running head: early implementation of...
TRANSCRIPT

Running head: EARLY IMPLEMENTATION OF CAPSULE ENDOSCOPY Chambers 1
Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia:
A Cost-Benefit Analysis
Winde R. Chambers
Texas Woman's University

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 2
Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia:
A Cost-Benefit Analysis
Contact information: Winde R. Chambers, APRN, FNP
156 Kingston Road
Benton, Louisiana 71006
318-426-0774
Capsule endoscopy has revolutionized the diagnosis and management of iron deficiency
anemia and obscure gastrointestinal bleeding over the past decade. It allows visualization of
areas of the small bowel that are not reached with conventional endoscopic procedures. In 2005,
the International Conference on Capsule Endoscopy published a consensus statement that
delineates the use capsule endoscopy as part of the initial evaluation for patients with obscure
gastrointestinal bleeding (Pennazio, Eisen & Goldfarb, 2005). Regardless of this consensus,
initial evaluation with capsule endoscopy in patients without gross gastrointestinal bleeding is
debatable (Rockey, 2005). Standard management is often to treat with iron supplementation,
followed by observation and/or repeat endoscopy (Rockey, 2010). The purpose of this study is
to evaluate the efficacy of early intervention with capsule endoscopy compared to standard
management, using cost effectiveness and time to diagnosis as quality outcome measures for care
of patients with iron deficiency anemia related to obscure gastrointestinal bleeding.
Context
Iron deficiency anemia is most frequently caused by chronic occult gastrointestinal
bleeding in men and postmenopausal women therefore the standard of care is
investigation of the gastrointestinal tract (Rockey, 2010).

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 3
Obscure bleeding is characterized by bleeding that persists or recurs without
identification of a source on initial evaluation with esophagogastroduodenoscopy (EGD)
or colonoscopy (American Gastroenterological Association [AGA], 2007b).
Obscure occult bleeding is distinguished by patients with iron deficiency anemia and
documented evidence of positive fecal occult blood test and obscure overt bleeding is
differentiated by recurrent melena, hematemesis or hematochezia (Rockey, 2010).
OGIB represents approximately 5% of all gastrointestinal bleeding with small bowel
sources identified in 75% of these cases (AGA, 2007a).
Capsule endoscopy has a positive impact on health outcomes, although evidence is
lacking regarding outcomes of interventions following capsule endoscopy (AGA, 2007b).
It has been estimated that the average cost associated with diagnosing obscure
gastrointestinal bleeding is $33,630 (Goldfarb, Phillips, Conn, Lewis & Nash, 2002),
however more recent literature asserts that these figures are significantly underestimated
(AGA, 2007b). Diagnosing the cause of obscure gastrointestinal bleeding may take a
significant amount of time which contributes to substantial medical cost (AGA, 2007b).
It takes from one month to eight years to diagnose patients with obscure gastrointestinal
bleeding with a median of two years (AGA, 2007b).
Medicare and private insurers require documentation of normal EGD and colonoscopy
within six months to one year prior to capsule endoscopy approval (AGA, 2007b).
Project Description
Goal/Objectives
The goal of this clinical inquiry is to investigate the efficacy of early capsule endoscopy
compared to conventional diagnostic evaluation based on cost effectiveness for patients with iron

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 4
deficiency anemia. Objectives include (a) developing a timely and cost effective practice
protocol for the management of patients with iron deficiency anemia; (b) and increasing
available evidence to support the development of a clinical practice guideline.
Research Question
The research question guiding this project is: What is the efficacy of early
implementation capsule endoscopy compared to conventional diagnostic evaluation for cost
effective care management in patients diagnosed with iron deficiency anemia? The intervention
is conceptually defined as the diagnostic approach for identifying the source of obscure
gastrointestinal bleeding and operationally defined as early implementation of capsule endoscopy
(immediate use following initial non-definitive scopes) compared to conventional diagnostic
evaluation (trial of iron therapy, repeated endoscopy). The conceptual definition for the outcome
variable is cost effective care management operationally defined as incurred procedural cost and
time between initial and problem resolution.
Methodology
A retrospective chart review of patients diagnosed with iron deficiency anemia will be
conducted in order to answer the proposed research question. Patients evaluated for iron
deficiency anemia from April 2007 to April 2008 will be identified data collected in the practice
electronic medical record (EMR). Inclusion criteria include men and postmenopausal women
ages 50 to 70 diagnosed with iron deficiency and obscure gastrointestinal bleeding. Patients
with history of gastric bypass, cases involving obscure overt gastrointestinal bleeding and those
with contraindications for capsule endoscopy will be excluded. Premenopausal women with
documentation of abnormal menstrual bleeding will be eliminated from the study. The
intervention group will be defined as patients diagnosed with iron deficiency anemia who

