screening, diagnosis, and assessment of liver disease in
TRANSCRIPT
Screening, Diagnosis, and Assessment of Liver Disease in
CKD Patients with HCV
Tawesak Tanwandee, MD. Department of Medicine, Faculty of Medicine Siriraj Hospital,
Mahidol University, Bangkok
KDIGO

DISCLOSURES
• Grant/research support
• Merck, Roche, Arbutus, Janssen, Exact Science
• No disclosure relevant to this talk KDIGO

TOPICS
• HCV problem in CKD
• Impact of advanced CKD on liver markers (ALT, AST)
• Non-invasive measures (biochemical and elastography) vs biopsies
• Relevant KDIGO guideline recommendation statements
KDIGO

Prevalence of HCV in dialysis and kidney transplantation
Authors Reference year
Country Patients, n Anti-HCV positive, n
Pereira B., et al. (study 1) 1997 USA 103 21 (22.8%)
Pereira B., et al. (study 2) 1997 USA 103 23 (22.3%)
Legendre C., et al. 1998 France 499 112 (22.4%)
Batty D., et al. 2001 USA 28 692 1624 (5.7%)
Breitenfeldt. M., et al. 2002 Germany 927 160 (17.2%)
Forman J., et al. 2004 USA 354 26 (7.3%)
Mahmond I.,et al. 2004 Egypt 133 80 (60.1%)
Bruchfeld A., et al. 2004 Sweden 571 51 (8.9%)
Aroldl A., et al. 2005 Italy 541 244 (45.1%)
Mitwalli A., et al. 2006 Saudi Arabia 448 286 (63.8%)
Einollahi B., et al. 2007 Iran 3028 NA
Ingsathit A., et al 2007 Thailand 346 22 (3.6%)
Luan F., et al. 2008 USA 79 337 3708 (4.7%)
Gentil M., et al. 2009 Spain 3861 232 (6.7%)
Ridruejo E., et al 2010 Argentina 542 180 (33.2%)
Morales J., et al. 2010 Spain 4304 587 (13.6 %)
Scott D., et al. 2010 Australia, NZ 7572 140 (1.8%)
Singh N., et al. 2012 USA 2169 154 (7.1%)
Country Anti-HCV Prevalence
(%)
Anti-HCV-Positive
Patients (n)
Reference
Belgium 11.8 51/433 Jadoul et al.
Netherlands 3.4 76/2286 Schneeberger et al.
Italy 22.5 2274/10097 Lombardi et al.
USA 22.3 88/394 Fabrizi et al.
France 16.3 216/1323 Salama et al.
Poordad F et al. Semin Liver Dis 2004
Fabrizi F et al. J Viral Hepat 2014
0.85% % in the general population
HCV infection is more frequent in patients with CKD but the prevalence is decreasing
Anti HCV positive after renal transplantation
KDIGO

0
5
10
15
20
25
30
35
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Year
Number of incident hepatitis C virus (HCV) infections from outbreaks in the United States dialysis facilities reported to the
Centers for Disease Control and Prevention, 2008-2017
Nguyen DB. et al. Seminar in Dialysis 2019
KDIGO

Prevalence of anti-HCV positive in advanced CKD not requiring dialysis
Authors Prevalence rate Year Country
Fabrizi et al 44/221(20%) 1994 Italy
Lopez-Alcorocho et al 6/35(17%) 2001 Spain
Bergman et al 57/396(14.4%) 2005 USA
De Los Rios et al 1/99(1%) 2006 Peru
Sit et al 12/171(7%) 2007 Turkey
Lemos et al 41/1041(3.9%) 2008 Brazil
Hammad et al 20/66(30.3%) 2009 Egypt
Li Cavoli et al 24/320(7.5%) 2011 Italy
Shafi et al 49/180(27.2%) 2017 Pakistan
Fabrizi et. al. Seminars in Dialysis 2019
KDIGO

Prevalence (%) of having anti-HCV antibodies amongst patients receiving PD (white bars) or HD (black bars) across different Asia-Pacific countries
Johnson DW. et al. Nephrol Dial Transplant 2009
KDIGO

