rom j morphol embryol 2011, 52(3 ... - journal of morphology · rom j morphol embryol 2011, 52(3...
TRANSCRIPT

Rom J Morphol Embryol 2011, 52(3 Suppl):1133–1137
CCAASSEE RREEPPOORRTT
Adjusting dento-alveolar morphology with orthodontic mini-implants (miniscrews).
A clinical case report CRISTINA DANA BRATU1), R. V. POP2), SILVIA-IZABELLA POP3),
EM. A. BRATU4)
1)Department of Pedodontics and Orthodontics, Faculty of Dentistry,
“Victor Babeş” University of Medicine and Pharmacy, Timisoara 2)Private practice, Targu Mures
3)Department of Pedodontics and Orthodontics, Faculty of Dentistry,
University of Medicine and Pharmacy of Targu Mures 4)Department of Implant Supported Restorations,
Faculty of Dentistry, “Victor Babeş” University of Medicine and Pharmacy, Timisoara
Abstract Mini-implants are increasingly popular for creating skeletal anchorage in clinical orthodontics. The aim of this article is to present and discuss the clinical uses, benefits and drawbacks of the miniscrew implants used to reorder and adjust the dento-alveolar morphology of the overerupted maxillary molars. The loss of the lower premolars and molars very often leads to overeruption of the opposing maxillary teeth, combined with insufficient space for prosthetic restorations. The available treatment options are either a significant reduction of the maxillary teeth, often associated with endodontic treatment, or a complex orthodontic treatment. In the previous years, different cases of orthodontic intrusion with mini-implants were described. In this report, the authors describe a case of a young patient who needed a maxillary molar intrusion in order to get sufficient prosthetic space for an implant supported fixed restoration in the third quadrant. This treatment type preserved maximum tooth structures and allowed a successful mandibular restoration. Keywords: dento-alveolar morphology adjustment, unilateral intrusion, overerupted molar, mini-implants (miniscrews), skeletal
anchorage.
Introduction
In recent years, orthodontic mini-implants or mini-screws have become very popular in the orthodontic community for providing anchorage [1–5]. They are an excellent alternative to conventional orthodontic anchorage systems such as intraoral dental anchoring units and extra-oral headgear devices. Mini-implants are especially useful for adults with an incomplete dentition as well as for adolescents when noncompliance during treatment is likely. Other advantages include their relatively small size, which results in minimal anatomical limitations, user-friendly protocol, immediate loading potential, adaptability to biomechanics in effecting orthodontic and orthopedic forces, high success rate, low cost and most importantly patient acceptability [4–6].
The loss of the mandibular molars, and absence of a prosthetic restoration right after this loss, often causes the opposing teeth to overerupt. This leads to a very small prosthetic space for restorations, occlusal interferences and a compromised periodontal health. This type of situations could be solved either by invasive techniques with a great loss of dental structure or with the help of extraoral headgears and other
complex orthodontic treatments [6]. A more conservative approach is to intrude orthodontically the extrusive molar [7–9]. Posterior intrusion is one of the most difficult tooth movements in orthodontics, because of the multiple molar roots. Intrusion requires more alveolar bone reaction as well as a longer treatment time [2, 3]. Therefore, using conventional orthodontic treatment for this movement is a big challenge. Three dimensional movement control is essential in this therapy. Vertical position, the arch form, the tooth axes, the inclination of the occlusal plane and the posterior torque should be the treatment objectives [2, 3]. The use of orthodontic mini-implants simplified the treatment plan and allowed a maximum conservation of tooth structures. There are some differences between the various extradental anchorage systems available: the type of metallic composition (from pure titanium to conventional stainless steel), the surgical procedure for insertion (major or minor surgical trauma), the possibility of osteointegration, and the application of immediate loading [2, 3, 10].
Intra-oral temporary anchorage devices (TADs) were developed to provide Type A anchorage, because this form of anchorage is difficult to accomplish with conventional biomechanics [11]. Different types of
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/
Cristina Dana Bratu et al.
1134
TADs are available with the proponents of each type, claiming that their device is superior to other systems [11]. Several reports on different systems have been published: osseointegrated implants onplants, zygoma wires and anchors, mini-plates and miniscrews.
Cortical bone thickness is an important factor in mini-implant stability [12, 13]. Placing the implant in areas of favorable bone thickness ensures better primary stability and long-term success [14]. Selecting the proper implant site is also an important factor in the overall success of this treatment approach. In contrast to dental implants, orthodontic miniscrews are loaded immediately, and most authors suggest the use of light forces early on [15].
