rotational atherectomy - livemedia.gr · rotational atherectomy. ... the correct choice of...
TRANSCRIPT

GRAIDIS CHRISTOS Interventional Cardiologist, FSCAI
Euromedica- Kyanous Stavros Thessaloniki
Rotational Atherectomy

Expansion of PCI indications to more challenging anatomic settings as a consequence of the improved restenosis rate following drug-eluting stents
*as reported to NHLBI Dynamic Registry. Bortnick, et. al. Am J Cardiol 2014;113:573-579.
Increasing Complexity and Calcification of PCI Patients
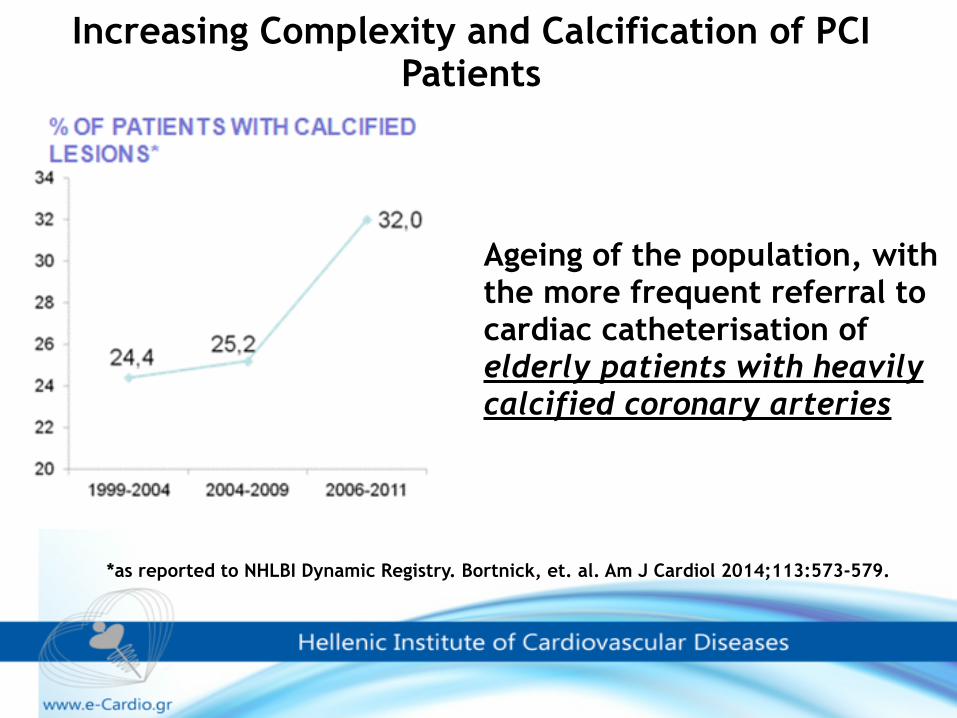
Ageing of the population, with the more frequent referral to cardiac catheterisation of elderly patients with heavily calcified coronary arteries
Increasing Complexity and Calcification of PCI Patients
*as reported to NHLBI Dynamic Registry. Bortnick, et. al. Am J Cardiol 2014;113:573-579.

✓The correct choice of equipment can make a complex intervention appear effortless,
✓whereas the less appropriate equipment choices can make a straightforward intervention, laborious and challenging.
Can we have the right tool to do the job ?A thorough knowledge of the basic angioplasty equipment is
required for coronary intervention.

Despite the development of more supportive catheters, very low profile balloons with higher inflation pressure facility, and alternative plaque modifying technology, the crossing of a heavily calcified lesion might require rotational atherectomy
ROTABLATOR: A qualified weapon in the fight against challenging coronary artery lesions

David Auth first described rotational ablation in 1986 as a technique for winding up coronary thrombus at low rotational speeds, thus capturing it on the rotating burr and shaft.
So what has happened since the introduction of rotational ablation?
We began with great enthusiasm……

Initial interest in its use dwindled following trials showing high restenosis rates
but it has undergone a resurgence of interest
The Dark Side of Adjunctive Rotational Atherectomy
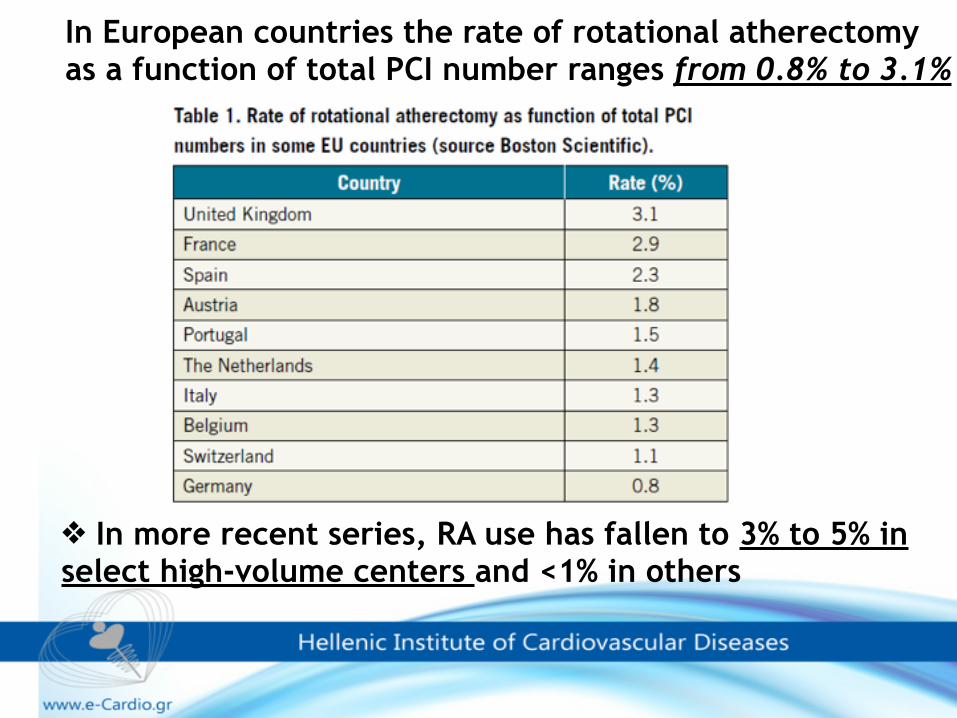
In European countries the rate of rotational atherectomy as a function of total PCI number ranges from 0.8% to 3.1%
❖ In more recent series, RA use has fallen to 3% to 5% in select high-volume centers and <1% in others
Universal adoption of this technique has been hampered by: •concern about the complexity of the rotablator procedures and potential procedure-related complications, •lack of standardised protocols, •lack of structured and widely available training programmes.
The Dark Side of Adjunctive Rotational Atherectomy
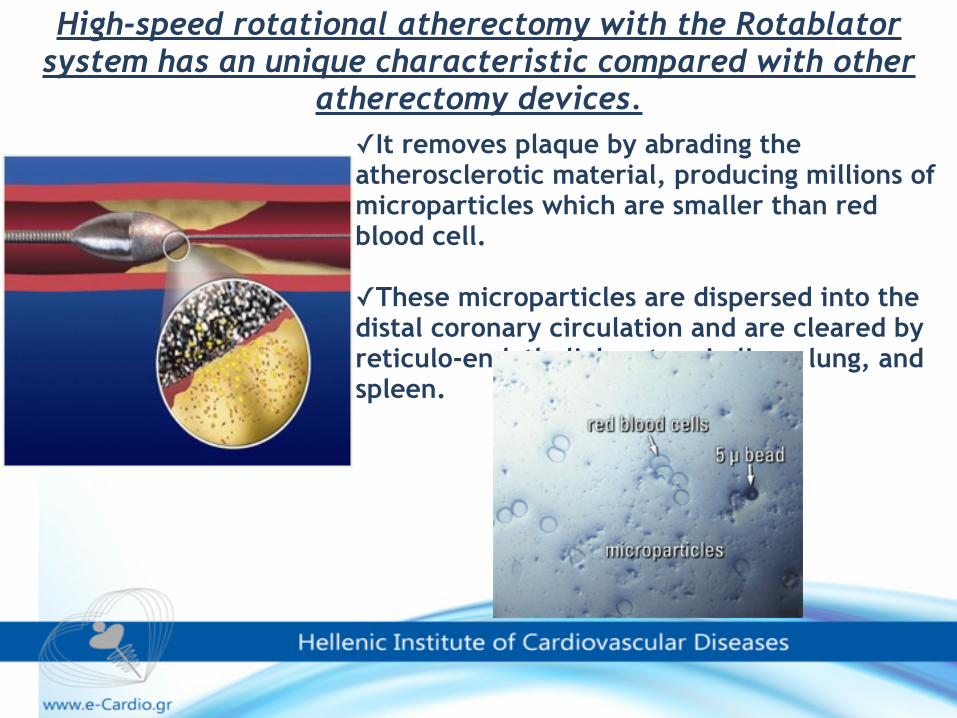
✓It removes plaque by abrading the atherosclerotic material, producing millions of microparticles which are smaller than red blood cell.
✓These microparticles are dispersed into the distal coronary circulation and are cleared by reticulo-endothelial system in liver, lung, and spleen.
High-speed rotational atherectomy with the Rotablator system has an unique characteristic compared with other
atherectomy devices.
5 Micron Bead

