scott w. smilen, md - gi health foundation · 2015-06-26 · endoanal ultrasound normal (sphincters...
TRANSCRIPT

Scott W. Smilen, MD Director, Division of
Urogynecology/Reconstructive
Pelvic Surgery NYU Langone Medical Center
New York, NY

Disclosure Statement
This activity has been planned and implemented in
accordance with the Essential Areas and policies of the
Accreditation Council for Continuing Medical Education
(ACCME) through the joint sponsorship of the Annenberg
Center for Health Sciences at Eisenhower and The Gi
Health Foundation. The Annenberg Center for Health
Sciences at Eisenhower is accredited by the ACCME to
provide continuing medical education for physicians.

Learning Objectives
• Describe the epidemiology and burden of illness,
pathophysiology, and diagnostic evaluation of fecal
incontinence (FI)
• Describe the current and future management of FI
• Discuss the pros and cons of medical vs. surgical
approaches for the management of patients with FI
• Formulate an appropriate treatment plan for fecal
incontinence, taking into account clinical
presentation and patient preference

Fecal Incontinence:
Epidemiology and
Burden of Illness

Prevalence of Fecal Incontinence:
Fast Facts
Overall prevalence of
fecal incontinence: 9.0%
Prevalence of fecal
incontinence occurring at
least once weekly: 1.1%
Prevalence in men: 7.4%
Prevalence in women: 9.1%
Prevalence in individuals
aged ≥70 years: 17.5% 0
2
4
6
8
10
2005/2006 2009/2010
Prevalence of FI
(≥1 time in previous month)*
Su
bje
cts
(%
)
*Data from NHANES 2005/2006 and 2009/2010 surveys. N=52,195.
Ditah I et al. Am J Gastroenterol. 2012;107:S717. Abstract 1762.

Fecal Incontinence is Associated
with High Economic Cost
Xu X et al. Dis Colon Rectum. 2012;55(5):586-598.
• Average annual cost to patients with FI is
$4,110
– Total costs range between $0 and $46,342
• Indirect costs resulting from lost productivity
at work and lost household productivity
average $1,549
• Direct medical and nonmedical costs
average $2,353
– Surgical costs up to $25,246
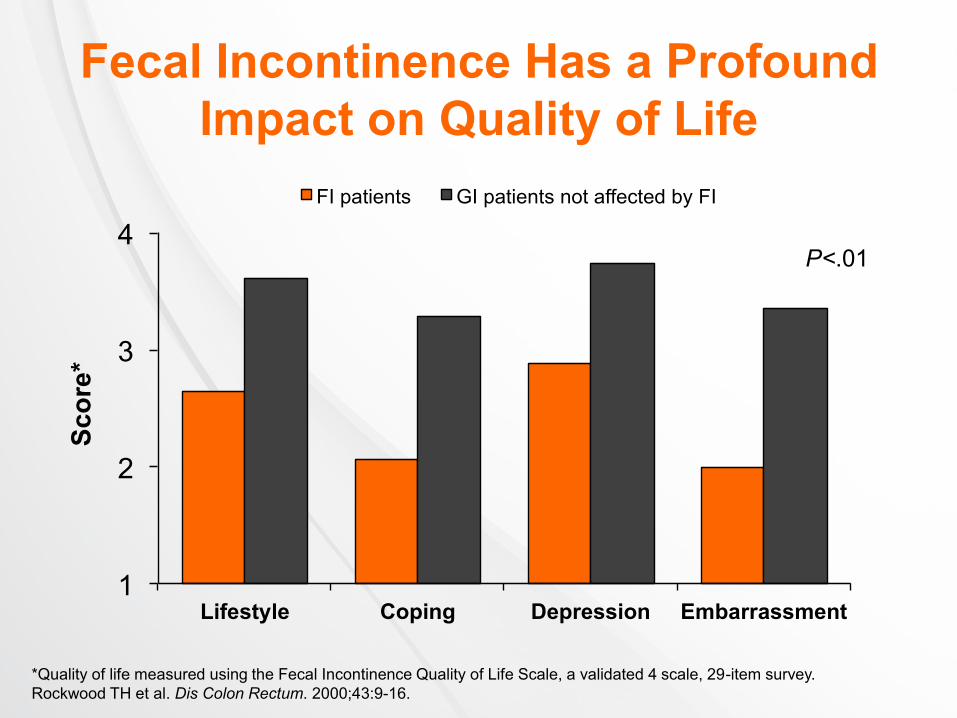
Fecal Incontinence Has a Profound
Impact on Quality of Life
1
2
3
4
Lifestyle Coping Depression Embarrassment
FI patients GI patients not affected by FI
P<.01
*Quality of life measured using the Fecal Incontinence Quality of Life Scale, a validated 4 scale, 29-item survey.
Rockwood TH et al. Dis Colon Rectum. 2000;43:9-16.
Sco
re*

