sedation and analgesia - robert wood johnson medical...
TRANSCRIPT

Sedation and AnalgesiaSedation and Analgesia
Hariprem Rajasekhar, MDHariprem Rajasekhar, MDAssistant ProfessorAssistant Professor
Division of Critical Care Medicine Division of Critical Care Medicine -- Department of PediatricsDepartment of PediatricsUMDNJUMDNJ--RWJMS, New Brunswick, NJRWJMS, New Brunswick, NJ

GoalsGoalsWhy discuss sedation and analgesia? Why discuss sedation and analgesia? GuidelinesGuidelinesDefinitionsDefinitionsLevels of sedationLevels of sedationPharmacologyPharmacologyWrap upWrap up

ABP Content SpecificationsABP Content SpecificationsXXXII PharmacologyXXXII PharmacologyC. Pain ManagementC. Pain Management
1. Minimal sedation (anxiolytic) 1. Minimal sedation (anxiolytic) 2. Moderate sedation 2. Moderate sedation
–– Understand the Understand the definitiondefinition of procedural sedation as opposed to deep of procedural sedation as opposed to deep sedation and general anesthesia sedation and general anesthesia
–– Understand what Understand what level of observation and monitoring level of observation and monitoring is is recommended for a patient undergoing procedural sedation recommended for a patient undergoing procedural sedation
–– Recognize Recognize side effectsside effects and signs and symptoms of an and signs and symptoms of an overdosageoverdosage of of commonly prescribed sedatives, and commonly prescribed sedatives, and manage appropriately manage appropriately
–– Understand the Understand the indications and contraindications indications and contraindications for moderate for moderate sedation sedation
–– Understand there should be an appropriate interval of Understand there should be an appropriate interval of fastingfasting before before moderate sedation moderate sedation
3. Sedative analgesia (3. Sedative analgesia (egeg, opioids, nitrous oxide, ketamine) , opioids, nitrous oxide, ketamine) 4. Non4. Non--pharmacologic techniques (pharmacologic techniques (egeg, biofeedback, hypnosis, distraction) , biofeedback, hypnosis, distraction)

Real world applicationReal world applicationSedation/analgesia may be needed to facilitate: Sedation/analgesia may be needed to facilitate: –– Imaging (CT/MRI)Imaging (CT/MRI)–– ER procedures (laceration repair) ER procedures (laceration repair) –– Outpatient procedures (bone marrow biopsy) Outpatient procedures (bone marrow biopsy)
Residents may be called to provide sedation in some of these Residents may be called to provide sedation in some of these settings.settings.

What can go wrong?What can go wrong?Deeper sedation than intendedDeeper sedation than intended
Most complications are due to airway/respiratory compromise. Most complications are due to airway/respiratory compromise.
Majority can be managed by supplemental O2, opening airway, Majority can be managed by supplemental O2, opening airway, suctioning, bag mask ventilation. suctioning, bag mask ventilation.
Occasionally need to intubate/place LMA.Occasionally need to intubate/place LMA.

Initial guidelinesInitial guidelinesAAPD/ASA guidelines for pediatric sedationAAPD/ASA guidelines for pediatric sedation–– First published in 1985 in response to 3 deaths in a single dentFirst published in 1985 in response to 3 deaths in a single dental al
office involved with dental sedation.office involved with dental sedation.
Guidelines addressed: informed consent, fasting, vital sign Guidelines addressed: informed consent, fasting, vital sign measurements, age appropriate equipment, BLS skills, recovery anmeasurements, age appropriate equipment, BLS skills, recovery and d discharge criteriadischarge criteria
Three levels of sedation:Three levels of sedation:–– conscious sedation conscious sedation –– deep sedationdeep sedation–– general anesthesiageneral anesthesia

Later guidelinesLater guidelinesAAP Committee on Drugs:AAP Committee on Drugs:–– Guidelines for Monitoring and Management of Pediatrics Patients Guidelines for Monitoring and Management of Pediatrics Patients
During and After Sedation for Diagnostic and Therapeutic During and After Sedation for Diagnostic and Therapeutic ProceduresProcedures
–– 1992 statement and 2002 addendum1992 statement and 2002 addendum–– 2006 addendum with AAPD2006 addendum with AAPD
ASA Task Force on Sedation and Analgesia by NonASA Task Force on Sedation and Analgesia by Non--Anesthesiologists:Anesthesiologists:–– Practice Guidelines for Sedation and Analgesia by NonPractice Guidelines for Sedation and Analgesia by Non--
AnesthesiologistsAnesthesiologists–– 1995 statement and 2002 updated report1995 statement and 2002 updated report