According to this principle, the burr preferentially abrades hard and even calcified atherosclerotic plaque while
deflecting the normal tissue, which is soft and elastic.
Helpful analogies: Shaving A nail file
Direction of motion Direction of motion
Elastic tissue deflects out of the way
Forceful mechanical breakdown of matter
Differential cutting means the ability to remove hard (inelastic) tissue while sparing soft (elastic) tissue which can deflect away
from the advancing rotating abrasive burr.
Differential atherectomy
✓Friction is minimized by a sliding motion perpendicular or orthogonal to the contact surface
✓The faster something is turned the more the friction is reduced
Provides easy passage of the burr through tortuous and diseased segments of the coronary tree.
Removal of cork from wine bottle. If a cork is twisted as it is pulled , the friction is reduced and the cork can be withdrawn easily
Helpful analogies Removing a cork from a champagne bottle Taking a ring off a finger
Orthogonal displacement of friction
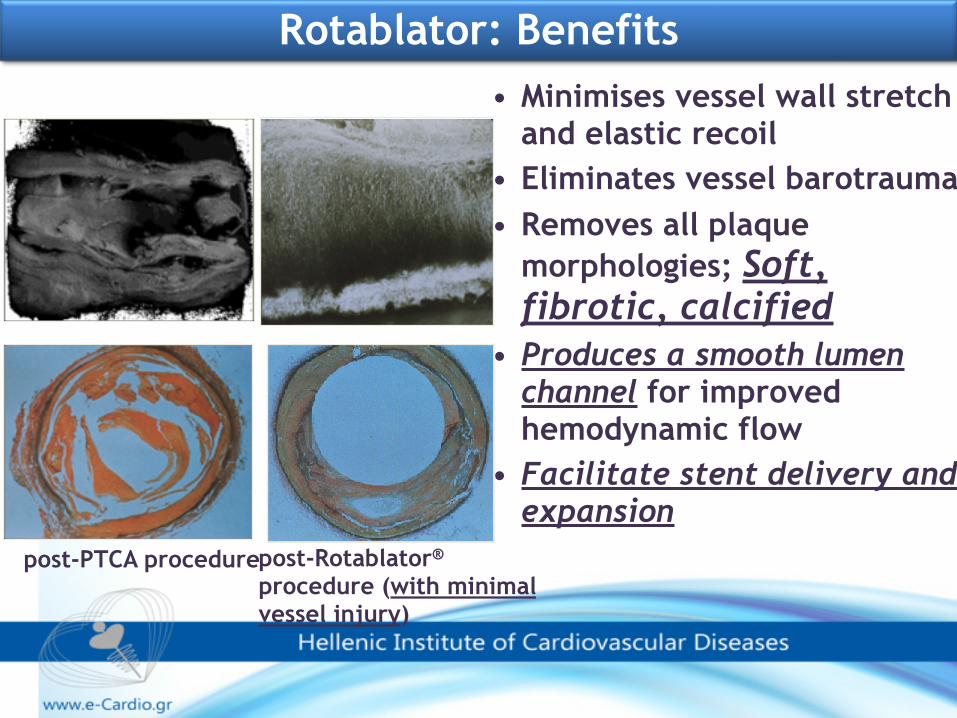
• Minimises vessel wall stretch and elastic recoil
• Eliminates vessel barotrauma • Removes all plaque
morphologies; Soft, fibrotic, calcified
• Produces a smooth lumen channel for improved hemodynamic flow
• Facilitate stent delivery and expansion
post-PTCA procedurepost-Rotablator® procedure (with minimal vessel injury)
Rotablator: Benefits

DynaGlide™ foot pedalConsole
Compressed air or nitrogen
Tank, regulators, attachments
Hardware Components Overview
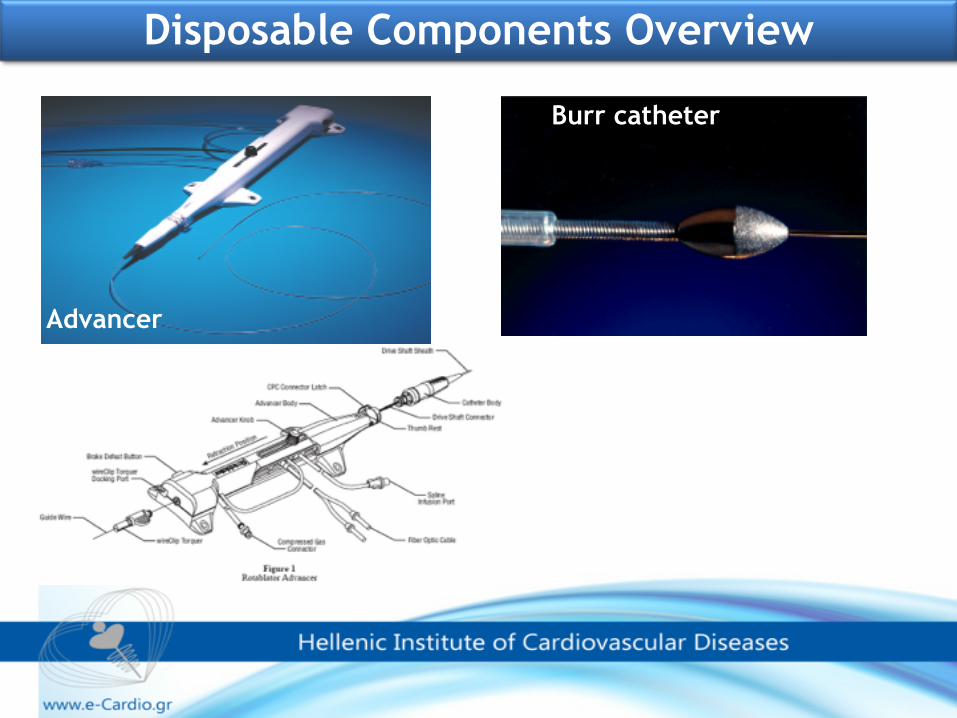
Burr catheter
Advancer
WireClipTM Torquer & Guidewires
Disposable Components Overview
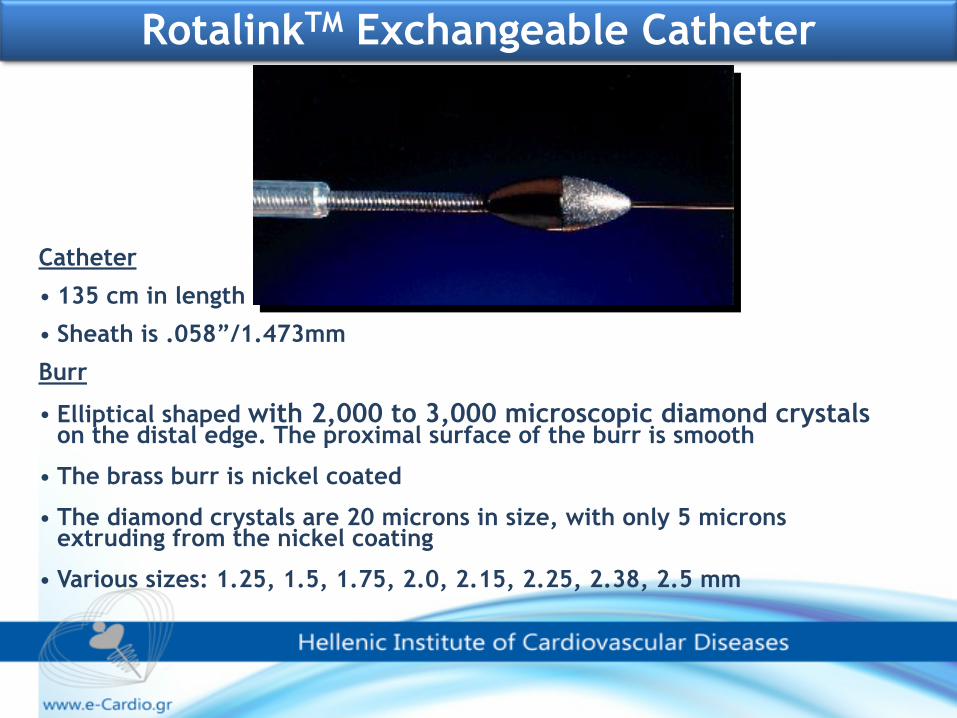
Catheter
• 135 cm in length
• Sheath is .058”/1.473mm
Burr
• Elliptical shaped with 2,000 to 3,000 microscopic diamond crystals on the distal edge. The proximal surface of the burr is smooth
• The brass burr is nickel coated
• The diamond crystals are 20 microns in size, with only 5 microns extruding from the nickel coating
• Various sizes: 1.25, 1.5, 1.75, 2.0, 2.15, 2.25, 2.38, 2.5 mm
RotalinkTM Exchangeable Catheter
•modification of a plaque
•improving the plaque and vessel compliance
•better performing PCI in difficult situations
Rotablator has been newly re-defined as a tool for:

