screening, diagnosis & antepartumrisk factors for gdm · 2014-06-27 · risk of diabetes after...
TRANSCRIPT

Screening, Diagnosis &
Antepartum Risk factors for GDM
Jae-Yoon Shim
Department of Obstetrics and Gynecology,
University of Ulsan College of Medicine, Asan Medical Center
1

Introduction
� 1960s, O’Sullivan JB
� Degree of glucose intolerance during pregnancy was related to the
risk of diabetes after pregnancy ( > 2 SD -> 22% overt DM)
� 100g OGTT 90 / 165 / 145 / 125
� 1980s, Minor modification of GDM (NDDG)
� Glucose intolerance with onset or first recognition during
pregnancy
� 100g OGTT 105 / 190 / 165 / 145
� Preexisting type-2 DM: confirmed postpartum
� Perinatal mortality: 6 times higher than mild GDM
� GDM with birth defects: higher FBS
→ presence of undiagnosed preexisting DM
2
Fetal & Maternal effects
� Adverse outcomes of GDM
• Preeclampsia
• Polyhydramnios
• Fetal macrosomia
• Birth trauma
• Operative delivery
• Perinatal mortality
• Neonatal metabolic complications
:hypoglycemia, hyperbilirubinemia, hypocalcemia,
erythremia
3
(Crowther et al., N Engl J Med. 2005)

Fetal & Maternal effects
� Long-term consequences of GDM
• Obesity and diabetes during childhood
• Impaired fine and gross motor function
• Inattention and hyperactivity
(Ornoy A et al. Pediatr Endocrinol 2005)
• 10% of patients : Diabetes soon after delivery(ADA. Diabetes Care 2002)
4

Fetal & Maternal effects5
(Lee et al. Diabetes Res Clin Pract. 2008)

Prevalence6
(Dana et al. Diabetes Care 2005)
Asian
Hispanic
A-American
Whitish

Screening test
� 50g, 1-hour OGCT (Oral glucose challenge test),
at 24-28 weeks
� 130 mg/dL : 90% detect
� 140 mg/dL : 80% detect
� Low threshold
� High sensitivity
� High false-positive rate, unnecessary diagnostic GTT
� 100g OGTT: 14%→23%
7

Diagnostic test
� There is no international agreement as to
the optimal glucose tolerance test to
identify gestational diabetes.
8

Diagnostic test
� 100g, 3-hour OGTT
� In the morning after an overnight fast of 8-14 hours
and after at least 3 days of unrestricted diet and
unlimited physical activity
� Remain seated, no smoking
� 2 or more thresholds be met or exceeded
� Best predictors for developing diabetes later in life
� 1 abnormal value
� macrosomia & other morbidities ↑
9

Criteria for diagnosis
Fasting 1 hr 2 hr 3 hr
100g – OGTT
NDDG(2 or more abnormal)
105 190 165 145
Carpenter & Coustan(2 or more abnormal)
95 180 155 140
75g – OGTT
WHO(1 or more abnormal)
126 - 140 -
ADA(2 or more abnormal)
95 180 155 -
10

Diagnostic test (75g-OGTT)
� Various threshold values for the diagnosis of
GDM- 75g OGTT
� Good compliance
� More economic
� Macrosomia delivery : Similar to 100g OGTT
11
Latest diagnostic criteria
� International Association of Diabetes and
Pregnancy Study Groups (IADPSG)
12
(IADPSG, Diabetes Care. 2010)
IADPSG 2010
� Based on data in HAPO study
� birthweight, cord C-peptide, and % body fat >
90p
� OR 1.75 than average glucose
� 75gm OGTT, 92/180/153, ≥ 1 abnormal value
� Overt DM
� FBS ≥ 126 or Random ≥ 200 or HbA1C ≥ 6.5%
13

IADPSG 2010 - strategy
� First prenatal visit� FBS, HbA1c, or random on all or high risk
women• Exclude overt DM
� GDM: 92 ≤ FBS < 126
� If FBS < 92, 75gm OGTT at 24-28wks
� 75gm OGTT at 24-28wks� Overt DM: FBS ≥ 126
� GDM: 92/180/153, ≥ 1 abnormal value
14

Controversy of Screening tests
Universal or Selective screening ?
How to screen ?
15