US Pharmacopoeia Report of Adverse EventsUS Pharmacopoeia Report of Adverse Events
1000+ pediatric specialists in survey. 95 adverse events from bo1000+ pediatric specialists in survey. 95 adverse events from both th hospital and nonhospital reviewed. hospital and nonhospital reviewed.
51 deaths, 9 neurologic injury, 21 prolonged hospital stay, 14 n51 deaths, 9 neurologic injury, 21 prolonged hospital stay, 14 no o harmharm
80% of complications during sedation/analgesia are secondary to 80% of complications during sedation/analgesia are secondary to adverse airway/respiratory events. adverse airway/respiratory events.
Remaining 20%: drug interaction/overdose, inadequate monitoring,Remaining 20%: drug interaction/overdose, inadequate monitoring,inadequate initial health evaluation, lack of independent observinadequate initial health evaluation, lack of independent observer, er, inadequate management of resuscitation. inadequate management of resuscitation.

Pediatric Sedation Research ConsortiumPediatric Sedation Research Consortium
2006 study: 30,000 sedations in 26 institutions for procedures 2006 study: 30,000 sedations in 26 institutions for procedures outside the ORoutside the OR
Dedicated sedation team (anesthesiologists, EM physicians, Dedicated sedation team (anesthesiologists, EM physicians, internists/hospitalists)internists/hospitalists)
No deaths, 1 No deaths, 1 cadiaccadiac arrest, 1 aspiration.arrest, 1 aspiration.
1/400 procedures had stridor, laryngospasm, wheezing, apnea1/400 procedures had stridor, laryngospasm, wheezing, apnea
1/200 procedures required airway/ventilation intervention1/200 procedures required airway/ventilation intervention

Adequately sedated?Adequately sedated?

DefinitionsDefinitionsSedative: Sedative: ““to calmto calm”” (calming of mental excitement or (calming of mental excitement or physiological function)physiological function)
Anxiolytic: Anxiolytic: ““relieving anxietyrelieving anxiety””
Amnestic: Amnestic: ““causing total or partial loss of memorycausing total or partial loss of memory””
Analgesic: Analgesic: ““relieving painrelieving pain””
Anesthetic: Anesthetic: ““general or local insensibility, to pain or other general or local insensibility, to pain or other sensations, with or without loss of consciousnesssensations, with or without loss of consciousness””

•• General DescriptionGeneral Description
•• ResponsivenessResponsiveness
•• AirwayAirway
•• VentilationVentilation
•• CardiovascularCardiovascular
SEDATION LEVELS

MinimalMinimal
•• General DescriptionGeneral Description ““AnxiolysisAnxiolysis””
•• ResponsivenessResponsiveness
•• AirwayAirway
•• VentilationVentilation
•• CardiovascularCardiovascular
““appropriateappropriate””
unaffectedunaffected
unaffectedunaffected
unaffectedunaffected
SEDATION LEVELS
Riskof
AdverseEvent
NoSedation
MildSedation

MinimalMinimal ModerateModerate
•• General DescriptionGeneral Description ““AnxiolysisAnxiolysis”” ““ConsciousConscious””
•• ResponsivenessResponsiveness
•• AirwayAirway
•• VentilationVentilation
•• CardiovascularCardiovascular
““appropriateappropriate””
unaffectedunaffected
unaffectedunaffected
unaffectedunaffected
““PurposefulPurposeful”” to light to light stimulationstimulation
No interventionNo intervention
AdequateAdequate
MaintainedMaintained
SEDATION LEVELS
Riskof
AdverseEvent
NoSedation
MildSedation
ModerateSedation

MinimalMinimal ModerateModerate DeepDeep
•• General DescriptionGeneral Description ““AnxiolysisAnxiolysis”” ““ConsciousConscious”” ““Deep sleepDeep sleep””
•• ResponsivenessResponsiveness
•• AirwayAirway
•• VentilationVentilation
•• CardiovascularCardiovascular
““appropriateappropriate””
UnaffectedUnaffected
UnaffectedUnaffected
UnaffectedUnaffected
““PurposefulPurposeful”” to light to light stimulationstimulation
No interventionNo intervention
AdequateAdequate
MaintainedMaintained
““PurposefulPurposeful”” to pain to pain stimulationstimulation
((±±) Intervention) Intervention
((±±) Inadequate) Inadequate
((±±) Maintained) Maintained
SEDATION LEVELS
Riskof
AdverseEvent
NoSedation
MildSedation
ModerateSedation
DeepSedation

Continuum of Depth of SedationContinuum of Depth of SedationMinimal Sedation (Anxiolysis) a drug-induced state during which patients respond normally to verbal commands. Although cognitive function and coordination may be impaired, ventilatory and cardiovascular functions are unaffected.
Moderate Sedation/Analgesia (Conscious Sedation) a drug-induced depression of consciousness during which patients respond purposefully* to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.
Deep Sedation/Analgesia a drug-induced depression of consciousness during which patients cannot be easily aroused but respond purposefully* following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained.
* Reflex withdrawal from a painful stimulus is not considered a purposeful response.

