screening and brief treatment for alcohol and illicit … · screening and brief treatment for...
TRANSCRIPT

Screening and brief treatment for alcohol and illicit drug use
in primary care
1
Elizabeth Byrne, NCC, LPC
Adam Brooks, PhD
Kimberly Malayter, LCSW

Research-Based Solutions Disclosure
As part of its mission, TRI develops and markets research-
derived products and solutions designed to advance evidence-
based practices and policies.
Proceeds from dissemination of these products are returned to
the organization to support future research in accordance with
TRI’s mission and values.
The TRI products discussed in this presentation are:
SBIRT Toolkit
Keep it Moving™ Graphic Novel
2

Collaborating Partners/Institutions
National Nursing Centers Consortium
Treatment Research Institute
Public Health Management Corporation
Family Practice and Counseling Network
Resources for Human Development
Drexel University
University of Pennsylvania
Lincoln University
3
Acknowledgements Pennsylvania Department of Health SAP No. 4100055578
Scientific Team:
Adam Brooks, Ph.D., David Metzger, Ph.D., Kimberly Kirby, Ph.D., Brenda Curtis, Ph.D., Jennifer Lauby, Ph.D., Daniel Polsky, Ph.D., Kevin Favor, Ph.D., Judith Thomas, Ph.D., Patricia Gerrity, Ph.D., Donna Torrisi, M.S.N., Thomas McLellan, Ph.D.
Collaborators:
Denise Gaither-Hardy (Lincoln University), Elizabeth Byrne (NNCC/PHMC), Mary Malnimow (PHMC), Tracy Weant (RHD), Michelle O’Connell (FPCN), Anne Kelly (PHMC), Ariel Adams (Drexel), Laura Line (RHD), Lisa Bond (PHMC), Caryn Gratz (PHMC)
Team Members:
Carolyn Carpenedo, Dan Knoblach, Jaclyn Chambers, Graham DiGuiseppi, Emily Ball, Christina Cruz, Nicolas Joseph, Roxana Arango, Tameka Williams
4

SUDs and Chronic Health Problems
SUDs related to increased risk:
Hypertension, heart failure, etc.
Renal and GI (liver failure, cirrhosis, Hep B and C,
kidney failure)
Neurological (stroke, ischemic events, TBI)
Pulmonary (pneumonia, edema, TB)
Perinatal, postnatal complications
Endocarditis
HIV transmission
5

What is SBIRT?
Screen Everyone for Risk in Primary Care
Brief Intervention (for those at Risk)
Give Feedback
Be Empathic
Give Advice / Offer a Menu of Change
Referral To Treatment (for Dependent Users)
Brief Treatment
Specialty Care / Detox / Rehab
6

Basic SBIRT Model Assess 2-3 min
Advise (Feedback) 1-2 min
REFER TO BHC?? OR:
Agree (Responsibility, Empathy) 5 min
Advise 2.0 (Advice, Menu of Options) 1-2 min
Assist (Support Self-Efficacy) 2-3 min
Arrange

Real-time decision and intervention
Hierarchy of broad to focused screening / assessment
Brief screener (AUDIT-C / DAST-1)
Full screener (AUDIT / DAST)
Functional Analysis
Trained to Provide Brief Intervention Based on
Readiness
Quit, Cut-Back, Watch for a while, Do Nothing for Now
Support quit attempts or make referrals
Provided support tools

SBIRT for Alcohol Use
Three decades of research supporting the efficacy of
brief intervention for alcohol
Strong evidence for brief intervention in primary care
and office based settings
Mixed or weak evidence for brief intervention in
hospitals and EDs
Possible that effect largely comes from reductions of
“at risk” drinkers who reduce

SBIRT for Illicit Drug Use More mixed evidence for the efficacy of SBIRT for
illicit drug use
Designs with straight controls have limited efficacy:
Screen only vs. Screen + BI
Screen + printed info vs. Screen + BI
Some indication that participation in more intensive
interventions yields results

Research Strategy
Decided to test a more intensive on-site approach
against classic SBIRT
Needed a flexible approach:
Met patients’ felt needs
Would respond to a variety of substance and
health issues
To facilitate implementation:
Toolkit to assist in patient communication
Guide clinicians to deliver with fidelity

What is SBIRT+? 2-6 sessions, based on client need
Based off of Motivational Enhancement Therapy
Multiple motivational interviewing sessions
Brief quit / reduction strategies
Relapse Prevention / Cognitive Behavioral Therapy
12-Step Facilitation
Focus on assisting severe users with accessing
specialty care treatment (multiple referrals, follow-up,
case management)
Ongoing follow-up by telephone
What are we studying?
Screening, Brief Intervention, Referral to Treatment
(SBIRT) in primary care
Is one brief-intervention session enough?
Will drug-users return for additional sessions?
Is expanded brief intervention (SBIRT+) more cost-
effective than traditional SBIRT?