This case report describes a maxillary molar intrusion with the use of four orthodontic mini-implants and third quadrant prosthetic implant supported restoration. The design of the MIS orthodontic implant, used in this case report, allowed a good primary stability and sufficient anchorage in order to apply the forces needed to complete the treatment.
Patient, Materials and Methods
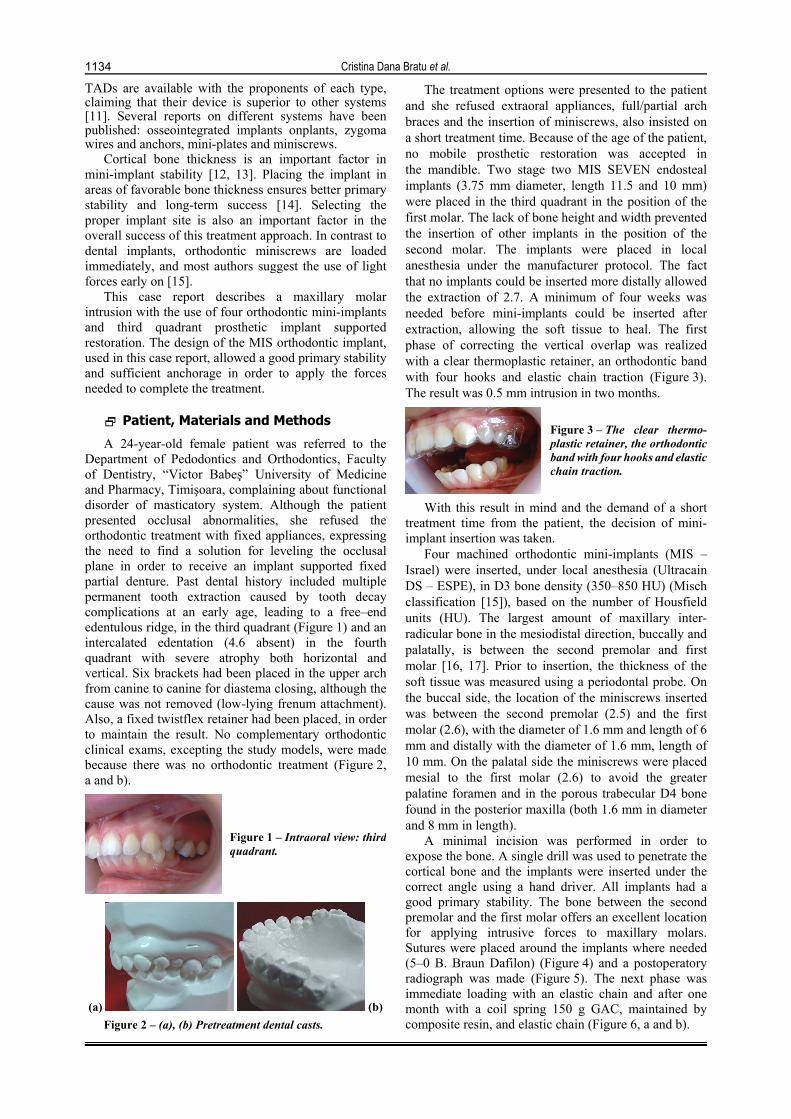
A 24-year-old female patient was referred to the Department of Pedodontics and Orthodontics, Faculty of Dentistry, “Victor Babeş” University of Medicine and Pharmacy, Timişoara, complaining about functional disorder of masticatory system. Although the patient presented occlusal abnormalities, she refused the orthodontic treatment with fixed appliances, expressing the need to find a solution for leveling the occlusal plane in order to receive an implant supported fixed partial denture. Past dental history included multiple permanent tooth extraction caused by tooth decay complications at an early age, leading to a free–end edentulous ridge, in the third quadrant (Figure 1) and an intercalated edentation (4.6 absent) in the fourth quadrant with severe atrophy both horizontal and vertical. Six brackets had been placed in the upper arch from canine to canine for diastema closing, although the cause was not removed (low-lying frenum attachment). Also, a fixed twistflex retainer had been placed, in order to maintain the result. No complementary orthodontic clinical exams, excepting the study models, were made because there was no orthodontic treatment (Figure 2, a and b).