WeWe’’ve Gone Too Far!ve Gone Too Far!General Anesthesia a drug-induced loss of consciousness during which patients are not arousable, even by painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired.
Because sedation is a continuum, it is not always possible to predict how an individual patient will respond. Hence, practitioners intending to produce a given level of sedation should be able to rescue patients whose level of sedation becomes deeper than initially intended.
Individuals administering Moderate Sedation/Analgesia (Conscious Sedation) should be able to rescue patients who enter a state of Deep Sedation/Analgesia, while those administering Deep Sedation/Analgesia should be able to rescue patients who enter a state of general anesthesia.

Levels of Sedation/AnalgesiaLevels of Sedation/Analgesia

Back to GuidelinesBack to Guidelines15 ASA Recommendations
Preprocedure evaluation Choice of Agents
Patient counseling Dose Titration
Preprocedure fasting Use of induction agents
Monitoring IV access
Personnel Reversal Agents
Training Recovery observation / discharge criteria
Emergency Equipment Special Situations
Supplemental Oxygen

ASA GuidelinesASA Guidelines1. Preprocedure evaluationRelevant history (major organ systems, sedation–anesthesia history, medications, allergies, last oral intake)Focused physical examination (to include heart, lungs, airway)Laboratory testing guided by underlying conditions and possible effect on patient managementFindings confirmed immediately before sedation
2. Patient counselingRisks, benefits, limitations, and alternatives
3. Preprocedure fastingElective procedures—sufficient time for gastric emptyingUrgent or emergent situations—potential for pulmonary aspiration considered in determining target level of sedation, delay of procedure, protection of trachea by intubation

NPO Guidelines ASA NPO Guidelines ASA vsvs AAPAAP
ASA: ASA: 2 2 hrshrs after clears liquidsafter clears liquids4 4 hrshrs after breast milk after breast milk 6 6 hrshrs after anything else (formula)after anything else (formula)
AAP: AAP: Any age Any age 2 2 hrshrs after clearsafter clearsUp to 5 months Up to 5 months 4 4 hrshrs after milk or solidsafter milk or solids6 to 36 months 6 to 36 months 6 6 hrshrs after milk or solidsafter milk or solidsOver 36 months Over 36 months 8 8 hrshrs after milk or solids after milk or solids

ASA GuidelinesASA Guidelines4. Monitoring(Data to be recorded at appropriate intervals before, during, and after procedure) Pulse oximetryResponse to verbal commands when practicalPulmonary ventilation (observation, auscultation)Exhaled carbon dioxide monitoring considered when patients separated from caregiverBlood pressure and heart rate at 5-min intervals unless contraindicatedElectrocardiograph for patients with significant cardiovascular disease
For deep sedation:Response to verbal commands or more profound stimuli unless contraindicatedExhaled CO2 monitoring considered for all patientsElectrocardiograph for all patients

A note on monitoringA note on monitoring
Pulse ox!!!Pulse ox!!!Not always required to have cardiac monitoring, but be Not always required to have cardiac monitoring, but be wary if you are not using it.wary if you are not using it.

ASA GuidelinesASA Guidelines5. PersonnelDesignated individual, other than the practitioner performing the procedure, present to monitor the patient throughout the procedure. This individual may assist with minor interruptible tasks once patient is stableFor deep sedation: The monitoring individual may not assist with other tasks
6. TrainingPharmacology of sedative and analgesic agentsPharmacology of available antagonistsBasic life support skills—presentAdvanced life support skills—within 5 minFor deep sedation: Advanced life support skills in the procedure room

ASA GuidelinesASA Guidelines7. Emergency EquipmentSuction, appropriately sized airway equipment, means of positive- pressure ventilation, intravenous equipment, pharmacologic antagonists, and basic resuscitative medicationsDefibrillator immediately available for patients with cardiovascular diseaseFor deep sedation: Defibrillator immediately available for all patients
8. Supplemental OxygenOxygen delivery equipment availableOxygen administered if hypoxemia occursFor deep sedation: Oxygen administered to all patients unless contraindicated

