selective serotonin reuptake inhibitors 2016
TRANSCRIPT

Mohamed sedky
Selective Serotonin Reuptake Inhibitors
(SSRIs)
Psychiatric specialistBMHH2016

Introduction
• SSRIs are a class of antidepressants used mainly in the treatment of depression and anxiety disorders.
• They are the most commonly prescribed group of antidepressants.antidepressants.
• SSRIs increase the extracellular level of the neurotransmitter serotonin by inhibiting its reuptake into the presynaptic cell.

• The first drug in the SSRI class was Prozac (Fluoxetine), which hit the United States market in 1987. Prozac was FDA approved in December 29, 1987. It is manufactured by Eli Lilly and Company.
• Subsequently other SSRIs were introduced.
History
SSRI YEARSSRI YEAR
Fluoxetine 1987
Sertraline 1992
Paroxetine 1993
Fluvoxamine 1994
Citalopram 1998
Escitalopram 2002
Chemical Structure
• These compounds are structurally unrelated.
• This may account for the differential response we see in some patients with one antidepressant vs. another.some patients with one antidepressant vs. another.
• Rationale for differential response may be related to different morphology of the serotonin transport protein.

Paroxetine
O
OO
CH2
HN
CH3
SSRI Structures
O
NC
CH2CH2CH2N(CH3)2·HBr
Fluvoxamine
F3C C CH2 CH2 CH2 CH2 O CH3
N
O CH2 CH2 NH2
N
Fluoxetine
O CH
CH2 CH2 N
CH3
H
Sertraline
Cl
Cl
CitalopramEscitalopram F

• SSRIs Inhibit serotonin reuptake so increase synaptic serotonin levels.
• Clinical effect usually takes weeks so mechanism goes beyond simply increasing synaptic serotonin levels.
Mechanism of action
levels.
• Serotonin receptors are located throughout the body (especially GI tract).

Mechanism of action
- inhibition of 5-HT reuptake- ↑ of postsynapt. 5-HT1A sensitivity

Licensed indication of SSRIs
Citalopram Escitalopram Fluoxetine Fluvoxamine Paroxetine Sertraline
Major depressive disorder
√ √ √ √ √ √
Generalized anxiety disorder
√ √ √
Social anxiety disorders
√ √ √disorders
OCD √ √ √ √ √
PTSD √ √
Panic disorder ±Agoraphobia
√ √ √ √
Premenstrual dysphoric disorder
√ √ √ √
Bulimia nervosa √
Off-label indications of SSRIs
• Bipolar depression
• Psychosomatic conditions
• Irritable bowel syndrome (IBS)
• Menopausal symptoms
• Premature ejaculation• Premature ejaculation
• Migraine headache prophylaxis
• Chronic headache
• Musculo-skeletal pain
• Fibromyalgia

• Absorption – Well absorbed orally and have peak effects in the range of 3-8 hrs. Absorption of Sertraline may be slightly increased by food.
• Distribution – Differences in plasma protein binding percentages; with Sertraline, Fluoxetine & Paroxetine most highly bound; & Escitalopram least bound.
Pharmacokinetics
least bound.
• Metabolism – All SSRIs are metabolized in the liver by CYP 450 enzymes.
Wide Therapeutic Index-So their concentration not affected by other drugs. But, potential for slowing/blocking the metabolism of many drugs.

