sani-clothedutracker.com/trktrnr/presentation/alh_athens_al/n9ic14.docx · web viewhepatitis a is...
TRANSCRIPT

Bacterial Survival in the EnvironmentHepatitis B 30 daysInfluenzae 18 hoursRSV 8 hoursRotavirus 10 DaysMRSA Weeks to monthsHIV 1-2 hoursVRE 7 daysClostridium (in spore form) Years
INFECTION PREVENTION AND CONTROL
Standard Precautions Fact Sheet
STANDARD PRECAUTIONS APPLY TO ALL PATIENTS IN ALL CIRCUMSTANCES
I. Barriers – Often called personal protective equipment, or PPE, these include the following:
A. Gloves: Must be worn for all potential hand contact with blood, contaminated equipment, waste or linen.Put on immediately before the task, removed immediately after the task.Never wear the same gloves for more than one patient.PPE should not be worn outside patient rooms. You need to be clean when in the public areas.Remove soiled gloves by rolling the soiled side inward.After removal, hands must be cleaned.
B. Gowns: The type of gown to be chosen is one that will prevent contamination of your clothes or skin
under “normal” conditions.Remove as soon as soiled and before leaving the area.Remove by rolling inward.
C. Masks/Eye Protection: Masks and eye protection (goggles or shields) should be worn together whenever spray or
splatter is possible.Glasses must have solid side panels to be considered protective.
D. Resuscitation Devices: Face masks with filters eliminate the
need for mouth-to-mouth resuscitation and are located near areas for potential use.
II. Work Practices
A. Hand Hygiene
Handwashing is the single most important way to prevent infection and is part of the Standard Precautions used in healthcare settings. Hand washing with soap and water is best performed by applying at least 15 seconds of friction to all surfaces of the hand and wrist. It can reduce the transmission of healthcare-associated infections and stop outbreaks of infectious diseases. Many infections are transmitted on the hands of healthcare personnel. Washing with soap and water or using an alcohol-based hand sanitizer before and after patient care is essential for proper infection control.
So when should you clean your hands:
* Before and after contact with a patient or the patients environment* After removing gloves-Gloves are not substitutes for handwashing and handwashing is not a substitute for gloves.* Before handling medication* After going to the restroom* Before eating* Before and after any procedure is performed* Whenever your hands are visibly dirty or contaminated * Before manipulating an invasive device * After having contact with bodily fluids or excretions, non-intact skin, wound dressings or contaminated items.
If hands are visibly soiled handwashing with soap and water is essential. Also, if you have a patient that has diarrhea or is positive for C diff (Clostridium Difficile) you must wash your hands with soap and water instead of hand sanitizer. Hand sanitizer containing at least 60% alcohol is recommended otherwise. Hand sanitizer is fast acting, causes less skin irritation and is as effective as hand washing except with visible soilage and diarrhea/C diff patients.
Handwashing, whether with soap and water or alcohol sanitizer, is a process of debridement as much as it is an attempt to disinfect the skin surface. For this reason, the hand and wrists should be vigorously scrubbed for a minimum of 15 seconds to ensure adequate debridement of the skin surface. It is best to remove rings and jewelry that may harbor would-be pathogens before handwashing. In fact, not wearing jewelry (rings, etc.) while providing health care to patients would be advisable. Likewise, fingernails should be kept short; ¼ inch from tip of finger. No artificial nails can be worn if you work in a patient care area or handle food!
Something to think about42% of healthcare workers who had NO DIRECT CONTACT with patients, but touched surfaces near MRSA patients, had contaminated gloves!!! They had only touched side rails, linens, and IV pumps.
Reported by John M. Boyce, MD, Professor of Medicine at Yale. Boyce JM et al. Infect. Control Hosp. Epidemiol 1997;18:622

B. Needle Use and Sharps Injury Prevention:
Never recap needles with 2-handed technique. If absolutely necessary to recap, use a one-handed process. Safety needles should always be used if available.
Don’t bend or break needles.
Place used needles in sharps container after use.
Never administer medications from the same syringe to more than one patient, even if the needle is changed or you are injecting through an intervening length of IV tubing.
Do not enter a medication vial, bag, or bottle with a used syringe or needle.
Never use medications packaged as single-dose or single-use for more than one patient. This includes ampoules, bags, and bottles of intravenous solutions. Do not use bags of intravenous solution as a common source of supply for more than one patient.
Always use aseptic technique when preparing and administering injections.
Limit the use of multi-dose vials and dedicate them to a single patient
whenever possible.
Always use facemasks when injecting material or inserting a
catheter into the epidural or subdural space.
One Needle-One Syringe-Only One Time
Example of how bloodborne pathogens can be transmitted with unsafe injection practices.Reference MMR May 16, 2008

C. General:
No eating, drinking, smoking applying of cosmetics or lip balm, or touching contact lenses is allowed in areas where there is risk of exposure to blood/body fluids.
Food and drink must be stored and consumed away from infectious material.
D. Waste and Linen:
Follow the procedures outlined in your work area procedure manual.Do not handle used linens anymore than necessary. Spills of blood or body fluids should be soaked up while wearing gloves, and the clean area sprayed or
wiped with the hospital disinfectant.
