sarah fuller april10
TRANSCRIPT
Paediatric Nutrition
Sarah FullerSpecialist Paediatric DietitianLuton and Dunstable Hospital
Outline of talk
Growth and growth charts Standard infant formulas – what’s in the milk? Faltering growth and high calorie formulas
First line advice ‘Allergy’ formulas
CMPI and lactose intolerance – what’s the difference? First line advice
Pre-term formulas When to prescribe and when to stop prescribing!
Anti-reflux formulas Lactose free formulas Weaning – when to start The Under 5’s diet – key points Obesity referrals
The new UK-WHO growth charts New growth charts are to be used in use in England, from
May 2009 (for new births only, so any baby who already has a red book will continue to use the chart already in that).
They show a pattern of healthy growth for all children. They are based on breastfed babies and should be used for all babies, however they are fed.
The new charts are suitable for all ethnic groups. There is a separate page on the charts for babies born
preterm <37 weeks. There are no lines between birth and 2 weeks – this is
because babies have very individual weight patterns at this age.
Babies should be weighed during this time and if there is a weight loss of 10% or more the baby should be examined and feeding reviewed.
The chart no longer has a bold line in the middle. This is to show that a baby growing normally may be anywhere on the chart.
© 2009 Royal College of Paediatrics and Child Health wwwgrowthcharts.rcpch.ac.uk
Infants and toddlers
What is a normal rate of growth?
• Measure length or height whenever concerned about weight gain or growth
• Measurements commonly show wide variation
– If worried measure on a few occasions
– Healthy children usually show a stable general pattern over time
• What is a normal rate of head growth?
– Head circumference usually tracks within one centile space
– Fewer than 1% of infants drop or rise through >2 centile spaces after the first few weeks
Should be carefully assessed

© 2009 Royal College of Paediatrics and Child Health www.growthcharts.rcpch.ac.uk
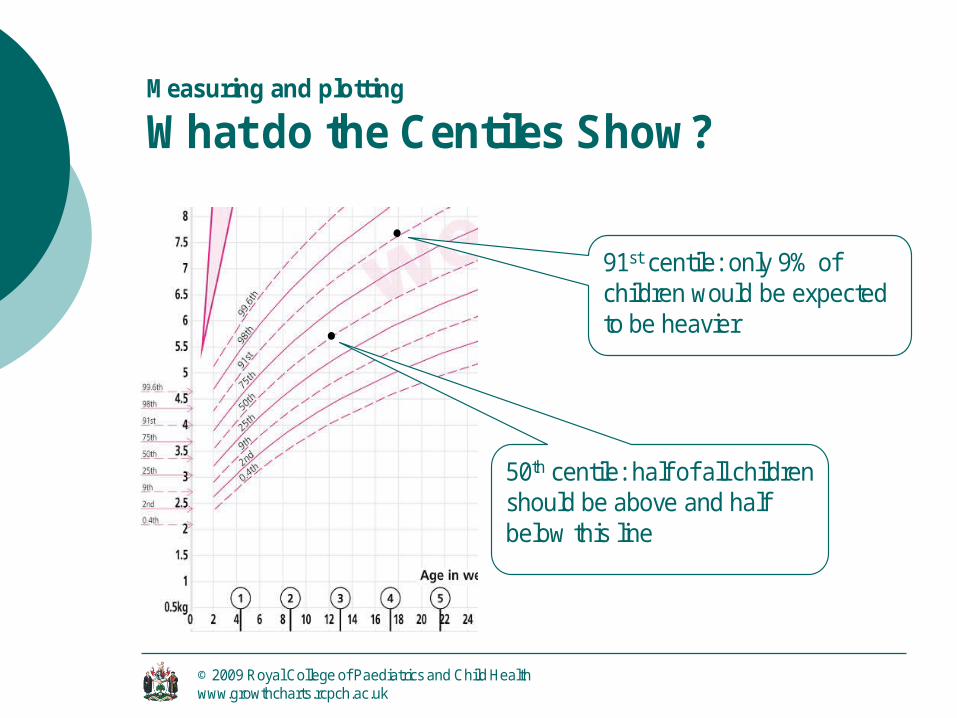
Measuring and plotting
What do the Centiles Show?
