scimitar syndrome with tetralogy of fallot and pulmonary ... · case report scimitar syndrome with...
TRANSCRIPT
The Egyptian Heart Journal (2015) 67, 275–277
HO ST E D BYEgyptian Society of Cardiology
The Egyptian Heart Journal
www.elsevier.com/locate/ehjwww.sciencedirect.com
CASE REPORT
Scimitar syndrome with tetralogy of fallot
and pulmonary atresia
* Corresponding author. Address: Department of Cardiac Sciences
(MC: 1420), King Abdulaziz Medical City, P.O. Box 22490, Riyadh
11426, Saudi Arabia. Fax: +966 118011111x16855.
E-mail address: [email protected] (S.R. Ismail).
Peer review under responsibility of Egyptian Society of Cardiology.
http://dx.doi.org/10.1016/j.ehj.2014.08.0031110-2608 ª 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Cardiology.
Sameh R. Ismail *, Mustafa A. Al-Muhaya, Mohamed S. Kabbani
King Abdulaziz Medical City, King Saud University for Health Sciences, Department of Cardiac Sciences, National Guardhospital Health Affairs, Riyadh, Saudi Arabia
Received 2 June 2014; accepted 27 August 2014Available online 18 September 2014
KEYWORDS
Scimitar syndrome;
Tetralogy of fallot;
Pulmonary atresia
Abstract Scimitar syndrome is a rare variant of partial anomalous pulmonary venous connection.
The association of Scimitar syndrome with another cardiac congenital anomaly such as tetralogy of
Fallot with pulmonary atresia is extremely rare; we are reporting a successful combined treatment
using transcatheter closure of major aorto-pulmonary collateral and a single-stage surgical
correction in eighteen month old boy diagnosed as Scimitar syndrome with tetralogy of Fallot
and pulmonary atresia.ª 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Cardiology.
1. Case report
An eighteen month old boy was referred to our center due tocyanosis and shortness of breath. He was a product of full term
normal vaginal delivery and the first child in his family. Hisbirth weight was 3.5 kg. On admission his weight was 14 kg(95% centile) and height 83 cm (95% centile), oxygen satura-
