safety, tolerability and early bactericidal activity in sputum of pnu-100480 (sutezolid) in patients...
TRANSCRIPT

Safety, tolerability and early bactericidal activity in sputum of PNU-100480 (sutezolid) in patients with pulmonary tuberculosis
RS Wallis1, AH Diacon2, R Dawson3, A Venter2, SO Friedrich2, D Paige1, T Zhu1, A Silvia1, J Gobey1, C Ellery1, Y Zhang1, E Kadyszewski1
1Pfizer, USA; 2Stellenbosch University and 3University of Cape Town, South Africa

PNU-100480 (sutezolid)
• Oxazolidinone antimicrobial– Sulfur-containing linezolid analog with an active sulfoxide metabolite– Bind 23S RNA and inhibit microbial protein synthesis– No cross resistance, neither inhibits nor induces CYP3A4
• Preclinical findings– Superior bactericidal activity vs. linezolid in mouse and whole blood TB models
regardless of LZD dose or concentration– Earlier sterilization (1-2 months) when combined with standard TB drugs
• Phase 1 findings– Doses to 600 mg BID generally safe and reasonably well tolerated to 28d– No significant safety signals, incl. hematology, biochemistry, QT
• Potentially can address 4 major unmet medical needs in TB– DR, HIV, DS, suspected DR-LTBI
• The present phase 2a study is its first in TB patients

3
Study inclusion criteria
• Men and women aged 18-65 years• Pulmonary tuberculosis
– CXR consistent with pulmonary tuberculosis– Positive sputum acid-fast smears– Culture or molecular confirmation of drug-susceptible Mtb
• Either HIV-1 uninfected, or HIV-1 infected with CD4 T cell counts >350/mm3 and not currently receiving ART
• Reasonably normal renal, hepatic, metabolic function• Willing to provide written informed consent according to ICH
guidelines

4
Study exclusion criteria
• Significant hemoptysis • TB treatment within the preceding 6 months
– Or positive test for urinary isoniazid metabolite at the time of screening
• Treatment with MAO inhibitors, tricyclic antidepressants, or adrenergic agonists such as pseudoephedrine or phenylpropanolamine within the preceding 7 days– Due to potential MAO-B activity

5
Randomization and treatment
• Subjects were recruited at 2 sites in South Africa, and were randomly assigned in blocks of 7 to:– PNU-100480 600 mg BID– PNU-100480 1200 mg QD– Fixed dose combination tablets consisting of isoniazid, rifampin,
ethambutol, and pyrazinamide (Rifafour© e275)
• Neither subjects nor investigators were blinded to assigned treatment
• Treatment duration was 14 days– After which all patients commenced standard TB treatment– Final safety evaluation was on day 42

Subject characteristics
Treatment arm600 mg BID 1200 mg QD HREZ
Number of subjects 25 25 9Age (years, mean±SD) 32.3±9.0 34.1±11.7 33.8±11.8Sex (male/female) 20/5 20/5 7/3Race (Black/other) 11/14 8/17 3/6Weight (kg, mean±SD) 54.6±6.5 51.1±6.7 51.3±7.5Height (cm, mean±SD) 167.4±8.2 167.0±6.1 166.5±11.8BMI (kg/m2, mean±SD) 19.6±2.9 18.3±1.8 18.4±0.5Baseline log CFU/ml (mean±SD) 6.88±1.11 6.91±1.20 7.22±0.71

