saf-pac/srmh/care kamlesh giri april 23 rd, 2013
TRANSCRIPT
IUD – A Quick Update
SAF-PAC/SRMH/CARE
Kamlesh Giri
April 23rd, 2013
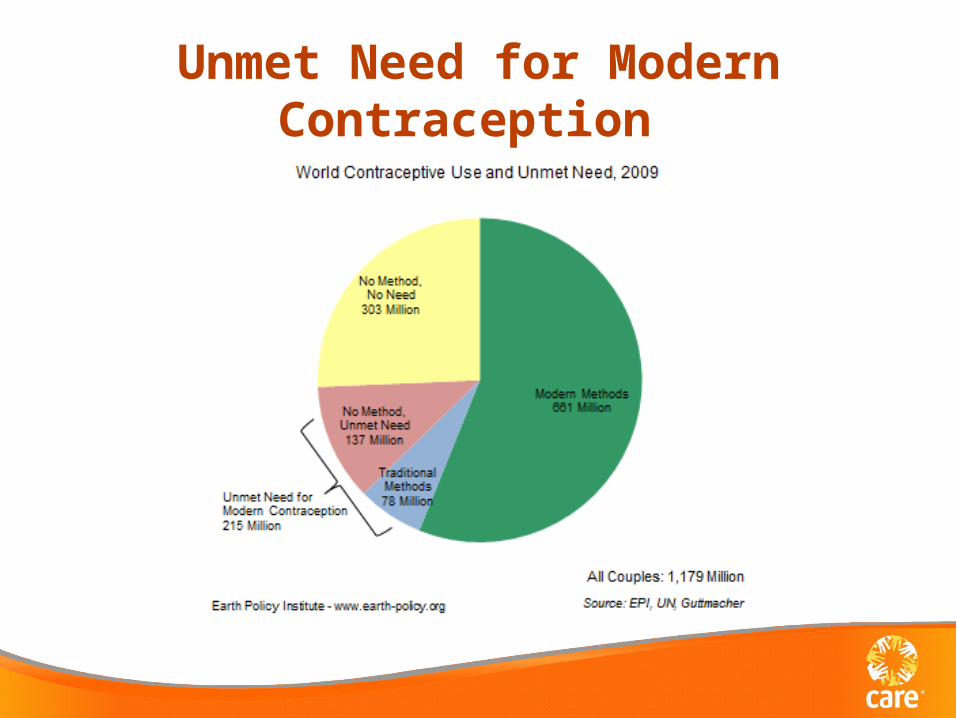
Unmet Need for Modern Contraception
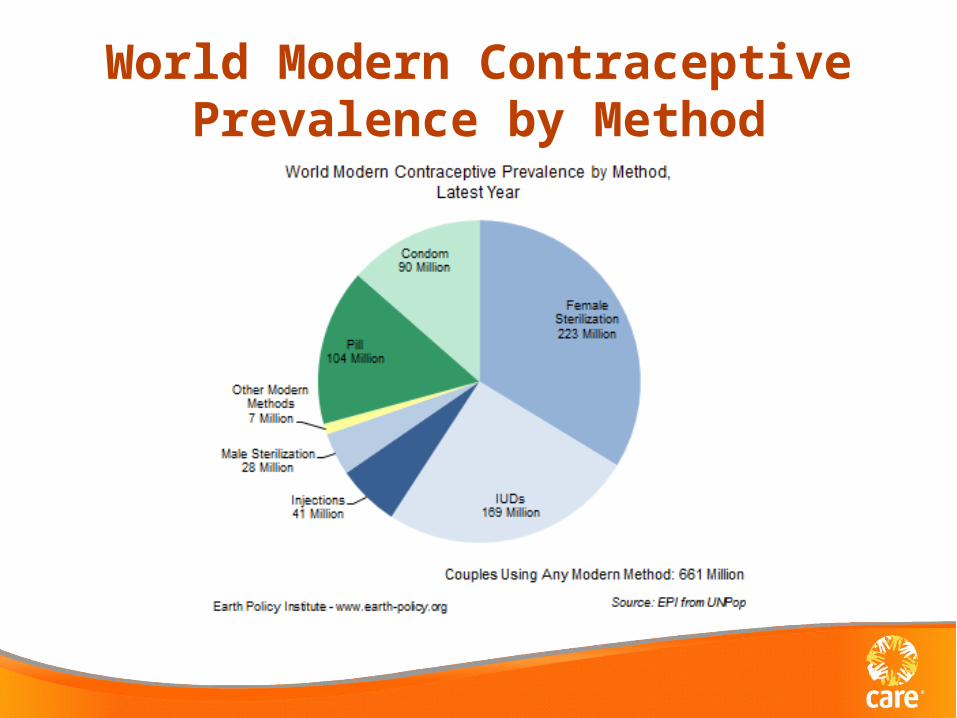
World Modern Contraceptive Prevalence by Method

