ruptured mitral chordaetendineae -...
TRANSCRIPT

Ruptured Mitral Chordae TendineaeBy PHILIP J. OSMUNDSON, M.D., JOHN A. CALLAHAN, M.D.,
AND JESSE E. EDWARDS, M.D.
AMONG THE LESIONS responsible forinsufficiency of the mitral valve is rup-
ture of the chordae tendineae. It is our pur-pose to describe the significant clinical andpathologic findings in 20 cases of insufficiencyof the mitral valve due to rupture of the chor-dae tendineae. This report is based on thosecases in which ruptured mitral chordae ten-dineae were found at necropsy at the MayoClinic during the years 1934 to 1958 inclusive.The important etiologic factors claimed for
rupture of the mitral chordae tendineae arebacterial endocarditis,15 rheumatic valvulardisease,6 7 and trauma.8 9 Cases have beenencountered, however, in which conclusive evi-dence of these conditions has not been demon-strated. In those cases in which evidence for aspecific etiologic factor is lacking, so-calledspontaneous rupture10' 11 must be considered.Though myocardial infarction is the promi-nent cause of mitral insufficiency due to rup-tured papillary muscles,12' 13 it has not beendemonstrated to be of importance in ruptureof the chordae tendineae.
Etiologic Factors of Ruptured Mitral ChordaeTendineae
Bacterial EndocarditisBacterial endocarditis is the major factor
in the etiology of ruptured chordae tendineae.In the first case of ruptured mitral chordaetendineae reported in the medical literature(Corvisart 1812) ,14 necropsy findings wererecognizable in retrospect as due to bacterial
From the May.o Clinic and the Mayo Foundation,Rochester, Minnesota. The Mayo Foundation is a
part of the Graduate School of the University ofMinnesota.
Supported in part by research grant no. H-4014from the National Heart Institute, National Insti-tutes of Health, U. S. Public Health Service.Abridgment of thesis submitted by Dr. Osmund-
son to the Faculty of the Graduate School of theUniversity of Minnesota in partial fulfillment ofthe requirements for the degree of Master of Sci-ence in Medicine.
42
endocarditis. The association between bacte-rial endocarditis and ruptured mitral chordaetendineae was well demonstrated in reports byClark15 and by Washbourn1 late in the nine-teenth century. Ruptured chordae tendineaehave been identified in cases of healed, some-times clinically unrecognized, bacterial endo-carditis3 as well as in cases of active bacterialendocarditis.The present study includes 20 cases of rup-
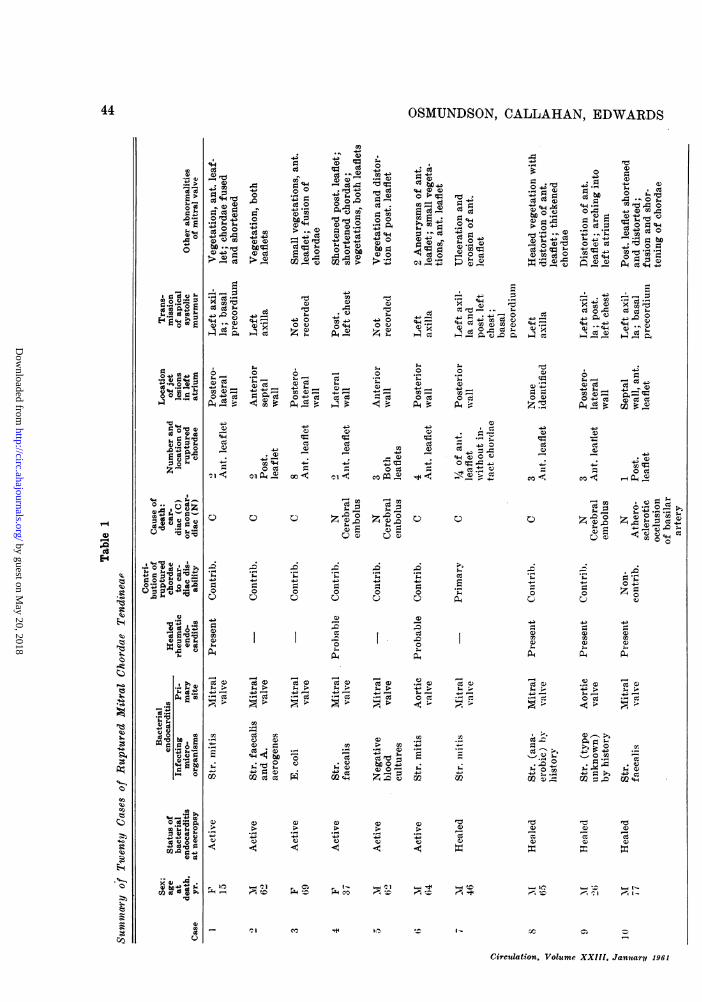
tured mitral chordae tendineae. In 10 casesthere was a history of bacterial endocarditis,active in six cases and healed in four (table1).Known Active Bacterial EndocarditisThe microorganisms cultured from the
blood of the six patients in this group wereStreptococcus mitis in two cases, Streptococ-cus faecalis alone in one case and associatedwith Aerobacter aerogenes in another case,and Escherichia coli in one case. The bloodcultures were repeatedly negative in the sixthcase, although active bacterial endocarditiswas demonstrated at necropsy. The report ofa representative case (case 4) follows.A 37-year-old woman entered the hospital in
February 1953. She had been treated first for bac-terial endocarditis caused by Str. faecalis 18 monthsbefore this admission when weakness, anorexia,and persistent fever had developed. Three monthsafter the onset she had hemiparesis on the rightside. Six months later a mycotic aneurysm wasexcised from the right forearm, and intermittentfever persisted despite continued treatment withantibiotics. Six days before her hospitalization,diplopia and left frontal headache had developed.On examination a high-pitched systolic murmur
of moderate intensity was heard over the precor-diuin which was maximal near the apex of theheart and transmitted posteriorly and to the left.The fingers were clubbed and the liver and spleenwere palpable. Str. faecalis was cultured from thepatient's blood. Treatment with penicillin com-bined with dihydrostreptonmycin was instituted.Suddenly the patient became comatose on hertwenty-fourth day in the hospital and died 48hours later.At necropsy the heart was found to be moder-
Circulation, Volume XXIII, January 1961
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
RUPTURED MITRAL CHORDAE TENDINEAE
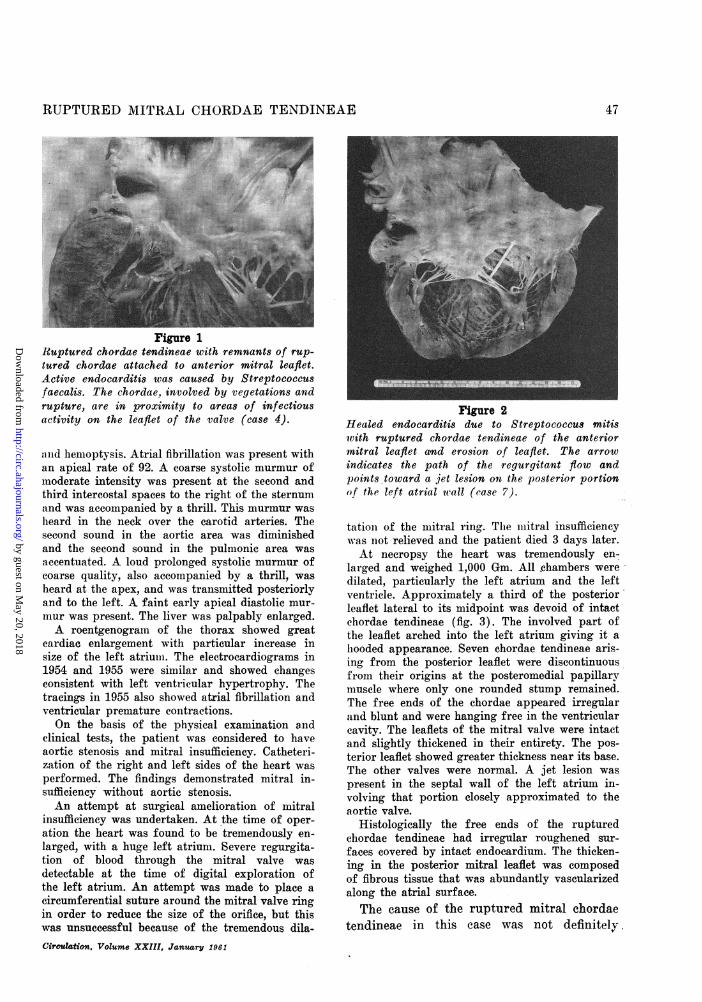