7
Safety and tolerability
600 mg BID
1200 mg QD HREZ
Subjects evaluable for adverse events 25 25 9Number of adverse events 23 (44%) 17 (33%) 12 (23%)Subjects with adverse events 15 (60%) 12 (48%) 5 (56%)Subjects with serious or severe adverse events 1 0 0Subjects discontinued due to adverse events 0 0 0Subjects with dose reduced or temporary discontinuation due to adverse events 0 0 0
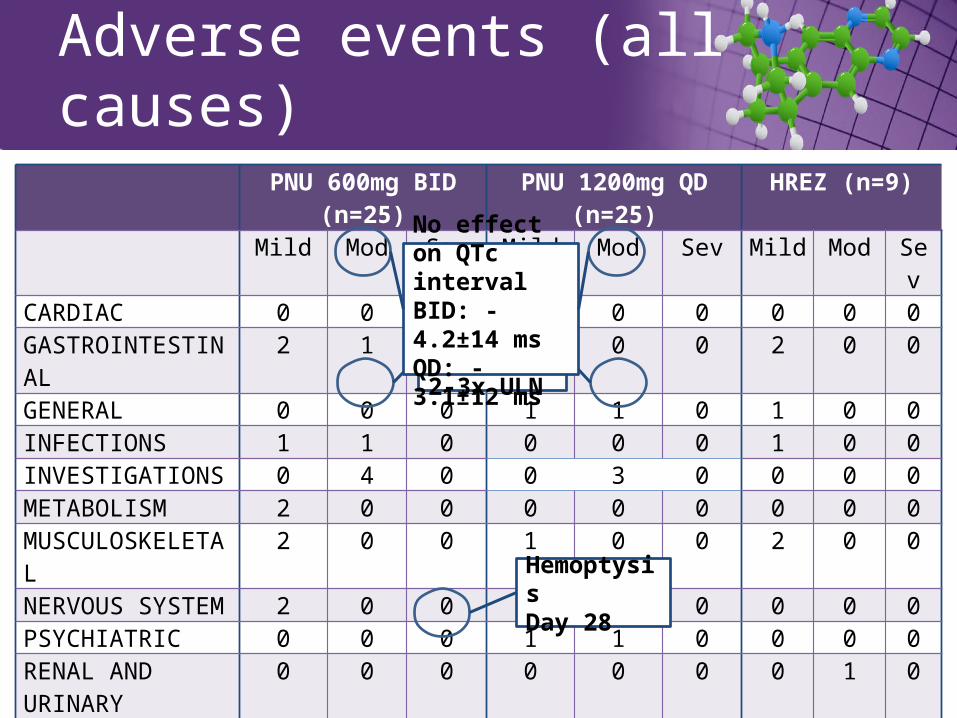
Adverse events (all causes)
PNU 600mg BID (n=25) PNU 1200mg QD (n=25) HREZ (n=9)
Mild Mod Sev Mild Mod Sev Mild Mod SevCARDIAC 0 0 0 1 0 0 0 0 0GASTROINTESTINAL 2 1 0 0 0 0 2 0 0GENERAL 0 0 0 1 1 0 1 0 0INFECTIONS 1 1 0 0 0 0 1 0 0INVESTIGATIONS 0 4 0 0 3 0 0 0 0METABOLISM 2 0 0 0 0 0 0 0 0MUSCULOSKELETAL 2 0 0 1 0 0 2 0 0NERVOUS SYSTEM 2 0 0 2 0 0 0 0 0PSYCHIATRIC 0 0 0 1 1 0 0 0 0RENAL AND URINARY 0 0 0 0 0 0 0 1 0REPRODUCTIVE 0 0 0 0 0 0 1 1 0RESPIRATORY 0 0 1 1 1 0 1 0 0SKIN 6 2 0 2 1 0 1 0 0TOTAL 15 8 1 11 7 0 10 2 0
HemoptysisDay 28
ALT increase2-3x ULN
No effect on QTc intervalBID: -4.2±14 msQD: -3.1±12 ms