✓Guide catheter selection
✓Rota-wire
✓RA protocols
✓D.R.A.W. – Pre Procedure
Test
✓Burr positioning
✓Ablating Technique
✓Other issues
✓Complications
▪Burr entrapment
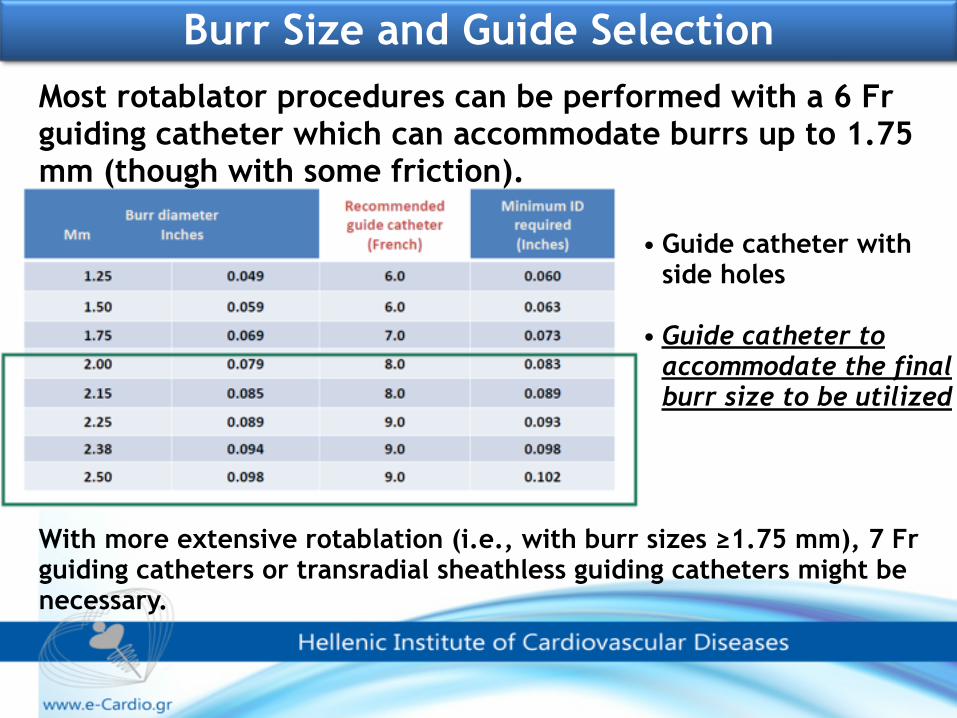
Burr Size and Guide SelectionMost rotablator procedures can be performed with a 6 Fr guiding catheter which can accommodate burrs up to 1.75 mm (though with some friction).
With more extensive rotablation (i.e., with burr sizes ≥1.75 mm), 7 Fr guiding catheters or transradial sheathless guiding catheters might be necessary.
• Guide catheter with side holes
• Guide catheter to accommodate the final burr size to be utilized

Single curve guiding catheters, i.e., EBU, XB or Judkins catheters, might be associated with less friction and resistance to the burr passage in the proximity of the tip of the catheter.
Burr Size and Guide Selection
Recommended Curves*
* Avoid abrupt primary and secondary curves.
Guide catheter that provides coaxial engagement will reduce unfavorable
guidewire bias
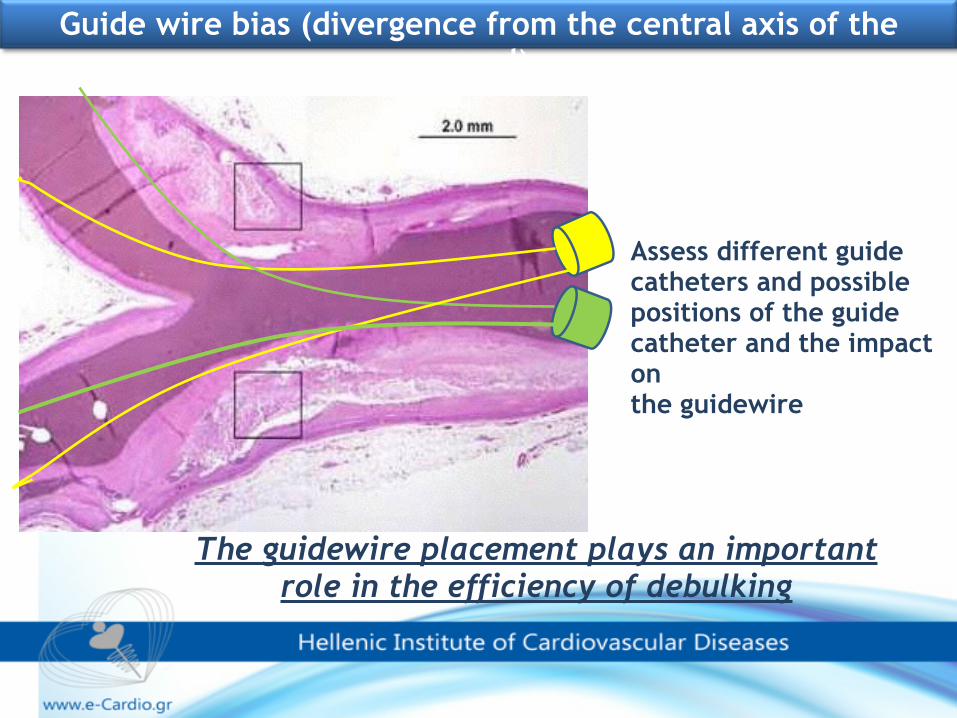
The guidewire placement plays an important role in the efficiency of debulking
Assess different guide catheters and possible positions of the guide catheter and the impact on the guidewire
Guide wire bias (divergence from the central axis of the vessel)
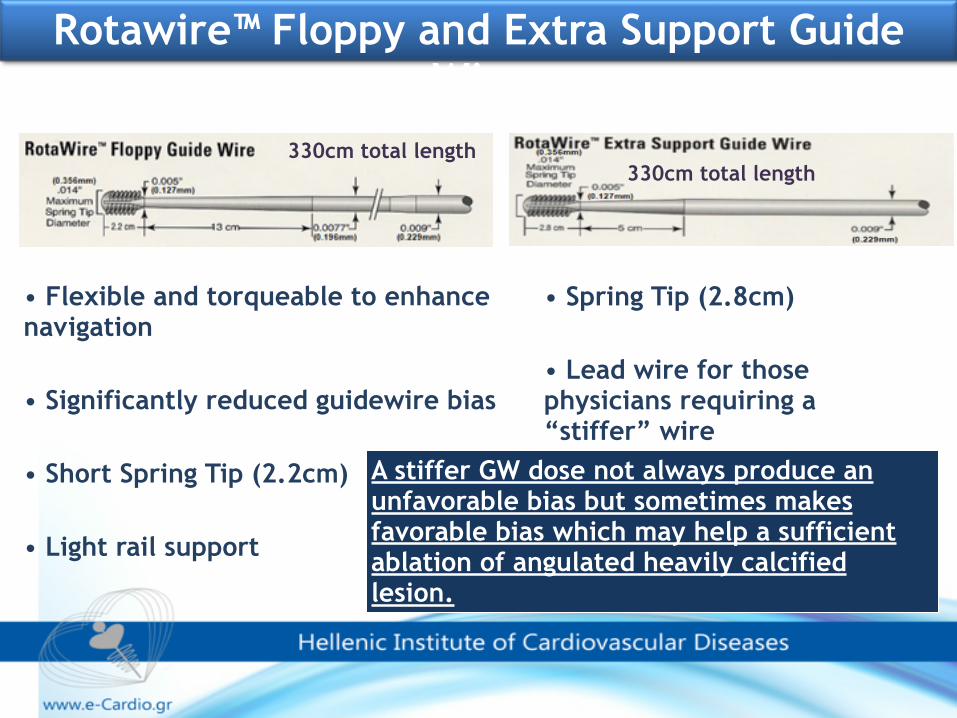
• Flexible and torqueable to enhance navigation
• Significantly reduced guidewire bias
• Short Spring Tip (2.2cm)
• Light rail support
330cm total length
• Spring Tip (2.8cm)
• Lead wire for those physicians requiring a “stiffer” wire
330cm total length
Rotawire™ Floppy and Extra Support Guide Wire
A stiffer GW dose not always produce an unfavorable bias but sometimes makes favorable bias which may help a sufficient ablation of angulated heavily calcified lesion.