III. Post-Exposure Protocol–
If an exposure to blood or body fluids occurs, report the incident immediately to your supervisor following your written policy. If your exposure is with a bloodborne pathogen positive patient you can contract the pathogen yourself. (Hep B 10-30% HIV <0.3% Hep C <10%)
A significant exposure occurs when blood or body fluids with visible blood, or when amniotic, synovial, pericardial, pleural or cerebrospinal fluid enter the body through a break in the skin, a cut or rash, or through a mucous membrane such as the mouth, nose or eye.
Employee ExposedSupervisor is notified and takes charge of the incident.
“Consent Form” is signed by employee and sources.
Supervisor and employee bring signed consent form to Laboratory.
Post Exposure Folder given to Employee/Supervisor.
Tests for HIV, Hepatitis B and C are ordered on Employee and Source.
Blood samples are obtained on employee and source. Test results will be given directly to the Emergency Dept.
Employee and Supervisor will go to the Emergency Department, register and be seen by the charge nurse on duty.
Employee will be treated, risk assessment will be made and prophylaxis provided depending upon recommendations made by the Emergency Department Physician.
Employee will return to work based on treatment by the recommendation of the Emergency Department Physician.
Post-Exposure folder will be completed and forwarded to Employee Health for Follow-Up if required.
Preventing Occupational HIV Transmission to Healthcare Workers
Although not a primary means of HIV transmission, occupational exposure to HIV has resulted in 54 documented cases of HIV seroconversion among healthcare workers (HCW’s) in the United States. To

underscore the importance of preventing occupational HIV transmission to healthcare workers, the Centers for Disease Control and Prevention (CDC) offers the following recommendations in this area.
Preventing Strategies: The primary means of preventing the HCW’s occupational exposure to HIV and the other blood-borne pathogens is to follow infection control precautions with the assumption that the blood and other body fluids from all patient are potentially infectious. These precautions include routinely using barriers (such as gloves and/or goggles) when anticipating contact with blood or body fluids, and carefully handling the disposing of sharp instruments during and after use.
Safety devices also have been developed to help prevent needle-stick injuries. If used properly, these types of devices may reduce the occupational HIV exposure risk. Furthermore, because many percutaneous injuries are related to sharps disposal, strategies for safer disposal, including safer design of disposal containers and placement of containers, are being developed.
Although the more important strategy for reducing the risk of occupational HIV transmission is to prevent occupational exposures, plans for post exposure management of HCW’s are in place. The administration of antiretroviral drugs as post exposure prophylaxis (PEP) should be considered. Using zidovudine as PEP has been shown to be safe and associated with decreased risk for occupationally related HIV infection. Newer antiretrovirals also may be effective, although there is less experience with their use as PEP. CDC recently issued guidelines for a management of HCW exposures to HIV and recommendations for PEP. These guidelines outline a number of considerations in determining whether or not an HCW should receive PEP and in choosing the type of PEP regimen. The recommendations will be updated if ongoing data collection and analysis show increased effectiveness of newer drug treatments. LATEX ALLERGY FACT SHEET
There is no treatment for latex allergy except complete avoidance of latex to prevent reactions and sensitization. Health Care Workers must never wear powdered latex gloves in the vicinity of sensitized patients.
I. Types of latex and other glove associated reactions
Signs and Symptoms include dry, crusty, hand bumps, and sores that may manifest as itchy dermatitis on the back of the hands under the gloves. Horizontal cracks may also form and extend up the forearm. Signs and symptoms may appear several hours after glove contact and may persist many days. Exposure to chemicals used in latex manufacturing is also a potential cause.
Immediate type hypersensitivity include latex allergies and protein allergies and can exhibit a wheal and flare response or itchy redness on the skin under the glove which occurs within minutes and fades away rapidly after removing the glove. The chronic form may mimic irritant and allergic contact dermatitis. Symptoms can include facial swelling, rhinitis, eye symptoms, generalized urticaria, respiratory distress, and asthma. In rare cases, anaphylactic shock may occur. Exposure to proteins in latex on glove surface and/or bound to powder and suspended in the air, settled on objects, or transferred by touch.
II. Strategies to decrease risk of sensitivity:
Use powder free glovesWear synthetic gloves or cotton liners with latex work gloves for wet work.Cleanse hands thoroughly after removing gloves or between glove changes.Use a pH-balanced soap and avoid cutaneous contact with damaging chemicals.Remove gloves at least hourly to air and dry hands.Use only non-oil-based hand care products with gloves while at work.Contact your supervisor immediately if you show any of the above signs and symptoms.
TRANSMISSION BASED PRECAUTIONS FACT SHEET
I. Contact Precautions
Gown if appropriate Gloves and hand hygiene
Used for MRSA, VRE, scabies, rotavirus, RSV and other Multi-drug resistant organisms
Patient Placement – Private room, if possible. Cohort if private room is unavailable.
Gloves – Wear gloves when entering patient room. Change gloves after having contact with infective material that may contain high concentrations of micro-organisms (fecal material and would drainage). Remove gloves before leaving patient room.
Hand Hygiene – After glove removal, cleanse your hands, ensure that hands do not touch potentially contaminated environmental surfaces or items in the patient’s room to avoid transfer of microorganisms to other patients or environments.