Figure 1 – Intraoral view: thirdquadrant.
(a) (b) Figure 2 – (a), (b) Pretreatment dental casts.
The treatment options were presented to the patient and she refused extraoral appliances, full/partial arch braces and the insertion of miniscrews, also insisted on a short treatment time. Because of the age of the patient, no mobile prosthetic restoration was accepted in the mandible. Two stage two MIS SEVEN endosteal implants (3.75 mm diameter, length 11.5 and 10 mm) were placed in the third quadrant in the position of the first molar. The lack of bone height and width prevented the insertion of other implants in the position of the second molar. The implants were placed in local anesthesia under the manufacturer protocol. The fact that no implants could be inserted more distally allowed the extraction of 2.7. A minimum of four weeks was needed before mini-implants could be inserted after extraction, allowing the soft tissue to heal. The first phase of correcting the vertical overlap was realized with a clear thermoplastic retainer, an orthodontic band with four hooks and elastic chain traction (Figure 3). The result was 0.5 mm intrusion in two months.
Figure 3 – The clear thermo-plastic retainer, the orthodontic band with four hooks and elasticchain traction.
With this result in mind and the demand of a short treatment time from the patient, the decision of mini-implant insertion was taken.
Four machined orthodontic mini-implants (MIS –Israel) were inserted, under local anesthesia (Ultracain DS – ESPE), in D3 bone density (350–850 HU) (Misch classification [15]), based on the number of Housfield units (HU). The largest amount of maxillary inter-radicular bone in the mesiodistal direction, buccally and palatally, is between the second premolar and first molar [16, 17]. Prior to insertion, the thickness of the soft tissue was measured using a periodontal probe. On the buccal side, the location of the miniscrews inserted was between the second premolar (2.5) and the first molar (2.6), with the diameter of 1.6 mm and length of 6 mm and distally with the diameter of 1.6 mm, length of 10 mm. On the palatal side the miniscrews were placed mesial to the first molar (2.6) to avoid the greater palatine foramen and in the porous trabecular D4 bone found in the posterior maxilla (both 1.6 mm in diameter and 8 mm in length).
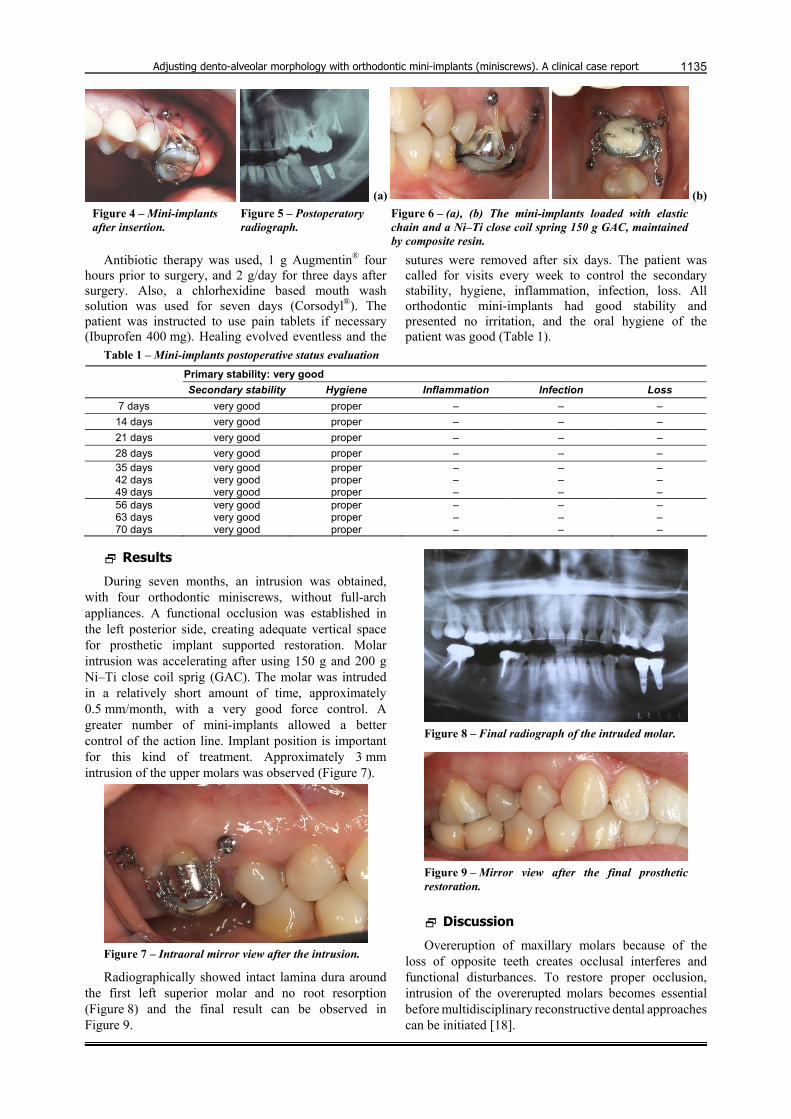
A minimal incision was performed in order to expose the bone. A single drill was used to penetrate the cortical bone and the implants were inserted under the correct angle using a hand driver. All implants had a good primary stability. The bone between the second premolar and the first molar offers an excellent location for applying intrusive forces to maxillary molars. Sutures were placed around the implants where needed (5–0 B. Braun Dafilon) (Figure 4) and a postoperatory radiograph was made (Figure 5). The next phase was immediate loading with an elastic chain and after one month with a coil spring 150 g GAC, maintained by composite resin, and elastic chain (Figure 6, a and b).