In cases where the rotawire cannot be advanced, past the lesion a conventional angioplasty wire with an exchange microcatheter or an over-the-wire balloon can be used. The rotawire can be advanced and positioned distally.
*** Finish the intervention on a normal wire
Use more frequently microcatheters for wire exchange
The rotawire is notoriously fickle in its performance as a standalone coronary guidewire.

• Visual • Smooth advancement under fluoroscopy • Contrast injection to discern lesion contours and borders
• Auditory • Pitch changes relative to resistance encountered by burr
• Tactile • Advancer knob resistance • Excessive drive shaft vibration: excessive load on burr
advanced too rapidly
Feedback During Ablation
Proper: Slow/Smooth/ShortAblating Technique

ROTATIONAL ATHERECTOMY PROTOCOLS
What is my concept of “rotablating a lesion”
To debulk plaque?
or
To modify plaque?

Different protocols for rotational atherectomy have been investigated in an attempt to obtain the highest acute and at long-term success rate with the lowest risk of procedural complications
Particular attention has been paid to:
➢Burr size (burr to artery ratio)
➢Rotablation speed
➢Motion pattern of the burr
ROTATIONAL ATHERECTOMY PROTOCOLS

500 patients
Routine Burr/artery ratio of 0.70 -
0.75 Adjunctive PTCA ≥ 4 ATM
Routine strategy (plaque modification) is better than aggressive debulking.
Results: Routine AggressiveProcedural results: Max. Burr size (mm) Burr/artery ratio Burrs used
1.8mm 0.71 1.9
2.1mm 0.82 2.7
Acute results: final MLD residual stenosis clinical success CK-MB rise >5 x nl
1.97 26%
93.5% 7%
1.95mm 27%
93.9% 11%
6 month results: TLR MLD loss index angiographic restenosis
22% 1.26mm
0.54 52%
31% 1.16mm
0.62 58%
Agresive Burr/artery ratio of 0.80 -
0.85 with or without ≤ 1 ATM
PTCA
STRATAS Study To Determine Rotablator And Transluminal Angioplasty Strategy

There has been a shift in the thinking about burr size as the technology has altered from a debulking tool to one that modifies plaque.
Size and number of burrs
burr/vessel ratio that does not exceed 0.6-0.7
➢Bigger burrs may debulk more of the lesion but they also may damage/activate more blood cells.
➢Starting with smaller burrs reduces the plaque burden to the distal bed and a patent lumen is achieved in a shorter period of time
➢Commonly, a single 1.5 mm burr represents a good compromise to tackle different lesion characteristics, achieving good plaque modification, i.e., burr-to-artery ratio of 0.6, while respecting budget constraints.
➢Nevertheless, a step-up approach starting with a 1.25 mm burr up to 1.5 mm (often) and to 1.75 mm (seldom) burr might represent a safer approach (aiming at a burr/vessel ratio that does not exceed 0.6-0.7).
➢However sometimes a single small burr is sufficient.
Step-up burr approach vs. single burr approach
Size and number of burrs
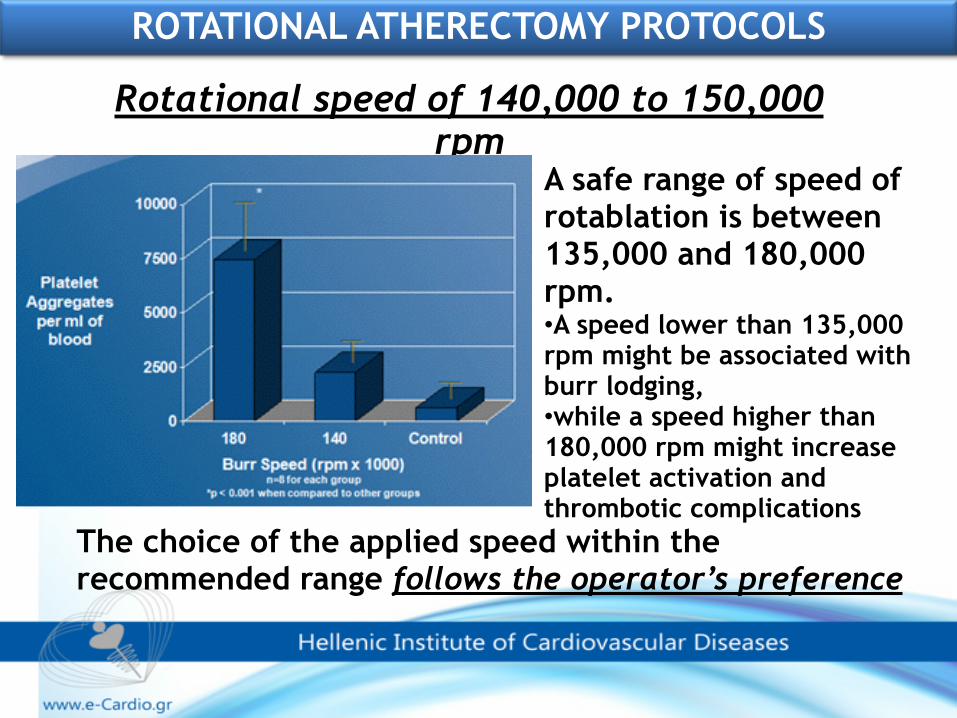
A safe range of speed of rotablation is between 135,000 and 180,000 rpm. •A speed lower than 135,000 rpm might be associated with burr lodging, •while a speed higher than 180,000 rpm might increase platelet activation and thrombotic complications
Rotational speed of 140,000 to 150,000 rpm
The choice of the applied speed within the recommended range follows the operator’s preference
ROTATIONAL ATHERECTOMY PROTOCOLS
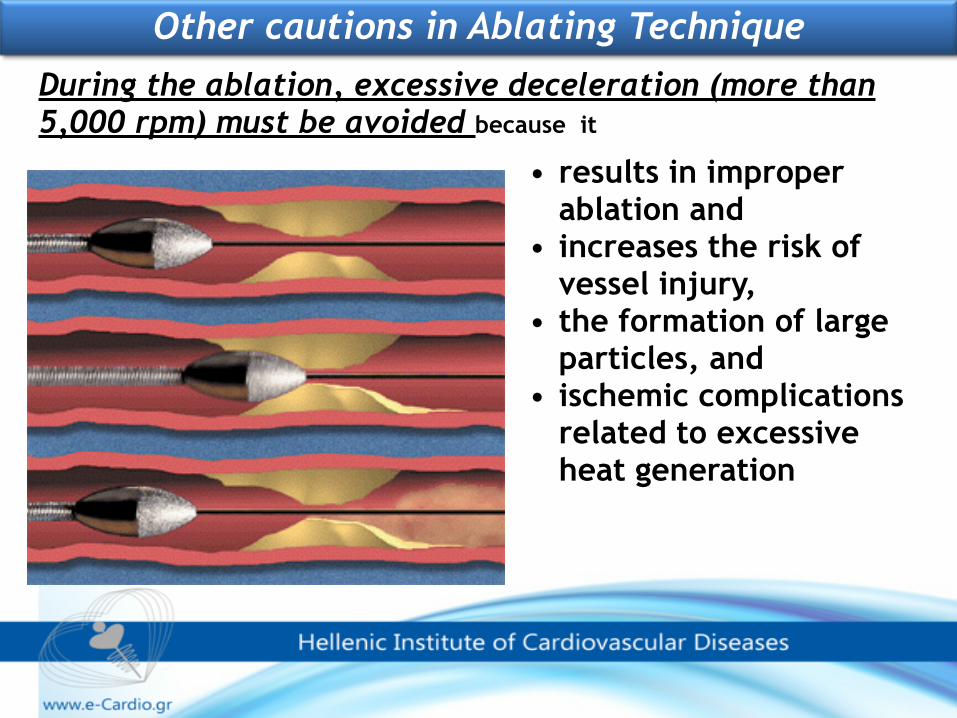
• results in improper ablation and
• increases the risk of vessel injury,
• the formation of large particles, and
• ischemic complications related to excessive heat generation
Other cautions in Ablating Technique
During the ablation, excessive deceleration (more than 5,000 rpm) must be avoided because it
Motion pattern of the burr
Do not push the rotablator into the lesion
Use “Pecking” technique i.e., a quick push-forward/pull-back
movement of the burr
(avoiding crossing the entire lesion during the initial passage)
Time of runs 15-20“ (no longer than 30 seconds)
Intermittent pull back for coronary perfusion and/or contrast injection