ASA GuidelinesASA Guidelines9. Choice of AgentsSedatives to decrease anxiety, promote somnolenceAnalgesics to relieve pain
10. Dose TitrationMedications given incrementally with sufficient time between doses to assess effectsAppropriate dose reduction if both sedatives and analgesics usedRepeat doses of oral medications not recommended
11. Use of anesthetic induction agents (methohexital, propofol)Regardless of route of administration and intended level of sedation, patients should receive care consistent with deep sedation, including ability to rescue from unintended general anesthesia
12. Intravenous AccessSedatives administered intravenously—maintain intravenous accessSedatives administered by other routes—case-by-case decisionIndividual with intravenous skills immediately available

ASA GuidelinesASA Guidelines13. Reversal AgentsNaloxone and flumazenil available whenever opioids or benzodiazepines administered
14. RecoveryObservation until patients no longer at risk for cardiorespiratory depressionAppropriate discharge criteria to minimize risk of respiratory or cardiovascular depression after discharge
15. Special SituationsSevere underlying medical problems—consult with appropriate specialist if possibleRisk of severe cardiovascular or respiratory compromise or need for complete unresponsiveness to obtain adequate operating conditions—consult anesthesiologist

ASA Discharge criteriaASA Discharge criteriaAlert and oriented / baseline patient. (Car seat forward Alert and oriented / baseline patient. (Car seat forward head rolling risk with head rolling risk with pedspeds))Stable vitals WNLStable vitals WNLMay use scoring systemsMay use scoring systemsSufficient time (up to 2 Sufficient time (up to 2 hrshrs) if reversal agents were used) if reversal agents were usedOutpatients discharged with responsible adult Outpatients discharged with responsible adult supervisionsupervisionOutpatients and escorts discharged with written Outpatients and escorts discharged with written instructions regarding diet, meds, activity, phone instructions regarding diet, meds, activity, phone number.number.

AAP Discharge criteriaAAP Discharge criteria
Cardiovascular function and airway patency satisfactory Cardiovascular function and airway patency satisfactory and stableand stableEasily Easily arousablearousable patient with protective reflexes intactpatient with protective reflexes intactPatient can talk and sit up unaided (if age appropriate) / Patient can talk and sit up unaided (if age appropriate) / baseline for childbaseline for childAdequate hydration status.Adequate hydration status.

PrePre--op completeop completeABP Content SpecsABP Content SpecsRisks of sedation/analgesiaRisks of sedation/analgesiaContinuum of levels of sedationContinuum of levels of sedationGuidelines for providing sedation/analgesiaGuidelines for providing sedation/analgesia
Start counting backwards from 10….

PharmacologyPharmacology
Pharmacokinetics (What the body does to the drug)Pharmacokinetics (What the body does to the drug)–– Study of drug deposition over timeStudy of drug deposition over time
AbsorptionAbsorptionDistributionDistributionMetabolism Metabolism EliminationElimination
Pharmacodynamics (What the drug does to the body)Pharmacodynamics (What the drug does to the body)–– Relationship between the concentration of drug at the site Relationship between the concentration of drug at the site
of action and the physiologic responseof action and the physiologic response
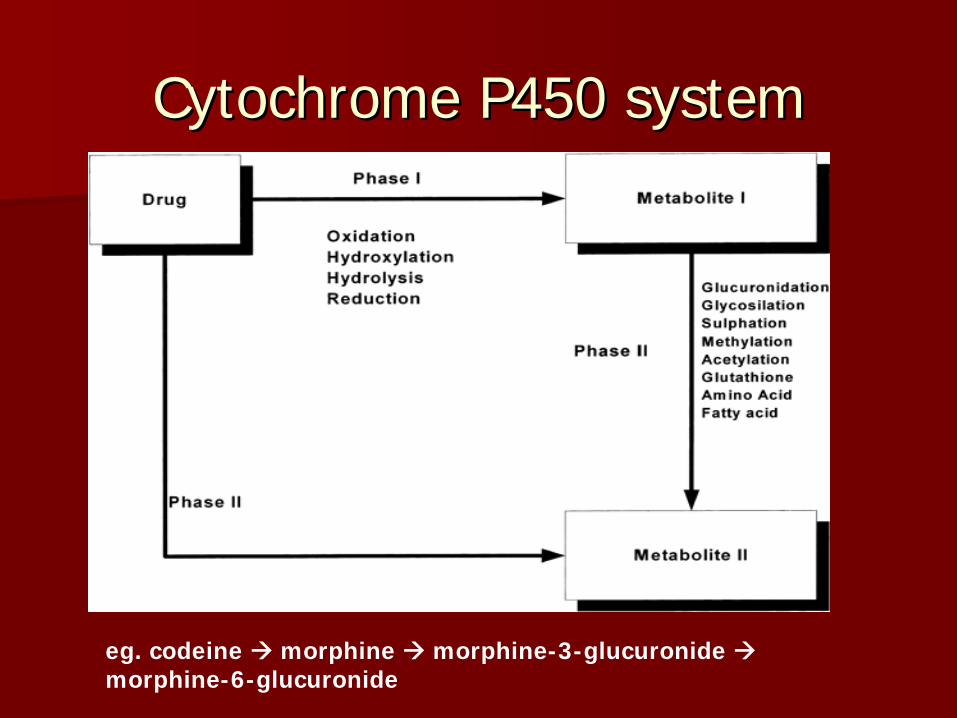
Cytochrome P450 systemCytochrome P450 system
eg. codeine morphine morphine-3-glucuronide morphine-6-glucuronide