50th centile: half of all children should be above and half below this line
91st centile: only 9% of children would be expected to be heavier
Standard infant formula
Curds and whey is cottage cheese!
In milk it refers to the protein Casein Whey

Standard infant formula
Whey Based For infants from birth to one year of age Protein content is 40% casein and 60%
whey same ratio as breast milk and is most suitable
for babies until they swap onto full fat milk Nutritionally complete and do not require
further vitamin or mineral supplementation.
E.g. Cow and Gate premium, SMA Gold, Aptamil First and Heinz Nurture (was known as Farleys First)
Standard infant formula
Casein Based - For ‘hungrier’ babies A higher ratio of casein to whey (80% casein:
20% whey) the same as standard cows milk
There is no reason why babies need to swap to these formulas as they are not higher is calories, protein or micronutrients
Always encourage parents to keep their babies on whey based formulas up to one year of age (can possibly cause constipation in some babies)
E.g. Cow and Gate plus, SMA White, Aptamil Extra, Heinz Nurture Hungry baby
Follow on milks
Higher levels of Fe, Ca, Zn, Vitamins A & C - but these are in a less bio-available form
Often contain pre and pro-biotics e.g.‘immunofortis’ a prebiotic mix in Aptamil
E.g. SMA progress, Cow and Gate (step up, next step and growing up milk), Heinz Nurture Growing
Not prescribable Marketed towards ‘the worried well’ but do
have a place in our local population who can struggle to wean
Standard infant formula – new research
Prebiotics and Probiotics – a new trend with all standard formula manufacturers (except SMA). No definitive research has shown any benefit However, they are found in breast milk
Change in protein – SMA Gold has reduced the total protein level, closer to breast milk and altered the quality of the protein Potential long term benefits from this – public
health impact, lower blood pressure and weight gain mirroring that of breast fed babies (Lien, 2007 & Lawson, 2007)
Lipil - Mead Johnson's special blend of DHA (omega-3 fatty acid) and ARA (omega-6 fatty acid), long chain polyunsaturated fatty acids that are important building blocks for baby's brain and eye development

Faltering growth
Up to 5% of babies Most common in the second 6 months of
life Early, effective intervention is key to
prevent prolonged periods of malnutrition If concerned measure the OFC & length as
well Don’t use the birth centile – babies will
settle to a weight centile ~12 weeks
High calorie formulas
Standard infant formula is 67Kcal and 1.5g protein per 100ml
High calorie formula from birth to 8kg or 1yr SMA High Energy:
Milk based nutritionally complete tube and sip feed
91kcal per 100ml and 2.0g protein per 100ml Infatrini:
Milk based nutritionally complete tube and sip feed
100kcal per 100ml, 2.6g protein per 100ml Lower osmolarity than SMA High Energy

High calorie formulas
Indications for use: Fluid restrictions e.g. in cardiac babies
(usually restricted to 100-120ml/kg/day)
Catch up growth e.g. in FTT Increased energy requirements e.g. CF,
respiratory diseases, prematurity
High calorie formulas/sip feeds
1-6 yr or 8kg – 20kg Paediasure: 101kcal, 2.8g protein per 100ml Paediasure Fibre: 101kcal, 2.8g protein,
0.73g fibre per 100ml Fortini: 150Kcal, 3.4g protein per 100ml Fortini multi fibre: 150Kcal, 3.4g protein,
1.5g fibre per 100ml
Tube feeds1-6years and 8-20kg Nutrini: 100Kcal, 2.8 g prot/100ml Nutrini energy: 150Kcal, 4.1gprot/100ml Nutrini low energy: 75Kcal, 2.1g prot/100ml7-12years and 21-45kg Tentrini: 100kcal, 3.3g prot/100ml Tentrini energy: 150kcak, 4.9g prot/100ml
Can be prescribed an adult feed after this Multi fibre varieties available in all these feeds

Faltering growth
Please monitor !!!!