✓If, after several passes of the burr, it becomes clear that the lesion cannot be crossed, downsizing of the burr is recommended.
✓If the smallest burr will not pass, then consider a change to a more supportive, or even larger French, guiding catheter.
✓Usually, with patience, the majority of lesions will be crossed, but occasionally one has to accept there are cases which this technology is unable to penetrate.
When to stop rotational atherectomy?
When to stop rotational atherectomy?
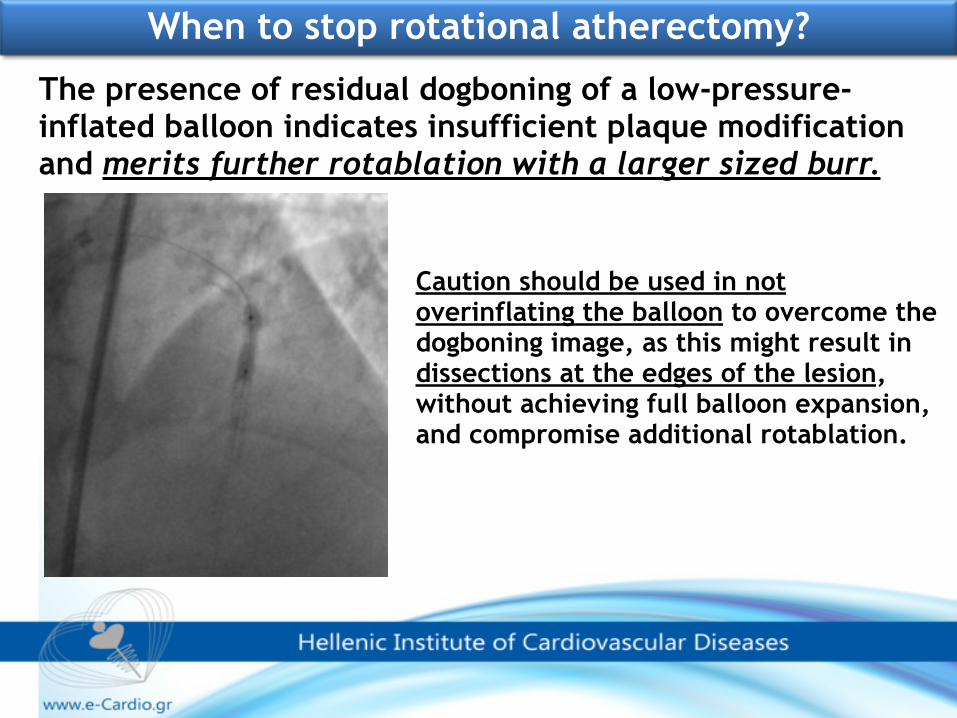
Caution should be used in not overinflating the balloon to overcome the dogboning image, as this might result in dissections at the edges of the lesion, without achieving full balloon expansion, and compromise additional rotablation.
The presence of residual dogboning of a low-pressure-inflated balloon indicates insufficient plaque modification and merits further rotablation with a larger sized burr.
35
CARAFE STUDY PILOT Cocktail Attenuation of Rotational Ablation Flow Effects
Virtually eliminates “Slow Flow” and “No-Reflow” phenomenon when used with current technique
modification:
USE RotaFlush
During RotA, 500 ml of heparinised (5000 units) normal saline solution with 5 mg verapamil and 1000 µg nitroglycerine is administered locally, with a view cool the rotablator turbine and to flush the coronary circulation from debris generated during the ablation ( preventing thrombus formation and vascular spasm, and avoiding the no-reflow phenomenon).
ROTAFLUSH - “COCKTAIL”
✓Transient AV blocks might occur during rotablation of the right coronary or dominant left circumflex artery. In this case, positioning a temporary pacemaker before rotablation might preclude complications, though it should be carefully performed.
✓There are few data to support the routine use of glycoprotein IIb/IIIa inhibitors, which should only be considered in bail-out situations.
✓Promising new platelet inhibitors (prasugral and ticagrelor) have demonstrated a superior pharmacological and clinical profile than clopidogrel and might be more effective alternative in preventing platelet activation induced by rotational atherectomy
Other issues in Rotational Atherectomy

The Rotablator is mainly used to improve procedural success rate in
heavily calcified lesions
In heavily calcified lesions procedural success rate with RA ranges from 93.4% to 98.6%, superior to rates reported separately in the absence of preceding plaque modification

Calcified Lesions
Can somebody help me?
Calicified Lesions: in the absence of plaque modification, confers an increased
✓likelihood of procedural failure,
✓stent underdeployment,
✓restenosis, and
✓major complications

Rotablator Enables You To Treat Calcified Vessels Effectively and facilitates GREAT RESULTS

Device Synergy
DES• Plaque compression • Scaffolding support • Prevents elastic recoil • Achieves larger MLD • Smooth lumen • Suppress neointimal proliferation
Rotational Atherectomy• Pulverizes plaque • Effective in calcified lesions • Changes lesion compliance • Decreases plaque shifting
Rota-DES
• Full stent expansion and deployment • Decrease subacute thrombosis • Better MLD • Decrease restenosis and TLR
Theoretically, RA and DES could act synergistically in complex lesions

MACE 6.8-30.1% TVR 3.3-25% ST 0.8-4.2%

However it should be emphasized that any reduction of restenosis might well have resulted from DES
platform alone , while Rotablator may only contributed by allowing stent delivery and proper deployment

Controversy exists over whether rotablation should be performed due to the presence of severe calcifications in the coronary angiogram (primary rotablation) or only after failed conventional coronary intervention
(secondary rotablation).
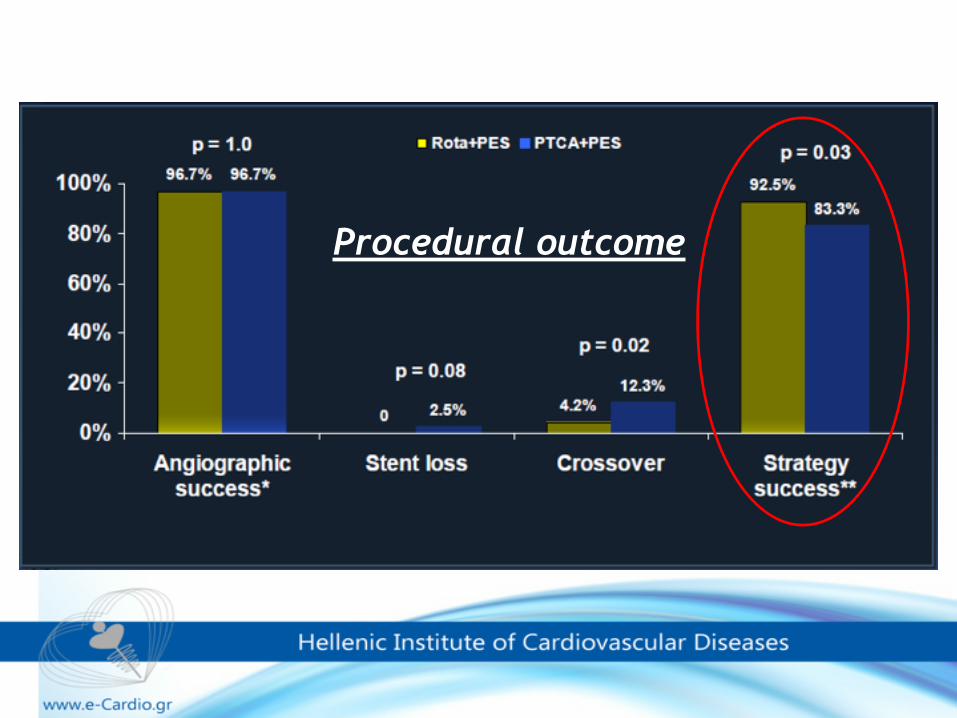
Procedural outcome



