role of workplace ergonomics on healthcare
TRANSCRIPT

i
ROLE OF WORKPLACE ERGONOMICS ON HEALTHCARE
EMPLOYEES’ PERFORMANCE: A CASE OF MUHIMBILI NATIONAL
HOSPITAL, TANZANIA
BY
VERONICA HELLAR
A Dissertation Submitted in Partial Fulfillment of the Requirements for Award
of the Degree of Master in Business Administration (Corporate Management)
of Mzumbe University
2020

i
CERTIFICATION
We, the undersigned, certify that we have read and hereby recommend for acceptance,
a dissertation entitled “The role of workplace ergonomics on healthcare employees’
performance: a case of Muhimbili National Hospital, Tanzania” in partial
fulfillment of the requirements for award of the degree of Master of Business
Administration in Corporate Management.
________________
Major Supervisor
_______________
Internal Examiner
________________
External Examiner
Accepted for Board of MU-DCC
______________________________________________________
PRINCIPAL/DAR-ES-SALAAM CAMPUS COLLEGE BOARD
ii
DECLARATION
AND
COPYRIGHT
I,Veronica Hellar, declare that this dissertation is my own original work and that it
has not been presented and will not be presented to any other university for a similar
or any other degree award.
Signature: ________________________
Date: __________________________
© 2020
This dissertation is copyright material protected under the Berne Convention, the
Copyright Act of 1999 and other international and national enactments, in that behalf,
on intellectual property. It may not be reproduced by any means, in full or in part,
except for short extracts in fair dealing; for research or private study, critical scholarly
review or discourse with an acknowledgement, without the written permission of
Mzumbe University, on behalf of the author.

iii
ACKNOWLEDGEMENT
Firstly, I give thanks to God Almighty, for endowing upon me the health, strength and
motivation to complete this work.
Secondly, I express my heartfelt appreciation and gratitude to my supervisor Dr.
Felichesmi Lyakurwa for his guidance and advice during the entire period of
undertaking this study whereas he always responded promptly and constructively.
Thirdly, to my parents Christopher and Agnes Hellar who have always supported me
morally and through prayers, I am forever grateful.
Lastly but not least, I must acknowledge the support received from the Management
and staff of the Muhimbili National Hospital without whom I wouldn’t have
completed this work.

iv
DEDICATION
This paper is dedicated to my lovely family; my husband Chediel Msuya who has
always supported me and my beautiful children Reuben, Stewart, Terence and Owen
Msuya who give me the reason for wanting to achieve more.

v
ABBREVIATIONS AND ACRONYMS
IEA International Ergonomics Association
ILO International Labor Organization
GDP Gross Domestic Product
IACs Industrially Advanced Countries
IDCs Industrially Developing Countries
OSHA Occupational Health and Safety Authority
MNH Muhimbili National Hospital
OPRAS Open Performance Appraisal System
HF/E Human Factors Ergonomics
ERFs Ergonomic Risk Factors
MSDs Musculoskeletal Disorders
CDC Centers for Disease Control and Prevention
LBP Lower Back Pain