ately enlarged and weighed 500 Gm. The left ven-tricle was dilated and hypertrophied and the leftatrium was dilated. Both leaflets of the mitralvalve were thickened throughout. Many small vege-tations were present on the atrial side of the freeedge of both leaflets. There was moderate fusionof the leaflets at the posteromedial commissure.Two chordae tendineae of the anterior leaflet,which were located between the midpoint of theleaflet and the anterolateral commissure, werefound to be discontinuous from their origins on theanterolateral papillary muscle (fig. 1). Thesechordae tendineae were thickened and shortenedand were the sites of multiple small vegetations.Nearby, intact chordae tendineae also were thick-ened and were the sites of vegetations. In the leftatrium, 0.5 cm. above the lateral portion of theposterior leaflet, was a 3 by 5 em. portion that wasraised, irregular, and had the gross appearance ofa jet lesion and mural vegetation. Histologic ex-amination of the heart confirmed the presence ofactive bacterial endocarditis.The ruptured chordae tendineae in this
case were only one of many complicationsassociated with the active bacterial endocar-ditis. The site of rupture was in a region ofactive infection with vegetation formed on thechordae tendineae and mitral leaflet.
Known Healed Bacterial Endocarditis
Ruptured mitral chordae tendineae werefound in four cases in which evidence ofhealed bacterial endocarditis was present atnecropsy and in which bacterial endocarditishad been diagnosed during life. Streptococciwere the infecting microorganisms in each caseand in each case it was stated that the infec-tion had been cured sometime prior to thepatient's death. The following case (case 7)is illustrative.A 42-year-old man was first admitted to the
hospital in January 1947 with a history of ano-rexia, fatigue, and night sweats of 4 months' dura-tion. One month prior to his admission a heartmurmur was discovered for the first time. Exam-ination disclosed fever, clubbing of the fingers,and generalized petechiae of the skin. A systolicthrill was noted at the apex of the heart. A loud,rough systolic murmur was heard at the apex andtransmitted widely, particularly to the left axilla.A softer systolic murmur was heard at the baseof the heart. Cultures of the patient's blood yieldedStreptococcus mitis. The day after admission, hemi-paresis on the left and complete left homonymoushemianopsia developed. Treatment with penicillinwas begun and the response was satisfactory.
Circulation, Volume XXIII, January 1961
Examination of the patient in October 1947, 10months after the initial hospitalization, did notshow evidence of active bacterial endocarditis. Thepatient's cardiac reserve was considered to be good.A loud systolic murmur and an early diastolicmurmur were heard.
Later, in September 1950, when the patient wasagain hospitalized, he gave a history of progres-sive cough, dyspnea, and dependent edema of 5months' duration. Atrial fibrillation was present.An apical thrill was noted as well as a harsh apicalsystolic murmur that was transmitted to the leftaxilla and posterior part of the thorax on the sameside. The diastolic murmur was heard again. Asystolic murmur was heard at the base of the heartalso. Findings typical of congestive heart failurewere present. The patient's condition deteriorateddespite treatment and he died on the eleventh dayof hospitalization.At necropsy the heart was found to be enlarged
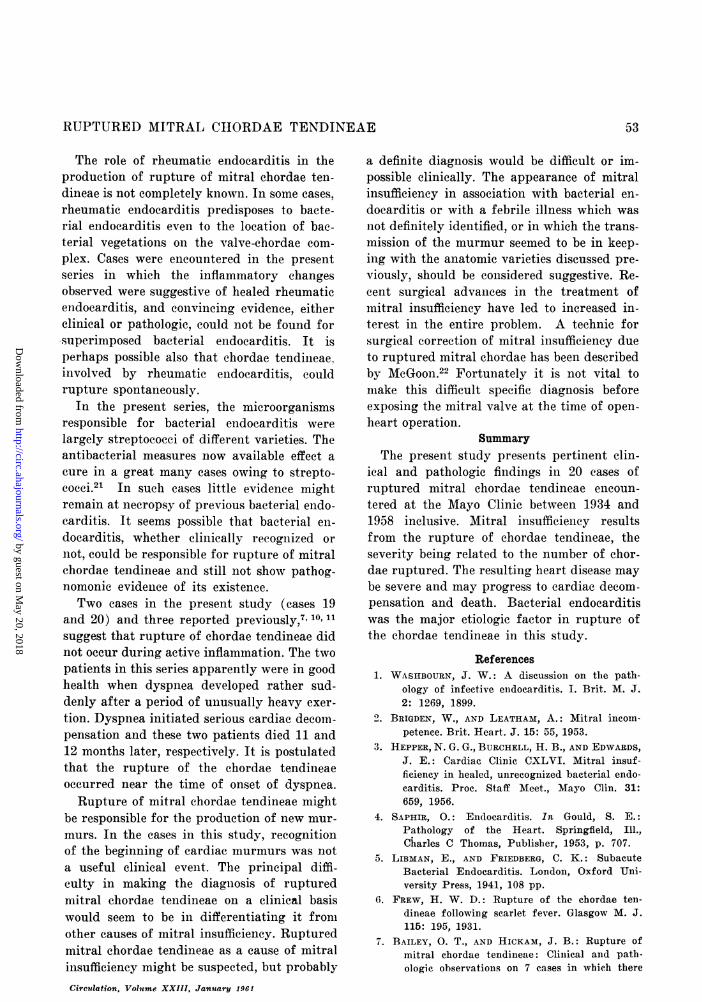
and weighed 600 Gm. The left atrium and the leftventricle were particularly dilated. Both ventricleswere hypertrophied. The anterior leaflet of theiiiitral valve was distorted in the portion adjacentto the posteromedial commissure. Approximately afourth of the leaflet in this region was devoid ofintact chordae tendineae (fig. 2). The leaflet wasmoderately thickened and arched up into the leftatrial cavity. It appeared that there had been aloss of substance of this part of the leaflet. Sev-eral of the intact chordae tendineae nearby wereslightly thickened. A thickened mural plaque meas-uring 1.6 cm. in diameter was found on the ven-tricular wall under the posterior mitral leaflet.This had the appearance of healed mural endocar-ditis. A jet lesion was found in the left atriumabove and posterior to the posteromedial commis-sure. The other heart valves did not appear to beabnormal.
