self management support
TRANSCRIPT

Patrick McGowan, PhD
University of Victoria
Describe self-management support
Community programs
Self-management support delivered by HCP’s
Effectiveness of self-management support
Lessons learned

Levels of Evidence
Ia – Evidence from meta-analysis or systematic review of randomized controlled trials.
Ib – Evidence from at least one randomized controlled trial.
IIa – Evidence from at least one well-designed controlled study without randomization.
IIb – Evidence from at least one other type of well-designed quasi-experimental study without randomization.
III – Evidence from well-designed non-experimental descriptive studies, such as comparative studies, correlation studies and case studies.
IV – Evidence from expert committee or opinions and/or clinical experiences of respected authorities.

Clinicians are present for only a fraction of the patient’s life.(Barlow, 2003)
Motivation is not enough. People also need self-confidence and certain skills that we can model and teach.
Nearly all outcomes are mediated through the patient’s behavior. (Bodenheimer et al., 2002)

Determinants of Health and
Their Contribution to Premature
Death
Schroeder, NEJM 357; 12
15%
5%
10%
40%
30% Social
Environmental
Medical
Behavioral
Genetic



There is no single commonly agreed definition of self-management support!


Problem solving
Decision making
Resource utilization
Patient-provider relationships
Taking action
Self-management refers to the behaviours that individuals engage in outside the health care context.
Self-management support refers to how individuals are supported in their self-management goals and activities by health care professionals.
Self-management support is defined as the
systematic provision of education and
supportive interventions by health care staff
to increase patients’ skills and confidence in
managing their health problems, including
regular assessment of progress and problems,
goal setting, and problem-solving support.
Independent variable Dependent variable
Self-management - intervention Self-management - outcomes
- strategies used by HCP’s - skills
- peer led self-management programs - attitudes
- behaviours


Self-Management Support Programs Aim to Change Patient Behavior
Self-management support programs assume a complex sequence of effects. Developers expect these programs to change patients’ behavior by increasing the patients’ self-efficacy and knowledge.
This sequence of assumptions gives self-management support programs multiple objectives and multiple endpoints for evaluation.
The pivotal objective, however, is to change people’s behavior.

Self-Management Support - Sequence
Self-management intervention
↓↑Patient’s confidence ↑knowledge & skills
↓↑Patient’s behaviour*
↑Health professional’s behaviour
↓↑Disease control
↓↑Health outcomes
↓Healthcare utilization
↓↑Patient satisfaction
↓Costs
RAND 2007
*Pivotal objective is to change people’s behaviour

“One’s belief that one can perform a specific behaviour or task in the future.”
Dr. Albert Bandura
• whether one even considers changing a health behaviour
• how much one benefits from the changed behaviour
• how well one maintains the change achieved
• how vulnerable one is to relapse

Self-efficacy Enhancing Strategies
Self-efficacy: Health outcomes
• Mastery Learning
• Modeling
• Reinterpreting Symptoms
• Persuasion

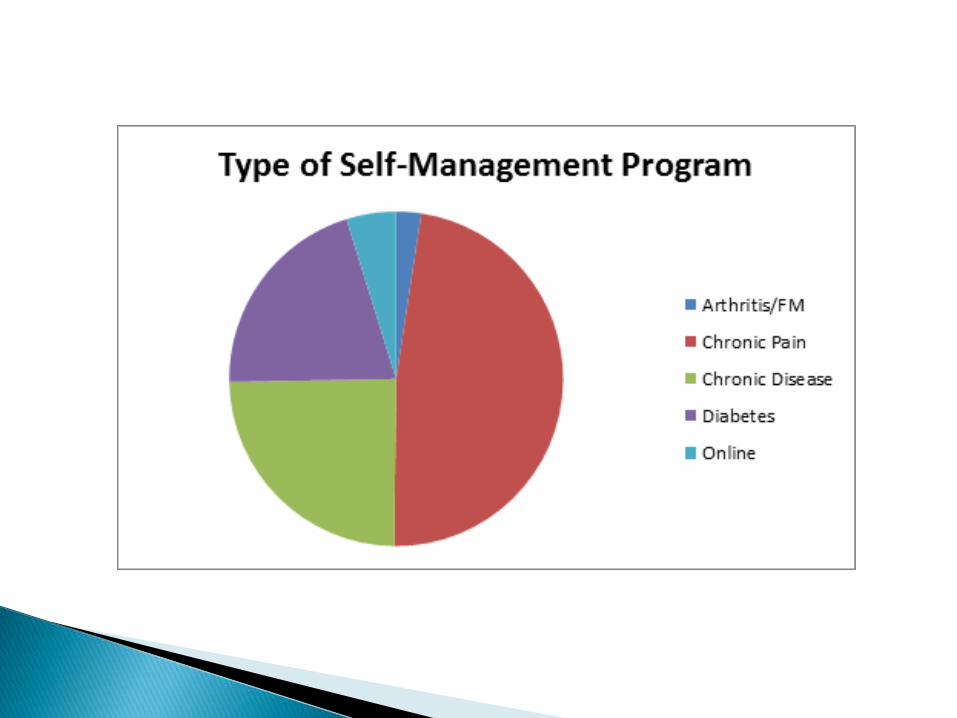
The Chronic Disease Self-Management Program (in English, Chinese, Punjabi)
The Chronic Pain Self-Management Program (in English)
The Diabetes Self-Management Program (in English, Chinese, Punjabi)
The Arthritis/Fibromyalgia Self-Management Program (in English)
The Active Choices Program (in English)
The Online Chronic Disease Self-Management Program (in English)