Adjusting dento-alveolar morphology with orthodontic mini-implants (miniscrews). A clinical case report
1135
(a) (b)Figure 4 – Mini-implants after insertion.
Figure 5 – Postoperatory radiograph.
Figure 6 – (a), (b) The mini-implants loaded with elastic chain and a Ni–Ti close coil spring 150 g GAC, maintained by composite resin.
Antibiotic therapy was used, 1 g Augmentin® four hours prior to surgery, and 2 g/day for three days after surgery. Also, a chlorhexidine based mouth wash solution was used for seven days (Corsodyl®). The patient was instructed to use pain tablets if necessary (Ibuprofen 400 mg). Healing evolved eventless and the
sutures were removed after six days. The patient was called for visits every week to control the secondary stability, hygiene, inflammation, infection, loss. All orthodontic mini-implants had good stability and presented no irritation, and the oral hygiene of the patient was good (Table 1).
Table 1 – Mini-implants postoperative status evaluation Primary stability: very good Secondary stability Hygiene Inflammation Infection Loss
7 days very good proper – – – 14 days very good proper – – – 21 days very good proper – – – 28 days very good proper – – – 35 days 42 days 49 days
very good very good very good
proper proper proper
– – –
– – –
– – –
56 days 63 days 70 days
very good very good very good
proper proper proper
– – –
– – –
– – –
Results
During seven months, an intrusion was obtained, with four orthodontic miniscrews, without full-arch appliances. A functional occlusion was established in the left posterior side, creating adequate vertical space for prosthetic implant supported restoration. Molar intrusion was accelerating after using 150 g and 200 g Ni–Ti close coil sprig (GAC). The molar was intruded in a relatively short amount of time, approximately 0.5 mm/month, with a very good force control. A greater number of mini-implants allowed a better control of the action line. Implant position is important for this kind of treatment. Approximately 3 mm intrusion of the upper molars was observed (Figure 7).
Figure 7 – Intraoral mirror view after the intrusion.
Radiographically showed intact lamina dura around the first left superior molar and no root resorption (Figure 8) and the final result can be observed in Figure 9.
Figure 8 – Final radiograph of the intruded molar.
Figure 9 – Mirror view after the final prosthetic restoration.
Discussion
Overeruption of maxillary molars because of the loss of opposite teeth creates occlusal interferes and functional disturbances. To restore proper occlusion, intrusion of the overerupted molars becomes essential before multidisciplinary reconstructive dental approaches can be initiated [18].

Cristina Dana Bratu et al.
1136
The use of mini-implants for molar intrusion is a simple and rapid therapy, but some steps can be tricky and lead to complications.
Force application is often limited because the
locations of the implants placement are limited. Implants are not always inserted in the ideal position. Adjustment of force direction will be required depending on the changes of the tooth movement during treatment time. It is a technique-sensitive treatment method and patients should be closely monitored.
It is essential that the mechanics of unilateral intrusion should have components, which can apply buccal and palatal intrusive forces.