What is Most Bothersome to
Patients With FI?
Rank Symptom
1 Urgency
2 Frequency
3 Mucous
4 Bothersome/embarrassment
5 Straining
6 Intestinal discomfort
7 Consistency
8 Volume
9 Gas
Heymen S et al. Digestive Disease Week 2014. Abstract no. Mo2024.

Pathophysiology of
Fecal Incontinence

Anatomy of the Anorectum
Welton ML et al. Anorectum. In: Doherty GM, ed. Current Diagnosis & Treatment Surgery. New York, NY: The McGraw-Hill
Companies, Inc.;2010:698-723.

Rao SSC. Gastroenterology. 2004;126:S14-S22.
Structural
Abnormalities
Functional
Abnormalities
Stool
Characteristics
Pathophysiology of
Fecal Incontinence

Structural Abnormalities
ANS=autonomic nervous system; CNS=central nervous system
Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
Anatomic Structure Cause Mechanistic Effect
Anal sphincter muscle • Obstetric injury
• Hemorrhoidectomy, anal dilation,
secondary to neuropathy
Sphincter weakness
Loss of sampling reflex
Rectum • Inflammation
• IBD
• Radiation
• Rectal prolapse
• Aging
• IBS
Loss of accommodation
Loss of sensation
Hypersensitivity
Puborectalis muscle • Excessive perineal descent
• Aging
• Trauma
Obtuse anorectal angle
Sphincter weakness
Pudendal nerve • Obstetric or surgical injury
• Excessive straining/perineal descent
• Rectal prolapse
Sphincter weakness
Sensory loss, impaired
reflexes
CNS, spinal cord, ANS • Spinal cord, head injury
• Back surgery
• Multiple sclerosis, diabetes, stroke,
avulsion injury
Loss of sensation
Impaired reflexes
Secondary myopathy
Loss of accommodation

Functional Abnormalities
1. Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Engel AF et al. Gut. 1994;35:857-859.
• Anorectal sensation impairment1
– May be caused by aging, neurologic damage, mental
impairment2
– Impairment in anorectal sensation may lead to:1
• Excessive accumulation of stool
• Fecal overflow
• Impairment of the sampling reflex
• Fecal impaction caused by dyssynergic defecation1
– May result in fecal retention with overflow and
leakage of liquid stool

Stool Characteristics
Rao SSC et al. Gastroenterology. 2004;126:S14-S22.
• Stool consistency, volume, and
presence of irritants in the stool
may contribute to fecal
incontinence
– Large-volume liquid stools require
intact sensation and unimpaired
sphincter function to be retained
• Stool characteristics may be
influenced by:
– Infection
– Inflammatory bowel disease
– Irritable bowel syndrome
– Medications
– Food intolerances

Other Mechanisms Underlying
Fecal Incontinence
Rao SSC et al. Gastroenterology. 2004;126:S14-S22.
• Limited physical mobility,
particularly among the
elderly and those with
neurologic diseases
• Decreased cognitive
function
• Willful soiling in patients
with psychosis