Selective screening 장단점
� Benefits
� Reduction of unnecessary screening test
� Defects
� 의사가귀찮다.
16
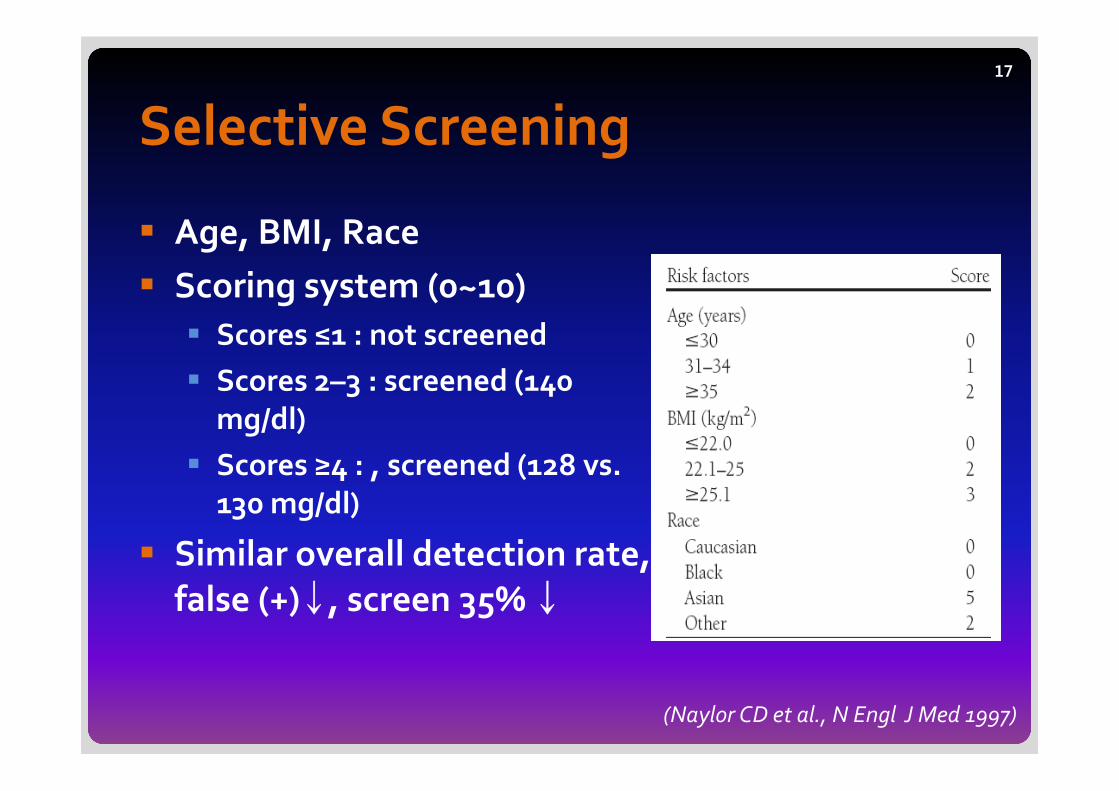
Selective Screening
� Age, BMI, Race
� Scoring system (0~10)
� Scores ≤1 : not screened
� Scores 2–3 : screened (140
mg/dl)
� Scores ≥4 : , screened (128 vs.
130 mg/dl)
� Similar overall detection rate,
false (+)↓, screen 35% ↓
17
(Naylor CD et al., N Engl J Med 1997)

Low risk group (ADA)
� Maternal age < 25 years
� Normal BMI
� No family History of DM
� No previous GDM
� No history of poor obstetric outcome
� No high-risk ethnic origin (Hispanic American,
Native American, Asian American, African
American, Pacific islander)
18
(ADA, Diabetes Care. 2009)

High risk group (ADA)
� Marked obesity
� Personal history of GDM
� Glycosuria
� Family History of DM
� Screening ASAP
19
(ADA, Diabetes Care. 2009)

Risk evaluation of GDM20
(Leeuwen et al., BJOG 2010)

21
(Leeuwen et al., BJOG 2010)

