schizophrenia: a neuro- developmental disorder of social and cognitive decline demian rose, md, phd
TRANSCRIPT

Schizophrenia: A neuro-developmental disorder of
social and cognitive decline
Demian Rose, MD, PhD

Take Home Point 1
• Schizophrenia is associated with three primary symptom domains: positive symptoms, negative symptoms and cognitive symptoms.– Of these, cognitive symptoms are most
associated with functional impairment, followed by negative symptoms
• Despite this, we have traditionally focused our conceptualization based on positive symptoms

Components of the Illness
Psychotic Symptoms
Negative Symptoms
CognitiveImpairment
hallucinationsdelusions
anergiaanhedoniaamotivation
attentionconcentration
memory

Percent of Patients Ever in Recovery
(5 Follow-ups Over 15-Years)
(Harrow et al., 2005, fig 2)

Take Home Point 2
• Schizophrenia is a neuro-developmental disorder involving abnormal brain development during adolescence and young adulthood– Multiple brain regions are affected in
measurable ways

Copyright restrictions may apply.
Schobel, S. A. et al. Arch Gen Psychiatry 2009;66:938-946.
Dysfunction in multiple regions in brain areas implicated in schizophrenia

Iowa Longitudinal Study of First Iowa Longitudinal Study of First Episode Schizophrenia Episode Schizophrenia
(Investigator: Nancy Andreasen, MD)(Investigator: Nancy Andreasen, MD)
• Hundreds of subjects recruited over 20 years– All adolescents or young adults
• Half of all subjects show significant brain tissue loss in the frontal lobes (at least 0.5% per year)– One-third of all subjects lose average of 1% per year– Normal loss is on the order of 0.1-0.2% per year– Most loss in Schizophrenia occurs in the first few
years after diagnosis

Take Home Point 3
• The cognitive and social dysfunction associated with schizophrenia typically pre-dates the onset of the more easily identified “psychotic” symptoms

Copyright restrictions may apply.
Insel, T. R. Arch Gen Psychiatry 2009;66:128-133.
Potential neurodevelopmental stages of schizophrenia

Cognitive deficits predate psychotic symptoms
• Simon (2007) Schizophrenia Bulletin, vol 33, pg 761-71
FE = first episode schizophrenia, UHR = ultra high risk for developing schizophreniaBS/PCO = controls

Take Home Point 4
• By the time of first diagnosis, a crucial time for successful intervention, abnormal brain development and cognitive deficits are already significant, and many psychosocial supports are already in jeopardy
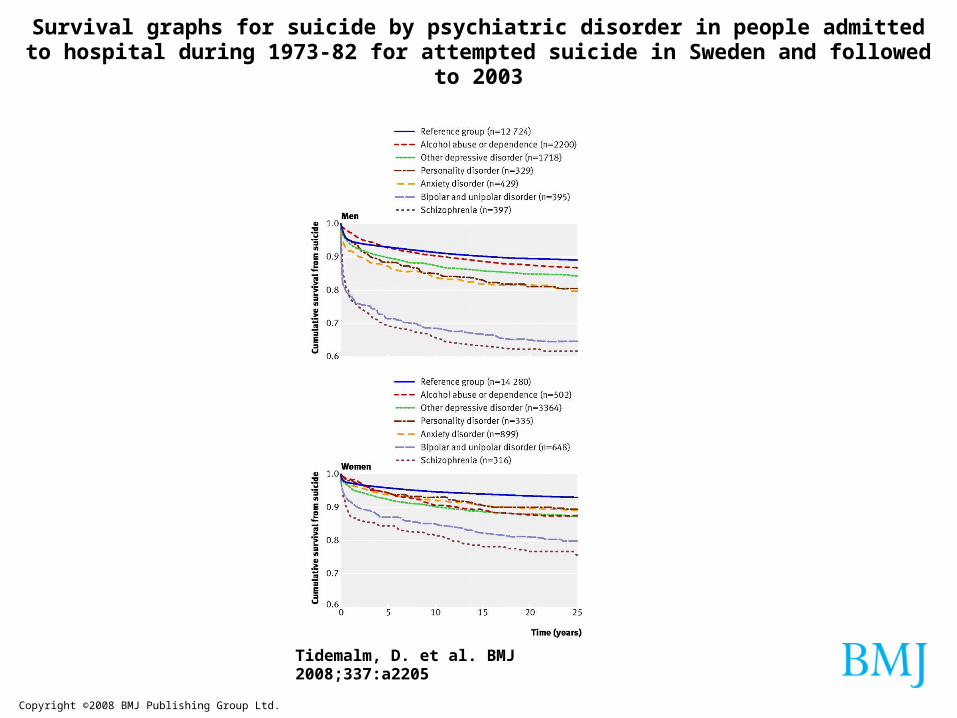
Copyright ©2008 BMJ Publishing Group Ltd.
Tidemalm, D. et al. BMJ 2008;337:a2205
Survival graphs for suicide by psychiatric disorder in people admitted to hospital during 1973-82 for attempted suicide in Sweden and followed to 2003

Duration of Untreated Psychosis Matters
Finding isconsistentacrossmany studies
Perkins (2005)AJP, 162:1785

