sadia a chowdhury the world bank may 26, 2010 the world bank’s reproductive health action plan...
TRANSCRIPT

Sadia A Chowdhury
The World Bank
May 26, 2010
The World Bank’s The World Bank’s Reproductive Health Action Plan Reproductive Health Action Plan
2010-20152010-2015
04/19/23 1

The World Bank has a long history of engagement in population and reproductive health
In 1970 the Bank gave its first health sector loan to Jamaica for family planning (US$ 2m)
In the past 10 years, the Bank has committed over US$ 1 billion for population and reproductive health
The Bank’s policy on population and reproductive health has evolved over time
• 1970-79: Focus on population • 1980-86: Focus on primary health care; population still priority; nutrition
gains importance• 1987-96: Focus on health reforms; Bank’s population agenda becomes
more comprehensive in response to ICPD 1994• 1997-06: Bank’s work remains guided by ICPD 1994; focus on high
fertility, low income countries; policy dialogue promoted
• The 2007 HNP strategy re-affirms Bank’s commitment to ICPD 1994, and places emphasis on comprehensive package of services through health systems
04/19/23 2

We know that progress on MDG 5 has been slow
The maternal mortality ratio in developing countries is 450/100,000 live births on average versus 9/100,000 in developed countries.
Fourteen countries – thirteen of which are in sub-Saharan Africa have maternal mortality rates in excess of 1000 per live births
Although the fertility rate in developing countries declined from 6 to 2.6 during 1960-2006, there are still 28 countries with TFR>5, mainly in Sub-Saharan Africa
Within countries there are significant variations in fertility rates by level of income, e.g. India, Colombia, Namibia
Under 25 population accounts for over 100 million STIs annually, other than HIV and 60% of unsafe abortions in Sub-Saharan Africa, yet their RH needs are not adequately addressed
04/19/23 3
Technical solutions are well-known, but not well implemented
Access to modern contraceptives and the ability to plan families is the first step in avoiding maternal deaths…
Yet less than half the demand for family planning is being met. Only 24% of the need is met in sub-Saharan Africa.
This is indicative of poor logistics and planning that often cause supply shortages.
Since complications are not predictable, all women need care from skilled health professionals during pregnancy, childbirth and in weeks after delivery…
Yet, a third of pregnant women do not receive care from skilled birth attendants during childbirth.
This is indicative to poor access to facilities and properly trained health workers. Health worker shortages are most acute in Africa.
… and demand for services remains low for the poorest households due to poor access and prohibitive costs.
04/19/234

Sustained political commitment and leadership is vital
At the national and local levels, the quality of overall governance directly affects the environment in which health systems operate and the ability of government health officials to exercise their responsibilities.
Government effectiveness countries in the High MMR-High TFR group rank consistently lower than other groups of countries
At the global level, despite a growing shared understanding on the solution set (Global Consensus), the issue has yet to be framed in a way to generate political commitment and subsequent action.
This is reflected in the ODA flows - we are not spending what we should and where we should.
04/19/23 5
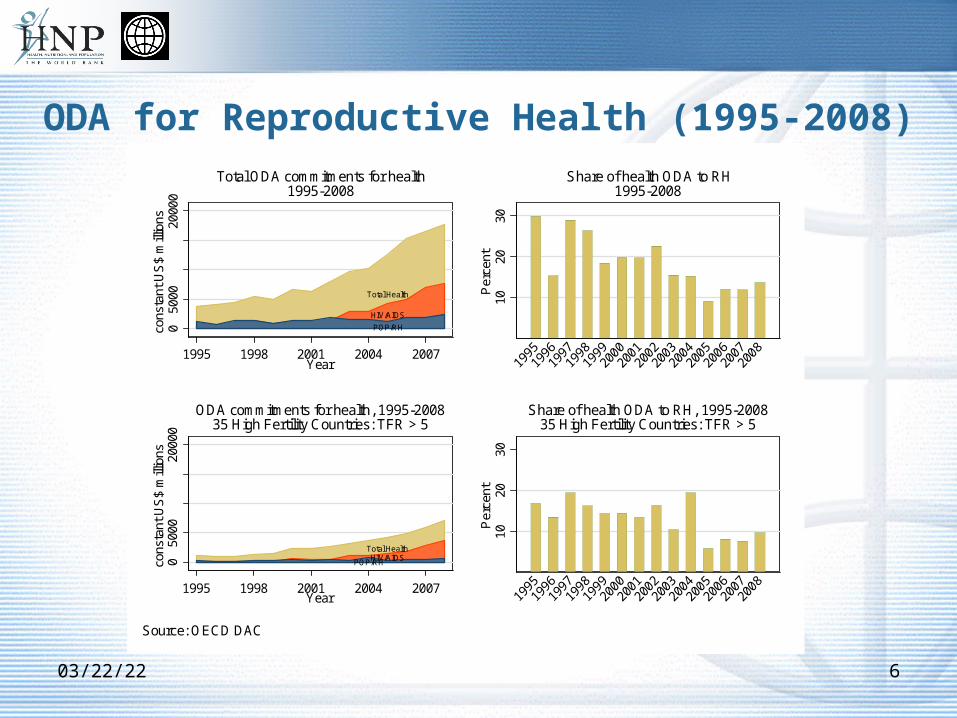
ODA for Reproductive Health (1995-2008)
04/19/23 6
HIV/AIDS
Total Health
POP/RH050
0020
000
cons
tant
US
$ m
illio
ns
1995 1998 2001 2004 2007Year
Total ODA commitments for health1995-2008
1020
30P
erce
nt
Share of health ODA to RH1995-2008
HIV/AIDSTotal Health
POP/RH050
0020
000
cons
tant
US
$ m
illio
ns
1995 1998 2001 2004 2007Year
ODA commitments for health, 1995-200835 High Fertility Countries: TFR > 5
1020
30P
erce
nt
Share of health ODA to RH, 1995-200835 High Fertility Countries: TFR > 5
Source: OECD DAC