day
0 2 4 6 8 10 12 14
log C
FU
-3
-2
-1
0
1200 QD
HREZ 600 BID
Early Bactericidal Activity
Shading indicates 90% confidence interval by mixed effects model repeated measures analysis
• Both PNU dosing schedules resulted in significant log CFU reductions from baseline over the 14 day period of treatment.
– 600 mg BID: -0.09 log/d, 90% CI -0.06 to -0.11
– 1200 mg QD: -0.07 log/d, 90% CI -0.04 to -0.09
• A trend was apparent toward superior responses with BID dosing
10
day
0 7 14 21 28 35 42
AL
T (
U/l)
0
50
100
150
200
250
300
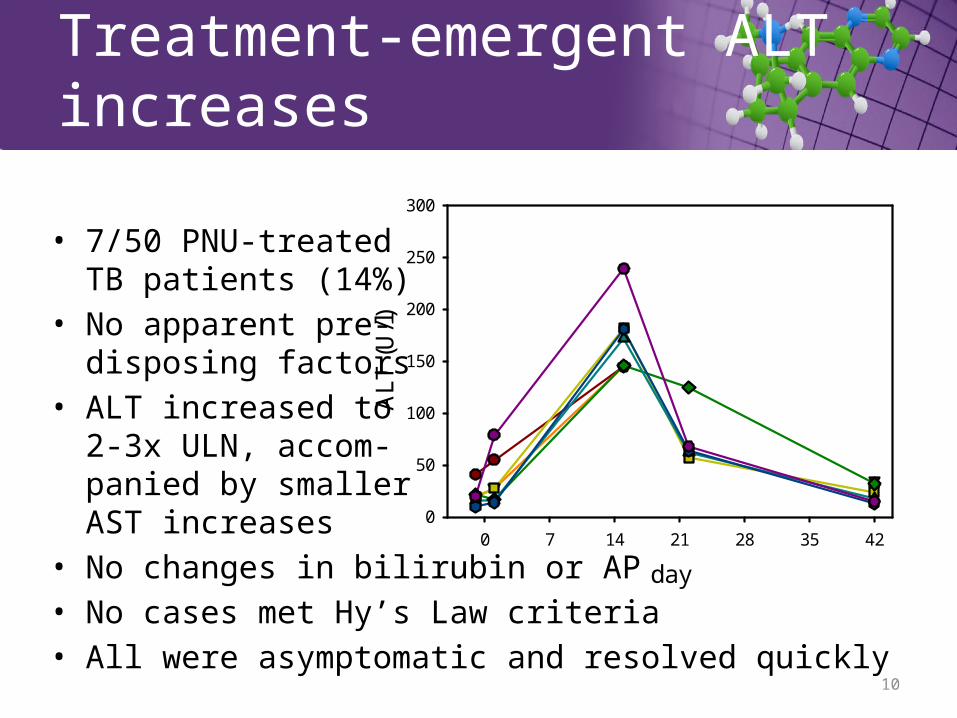
Treatment-emergent ALT increases
• 7/50 PNU-treated TB patients (14%)
• No apparent pre-disposing factors
• ALT increased to 2-3x ULN, accom-panied by smaller AST increases
• No changes in bilirubin or AP• No cases met Hy’s Law criteria• All were asymptomatic and resolved quickly

11
Glutathione (GSH) depletion hypothesis
• Drug-induced liver injury is common in TB (10-20%)– HRZ all are implicated
• GSH, which ordinarily protects against oxidative injury, is decreased in TB– GSH is decreased in TB animal models and in TB patients
– Palanisamy, PLoS ONE 2011, and Venketaraman, Microb Path 2008– Apparently is consumed to protect host cells from the cellular antimicrobial host
response (peroxides, superoxides, NO)
– Lowest levels are in TB patients with drug-induced liver injury– Chowdhury, Indian J Gastro 2001
• Liver injury due to HRZ can be prevented by supplementationwith N-acetylcysteine (NAC)
– (Baniasadi, Eur J Gastro Hepatol 2010)

Summary
• Treatment with PNU-100480 at doses of 600 mg twice daily or 1200 mg once daily for 14 days resulted in significant reductions in sputum bacillary burden– A trend toward superior bactericidal effect was apparent when given
twice daily
• Both dosing schedules were generally safe and relatively well tolerated
• New TB regimens containing PNU-100480 can potentially address major unmet medical needs in TB treatment

Contact:[email protected]

Questions?
• LZD• NAC• MPS• Parent – metabolite• Proposed clinical plan


EBA comparison with linezolid
Drug Dose and duration*
mean log/d(90% CI)
Study
Linezolid 600 mg BID and QDdays 0-7
-0.082(-0.054 to -0.110)
Dietze, AJRCCM 2008
Sutezolid 600 mg BIDdays 0-6
-0.146 ( 0.102 to -0.191)‑
(current study)
* Both LZD doses appeared equivalent, and here are combined to increase precision. LZD data indicate effects over the entire treatment period (7 days). Sutezolid data were limited to days 0-6 for comparison, as log CFU data were not collected on day 7. Caution is warranted when comparing with historical data.