• Elimination
Pharmacokinetics
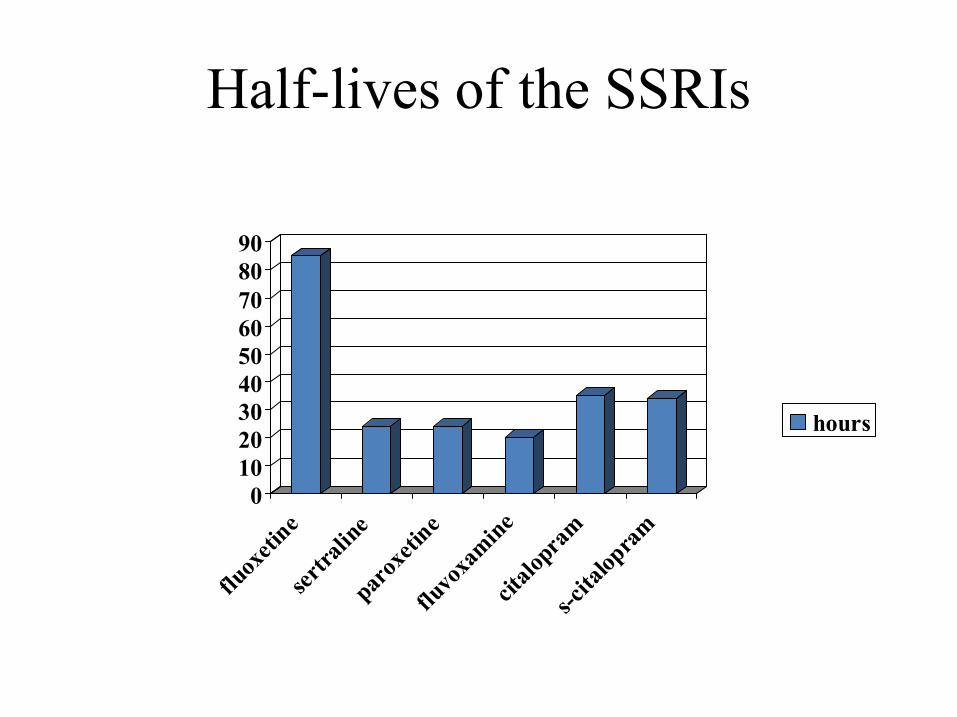
Drug Half-life
1. Fluoxetine 4-6 days
Norfluoxetine (Active Metabolite) 7-9 days
2. Citalopram 35 hours2. Citalopram 35 hours
3. Escitalopram 27-32 hours
4. Sertraline 26 hours
(Less active metabolite) 3-5 days
5. Paroxetine 21 hours
6. Fluvoxamine 15 hours
Half-lives of the SSRIs
5060708090
01020304050
fluox
etin
e
sert
ralin
e
parox
etin
e
fluvo
xam
ine
cital
opra
m
s-cita
lopra
m
hours
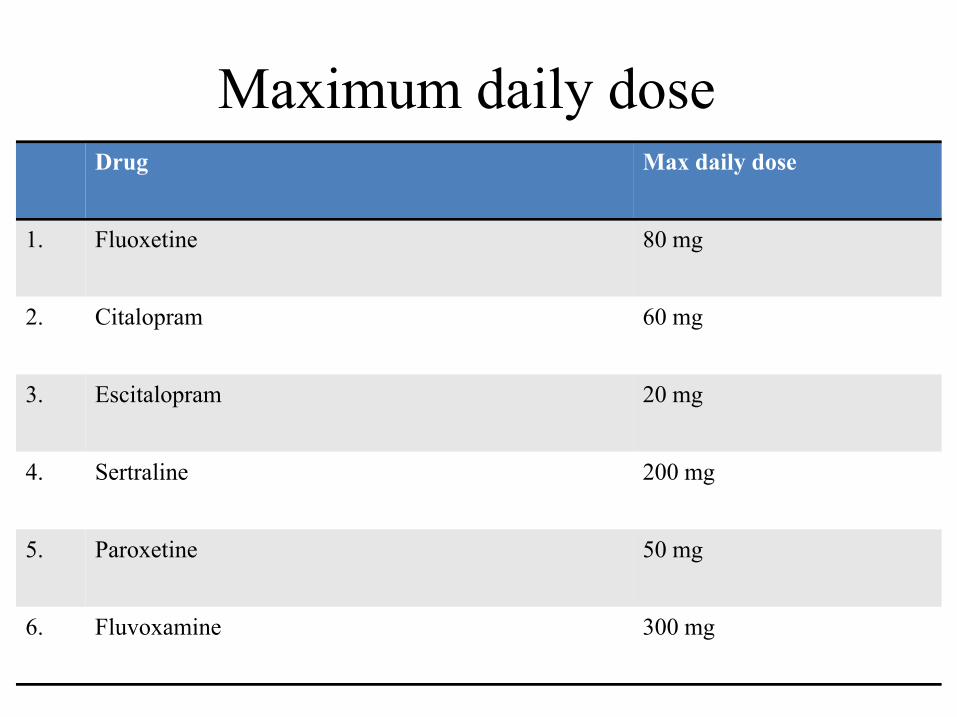
Maximum daily doseDrug Max daily dose
1. Fluoxetine 80 mg
2. Citalopram 60 mg
3. Escitalopram 20 mg
4. Sertraline 200 mg
5. Paroxetine 50 mg
6. Fluvoxamine 300 mg


SSRIs Selectivity
SSRIs specifically inhibit serotonin reuptake, having300- to 3000-fold greater selectivity for the serotonintransporter as compared to the norepinephrinetransporter.transporter.
As a class, SSRIs have little affinity for cholinergic,β-adrenergic or histamine receptors.