vi
ABSTRACT
The study explored the role of workplace ergonomics on healthcare employees’
performance using the Muhimbili National Hospital (MNH) as a case study. The
specific objectives of this study were to determine the extent to which workplace
ergonomics influence healthcare employees’ performance at the workplace, to
examine healthcare employees’ awareness about ergonomics design of the
workplaces, to document the barriers towards ergonomic design of workplaces as a
tool for improving employees’ performance in healthcare facilities, the case of MNH.
The study employed case study research design where both qualitative and
quantitative data were collected by distributing questionnaires to 96 staff at MNH.
This included clinical staff, non – clinical staff, nursing staff and management. In
addition, the interview method was also used to complement the data that was
collected through questionnaires especially those that required more qualitative data.
The findings of the study revealed that office size, workplace temperature, airflow and
light, office furniture, workplace environment and level of noise all affect employee’s
performance. Also it was found that 36% of all the respondents were aware about the
workplace ergonomics issues. Lastly, budgetary constraints, technological factors and
old design of the hospital were ranked as the top barriers towards ergonomics design
at MNH. This implies that healthcare facilities need to consider and improve
workplace ergonomics as a tool for improving healthcare employees’ performance.
Furthermore, there is a need to take initiatives for improvement of awareness on
workplace ergonomics in the healthcare facilities.
The study therefore recommends more training on workplace ergonomics aimed at
boosting up employee’s awareness. Also, healthcare facilities need to invest in
technology advancements as well as allocation of more financial resources for
improvement of workplace ergonomics. The study also recommends that healthcare
facilities should be designed in ways that support workplace ergonomics.
vii
TABLE OF CONTENTS
CERTIFICATION ...................................................................................................... i
DECLARATION ........................................................................................................ ii
AND ............................................................................................................................. ii
COPYRIGHT ............................................................................................................. ii
ACKNOWLEDGEMENT ........................................................................................ iii
DEDICATION ........................................................................................................... iv
ABBREVIATIONS AND ACRONYMS .................................................................. v
ABSTRACT ............................................................................................................... vi
LIST OF TABLES ................................................................................................... xii
LIST OF FIGURES ................................................................................................ xiii
CHAPTER ONE ........................................................................................................ 1
PROBLEM SETTING ............................................................................................... 1
1.1 Background of the Study ........................................................................................ 1
1.2 Statement of the Problem ....................................................................................... 6
1.3 Objectives of the Study .......................................................................................... 8
1.3.1 General Objective................................................................................................ 8
1.3.2 Specific Objectives.............................................................................................. 8
1.4 Research Questions ................................................................................................ 8

viii
1.5 Significance of the Study ....................................................................................... 9
1.6 Limitations of the Study ......................................................................................... 9
CHAPTER TWO ..................................................................................................... 11
LITERATURE REVIEW ........................................................................................ 11
2.1 Conceptual Definitions ........................................................................................ 11
2.1.1 Ergonomics ....................................................................................................... 11
2.1.2 Workplace ......................................................................................................... 13
2.1.3 Workplace Ergonomics ..................................................................................... 13
2.1.4 Ergonomics Risk Factors (ERFs) ...................................................................... 13
2.1.5 Musculoskeletal Injury and Disorders (MSD) .................................................. 14
2.1.6 Employee Performance ..................................................................................... 14
2.1.7 Performance Management ................................................................................ 14
2.1.8 Performance Review ......................................................................................... 15
2.2 Theoretical Literature Review.............................................................................. 15
2.2.1 Ergonomics Science Theory ............................................................................. 15
2.2.2 Theories on Employees’ Motivation for performance and Ergonomics ........... 16
2.3. Empirical Review ................................................................................................ 18
2.3.1 Factors Affecting Performance ......................................................................... 18
2.3.2 Ergonomic Considerations at the Workplace .................................................... 20
2.3.4 Workplace ergonomics and Healthcare Employees .......................................... 22

ix
2.3.5 Workplace Ergonomics Awareness .................................................................. 24
2.4 Conceptual Framework ........................................................................................ 25
CHAPTER THREE ................................................................................................. 27
RESEARCH METHODOLOGY ........................................................................... 27
3.1 Study Area ............................................................................................................ 27
3.2 Research Paradigm ............................................................................................... 27
3.3 Research Design ................................................................................................... 28
3.4 Population, Sample method and Sample size ...................................................... 28
3.4.1 Study population ............................................................................................... 28
3.4.2 Sampling procedures ......................................................................................... 29
3.4.3 Sample Size ....................................................................................................... 29
3.5 Types of Data and Data Collection Techniques ................................................... 30
3.5.1 Primary Data ..................................................................................................... 30
3.5.1.1 Questionnaire ................................................................................................. 31
3.5.1.2 Interview ........................................................................................................ 31
3.6 Validity and Reliability ........................................................................................ 31
3.7 Data Measurement and Analysis .......................................................................... 32
3.8 Ethical Issues ........................................................................................................ 32
CHAPTER FOUR .................................................................................................... 34
PRESENTATION OF FINDINGS ......................................................................... 34