tion on room air 75–80%. The chest radiography showed mes-ocardia and curvilinear shadow in the right chest (Scimitarsign). Based on the clinical and chest radiography findingsScimitar syndrome was suspected. 2D echocardiogram
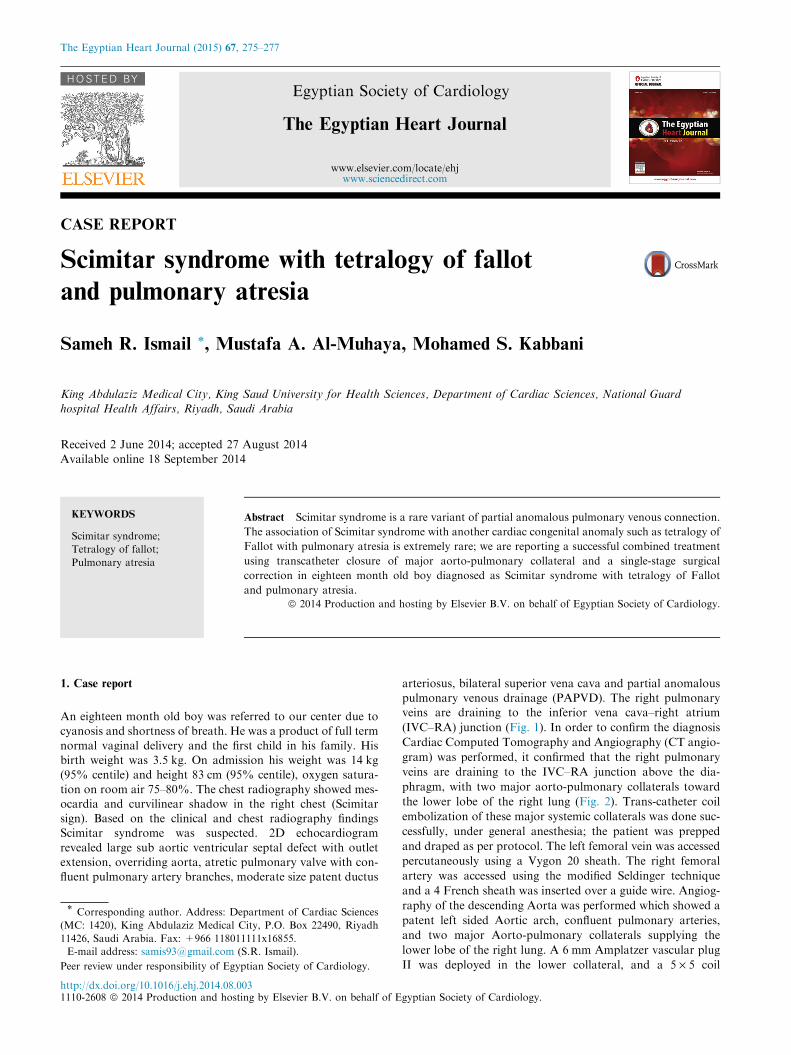
revealed large sub aortic ventricular septal defect with outletextension, overriding aorta, atretic pulmonary valve with con-fluent pulmonary artery branches, moderate size patent ductus
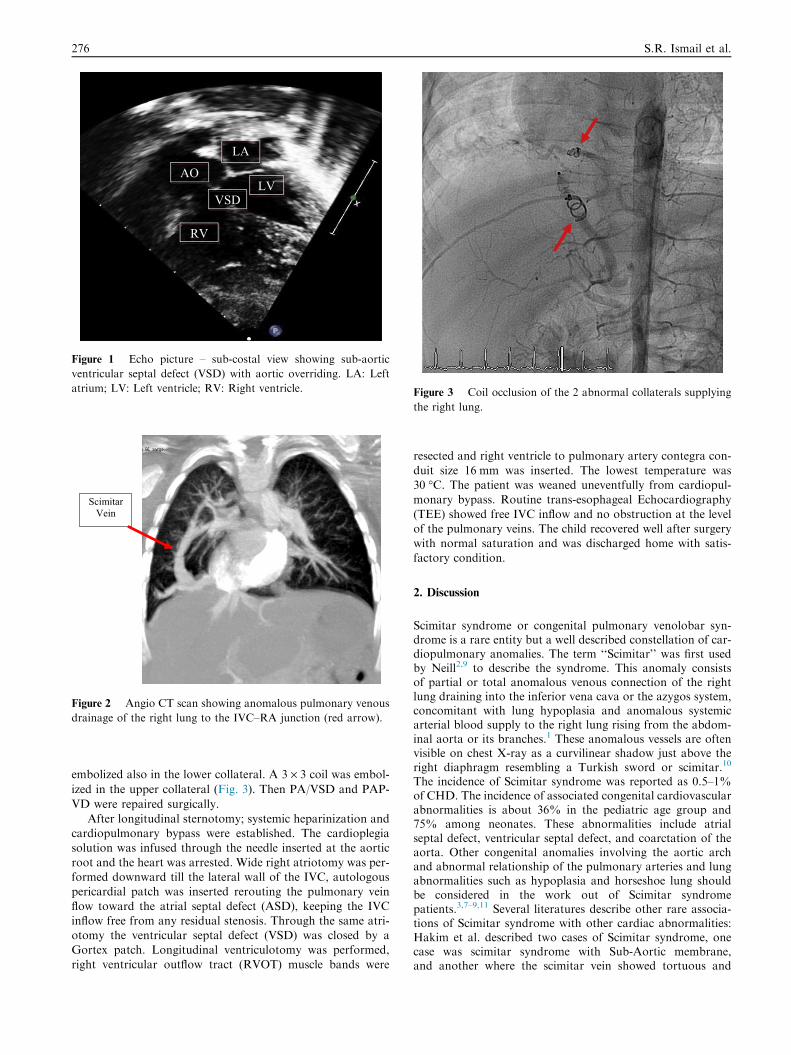
arteriosus, bilateral superior vena cava and partial anomalouspulmonary venous drainage (PAPVD). The right pulmonaryveins are draining to the inferior vena cava–right atrium
(IVC–RA) junction (Fig. 1). In order to confirm the diagnosis
Cardiac Computed Tomography and Angiography (CT angio-
gram) was performed, it confirmed that the right pulmonary
veins are draining to the IVC–RA junction above the dia-
phragm, with two major aorto-pulmonary collaterals toward
the lower lobe of the right lung (Fig. 2). Trans-catheter coil
embolization of these major systemic collaterals was done suc-
cessfully, under general anesthesia; the patient was prepped
and draped as per protocol. The left femoral vein was accessed
percutaneously using a Vygon 20 sheath. The right femoral
artery was accessed using the modified Seldinger technique
and a 4 French sheath was inserted over a guide wire. Angiog-
raphy of the descending Aorta was performed which showed a
patent left sided Aortic arch, confluent pulmonary arteries,
and two major Aorto-pulmonary collaterals supplying the
lower lobe of the right lung. A 6 mm Amplatzer vascular plug
II was deployed in the lower collateral, and a 5 · 5 coil
AO
VSD
LA
LV
RV
Figure 1 Echo picture – sub-costal view showing sub-aortic
ventricular septal defect (VSD) with aortic overriding. LA: Left
atrium; LV: Left ventricle; RV: Right ventricle.