Gown – Wear gown when entering patient room if you anticipate that your clothing will have substantial contact with the patient, environmental surfaces, or items in the patient’s room or if the patient has incontinence, diarrhea, an ileostomy, a colostomy, or wound drainage not contained by a dressing. Remove gown before leaving the patient’s environment and ensure that clothing does not contact potentially contaminated environmental surfaces to avoid transfer of microorganisms to other patients or environments.
Patient Transport – Limit transport to essential purposes only. During transport, ensure that precautions are maintained to minimize the risk of transmission of micro-organisms to other patients and contamination of environmental surfaces and equipment. There should always be one clean person transporting the patient who can touch surfaces such as the elevator buttons.
Patient-Care Equipment – Dedicate the use of non-critical patient-care equipment to a single patient. If common equipment is used, clean and disinfect the equipment between patients.

II. Airborne Precautions
N-95 Mask
Used for pulmonary TB (confirmed or suspected), Varicella-Zoster (chickenpox or shingles), smallpox, measles and other organisms that can be transmitted via airborne route.
Patient Placement – Use a private room that has monitored negative air pressure, 6-12 air changes per hour, discharge of air outdoors or HEPA filtration if re-circulated. Keep room door closed and patient in room.
Respiratory Protection – Employees need to wear either a N95 respirator mask or a PAPR unit when entering the patient’s room.
Patient Transport – Limit transport of patient from room to essential purposes only. Use surgical mask on patient during transport. Surgical mask are designed to prevent the respiratory secretions of the person wearing the mask from entering the air.
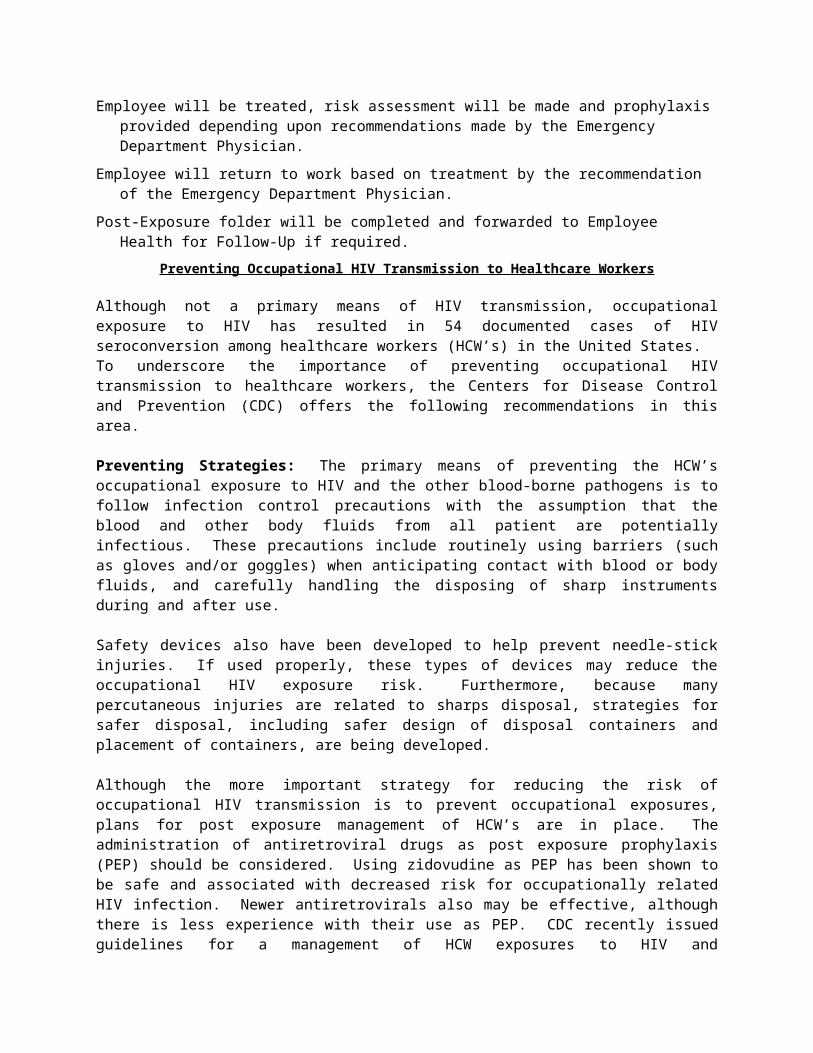
III. Droplet Precautions
Surgical mask If within 3 feet of patient
Used for Influenza, N. meningitides, Pertussis, Parvovirus, Group A streptococcus (strep throat), and RSV. Used for organisms that can be spread by close contact with the patient when they are coughing, sneezing, or talking.
Patient Placement – Private room, if possible. Cohort or maintain spatial separation of three feet from other patients or visitors if private room is not available.
Mask – Wear surgical mask when working within three feet of patient (or upon entering room).
Patient Transport – Limit transport of patient from room to essential purposes only. Use surgical mask on patient during transport.

Gloves - Must be worn if handling respiratory secretions or objects recently contaminated with respiratory secretions.