Annual incidence of anti-HCV antibody amongst patients receiving PD (white bars) or HD (black bars) across different Asia-Pacific countries
Johnson DW. et al. Nephrol Dial Transplant 2009
KDIGO

Global estimates of HCV infection in HIV-infected individuals by global burden of disease region
Platt L. et al. Lancet Infect Dis 2016
KDIGO

More fibrosis progression in coinfected patients
Naggie S, Sulkowski MS. Gastroenterology 2012
KDIGO

Prevalence of cirrhosis in HIV-infected patients
Castellares C. Journal of Viral Hepatitis, 2008
KDIGO

Detection and evaluation of HCV in CKD Anti-HCV
Negative Positive
NAT
Positive Negative
Current infection
Liver test and evaluation for treatment
Resolved or low viremic
Monthly ALT
NAT q 6 months
Monthly ALT
HBsAg Anti-HBs
Anti-HCV q 6 months
Modified from KDIGO guideline 2018
HCV Ag?
KDIGO

Comparison between HCVcAg and PCR HCV-RNA test in dialysis patients
Cavoli GL. Hepatitis Research and Treatment 2012
KDIGO

Impact of advanced CKD on liver markers (ALT, AST)
KDIGO

AST levels were significantly lower in both Group A (18.48 ± 4.14) and Group B (10.08 ± 3.49) as compared to controls in Group C (30.5 ± 10.75), (P < 0.001).
Ray L. Int J Appl Basic Med Res 2015
KDIGO
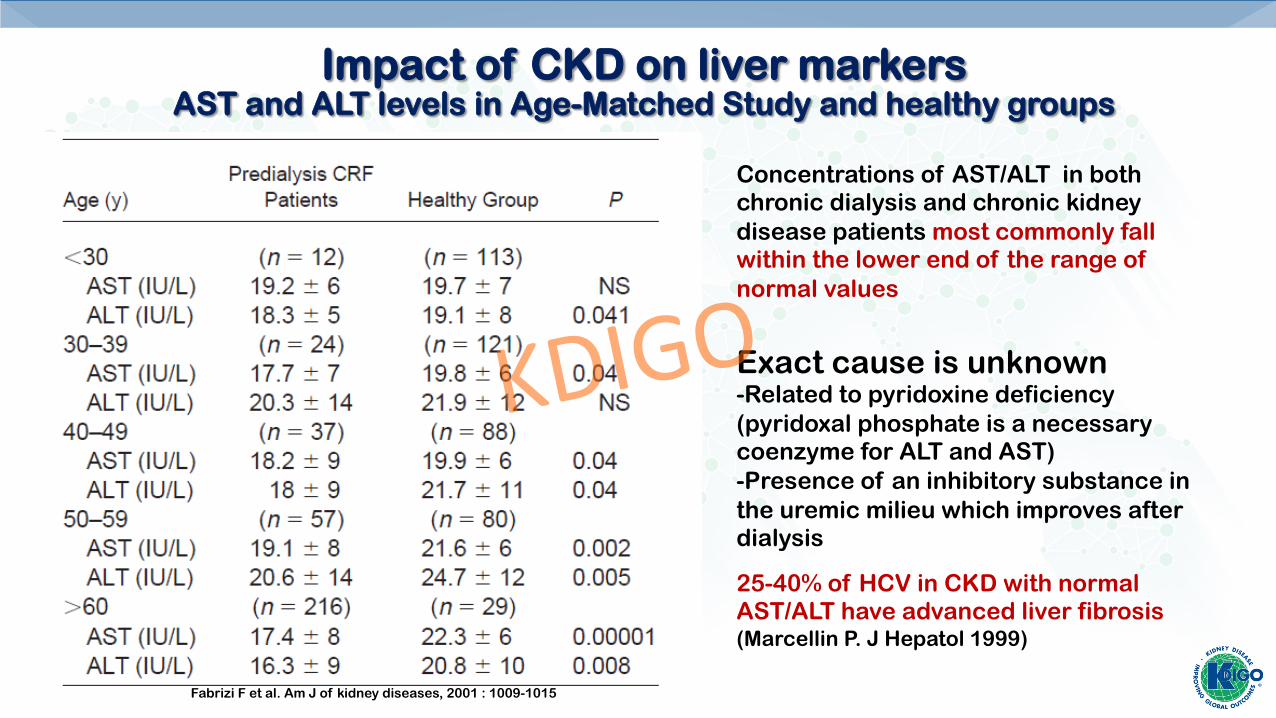
Impact of CKD on liver markers AST and ALT levels in Age-Matched Study and healthy groups
Fabrizi F et al. Am J of kidney diseases, 2001 : 1009-1015
Concentrations of AST/ALT in both chronic dialysis and chronic kidney disease patients most commonly fall within the lower end of the range of normal values
Exact cause is unknown -Related to pyridoxine deficiency (pyridoxal phosphate is a necessary coenzyme for ALT and AST) -Presence of an inhibitory substance in the uremic milieu which improves after dialysis
25-40% of HCV in CKD with normal AST/ALT have advanced liver fibrosis (Marcellin P. J Hepatol 1999)
KDIGO