Kearns GL, Abdel-Rahman SM, et al. Developmental pharmacology--drug disposition, action, and therapy in infants and children N Engl J Med. 2003 Sep 18;349(12):1157-67

Managing PainManaging Pain
Definition of Pain: Definition of Pain: ““an unpleasant sensory and emotional an unpleasant sensory and emotional experience associated with actual or potential tissue damage experience associated with actual or potential tissue damage or described terms of such damageor described terms of such damage””–– International Association for the Study of Pain, late 1970sInternational Association for the Study of Pain, late 1970s
Wong-Baker Scale

Physiology of PainPhysiology of Pain
NociceptionNociceptionPeripheral APeripheral Aδδ and C fibers send and C fibers send signals to spinal cord and signals to spinal cord and brainstem which relays brainstem which relays information to higher cortical information to higher cortical centerscenters

Do children deal with pain same as Do children deal with pain same as adults?adults?
All nerve pathways for conduction of painful stimuli and awareneAll nerve pathways for conduction of painful stimuli and awareness of ss of pain are formed by 24 weeks of gestationpain are formed by 24 weeks of gestation
Failure to manage painful stimuli increases pain for future evenFailure to manage painful stimuli increases pain for future eventsts–– Pain in the newbornPain in the newborn–– Postoperative PainPostoperative Pain–– Chronic PainChronic Pain

AcetaminophenAcetaminophen
Analgesic, antipyreticAnalgesic, antipyreticCOX 3 inhibitionCOX 3 inhibition15 mg/kg every 415 mg/kg every 4--6 6 hrhr PO, PRPO, PROnset of action: 30 minutesOnset of action: 30 minutesCeiling effectCeiling effectHepatotoxicityHepatotoxicity

NSAIDsNSAIDs
IbuprofenIbuprofen–– 10 mg/kg every 8 10 mg/kg every 8 hrhr PO PO
KetorolacKetorolac–– 0.5 mg/kg every 60.5 mg/kg every 6--8 8 hrhr for 3for 3--5 days5 days
COX 1, COX 2 inhibitorsCOX 1, COX 2 inhibitorsGI irritation, platelet dysfunctionGI irritation, platelet dysfunction

OpiatesOpiatesActivate CNS descending tractsActivate CNS descending tracts–– via via μ1 μ1 –– supraspinalsupraspinal analgesiaanalgesia–– via via μ2 μ2 –– respiratory depression, GI effectsrespiratory depression, GI effects–– via via κ κ –– analgesia, sedation, analgesia, sedation, miosismiosis, , dysphoriadysphoria–– via via δ δ -- analgesiaanalgesia
Reversal agent availableReversal agent availablePCA PCA

OpiatesOpiates
CodeineCodeineMorphineMorphineFentanylFentanylHydromorphoneHydromorphone
HydrocodoneHydrocodoneMethadoneMethadoneOxycodoneOxycodoneMeperidineMeperidine

FentanylFentanyl
Quick onset: < 1 minQuick onset: < 1 minDuration: 30Duration: 30--45 min45 minConsidered most Considered most hemodynamicallyhemodynamically stablestable0.50.5--1 mcg/kg IV 1 mcg/kg IV 0.50.5--2 mcg/kg/2 mcg/kg/hrhr IVIVUseful in BM biopsy, Chest Useful in BM biopsy, Chest tube placement, Fracture tube placement, Fracture ReductionReduction
100x more potent than 100x more potent than morphinemorphineHighly lipophilicHighly lipophilicLiver (Liver (glucuronidationglucuronidation), ), renal excretionrenal excretionRigid chest syndromeRigid chest syndrome–– At doses above 5 At doses above 5
mcg/kg and with rapid mcg/kg and with rapid titrationtitration
MorphineMorphine
Onset: < 5 minutesOnset: < 5 minutesDuration: 3Duration: 3--5 5 hrshrs0.1 mg/kg IV0.1 mg/kg IVIV:PO 1:3IV:PO 1:3Metabolized by liver to MMetabolized by liver to M--66--G (active) G (active)
In newborns and In newborns and ptspts with with decdec GFR, watch for GFR, watch for prolonged effect and prolonged effect and resprespdepressiondepressionHistamine release, Histamine release, bronchospasmbronchospasm