CMPI and Lactose intolerance
CMPI = Cow’s Milk Protein Intolerance. ~5% of all newborns can have CMPI.
80% of these will grow out of it by 1y, 95% by 3y
Symptoms: Diarrhoea, vomiting, constipation, blood in stools, eczema, refusal of milk, FTT
Treatment – 1st line: Nutramigen 1. IF FTT as well, Neocate LCP.
Refer to Dietetics for milk free weaning advice.
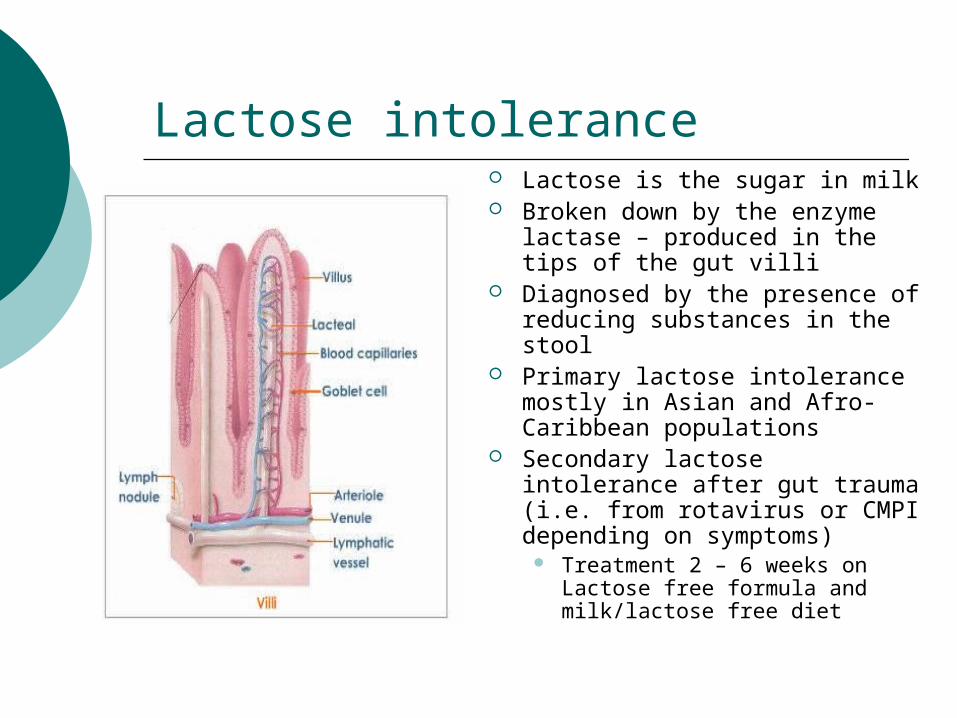
Lactose intolerance Lactose is the sugar in milk Broken down by the enzyme
lactase – produced in the tips of the gut villi
Diagnosed by the presence of reducing substances in the stool
Primary lactose intolerance mostly in Asian and Afro-Caribbean populations
Secondary lactose intolerance after gut trauma (i.e. from rotavirus or CMPI depending on symptoms)
Treatment 2 – 6 weeks on Lactose free formula and milk/lactose free diet
Colic and lactose intolerance
Colic ~ 1 in 5 babies intensity of crying: the baby's face is red and
flushed, the crying is intense and furious, and there is little, or nothing, you can do to comfort them,
body posture – the baby may clench their fists, draw up their knees, or arch their back.