Selectivity for 5-HT vs. NE Transporter
500600700800900
0100200300400500
fluox
etin
e
sertr
alin
e
paro
xetin
e
fluvo
xam
ine
citalo
pram
s-cita
lopr
am
selectivity
Richelson E, Synaptic Effects of Antidepressants, Journal of Clinical Psychopharmacology,Vol. 16, No3, Suppl. 2, June 1996
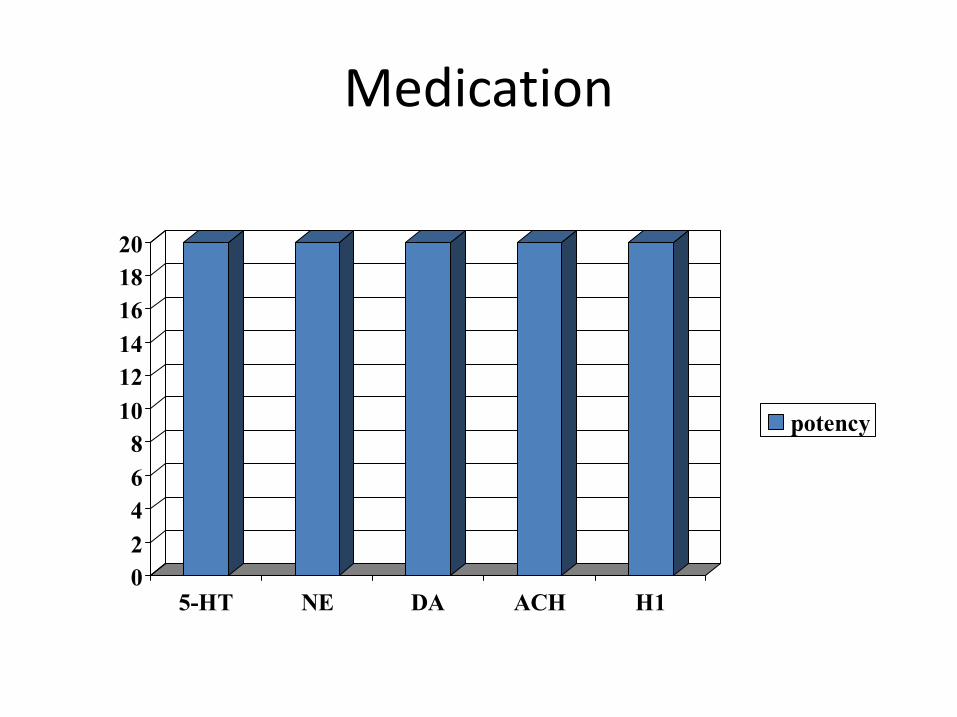
Medication
14
16
18
20
0
2
4
6
8
10
12
14
5-HT NE DA ACH H1
potency

Fluoxetine (Prozac)
6
7
8
9
0
1
2
3
4
5
6
5-HT NE DA ACH H1
potency
Richelson E, Synaptic Effects of Antidepressants, Journal of Clinical Psychopharmacology,Vol. 16, No3, Suppl. 2, June, 1996

Sertraline (Lustral)
20
25
30
0
5
10
15
20
5-HT NE DA ACH H1
potency
Richelson E, Synaptic Effects of Antidepressants, Journal of Clinical Psychopharmacology,Vol. 16, No3, Suppl. 2, June, 1996

paroxetine (Seroxat)
100
120
140
0
20
40
60
80
5-HT NE DA ACH H1
potency
Richelson E, Synaptic Effects of Antidepressants, Journal of Clinical Psychopharmacology,Vol. 16, No3, Suppl. 2, June, 1996
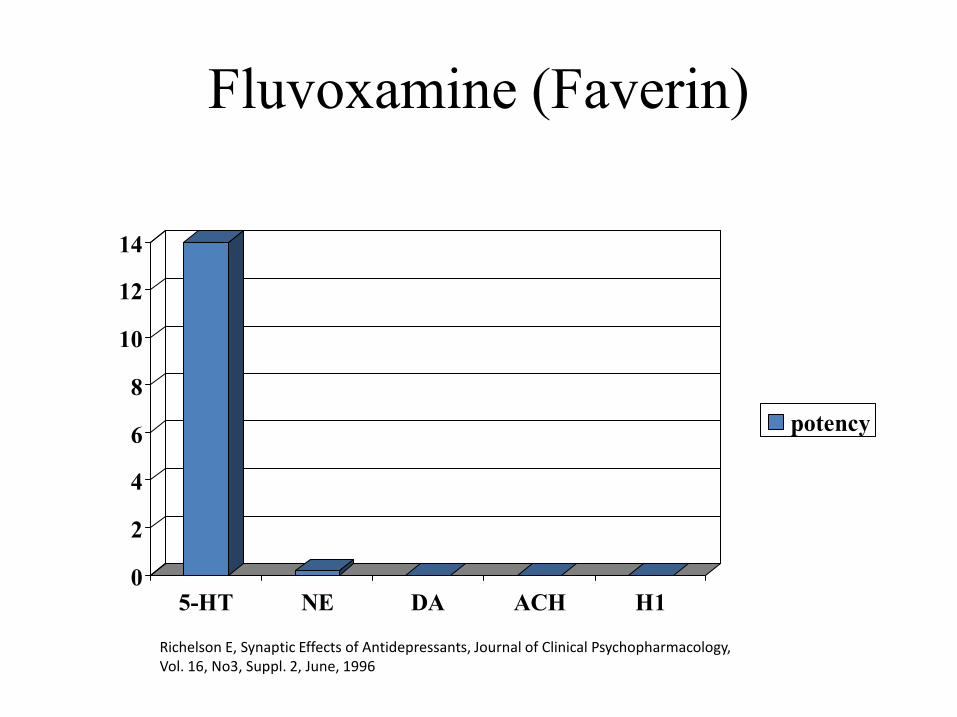
Fluvoxamine (Faverin)
10
12
14
0
2
4
6
8
5-HT NE DA ACH H1
potency
Richelson E, Synaptic Effects of Antidepressants, Journal of Clinical Psychopharmacology,Vol. 16, No3, Suppl. 2, June, 1996

Citalopram (Cipram)
1.4
1.6
1.8
2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
5-HT NE DA ACH H1
potency