HydromorphoneHydromorphone
Rapid onsetRapid onsetDuration: 4Duration: 4--6 6 hrshrsMorphine derivativeMorphine derivativeMorphine alternativeMorphine alternative
55--20 mcg/kg IV20 mcg/kg IV33--5 mcg/kg hr IV5 mcg/kg hr IVHalfHalf--life: 3life: 3--4 hr4 hr

MethadoneMethadone
Long half lifeLong half lifeLong duration (days)Long duration (days)Metabolized to morphineMetabolized to morphineWithdrawalWithdrawal
Useful for postoperative Useful for postoperative pain, intractable painpain, intractable pain0.1 mg/kg every 60.1 mg/kg every 6--8 8 hrhrPO/IVPO/IVDecent oral bioavailabilityDecent oral bioavailability

Levels of Sedation/AnalgesiaLevels of Sedation/Analgesia

Providing minimal sedationProviding minimal sedationMinimal sedation (Minimal sedation (anxiolysisanxiolysis))–– Peripheral nerve blocksPeripheral nerve blocks–– Local / topical anesthesiaLocal / topical anesthesia
Interferes with impulse conduction of peripheral nerve fibers byInterferes with impulse conduction of peripheral nerve fibers byinhibiting Na channelsinhibiting Na channels
LidocaineLidocaine with or without epinephrinewith or without epinephrine–– No epinephrine at end arterial sites No epinephrine at end arterial sites egeg digitsdigits–– Max dose 4.5 mg/kg (7 mg/kg with Max dose 4.5 mg/kg (7 mg/kg with epiepi))
Topical Topical lidocainelidocaine//prilocaineprilocaine creamcream–– Apply with occlusive dressing 30Apply with occlusive dressing 30--60 min prior to procedure60 min prior to procedure

Providing Moderate SedationProviding Moderate Sedation
Are you prepared?Are you prepared?
S S -- SuctionSuctionO O -- OxygenOxygenA A -- Airway equipmentAirway equipmentP P -- Pharmacologic agentsPharmacologic agentsM M -- MonitorsMonitorsE E -- EquipmentEquipment

© 2007 American Association of Critical‐Care Nurses. Published by Lippincott Williams & Wilkins, Inc.
Perspectives on Sedation Assessment in Critical Care. Olson,
DaiWai; BSN, RN; Thoyre, Suzanne; PhD, RN; Auyong, DavidAACN Advanced Critical Care. 18(4):380‐395, October/December
2007. DOI: 10.1097/01.AACN.0000298630.53276.be
Table 1 : Ramsay Scale With the Response Variable Underlined
Ramsay Sedation ScaleRamsay Sedation Scale

SedativesSedatives
BenzodiazepinesBenzodiazepinesBarbituratesBarbituratesChloral HydrateChloral HydratePropofolPropofolKetamineKetamineαα--2 Agonists2 Agonists

BenzodiazepinesBenzodiazepines
AmnesiaAmnesiaAnticonvulsantAnticonvulsantSedativeSedativeHypnoticHypnoticSkeletal muscle relaxantSkeletal muscle relaxantAugments GABA (brain) and Augments GABA (brain) and glycine (brain stem and glycine (brain stem and spinal cord) transmissionspinal cord) transmission
Reduce cerebral metabolism Reduce cerebral metabolism and blood flowand blood flowCombined with narcotics, Combined with narcotics, respiratory depression respiratory depression and/or hemodynamic and/or hemodynamic instability can occurinstability can occurAntagonist (flumazenil)Antagonist (flumazenil)Withdrawal after prolonged Withdrawal after prolonged infusioninfusion

BenzodiazepinesBenzodiazepines
Midazolam (Versed)Midazolam (Versed)–– Ultra short acting, Ultra short acting,
potent sedative, potent sedative, anxiolytic and amnesticanxiolytic and amnestic
–– NO analgesiaNO analgesia–– 0.05 mg/kg 10.05 mg/kg 1--2 2 hrshrs, IV, IM, IV, IM–– Can be given PO, rectally Can be given PO, rectally
or or intranasallyintranasally at higher at higher dosesdoses
–– 0.5 mg/kg PO 200.5 mg/kg PO 20--30 30 minutes prior to procedureminutes prior to procedure
–– CYT p450 metabolism in CYT p450 metabolism in liverliver
LorazepamLorazepam (Ativan)(Ativan)–– 0.050.05--0.1 mg/kg q 40.1 mg/kg q 4--6 6 hrshrs, ,
IV, IM, POIV, IM, PO–– 0.05 mg/kg/0.05 mg/kg/hrhr, titrate to , titrate to
effecteffect