x
4.1 Introduction .......................................................................................................... 34
4.2. Socio-demographic data of the respondents ....................................................... 34
4.2.1 Gender of respondents ...................................................................................... 34
4.2.2 Age distribution of respondents ........................................................................ 35
4.2.3 Field of work ..................................................................................................... 35
4.2.4 Level of work .................................................................................................... 36
4.2.5 Department/unit................................................................................................. 36
4.2.6 Working experience .......................................................................................... 37
4.3 Research Question 2: Level of health care employee’s awareness on workplace
ergonomics ................................................................................................................. 37
4.4 Health care employee’s satisfaction with the offices/workplaces........................ 39
4.5 Workplace ergonomics and employee’s health and safety .................................. 41
4.6 Research Question No. 1: Workplace ergonomics and healthcare employee’s
performance................................................................................................................ 45
4.6.1 Correlation......................................................................................................... 48
4.6.2 Regression ......................................................................................................... 49
4.7.1 Old design of the hospital ................................................................................. 50
4.7.2 Old infrastructure of the hospital ...................................................................... 51
4.7.4 Space limitations ............................................................................................... 53
4.7.5 Insufficient staffing ........................................................................................... 53

xi
4.7.6 Budgetary constraints ........................................................................................ 54
4.7.7 Technological factors ........................................................................................ 55
4.7.8 Respondents’ suggestions on improving comfortability, safety, health and
security at workplace.................................................................................................. 56
CHAPTER FIVE ...................................................................................................... 58
DISCUSSION OF FINDINGS ................................................................................ 58
5.1 Introduction .......................................................................................................... 58
5.2 Workplace ergonomics and healthcare employee’s performance ........................ 58
5.3 Health care employee’s awareness on workplace ergonomics ............................ 60
5.4 Barriers toward ergonomic design of workplaces ................................................ 60
CHAPTER SIX ........................................................................................................ 63
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS ......................... 63
6.1 Introduction .......................................................................................................... 63
6.2 Summary .............................................................................................................. 63
6.3 Conclusion ........................................................................................................... 64
6.4 Recommendations ................................................................................................ 65
6.5 Areas for further study ......................................................................................... 66
REFERENCES ......................................................................................................... 67
APPENDIX II ........................................................................................................... 84
xii
LIST OF TABLES
Table 3. 1: Sample of Informants and its Distribution .............................................. 30
Table 4. 1: Gender of respondents ............................................................................. 34
Table 4. 2: Age distribution of respondents ............................................................... 35
Table 4. 3: Field of work ............................................................................................ 35
Table 4. 4: Level of work ........................................................................................... 36
Table 4. 5: Directorates .............................................................................................. 36
Table 4. 6: Working experience ................................................................................. 37
Table 4. 7: Level of health care employee’s awareness on workplace ergonomics .. 39
Table 4. 8: Level of health care employee’s satisfaction with office......................... 41
Table 4. 9: Healthcare employee’s performance........................................................ 47
Table 4. 10: Model summary of the study ................................................................. 49
Table 4. 11: ANOVAa ................................................................................................ 49
Table 4. 12: Coefficients ............................................................................................ 50
xiii
LIST OF FIGURES
Figure 2. 1: Maslow’s Hierarchy of Needs(Source:(Maslow, 1954)) ........................ 17
Figure 4. 1. Office space and workplace ergonomics (Source: Survey Data,
(2020)) ........................................................................................................................ 41
Figure 4. 2. Office space and workplace ergonomics (Source: Survey Data,
(2020)) ........................................................................................................................ 42
Figure 4. 3. Level of stress (Source: Survey Data, (2020))........................................ 43
Figure 4. 4. Effect on employee’s health (Source: Field Findings, (2020)) .............. 44
Figure 4. 5: Injury (Source: Survey Data, (2020)) ..................................................... 45
Figure 4. 6: Old design of the hospital (Source: Field Findings, (2020)) .................. 51
Figure 4. 7: Old infrastructure of the hospital(Source: Survey Data, (2020)) ........... 51
Figure 4. 8: Patient congestion (Source: Survey Data, (2020)) ................................. 52
Figure 4. 9: Space limitations (Source: Survey Data, (2020)) ................................... 53
Figure 4. 10: Insufficient staffing (Source: Survey Data, (2020) .............................. 54
Figure 4. 11: Budgetary constraints (Source: Survey Data, (2020)) .......................... 55
Figure 4. 12: Technological factors (Source: Survey Data, (2020)) .......................... 56