Histologically, one of the ruptured chordaetendineae had an enlarged fragmented end withcalcified and necrotic debris adjacent to the tip.The thickened anterior mitral leaflet was composedof fibrous and collagenous tissue. The plaquelikestructure on the endocardium of the left ventric-ular wall was composed of thickened endocardiumwith foci of calcified debris. The adjacent fibroustissue was vascularized.
Mitral insufficiency occurred as a compli-cation of bacterial endocarditis in this caseand caused cardiac decompensation that re-sulted in death. Mitral insufficiency resultedfrom rupture of the mitral chordae tendineaeattached to a portion of the anterior mitralleaflet. Erosion of a portion of the mitral leaf-let was an additional complication of the bac-terial endocarditis.
43
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
OSMUNDSON, CALLAHAN, EDWARDS
4-; 4
'-
Cc .00 cct
0~~~~C 0 e 9;0 .'
CCCC~~~~~~~~~~~)CC~ ~ ~~~~-. '
CC C44~-4. U"0) :CO)~~~~~~~ g~~~~~~~ C' MccCM -W )~). CC )C 00oM~C) 4-4 g)0 C)CC.CC02 >4-* C) #'>
----4- ---C - )Cd
0> ce C 4.4C C)e ..? .4 .1 -4 .4d~~~~~~~~~~~~~~'4 44
ho
Ccg 0,C
CCd44C) C)C .02 +C4~~~~~~~~~~~C) CC C)
cc~ o4 o Cc.U) ) U ) '4m m r044 0CCO4
o o - X - 0 o-;t-;)
C Cc) * C
* e * ~C PAzvew Q
W ot o v X v w: v OW cc
C) C ) C)
c,]p- 4o~C J 4-
O O O CO OV0)-
V V4V-VP C QCP4> 4 4 4: 4 4
CC~~~~~~~~~~.4- 4- 4-4- 4- 4-~~~~~~~~~~~~~~~~~~~~~~a
CC CC CC~~~~~~~~~~~o 00 0 0 0 44~~~~~~~~
o 00 0 0 0 ~~~~~
4- C) C
44) c
p44
Beces. C)
-¢
t E n ; QQ0DC
0d0
An-
4- 0 *0 To0 C)
4 4-4a)
X
CCC) occ ) C C) cc C)
ct -cc *cc C 0 cC
CC or .-C.)- e- Q e O Q 'Q ) . cc,~
C)cc C&4 CCC
C ) C C ) X C ) C) C ) C ) a c )
-;-O-
Circulation, Volume XXIII, January 1961
44
E. >
0.0
r.
Z
4.3
CO
X
3W.._
b Cd .As
o- odA-°
'-44)
'4
pm
'4)
33
l)
:9
rt3
14)
0"C
lie
a)
0)'4)0)
h.
Z8*
zt
a.-
a0
*
-4.4 U)4e.o "6X
al.b
U44440
G2.0 CC.4
W talol:_a & 1i _ >1m dCd 9 F.. 5f -2 > ~ to P6 tz P1 c, to > z * -to W.r, In. h_4 t_rln 1-0 r'. 1: r-1, a -
Wcc - e., 1 CYID 1 (". l= 1-0c
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
RUPTURED MITRAL CHIORDAE TENDINEAE
x; ;., ° ° E X * _, 4i
4-' 4-° Q @ s < a°; E ; C E
Q).C .4. --0
004
b£+ *ce CC
CC0 ec 74c
). ; ; Y ;- ;
5
42 C-0C02
cc Cc cc0
---
C)
W
AJ CC_
ce ...eFi- O
;I-
r.
. 9 ~
C) 0
¢- C4.44
O11OWCfx o
4-J,~ ~~~UM
g 4, Q
a),
o r*= ;o0ccC.
4->
4-0g-4Z000P
Acc QQ
(D a e 0P0. a) c
m ~: CO --400~
cd P.c
4--4-5Z
toGO ^V °:ov40Q
0ec
ce0CL
* 0
+ O0
o4 + Cz
0 'm-Ct4- (.
0~~~~~~~rZo.-W z 91---1
0)r 4~'F
qHI"
0 0 00
eH
g
. S- -
;Q
4*00 c
cl J~
40.i*2v
0 c
L- P4 c)
cc.4-
ce 9)W P-
O
P,.~
00X x:
o s a) WC'1 X Q ¢ Q V e o=;C)ceP
f. 8
A~0 00-- 0 ~
oZ0-
05, A04P.
0
4
0
P4
00
4._
0W^
I
*- P
* * *
a a
* *
cid cc ce10 0
e =occ0 ,r 0 -
0e , , e ,D 0..,,3
o F ~~~~~~cc ce +) c
tCxW
PI &Cm0
,,0 , 10
04- 0 4D .
0 0
CI C.
* *
0 a)14-4
-0
0 0o 0*--- ---
4- 4-
000Y 0~
*
a)0Cd00
0201
cy0 t ~ .