Opiates + BenzodiazepinesOpiates + Benzodiazepines
Probably why the combination of opiates and benzodiazepines is used so frequently in critical care

BarbituratesBarbituratesGABA agonists, CNS depressant, provides sedation without analgesGABA agonists, CNS depressant, provides sedation without analgesiaiaHistorically used pentobarbital, thiopental and Historically used pentobarbital, thiopental and secobarbitalsecobarbitalPentobarbital has been used as premed for cardiac catheterizatioPentobarbital has been used as premed for cardiac catheterizationn–– IV onset 3IV onset 3--5 minutes, duration 305 minutes, duration 30--60 minutes60 minutes
Significant disadvantages Significant disadvantages –– Not much used anymoreNot much used anymore–– Respiratory depressionRespiratory depression–– HypotensionHypotension–– Bronchospasm, pruritus due to histamine releaseBronchospasm, pruritus due to histamine release–– Can enhance pain perceptionCan enhance pain perception–– No reversal agentNo reversal agent

Chloral HydrateChloral HydrateHypnotic, Sedation, Hypnotic, Sedation, AnxiolysisAnxiolysis, NO analgesia, NO analgesiaPO, PR administrationPO, PR administration5050--100 mg/kg 100 mg/kg Onset 15Onset 15--30 minutes, can last up to 12 hours 30 minutes, can last up to 12 hours longer monitoring!longer monitoring!Useful in children less than 3 Useful in children less than 3 yrsyrs for noninvasive proceduresfor noninvasive proceduresDisadvantagesDisadvantages–– AlcoholAlcohol–– No reversal agentNo reversal agent

KetamineKetamineDissociative anesthetic - blocks association pathways, sometimes inducing dreamlike states of mind and hallucinations before it produces a sensory blockade.
Ketamine produces both analgesia and sedation at moderate doses,while usually maintaining airway tone.
Useful in Laceration repairs, Central line placement.
Sympathomimetic effects increase heart rate and blood pressure, secretions. Consider atropine or glycopyrrolate prior to ketamine adminstration.
Emergence hallucinations: Midazolam can be administered in conjunction with ketamine to minimize severity.

PropofolPropofol
Soy, Glycerol, EggSoy, Glycerol, Egg““Milk of AmnesiaMilk of Amnesia””Rapid onset and recoveryRapid onset and recoveryGABAGABAAA receptor potentiates receptor potentiates CNS inhibitionCNS inhibition
Sedative, NOT analgesicSedative, NOT analgesic11--2 mg/kg IV push2 mg/kg IV push1 mg/kg/1 mg/kg/hrhr or 50or 50--150 150 mcg/kg/min mcg/kg/min Painful on IV injectionPainful on IV injection–– Can use Can use lidocainelidocaine/ketamine/ketamine
Risk of bacterial Risk of bacterial contaminationcontamination

PropofolPropofolDisadvantagesDisadvantages–– Respiratory depressionRespiratory depression–– Hypotension (negative inotrope, potent vasodilator)Hypotension (negative inotrope, potent vasodilator)–– ““PropofolPropofol Infusion SyndromeInfusion Syndrome””
Fatal lactic acidosisFatal lactic acidosisUse > 6 hours not recommendedUse > 6 hours not recommended

αα--2 Agonists2 Agonists
ClonidineClonidineDexmedetomidineDexmedetomidine
AntihypertensiveAntihypertensiveSedative & AnalgesiaSedative & Analgesia

ClonidineClonidine
Binds Binds αα--2:2:αα--1 receptors 200:1 1 receptors 200:1 Acts on Acts on αα--2 receptors in locus 2 receptors in locus ceruleusceruleusPrevents presynaptic release of NE Prevents presynaptic release of NE Routes: PO, IV, SQ, PR, TD, IN (good Routes: PO, IV, SQ, PR, TD, IN (good bioavailibilitybioavailibility))Long halfLong half--life: 12life: 12--24hrs24hrs