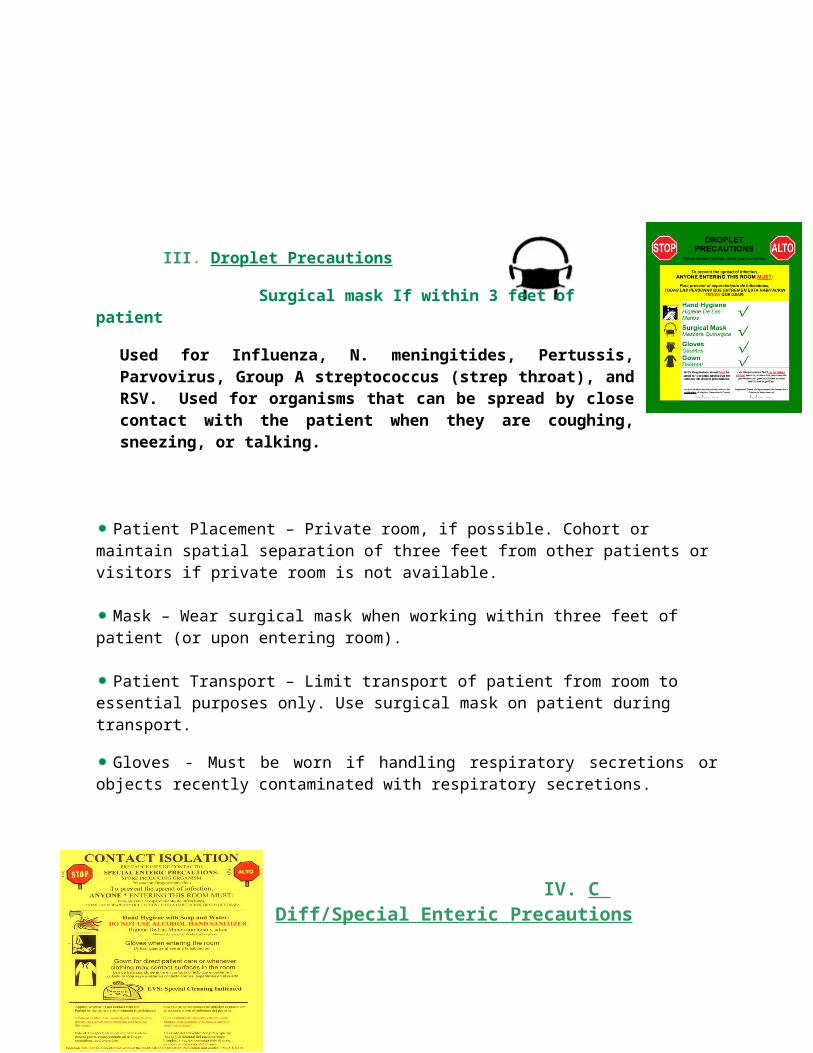
IV. C Diff/Special Enteric Precautions
Gown Gloves Wash with SOAP & WATER
Patient Placement – Private room.
Gloves – Wear gloves when entering patient room. Change
gloves after having contact with infective material that may contain high concentrations of micro-organisms (fecal material and would drainage). Remove gloves before leaving patient room.
Gown – Wear gown when entering patient room if you anticipate that your clothing will have substantial contact with the patient, environmental surfaces, or items in the patient’s room or if the patient has incontinence, diarrhea, an ileostomy, a colostomy, or wound drainage not contained by a dressing. Remove gown before leaving the patient’s environment and ensure that clothing does not contact potentially contaminated environmental surfaces to avoid transfer of microorganisms to other patients or environments.
Hand Hygiene – After glove removal, cleanse your hands with SOAP AND WATER, ensure that hands do not touch potentially contaminated environmental surfaces or items in the patient’s room to avoid transfer of microorganisms to other patients or environments. DO NOT USE ALCOHOL HAND SANITIZER IN A PATIENTS ROOM WHO HAS C. DIFF OR DIARRHEA!! You must clean hands with soap and water to remove potential spores.
Hospital-Approved Agents for Cleaning and Disinfection
pH7Q UltraOne step disinfectant/germicidal/detergent• Primarily used by Environmental Services• Used on floors, glazed porcelain, plastic surfaces, toilet and urinals, and walls• Kills bacteria and viruses• Kills Hepatitis B, Hepatitis C, HIV-1, Rotavirus, MRSA, and VRE. Has a 10 minutes contact time.

Clorox Wipes• Bleach solution equivalent to the 1:10 dilution recommended by the CDCfor healthcare settings.• Used on hard, non porous surfaces and equipment• Kills bacteria, TB, and viruses• Kills C. diff and TB in 3 minutes and Norovirus in one minute.• 30-60 second contact time for most bacteria and viruses.
Used for patient room with C. diff with a 3 minutes contact timeSuper Sani-Cloth Germicidal Disposable Wipes
• A Quaternary disinfectant with high alcohol content (55%)• Used on hard, non porous surfaces and equipment• Kills bacteria, TB, and viruses• Kills TB and RSV in 1 minute• Kills Hepatitis B, Hepatitis C, Human Coronavirus, Rotavirus, MRSA, VRE, and ESBL Producing E. coli in 2 minutes• Has been tested effective against 22 microorganismsUSE 2 minute contact time. DOES NOT KILL C DIFF SPORES
Sani-Cloth ® HB Germicidal Disposable Wipes A quaternary alcohol free formula used by Radiology for the disinfection of
equipment. Kills bacteria, fungus and viruses Kills HBV, Influenza A-2 virus, Acinetobacter and Aspergillus niger plus over 100 other
microorganisms with a 10 minute contact time.________________________________________________________________________ CONTACT OR WET TIME for each disinfectant is the minimum length of time that the surface must remain wet to destroy the microorganisms. The surface may have to be wiped or sprayed more than one time for the surface to remain wet for the required contact time.