45
*_4
00
0
W C0
*
0
0
z
.,
ro
4-.0
4A0
0m
.C0z60
*
Circulation, Volutme XXIII, *January 1961
c
,. CC---4 c.-4 c -14m C) E C.)c -,, ~ . - W :i Q)
r...g 4.> -14 ~
4.; 00 P.4 -,_%.4 z m Qc> cc 0 A., cc 0 ~b-. ---, ;:. W m C.) =
.m CWM a)cc rC
. 4J.)+. 9 +i a)C4-4 CO m a)9) ce 0 CS. 1. P4 (W
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
OSMUNDSON, CALLAHAN, EDWARDS
No History of Bacterial Endocarditis
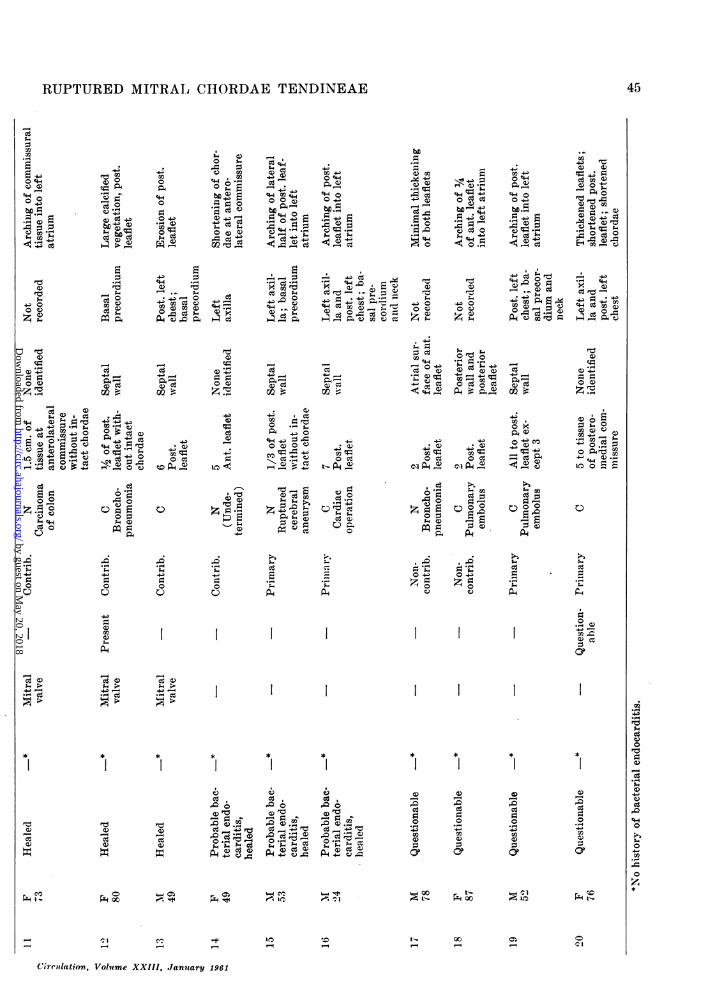
Pathologic Evidence of Healed BacterialEndocarditis. Ten of the 20 patients in thisstudy did not have a history of bacterial en-
docarditis. Necropsy disclosed evidence con-
sidered positive for healed bacterial endocar-ditis in three of the 10 cases, while in an
additional three cases the cardiac abnormali-ties, in addition to the ruptured chordaetendineae, were suggestive though not conclu-sive evidence of healed bacterial endocarditis.The report of a representative case (case 13)follows.A 49-year-old man entered the hospital in May
1957. He did not have a history of rheumatic feveror any significant febrile illness. The presence ofa heart murmur had been known only since theonset of the patient's symptoms 8 months beforehis last admission. Exertional dyspnea and de-pendent edema developed 8 months prior to hisadmission to the hospital. Orthopnea and paroxys-mal nocturnal dyspnea appeared 10 days beforehis admission.
Physical examination showed the heart to beenlarged. A slight apical thrill was detected. Aloud systolic murmur was present over the entireprecordium. This was loudest in the fourth inter-costal space near the midelavicular line and was
transmitted posteriorly and to the left. Rales were
present in the lungs; the liver was enlarged to4 cm. below the right costal margin, and consider-able pretibial edema was present. A roentgenogramof the thorax disclosed cardiac enlargement withpulmonary vascular congestion. An electrocardio-gram showed a sinus rhythm with multiple prema-ture contractions and nodal escape beats. A sub-sequent electrocardiogram made 2 days latershowed variation between a sinus rhythm and an
idioventricular rhythm. The patient did not re-
spond despite intensive treatment for congestiveheart failure and died on the fourth hospital day.At necropsy the heart was found to be moder-
ately enlarged and weighed 430 Gm. All chamberswere dilated and the left ventricle particularlywas hypertrophied. The mitral valve was the siteof considerable abnormality. The posterior mitralleaflet was lacking in substance along its free edge,apparently from an old ulcerative process. Theposterior leaflet projected up into the left atrialcavity. Approximately two thirds of the posteriormitral leaflet was without intact chordae tendineae.Remnants of the ruptured chordae were foldedunder the deformed posterior leaflet and their endswere round and smooth. The anterior mitral leafletnear the anterolateral commissure also appearedto be altered by an ulcerative process, which later
healed. A small projection from the posteromedialpapillary muscle represented the origin of the rup-tured chordae tendineae. The intact chordae ten-dineae appeared normal. A jet lesion measuringapproximately 2 by 3 cm. was present on the sep-tal wall of the left atrium beginning 1 cm. abovethe anterior mitral leaflet. Histologically the thick-ened, deformed posterior mitral leaflet was com-posed of irregular masses of collagenous andfibrous tissue.
This case demonstrates the finding of rup-tured chordae tendineae in a patient who didnot have a history of bacterial endocarditisbut at necropsy definite evidence of healedbacterial endocarditis was found. Mitral in-sufficiency resulted from rupture of the chor-dae tendineae and led to the death of thepatient.Without Pathologic Evidence of Healed
Bacterial Endocarditis. The cause of rupturedchordae tendineae in the other four cases wasnot determined. At necropsy evidence of aninflammatory process which had healed priorto the death of the patient was present in eachof the four cases, but the lesions were non-specific and did not allow a precise identifi-cation of their causes. The following case isan example (case 16*).A 23-year-old man was examined in November
1955 for evaluation of a heart murmur first dis-covered 7 years previously. There was no historyof rheumatic fever or trauma to the thorax. Ex-amination of the heart in 1944 gave essentiallynegative results. In December 1948 an illness be-gan that lasted 6 weeks and was characterized byfever, lassitude, and weakness. The patient washospitalized during this illness and the roentgeno-gram of the thorax disclosed inflammation in onelung. The heart murmur was heard first at thistime. Exertional dyspnea, severe enough to preventparticipation in vigorous activities, was presentfrom the time of this illness. Gradual diminutionin the patient's tolerance for exercise developedduring the next 5 years.On first examination at the Mayo Clinic in Oc-
tober 1954, loud systolic murmurs accompanied bythrills were heard over both the aortic and apicalareas. Little symptomatic change took place afterthis visit until 1 month prior to registration inNovember 1955. At this time the patient experi-enced dyspnea with minimal exertion, paroxysmalnocturnal dyspnea, vague epigastric discomfort,
*This case formed the basis of a previous publi-cation.16
Circulation, Volume XXIII, January 1961
46
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
RUPTURED MITRAL CHIORDAE TENDINEAE
Figure 1iRuptured chordae tendineae with remnants of rup-tured chordae attached to anterior mitral leaflet.-Active endocarditis wias caused by Streptococcusfaecalis. The chordalc, in volved by veyetations andrupture, are in proximity to areas of infectiousactivity on the leaflet of the ralve (case 4).