World Map showing IUD Use
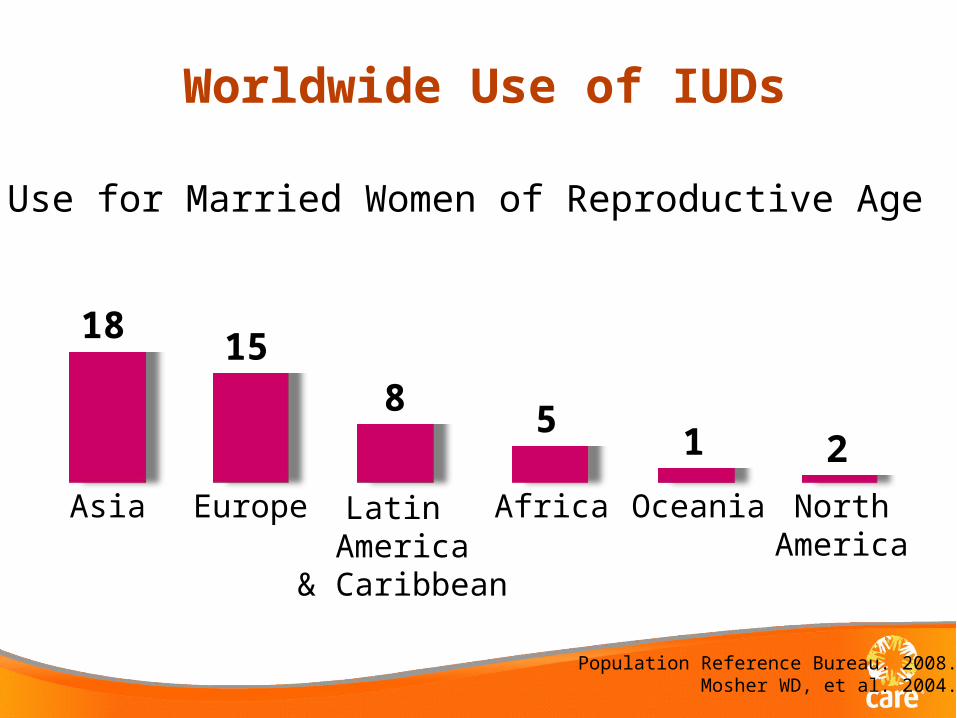
Worldwide Use of IUDs
Population Reference Bureau. 2008.Mosher WD, et al. 2004.
Asia
18
Europe
15
Latin America
& Caribbean
8
Africa
5
Oceania
1
NorthAmerica
2
% Use for Married Women of Reproductive Age
What others are saying about FP!