Patient Transport Generally speaking, healthcare workers should not wear isolation attire to transport a patient. Using appropriate barriers on the patient is sufficient to protect the healthcare worker. For those instances when direct patient contact is needed during the transport (example: bagging
patient on ventilator, emergency transport performing CPR, etc.) or when using barriers on the patient is not appropriate, then two or more healthcare workers are required to perform the transport.
One healthcare worker remains “clean” and walks ahead to push elevator buttons and open doors etc. While the other healthcare worker(s) are garbed appropriately (according to type of precautions) and helps push the bed and perform the necessary patient contact activities.
INFLUENZA (FLU) INFORMATIONKinds of Flu:
Seasonal (or common) flu is a respiratory illness that can be passed from person to person. The flu is a contagious respiratory illness caused by influenza viruses. It can cause mild to severe illness, and at times can lead to death. The best way to prevent this illness is by getting a flu vaccination each year. The symptoms include fever, body aches, and cough.
Every year in the United States, on average 5-20% of the population gets the flu and more that 200,000 people are hospitalized from flu complications. Approximately 36,000 people die from flu every year.
The elderly and young children as well as people with certain health conditions, such as cardiac or lung diseases or cancer, are at high risk for serious flu complication or death. Flu viruses spread in respiratory droplets caused by coughing and sneezing. Though usually spread person to person, sometimes people become infected by touching something with flu viruses on it and then touching their mouth or nose. Most healthy adults may be able to infect others beginning 1 day before symptoms develop and up to 5 days after becoming sick. That means that you can pass on the flu to someone else before you know you are sick, as well as while you are sick.
Avian (or bird) flu is caused by flu viruses that occur among wild birds. The H5N1 variant is deadly to birds and can be passed from birds to humans. It is not known if this is passed from person to person. There is no human immunity and no vaccine is available.
The risk from avian flu is low to most people, because the viruses do not usually infect people. Most cases of avian flu infection in humans come from contact with infected poultry (e.g. domesticated chickens, ducks, and turkeys). Symptoms of avian influenza in humans have ranged from typical human influenza-like symptoms (e.g. fever, cough, sour throat and body aches) to eye infections, pneumonia, severe respiratory diseases (such as acute respiratory disease), and other severe and life-threatening complications.
Pandemic flu is a strong human flu virus that causes a worldwide outbreak (called pandemic) of a serious illness. Because there is little human immunity, the disease can spread easily from person to person.
A pandemic is an international disease outbreak. A flu pandemic occurs when a new flu virus comes around and people have little or no immunity, and there is no vaccine. Pandemic flu virus spreads easily person to person, causes serious illness even death, and can sweep across the country and around the world in very short time. No one knows when or if the next flu pandemic will occur or how bad it will be. It is thought that a flu pandemic could lead not only to a great deal of illness and death but also social disruption (closing schools and churches) and economic loss.
When to get vaccinated
The CDC recommends that we start getting vaccinated once the flu vaccine is available. People can get sick with flu as early as September and as late as May. Healthcare workers, as a group, have a low vaccination rate but can get exposed to flu on a regular basis and can bring home the illness to love ones.
For the flu vaccine to work to protect a person from flu depends on the age and health of the person getting the vaccine and if the vaccine matches the flu in circulation. Testing has shown that both the flu shot and the nasal-spray vaccine are about 80% effective at preventing the flu. Those who do get the
vaccine and then go on to get the flu, tend not to be as sick as those who did not receive the vaccine and they recover at a quicker rate.
Who should NOT be Vaccinated
Some people should not be vaccinated without first consulting a physician. These include:
• People who have a severe allergy (anaphylaxis) to eggs although now there is Flubok vaccine
• People who have had a severe reaction to an influenza vaccination in the past
• People who developed Guillain-Barre´ syndrome within 6 weeks of getting an influenza vaccine previously
• Influenza vaccine is not approved for use in children less than 6 months of age (That is why it is important for Mom to be vaccinated during pregnancy)
• People who have a moderate or severe illness with a fever should wait to be vaccinated until their symptoms lessen.
Vaccine Side Effects (What to Expect)
The flu shot: The viruses in the flu shot are killed (inactivated), so you cannot get the flu from a flu shot. Some minor side effects that could occur are soreness, redness, or swelling where the shot was given, fever (low grade) and body aches. If these problems occur, they begin soon after the shot and usually last 1-2 days. Almost all people who receive influenza vaccine have no serious problems from it. YOU DO NOT GET THE FLU FROM THE VACCINE.
HEALTHCARE WORKERS:
All health-care workers should be vaccinated against influenza every year. This will protect co-workers, patients, family members, and the community. There is a trend for some states to require flu vaccination of HCW. While this in not currently true in Alabama, vaccination is strongly recommended. The flu vaccine is provided free to all employees.