History, Physical Exam,
and Diagnostic Tests
Diagnosis of
Fecal Incontinence

Diagnostic Evaluation
Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
• History
• Physical exam, including digital rectal exam
• Diagnostic tests

Adapted from Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
A Detailed History is Critical When
Evaluating Patients With Suspected Fecal
Incontinence
1. Severity, duration, and timing
2. Obstetric history (eg, forceps, tears,
presentation, repair)
3. Assess diet and lifestyle
4. History of fecal impaction
5. Determine clinical subtype (passive
incontinence, urge incontinence, fecal
seepage)

23%
87%
0
20
40
60
80
100
Disclosed FI Disclosed UI
Pa
tie
nts
(%
)
Relative disclosure of UI and FI in
women with dual incontinence
UI=urinary incontinence.
Cichowski SB et al. Int Urogynecol J. 2014.
Patients are Far Less Likely to
Disclose FI than UI
1. Determine the Severity, Duration,
and Timing of Fecal Incontinence

*Other than none; †Higher scores indicate more severe incontinence
1. Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Seong M-K et al. J Korean Surg Soc. 2011;81:326-331.
Frequency Type Impact Range†
Lowest* Highest Gas Liquid Solid Others Pad
usage
Lifestyle
alteration
Wexner <1/month >1/day + + + — + + 0-20
FISI 1-3/month >2/day + + + Mucus — — 0-61
Scoring Systems for Measuring the Severity of Fecal Incontinence2
1. Determine the Severity, Duration,
and Timing of Fecal Incontinence
• Severity can be formally quantified and tracked
during treatment using grading systems1,2

1. Determine the Severity, Duration,
and Timing of Fecal Incontinence
1. Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Seong M-K et al. J Korean Surg Soc. 2011;81:326-331.
• A stool diary1 can be used to quantify frequency,
impact, subtype, and potential correlations2

2. Obstetric History
1. Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Kamm MA. Lancet. 1994;344:730-733; 3. Engel AF et al.
Int J Colorectal Dis. 1995;10:152-155; 4. Gee AS, Durdley P. Br J Surg. 1995;1179-1182; 5. Hill J et al. Dis Colon Rectum.
1994;37:473-477.
• In adult women, obstetric trauma may increase risk for fecal
incontinence1-4
– ~35% of primiparous women show evidence of sphincter disruption
following normal vaginal delivery1
• Injury may involve:1
– External anal sphincter
– Internal anal sphincter
– Pudendal nerves
• Obstetric risk factors:1,5
– Forceps delivery
– Prolonged second stage of labor
– High birth weight
– Occipito-posterior presentation

3. Assess Diet, Medications,
and Lifestyle
Adapted from National Institute for Health and Clinical Excellence (NICE). CG49 Faecal incontinence: tables.
Available at: http://www.nice.org.uk/CG49Tables#table2. Accessed March 30, 2013.
Dietary components that may elicit or exacerbate fecal incontinence
Fiber Fiber supplements, whole-grain cereals or bread,
whole-wheat based cereals
Certain fruits and
vegetables Rhubarb, figs, prunes, plums, beans, cabbage, sprouts
Spices Chili powder
Alcohol Especially stouts, beers, or ales
Lactose/fructose Milk, other high-lactose or high-fructose foods
Caffeine Coffee, tea, sodas
Vitamin and mineral
supplements
Excessive vitamin C, magnesium, phosphorus, and/or
calcium
Olestra fat substitute Can cause loose stools