‘Colief’ Drops: Helps compensate for a possible lactase deficiency in the infant’s digestive system – Prescribable Add to the baby’s usual milk (breast milk or formula)
will reduce the level of lactose by up to 70% by breaking down lactose into glucose and galactose, before the baby is fed.
Hydrolysed infant formulas
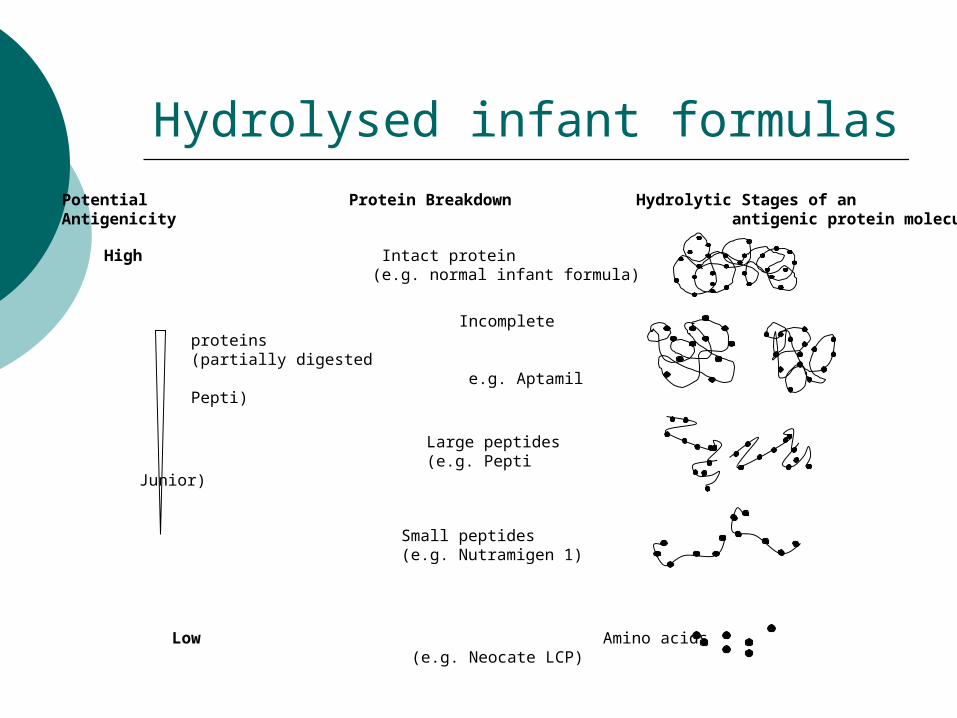
Potential Protein Breakdown Hydrolytic Stages of anAntigenicity antigenic protein molecule
High Intact protein (e.g. normal infant formula)
Incomplete proteins (partially digested e.g. Aptamil Pepti)
Large peptides (e.g. Pepti Junior)
Small peptides (e.g. Nutramigen 1)
Low Amino acids(e.g. Neocate LCP)
Hydrolysed milks
For those suspected of being allergic, intolerant (e.g. CMPI) or mal-absorbing
E.g. Nutramigen 1&2/Pregestimil (Casein based, 95% <1000 Daltons), Pepti-junior (Whey based, 63% <1000 Daltons). Cost ~£9/400g tin and are lactose free Nutramigen has LCT whereas Pregestimil has MCT Note! If >6m babies may not tolerate hydrolysed
formulas due to their bitter taste. They can be flavoured with milkshake or syrups. BUT, this will increase the osmolarity.
Nutramigen 2 has 2g fructose added (puree apple = 19g)
Nutrini Peptisorb – NEW!!! Semi-elemental, 1Kcal/ml, 1-6 years or 8-20Kg. Contains some MCT fat and small amounts of lactose.