Escitalopram (Cipralex)
20
25
30
0
5
10
15
20
5-HT NE DA ACH H1
East
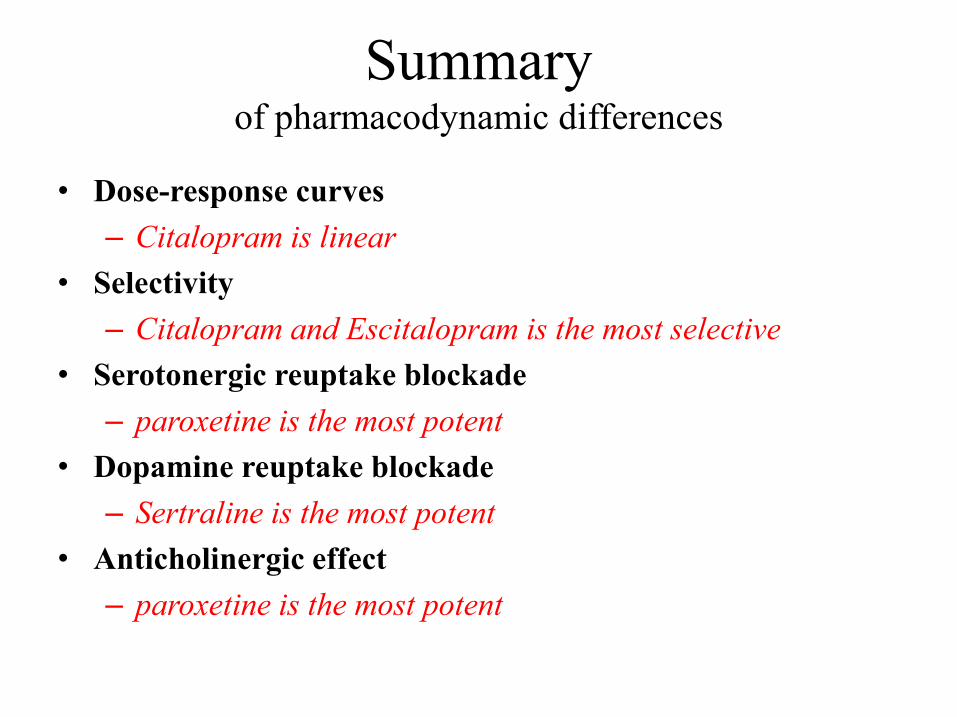
Summaryof pharmacodynamic differences
• Dose-response curves
– Citalopram is linear
• Selectivity
– Citalopram and Escitalopram is the most selective
• Serotonergic reuptake blockade• Serotonergic reuptake blockade
– paroxetine is the most potent
• Dopamine reuptake blockade
– Sertraline is the most potent
• Anticholinergic effect
– paroxetine is the most potent
drug-drug interactions
The SSRIs are potent inhibitors of the CYP450.
The potential for drug-drug interactions differssignificantly across the SSRIs.significantly across the SSRIs.
Fluvoxamine, Paroxetine and Fluoxetine are potentCYP2D6 inhibitors responsible for the elimination ofTCA drugs, neuroleptic drugs, and someantiarrhythmic and β-adrenergic antagonist drugs.
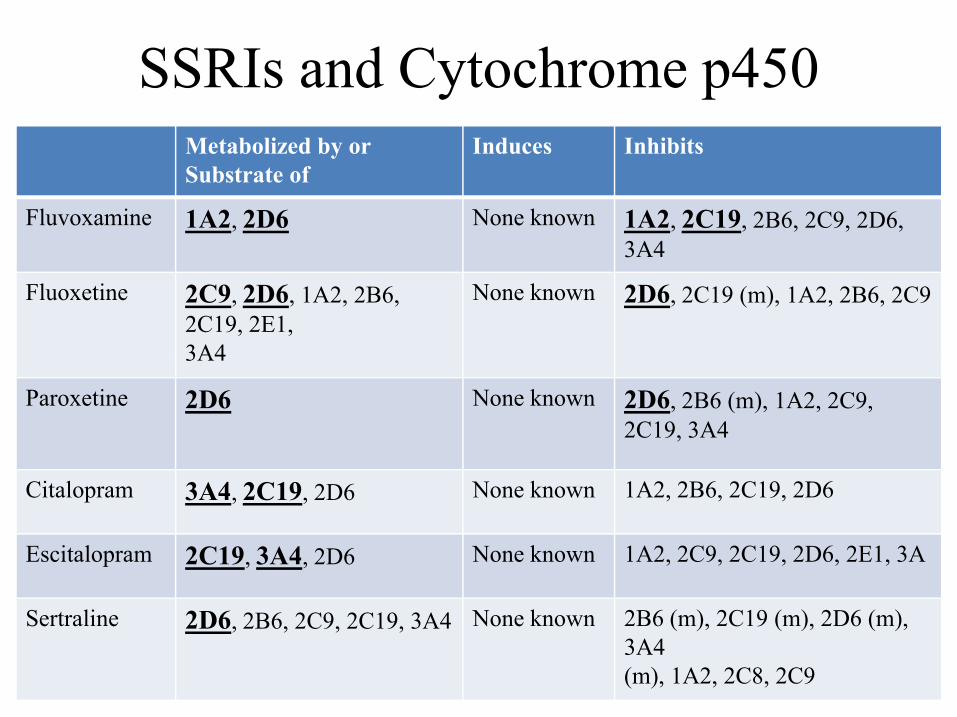
SSRIs and Cytochrome p450Metabolized by or Substrate of
Induces Inhibits
Fluvoxamine 1A2, 2D6 None known 1A2, 2C19, 2B6, 2C9, 2D6, 3A4
Fluoxetine 2C9, 2D6, 1A2, 2B6, 2C19, 2E1, 3A4
None known 2D6, 2C19 (m), 1A2, 2B6, 2C9
3A4
Paroxetine 2D6 None known 2D6, 2B6 (m), 1A2, 2C9, 2C19, 3A4
Citalopram 3A4, 2C19, 2D6 None known 1A2, 2B6, 2C19, 2D6
Escitalopram 2C19, 3A4, 2D6 None known 1A2, 2C9, 2C19, 2D6, 2E1, 3A
Sertraline 2D6, 2B6, 2C9, 2C19, 3A4 None known 2B6 (m), 2C19 (m), 2D6 (m), 3A4 (m), 1A2, 2C8, 2C9
Fluoxetine (Prozac)
Pros Long ½ life so:
• Good for pts with medication noncompliance issues.• decreased incidence of discontinuation syndromes.• can be used to taper someone off SSRI when trying to prevent SSRI Discontinuation
Syndrome.• Once daily dosing (or even day after day).• Once daily dosing (or even day after day).
Initially activating so may provide increased energy.
Cons Long ½ life + active metabolite ↑ build-up of metabolites (e.g. not a
good choice in patients with hepatic illness). Significant P450 interactions so this may not be a good choice in pts
already on a number of meds (increased seizure risk with clozapine). Initial activation may increase anxiety and insomnia.
Sertraline (Lustral)
Pros Relatively fewer side-effects (watch for GI).
Lower potential for drug-drug interactions (very weak P450 interactions).
Intermediate ½ life + less active metabolite lower build-up of metabolites.metabolites.
Less sedating when compared to paroxetine.
Cons Max absorption requires a full stomach.
Increased number of GI adverse drug reactions (associated with a higher incidence of diarrhoea than other SSRI).