Scimitar Vein
Figure 2 Angio CT scan showing anomalous pulmonary venous
drainage of the right lung to the IVC–RA junction (red arrow).
Figure 3 Coil occlusion of the 2 abnormal collaterals supplying
the right lung.
276 S.R. Ismail et al.
embolized also in the lower collateral. A 3 · 3 coil was embol-
ized in the upper collateral (Fig. 3). Then PA/VSD and PAP-
VD were repaired surgically.
After longitudinal sternotomy; systemic heparinization andcardiopulmonary bypass were established. The cardioplegiasolution was infused through the needle inserted at the aortic
root and the heart was arrested. Wide right atriotomy was per-formed downward till the lateral wall of the IVC, autologouspericardial patch was inserted rerouting the pulmonary vein
flow toward the atrial septal defect (ASD), keeping the IVCinflow free from any residual stenosis. Through the same atri-otomy the ventricular septal defect (VSD) was closed by aGortex patch. Longitudinal ventriculotomy was performed,
right ventricular outflow tract (RVOT) muscle bands were
resected and right ventricle to pulmonary artery contegra con-
duit size 16 mm was inserted. The lowest temperature was30 �C. The patient was weaned uneventfully from cardiopul-monary bypass. Routine trans-esophageal Echocardiography
(TEE) showed free IVC inflow and no obstruction at the levelof the pulmonary veins. The child recovered well after surgerywith normal saturation and was discharged home with satis-
factory condition.
2. Discussion
Scimitar syndrome or congenital pulmonary venolobar syn-drome is a rare entity but a well described constellation of car-diopulmonary anomalies. The term ‘‘Scimitar’’ was first usedby Neill2,9 to describe the syndrome. This anomaly consistsof partial or total anomalous venous connection of the rightlung draining into the inferior vena cava or the azygos system,concomitant with lung hypoplasia and anomalous systemicarterial blood supply to the right lung rising from the abdom-inal aorta or its branches.1 These anomalous vessels are oftenvisible on chest X-ray as a curvilinear shadow just above theright diaphragm resembling a Turkish sword or scimitar.10
The incidence of Scimitar syndrome was reported as 0.5–1%of CHD. The incidence of associated congenital cardiovascularabnormalities is about 36% in the pediatric age group and75% among neonates. These abnormalities include atrialseptal defect, ventricular septal defect, and coarctation of theaorta. Other congenital anomalies involving the aortic archand abnormal relationship of the pulmonary arteries and lungabnormalities such as hypoplasia and horseshoe lung shouldbe considered in the work out of Scimitar syndromepatients.3,7–9,11 Several literatures describe other rare associa-tions of Scimitar syndrome with other cardiac abnormalities:Hakim et al. described two cases of Scimitar syndrome, onecase was scimitar syndrome with Sub-Aortic membrane,and another where the scimitar vein showed tortuous and

Scimitar syndrome 277
abnormal course of the pulmonary veins with normal drainageinto the left atrium.1 Takeda reported two cases: in one casethe scimitar vein entered both the inferior vena cava and theleft atrium without any intracardiac shunt; in the other casethe Scimitar vein showed a meandering course and thendrained into the left atrium, so surgical intervention was notrequired.6 Bilateral scimitar syndrome with abnormal venousdrainage to inferior vena cava has also been described.11