Extensively hydrolysed milks
Some babies may still be intolerant to Hydrolysed formulas. Cost ~£25/400g tin Neocate – standard conc. 15% (71Kcal, 2g
prot/100ml), osmolarity is 360mosm/kg Neocate Advance – standard conc. 25%
(100Kcal, 2.5gprot/100ml) osmolarity 610mosm/kg. >1y of age. Complete in 600ml.
Neocate Active – standard conc. 21% (100kcal, 2.8g prot/100ml) osmolarity 520mosm/kg extra Ca, Fe and P. 1 – 10y. Complete in 600ml
Nutramigen AA – NEW!!! 17.5% cheaper, more Na (high levels when concentrated) and Ca. Lower osmolarity than Neocate.
Hydrolysed formulas – non vegetarian
Neocate, Neocate Advance, Neocate Active
Animal ingredients: L-Tyrosine is derived from 2 sources, one
is from chicken feathers One of the vitamins is “carried on” trace
amounts of hydrolysed fish skin gelatine

Hydrolysed formulas – non vegetarian
Nutramigen and Pregestimil Not vegetarian or Halal approved. They use pork enzyme to break down the protein. This equates to: In a standard concentration of
feed there is 0.0125% pork enzyme in 100ml of feed.
Aptamil Pepti and Pepti junior Not Halal approved. No animal ingredients. However animal (calf) rennet is used in the
processing of the feed.
Hydrolysed formulas – non vegetarian
World Health Organisation, July 2001. A seminar held by the Islamic Organisation for
Medical Sciences attended by leading religious spokesmen
‘Transformation which means the conversion of a substance into another substance, different in characteristics, changes substances that are judicially impure or are found in an impure
environment, into pure substances, and changes substances that are prohibited into lawful and
permissible substances’
‘Necessities overrule prohibitions’ – Dire need for specialist infant formula
Elemental feeds
Nutritionally complete liquid diet containinga mix of essential and non-essential aminoacids, carbohydrates, fats, vitamins, minerals, trace elements with added flavourings
Elemental 028 Extra From 1 year of age, but higher osmolarity so we use
>5y 89Kcal, 2.5g protein per 100ml
Emsogen – as Elemental 028, but with MCT fats 88kcal, 2.5g protein per 100ml
Soya formulas Soya e.g. Infasoy, Wysoy, Perjomin Can be given from 6 months. Babies with a family history of atopic disease
(asthma, eczema, hay-fever etc…) should be given a hydrolysed formula
Ideally should be used after 1 year, but can be used from 6m. (BDA Consensus statement, 2009)
Potential long term risks if used <1y – high levels of Phytoestrogens result in longer and heavier periods in females and reduced fertility in males
OK in Galactosaemia
Allergy advice
Refer to a Paediatric Dietitian for specific tailored advice
Useful to know… 90% of ‘may contain’ labels don’t actually
contain the allergen they warn about Use the ingredient list not the free from
advertising (this can be wrong) Foods made in the EU now have the 12
greatest allergens labelled by law Restricted diets often lead to poor bone
health so we will request a Calcium and Vitamin D supplement for patient or mother if breastfeeding

Lactose free formulas
Hydrolysed formulas usually don’t contain lactose e.g. Nutramigen, Neocate etc...
‘Enfamil-O-lac’ or ‘SMA LF’– tastes better as it is not hydrolysed, just lactose free
If >1y - Soya as lactose free. Should not advise the pre-made soya milks under
the age of 2years old as they have the same calorie content as semi skimmed milk.
Can be used over 2y if the child's diet is nutritionally adequate, ensure that the ones fortified with Ca are purchased.
Note: these feeds will have extra Ca as lactose aids the absorption of Ca.

Express delivery! What about the little ones?