Paroxetine (Seroxat)
Pros Short ½ life + No active metabolite No build-up of metabolites.
Sedating properties (dose at night) offers good initial relief from anxiety and insomnia.
Available in sustained release form. Available in sustained release form.
Cons Likely to cause a discontinuation syndrome (short ½ life ).
Worst side effect profile (sedation, weight gain, sexual dysfunction and anticholinergic side effects).
Potential for drug-drug interactions (Significant CYP2D6 inhibition).

Fluvoxamine (Faverin)
Pros Short ½ life + No active metabolite No build-up of metabolites.
Found to possess some analgesic properties.
Cons Likely to cause a discontinuation syndrome (short ½ life ).
Side-effect profile is relatively worse (GI distress, headaches, sedation, weakness).
Strong inhibitor of CYP1A2 and CYP2C19 (Highest potential for drug-drug interactions with increased serum levels of Agomelatine and theophylline).

Citalopram (Cipram)
Pros Lower potential for drug-drug interactions (Low inhibition of P450
enzymes).
Fewer side effects at low doses.
Intermediate ½ life ( once daily dosing). Intermediate ½ life ( once daily dosing).
Cons Dose-dependent QT interval prolongation with doses of 10-40mg/day
(doses of >40mg/day needs monitoring of QT interval).
Can be sedating (has mild antagonism at H1 histamine receptor).
GI side effects (less than Sertraline).

Escitalopram (Cipralex)
Pros Low overall inhibition of P450s enzymes so fewer drug-drug
interactions.
Intermediate ½ life ( once daily dosing).
More effective than Citalopram in acute response and remission. More effective than Citalopram in acute response and remission.
Cons Dose-dependent QT interval prolongation with doses of 10-30mg daily
(doses of >30mg/day needs monitoring of QT interval).
Nausea, headache.
Adverse Effects Of SSRIs
Most common
Nausea (esp. Sertraline)
Sexual Dysfunction (esp. paroxetine & Sertraline)
Headache (esp. Fluoxetine)
Vomiting
Dry mouth (esp. paroxetine)
Abdominal pain

Adverse Effects Of SSRIs
Weight changes: Weight gain (esp. paroxetine)
Or Weight loss (esp. Fluoxetine)
Increased risk of Bleeding
Discontinuation syndrome (esp. paroxetine & Fluvoxamine)
Increased potential for drug-drug interaction (esp. Fluvoxamine)
Risks during pregnancy: Teratogenicity
Persistent pulmonary hypertension
Neonatal withdrawal syndrome

Adverse Effects Of SSRIsMental and behavioral side effects
Apathy and Emotional blunting
Paradoxical anxiety (esp. Fluoxetine & Sertraline)
Nervousness
Irritability Irritability
Akathisia / restlessness
Suicidality (emergence of suicidal ideation)
Hypomania or mania (manic switching)
Abnormal dreaming