Liver Fibrosis Assessment Non-invasive tests vs Liver biopsy
• Liver biopsy is goal standard, especially to assess liver status before KT • Safe but considered invasive • Risk of bleeding (platelet dysfunction, recurrent anticoagulant) • Sampling error, intra-, inter-observer variability of histological
reading
• Non-invasive tests have become available and validated in CKD
• Liver biopsy only reserved for those with discordance result
KDIGO

Liver biopsy Liver biopsy is the current gold standard for the evaluation of hepatic f i b r o s i s b u t h a s s e v e r a l l i m i t a t i o n s :
ü lacks reproducibility and accuracy • liver sample represents only 1/50,000 of the total liver • 10-20% of inter and intra observer variability to assess fibrosis
è 24% false negatives for the detection of cirrhosis
ü followed by complications requiring hospitalization in 1-3% patients
• 20-30% pain • 0.3% morbidity (hemorrhages) • 0.03% mortality
è poor acceptance from both patients and prescribing physicians
KDIGO

Biomarker Groups Example of Individual Components Example of Panel Biomarkers
Direct
Collagen and extracellular matrix components
HA,MMP 1 MMP 8, PIII NP Laminin
ELF, Fibrospect HA score, Hepascore Leroy score
Hepatic stellate cell and fibrogenic cell mediators
TIMP 1, TGF b Angiotensin II, YKL 40
ELF Fibrospect
Indirect
Portal hypertension Platelet count Spleen size
Fibrometer, Fibroindex FIB-4, Pohl index Testa index, Wai score
Synthetic parameters Albumin Platelet count
PGAA index Fibrometer
Liver enzymes and bilirubin
AST, ALT AST/ALT ratio GGT, Bilirubin
APRI, BAAT score Fibrometer, Fibroindex Fibrotest, Forns Hepascore, HA score NAFLD simple index Pohl index, Wai score
Miscellaneous Cholesterol Insulin resistance
NAFLD simple index BAAT score Forns
KDIGO

ROC curves of APRI* in predicting HD patients with CHC presenting significant hepatic fibrosis ( >F2)
Liu CH. Kidney Int 2010 *AST-to-platelet ratio index(AST/ULN)/Platelet x 100
KDIGO

APRI is more accurate than FIB-4
APRI (AUROC=0.97) FIB-4 (AUROC=0.74)
Wadhva RK. J Transl Int Med 2018 FIB-4, Age (year) x AST/platelet x √ALT
KDIGO

Fibrotest
Logistic regression equation of 6 parameters
• Alpha-2-macroglobulin • Haptoglobin • apolipoprotein A1 • GGT • total bilirubin • ALT
KDIGO

Various tests and thresholds to evaluate liver fibrosis
Test Cut-off Interpretation
APRIa <0.4 >0.95
No fibrosis to mild fibrosis (F0-F2) Advanced fibrosis (F3-F4)
FIB-4a <1.45 >3.25
No fibrosis to mild fibrosis (F0-F2) Advanced fibrosis (F3-F4)
Fibrotest/Fibrosure 0-0.58 0.59-1
No fibrosis to mild fibrosis (F0-F2) Advanced fibrosis (F3-F4)
HVPG 6-10 mmHg >12 mmHg
Compensated cirrhosis Decompensated cirrhosis with significant PHT
aAPRI, AST-to-platelet ratio index (AST/ULN)/Platelet x 100) aFIB-4, Age (year) x AST/platelet x √ALT
Adapted from Cottone C. Seminars in Dialysis 2019
KDIGO