• "[Family planning] means the difference between being empowered and feeling powerless. It means the difference between celebrating a daughter's graduation and watching her drop out of school. It even means the difference between life and death.” Melinda Gates, HuffPost Blog

What is an IUD? • T-shaped plastic frame with copper wire/sleeves
• Highly effective in preventing pregnancy – failure
rate is less than 1% • Copper T 380A lasts for 12 years once inserted• Works mainly by preventing fertilization of an
egg by sperms • Most women can use IUDs, including women
who have never been pregnant • Fertility returns very quickly after removal • Very effective as emergency contraception
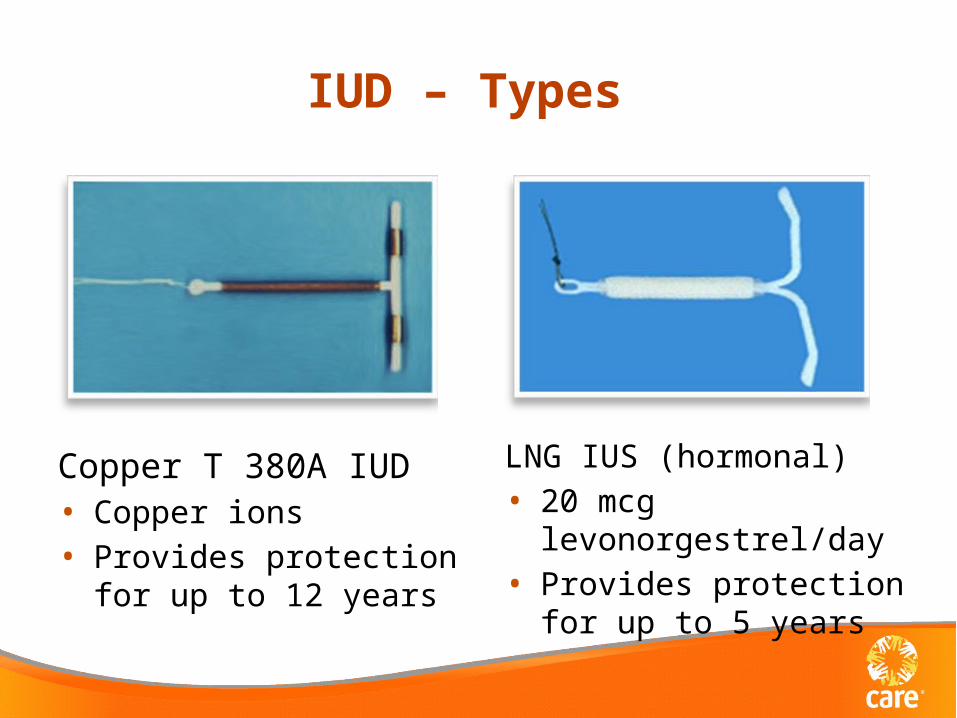
IUD – Types
Copper T 380A IUD• Copper ions• Provides protection for up
to 12 years
LNG IUS (hormonal)• 20 mcg levonorgestrel/day• Provides protection for up
to 5 years

IUD and IUS: Return to Fertility
0
20
40
60
80
100
3 6 9 12Months
Cu
mu
lati
ve p
reg
na
ncy
ra
te (
%)
LNG IUS
Copper IUD
Andersson et al. Contraception 1992;46:575Belhadj et al. Contraception 1986;34:261
Copper-bearing IUD: Timing of Insertion
Can insert any time reasonably sure woman is not pregnant
• Within 12 days after start of menses • Later in cycle/during amenorrhea if reasonably sure