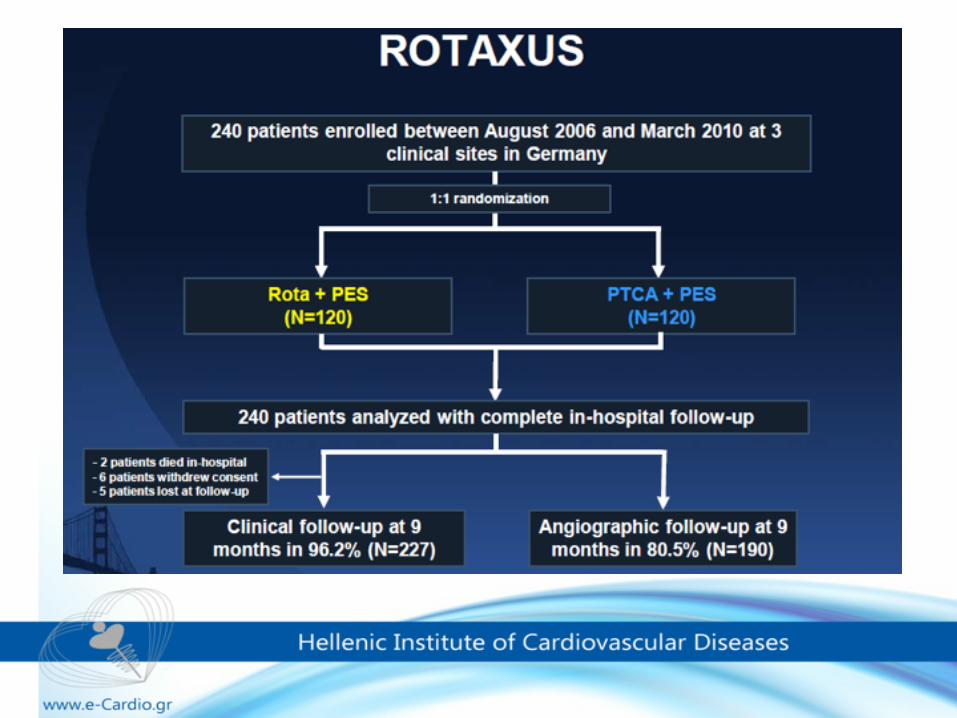
✓A strategy of balloon dilation with provisional rotablation before stenting should remain the default strategy for complex fibrotic/calcified lesions in the DES era.
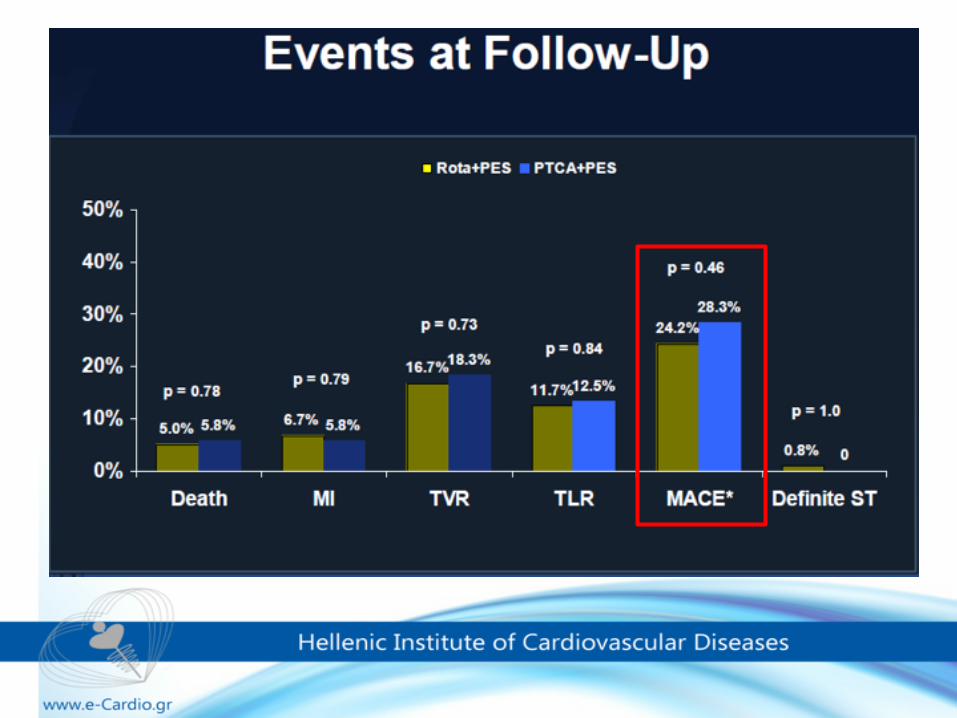
✓Although routine RA did not improve DES efficacy, RA remains an important tool for uncrossable or undilatable lesions and improves overall procedural success in this setting.
ROTAXUS-CONCLUSIONS

Rotational atherectomy of severely calcified coronary artery lesions: experience at Zurich University Hospital
Marietta Puck, Charlotte Regli, Stefan Toggweiler, Thomas F. Lüscher, Nils Kucher Cardiovascular Centre, University Hospital Zurich
In patients with failed conventional intervention rotablation is feasible and associated with periprocedural complications and clinical outcomes at 6 months
similar to those for primary rotablation.

Rotablation is recommended for preparation of heavily calcified or severely fibrotic lesions that cannot be crossed by a balloon or adequately dilated before planned stenting

Although routine use of rotational atherectomy did not improve outcomes after DES, such a device might technically be required in cases of tight and calcified lesions, to allow subsequent passage of balloons and stents. There is a resurgence in the use of rotational atherectomy for the purpose of optimal lesion preparation among patients undergoing implantation of bioresorbable stents.
Rota-Rescue defined as Rotational Atherectomy for:
✓Inability to cross the lesion with the balloon ✓Inability to completely inflate the balloon
✓Inability to deliver a stent
Can we with DES and balloons alone?
✓Failure to cross with a balloon is a well recognised cause of failure to recanalise a CTO or calcified /tortuous vessels despite successfully positioning a guidewire into the distal true lumen and accounts for 10%–15% of all procedure failures
✓RotA is a safe and effective technique to overcome this frustrating situation
✓Initiating treatment with the smallest burrs (1.25 mm) is the safest approach (subintimal tracking of the guide wire frequently created during CTO crossing-minimize the risk of vessel perforation).
Rota-Rescue Inability to cross the lesion with the balloon
Rota-Rescue Inability to cross the lesion with the balloon
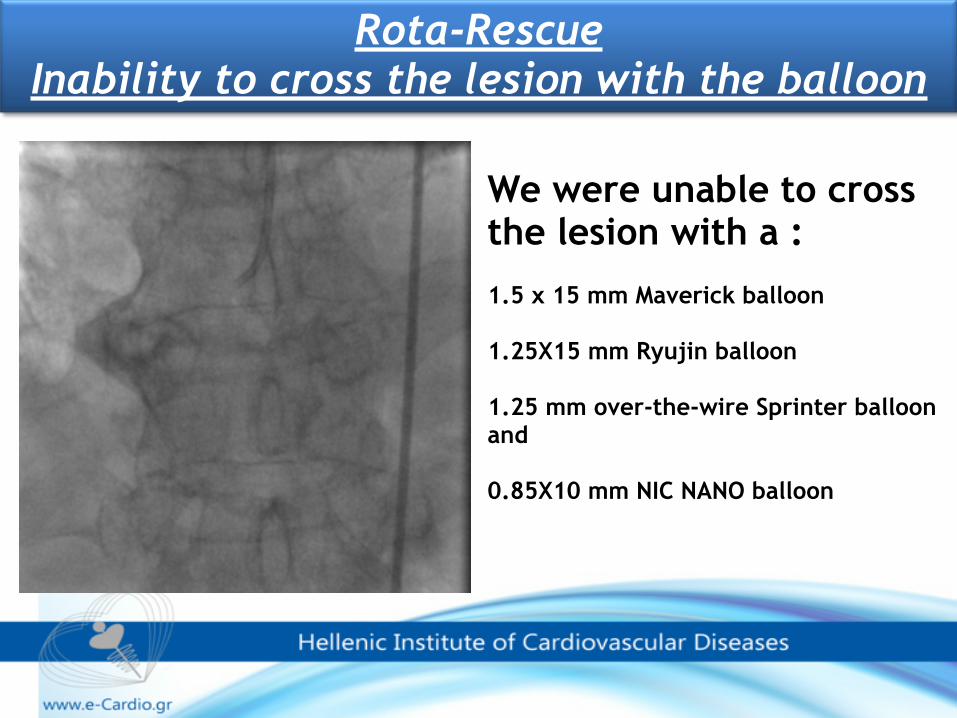
We were unable to cross the lesion with a :
1.5 x 15 mm Maverick balloon
1.25X15 mm Ryujin balloon
1.25 mm over-the-wire Sprinter balloon and
0.85X10 mm NIC NANO balloon

