvement m their reportmgwas calculated The resultmg percentages are given mTable 3
For each session and each response vanable, a chi-squared test was used to compare the proportions improv-ing between the three treatments The difference betweenthe proportions of patients in the three groups whosereported level of anxiety improved m the first session wassignificant at the 5% level (P=0 05) This difference wasdue to there being greater proportions of patients whoseanxiety improved for aromatherapy compared to rest
There were no treatment differences in the proportionsof patients registenng an improvement m anxiety level inthe other two sessions Neither were there any significantdifferences m the proportions whose mood or copingability improved m any session
The technique of lmear logistic modelling (Collett 1991)was used to determine if there were treatment differencesafter allowing for age and sex differences amongst patientsThe results of this analysis were very similar to those fromthe analysis descnbed above, so fuller details are omitted
DISCUSSION
Although every attempt weis made to maximize recruitmentto the study, the numbers who were not recruited highhghtthe difficulties of conductmg tnals in ICU where the cir-cumstances of admission are so traumatic Moreover, theduration of stay is extremely unpredictable and consider-able influenced by decisions relating to the demand for
mtensive care facilities It was for this practical reason thatpabents m the tnal were offered a maximum of three treat-ments only, as few remam for longer penods of time Inthis tnal the ma)onty of patients received at least two ther-apy sessions, more than half receiving all three sessions
The study did not differentiate between the possibleeffects of the aromatherapy oil by mode of use, l e throughinhalation or by application to the skin Many patients mICU expenence a distorted sense of smell due to the pres-ence of nasal or oral tubes, drugs, etc Pnor to recruitmentthe patient or nearest relative was mformed of the use oflavender oil to ensure that no-one who participated m thestudy was knowingly averse to the smell of lavenderNevertheless the response of the individual to a particularsmell or its association with past events should always beconsidered in any study involving aromatherapy
The study demonstrated that the condition ofthe patientwas not destabilized as a consequence of any of theinterventions This consideration is obviously of primeimportance when canng for those who are cntically illThe physiological observations failed to demonstrate animprovement m vital signs, which may have provided anindicator of reduced anxiety levels However, it is alsoacknowledged that small fluctuations m a patient's vitalsigns are to be expected even under normal conditions
Rest
Rest proved as effective as massage in reducing reportedanxiety and improving mood, and as good as aromatherapyin patients reporting improvements in their coping abilityThis finding has implications for practice, as ensurmg thatpatients are allocated penods of good quality rest is some-thing that most nurses can safeguard this should beregarded as a positive treatment
The 1% concentration of lavender oil used m the studywas at the lower end of the range of recommendeddilution This was in recognition of the cntical condition
Table 3 Percentage of patientswhose psychologicalassessment improved as aresult of treatment
Response vanable
Session
11
1
222
333
Treatment
AromatherapyMassageRest
AromatherapyMassageRest
AromatherapyMassageRest
No of patients
3639
36
293230
21
2322
Anxiety
72*59
44*
766967
706550
Mood
5649
42
695660
554345
Copmg
504642
554157
453936
* Statistically sigmficant, P=0 05, z = 5 73, 2 d f
39

C Dunn et al
of the participants It is possible that 2% concentrationmay have produced more beneficial effects Other essentialoils also remain to be tested m climcal settings At thetime this study was conducted there were no male mem-bers of the nursing team, consequently all massage ses-sions were conducted by female staff The gender of thenurse raises interesting issues regardmg the response ofpatients to massage treatments
Patients' comments reported followmg each session pro-vided an insight into their expenence of the treatment andof ICU in general Although detailed analysis was not per-formed, responses covered a range of issues mcludmgpositive or negative feelings about the therapy andICU, comments relating to their state of relaxation andthose concemed with their body image or self-esteemExamples include