.i11(1 heiloptysis. Atrial fibrillatioii wNvas present wsitlhan apical rate of 92. A coarse systolic murmur ofmoderate intensity was present at the second andthird intercostal spaces to the right of the sternumand was accompanied by a thrill. This murmur washeard in the neck over the ecarotid arteries. Thesecond sound in the aortic area wvas diminishedand the second sound in the pulhnonie area wasaccentuated. A loud prolonged systolic murmur ofcoarse quality, also accompanied by a thrill, washeard at the apex, and wvas transmitted posteriorlyand to the left. A faint early apical diastolic mur-imur was present. The liver was palpably enlarged.A roentgenograiii of the thorax showed great
cardiac enlargement with particular increase insize of time left atrium. Time electrocardiograms in1954 and 1955 were simtiilart and showed changesconsistent with left ventricular hypertrophy. Thetracings in 1955 also showled atrial fibrillation andventricular premature conitra(tions.On the basis of the phiylsilcal examinationl and
clinical tests, the patient was considered to have('aortic stenosis and mitral insufficiency. Catheteri-zation of the right and left sides of the heart wBasperformed. The findings demonstrated mitral in-stfficiency without aortic stenosis.An attempt at surgical amelioration of mitral
insufficiency was undertaken. At the time of oper-ation the heart was found to be tremendously en-larged, with a huge left atrium. Severe regurgita-tion of blood through the mitral valve wasdetectable at the time of digital exploration ofthe left atrium. An attempt was made to place acircumferential suture around the mitral valve ringin order to reduce the size of the orifice, but thiswas unsuccessful because of the tremendous dila-Circulation, Volume XXIII, January 1961
Figure 2Healed endocarditis due to Streptococcus mitiswith ruptured chordae ten;,dineaie of the anteriormitral leaflet awd erosion) of leaflet. The arrowindicates the path of the rcfloyitwatow andj)oints toward a jet lesion ow the posterior portionof the left atrila wall ('SCas v).
ta.tim()ii of the iaitral rimlc. Time iitral insuifficienieywas not relieved and the patient died 3 days later.At necropsy the heart was tremendously en-
laitged and weighed 1,000 Gm. All chambers weredilated, particularly the left atrium and the leftventricele. Approximately a third of the posteriorleaflet lateral to its miidpoint was devoid of intactchordae tendineae (fig. 3). The involved part ofthe leaflet arched into the left atrium giving it ahooded appearance. Seven chordace tendineae aris-ilng froin the posterior leaflet were discontinuousfroom their origins at the posteromedial papillarymuscle where only one rounded stump remained.The free ends of the chordae appeared irregularand blunt and were hanoing free in the ventricularcavity. The leaflets of the mitral valve were intactand slightly thickened in their entirety. The pos-terior leaflet showed greater thickness near its base.The other valves were normal. A jet lesion waspresent in the septal wall of the left atrium in-volving that portion closely approximated to thesortie valve.
Histologically the free ends of the rupturedehordae tendineae had irregular roughemned sur-faces covered by intact endocardium. The thicken-ing in the posterior mitral leaflet was composedof fibrous tissue that was abundantly vascularizedalong the atrial surface.The cause of the ruptured mitral chordae
tendineae in this case was not definitely.
4 -
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMUNDSON, CALLAHAN, EDWARDS
known. The evidence, although not absolutelyconclusive, suggested that bacterial endocar-ditis had been present. The lesion causingthickening of the base of the posterior mitralleaflet was consistent with a healed vegetationof bacterial endocarditis. The history of theonset of the murmur during a febrile illnessfurther supported the opinion that the rup-tured chordae tendineae were a complicationof bacterial endocarditis that healed later.The report of another representative case
(case 19) follows.A 52-year-old farmer was admitted to a hospital
ill November 1948 because of dyspnea and weak-ness of 1 year's duration. There was no historyof rheumatic fever. The illness leading to hospital-ization had begun suddenly in November 1947when the patient became short of breath afterworking strenuously to harvest grain. He was un-able to work after the onset of this illness andsubsequently orthopnea and pedal edema devel-oped accompanied by loss of weight.
Physical examination at the time of admissionto the clinic disclosed a blood pressure of 105 mm.Hg systolic and 85 mm. Hg diastolic. A loud harshapical systolic murmur and a presystolic murmurwere heard. A systolic murmur also was heard atthe base of the heart with transmission to the ves-sels in the neck. Venous distention indicated anelevated venous pressure. Pulmonary rales, hepato-megaly, and pedal edema were present. A roent-genogram of the thorax disclosed cardiac enlarge-ment and pulmonary edema.The patient responded to the prescribed medical
program at first, but cough, fever, and hemoptysisdeveloped on the fifteenth hospital day. His condi-tion deteriorated and he died on the twenty-secondhospital day.At necropsy the heart was found to be enlarged
and weighed 555 Gm. The left atrium was dilated.Both ventricles were dilated and hypertrophied.The posterior mitral leaflet projected up into theleft atrial cavity giving it a hooded appearance(fig. 4). Approximately four fifths of the posteriorleaflet was without intact chordae tendineae. Onlythree chordae tendineae remained intact, and thesewere in the region near the posteromedial commis-sure. The other cardiac valves appeared normal.Portions of both the anterolateral and the postero-medial papillary muscles were atrophied. Minimalthickening of the posterior mitral leaflet was pres-ent. Neither the remnants of the ruptured chordaetendineae nor the remaining intact chordae teni-dineae appeared thickened or fused, or the site ofvegetation. The endocardium of the septal wall ofthe left atrium above the anterior mitral leaflet
was irregularly roughened and thickened, haviagthe appearance of a jet lesion. A thrombus waspresent in the right atrial appendage.
Microscopically the ends of the ruptured chor-dae tendineae were covered by intact endotheliunii.Moderate fibrosis was present between the musclefibers and the adjacent papillary muscle. The junc-tion of the papillary muscle with one of the rup-tured chordae tendineae was vascularized in onearea near the endocardial surface. The microscopicappearance of the left atrial wall in the region ofthe septum supported the opinion gained fromgross examination that this was a jet lesion.
Evidence of a healed inflammatory processin the heart of this patient was minimal. Thelesions remaining as residuals of the inflamn-matory process that had healed prior to deathof the patient were not specific enough to al-low an etiologic diagnosis. The sudden appear-ance of cardiac decompensation 1 year priorto death suggested that the chordae tendineaehad ruptured at that time.
Other Etiologic Factors. Rheumatic heartdisease was a factor of etiologic importancein the 20 cases comprising this study prima-rily in predisposing to bacterial endocarditis.In each of the five cases with evidence at nec-ropsy of quiescent rheumatic heart diseasethere also was conclusive evidence of super-imposed bacterial endocarditis, active in onecase and healed in four cases. In two addi-tional cases necropsy findings were consideredsuggestive of inactive rheumatic endocarditisand valvulitis. In both cases, evidence of ac-tive bacterial endocarditis was found.No evidence of direct trauma to the thorax
of an unusual nature was found in any of the20 cases. In all cases the findings iimdicatedthat the abnormality of the chordae tendineaewas acquired and not congenital.
Pathologic Anatomy in Ruptured Mitral ChordaeTendineae
In this series of 20 cases, chordae tendineaearising from the anterolateral papillary mus-cle were ruptured in nine cases; chordae aris-ing from the posteromedial muscle were rup-tured ill eight cases; and chordae arisingfront both group)s were ruptured in threecases.