ROC curves of Fibroscan® and APRI ≥F2, TE (0.96, 95% CI: 0.94 to 0.98) and APRI (0.84, 95% CI: 0.79 to 0.88; P < 0.001 ≥F3, TE (0.98, 95% CI: 0.97 to 1.00) and APRI (0.93, 95% CI: 0.90 to 0.97; P = 0.04) F4, AUC of TE (0.99, 95% CI: 0.98 to 1.00) and APRI (0.92, 95% CI: 0.89 to 0.96; P = 0.13
Liu CH. Clin J Am Soc Nephrol 2011.
APRI vs Transient Elastography (TE)
KDIGO

Transient elastography and histologic correlation
TE score (kPa METAVIR Stage Histological finding
<7 F0-1 No fibrosis, periportal fibrosis without septa
7.1-9.5 F2 Portal fibrosis with septa
9.6-12.4 F3 Bridging fibrosis
>12.5 F4 Cirrhosis
Adapted from Cottone C. Seminars in Dialysis 2019
KDIGO

Transient elastography
• Most reliable non-invasive test • Limitation
• Level increases • After meal (return to baseline 120 min. after meal)$ • Elevated central venous pressure (CHF, hypervolemia)
• Significant reduction if done after net ultrafiltration >2.5 L post HD* • Difficult to perform in PD (fluid left in abdominal space may prevent
propagation of shear wave)
$ Palazzo H et. Al. Inter J Hepatol 2015 * Taneja S. et. al. Dig Dis Sci 2017; Khunpakdee N et. al. Blood Purif 2015
KDIGO

Magnetic Resonance Elastography (MRE)
• MRE has high accuracy for diagnosis of significant or advanced fibrosis and cirrhosis, independent of BMI and etiology of CLD
Singh S et al. Clin Gastroenterol Hepatol. 2015
KDIGO
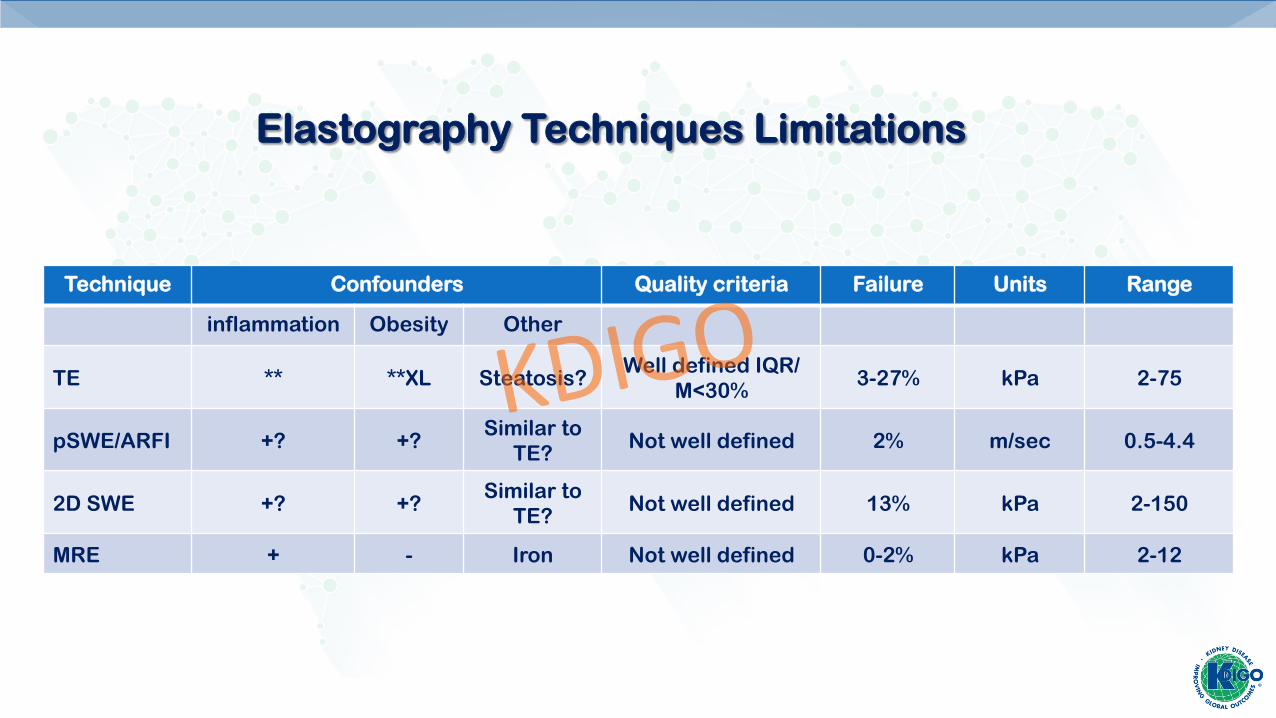
Technique Confounders Quality criteria Failure Units Range
inflammation Obesity Other
TE ** **XL Steatosis? Well defined IQR/
M<30% 3-27% kPa 2-75
pSWE/ARFI +? +? Similar to
TE? Not well defined 2% m/sec 0.5-4.4
2D SWE +? +? Similar to
TE? Not well defined 13% kPa 2-150
MRE + - Iron Not well defined 0-2% kPa 2-12
Elastography Techniques Limitations
KDIGO