6F Guideliner catheter deeply into the RCA, just proximal to the point of the lesion
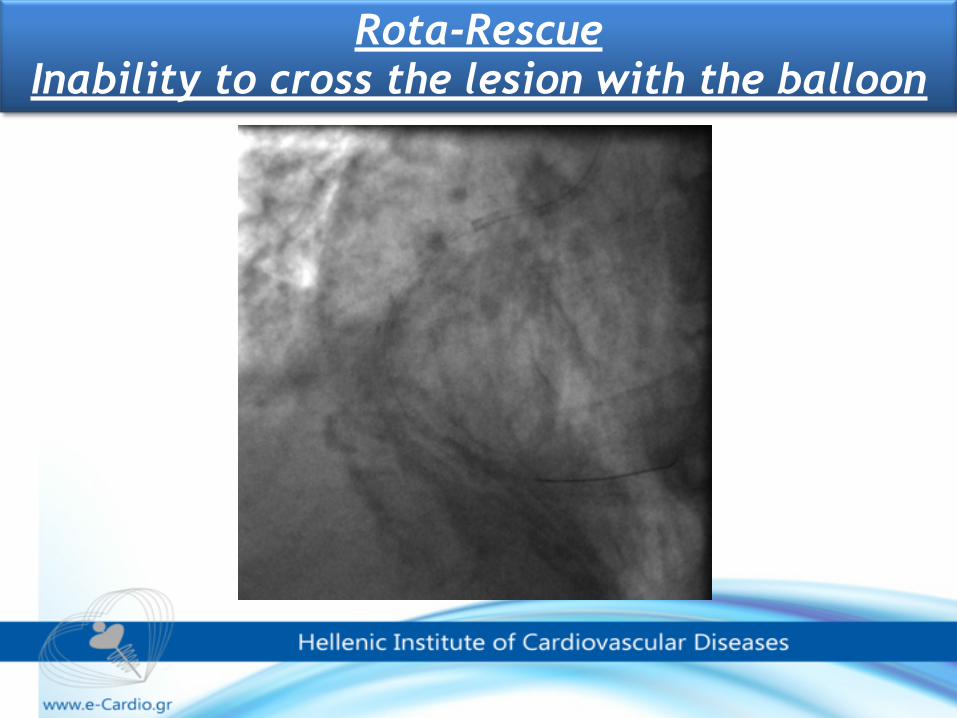
Inability to cross the lesion with the same balloons
Rotational Atherectomy (RA) was first performed using a 1.25-mm Rotablator burr
Rota-Rescue Inability to cross the lesion with the balloon

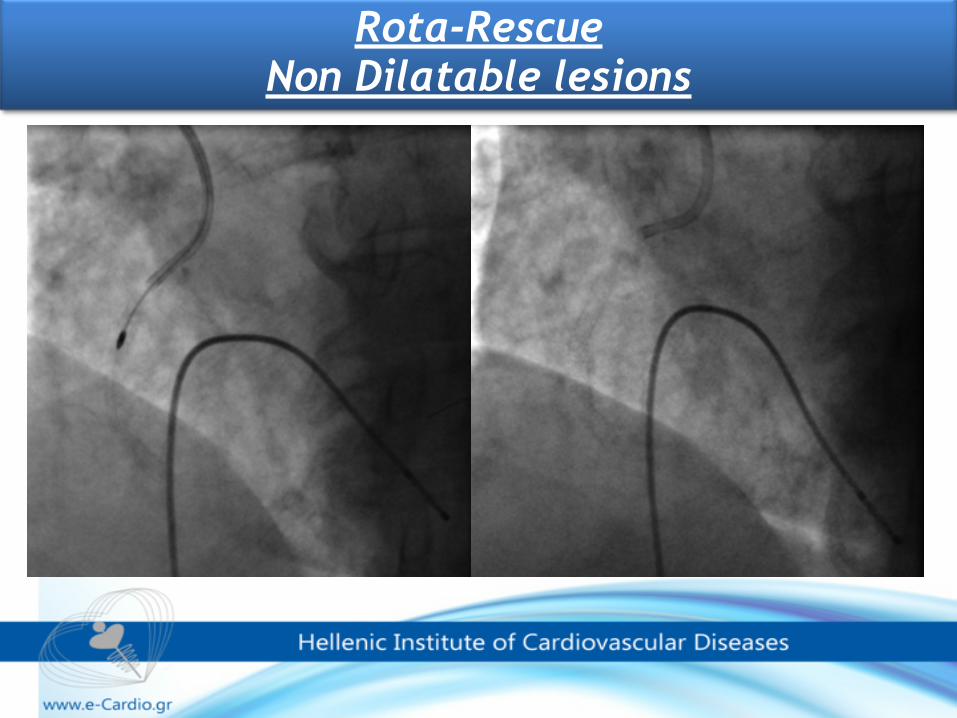
Author Lesion N Success (%) Reisman (1993) Non dilatable 34 97 Brogan (1993) Non dilatable 41 90 Sievert (1993) Non dilatable 32 97
Rosenblum (1992) Non dilatable 40 97
Rotablator Published Reports :Non dilatable lesions
Rota-Rescue Non Dilatable lesions

Rota-Rescue Non Dilatable lesions
Rota-Rescue Non Dilatable lesions

Rota-Rescue Inability to deliver a stent
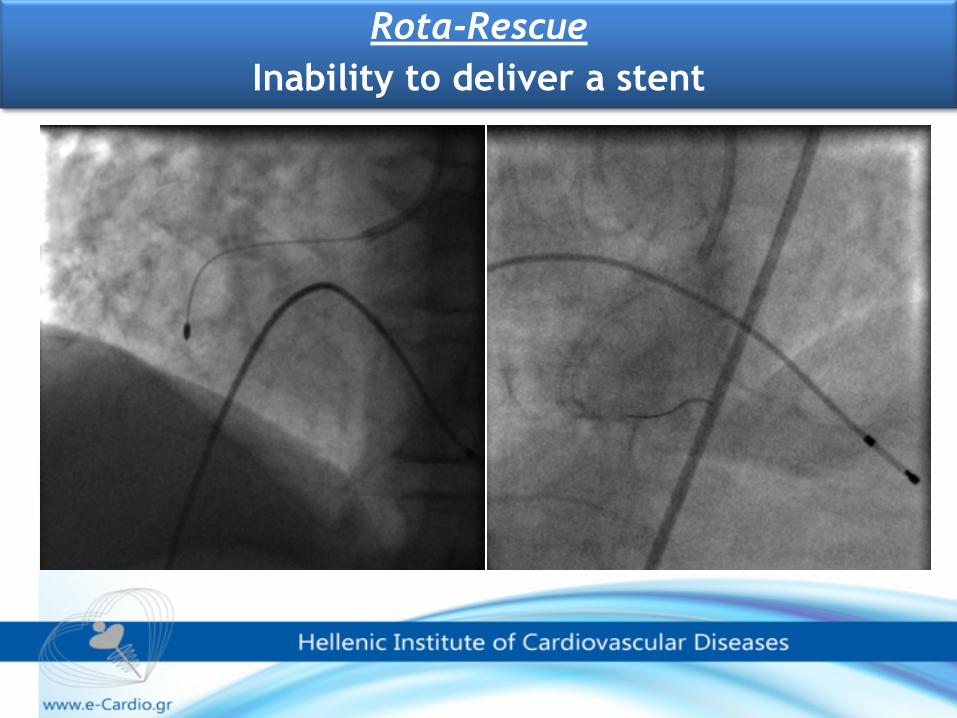
Rota-Rescue Inability to deliver a stent
JUST DO IT ………….. EARLY
The decision to use rotablation should be made early, before large dissections
appear.