Adverse Effects Of SSRIsCentral & Peripheral Nervous System side effects
Sleep disturbance : Insomnia (esp. Fluoxetine)
Somnolence (esp. paroxetine & Fluvoxamine)
excessive dreaming
Headache (esp. Fluoxetine)
Dizziness
Yawning
Paraesthesia
Tremor
Extrapyramidal disorder
Adverse Effects Of SSRIsGastro-Intestinal System side effects ( esp. Sertraline and Fluvoxamine )
Nausea
Vomiting
Constipation
Diarrhoea Diarrhoea
Anorexia
Abdominal pain
Dyspepsia
Flatulence
Dry mouth
Adverse Effects Of SSRIs
Cardiovascular side effects
QT- Prolongation and Torsade de Pointes ( esp. Citalopram & Escitalopram)
Palpitation
Autonomic side effects
Increased sweating
Flushing
Adverse Effects Of SSRIs
Rare Adverse Effects
Serotonin syndrome
Hyponatraemia (probably more of an issue in the elderly)
hyperprolactinemia
Galactorrhea
Mammary hypertrophy and gynaecomastia
Extrapyramidal symptoms
Seizure (esp. Fluoxetine ≥ 100mg/ day)
Sexual Dysfunction
• Clinical rates approximate 50% of patients.
• Paroxetine and Sertraline appear to cause higher rates of sexual dysfunction in most head to head studies.of sexual dysfunction in most head to head studies.
SSRIs Affect all phases of the sexual response
Sexual Dysfunctions occurring in male includes:
Decreased libido
Erectile dysfunction
Delayed orgasm
Penile anaesthesia
Painful ejaculation
Priapism
Sexual Dysfunctions occurring in female includes
Decreased libido
Delayed orgasm
Decreased vaginal lubrication
Vaginal anaesthesia
Dyspareunia
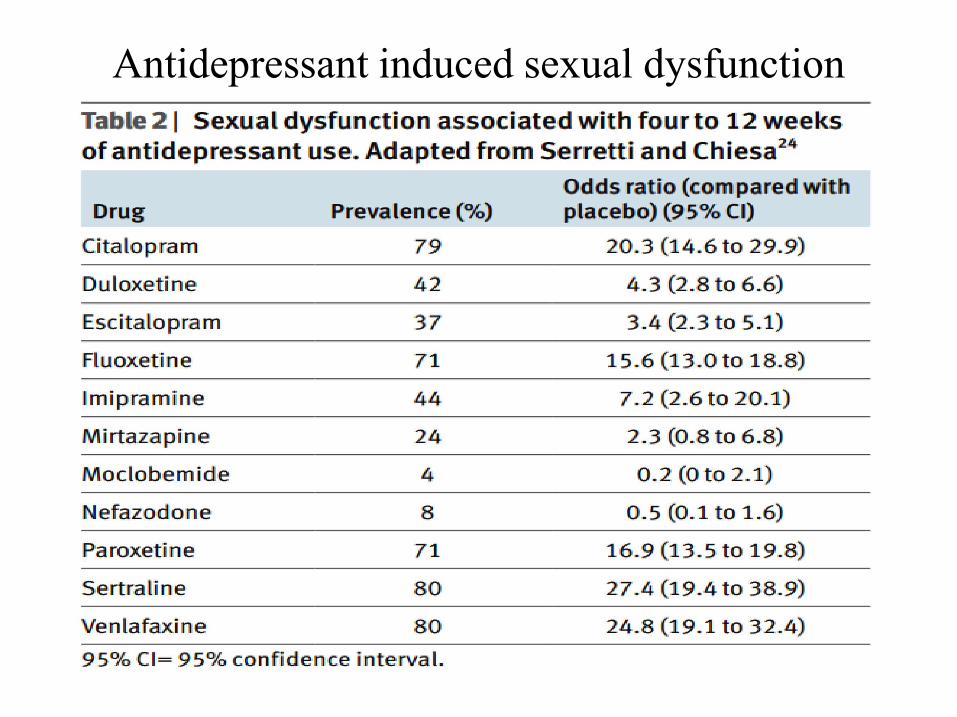
Antidepressant induced sexual dysfunction

‘strategies for managing sexual dysfunction induced by antidepressant medication’
Reduce the dose
Delayed dosing
Drug ‘holidays’ Drug ‘holidays’
Switch to a different antidepressant that is less likely to cause the specific sexual problem experienced (e.g. Bupropion and Agomelatine).
Adding adjunctive or ‘antidote’ drugs: Bupropion, Mirtazapine, Trazodone, Sildenafil (Viagra) and Tadalafil (Snafi).
Serotonin Syndrome
• Administration of an SSRI in presence of another highly presence of another highly serotonergic drug life-threatening ‘serotonin syndrome’