Isolated partial anomalous pulmonary venous return to theinferior caval vein is also called incomplete scimitar syn-
drome.4 The typical scimitar sign was present in 57 of the 67cases reviewed by Kiely et al.1,5 Association of pulmonaryatresia, ventricular septal defect and Scimitar syndrome is a
very rare combination. Our case had the classical characteris-tics of Scimitar syndrome with pulmonary atresia andventricular septal defect. Pre-operative diagnostic cardiaccatheterization and CT angiography have central role in the
diagnosis of such variation especially when the pattern ofpulmonary venous drainage is not clearly identified byechocardiography.4 After successful combined trans-catheter
and surgical repair, the patient had smooth outcome andwas discharged home with full recovery. One month later anechocardiography follow-up was performed showing no
residual cardiac lesions and pulmonary vein flow pattern wasnormal. As the risk of baffle obstruction at follow-up is wellreported12 we keep our patients on low dose aspirin therapy
for prophylaxis.We can conclude from this case study that CT angiogram
and cardiac angio catheterization are the most appropriatediagnostic modalities to confirm the anatomy of this unusual
variant of Scimitar syndrome. Combination of therapeuticangiography and surgery was feasible, and contributed to thesuccess of this case management. Elimination of collateral
flow, correcting the venous drainage and correcting intra-cardiac abnormality help in preventing the development ofpulmonary hypertension and normalize the blood flow to the
lung which make the hybrid approach ideal for short and longterm results.
Conflict of interest
I disclose that there were no conflict of interest and no fundingfor this study and it was approved by the hospital ethics
committee.
References
1. Hakim F, Madani A, Abu Haweleh A. Two cases report of
scimitar syndrome: the classical one with subaortic membrane and
the scimitar variant. Bahrain Med Bull 2000;22(1):1–5.
2. Neill CA, Ferencz C, Sabiston DC, Sheldon H. The familial
occurrence of hypoplastic right lung with systemic arterial supply
and venous drainage ‘‘scimitar syndrome’’. Bull Johns Hopkins
Hosp 1960;107:1–21.
3. Moss, Adams. Heart disease in infant children andadolescent:
including the fetus and young adult. In: Emmanouilides GC, Allen
A, Thomas A, et al., editors. Baltimore: Williams and Wilkins;
2008. p. 761–92, 7th ed.
4. Shegal Arvind, Loughran-Fowlds Alison. Scimitar syndrome.
Indian J Pediatr 2005;72(3):249–51.
5. Kiely B, Flier J, Stenes, et al. A syndrome of anomalous venous
drainage of the right lung to inferior vena cava. Am J Cardiol
1967;20:102.
6. Takeda SI, Imachi T, Arunitsu K, et al. Two cases of scimitar
variant. Chest 1994;105(1):292–3.
7. Morgan JR, Forker AD. Syndrome of hypoplasia of the right
lung. Circulation 1971;43(1):27–30.
8. Gikonyo DK, Tandon R, Lucas Jr RV, Edwards JE. Scimitar
syndrome in neonates: report of four cases and review of the
literature. Pediatr Cardiol 1986;6:193–7.
9. zadeh Soheila Khalil, Hassanzad Maryam, Khodayari Amir-Ali.
Scimitar syndrome. Arch Iran Med 2009;12(1):79–81.
10. Mulligan ME. History of scimitar syndrome. Radiology
1999;210(1).
11. Kabbani M, Haider N, Abu-Sulaiman R. Bilateral scimitar
syndrome. Cardiol Young 2004;14(4):447–9.
12. Najm HK, Williams WG, Coles JG, Rebeyka IM, Freedom RM.
Scimitar syndrome: twenty years experience and results of repair. J
Thorac Cardiovasc Surg 1996;112:1161–9.