Study Design
Test SBIRT vs. SBIRT+
Identify 1000+ Harmful Users
Consent and Randomly Assign 600
300 to SBIRT 300 to SBIRT+
3, 6, 9, and 12 mo. Follow-up Assessments
Screen 5000 Patients at 3 Clinics for Drug or Alcohol Use

SBIRT Training
Supervisors and staff trained by IRETA in December of
2011
Trained BHCs in SBIRT protocol in four 4-hour
trainings
Trainings included:
Readings
Didactics
Video Examples
Role Play

SBIRT Training Accomplishments
BHCs were identifying dependent users—and referring
Pushed BHCs to rethink – and rededicate to – a brief
consultation model
New tools and education for identifying risky users
Knowledge gaps on standardized drinks / healthy
drinking limits
How to intervene when risky use was detected
How to use standardized assessments for decision
support

SBIRT+ Training
Conducted two 4-hour trainings in SBIRT+
Used Standardized Patient in place of live practice
cases:
All BHCs saw an actor for 4 SBIRT+ sessions
Audiotaped plus feedback
Ongoing supervision with tape review of BHCs with
SBIRT and SBIRT+ cases

Participating Heath Centers
Three Urban Federally Qualified Health Centers
PHMC Care Clinic
FPCN Abbottsford-Falls Clinic
11th Street Family Health Services of Drexel Univ
Clinics provide comprehensive primary care, family
planning, social services, out-patient counseling (Abb-
Falls and 11th Street) and complimentary care (11th St)
Care is delivered primarily by nurse-practitioners
Annual unduplicated patients: 2,000 (CC); 4,000 (AB);
6,500 (11th St) in 2009
Involving the Entire Team
Clinical staff (nurse practitioners, physician assistants,
nurses, social workers) were trained on the delivery of
the SBIRT intervention
Primary care teams (clinical personnel, medical
assistants, front desk) received all-staff trainings about
SBIRT and presentations about the study
Clinics created their own huddle teams of essential staff
for weekly or monthly SBIRT huddles
Additional support and training was made available as
the study progressed
19

Starting the Conversation
Concerns about asking drug and alcohol use questions
without a warm up
Concerns about length of time of screening
Who starts the conversation? BHC? MA? PCP?
Clinics individualized their process to suit their particular
clinic flow and staff engagement
Various initial screeners created
20

Wellness Screeners Please take a moment to answer a few questions so that we may best serve you.
1. Generally, how is your physical health?
2. Do you have High Blood Pressure, Diabetes, Asthma, HIV/AIDS, Hepatitis C, or any other chronic conditions?
3. How often do you keep up with the changes your providers recommend, like adjusting your diet, exercise habits, medication routine, etc.?
4. Do you take prescription medication?
4a. How often do you take your medication as prescribed?
5. How often do you get 30 minutes of exercise during which your heart beats faster or your breath speeds up?
6. Which of the following best describes your food situation?
7. Do you smoke cigarettes, cigars, or use any type of tobacco?
8. How often do you have a drink containing alcohol?
9. How many drinks containing alcohol do you have on a typical day when you are drinking?
21

10. How often in the past year have you used an illegal (street) drug?
11. How often in the past year have you used a prescription medication in order to get high, or in greater amounts than recommended by your provider?
12. How stressed have you felt in the past week?
13. How many times in the past 3 months has any partner, ex-partner, relative, or friend: Pushed, grabbed, or shoved you? _________ Slapped or hit you? ________
14. In your life, have you ever had any experience that was so frightening, horrible, or upsetting that, in the past month, you had nightmares about it or thought about it when you did not want to?
15. How interested are you in working with your provider to make some changes to improve your health?
16. How do you feel about the progress you have made for your health recently?
17. Is there anything else we can help you with today at the clinic?
Thanks so much for answering these health questions.
Your provider may want to talk with you about some of your answers.
Please feel free to raise any areas of concern with your primary care team.
22