DexmedetomidineDexmedetomidine
Binds Binds αα--2:2:αα--1 receptors 1600:11 receptors 1600:1Affects vasomotor center of medulla Affects vasomotor center of medulla Increases sympathetic toneIncreases sympathetic toneAlso acts on Also acts on αα--2 receptors in locus 2 receptors in locus ceruleusceruleus Stimulating Stimulating parasympathetic while decreasing sympathetic outflowparasympathetic while decreasing sympathetic outflowHalfHalf--life: 1.5life: 1.5--3 3 hrshrsApproved in adults, not in childrenApproved in adults, not in children11--2 mcg/kg slow load over 10 minutes2 mcg/kg slow load over 10 minutesInfusion runs 0.2Infusion runs 0.2--1 mcg/kg/1 mcg/kg/hrhrAdverse effects include hypotension, Adverse effects include hypotension, bradycardiabradycardia, hypertension, hypertensionUseful for MRI and other noninvasive proceduresUseful for MRI and other noninvasive procedures

Neuromuscular BlockadeNeuromuscular BlockadeMuscle relaxantsMuscle relaxants–– Depolarizing (mimics action of acetylcholine)Depolarizing (mimics action of acetylcholine)
SuccinylcholineSuccinylcholine–– NondepolarizingNondepolarizing (competitively blocks actions of acetylcholine)(competitively blocks actions of acetylcholine)
MivacuriumMivacuriumVecuroniumVecuroniumAtracuriumAtracurium & & ciscis--atracuriumatracuriumPancuroniumPancuroniumRocuroniumRocuronium
NEVER muscle relax a patient without assuring adequate NEVER muscle relax a patient without assuring adequate sedation/analgesia beforehand.sedation/analgesia beforehand.
ALWAYS confirm the patient is easily handALWAYS confirm the patient is easily hand--bagbag--ventilated ventilated prior to paralyzingprior to paralyzing

Final Thoughts Final Thoughts Remember this:Remember this:Conscious sedation = moderate sedation/analgesiaConscious sedation = moderate sedation/analgesiaFalls on a continuum from mild sedation to general anesthesia.Falls on a continuum from mild sedation to general anesthesia.Must be prepared to rescue patient from deeper levels of sedatioMust be prepared to rescue patient from deeper levels of sedation.n.Be aware of NPO times and monitoring options.Be aware of NPO times and monitoring options.Medication choices are dictated by the clinical situation.Medication choices are dictated by the clinical situation.

ReferencesReferencesConscious Sedation: Reality or Myth? Conscious Sedation: Reality or Myth? Jeffrey L. Koh and Tonya Palermo Pediatr. Rev. 2007;28;243-248
American Academy of Pediatrics: Committee on Drugs. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatrics. 1992;89:1110–1115
American Academy of Pediatrics: Committee on Drugs. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures: addendum. Pediatrics. 2002;110:836–838
American Society of Anesthesiologists: Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96:1004–1017
Pediatric procedural sedation and analgesia outside the operating room: anticipating, avoiding and managing complications. R. Ramaiah, S. Bhananker Expert Rev. Neurother. 2011; 11(5): 755-763

ReferencesReferencesYasterYaster M et al. Pain and Sedation Management in the Critically Ill ChiM et al. Pain and Sedation Management in the Critically Ill Child. ld. RogersRogers’’ Textbook of Pediatric Critical Care. 4Textbook of Pediatric Critical Care. 4thth ed. Baltimore, MD: Lippincott ed. Baltimore, MD: Lippincott Williams and Wilkins, 2008, ed. Nichols DG et al. Williams and Wilkins, 2008, ed. Nichols DG et al. PossPoss WB. Analgesia and Sedation and the use of Neuromuscular BlockinWB. Analgesia and Sedation and the use of Neuromuscular Blocking g Agents. SCCM Pediatric Agents. SCCM Pediatric MultiprofessionalMultiprofessional Critical Care Review, 2008, ed. Critical Care Review, 2008, ed. ShanleyShanley T. T. Olson, Olson, DaiWaiDaiWai BSN, RN; BSN, RN; ThoyreThoyre, Suzanne PhD, RN; , Suzanne PhD, RN; AuyongAuyong, David , David Perspectives on Sedation Assessment in Critical Care. AACN AdvanPerspectives on Sedation Assessment in Critical Care. AACN Advanced ced Critical Care. 18(4):380Critical Care. 18(4):380--395, October/December 2007.395, October/December 2007.Kearns GL, AbdelKearns GL, Abdel--RahmanRahman SM, et al. Developmental pharmacologySM, et al. Developmental pharmacology----drug drug disposition, action, and therapy in infants and children N disposition, action, and therapy in infants and children N EnglEngl J Med. 2003 J Med. 2003 Sep 18;349(12):1157Sep 18;349(12):1157--67 67
www.sccm.orgwww.sccm.orgwww.pedsedation.orgwww.pedsedation.org