1
CHAPTER ONE
PROBLEM SETTING
1.1 Background of the Study
Over the past several decades, studies on ergonomics design of workplaces has
attracted high research interests by many researchers in different countries due to its
significant contribution on performance in various industries i.e., manufacturing and
service organizations. This is because workplace ergonomics has been found to be
one of the critical factors for enhancing employees’ performance at workplaces. The
quality of workplace environment has a significant impact on the level of employee’s
motivation and subsequently on their performance (Kingsley, 2012). Furthermore, it
has been established that the level of employee engagement within the organization,
especially with their working environment, has a significant contribution on the
mistakes made, rate of errors, level of motivation and how well the employees interact
and relate amongst themselves at the workplace. It also has an effect on absenteeism
as well as job retention determination within an organization (Al-Anzi, 2009).
The World Health Organization has established that the workforce is among the six
building blocks of a health system and emphasized on giving the desired focus and
consideration to that valuable resource (WHO, 2010). By recognizing the importance
of workforce, there should be significant consideration on improving workplace
conditions as the motivational factors for employee performance (Tarus, 2011).
Furthermore, WHO recognizes the health workforce to include all employees engaged
in activities or actions whose primary intent is to enhance health services. Among the
motivational factors for health care employees is the setup of the working environment
which includes design and layout of the office, furniture and equipment. In workplace
ergonomics, all these should fit the human i.e. the employee using them (Al-Anzi,
2009).
2
Accordingly, the workplace ergonomics considerations include thermal comfort
which indicates the right combination of temperature, airflow and humidity (Carmen,
2013; Mendis, 2016). There are also many other factors that have a significant
contribution on the level of performance and productivity at the workplace which
include wellness and comfort in the design of the office, availability and design of
machinery and the working tools. Other factors are vibration, noise and hygiene
(Pickson, 2017). The word ergonomics has its origins from Greek and it comes from
the words “ergo” which stands for work and “nomics” which means study (Te-Hsin
and Kleiner, 2001). It is further defined as the science of designing a workplace to fit
the needs of the user (Dul and Weerdmeester, 2008) According to the Washington
State Department of Labour and Industries (2002) a safer and healthy work
environment is created when there are ergonomic improvements to the work
environment and that is the primary use of ergonomics (Kingsley, 2012).
According to the IEA, ergonomics is a scientific study on the interactions and
compatibility between people and other aspects of his life or environment including
machines, tools and systems. It takes into consideration the theories and principles that
aim to design machines, tools and work environment in a way that fits the people using
them in order to optimize performance (Dul and Weerdmeester, 2008). The ergonomic
way of designing the workplace and environment aims at minimizing the risks of
injuries or harm that may occur at the work place by establishing safe, comfortable
and productive workplaces which consider human abilities and limitations into the
design of a workplace (Kingsley, 2012). Matching workplace environment with
employees’ needs is very essential for an organization to obtain their maximum
contribution towards the organizational objectives. Employees’ morale, productivity
and engagement is affected by the workplace environment both positively and
negatively. An unsafe and unhealthy work place environment is exhibited by poorly
designed workstations, unfitting furniture, lack of enough ventilation, poor lighting,
excessive noise, inadequate safety measures in case of fire and other emergencies as
well as lack of protective gear against the various workplace hazard (Mendis, 2016).