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 5
underwent capsule endoscopy within 6 months of initial EGD and colonoscopy. The
conventional group will be defined as patients diagnosed with iron deficiency anemia that did not
have capsule endoscopy following normal EGD and colonoscopy (Appendix C).
Data collection tools (Appendix E) developed by the researcher will be used to collect
anonymous data from the patients' medical records. Demographics and pre-procedure
hemoglobin, mean corpuscular volume, serum iron, total iron binding capacity will be recorded
for both groups. Results of fecal occult blood testing and prior blood transfusions will be
documented if available. Information regarding use of non- steroidal anti-inflammatory drugs,
antiplatelets and anticoagulants will be obtained for both groups. For the intervention group,
capsule endoscopy date, findings and recommendations will be recorded. Follow-up laboratory
data and clinical outcomes will be recorded. A positive outcome will be defined as identification
of the source of bleeding and/or resolution of anemia. A negative outcome will be defined as
retained capsule, persistent anemia and/or no definite source of bleeding identified on capsule
endoscopy. For the conventional group, the length of time from negative EGD and colonoscopy
to date of symptoms resolution or capsule endoscopy will be recorded. The number of
endoscopic procedures, radiological images, follow-up visits, laboratory test (including CBC,
iron studies) and blood transfusions between these dates will be collected.
Timeline and Duration
The study is projected to last approximately six months. An exempt application will be
submitted to the Texas Woman's University (TWU) Institutional Review Board in September
2010. The written document will be submitted to the capstone committee by March 2011.
Specific dates and activities are illustrated in Table 1.

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 6
Table 1
Projected Timeline
Date Activity
September 1-31, 2010 TWU IRB approval
October 1-7, 2010 Educate data collectors
October 8- November 31, 2010 Data collection
December 1-31, 2010 Statistical analysis
January 1- March 15, 2011 Complete project/paper
Sites, Support and Personnel Required for Project
The study will be conducted a private gastroenterology practice in the Southern United
States. No financial support will be needed from the practice. The researcher will require
assistance from the health information manager at the practice to obtain the sample from the
EMR. The researcher will be responsible for data collectors and statistician.
Deliverables to Institution
The results of the study will be discussed with the health care providers and personnel at
the gastroenterology practice. These findings will aid in the development of a timely and cost
effective practice protocol for the management of patients with iron deficiency anemia. A copy
of the written documented will be provided by the researcher.
Benefits/Anticipated outcomes
Findings from this study will increase available evidence to support the development of
clinical practice guidelines. The placement of capsule endoscopy immediately after
conventional endoscopic evaluation in diagnostic algorithms for iron deficiency anemia will be
beneficial for all stakeholders. Patients will reduce losses in productivity and quality of life as

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 7
evident by decreasing time off from work for unwarranted testing and preparation for
endoscopic procedures. Providers will improve diagnostic precision and enhance patient
satisfaction in care provided.