임산부경구당부하검사급여인정
� 임신성당뇨병의고위험군의경우� 소변검사상당검출� 4kg 이상의거대아분만력� 당뇨의가족력� 원인불명의자궁내태아사망의분만력� 비만� 30세이상산모
� 당뇨기왕력또는의심되는임산부� 100g 경구당부하검사는
50g 경구당부하검사결과 140 mg/dl 이상인경우인정(2007.06.)
22
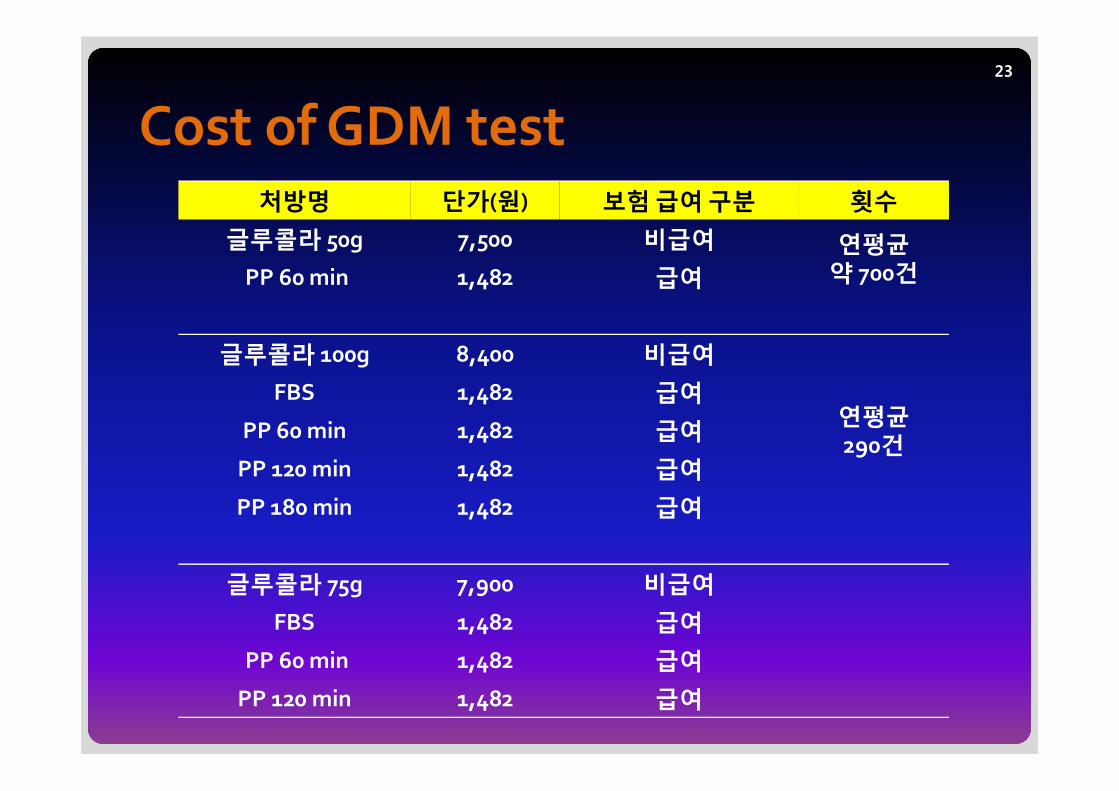
Cost of GDM test23
처방명 단가(원) 보험급여구분 횟수
글루콜라 50g 7,500 비급여 연평균약 700건PP 60 min 1,482 급여
글루콜라 100g 8,400 비급여
연평균290건
FBS 1,482 급여
PP 60 min 1,482 급여
PP 120 min 1,482 급여
PP 180 min 1,482 급여
글루콜라 75g 7,900 비급여
FBS 1,482 급여
PP 60 min 1,482 급여
PP 120 min 1,482 급여

Which blood?
� Whole blood vs. serum or plasma vs. capillary
� Originally venous whole blood
� 10-15% lower than serum or plasma
� Generally venous plasma
� In fasting: capillary = venous
� After meal: capillary > venous
� Low resource setting
24

Postpartum screening
� 6-12 weeks after delivery, FBS or 75g GTT
DM Impaired
fasting glucose
Impaired
glucose tolerance
Normal
FBS ≥ 126 100 - 125 NA < 100
75g 2-hr
OGTT
FBS≥ 126 or
PP2 ≥ 200
100 ≤ FBS ≤ 125 140 ≤ PP2 ≤ 199 FBS < 100 and
PP2 < 140
Wt reduction, Physical activity
Medical nutrition therapy
75g 2hr OGTT yearly
75g 2hr OGTT
every 3 years
25

Pre-conceptional care
(Merlob P. et al. The textbook of diabetes and pregnancy. 2008.53)
26

Conclusions
� 선별검사및 risk factor evaluation
� Another selective screening tool in Korea
� 진단검사� Expansion in medical insurance
� 학회및국민계몽� 출산후검사및임신전검사
� 협진
27
경청해주셔서감사합니다람쥐~~~
28

29

30

Controversy of Screening tests
• Universal screening
• Prevalence of GDM in low risk group : 2.8% & similar pregnant outcome
• 80% of all pregnancy - screening
: 10% of GDM – missed
(Moses, RG Diabetes Care1998)
31

GDM diagnostic tool
� Recommended screening strategy(5th International Workshop-Conference on Gestational diabetes)
� Based on risk assessment for detecting gestational diabetes
� GDM risk assessment should be ascertained at the first
prenatal visit
32

GDM diagnostic tool
� Low risk group� Consists of member of an ethnic group with a low prevalence of
GDM
� Age<25 years
� Normal weight before pregnancy
� Normal weight at birth
� No history of abnormal glucose metabolism
� No history of poor obstetrical outcome
� Blood glucose testing not routinely required
in low risk group
33

GDM diagnostic tool
� Average risk group� Blood glucose testing at 24 to 28wks
� Two step procedure
: 50-g oral glucose challenge test
� Diagnostic 100-g oral glucose tolerance test
(meeting threshold value in the glucose challenge test)
� One step procedure (performed on all subjects)
: Diagnostic 100-g oral glucose tolerance test
34

GDM diagnostic tool
� High risk group� Consists of severe obesity
� Strong family history of type 2 DM
� Previous history of GDM
� Impaired glucose metabolism or glucosuria
� Blood glucose testing as soon as feasible
� If GDM is not diagnosed � Should be repeated� 24 to 28 weeks
� Any time there are symptoms or signs suggestive of hyperglycemia.
35