Precautions
Droplet Isolation should be used with any patient with suspected or confirmed influenza for 5 days after the onset of illness or for the duration of illness for immunocompromised patients. During the care of any patient with symptoms of a respiratory infection, HCW should:
• Wear a surgical or procedure mask when entering the patient’s room or when working within 6 feet of the patient. Remove the mask when leaving the patient’s room and dispose of the mask. If patient movement or transport is necessary, have the patient wear a surgical mask.
• Wear gloves if hand contact with respiratory secretions or potentially contaminated surfaces is anticipated.
• Wear a gown if soiling of clothes with a patient’ respiratory secretions is anticipated.
• Change gloves and gowns after each patient encounter and perform hand hygiene.

FLU PREVENTION
• Get a flu vaccine!!!!! • Stay home when you are ill. • Cover your mouth and nose with tissue when coughing or sneezing. • CLEAN YOUR HANDS BEFORE AND AFTER PATIENT CARE • Avoid touching your eyes, nose or mouth.
Title: Employee Influenza Plan Developed by: Flu Committee Developed: July 1, 2014 M. Estremera, A. Sowell, S. Weaver, S. Ritter,
D. Pryor
2014 Employee Influenza Vaccination Plan
I. Actions Enhancing Vaccination Rates A. Early staff education
1. August 1, 2014 initiate employee education a. Place in Huddle b. Discuss in Department Head meeting c. Send global time clock message d. Attach to payroll
2. Post 2014 Flu Plan B. Rolling carts with flexible hours C. FluMist™ availability D. Flublok™ availability for latex and egg protein allergies E. Place Flu Sticker 2014 on badge for those receiving vaccine F. Set date for employee compliance/completion of plan
1. Compliance/Completion—November 5, 2014 II. Actions Addressing Vaccine Declination
A. Signing of declination required 1. Must come to Education or Employee Health to sign
B. Required to wear a mask when within 6 feet of a patient C. Letter from physician validating medical reason D. Letter from clergy validating religious reason E. “Flu Camp” attendance for all declining vaccine
1. view video on influenza 2. interview with employee health CRNP
III. Reprimand for Employee Noncompliance A. Those employees with a validated medical reason or a validated religious reason
not to get the flu vaccine will still be required to wear a mask when within 6 feet of a patient. Failure to do so will result in disciplinary action for failure to follow their supervisor’s instructions. First time—warning, Second time—disciplinary action up to and including termination.
B. Noncompliance with the program by November 5th will result in a written warning and suspension without pay. Failure to not become compliant by November 12th will result in further disciplinary action up to and including termination.
IV. Incremental Influenza Vaccination Goals A. 2014: Minimum 90% with stretch 96% or higher B. Maintain 90% or higher—2018-2020
HEPATITIS FACT SHEET
Viral Hepatitis is one of the most common infectious diseases in the world. There are at least five hepatitis viruses; all of them affect the liver in one way or another.
I. Hepatitis A (HAV) – This is the most common infection. But it’s also the least serious. Most infected people recover completely within a month and have no permanent damage. Once you have it, you can never get sick from it again because your body develops immunity. Hepatitis A is spread through contaminated food or water. Hepatitis A vaccines are usually given to people traveling to countries where there have been outbreaks.
II. Hepatitis B (HBV) – Hepatitis B is the next most common. It can be either acute or chronic. In enters the body through infected body fluids, such as blood and semen. It can be transmitted sexually and from infected needles (drugs, tattooing, acupuncture, etc.) Infected mothers can pass it on to their newborns during birth.
Hepatitis B vaccines are recommended for healthcare workers performing tasks associated with high risk of exposure. The Hepatitis B vaccine is increasingly being recommended as a routine childhood vaccination. The vaccination process consists of three injections: the first two are one month apart, and the last one is six months from the first injection. The duration of the protective effect from Hepatitis B vaccine is not known, but booster doses are not shown to be necessary. Efficacy is 90-95% when administered as recommended. A follow-up blood test confirms immunity. With an exposure to Hepatitis B you have a 10-30% chance of contracting the disease if you are not protected.
According to the literature, the most common side effect of the vaccine is a sore arm, although the possibility of nausea, vomiting, low-grade fever, and headache exists. Joint pain has been reported; rash has been reported rarely. Studies have shown no apparent adverse effects to developing fetuses when pregnant women have received the vaccine.
III. Hepatitis C (HCV) – It used to be transmitted primarily through blood transfusions, but since 1992 blood supplies are routinely screened for the virus and the incidence has been greatly reduced. It’s mainly spread through unprotected sex and infected needles. Hepatitis C is the most likely of the viruses to cause chronic illness. It progresses slowly, usually over a course of 10 to 30 years.
IV. Hepatitis D (HDV) – Hepatitis D is only seen in conjunction with Hepatitis B.
V. Hepatitis E – This is very rarely seen in the United States.
VI. Symptoms of Hepatitis – Many people with hepatitis will feel only mildly ill, if at all. Common symptoms include:
Fever, Headache, Malaise (ill feeling), Diarrhea, Nausea and vomiting, Anorexia, Abdominal pain, Jaundice (yellow skin and eyes) and Fatigue.
There is no specific treatment once Hepatitis occurs.