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 8
References
American Gastroenterological Association Institute. (2007a). American Gastroenterological
Association Institute medical position statement on obscure gastrointestinal bleeding.
Gastroenterology, 133, 1694-1696. doi:10.1053/j.gastro.2007.06.008
American Gastroenterological Association Institute. (2007b). American Gastroenterological
Association Institute technical review on obscure gastrointestinal bleeding.
Goldfarb, N., Philips, A., Conn, M., Lewis, B., & Nash, D. (2002). Economic and health
outcomes of capsule endoscopy: Opportunities for improved management of the
diagnostic process for obscure gastrointestinal bleeding. Disease Management, 5(3), 123-
135.
Pennazio, M., Eisen., & Goldfarb, N. (2005). ICCE consensus for obscure gastrointestinal
bleeding. Endoscopy, 37, 1046-1050.
Rockey, D. (2005). Occult gastrointestinal bleeding. Gastroenterology Clinics of North America,
31, 699-718. doi: 10.1016/j.gtc.2005.08.010
Rockey, D. (2010). Occult and obscure gastrointestinal bleeding: causes and clinical managment.
Natures Reviews: Gastroenterology and Hepatology, 7(5), 265-279. doi:
10.1038/nrgastro.2010.42

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 9
Appendix A
August 7, 2010
156 Kingston Road
Benton, Louisiana 71006
GastroIntestinal Specialist, AMC
3217 Mabel Street
Shreveport, Louisiana 71103
Attn: Linda Ray, Administrator
Dear Mrs. Ray:
As you know, I am currently pursuing my Doctor of Nursing Practice degree at Texas Woman's
University and will be starting my professional capstone project in September. I am seeking
approval to conduct a retrospective chart review in order to determine the efficacy of early
capsule endoscopy in patients with iron deficiency anemia. The practice has performed
thousands of capsule endoscopies since the development of this innovative diagnostic tool.
Findings from this study will contribute to the delivery of high quality gastroenterology
endoscopic services in an professional and cost effective manner.
I have attached my concept paper that describes elements of the proposed research.
If any other information is needed you can contact me by phone at (318) 426-0774 or email at
Sincerely,
Winde R. Chambers, APRN, FNP-BC

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 10
Appendix B
Research Project Overview
Research Questions and Hypothesis
Research Question: What is the efficacy of early implementation capsule endoscopy
compared to conventional diagnostic evaluation for cost effective care management in
patients diagnosed with iron deficiency anemia?
PICO Question: In patients with iron deficiency anemia, is early implementation of capsule
endoscopy more cost effective than conventional diagnostic evaluation?
Null Hypothesis: There is no difference in cost of early implementation of capsule endoscopy
compared to conventional diagnostic evaluation in patients diagnosed with iron deficiency
anemia.
Proposed Statistical Analysis of Project
Simple frequencies will be obtained on demographics such as age, gender, ethnicity as
well as capsule endoscopy findings and recommendations.
Chi-square test for independence or the Fisher's Exact Probability Test will be used in
order to explore the relationship between categorical variables. For example, the
relationship between interventions based on capsule endoscopy findings and clinical
outcomes will be examined.
Cost-Analysis

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 11
Appendix C
Sample
IDA Exclude Patients with:
Overt GI bleeding
History gastric bypass
Capsule endoscopy contraindicated
Pre-menopausal women
EGD/Colon
(Negative
findings)
Exclude:
EGD/Colon
positive findings
Intervention
Group:
Capsule endoscopy
within 6 months
Conventional
Group:
Second look
iron trial