-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
GlobalCognition
Speed ofProcessing
VerbalWorkingMemory
VerbalLearning
VerbalMemory
ProblemSolving
Non-VerbalWorkingMemory
VisualLearning
VisualMemory
SocialCognition
Bas
elin
e Z
-Sco
re
AT (N=29) CG (N=26)
People with schizophrenia have significant deficits in many measurable domains of cognition (1 to 2 standard deviations below the mean, i.e. as low as 5th percentile)
Schizophrenia is defined as much by cognitive deficits as by psychotic symptoms
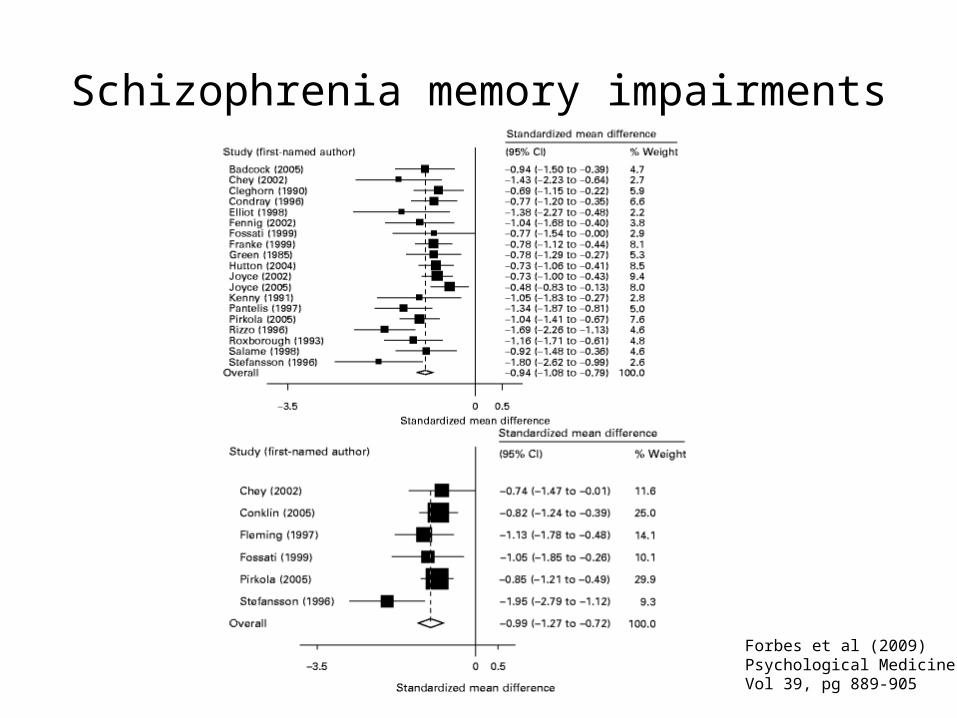
Schizophrenia memory impairments
Forbes et al (2009) Psychological MedicineVol 39, pg 889-905

Impairments affect “real world” activities of daily living
• When cooking a meal:– “Sequencing errors, repetitions and
omissions were significantly higher [in people with schizophrenia] compared to controls”
Stip (2006) Encephale, vol 3, pg 341-50

Social deficits can be comparable to Autism in type
• People with schizophrenia have deficits in social cognition that are comparable to people with high-functioning autism– Poor emotion perception– Poor ability to accurately guess at the motives
of others
Couture (2009) Psychological Medicine vol 12, pg 1-11

Cognitive deficits can be comparable to Alzheimer’s in severity
• People with schizophrenia have a different pattern of cognitive deficits than people with Alzheimer’s Disease, but are equally or more impaired on measures of: – Naming– Object construction– New learning (encoding)
Davidson (1996) American Journal of Psychiatry vol 153, pg 1274-1279

Take Home Point 5
• If we are to reduce the lifetime morbidity burden of schizophrenia and work towards functional recovery, we must provide a psychosocial framework that allows for evidence-based recovery strategies– In this context, disability benefits can help
ensure recovery, by allowing for a shift from necessary external decision-making to independent living and recovery

Cognitive Impairment and Recovery
• For persons so seriously impaired in their decision
making capacity that they are incapable of
determining what is in their best interest, a
paternalistic externally reasoned treatment approach
seems not only appropriate but also necessary
… .However, as these impaired persons begin to
benefit from externally initiated interventions the
locus of control should increasingly shift from the
treatment provider to the person who is recovering
Frese et al (2001), Psychiatric Services, vol 52, pg 1462-1468

Supported Employment Works (Cook et al., 2005)
Fig 1. Proportion of subjects employed competitively by month

Keeping families involved leads to better outcomes
• Average relapse rates across 11 RTC’s (N = 895)
• Mean length of treatment = 19.7 months
McFarlane, W. R., Dixon, L., Lukens, E., Lucksted, A.
(2003). Family psychoeducation and schizophrenia: a
review of the literature. Journal of Marital and Family
Therapy, 29(2), 223-245.
0
10
20
30
40
50
60
70
TAU SF MF
TAU = treatment as usual, SF = single family group, MF = multifamily group

Cognitive training can enhance back-to-work programs (McGurk et al., 2007)

And all of these evidence-based interventions require:
• Adequate, sustained financial and social services support that begins as soon as possible after diagnosis and assumes a timeline of recovery that is from months to years