AIDS FACT SHEETI. Overview –In 2009, the World Health Organization (WHO) estimated that there were 33.4 million people worldwide living with HIV/AIDS, with 2.7 million new HIV infections per year and 2.0 million annual deaths due to AIDS.
When the human immunodeficiency virus (HIV) enters your body, it weakens the natural defenses and makes you vulnerable to a number of potentially fatal diseases and infections called AIDS. Currently, there is no cure for HIV disease.
AIDS is a hard disease to get; it’s not spread by casual contact. You can prevent getting HIV by using a latex condom during intercourse – or abstaining from sex – by not sharing needles and using standard precautions when appropriate in your work activities.
The HIV virus is not in itself deadly. The problem comes when the virus weakens and eventually depletes the immune system, allowing infections to take hold. It attaches itself to and destroys white blood cells also known as helper T cells, essential components of the immune system. As the virus depletes the T cells, you body becomes increasingly susceptible to an array of other infections and diseases.
There is good news in the form of protease inhibitors, a new class of drugs. Protease inhibitors helped cut the number of U.S. AIDS deaths by almost half from 1996 to 1997. As a result, AIDS dropped from the eighth leading cause of death in the United States to the 14th.
II. Disease Association – HIV can lie dormant for years. Although HIV infection and its progression to AIDS is generally a slow process, HIV can develop at an extremely variable rate; it can take less than five years, or as long as 15 years, to progress to AIDS. Some of the more common AIDS-defining illnesses include:
Pneumoncystis carinii pneumonia (PCP)Esophagitis, inflammation of the esophagusCryptosporidiosis infection of the intestine for more than four weeksPrimary lymphoma of the brainKaposi’s sarcomaHerpes simplex ulcers
III. Symptoms – Initial symptoms are similar to the flu and can last three to 14 days:Fever ChillsChills General discomfortNight Sweats MalaiseSkin Rash HeadacheSwollen lymph nodes (immune system organs easily felt in the neck and groin)
Within the several months following HIV infection, you may have repeated episodes of these flu-like symptoms. After that, an average period of five to seven years will pass without another sign of HIV infection – though that delay can range from a few months to more than 10 years. However, even when you don’t have symptoms, the virus is still multiplying in your body, and your can spread it to other people.
IV. Later Symptoms (months to years before onset of AIDS. Symptoms may include:
Fatigue Persistent yeast infections
Mild weight loss Persistent skin rashesFrequent fevers or sweats Swollen lymph glands
Short term memory lose Painful nerve disease (shingles)Pelvic inflammatory disease that does not respond to treatmentFrequent and severe herpes infections causing mouth, genital or anal sores
V. Chronic HIV – The immune system grows weaker and weaker until it can no longer prevent diseases and/or “opportunistic” infections (those that would not usually happen in a person with a normal immune system).
These include: Pneumonia caused by Pneumoncystis LymphomaHIV infection of the brain Herpes Simplex virusCryptococcus infection Kaposi’s sarcomaHIV wasting syndrome Tuberculosis
HIV Testing – An HIV test looks for antibodies your immune system creates in response to the virus. These antibodies may not appear in your blood until three to six months after HIV infection. Therefore, a negative test for HIV does not necessarily mean you aren’t infected.
The key to preventing the spread of HIV is dependent upon each of us protecting ourselves with careful personal and professional practices.
TURBERCULOSIS FACT SHEET
Overview – Tuberculosis (TB) is caused by an organism called Mycobacterium tuberculosis or tubercle bacillus. TB is spread from person to person through the air.
When a person with infectious TB coughs or sneezes, tiny droplets containing tubercle bacilli are expelled into the air. These droplets, called droplet nuclei, can remain suspended in the air for several hours. If another person inhales air that contains these droplet nuclei, they may become infected with tuberculosis. Once inhaled, most of the larger droplets become lodged in the nose and throat, where infection is unlikely to develop. However, the droplet nuclei may reach the small air sacs of the lung where infection begins. At first, the tubercle bacilli multiply in the lungs. A small number can enter the bloodstream and spread throughout the body. Within 2 to 10 weeks, the body’s immune system usually responds by producing special immune cells that surround the tubercle bacilli, forming a protective shell. This stops multiplication and prevents further spread. It’s important to note the difference between Tb infection and disease. TB infection means that the tubercle bacilli are in the body, but the body’s immune system is keeping them under control. People with TB infection without disease, are not infectious. That means they cannot spread their infection to other people. Some people with infection do go on to develop disease. TB disease develops when the immune system cannot keep the tubercle bacilli under control. The bacilli begin to multiply rapidly in the lungs and cause damage to tissue and create the

symptoms of tuberculosis. About 85% of tuberculosis cases are pulmonary TB – TB that occurs in the lungs. Extra pulmonary TB occurs in places other than the lungs, such as the larynx, the lymph nodes, the brain, the kidneys, or the bones and joints. In the United States, about 10% of people infected with TB will go on to develop disease. But for those with specific risk factors, that percentage is much higher. HIV infection is the strongest risk factor for the development of TB disease.
Contributing Factors – Other conditions that appear to increase the likelihood of developing TB disease once infected include:
Illegal drug useDiabetesLong-term steroid therapyChemotherapyCertain types of cancer such as leukemia and Hodgkin’s diseaseSevere kidney diseaseInfection with tuberculosis within the past 2 yearsBecause the risk of developing TB disease is highest in the first two years after infection, it is
important to detect new infections early. People with TB infection can be given medications to prevent the infection from progressing to TB disease.