3. Assess Diet, Medications,
and Lifestyle
Adapted from National Institute for Health and Clinical Excellence (NICE). CG49 Faecal incontinence: tables.
Available at: http://www.nice.org.uk/CG49Tables#table2. Accessed March 30, 2013
Medications that may elicit or exacerbate fecal incontinence
Drugs that alter
sphincter tone
Nitrates, calcium channel antagonists, beta-blockers,
sildenafil, SSRIs
Broad-spectrum
antibiotics Cephalosporins, penicillins, erythromycin
Topical drugs applied
to anus
Glyceryl trinitrate ointment, diltiazem gel, bethancechol
cream, botulinum toxin A injection
Drugs causing
profuse loose stools
Laxatives, metformin, orlistat, SSRIs, magnesium-
containing antacids, digoxin
Tranquilizers or
hypnotics Benzodiazepines, SSRIs, antipsychotics

4. History of Fecal Impaction
Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
• Fecal impaction:
– Results in prolonged
relaxation of internal
anal sphincter tone
– Allows liquid stool to
flow around
impacted stool and
escape through the
anal canal

5. Determine Clinical Subtype of
Fecal Incontinence
EAS=external anal sphincter; IAS=internal anal sphincter
1. Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604; 2. Rao SSC et al. Gastroenterology. 2004;126:S14-S22.
• Passive incontinence1,2
– Unaware of stool or gas passage; associated with
diseased or disrupted IAS
• Urge incontinence1,2
– Release of feces despite awareness and attempted
retention; 88% associated with EAS dysfunction
• Fecal seepage1,2
– Presence of small amount of fecal material on
undergarments; thought to be due to impaired rectal
sensation

The Physical Exam
Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
• Inspect for presence of:
– Fecal matter
– Prolapsed hemorrhoids
– Dermatitis
– Scars
– Skin excoriation
– Absence of perianal creases
– Gaping anus

The Physical Exam (continued)
Rao SSC et al. Am J Gastroenterol. 2004;99:1585-1604.
• Examine for excessive perineal descent or
rectal prolapse
– Ask patient to attempt defecation
– A bulge that exceeds 3 cm is usually defined as
excessive
• Check perianal sensation
– Gently stroke perianal skin with cotton bud in each
quadrant
– Normal response: brisk contraction of anal sphincter
– Impaired or absent anocutaneous reflex suggests
afferent or efferent neuronal injury

The Physical Exam
Wald A. N Engl J Med. 2007;356:1648-1655.
Position 1—Check Anal
Tone at Rest
Position 2—Insert Finger More Deeply
and Feel Puborectalis Muscle

Diagnostic Testing
Physiologic Test Measurements Evidence
Anorectal
manometry
Quantifies sphincter pressures,
sensation, rectal compliance and
recto-anal reflexes
Good
Endoanal
ultrasound
Assesses IAS and EAS
thickness, integrity Good
Needle EMG
Distinguishes between
neuropathy and myopathy Fair
Surface EMG
Provides information on normal
or weak tone Fair
Adapted from: Rao SSC. Clin Gastroenterol Hepatol. 2010;8:910-919.

Endoanal Ultrasound
Normal (Sphincters Intact) Abnormal (Sphincters Disrupted)
Subjective interpretation of ultrasound results may limit its value
E=external anal sphincter; I=internal anal sphincter
Rottenberg GT, Williams AB. Br J Radiol. 2002;75:428-488.

Management of
Fecal Incontinence Dietary, Lifestyle, Pharmacologic
Interventional/Surgical

Management of
Fecal Incontinence Surgical Modalities

Surgical Management of
Fecal Incontinence
Intervention Mechanism of
Action Side Effects Comments
Sacral nerve stimulation
Increases stool
consistency and
anal sphincter tone;
decrease urgency
Infection; lead fracture
or migration Relatively safe
Secca procedure
Healing of RF-
induced lesions
changes tone
Tissue damage Relatively safe
Artificial sphincter Restores anal
barrier
Device erosion, failure,
infection
High morbidity; seldom
used
Sphincteroplasty for
sphincter defects
Restores sphincter
integrity
Wound infection
delayed recurrent FI
Beneficial effects
decrease over time;
indicated for IAS defects
without denervation
Colostomy Reserved for
most severe
IAS=internal anal sphincter.