3
Ergonomics is one of the strategic tools that can be used to attract and retain well
performing employees in an organization since it applies information about human
behaviour, abilities and limitations and other characteristics to the design of tools,
machines, tasks, jobs and environments for productive, safe, comfortable and effective
human use (McCormick and Sanders, 1992). According to the Ireland Health and
Safety Authority (2015) which has published a number of books and articles on the
subject of ergonomics, in proactive ergonomics emphasis is put on the prevention of
work related musculoskeletal disorders by taking cognizance of and reducing the risk
factors during planning stages of new systems of work and workplaces.
Ergonomics is one of the factors in occupational health and safety. According to the
ILO, occupational health and safety and ergonomic issues are on the rise and from the
2.78 million work-related deaths recorded, 2.4 million are a result of occupational
diseases and injuries (ILO, 2013). Some of the effects of the occupational diseases and
injuries include early retirements, loss of skilled workforce and absenteeism which all
have significant impact on productivity. In the ILO report, occupational accidents and
diseases not only affect the GDPs of the affected countries but also globally, estimated
at a 4 percent loss. According to Alli (2008), the financial impact from the injuries and
deaths arising from occupational health and safety are colossal at the organizational,
national and international levels due to the compensation costs, loss of working time,
medical expenses and production interruptions. The ILO is mandated to ensure that
workers are protected against work related diseases and injuries risk factors by
developing international standards (Shengli, 2010).
The ILO has adopted more than 40 instruments on various health and safety issues
among them is the Working Environment (Air pollution, Noise and Vibration)
Convention No. 148 of 1977. The Convention has been ratified by 46 countries
including the United Republic of Tanzania which has ratified the same on-air pollution
only. Noise and vibration are among the working environment considerations in
ergonomics.