Pre-term or low birth-weight formulas
Very difficult to meet the energy and protein requirements in premature babies especially if they have restricted fluids due to reflux or CLD Can need volumes up to 200ml/kg/day
Term baby needs 150ml/kg/day Adult needs 30-35ml/kg/day
They can be given SMA High Energy or Infatrini if their needs require
A combination of EBM and formula may be used to help meet their requirements
Breast milk fortifier – increases the level of protein, energy, Ca, P, vitamins and minerals
Pre-term or low birth-weight formulas- Assists with catch-up growth
Nutriprem 1: 150 – 200ml/kg/day until the infant reaches 1800-
2000g 80Kcal, 2.4g protein per 100ml Higher levels of nearly all vitamin and minerals –
especially Ca, Fe, Phosphate Nutriprem 2:
A post discharge formula or if over 2000g Used until 6 months of corrected age 75Kcal, 2g protein per 100ml Higher levels of nearly all vitamin and minerals –
especially Ca, Fe, Phosphate
Pre-term or low birth-weight formulas- Assists with catch-up growth
Nutriprem breast milk fortifier: A breast milk powder supplement for low birth
weight babies and born before the sucking reflexes have been established (34-36weeks of gestation)
1 sachet (2.1g) to 50ml or 2 to 100ml Extra energy, protein, CHO, vitamins &
minerals EBM ~ 66-70KCal and 1.8g protein Fortified EBM ~ 86Kcal and 2.6g protein
Not ACBS but may be provided from a Neonatal Unit
Pre-term formulas – when to prescribe
Not to term babies that are low birth weight (these need a term formula ? High energy formula)
Prescribable until 6 months of corrected age (not actual) – unless otherwise directed by a Dietitian. If still concerned re: growth/weight then
can change to a high calorie infant formula and refer to Dietetics
‘Crying over spilt milk’, anti-reflux formulas Enfamil AR and SMA Staydown
Designed to thicken on contact with stomach acid and therefore prevent regurgitation.
Should not be used with Ranitidine as this makes the feed ineffective.
ESPGAN, 1996: recommend the use of this type of formula for the first line treatment of mild reflux.
These formulae can be used in conjunction with other standard treatments for reflux
Enfamil AR is available on prescription These are made up differently, cool boiled water
needs to be left to stand for 1 hr before powder is added – to prevent the milk thickening too early

Weaning
When to wean? Not before 17 weeks No later than 6 months BLISS recommend premature babies be weaned
between 5-7 months actual age not corrected age
In April 2001, the WHO issued recommendations to endorse exclusive breastfeeding until six months of age.
In May 2003, the Department of Health issued guidelines recommending that babies are weaned at 6 months of age.
Weaning cont…
Go by development rather than age: Greater strength and stability of the trunk,
shoulder and neck muscles Independent head control Tongue thrust mechanism Fine motor co-ordination of muscles e.g.