not pregnant• < 48 hours postpartum (if no puerperal sepsis)• ≥ 4 weeks postpartum (if not pregnant)• Within 7 days postabortion
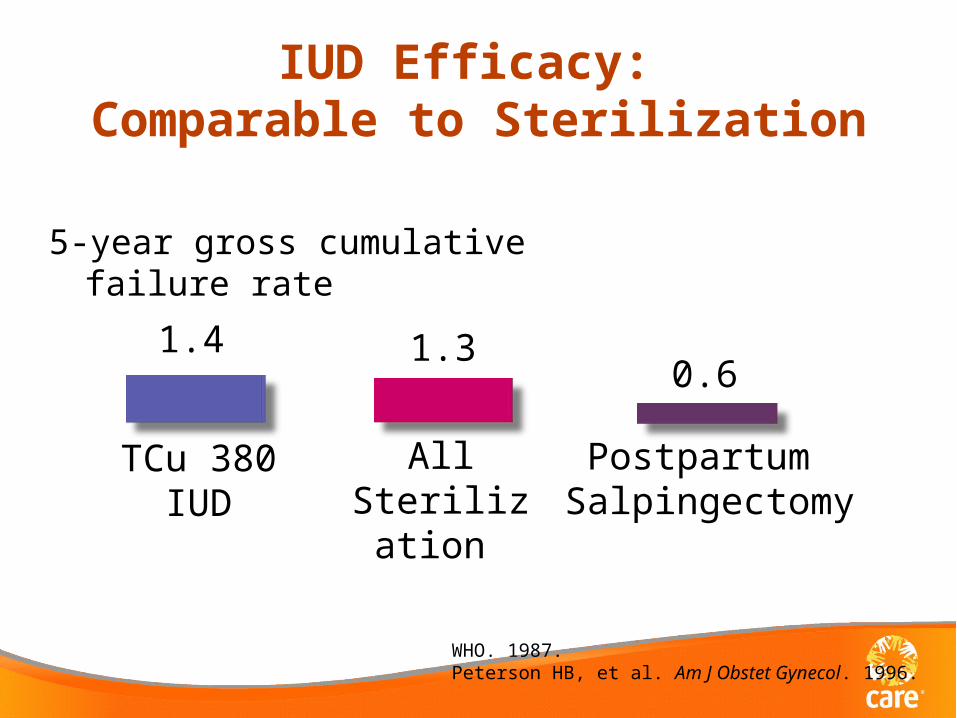
IUD Efficacy: Comparable to Sterilization
5-year gross cumulative failure rate
WHO. 1987.Peterson HB, et al. Am J Obstet Gynecol. 1996.
All Sterilization
1.3
TCu 380IUD
1.4
Postpartum Salpingectomy
0.6
Side Effects and Complications
• Might increase menstrual bleeding or cramps • Usually gets better after first 3 months
Complications • Rare
– Perforation of the wall of uterus by IUD or an instrument
– Pelvic inflammatory disease (PID) may occur if the woman has Chlamydia or gonorrhea at the time of IUD insertion
IUDs Can Be Used by MostHIV-Positive Women
• No increased risk of complications compared with HIV-negative women
• No increased cervical viral shedding• MEC Category:
• Initiation: not recommended if not fully controlled but can be initiated if clinically well on ARVs if other methods are not available or not appropriate
• Continuation: Can continue if more appropriate methods are not available
WHO. Medical Eligibility Criteria for Contraceptive Use. 2009.Morrison CS, et al. Brit J Obstet Gynaecol. 2001.
Richardson B, et al. AIDS. 1999.