III. Controls – Our infection control program involves three types of controls:
Administrative ControlsEngineering ControlsPersonal Respiratory ProtectionThe intent of these controls is to detect the disease early and to promptly isolate and treat
people who have TB disease.
IV. Symptoms & Indications – TB disease should be suspected in patients who have any of the following symptoms:
A persistent cough FatigueBlood/sputum Fever
Night sweats Weight loss or loss of appetite
V. Management – Patients who have signs and symptoms of TB disease should be placed away from other patients. They should be given a mask and instructed to keep it on until they can be
evaluated. The patient should be given tissue and encouraged to cover their mouth and nose when coughing or sneezing.
The infectiousness of a TB patient is directly related to the number to tubercle bacilli that are expelled into the air. This number of organisms will depend on the location of the disease, whether or not the patient is coughing and the results of the chest x-ray and sputum smear.
Decisions will be made on isolation and isolation duration (whether or not to isolate a patient or how long to leave them in isolation) based on the infectiousness of the individual patient.
Screening healthcare workers for TB infection is also an important part of each hospital’s TB plan. Administering a simple skin test does screening. This test is given by injecting a small

amount of a substance called tuberculin between the layers of the skin on the forearm. The site is examined 48-72 hours after the tubculin is injected. Anyone found to have a positive reaction should be evaluated for the presence of TB disease and the need for preventive therapy. Most
people who have a positive reaction will continue to have a positive reaction if tested late in their lives, regardless of whether they receive treatment.
As a healthcare provider, you will be required to wear special respiratory protection if you are at risk of exposure. Your supervisor will assure you receive instruction on how and when to use
respiratory protection.


Handwashing is the single most effectivedeterrent to the spread of infection.
I. Policy: When hands are visibly dirty or contaminated with proteinaceous material or are visibly soiled with blood or
other body fluids, wash hands with either a non-antimicrobial soap and water or an antimicrobial soap and water.
If hands are not visibly soiled, use an alcohol-based hand rub for routinely decontaminating hands in all other clinical situations.
Decontaminate hands before having direct contact with patients.Decontaminate hands before donning sterile gloves when inserting a central intra-vascular catheter.Decontaminate hands before inserting indwelling urinary catheters, peripheral vascular catheters, or other
invasive devices that do not require a surgical procedure.Decontaminate hands after contact with a patient’s intact skin; e.g. when taking a pulse or blood pressure, and
lifting a patient.Decontaminate hands after contact with body fluids or excretions, mucous membranes, non-intact skin, and
wound dressings if hands are not visibly soiled.Decontaminate hands if moving from a contaminated body site to a clean body site during patient care.Decontaminate hands after contact with inanimate objects (including medical equipment in the immediate
vicinity of the patient).Decontaminate hands after removing gloves.Before eating and after using a restroom, wash hands with a non-antimicrobial soap and water or with an
antimicrobial soap and water.Antimicrobial-impregnated wipes (towelettes) may be considered an alternative to washing hands with non-
antimicrobial soap and water. Because they are not as effective as alcohol based hand rubs or washing hands with an antimicrobial soap and water for reducing bacterial counts on the hands of health care workers, they are not a substitute for using an alcohol based hand rub or antimicrobial soap.
Wash hands with non-antimicrobial soap and water or with antimicrobial soap and water if exposure to Bacillus anthracis or Clostridium difficile is suspected or proven.
II. Procedure for Routine Hand HygieneWhen decontaminating hands with an alcohol-based hand rub, apply product to palm of one hand and rub hands
together, covering all surfaces of hands and fingers, until hands are dry. Follow the manufacturers recommendations regarding the volume of product to use.
When washing hands with soap and water, wet hands first with water, apply an amount of product recommended by the manufacturer to hands, and rub hands together vigorously for at least 15 seconds, covering all surfaces of the hands and fingers. Rinse hands with water and dry thoroughly with a disposable towel. Use a clean towel to turn off the faucet. Avoid using hot water, because repeated exposure to hot water may increase the risk of dermatitis.
Liquid, bar, leaflet or powdered forms of plain soap are acceptable when washing hands with a non-antimicrobial soap and water. When bar soap is used, soap racks that facilitate drainage and small bars of soap should be used.
III. Procedure for Surgical Hand Antisepsis Remove rings, watches, and bracelets before beginning the surgical hand scrub.
Remove debris from underneath fingernails using a nail cleaner under running water. Perform surgical hand antisepsis using either an antimicrobial soap or an alcohol based hand rub with persistent activity is recommended before donning sterile gloves.

When performing surgical hand antisepsis using an antimicrobial soap, scrub hands and forearms for the length of time recommended by the manufac turer, usually 2 to 6 minutes. When using an alcohol based surgical hand scrub product with persistent activity, follow the manufacturer’s instructions. Before applying the alcohol solution, prewash hands and forearms with a non-antimicrobial soap and dry hands and forearms completely. After application of the alcohol-based product, allow hands and forearms to dry thoroughly before donning sterile gloves.
___________________________________ ____________________
Print Employee Name Date
_________________________________________ ___________________________