Posterior intrusion is not just a matter of vertical control. The dentoalveolar space between the second premolar and the first molar provides sufficient bone for screw insertion, but care must be given to modify the insertion axis according to the bone contour. Also, the length of the screw depends on the thickness of the soft tissue, so careful evaluation of this parameter in necessary before insertion, otherwise only a short part of the screw will penetrate the bone. This is especially important for the palatal screws. Perfect positioning of the mini-implants is critical in order to avoid injury of the roots. This is why we recommend taking several intraoral X-rays, and if possible a DVT-SCAN for better 3D evaluation. Angulation of the screws at 450, allows a better force distribution in the bone, but it is also important for avoiding penetration into the maxillary sinus. It is important to probe the cavity before implant insertion in order to avoid this complication.
Although different authors recommend the flapless insertion, our experience showed a better primary stability and a higher success rate for the miniflap technique. Because of the need of the three-dimensional movement control of the molars, the therapy solution with four mini-implants is better than the one with two, allowing better force distribution and control. Vertical axial intrusion must be accompanied by arch form control and tooth axis inclination on the occlusal plane. The use of palatal interdental implants or midpalatal implants to apply intrusive force from palatal side is strongly recommended. Palatal root control is the key to maxillary molar intrusion [19]. The palatal root control is more important and more difficult because the center of resistance of maxillary molars is located toward the palatal side [19].
Most patients with a localized problem do not perceive the difficulty of intrusion and reconstruction. The surgical impaction or crown reduction of the over-erupted teeth immediately corrects the uneven occlusal plane, but the patients are often reluctant to accept such a proposal because of the invasiveness and consequences of the procedures [20]. The purpose of using implants as skeletal anchorage is to totally eliminate the need for patient compliance and the need to wear extraoral auxiliaries [20]. The use of 1.6 mm diameter implants can sustain forces greater then 300 g. Therefore, under constant loading with medium forces of 150 to 200 g from elastic modules on the buccal or both buccal and palatal sides, as needed in this case, the molars intrude, whereas the implants remain stable [21, 22].
In a study using finite element analysis, was found that immediate loading should be limited to 50 cN of force in a 2 mm diameter miniscrew implant [13, 14]. No significant association between the success rate and immediate loading was found on 51 patients, in which 134 titanium screws of three types (1.0 mm, 1.5 mm, and 2.0 mm in diameter) and 17 miniplates were used. It was concluded that immediate loading is possible if the applied force is less than 2 N [14].
From the biomechanical point of view, for posterior segment intrusion many authors recommend midpalatal implants with attachments, in comparison with inter-dental miniscrew, but these are more comfortable for the patients [20, 23, 24].
There are controversies about the intrusion of peri-odontally involved teeth [14–16], but in some reports authors concluded that if the inflammation would be well controlled, intrusion of teeth would not result in the loss of the marginal bone level [16–20]. Therefore, it was concluded that mini-implants are very fascinating devices for over erupted teeth intrusion even if the patient has periodontal disease.
Conclusions
The use of miniscrews is highly indicated as anchorage for the intrusion of maxillary molars. The patient was treated using mini-implants without full-arch technique, which offered a good esthetic alternative. Short-term molar intrusion and change of alveolar process morphology was achieved within a limited amount of time, without clinically detectable apical root resorption. No discomfort has been reported in our case. The machined mini-implants (MIS, Israel) used in the present article proved to be efficient in maintaining the type of extradental anchorage required in this clinical situation. None of the implants showed signs of osseointegration and could easily be removed from the bone.
References [1] Costa A, Raffaini M, Melsen B, Miniscrews as orthodontic
anchorage: a preliminary report, Int J Adult Orthodon Orthognath Surg, 1998, 13(3):201–209.
[2] Lee JS, Kim JK, Park YC, Vanarsdall RL, Applications of orthodontic mini-implants, Quintessence Publishing Co. Ltd., Canada, 2007.
[3] Ohmae M, Saito S, Morohashi T, Seki K, Qu H, Kanomi R, Yamasaki KI, Okano T, Yamada S, Shibasaki Y, A clinical and histological evaluation of titanium mini-implants as anchors for orthodontic intrusion in the beagle dog, Am J Orthod Dentofacial Orthop, 2001, 119(5):489–497.
[4] Kyung HM, Park HS, Bae SM, Sung JH, Kim IB, Development of orthodontic micro-implants for intraoral anchorage, J Clin Orthod, 2003, 37(6):321–328; quiz 314.
[5] Fritz U, Ehmer A, Diedrich P, Clinical suitability of titanium microscrews for orthodontic anchorage – preliminary experiences, J Orofac Orthop, 2004, 65(5):410–418.