We need to address these implementation constraints at various levels At the community and household level (e.g., increasing the demand for
services and removing financial and geographic barriers to maternal health services);
Health-services delivery level (e.g., effective human resource management to ensure health personnel attend to deliveries; upgrading and equipping health facilities; strengthening health management information systems for monitoring and evaluation);
Health-sector policy and strategic management level (e.g., strategic public-private partnerships to ensure universal access to health services);
In public policies cutting across sectors (e.g., promoting education of girls, expand road networks and making available affordable transport);
Addressing fragmentation of donor efforts and financing (e.g., harmonizing and coordinating the efforts of donors at country level to support countries to improve maternal health).
04/19/23 7

The Reproductive Health Action Plan leverages the Bank’s focus in 5 areas…
Countries with high maternal mortality and high
fertility
Key reproductive health interventions as part of
health systems strengthening
Reaching the poorest of the poor
Meeting the reproductive health needs of the youth
Leveraging partnerships
04/19/23 8

Belize
Botswana
EthiopiaNigeria
Chad
Uganda
Ukraine
Brazil
Mali
Niger
China
IndonesiaIndia
Mexico
Poland
Bangladesh
Egypt
55010
022
050
015
00
Mate
rnal m
ort
ality
ratio
(M
MR
)
1 1.5 2 2.5 3 4 5 6 7Total fertility rate (TFR)
Source: WDINote: Median TFR=3; Median MMR=220Note: Colors mark HIV prevalence among females aged 15-24Red=high prevalence (greater than 1.3%)Yellow=middle prevalence (between 0.3% and 1.3%)Green=low prevalence (less than 0.3%)
Maternal mortality vs fertility in developing countries, 2005
The Bank will prioritize high burden countries …
04/19/23 9

We will emphasize reproductive health in health systems strengthening by supporting…
Training of health workers and task shifting to fill gaps in skilled birth attendants
Performance incentives for skilled birth attendants and doctors
Country efforts to ensure proper facilities are available and adequate for rapid access to emergency obstetrics care.
Establishment of robust logistics, regulatory and quality assurance systems
Efforts to improve health monitoring systems, especially civil registration
04/19/23 10

We will support countries in their effort to reach the poor
We will proactively pursue strategies that ensure access to family planning and maternal health services among the poor
Our focus will be on helping countries reach the most vulnerable households – those in the lowest two income quintiles
We will support demand generation for reproductive health services through innovative financing
04/19/23 11
Training doctors and nurses to address special reproductive health needs of the youth
Supporting program that expanding information/knowledge about family planning and avoiding HIV/AIDS and sexually transmitted infections,
Supporting countries to motivate adolescents to stay in school and pursue their studies and acquire life skills before starting their families
We will assist countries to improve access to reproductive services for the youth
04/19/23 12

Harmonize support for country-led health system strengthening strategies to produce, finance and deliver and increase utilization of reproductive health services.
Ensure reproductive health benefits from ongoing efforts by the GAVI Alliance, Global Fund, World Bank and World Health Organization to develop a Health Systems Funding Platform, which aims at supporting country progress towards national health goals and the MDGs.
Support countries and civil society in strengthening national capacity for achieving MDG 5 through its work with UNFPA, UNICEF, and WHO (H4).
We will further leverage our partnerships with global partners and civil society
04/19/23 13

Moving Forward
Many countries are not on track to meet the MDG 5 target – and have only 5 years left in which to scale up their efforts
Its not only that we need more money and more resources – we also need to do much better than we are doing today and change the ways in which we define, design and implement actions to address issues related to reproductive health
Indeed, it’s a lot about attitudes and established paradigms – which must change if we want to have an impact
Not for Quotation04/19/23 14

Contact:
The World Bank’s The World Bank’s Reproductive Health Action Plan Reproductive Health Action Plan
2010-20152010-2015
04/19/23 15