23
Health Questionnaire – Clinician Guide Version
J. How often do you have a drink containing alcohol?
1) 3 days or more per week* 2) 1-2 x per week 3) Less than Weekly 4) Monthly or less 5) Never 6) Prefer not to answer*
*Refer to BHC for further screening if response is 1 or 6
K. How many drinks containing alcohol do you have on a typical day when you are drinking?
1) 5 or more* 2) Usually 3 or 4* 3) Usually 2 4) Usually 1 5) Prefer not to answer* *Refer to BHC for further screening if response is 1, 2, or 6
L. How often in the past year have you used an illegal (street) drug?
1) 3 x per week or more* 2) 1-2 x per week* 3) Less than weekly* 4) Less than monthly* 5) Once or twice* 6) Never 7) Prefer not to answer*
*Refer to BHC for further screening if response is 1, 2, 3, 4, 5, or 7
M. How often in the past year have you used a prescription medication in order to get high, or in greater amounts than recommended by your provider?
1) 3 x per week or more* 2) 1-2 x per week* 3) Less than weekly* 4) Less than monthly* 5) Once or twice* 6) Never 7) Prefer not to answer*
*Refer to BHC for further screening if response is 1, 2, 3, 4, 5, or 7
What Is One Drink?
BEER or COOLER
12 oz. ~5% alcohol
12 oz. = 1 40 oz. = 3.3
MALT LIQUOR
8-9 oz. ~7% alcohol
12 oz. = 1.5 40 oz. = 4.5
TABLE WINE
5 oz. ~12% alcohol
1 bottle (750ml) of Moscato = 5.5 1 Magnum (1.5L) = 7
SPIRITS AND LIQUOR
1.5 oz. ~40% alcohol
1 shot or mixed drink = 1 a pint (16 oz.) = 11

AUDIT (Alcohol Use Disorders Id Test)
How often do you have a drink containing alcohol?
How many drinks containing alcohol do you have on a typical day when you are drinking?
How often do you have six or more drinks on one occasion?
How often during the last year have you found that you were not able to stop drinking once you had started?
How often during the last year have you failed to do what was normally expected of you because of drinking?
How often during the last year have you needed a first drink in the morning to get yourself going after a heavy drinking session?
How often during the last year have you had a feeling of guild or remorse after drinking?
How often during the last year have you been unable to remember what happened the night before because of your drinking?
Have you or someone else been injured because of your drinking?
Has a relative, friend, doctor, or other health care worker been concerned about your drinking or suggested you cut down?
24

DAST (Drug Abuse Screening Test)
Have you used drugs other than those required for medical reasons?
Do you abuse more than one drug at a time?
Are you always able to stop using drugs when you want to?
Have you had “blackouts” or “flashbacks” as a result of drug use?
Do you ever feel bad or guilty about your drug use?
Does your spouse (or parents) ever complain about your involvement with drugs?
Have you neglected your family because of your use of drugs?
Have you engaged in illegal activities in order to obtain drugs?
Have you ever experienced withdrawal symptoms (felt sick) when you stopped taking drugs?
Have you had medical problems as a result of your drug use (memory loss, hepatitis, convulsions, bleeding, etc)?
25

Motivational Enhancement Therapy
3-4 sessions
2 sessions in first two weeks
Develop a solid, well negotiated, realistic change
plan
Follow-ups at week 6 and 12
To examine progress, renew motivation, redo
commitment
Evaluate if a further referral is needed
40 minute sessions
Greater emphasis on the client’s reaction to feedback
Possible involvement of 1-2 sessions with a significant
other

Phase 1 - MET Exploring and Resolving Ambivalence
Set the stage – “personal health coaching”
Provide feedback based on screening
Link habits and problems
Explore past times when client has made or tried
habit change, affirm their efforts
Help the client weigh the pros and cons of making a
change
What does the client think they’ll do about the
situation?
This process can begin and resolve in session one, but
is cyclical – throughout the coaching, across weeks,
client will return to ambivalence