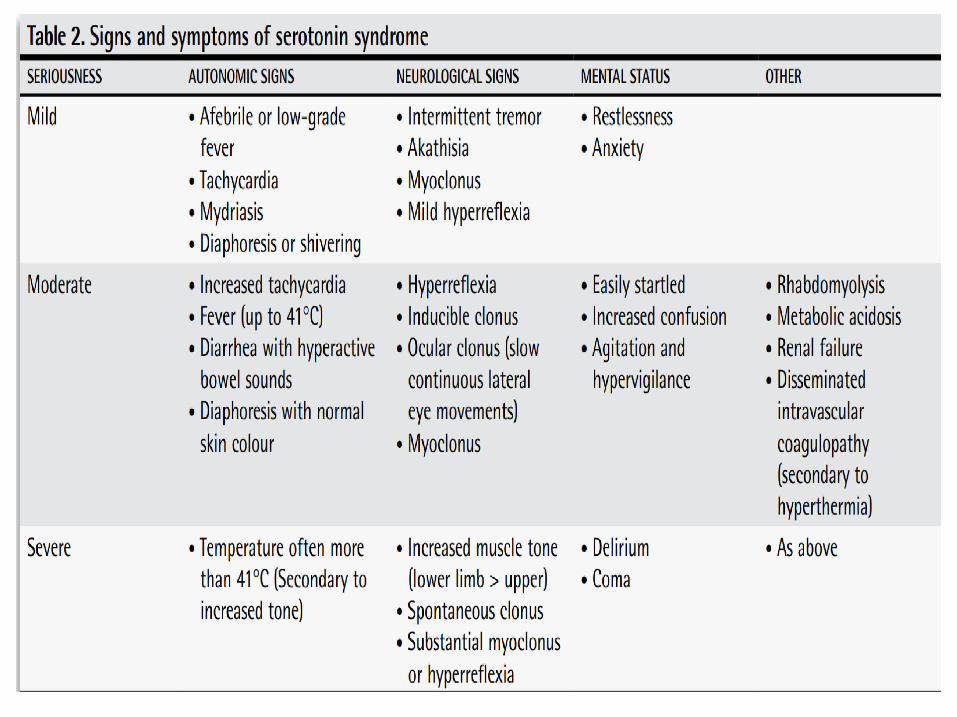
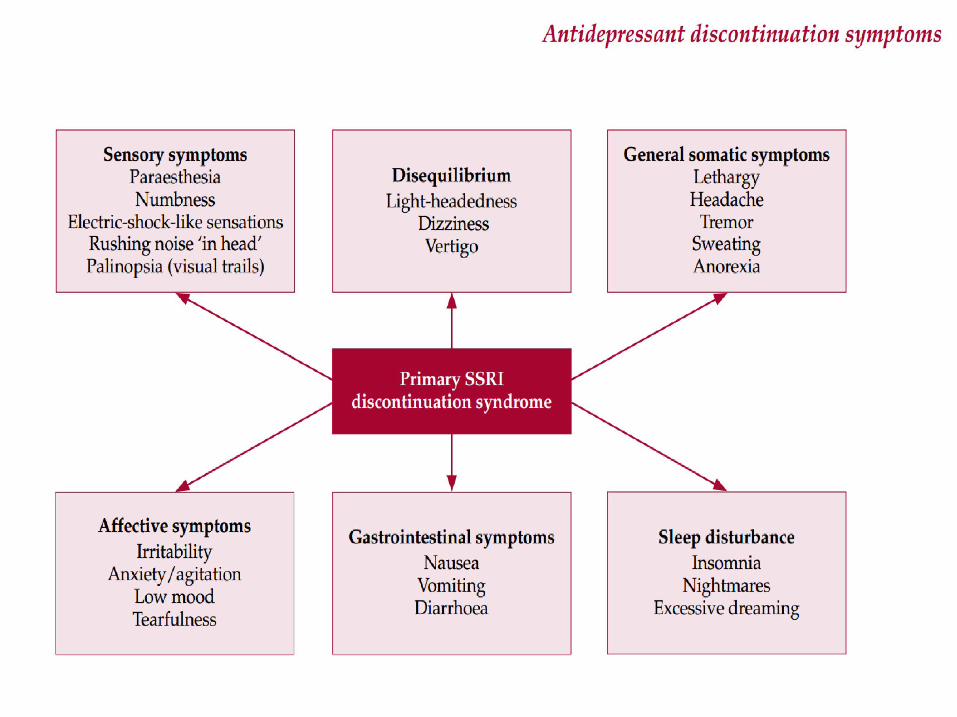
Manifestations of serotonin syndrome
– NEURO: Myoclonus, Nystagmus, Headache, Tremors, Rigidity and Seizures.
–MENTAL STATE: Irritability, Confusions, –MENTAL STATE: Irritability, Confusions, Agitations, Hypomania and Coma.
– AUTONOMIC: Hyperpyrexia, sweating, diarrhea, cardiac arrythmia and death.

Management of serotonin syndrome
Discontinuation of all serotonergic agents
Supportive care aimed at normalization of vital signs (oxygen and intravenous fluids, continuous cardiac monitoring, and correction of vital signs).monitoring, and correction of vital signs).
Sedation with benzodiazepines
Administration of serotonin antagonists (Cyproheptadine)
SSRI discontinuation syndrome
Occurs on abrupt withdrawal of SSRIs.
Agents with short half-lives (Paroxetine/ Fluovoxamine), inactive metabolites abrupt washout higher risk.
So, Fluoxetine lowest risk for discontinuation syndrome.
No definitive pathophysiologic explanation.

SSRI discontinuation syndrome
experienced by at least a third of patients.
Doesn’t appear until at least 6 weeks of treatment & The onset of symptoms is usually within 3 days of stopping treatment and usually resolves spontaneously within 2 weeks.
‐ They are usually mild and self‐limiting (but can occasionally be severe
and prolonged).
the most commonly reported symptoms include: dizziness, nausea, lethargy, headache, electric shock-like sensations, sweating, , insomnia and tremor.