Female Pelvic Anatomy


Sphincter Repair
• Overlapping or end-to-end
• Recovery from surgery
– Bowel management
– Wound care
• Outcomes
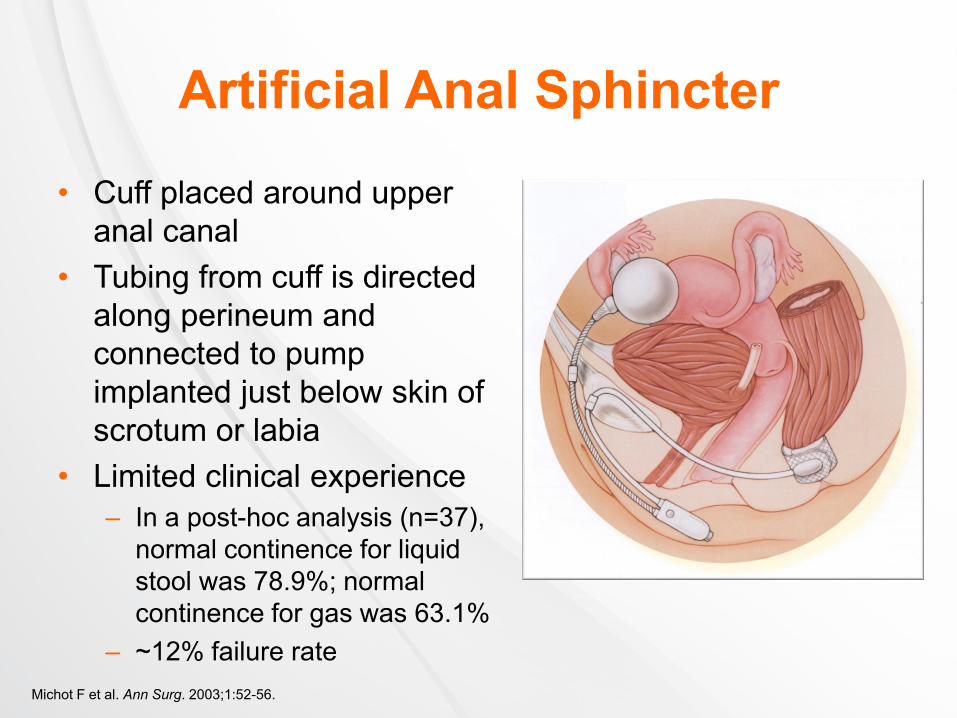
Artificial Anal Sphincter
• Cuff placed around upper
anal canal
• Tubing from cuff is directed
along perineum and
connected to pump
implanted just below skin of
scrotum or labia
• Limited clinical experience
– In a post-hoc analysis (n=37),
normal continence for liquid
stool was 78.9%; normal
continence for gas was 63.1%
– ~12% failure rate
Michot F et al. Ann Surg. 2003;1:52-56.

Conclusions
• Fecal incontinence is multifactorial
• Physiological evaluation facilitates optimal
therapy
• Lifestyle measures
– Avoid coffee
– Lactose-free diet
• Biofeedback training main type of
conservative therapy

Conclusions
• Most parous women with FI have
anatomic sphincter defects
• Sphincter defects can be repaired
surgically, but continence will not always
be restored
• Newer modalities may be of benefit
(Solesta, magnetic sphincter)

Conclusions

Treatment Options for
Fecal Incontinence
Conservative
Therapies
Conservative
Therapies
Dextranomer
Microsphere
Injection
Dextranomer
Microsphere
Injection
Surgical
Therapies
Surgical
Therapies
• Generally safe
• Limited evidence
of benefit
• Generally safe
• Limited evidence
of benefit
• Generally safe
• Requires in-office
procedure
• Longer-term evidence for
benefit required
• Generally safe
• Requires in-office
procedure
• Longer-term evidence for
benefit required
• Invasive
• Potential safety issues
• Long-term benefit may
be limited
• Invasive
• Potential safety issues
• Long-term benefit may
be limited