➢In ostial lesions (specifically in RCA) the frequent fibrocalcific characteristics of these lesions make them well suited for rotablation treatment.
➢In addition, aggressive balloon dilatation of aorto-ostial lesions might even be associated with retrograde dissections from the coronary ostium to the ascending aorta.
➢In performing rotablation of aorto-ostial lesions, it is important to keep the guiding catheter coaxial in order to avoid burr lodging
Rotablator :ostial lesions

66
In ostial lesions, the success rate of the Rotablator procedure is > 90%
Author lesion N Success (%)
Koller (1994) Ostial 29 93
Zimarino (1994) Ostial 69 92
Popma (1993) Ostial 105 97
Rotablator :ostial lesions

Rotablator :ostial lesions

Rotablator :ostial lesions
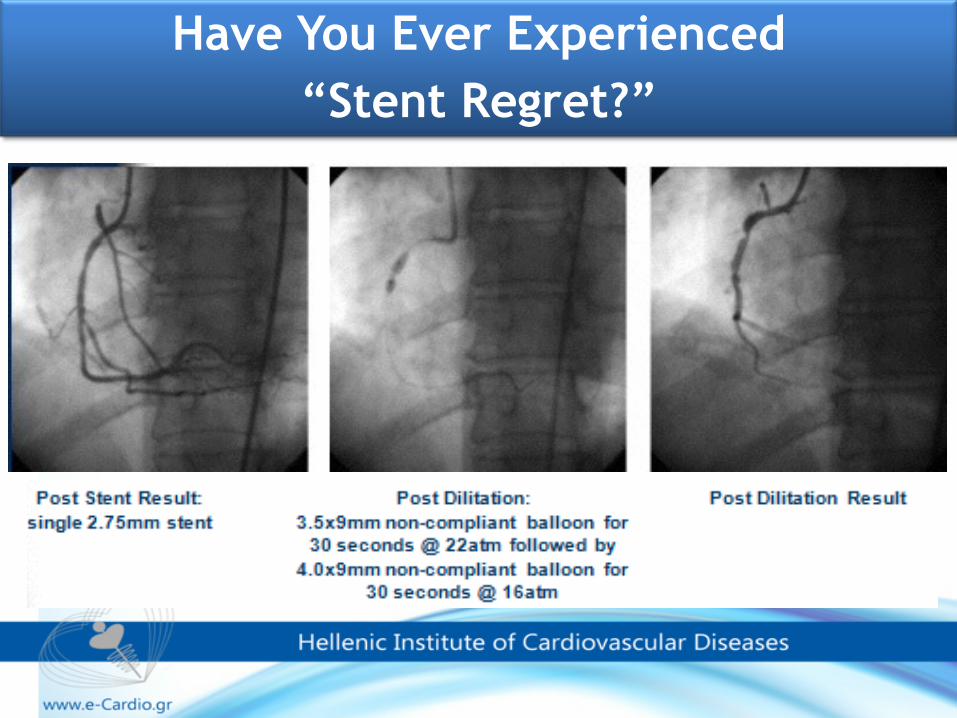
Have You Ever Experienced “Stent Regret?”

✓This situation should be prevented by avoiding stent implantation unless adequate stenosis preparation has been performed with either balloon (inflated without waisting) or rotational atherectomy.
✓When aggressive post-dilatation has been attempted unsuccessfully, rotational atherectomy of under expanded stent (STENT ABLATION) has been reported as a viable option
SEVERE STENT UNDEREXPANSION

Coronary angiography reveals a 90% stenosis of the right coronary artery (RCA) (A). Direct stenting of the bare metal stent (BMS) results in an underexpansion (B) and residual stenosis in the mid-part (C).

Rotational atherectomy of the remaining calcified stenosis within the stent and the underexpanded stent struts (stentablation) (A) with acceptable result in the following angiography. Drug eluting stent (DES) implantation (rotastenting) (B) after rotational atheterctomy without any evidence for residual stenosis in final angiogram (C)
➢Rotablation of an underexpanded stent should be considered with extreme caution in highly experienced hands, preferably with surgical back-up.
➢This procedure has a high risk of burr lodging and should be discouraged.
➢In this case it might be advisable to proceed step by step by increasing burr size and by careful, slow advancement of the burr across the stent, in order to avoid burr entrapment
STENT ABLATION

Labeled contraindications to RA include: ✓saphenous vein graft lesions, ✓thrombus, ✓dissection, and ✓occlusions through which a guidewire will not pass.
Relative contraindications include ✓unavailability of bypass surgery (whether due to patient ineligibility or lack of cardiac surgery on site), ✓Severe 3-vessel or unprotected left main disease, ✓Last remaining vessel ✓severe left ventricular dysfunction, lesion length in excess of 25mm, and ✓lesion angulation in excess of 450.
Contraindications to RA

✓Slow/no reflow
✓Distal embolization
✓Coronary spasm
✓Coronary perforation
✓Coronary dissection.
✓Burr entrapment is one of rare but serious complications of the Rotablator, and previous report indicated that it occurred in 6 of 1,403 procedures (0.4%)
Complications specifically seen with Rotational Atherectomy

•Death 1.0% •Q-Wave myocardial infarction (MI) 1.2% •Coronary Artery Bypass Graft (CABG) 2.5%
76
N = 2,953 Procedures
Wart DC, Leon MB. O’Neill W, et al. Rotational Atherectomy Multicenter Registry. Acute results, complications and 6 month follow-up in 709 patients. J Amer Coll Cardiol 1994; 24(3): 641-8 (unfinished report). Industry-sponsored Reisman M, Harms V, Feldman T, Fortuna R, Buchbinder et al. Comparison of Early and Recent Results With Rotational Atherectomy. J Am Coll Cardiol 1997; 29:353-7. Industry-sponsored.
Overall Major Complications

➢Complications of RA are uncommon in experienced hands. ➢ ➢The nature of the device does mean, however, that occasional high-risk complications can occur, and under these circumstances the availability of immediate bypass facilities can be lifesaving.
➢The availability of surgical back-up during the learning curve may be a good compromise before starting a regular rotational atherectomy programme in a cathlab without an on-site surgical facility.
ON-SITE SURGICAL COVER

Proposed Algorithm for Use of Rotational Atherectomy in Management of de Novo Calcified Lesions
•Consideration of RA requires determining calcification severity, because benefits of RA are attenuated when calcification is mild or absent. •In practice, calcification severity is customarily graded by qualitative assessment of angiography
➢severe calcification defined by radio-opacities noted without cardiac motion before contrast injection, generally involving both sides of the arterial wall, and ➢moderate calcification defined by densities noted only during the cardiac cycle before contrast injection
•Angiography is insensitive for detection of calcification in comparison with intravascular ultrasound (IVUS), but visible calcification on angiography predicts a larger arc of calcification on IVUS

Proposed Algorithm for Use of Rotational Atherectomy in Management of de Novo Calcified Lesions

Proposed Algorithm for Use of Rotational Atherectomy in Management of de Novo Calcified Lesions

CONCLUSIONS
✓We view RA as a tool to make PCI possible in complex lesions with moderate or severe calcification when clinical variables make PCI appropriate
✓RA is a technically demanding procedure reliant on operator experience
❖Optimal outcomes for rotational atherectomy procedures are achieved by regular users of this technology
✓We must emphasise that, as with all things, good training and support lead to better outcomes for the operator and the patient.
CONCLUSIONS
✓The persistence of angiographic and clinical complications of RA underscores the potential for further progress in technology and technique
✓Finally, global declines in volume of coronary revascularization, in particular PCI for stable ischemic heart disease, will further reduce the already uncommon use of RA. This will have important implications for efficacy and safety of RA.
✓We believe the solution to this problem will be to maintain referral centers of excellence for PCI of complex lesions, including RA.

Thank you for your attention!!!!!!!
WHO SHOULD DO RA? Optimal outcomes for rotational atherectomy procedures are achieved by regular users of this technology. Therefore, it might be safer to consider transferring the patient to a high-volume centre, experienced in the rotablation procedure.
emphasises that, as with all things, good training and support lead to better outcomes for the operator and the patient.

The persistence of angiographic and clinical complications of RA underscores the potential for further progress in technology and technique. New devices are in development, including a novel RA device to reduce microcavitation (84) and an orbital atherectomy system for use with coronary lesions.
Finally, global declines in volume of coronary revascularization, in particular PCI for stable ischemic heart disease (86), will further reduce the already uncommon use of RA. This will have important implications for efficacy and safety of RA, a technically demanding procedure reliant on operator experience. We believe the solution to this problem will be to maintain referral centers of excellence for PCI of complex lesions, including RA.
WHO SHOULD DO RA? Optimal outcomes for rotational atherectomy procedures are achieved by regular users of this technology. Therefore, it might be safer to consider transferring the patient to a high-volume centre, experienced in the rotablation procedure.
emphasises that, as with all things, good training and support lead to better outcomes for the operator and the patient.
The impact of the new
agents on complications of RA is unknown and merits study.