Phase 2 - MET Strengthening Commitment to Change
How important is this change? Scale of 1-10
How confident are you that you could make this
change?
What are your next steps?
What has worked before?
Selecting and negotiating a change plan
Securing social support
Securing commitment to stay with the coaching –
setting the next appointment
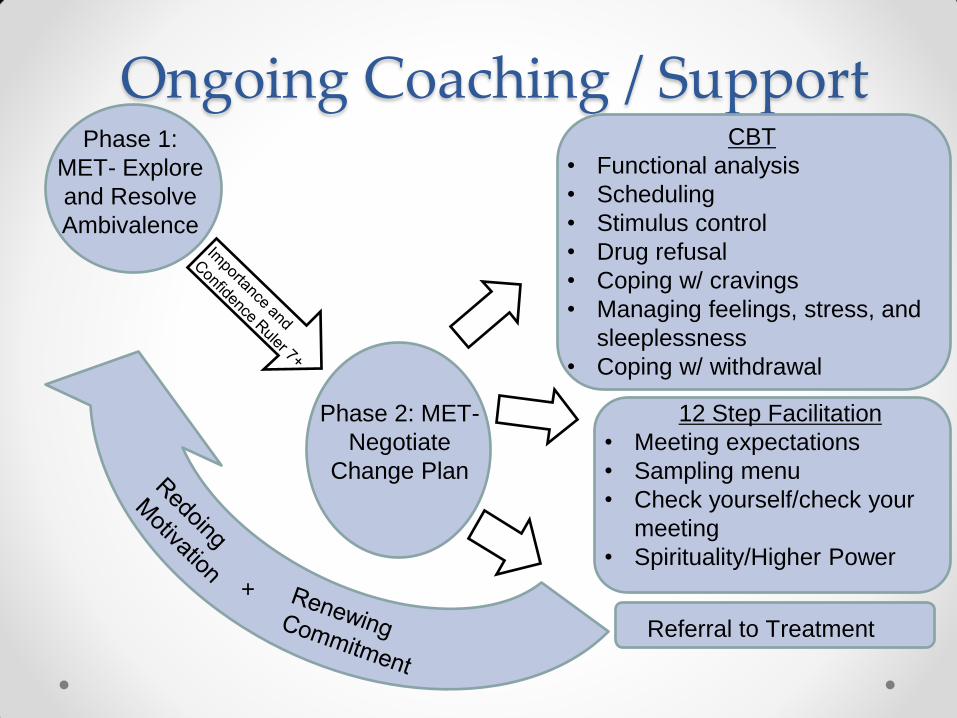
Ongoing Coaching / Support Phase 1:
MET- Explore
and Resolve
Ambivalence
Phase 2: MET-
Negotiate
Change Plan
Referral to Treatment
CBT
• Functional analysis
• Scheduling
• Stimulus control
• Drug refusal
• Coping w/ cravings
• Managing feelings, stress, and
sleeplessness
• Coping w/ withdrawal
12 Step Facilitation
• Meeting expectations
• Sampling menu
• Check yourself/check your
meeting
• Spirituality/Higher Power
+

SBIRT+ Follow-up
Check in on a monthly basis with SBIRT+ clients
In person
Telephone
10-15 minutes
Administer RecoveryTrack™ (computerized tool to
assess clients risk for relapse)
Give Feedback / Express Concern
Offer Referral / Encourage Continued Efforts
Why a Toolkit?
Improved fidelity and retention when counselors are
trained and equipped with a Toolkit
Provides a cost-effective dissemination approach
Improved counselor and patient satisfaction
Tailor interventions to primary care
Broaden use of interventions beyond substances
(health habit change)
Multimedia materials provide a chance to influence
what patients receive beyond the scope of this study
Make lasting impact in equipping BHCs to integrate
brief treatment in primary care

The SBIRT+ Toolkit 35 Brief Tools (in a box!)
8 SBIRT / SBIRT+ Cards for Phase I (Resolve
Ambivalence; for use with either condition)
8 SBIRT+ Cards for Phase II (Negotiate Change,
Strengthen Commitment)
9 SBIRT+ Cards for conducting Behavioral Change
4 SBIRT+ Cards for promoting 12 Step
6 SBIRT+ Cards for referring / promoting formal
treatment
Quick Guides to Help Clinicians Understand How to
Use Any of them
Keep it Moving™ Graphic Novel / Activity Book

Toolkit Examples

Toolkit Examples

Toolkit Examples

Toolkit Examples
Keep it Moving™ Features
Few health education communication materials are
designed specifically for this population
Theory-based
Exercises integrated into storyline
Serves as a workbook
Engaging
Culturally sensitive
Format
Low-cost
Revisable
Scalable
Text or Digital