The site of insertion of the chordae tendin-cae on the valve leaflet is of importance in
Circulation, Volume XXIII, January 1961
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

RUPTURED MITRAL CHORDAE TENDINEAE
Figure 3 Efigure %Ruptured chordae tendineae of the posterior mni- Ruptured chordae tendineae of the posterior leaflettral leaflet with arching of this portion (R) into with only remnants of the chordae present on thethe left atrium. An arrow demonstrates the path leaflet. The hooded appearance of the posteriorof the regurgitant blood from the posterior leaflet leaflet is demonstrated (case 19).to the septal wall where a jet lesion is located.The close relationship of the jet lesion and theaortic valve (A.V.) is demonstrated. The septalwtall and aortic valve in sagittal section are shown.An artifact is beneath the base of arrow (ease 16).
cases of ruptured chordae tendineae. In thepresent study, chordae inserting on the ante-rior leaflet were ruptured in nine cases, thoseinserting on the posterior leaflet in eight cases,those inserting on both -leaflets in one case,those inserting in the region of the antero-lateral commissure in one case, and those in-serting in the region of the posteromedialcommissure in one case.Ruptured chordae numbered from two to
nearly all those inserting on one leaflet. Therewas a general correlation between the numberof ruptured chordae and the degree of mitralinsufficiency as estimated at the time of nec-ropsy.Location of Ruptured Chordae Tendineae
In patients with bacterial endocarditis twoimportant factors apparently influence thelocation of the ruptured chordae. In cases inwhich the infection involves the mitral valveit appears that the involved chordae are lo-cated adjacent to sites of most active infec-tion. This situation prevailed in 11 of 13 casesin the present series that were considered tohave definite evidence of bacterial endocardi-
tis, active or healed, during the patient's lifeor at necropsy. The mechanism that deter-mined this location appeared to be extensionof the infectious process from the leaflet to theadjacent chordae, as stated by Saphir,4 andby Libman and Friedberg5 (fig. 1).The other important factor determining
location of the ruptured chordae prevails ina special situation in which bacterial endocar-ditis involves the aortic valve causing aorticinsufficiency. In such a case the regurgitantstream of blood often strikes the ventricularsurface of the anterior mitral leaflet and thechordae attaching to the midportion of theanterior mitral leaflet. It is probable that theinfectious process extends from the aortievalve to the chordae of the anterior mitralleaflet by this means, with subsequent ruptureof the involved chordae. Two cases in thisgroup of 20 demonstrated this situation. Inboth cases there were residual defects of theaortie cusps resulting from bacterial endo-earditis (fig. 5).Jet Lesions
Endocardial roughening and thickenicharacteristic of so-called jet lesions werefound on the left atrial wall in 16 of the 20cases. These lesions usually were found onthe atrial wall opposite the part of the leaflet
Circulation, Volume XXIII, January 1961
49
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMUNDSON, CALLAHAN, EDWARDS
that was the site of the ruptured chordae.Other factors that contributed to the locationof the jet lesions were abnormalities of theleaflets such as vegetations, fixed deformitiesresulting from old vegetations, and loss of val-vular substance from ulcerative processes. Thejet lesions usually were situated in the lowerpart of the left atrium (fig. 6).The manner in which blood regurgitates
through the mitral valve in cases of rupturedchordae tendineae can be deduced from cer-tain anatomic findings. In cases in which theruptured chordae had been present for sometime, the involved mitral leaflet could be ob-served at necropsy to be arched up into theleft atrial cavity leaving the leaflet fixed in acharacteristic hooded appearance (fig. 4). Incases in which rupture of the chordae prob-ably occurred shortly before death, this find-ing was not observed. It is postulated thatduring systole the ruptured chordae allow theinvolved mitral leaflet to extend beyond itsnormal position of coaptation with the oppo-site leaflet and beyond the level of the unin-volved part of the same leaflet. The regurgi-tant blood striking the leaflet is deflectedrather sharply across the left atrium whereit strikes the atrial wall or atrial surface ofthe intact mitral leaflet.
In two of the four cases in which no jetlesions could be definitely identified, somechordae had ruptured that were normallyattached in the vicinity of the commissures.It has been postulated that the reason for theinfrequent occurrences of left atrial jet le-sions in association with rheumatic mitralinsufficiency is that the energy of the regur-gitant stream is dissipated by the directionthe regurgitant stream takes into the leftatrium. This also may explain the absence ofleft atrial jet lesions in these two cases ofruptured chordae to the commissural regionsin which, probably, the regurgitant streamwas directed more centrally into the left atrialcavity.
Findings in Study of Clinical RecordsMurmurs
The theory has been advanced that the loca-tion of jet lesions may explain some of the
characteristics of heart murmurs.'17 18 Thelocation of the ruptured chordae (the partic-ular portion of the leaflet that allows regur-gitation) and the evidence of jet lesions in theleft atrium form the anatomic bases for anexplanation of some characteristics of themurmurs.
The murmur most frequently recorded inthis series of cases was an apical systolic mur-mur, which was present in every case. Theadjectives used to describe the murmursvaried considerably but included the terms" harsh," " high pitched, " " whistling, ""blowing," and "coarse," as well as variousestimations of the intensity. An associatedsystolic thrill at the apex was recorded in fivecases. In the cases in which no lesions of othervalves existed, a diastolic murmur was re-corded in three instances. This was specifi-cally described in one patient as a presystoliccomponent of the systolic murmur.
In the group as a whole there was no uni-formity in the transmission of the systolicmurmurs. The areas to which transmissionoccurred were those in which the murmur ofmitral insufficiency is typically transmitted,namely, the left axilla, the left posterior por-tion of the thorax, and the basal area of theplecordium. There appeared to be a definitecorrelation between the location of the rup-tured chordae and the transmission of mur-nurs in some cases.Definite left atrial jet lesions were recog-
nized in all eight cases involving chordae ofthe posterior leaflet. In one case the jet lesionwas located on the anterior mitral leaflet op-posite the site of ruptured chordae. In sevencases the lesions were located on the septalwall of the left atrium. In one case of ruptureof chordae to the posterior mitral leaflet thejet lesion was located in the septal wall of theleft atrium adjacent to the aortic valve (fig.3). The apical systolic murmur was trans-mitted to the aortic area and to the vessels ofthe neck; it simulated the murmur of aorticstenosis. The proximity of the jet lesion to theaortic valve forms the anatomic basis for thetheory of the production of the aortic systolicmurmur in this case.
Circulation, Volume XXIII, January 1961
50
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

RUPTURED MITRAL CHORDAE TENDINEAE
Figure 5Case 6. Active endocarditis due to Streptococcusmitis with involvement of the aortic valve, withaortic insufficiency and secondary spread of theinfectious process to the chordae of the anteriormitral leaflet. Vegetations on the chordafe are dem-onstrated. Ruptured chordae, though not clearlyevident, were located in the region of this infec-tious activity. (The arrow points in the presumeddirection of the regurgitant stream originating atthe aortic valve.)
An additional patient ill the present study(case 19) had auscultatory findings similar tothose in the case described (case 16). Thesefindings were a basal systolic murmur withtransmission to the cervical vessels in additionto the apical systolic murmur. The aortic valvewas normal at necropsy in this case also, andthe jet lesions on the septal wall were ana-
tomically close to the aortic valve.Two other cases of mitral insufficiency due
to ruptured chordae tendineae simulatingaortic stenosis have been described.19' 20 Inboth cases, however, the chordae to the ante-rior mitral leaflet were ruptured rather thanthe chordae to the posterior mitral leaflet. Inone the jet lesions were partially adjacent tothe aortic valve, but in the other the jet le-sions were on the posterior atrial wall.