Dispelling Myths: IUDs……
• Do not cause abortion• Do not cause ectopic pregnancies• Do not cause PID• Do not cause infertility• Are not too large for small women• Are unlikely to cause discomfort
for male partner• Do not travel to distant parts of the body• Are not contraindicated for HIV-positive women
Clinical Aspects
• Counseling – foundation for FP programs • Client screening
– Medical Eligibility Criteria – Pelvic exam
• Insertion procedure – doctors, nurses, mid-wives, health assistants, clinic officers
• Follow-up
IUD in Humanitarian Settings
• Barriers – usual suspects – Weak health infrastructure – Lack of trained providers – Lack of good logistics support – Poor supervision of services
IUD in Humanitarian Settings – contd
• Funding – small portion of the overall humanitarian funding pie for FP in general – and even smaller for IUD
• An average of $20.8 billion in total ODA annually to 18 conflicted-affected countries in study – $509.3 million (2.4%) for reproductive health – FP represents only 1.7% of RH activities
IUD in Humanitarian Settings – contd
• A few caveats: – SGBV is not coded as RH but rather as post-
conflict peace building by ODA – Does not include $ from philanthropic
organizations: e.g. Gates Foundation, Buffet Foundation
– Does not include $ from multilateral organizations: WHO, UNHCR, UNOCHA, WFP

Supporting Access to FP-PAC
• Program in 3 countries – Chad, DRC and Pakistan – Supported by Large Anonymous Donor – Emphasis on providing LARC to most underprivileged
women – women in crisis and post-crisis settings
• LARC as part of comprehensive FP method mix • SAF-PAC also supports RH services in Mali and
Djibouti but at a smaller scale

Contraceptive Method Mix – SAF-PAC
Chad DRC PAK
500847
3420
6501
5467
310
8741090
4259
1546
800
4397
23 93497
0 14 5
SAF-PAC Contraceptive Method Mix
IUD Implants OCP Injectables tublig vas
• Though widely used contraceptive method globally, IUDs are poorly utilized in Sub-Saharan Africa
• IUDs can be safely used by nulliparous women, HIV+ women, post-partum women
• IUD effectiveness comparable to permanent FP methods
• IUD does not cause PIDs • IUD considered best option as an EC • Need to improve funding $ for FP in general and
LARC in particular
Conclusion
Thank you
• Questions?
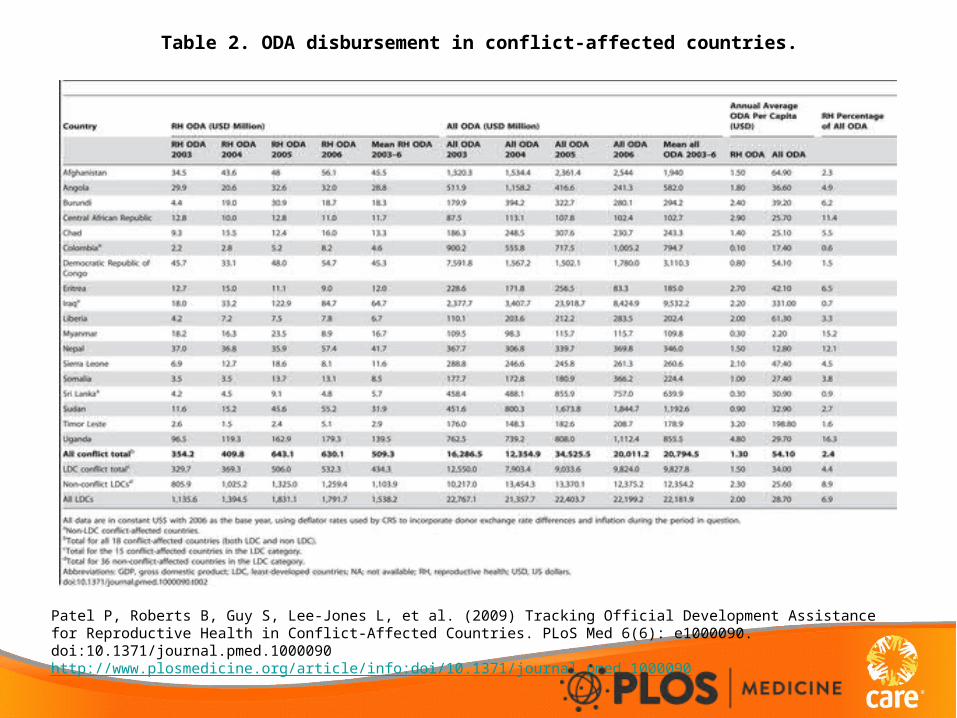
Table 2. ODA disbursement in conflict-affected countries.
Patel P, Roberts B, Guy S, Lee-Jones L, et al. (2009) Tracking Official Development Assistance for Reproductive Health in Conflict-Affected Countries. PLoS Med 6(6): e1000090. doi:10.1371/journal.pmed.1000090http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1000090