Keep it Moving™ Example

Keep it Moving™ Example

Keep it Moving™ Example

Core RecoveryTrack™ Items
Substance Use
Medical/Emotional Issues
Risk Factors (e.g., Days of Craving)
Protective Factors (e.g., Days Attending Treatment or
Support Groups)
15 Questions = 5 minutes

Case Studies
Case presentation #1
African American male, 55 year old, veteran
Uses cocaine (1-2 occasions/week)
Initially denied use to Primary Care Provider
Reported use on paper wellness screener
Treatment limited to programs during incarcerations
Challenges
Strengths

Motivational Enhancement Therapy

Better relationships with
family
Not having to worry about
drug tests with parole
officer
More money
Forgetting about problems
Feeling high
Let’s me be by myself
Depression and Guilt
Legal problems
Upsets my family members
Drug screening for new jobs
Money
Avoiding my pastor and others
who try to help me
Not sure

- Quit using cocaine
- To know myself better
- I deserve to feel happier.
- I want to work and have my own place.
- Keep appointment next week -Spend time with family
- Go back to church >1x per week
- Consider IOP treatment & attending 12 step meeting
- Not judging me
- Listening to me and giving me honest feedback
- People/places/things
- Isolating

Shame
Guilt
Disappointing
my family
Worried about
legal issues
Used cocaine
By myself
Friday afternoon
My son’s home
Disconnected, not thinking
about my situation
-Feeling down
about situation
-Not wanting to
be around
people
-Thinking about
using
- Son asked me
to have dinner
with the family
- Friday night
Not thinking
about my
situation for a
few moments;
feeling high

- Son/Family
- Pastor
- Veterans
Resources
- Narcotics Anon
-Emotional/spending
time together
- Spiritual
- Understanding /
Link to resources
- Recovery support
- Say yes when they
ask me to spend time
with them
- Return phone call
- Go to multiservice
center
- Attend a meeting

Church
Computer
class
Veteran
Support
Group
Job
search
Job
search
Call
pastor Dinner
with
family
NA
Meeting
Read at
library
Walk
near
Penns
Landing
Spend
time with
grandson



Plan meals ahead of time.
Get something to eat.
Go for a walk. Call my pastor. Write
in my journal. Think of the big picture.
Write a letter. Spend time with my
son and grandson. Just “Be”
Prioritizing sleep. Taking a nap.
Resting.
Reach out to recovery supports. Go
to the library and get a new book.
Take pictures around the city.
Spend time with family. Think of big
picture. Call recovery supports.

Case Studies
Case Presentation #2
Caucasian male in his late 40s
Uses cocaine, ETOH, marijuana on an
almost daily basis
History of intravenous drug abuse
Last in substance abuse treatment 5 years ago
Challenges
Strengths

Factors Associated with
Successful Outcomes
Integrated Health Clinics
Primary Care Providers addressing substance abuse
as part of a person’s medical visit
Knowledge of available resources
Developing community partnerships with substance
abuse treatment facilities

Preliminary Results Screening and Enrollment Rates
Participant Characteristics
Demographic Characteristics of Sample
Substance Use Characteristics of Sample
Patient Engagement with Intervention
Satisfaction
Compliance with Intervention
Referral Rates

Screening and Enrollment Rates
Site 1 Site 2 Site 3 Total
Received Initial
Screener 5,112 1,769 3,575 10,456
Flagged for
Drug/Alcohol Use 1,382 772 1,083 3,237
Screened for Study
Eligibility 830 475 638 1,943
Ineligible 547 184 240 971
Eligible 280 289 397 966
Enrolled 113 223 227 563
SBIRT 57 111 115 283
SBIRT+ 56 112 112 280

Participant Characteristics Mean Age (SD) 39.69 (12.80)
Female 45%%
Black 81%
White 7%
Other 12%
Hispanic 8%
Less than HS 25%
HS/GED 61%
More than HS 14%
Employed (FT or PT) 30%
Married 10%
Widowed/Divorced/Separated 23%
Never Married 67%
Homeless 14%
• There were no
significant
differences
between
conditions on
any of these
characteristics