In the present study there were four othereases in which ruptured chordae of the pos-terior leaflet were found and basal systolicmurmurs were recorded. Thus, in six of theeight cases with ruptured chordae of the pos-terior leaflet, transmission of an apical sys-
tolic murmur to the basal area of the precor-
Circulation, Volume XXIII, January 1961
Figure 6Case 6. Section of left ventricle, left atrium, andposterior mitral leaflet in case of ruptured chordaetendineae of the anterior mitral leaflet shown infigure 5. The jet lesion on the left atrial wall andadjacent posterior mitral leaflet is demonstrated.Verhoeff's elastic-tissue stain counterstained withvan Gieson's (onniective tissue stain.
dium was present. In these eight cases theapical systolic murmur was transmitted alsoto the left axilla in three, to the posterior leftpart of the thorax in two, and to both of theseareas in one case. An anatomic basis for thetransmission of the murmurs posteriorly tothe left in these cases was not apparent.
Jet lesions were identified in the left atriumill seven of the nine cases in which the ante-rior leaflet was the site of the ruptured chor-dae tendineae. The location in the atrial wallranged from the posteromedial atrial wall tothe lateral wall, being generally opposite thesite of incompetency of the anterior leaflet.The systolic murmurs were heard in other
areas in addition to the apex in seven of theiiine cases. The apical systolic murmur wastransmitted to the left axilla and posteriorportion of the left side of the thorax in two,to the left axilla alone in four, and to theposterior left portion of the thorax alone inone. Basal systolic murmurs were recorded infour cases in this subgroup of nine cases, butin two cases aortic stenosis was verified atriecropsy, while in two cases the aortic valvewas not stenotic.
51
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMUNDSON, CALLAHAN, EDWARDS
The findings relating particularly to thetransmission of the apical systolic murmurto the basal precordial areas in cases withrupture of chordae to the posterior leaflet,and those relating to the transmission of themurmurs posteriorly to the left in cases withrupture of chordae to the anterior leaflet,offer support to the theory that the transmis-sion of murmurs is related in part to the di-rection of regurgitant flow and possibly totlie impact of blood on the left atrial wall.The lack of complete correlation between thesites of rupture and the location of the jetlesions to the areas in which the murmurswere recorded in these cases suggests thatthere are other factors that were not apparent.Time of Rupture of Chordae Tendineae
The sudden appearance of a previously uni-recognized precordial systolic murmur hasbeen considered to be of significance in thediagnosis of ruptured mitral chordae tendin-eae.7 This situation, however, was not suffi-ciently well defined in any case in the presentstudy to provide evidence for ruptured chor-dae as the cause of the mitral insufficiency.It was impossible to determine the time ofappearance of the murmurs except in threeinstances in which a murmur was knownto have begun during active bacterial endo-carditis.In those cases in which heart murmurs were
known to be present prior to bacterial endo-carditis, there was no good evidence fordefinite or significant change of the murmursduring the bacterial endocarditis.Cardiac DecompensationThe sudden onset of cardiac decompensa-
tion or a sudden worsening of the state ofcardiac compensation has been noted pre-viously in patients with rupture of the mitralchordae tendineae.10 11 It has been postulatedthat this event may be temporally related tothe rupture. This phenomenon was present illtwo cases in the present study (cases 19 and20).
In these two cases the rapid and suddenappearance of symptoms and signs of cardiacdecompensation appeared 12 and 11 monthsprior to death, respectively. In one of them
(case 19) an apical systolic heart murmur wasnoted prior to this sudden appearance of fail-ure. The characteristics of the murmurs werenot significantly changed during the courseof this patient's illness.The clinical features of these two cases bear
certain resemblances to those of the cases ofspontaneous rupture of the mitral chordaetendineae reported by Horton-Smith,10 Froth-ingham and Hass,1" and one of the cases re-ported by Bailey and Hickam.7
Signs and symptoms of cardiac decompen-sation were present in 16 of 20 cases in thisstudy. In four cases cardiac decompensationwas minimal, and in each of these only one ortwo ruptured chordae were found. In the pa-tients in whom ruptured chordae were theprimary factors in the cardiac disability therewas a good correlation between the severityof the heart disease and the number of rup-tured chordae.
DiscussionBacterial endocarditis was the factor of
major etiologic importance in the cases inthis study. Of the 20 cases presented, bacterialendocarditis was known to be present duringlife in 10. In these cases necropsy showedthe infection to be active in six and healedin four. In the other 10 cases there was nohistory of bacterial endocarditis, but in threeof these there were findings at necropsy thatwere interpreted as those of healed bacterialendocarditis. In three additional cases nec-ropsy findings were less definite but never-theless suggestive of healed bacterial endo-earditis. In the remaining four cases residualabnormalities from inflammatory processes inthe heart were demonstrated but these changeswere not specific. Mitral insufficiency in pa-tients who have had bacterial endocarditismay be the result of one or of several abnor-malities in addition to rupture of the chordaetendineae. These include destruction of theleaflet tissue, fixation of the posterior leafletto the left ventricular wall by organized vege-tations, and distortion of the leaflets by largevegetations and enlargement of the mitralorifice.17 In the 20 cases of this study, ruptureof the chordae tendineae was the primaryfactor in mitral insufficiency in five.
Circulation, Volume XXIII, .Janmary 1.961
52
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
RUPTURED MITRAL CHORDAE TENDINEAE
The role of rheumatic endocarditis in theproduction of rupture of mitral chordae ten-dineae is not completely known. In some cases,rheumatic endocarditis predisposes to bacte-rial endocarditis even to the location of bac-terial vegetations on the valve-chordae com-plex. Cases were encountered in the presentseries in which the inflammatory changesobserved were suggestive of healed rheumaticendocarditis, and convincing evidence, eitherclinical or pathologic, could not be found forsuperimposed bacterial endocarditis. It isperhaps possible also that chordae tendineae,involved by rheumatic endocarditis, couldrupture spontaneously.