[6] Kanomi R, Takada K, Application of titanium mini-implant system for orthodontic anchorage. In: Mah J, Davidovitch Z (ed), Biological mechanisms of tooth movement and cranio-facial adaptation, EBSCO Media, Birmingham (AL), 2000, 253–258.
[7] Büchter A, Wiechmann D, Koerdt S, Wiesmann HP, Piffko J, Meyer U, Load-related implant reaction of mini-implants used for orthodontic anchorage, Clin Oral Implants Res, 2005, 16(4):473–479.

Adjusting dento-alveolar morphology with orthodontic mini-implants (miniscrews). A clinical case report
1137[8] Park HS, Lee SK, Kwon OW, Group distal movement of
teeth using microscrew implant anchorage, Angle Orthod, 2005, 75(4):602–609.
[9] Ludwing B, Baumgaertel S, Bowman SJ, Mini-implants in orthodontics. Innovative anchorage concepts, Quintessence Publishing Co. Ltd., Germany, 2008.
[10] Fortini A, Caciafesta V, Sfondrini MF, Cambi S, Lupoli M, Clinical applications and efficiency of miniscrew for extra-dental anchorage, Orthodontics, 2004, 1(2), http://www. westconsult.se/news/Mini-implantat.pdf.
[11] Melsen B, Fiorelli G, Upper molar intrusion, J Clin Orthod, 1996, 30(2):91–96.
[12] Alessandri Bonetti G, Giunta D, Molar intrusion with a removable appliance, J Clin Orthod, 1996, 30(8):434–437.
[13] Chun YS, Woo YJ, Row J, Jung EJ, Maxillary molar intrusion with the molar intrusion arch, J Clin Orthod, 2000, 34(2):90–93.
[14] Melsen B, Agerbaek N, Eriksen J, Terp S, New attachment through periodontal treatment and orthodontic intrusion, Am J Orthod Dentofacial Orthop, 1988, 94(2):104–116.
[15] Misch CE, Contemporary implant dentistry, 2nd edition, Mosby, St. Louis, 1998.
[16] Melsen B, Agerbaek N, Markenstam G, Intrusion of incisors in adult patients with marginal bone loss, Am J Orthod Dentofacial Orthop, 1989, 96(3):232–241.
[17] Hoste S, Vercruyssen M, Quirynen M, Willems G, Risk factors and indications of orthodontic temporary anchorage devices: a literature review, Aust Orthod J, 2008, 24(2):140–148.
[18] Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen CM, The application of mini-implants for orthodontic anchorage, Int J Oral Maxillofac Surg, 2006, 35(8):704–707.
[19] Yao CC, Lee JJ, Chen HY, Chang ZC, Chang HF, Chen YJ, Maxillary molar intrusion with fixed appliances and mini-implant anchorage studied in three dimensions, Angle Orthod, 2005, 75(5):754–760.
[20] Seth V, Kamath P, Venkatesh MJ, Prasad R, Vishwanath, Micro-implants: innovative anchorage concepts in ortho-dontics, The Orthodontic CYBERjournal, January 2011, http://orthocj.com/2011/01/micro-implants-innovative-ancho rage-concepts-in-orthodontics/.
[21] Ohashi E, Pecho OE, Moron M, Lagravere MO, Implant vs. screw loading protocols in orthodontics: a systematic review, Angle Orthod, 2006, 76(4):721–727.
[22] Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano-Yamamoto T, Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage, Am J Orthod Dentofacial Orthop, 2003, 124(4):373–378.
[23] Kravitz ND, Kusnoto B, Tsay PT, Hohlt WF, Intrusion of overerupted upper first molar using two orthodontic mini-screws. A case report, Angle Orthod, 2007, 77(5):915–922.
[24] Schnelle MA, Beck FM, Jaynes RM, Huja SS, A radiographic evaluation of the availability of bone for placement of mini-screws, Angle Orthod, 2004, 74(6):832–837.
Corresponding author Cristina Dana Bratu, Assistant Professor, Department of Pedodontics and Orthodontics, Faculty of Dentistry, ”Victor Babeş” University of Medicine and Pharmacy, 73 Liviu Rebreanu Avenue, 300755 Timişoara, Romania; Phone +40744–835 314, Fax +40256–491 943, e-mail: [email protected] Received: August 10th, 2011
Accepted: October 10th, 2011