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 12
Appendix D
SPSS Code Book
FULL VARIABLE NAME SPSS VARIABLE NAME CODING INSTRUCTIONS
Identification number
ID Number assigned to each subject. Last four numbers of subjects’ medical record number.
Group Group 1= Intervention group 2=Conventional group
Age Age Age in years Gender Gender 1= Male 2= Female Ethnicity Ethnicity 1=White/Caucasian
2= Black/African American 3= Asian 4=Hispanic 5= American Indian 6= Not indicated
Hemoglobin HgB Total in grams/dl Mean corpuscular volume MCV Total in femtoliters/cell Serum iron Iron Total in nanograms/ml Total iron binding capacity TIBC Total in ng/ml Ferritin Ferritin Total in ng/ml Fecal occult blood test FOBT 1= Negative
2= Positive 3= Not available
Blood transfusion Blood 1= No 2= Yes
Medications Medications 1= No risk medications 2= NSAIDS 3= Plavix 4= Coumadin
Capsule endoscopy findings CE findings 1= Normal 2= AVM/Angiodysplasia 3=Tumor 4= Stricture 5= Ulcer 6= Erosion
Complications Complication 1= No complications 2= Capsule failure 3= Retained capsule
Recommendations Recs 1= Monitor laboratory data/CBC 2= Medication 3= Endoscopy 4= Surgery
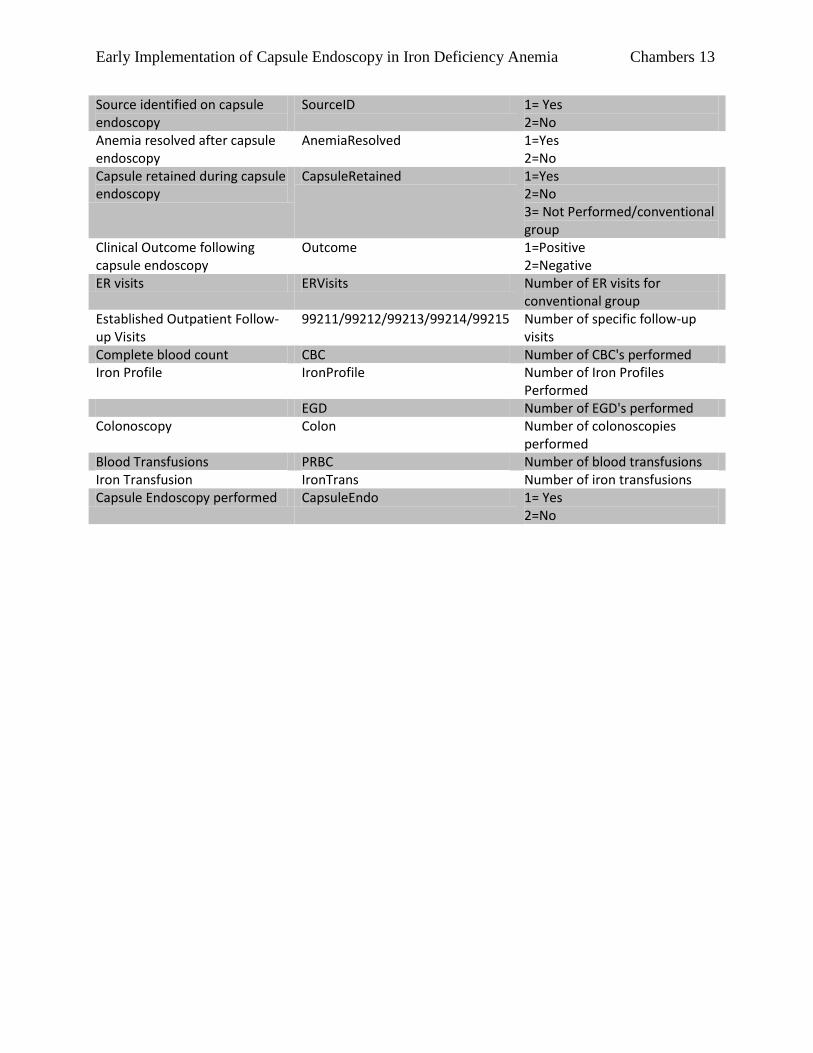
Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 13
Source identified on capsule endoscopy
SourceID 1= Yes 2=No
Anemia resolved after capsule endoscopy
AnemiaResolved 1=Yes 2=No
Capsule retained during capsule endoscopy
CapsuleRetained 1=Yes 2=No 3= Not Performed/conventional group
Clinical Outcome following capsule endoscopy
Outcome 1=Positive 2=Negative
ER visits ERVisits Number of ER visits for conventional group
Established Outpatient Follow-up Visits
99211/99212/99213/99214/99215 Number of specific follow-up visits
Complete blood count CBC Number of CBC's performed Iron Profile IronProfile Number of Iron Profiles
Performed EGD Number of EGD's performed Colonoscopy Colon Number of colonoscopies
performed Blood Transfusions PRBC Number of blood transfusions Iron Transfusion IronTrans Number of iron transfusions Capsule Endoscopy performed CapsuleEndo 1= Yes
2=No

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 14
Appendix E
Data Collection Tools

Early Implementation of Capsule Endoscopy in Iron Deficiency Anemia Chambers 15