In the present series, the microorganismsresponsible for bacterial endocarditis werelargely streptococci of different varieties. Theantibacterial measures now available effect acure in a great many cases owing to strepto-cocci.2' In such cases little evidence mightremain at necropsy of previous bacterial endo-carditis. It seems possible that bacterial en-docarditis, whether clinically recognized ornot, could be responsible for rupture of mitralchordae tendineae and still not show pathog-nomonic evidence of its existence.Two cases in the present study (cases 19
and 20) and three reported previously,7 10 11suggest that rupture of chordae tendineae didnot occur during active inflammation. The twopatients in this series apparently were in goodhealth when dyspnea developed rather sud-denly after a period of unusually heavy exer-tion. Dyspnea initiated serious cardiac decom-pensation and these two patients died 11 and12 months later, respectively. It is postulatedthat the rupture of the chordae tendineaeoccurred near the time of onset of dyspnea.Rupture of mitral chordae tendineae might
be responsible for the production of new mur-murs. In the cases in this study, recognitionof the beginning of cardiac murmurs was nota useful clinical event. The principal diffi-culty in making the diagnosis of rupturedmitral chordae tendineae on a clinical basiswould seem to be in differentiating it fromother causes of mitral insufficiency. Rupturedmitral chordae tendineae as a cause of mitralinsufficiency might be suspected, but probablyCirculation, Volume XXIII, January 1.961
a definite diagnosis would be difficult or im-possible clinically. The appearance of mitralinsufficiency in association with bacterial en-docarditis or with a febrile illness which wasnot definitely identified, or in which the trans-mission of the murmur seemed to be in keep-ing with the anatomic varieties discussed pre-viously, should be considered suggestive. Re-cent surgical advances in the treatment ofmitral insufficiency have led to increased in-terest in the entire problem. A technic forsurgical correction of mitral insufficiency dueto ruptured mitral chordae has been describedby MeGoon.22 Fortunately it is not vital tomake this difficult specific diagnosis beforeexposing the mitral valve at the time of open-heart operation.
SummaryThe present study presents pertinent clin-
ical and pathologic findings in 20 cases ofruptured mitral chordae tendineae encoun-tered at the Mayo Clinic between 1934 and1958 inclusive. Mitral insufficiency resultsfrom the rupture of chordae tendineae, theseverity being related to the number of chor-dae ruptured. The resulting heart disease maybe severe and may progress to cardiac decom-pensation and death. Bacterial endocarditiswas the major etiologic factor in rupture ofthe chordae tendineae in this study.
References1. WASHBOURN, J. W.: A discussion on the path-
ology of infective endocarditis. I. Brit. M. J.2: 1269, 1899.
2. BRIGDEN, W., AND LEATHAM, A.: Mitral incoin-petence. Brit. Heart. J. 15: 55, 1953.
3. HEPPER, N. G. G., BURCHELL, H. B., AND EDWARDS,J. E.: Cardiac Clinic CXLVI. Mitral insuf-ficiency in healed, unrecognized bacterial endo-carditis. Proc. Staff Meet., Mayo Clin. 31:659, 1956.
4. SAPHIR, 0.: Endocarditis. In Gould, S. E.:Pathology of the Heart. Springfield, Ill.,Charles C Thomas, Publisher, 1953, p. 707.
5. LIBMAN, E., AND FRIEDBERG, C. K.: SubacuteBacterial Endocarditis. London, Oxford Uni-versity Press, 1941, 108 pp.
6. FREW, H. W. D.: Rupture of the chordae ten-dineae following scarlet fever. Glasgow M. J.115: 195, 1931.
7. BAILEY, 0. T., AND HICKAM, J. B.: Rupture ofmitral chordae tendineae: Clinical and path-ologic observations on 7 cases in which there
53
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
OSMUNDSON, CALLAHAN, EDWARDS
was no bacterial endocarditis. Am. Heart J.28: 578, 1944.
8. BARBER, H.: The effects of trauma, direct andindirect, on the heart. Quart. J. Med., n.s.,13: 137, 1944.
9. KAY, E. B., AND CROss, F. S.: Surgical treat-ment of mitral insufficiency. Surgery 37: 697,1955.
10. HORTON-SMITH, P.: A clinical lecture on mitralregurgitation. Clin. J. 19: 252, 1902.
11. FROTHINGHAM, C., AND HASS, G. M.: Ruptureof normal chordae tendineae of the mitralvalve. Am. Heart J. 9: 492, 1934.
1 2. ASKEY, J. M.: Spontaneous rupture of a papillarymuscle of the heart: Review with eight addi-tional cases. Am. J. Med. 9: 528, 1950.
13. CRADDOCK, W. L., AND MAHE, G. A.: Rupture ofpapillary muscle of heart following myocardialinfarction: Differential criteria from perfora-tion of interventricular septum. J.A.M.A. 151:884, 1953.
14. CORVISART, J. N.: An Essay on the OrganicDiseases and Lesions of the Heart and GreatVessels. (Translated by Jacob Gates.) Boston,A. Finley, 1812, 344 pp.
15. CLARK, A.: Lectures on Diseases of the Heart.Delivered at the College of Physicians andSurgeons, New York. New York, E. B. Treat,1887, 251 pp.
16. OSMUNDSON, P. J., CALLAHAN, J. A., AND
EDWARDS, J. E.: Mitral insufficiency fromruptured chordae tendineae simulating aorticstenosis. Proc. Staff Meet., Mayo Clin. 33:235, 1958.
17. EDWARDS, J. E., AND BURCHELL, H. B.: Path-ologic anatomy of mitral insufficiency. Proc.Staff Meet., Mayo Clin. 33: 497, 1958.
18. EDWARDS, J. E., AND BURCHELL, H. B.: Endo-cardial and intimal lesions (jet impact) aspossible sites of origin of murmurs. Circulation18: 946, 1958.
19. SHAPIRO, H. A., AND WEISS, D. R.: Mitralinsufficiency due to ruptured chordae tendineaesimulating aortic stenosis. New England J.Med. 261: 727, 1959.
20. MILLER, R., JR., AND PEARSON, R. J., JR.:Mitral insufficiency simulating aortic stenosis:Report of an unusual manifestation of Mar-fan's syndrome. New England J. Med. 260:1210, 1959.
21. GERACI, J. E.: The antibiotic therapy of bac-terial endocarditis: Therapeutic data on 172patients seen from 1951 through 1957: Addi-tional observations on short-term therapy (twoweeks) for penicillin-sensitive streptococcal en-docarditis. M. Clin. North America, July, 1958,p. 1101.
22. MCGooN, D. C.: Repair of mitral insufficiencydue to ruptured chordae tendineae. J. Thoracic& Cardiovas. Surg. 39: 357, 1960.
The area of the transverse section of the pulmonary artery being in one part, beforeit divaricates into branches, of the same dimension with the orifice of the aorta, thevelocity of the blood in that part may be accounted the same as in the orifice of theaorta. But though the quantities and velocities of the blood, in passing out of bothventricles, be the same, yet it does not thence follow, that their expulsive forces must beboth the same: for if the blood in passing into the pulmonary artery, finds less resistancefrom the preceding blood, than the blood does in entering into the aorta, then a lessforce will expel it out of the right ventricle with equal velocity; and accordingly, asthere is not so much force required to drive the blood thro' the lungs, as thro' the restof the whole body, so we may observe, that the substance of the muscle of the right ven-tricle has not near the thickness of that of the left.-STEPHEN HALES, B.D., F.R.S.,Haemastatics, Vol. II, London, 1733.
Circulation, Volume XXIII, January 1961
54
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

PHILIP J. OSMUNDSON, JOHN A. CALLAHAN and JESSE E. EDWARDSRuptured Mitral Chordae Tendineae
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1961 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.23.1.421961;23:42-54Circulation.
http://circ.ahajournals.org/content/23/1/42located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from