Lips and hands Increased demand for feeds especially at
night
Start teeth cleaning as soon as teeth appear with a smear of toothpaste
twice a day
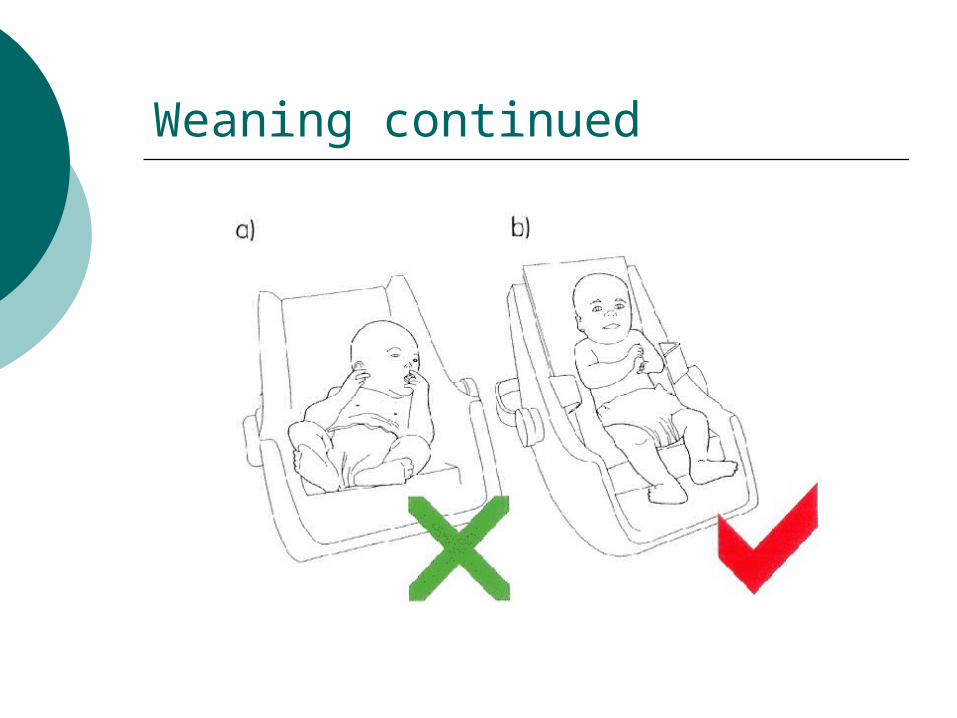
Weaning continued
Weaning cont…Risk of early weaning Kidney immaturity (hypernataemia) Gut immaturity (tolerance problems) Increase risk of infection and disease such as:
Diabetes Obesity Allergy and intolerance Reduced absorption of nutrients in breast milk
Risk of late weaning Poor weight gain Anaemia Food refusal / faddy eating when older Miss developmental cues
Baby led weaning
Gives the control to the infant Claims that giving puree is unnatural and
babies should be weaned onto hand-held solid foods
May reduce ‘fussy eating’ Claims that introducing puree could delay
the development of chewing skills. But if the child is exclusively weaned onto
solids from 6m there may be a limit to the amount of food and therefore nutrients that are swallowed and absorbed as only foods the baby can ‘grasp’ will be offered
Not enough research to date
The Healthy Childs Under 5’s diet the key points
Only offer milk and water as a drink with snacks Offer drinks from a open top cup at 6 months and
the bottle should be gone by 12 months! Sugar free snacks e.g. breadsticks, fresh fruit,
vegetables, cheese etc… Don’t add salt or sugar in cooking or onto foods Vitamin supplements e.g. healthy start vitamins,
Abidec, Dalavit etc… From 6m if breastfed From 1y if on blue top milk Only to stop prescribing when 5y old!
Healthy Under 5’s scheme – in all children’s centres and many nurseries in Luton and Bedfordshire.

Obesity Should measure both Ht
and Wt. Concern when Wt is 2
centiles above Ht Being on the 98thC for Ht
and Wt does not make you obese – just tall and in proportion!
Many South-Asian children will be on or <0.4thC
BMI charts and ranges are different in children a BMI of 15kg/m2 for a 6y old is on 50thC, but 0.4th C for a 16y old
New growth charts are multi-centre, mixed race and show how well children should grow
© 2009 Royal College of Paediatrics and Child Health www.growthcharts.rcpch.ac.uk
Measuring and plotting
What do the Centiles Show?
50th centile: half of all children should be above and half below this line
91st centile: only 9% of children would be expected to be heavier
Childhood obesity referrals
Simple i.e. no co-morbidities or underlying conditions (Diabetes), allergy, behavioural problems etc…
Available schemes – run by active Luton Mini-MEND 2-4y MEDN 5-7y MEND 7-13
Contact Suliman Rafiq. NHS Luton,94 Inkerman Street, Luton, LU1 1JD
Complex obesity who want to make lifestyle changes or those who have attended MEND and need further advice – refer to Dietetics.

Any questions?Any questions?
Paediatric Dietitian, Dietetics Department, Luton & Dunstable Hospital, Lewsey Road, LU4 0DZ
Tel: 01582 49 71 62 Fax: 01582 49 73 61