Self-Management Programs
1. Persons with any type of chronic health conditions
2. Self-referral
3. Spouses and significant others may participate
4. Led by pairs of lay persons with chronic health conditions
5. Leaders receive a 4-day training workshop

6. Leaders follow a scripted Leader’s Manual
7. Course is given once a week for 2 ½ hours for 6 weeks
8. Ideal class size is 10 to 12 persons
9. Participants receive “Living a Healthy Life with Chronic Conditions” workbook
10. No cost to participants


What do people learn in self-management programs?
Information
• From the program
• From other participants
Practical Skills
• Getting started skills (e.g., exercise)
• Problem-solving skills
• Communication skills
• Working with health care professionals
• Dealing with anger/fear/frustration

Practical Skills (cont’d)• Dealing with depression• Dealing with fatigue• Dealing with shortness of breath• Evaluating treatment optionsCognitive Techniques• Self-talk• Relaxation techniques


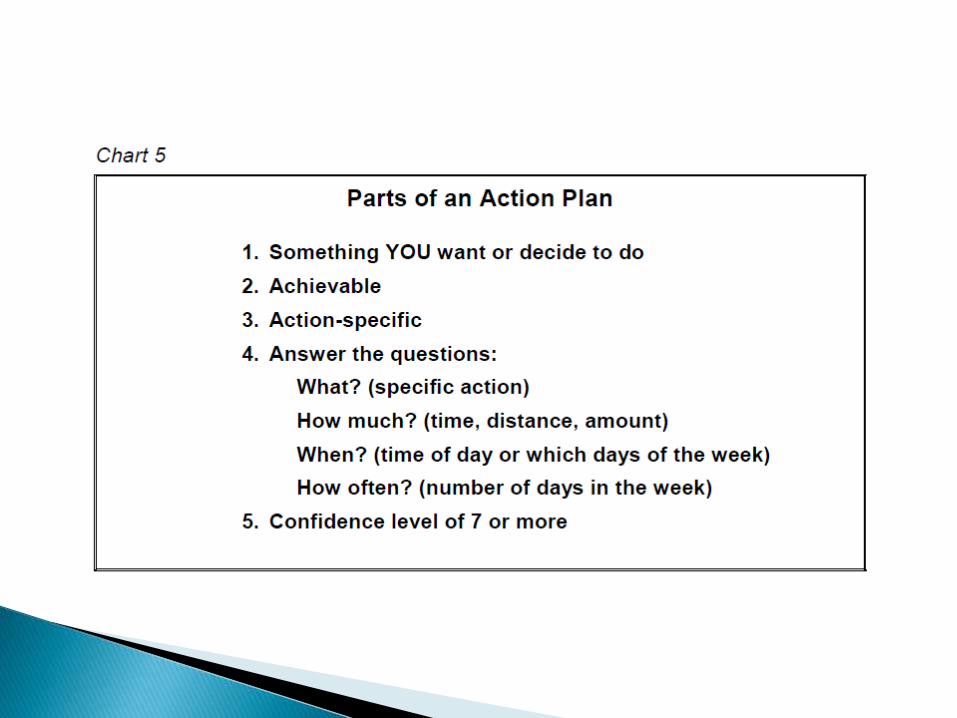
Problem solving
Action plans
Making decisions



Conducted 496 four-day leader training workshops
Trained 4843 Program Leaders
Leaders conducted 2382 six-week self-management programs
To 27,259 persons with chronic health conditions
Self-management is a Minimal Intervention Strategy
Minimal interventions are defined as those interventions that
yield varied therapeutic effects with little expense in time or
money and have few side effects.
Rose, 1985; Hovell et al.,1986; Geller et al., 1991.











Percentage of British Columbians with chronic health
conditions who will have access to self-management
education programs
Goal: 75% in 2010
Access = the program is offered at least once
a year within a 50 km radius
Result87% of population in communities
of 3,000+ had access.