Substance Use Characteristics SBIRT SBIRT+
Primary Substance
Alcohol 33.0% 35.5%
Marijuana 37.9% 37.1%
Other Illicit Substances 29.1% 27.4%
Days of Any Alcohol Use (SD) 9.51 (9.77) 10.44 (10.07)
Days of Heavy Alcohol Use (SD) 5.39 (8.29) 5.33 (8.44)
Days Marijuana Use (SD) 11.29 (12.61) 11.45 (12.75)
Days Any Illicit Drug Use (SD) 14.44 (12.3) 13.81 (12.29)
Days Used Primary Substance (SD) 16.71 (11.12) 15.94 (11.48)
Previously In Treatment 49.2% 50.4%
• There were no significant differences between
conditions on any of these characteristics.
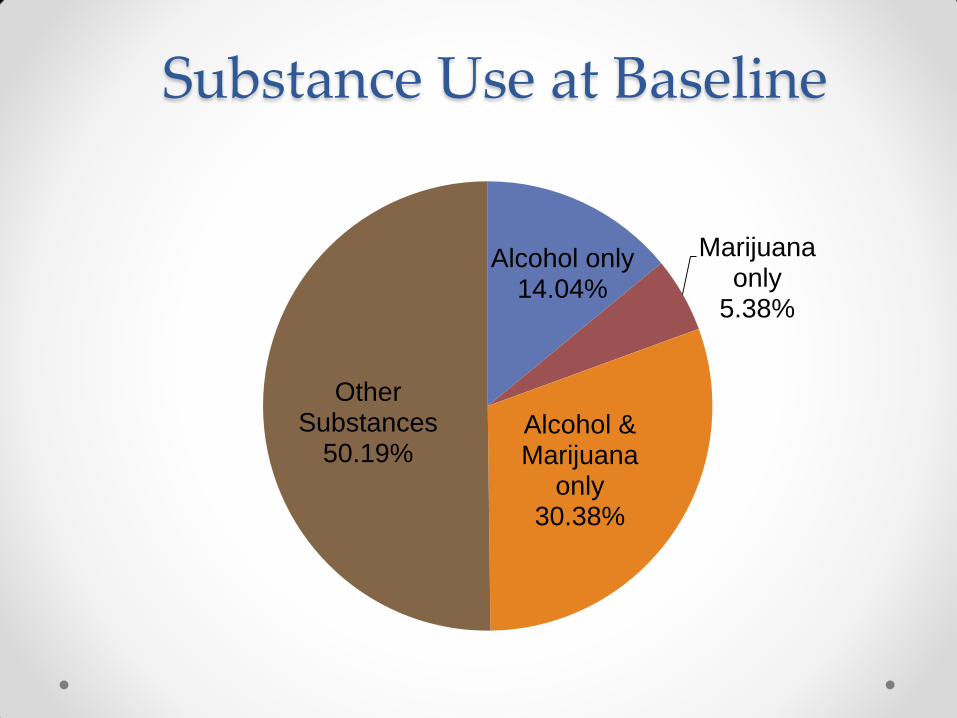
Substance Use at Baseline
Alcohol only 14.04%
Marijuana only
5.38%
Alcohol & Marijuana
only 30.38%
Other Substances
50.19%

Primary Alcohol Users

Primary Marijuana Users

Primary Other Substance Users
0%
20%
40%
60%
80%F
req
uen
cy
Primary Substance

Patient Satisfaction
How helpful was it to be asked about your drug and
alcohol use at the health center:
M=8.59 (SD=2.23) out of 10
How comfortable were you discussing your drug and
alcohol use:
M=9.29 (SD=1.55) out of 10

Intervention Engagement
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6
Sessions Completed
SBIRT
SBIRT+
Percent Attending Intervention Sessions

Treatment Referrals
57.8% of patients reported receiving a referral for
specialty services.
Of those, 59.5% reported that they did not receive
any services
20.4% of patients reported entering treatment

Conclusions
FQHC patients with substance use disorders will return
for brief treatment visits focused on harm reduction /
abstinence
Patients reported significant comfort and acceptability
of screening and brief treatment in primary care
Despite efforts to increase specialty care treatment
entry, actual engagement rates remained low
Our future reporting will analyze differences in
outcomes between SBIRT / SBIRT+ patients on
substance use and medical health variables

For More Information
67
Elizabeth Byrne 215-439-4549 [email protected]
Adam Brooks 215-399-0980 [email protected]
Kimberly Malayter 215-219-9661 [email protected]