I wouldn't have though anyone would want to touch me like that[massage]It [aromatherapy] made me feel clean and a whole personThe rest penod was not long enough
These types of issues remam a nch source for furtherresearch
CONCLUSION
This study has formally evaluated the effects of massageand aromatherapy for one group of pabents nursed in ageneral intensive care setting The evidence suggests thatmassage may offer a useful therapy for nurses to considerwhen plannmg the psychological care of such patientsThe addition of 1% essential oil of lavender appears toenhance the effects of massage and may help contribute tothe patients' emotional well being Ensunng that patientsm ICU have penods of undisturbed rest would also appearto be beneficial
The results of this study cannot be generalized to othersettmgs, such as care of elderly or mentally ill patients, orneonatal care However, the findings raise a number ofmteresting issues for nurses to consider when plannmgC£ire for cntically ill patients It is important tbat nursescontmue to evaluate the effects of complementary therap-ies through well-designed studies usmg appropnateresearch methods, m order to ensure that patient care isbased upon sound evidence rather than m response tocurrent trends or fashion
Acknowledgements
We would like to thank Pat Tseng, who was responsiblefor traimng staff and supervising tbe conduct of tbe therap-ies, all the nursing and medical staff associated with theIntensive Care Umt, Battle Hospital, for their enthusiasm,commitment and support, the patients and their familieswho made the study possible, Mrs Margaret Jones, pre-
viously Director of Nursing Services, Battle Hospital, andMrs Manlyn Collins, Department of Applied Statistics,Umversity of Reading, for help with statistical computmg
References
Bamett K (1972) A survey of the current utilisation of touch byhealth team personnel with hospitalized paUents InternationalJoumal of Nursing Studies 9, 195—208
Birchall A (1990) A whiff of happiness New Scientist127(1731), 45-47
Byass R (1988) Soothing body and soul Nursing Times 84(24),39-41
Clement J M (1983) A descnptive study of the use of touch bynurses with patients m cntical care Doctoral thesis. Universityof Texas, Austin, Texas
CoUett D (1991) Modelling Binary Data Chapman and Hall,London
Eyerman K (1987) Massage Sidgwick and Jackson, LondonFrank LE (1957) TacUle conunumcaUon Genetic Psychology
Monographs 56(2), 211-251Hamson A (1986) Cetting the massage Nursing Times 82(48),
34-35HoUinger L (1980) Perception of touch in the elderly Joumal of
Cerontologicol Nursing, Dec (6), 742-746Kaufman M A (1964) Autonomic responses as related to nursing
comfort measures Nursing Research 13(1), 45-55Longworth J C (1982) Psychophysiological effects of slow stroke
back massage in nonnatensive females Advances m NursingScience 4(4), 45-47
McCorkle R (1974) Effects of touch on seriously ill peopleNursing Research 23(2), 125
Meyer B C , Blacher R S & Brown F (1961) A clinical study ofpsychiatnc and psychological aspects of mitral surgeryPsychosomatic Medicine 23(3), 194-218
Montagu A (1971) Touching The Human Significance of theSkin Columbia Umversity Press, New York
O'BnenD & Alexanders (1985) High Dependency Nursing CareChurchill Livingstone, Edinburgh
Passant H (1990) A hohstic approach on the ward Nursing Times86(4), 26-28
Pearson A (1988) Pnmary Nursing — Nursing m the Burford andOxford Development Umts Chapman and Hall, London
Rubin R (1963) The matemal touch Nursing Outlook Nov (2),828-831
Simms S (1986) Slow stroke back massage for cancer patientsNursing Times 32(18), 47-50
Tattum A (1992) The gentle touch Nursing Times 8(3), 16-17Teasdale C & Jennett B (1974) Assessment of coma and impaired
consciousness a practical scale The Lancet u, 81-84Tisserand R (1989) Essential Oil Safety Data Manual Tisserand
Institute, BnghtonValnet J (1986) The Practice of Aromatherapy C W Daniel,
Saffron WaldenWeiss SJ (1979) The language of touch Nursing Research
28(2), 76-80Wise R (1989) Flower power Nursing Times 85(22), 45-47Worrell J D (1977) Nursmg implications of sensory deprivaUon
In Advanced Concepts m Clinical Nursing 2nd edn (Kintze-Gorman K ed), Lippincott, Philadelphia, pp 618-638
40