Applicability of non-invasive tests
90% 80%
= reliability+ failure rate
N=342,346 N=13,669
Poynard T, et al BMC Gastroenterol 2011 Castera L, et al Hepatol 2010
TE Fibrotest
KDIGO

Evaluation of patients with CKD and HCV
Viremic HCV in CKD
Non-invasive evaluation of liver fibrosis
Non-conclusive/discordant
Liver biopsy
Advanced fibrosis (F3-F4)
Assessment of PHT Endoscopy, non-invasive
radiological or HVPG
Modified from KDIGO guideline 2018
KDIGO

Other testing of patients with HCV infection
• All patients with CKD at the time of HCV diagnosis • Urinalysis, eGFR • If no evidence of kidney disease, repeat screening for
kidney disease if NAT still positive • All CKD with history of HCV (NAT+ or -) • Follow-up for progression of kidney disease • Vaccination against HAV and HBV • Screening for HIV • Evaluation of portal hypertension in advanced fibrosis
Modified from KDIGO guideline 2018
KDIGO

Prasad N. Kidney Dis 2015 World Bank economic classification Low income of Asian countries
Asia represents countries with wide range of economic incomes and healthcare spending
KDIGO

Registry name (common abbreviation), year of establishment
Accessibility Patient-level
data availability
Treatments Out-comes
Hong Kong Renal Registry (HKRR), 1995 + + +++ +++
Korean Renal Registry, 1985 ++ ++ +++ +++
Malaysian National Renal Registry (NRR), 1993 ++ +++ +++ +++
Shanghai Dialysis Registry, 1996 + + ++ +++
Singapore Renal Registry, 2001 +++ ++ +++ +++
Taiwan Renal Registry Data System (TWRDS), 1987 + + +++ +
Thailand Renal Replacement Therapy Registry (TRT), 1997 ++ + +++ +
Features of dialysis registries in Asia
Prasad N. Kidney Dis 2015
KDIGO
Unique challenges in Asia
• No standard practices in CKD in many countries, even different centers in the same country • Diversity of clinical practice • Application of universal precaution • Application of HCV tests and evaluation for fibrosis • Many countries cannot afford NAT, HCV Ag as alternative? • Fibrosis assessment?
• Access to HCV treatment, especially where there is no SOF-free generic drug for CKD with eGFR < 30
KDIGO

Conclusion • HCV infection in various stages of CKD is still common
• New infection is now less frequent but still occurs
• Standard practice for HCV prevention varies
• Co-infection with HBV, HIV can have more progressive disease
• Assessment of liver fibrosis is important, not only to guide treatment but also decision for KT
• Diferrent economic background in Asian countries can affect current standard practice
• How should we optimize KDIGO guideline especially in countries with low income
KDIGO