Human Pulmonary TuberculosisExtracellular infection
• Cavities contain large numbers of log phase bacilli that can give rise to resistance
• Inadequate treatment results in failure
• Eradication is termed bactericidal activity
Intracellular infection
• Granulomas contain small numbers of semi-dormant bacilli that can give rise to persistence
• Inadequate treatment results in relapse
• Eradication is termed sterilizing activity

Plasma concentration/MPS IC50
1200 mg QD600 mg BID300 mg BID100 mg BID
600 mg BID300 mg QD
Hours
0 6 12 18 24
Fol
d M
PS
IC
50
0
1
2
3
4
5
Hours
0 6 12 18 24
Fol
d M
PS
IC
50
0
1
2
3
4
5
PNU-100480 Linezolid
Wallis, AAC 2011

Concentration (g/ml)
0 1 2 3
log
/d
-0.6
-0.4
-0.2
0.0
0.2
0.4LZDPNU
Intracellular bactericidal activityex vivo whole blood culture

Linezolid, sutezolid & metabolites
MIC (mg/ml)
MPS IC50 (mg/ml)
Plasma conc vs. parent
Critical activity
Linezolid 0.5 5.5 -Sutezolid 0.25 15.5 -PNU-101603 0.5 4.4 5XPNU-101244 0.5 5 0.1X
LinezolidSutezolidPNU-101603PNU-101244
MIC (mg/ml)
MPS IC50 (mg/ml)
Plasma conc vs. parent
Critical activity
Linezolid 0.5 5.5 -Sutezolid 0.25 15.5 - IntracellularPNU-101603 0.5 4.4 5X ExtracellularPNU-101244 0.5 5 0.1X -

2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4
rela
pse
rate
(lo
g ra
tio)
-3
-2
-1
0
1
2
3
LocationAfrica Hong
KongSinga-pore
IndiaTreatmentmodification
T added
Z addedR added
S added
IP shortened3x/wk2x/wk
E->Z
S removed, IP lengthened
Intensive phase shortened
2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4
rela
pse
rate
(lo
g ra
tio)
-3
-2
-1
0
1
2
3
Intermittent treatment
2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4-3
-2
-1
0
1
2
3
Streptomycin added
2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4-3
-2
-1
0
1
2
3
Pyrazinamide added
2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4-3
-2
-1
0
1
2
3
Rifampin added
2-month conversion rate (log ratio)
-0.2 0.0 0.2 0.4-3
-2
-1
0
1
2
3
A
B C D E F
2-mo culture statushighly related to relapse-free cure
Wallis, Lancet ID 2010

Sutezolid Clinical Plan
Adaptive licensing / Accelerated approval
Confirmatory trial:
Novel DR regimenNovel DS regimen (UJRbZ)
vs. SOC
Selection of regimens & durations
Ph1 EBA*
Compound 1
Ph1 EBA*
Compound 2
Ph1 EBA*
Compound 3
Ph1 EBA*
Compound 4
Non-relapsing
cure
2-mo status
*or alternative
2-mo status
Outcomes Registry
3 yrs
2-moregimen
selection trial:
PNU-100480 (U)Bedaquiline (J)
plus one of:SQ109PA-824
ClofazimineImatinib
Rifabutin/PZA
XDR MDR DS

23
NAC Supplementation Prevents TB Drug-Induced Liver Injury
Baniasdai, Eur J Gastro Hepatol 2010
AST
Week
0 1 2
U/l
0
100
200
300
ALT
Week
0 1 2
U/l
0
50
100
150
200
HREZHREZ+NAC
T Bili
Week
0 1 2
mg/
dl
0.0
0.5
1.0
1.5
2.0
2.5
12/32 0/28 P =.002