Treatment
Group
Control
Group Difference (%)
11. East Kootenay $54,128 $55,493 -$1,365 -2.5%
12. Kootenay Boundary $50,391 $50,587 -$196 -0.4%
13. Okanagan $50,731 $51,183 -$452 -0.9%
14. Thompson Cariboo Shuswap $53,357 $51,480 $1,877 3.6%
21. Fraser East $53,110 $54,440 -$1,330 -2.5%
22. Fraser North $59,326 $60,123 -$797 -1.3%
23. Fraser South $63,489 $65,348 -$1,859 -2.9%
31. Richmond $58,006 $56,005 $2,001 3.5%
32. Vancouver $57,943 $56,946 $997 1.7%
33. North Shore / Coast Garibaldi $65,114 $68,621 -$3,507 -5.2%
41. South Vancouver Island $58,342 $60,797 -$2,455 -4.1%
42. Central Vancouver Island $50,231 $50,954 -$723 -1.4%
43. North Vancouver Island $54,798 $53,688 $1,110 2.0%
51. Northwest $58,127 $53,728 $4,399 7.9%
52. Northern Interior $59,030 $57,897 $1,133 1.9%
53. Northeast $64,019 $65,274 -$1,255 -1.9%
OVERALL MEAN $56,939.19 $57,578.33 -$639 -1.1%
Standard Error of Mean $162.06 $93.95 $187.33
Mean Family Income of Persons in the Treatment and Control Groups in HSDA’s

Mean family incomes, St Errors and confidence intervals for Treatment and Control Groups
Mean Family Income St Error of MeanTreatment Group $56,939.19 $162.06Control Group $57,578.33 $93.95Difference -$639.14 $187.33
Conclusion There is only a 1.1% difference between the mean income of CDSMP participants and controls. People who take the CDSMP have similar mean family incomes as people who do not take the CDSMP in every Health Service Delivery Area.

Self-management support by health care professionals


ACTION
PLANS
PROBLEM
SOLVING
MAKING
DECISIONS
COMMUNICATION
SKILLS
ASSESSING
READINESS &
STRATEGIES
STANFORD
GROUP
PROGRAMS
BRIEF
ACTION
PLANNING
5 A’s
M.I.
CHOICES &
CHANGES



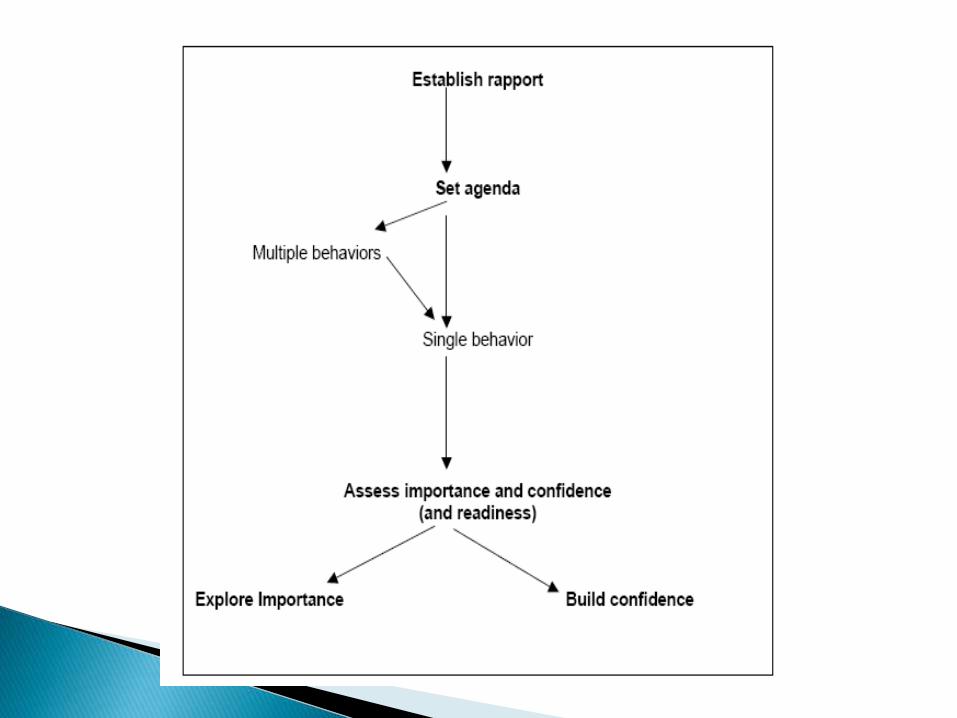
1. Assess Establish rapport
Establish visit agendaAssess client readinessUse health risk appraisals
2. Advise Ask-tell-ask
Closing the Loop
3. Agree Action plans and follow-up
4. Assist Motivational Interviewing
Teach problem solvingAwareness of community resources
5. Arrange Follow-up
I. Self-efficacy, knowledge, experience, empowerment and satisfaction with care
II. Patient engagement in more “healthy” behaviours or general behaviour change
III. Clinical and quality of life outcomes
IV. Cost and resource implications for health and social services

Evidence of impact tends to be greatest for self-efficacy and weakest for health care utilization and costs
however…
Outcomes vary depending on the type of intervention and health condition of the target patient group

Some studies suggest that the evidence for supporting self-management is only moderate but this is because a wide range of activity is described as ‘self-management support’ and some interventions may be more effective than others.