Management
If symptoms are mild reassurance.
If symptoms are severe:If symptoms are severe:Reintroduce the original antidepressant.
Or another with a longer half‐life (e.g. Fluoxetine).
SSRIs and bleeding
SSRIs will deplete platelet serotonin, leading to a reduced ability to form clots and a subsequent increase in the risk of bleeding.
SSRIs also increase gastric acid secretion and therefore may be irritant to the gastric mucosa. Use of SSRIs seems to increase the risk of peptic ulcer.
SSRIs increase the risk of GIT, cerebral and perioperative bleeding (those undergoing orthopaedic or breast surgery may be at greatest risk).
Risk is increased still further in those also receiving aspirin, NSAIDs or oral anticoagulants.

SSRIs and bleeding
SSRI + ASPIRIN, NSAIDs increases the risk of GIT bleeding.
SSRI + oral anticoagulants increases the risk of Non GIT bleeding.
Try to avoid SSRIs in patients receiving NSAIDs, aspirin or oral anticoagulants or with history of cerebral or GI bleeds.
If SSRI use cannot be avoided (in any anticoagulated or aspirin‐treated patient), monitor closely and prescribe gastroprotective proton pump inhibitors.
In patients taking Warfarin, suggest Citalopram or Escitalopram (probably lowest interaction potential).
Cardiac effects of SSRIs
SSRIs are generally safe in cardiac disease.
But, be aware of antiplatelet activity and ‐ ‐
But, be aware of antiplatelet activity and cytochrome‐mediated interactions with co‐administered cardiac drugs.

Cardiac effects of SSRIsDrug Heart rate Blood pressure QTc Arrhythmia Conduction
disturbancLicensed restrictions post M
Comments
Fluoxetine Small decrease in mean heart rat
Minimal effect on blood pressur
No effect on QTcinterval
None None caution. Clinical experience is limited
Evidence of safety post MI
Fluvoxamine Minimal effect on heart rate
Small drop in systolic blood pressure
No significant effect on QTc
None None Caution Limited changes in ECG have been observed
Paroxetine Small decrease in mean heart rate
Minimal effect on blood pressure
No effect on QTcinterval
None None General caution in cardiac patients
Probably safe post MI
Sertraline Minimal effect on heart rate
Minimal effect on blood pressure
No effect on QTcinterval
None None None – drug of choice
Safe post MI and inheart failure
Citalopram(assume same for escitalopram)
Small decrease inheart rate
Slight drop in systolic blood pressure
Dose‐related increase in QTc
Torsades de pointesreported, mainly in overdose
None Caution but some evidence of safety in cardiovascular disease
Minor metabolite which may ↑ QTcinterval. No clear evidence of increased risk of arrhythmia at any licensed dose

Use of SSRIs In Special Patient GroupsIn Special Patient Groups

Special patient groups
Pregnancy All SSRIs are rated pregnancy category C, with the exception of
paroxetine, which is a category D.
There is most experience with Sertraline and Fluoxetine
Paroxetine may be less safe than other SSRIs. Paroxetine may be less safe than other SSRIs.
Breast Feeding Sertraline is the drug of choice followed by Paroxetine.

Special patient groupsGeriatric• SSRIs are Safe & well tolerated in geriatric population.
• Minimal cardiotoxic, anticholinergic, antihistaminic or α adrenergic adverse effects except for Paroxetine which has some anticholinergicactivity.
PaediatricPaediatric

Special patient groups
Renal Impairment No agent clearly preferred to another.
However Citalopram and Sertraline are suggested as reasonable choices.
Hepatic ImpairmentHepatic Impairment Fluoxetine (longer half life) to be avoided.
Citalopram & Escitalopram have minimal effects on hepatic enzymes so they are SSRIs of choice.

Special patient groups
Diabetes Mellitus Fluoxetine has been associated with improvement in HbA 1c levels,
reduced insulin requirements, weight loss and enhanced insulin sensitivity.
Hypertention No agent clearly preferred to another (Minimal effect on blood pressure).
Special patient groups
Cardiac Disorders Sertraline is recommended.
but other SSRIs are also likely to be safe.
Caution with Citalopram and Escitalopram (Dose‐related increase in QTc, especially with overdose).
‐especially with overdose).
Post Stroke Depression Fluoxetine, Citalopram are the most studied and seem to be effective and
safe and widely recommended for post-stroke depression.
Stroke can be embolic or haemorrhagic –SSRIs may protect against the former and provoke the latter.

Special patient groups
Parkinson’s Disease SSRIs are considered to be first-line treatment.
Motor symptoms may be worsened (low risk).
SSRIs + Selegiline → Risk of Serotonin Syndrome
Epilepsy For SSRIs, the risk is generally considered to be low if no predisposing
factor is seen and it is not significantly different from the incidence of first seizure in the general population.
Reports of seizure with Fluoxetine and Citalopram overdose.
Special patient groups
Cancer Pts Sertraline, Escitalopram are preferred due to least risk of drug
interaction.
Dementia the most common antidepressants used in dementia are sertraline followed
by citalopram.
citalopram up to 30 mg/day for agitation ??