Levels of Evidence
Ia – Evidence from meta-analysis or systematic review of randomized controlled trials.
Ib – Evidence from at least one randomized controlled trial.
IIa – Evidence from at least one well-designed controlled study without randomization.
IIb – Evidence from at least one other type of well-designed quasi-experimental study without randomization.
III – Evidence from well-designed non-experimental descriptive studies, such as comparative studies, correlation studies and case studies.
IV – Evidence from expert committee or opinions and/or clinical experiences of respected authorities.


Self-management works
This review of more than 550 pieces of high quality research suggests that it is worthwhile to support self-management, in particular through focusing on behaviour change and supporting self-efficacy.
Whilst the findings of individual studies are mixed, the totality of evidence suggests that supporting self-management can have benefits for people’s attitudes and behaviours, quality of life, clinical symptoms and use of healthcare resources.




The 5A’s approach to Self-Management Support
1. Getting patients to complete a Health Risk Appraisal at home. Thisprovides an opportunity for patients to obtain independent objectiveinformation about their health and what they need to do to address theseconcerns. The information the client receives from the appraisal is discussed with the health professional. Ib
2. Assessing the patient’s readiness to change a behavior. This helps thehealth professional to use an appropriate behaviour change strategy withthe patient. III
3. Setting a visit agenda with patients ensures that both the health professionals’ and patients’ concerns are addressed in the visit. IIb
4. Establishing rapport with patients – ensures patients have opportunitiesto express their priority concerns. III

4. Teaching patients how to make action plans helps patients start and maintain a behaviour. Ia
5. The problem-solving process teaches the patient a process they can use to solve problems when they arise in their daily lives. Ia
6. Ensuring that follow-up takes place facilitates the success of making action plans. Ia
7. Appropriately trained nurses should use motivational interviewing. Ia
8. The “ask-tell-ask” strategy is a technique to ensure the patient gets the information he/she is after. III
9. The “closing the loop” technique is used to ensure the patient understands the information provided by the health professional. III


Activation refers to people’s ability and willingness to take on the role of managing their health and health care.
The Patient Activation Measure (PAM) was designed to assess an individual’s knowledge, skill and confidence in managing their health.
PAM segments people into one of four progressively higher level of activation.



- Increased patient participation was associated with higher PAM scores
- Patients with higher PAM scores reported significantly better health and significantly lower rates of doctor office visits, emergency room visits, and hospital nights
- Individuals with higher PAM scores are significantly more likely to exhibit healthy behaviours
- PAM scores were strongly associated with improved adherence to treatment
- PAM score was strongly associated with doctor-patient communication

At 6-months post program the proportion of participants:
- who were in Level 1 at baseline had decreased by 11%;- who were In Level 2 at baseline had decreased by 9%;- who were In Level 3 at baseline had decreased by 8%; and- who were In Level 4 at baseline had increased by 27%.

1. Tools alone are not enough
2. Offer people a range of support options, so they can select to suit their preferences and needs
3. Recognize that people are different, and tailor interventions appropriately
4. Changing professional roles, behaviours and mindsets is vital, challenging, but not impossible
5. Train whole teams, not just individuals
6. Engage health care professionals as change agents

7. Work with the voluntary and community sector
8. Local context is a vital factor in implementation
9. Use a whole system approach to implementing
10. Have a change strategy in place from the start, one that is clear about goals but flexible on implementation
11. Consider sustainability from the outset
12. Evaluation should be designed into change processes from the start, balancing robustness and feasibility considerations
Health care professional characteristics
- mindsets and preconceptions
- concerns about risk
- knowledge of wider support services

Senior level support and ongoing commitment
Core team to drive change
Alignment with wider priorities and agendas
IT systems and system capacity
Supportive commissioning and payment systems

Toll-free line:
1-866-902-3767
Web site:
www.selfmanagementbc.ca
Contact Information




Shared Decision Making
Shared decision making is both a philosophy and a process. It requires a partnership between patients and professionals, working together to select tests, treatments and support packages based on patient preferences, clinician experience and research evidence.

are both underpinned by the same principles and expectations for respect and collaboration between patients and professionals
neither can be successful without a more equal distribution of power in the professional-patient relationship
“working with” rather than “doing for”