4
Looking at ergonomics in the developed countries, also referred to as the Industrially
Advanced Countries, they are seen to have more advances in the knowledge and
application of ergonomics and its principles. Most of the ergonomics principles were
originally formulated the IACs and there is significant improvement on ergonomics
applications in the countries (Shahnavaz, 2000). This is because of the technological
advancement in the countries, lower levels of poverty and the smallness of their
populations as compared to the IDCs. The level of ergonomic awareness, applications,
advancements in the IACs can be seen through the richness of literature on the subject
and the systematic approach of addressing ergonomics issues including the formation
of ergonomics societies in most of the countries. However, over the past few decades
there has been a significant improvement and interest on ergonomics in the IDCs as
seen through various publications (Huck and Richardson, 2012).
As for developing countries, also referred to as Industrially Developing Countries,
they are mostly characterized by larger populations, higher levels of poverty and lesser
advancements in technology making them to have the greatest needs in improvement
of ergonomics (O’Neil, 2000). The IDCs have challenges of poor infrastructure and
insufficient finances to facilitate and support ergonomic applications and interventions
(Jafry and O'Neil, 2000). These challenges, as suggested by (Mc Neill et.al, 2000) are
the attributes toward low machine utilization, insufficient skills, unmotivated
workforce, excessive environmental hardships and heavy physical loads. Most of the
IDCs rely on agriculture which has extremely difficult conditions including heavy
work and poor working tools. It is suggested that the rate of injuries resulting from
accidents in the workplaces in the IDCs is significantly higher than that of the IACs
(Jafry and O'Neil, 2000).
Tanzania as one of the IDCs has limited knowledge and awareness on the subject of
ergonomics and as a result there is sanctity of research material and publications on
the subject. Like other IDCs, Tanzania faces the same challenges in ergonomics
development as discussed. In cognizance of the issues of employees’ welfare including
safety at the workplace, and the ILO’s efforts to ensure that employers provide
5
workplaces are safe for the employees, the Government of Tanzania has taken
initiatives to improve health and safety. The Occupational Health and Safety Act, No.
5 of 2003 was enacted for the purpose of making provisions for the safety, health and
welfare of employees at their workplaces. The Act has also established the
Occupational Health and Safety Authority (OSHA) which is mandated among other
things to oversee the implementation of the Act and to advise the Government of the
United Republic of Tanzania on issues of health and safety of the workplace. Among
the activities undertaken by OSHA in enhancing health and safety of workers is risk
assessment of workplaces, statutory inspection as well as scrutiny and approval of
workplace drawings and plans.
Furthermore, through the National Employment Policy of 2008, the Government of
United Republic of Tanzania undertakes to continue enforcing health and safety in the
workplaces by ensuring that they are conducive to physical, psychological and social
wellbeing of the workforce (National Employment Policy, 2008). In addition to that,
the National Occupational Health and Safety Policy was developed in 2009. The
Policy emphasizes on the importance of occupational health and safety for sustainable
development enhanced through reduction of occupational accidents and diseases
which have a negative impact on individual, enterprise and national levels. It further
recognizes the positive impact of health and safety of the workers in productivity,
higher morale, job satisfaction and hence industrial harmony (National Occupational
Health and Safety Policy, 2008). The undertaking of the Policy is to improve health
and safety for workers through regular review of legislation and standards as well as
creating awareness on health and safety culture among workers and employers.
The Muhimbili National Hospital (MNH), the case for this study, has its origins going
back to the 1910 to 1920s when it was known as Sewahaji Hospital and 1956 when it
was known as Princess Margareth Hospital, the MNH was established as an
autonomous public institution by the Muhimbili National Hospital Act No. 5 of 2000.
This was after the dissolution of the previously existing Muhimbili Medical Centre
and the establishment of the hospital and the university as two separate entities
6
(Muhimbili National Hospital Act, 2000). The Hospital has a bed capacity of 1,500
beds for inpatients and attends an average of 2000 outpatients per day. The Hospital
has a total of around 2,700 employees of whom about 300 are doctors, 1,200 are nurses
and health attendants while the rest are supporting operational employees (Muhimbili
National Hospital, 2019). The Hospital’s vision is to be a centre of excellence in
specialist and highly specialized services in medicine, training and research by 2022
and the mission is to provide sustainable, effective, efficient and high quality tertiary
specialist services and highly specialized medical services for local and international
referred patients, as well as providing conducive environment for training and research
(Muhimbili National Hospital, 2017).
1.2 Statement of the Problem
Over a period of several years the demand for improved performance in the public
health facilities has been increasing. This started with the integration of private
practice in public institutions whereby they were required to attend private patients as
a means of increasing their financial capacity (Museru and Grobb, 2003). This means
that public health facilities were to compete with private facilities in order to attract
private patients and thus were expected to operate more efficiently similar to private
facilities. Furthermore, the demand for improved performance in public health
facilities has continued to increase whereby public health facilities are expected to
improve performance by introducing new tertiary services which before required
patients to be referred abroad as they were not available in the country.
Despite this increased demand and expectations which reflects the need for
improvement of employees’ performance, public health facilities in Tanzania have not
considered workplace ergonomics as a tool for improvement of employees’
performance. Rather, public institutions’ efforts to improve performance are directed
to appraisals, performance contracts, trainings and monetary incentives. Performance
assessment in the public institutions is currently mostly done by using the Open
Performance Appraisal System (OPRAS) which was introduced by the Tanzania
Government in 2004 (Nchimbi, 2019). However, such traditional tools used for
7
assessment and improving performance have not been very successful as they do not
take into consideration the issue of workplace ergonomics as among the factors which
enhance employee and ultimately organizational performance.
It has been established that a well-designed facility will facilitate the smooth and
quality delivery of services (Haynes, 2008). This will also allow the optimal utilization
of the space, reduce likelihood of injury and ensure safety, which are all favorable
factors for improved performance. However, failure of public health institutions to
consider workplace ergonomics has led to having unfavorable working conditions.
This has resulted in, among others, complaints of musculoskeletal injuries and back
pain, for example, anecdotal evidence shows that back pain is one of the major
complaints among the nursing staff of Muhimbili National Hospital.
These complaints are the cause of many cases of absenteeism and demands for light
duty, and excuse duty which eventually impact the performance. According to
(Yankson, 2012), when studying the effects of health and safety standards on
productivity in the rubber industry in Ghana, employees working in an unfavorable
working environment may be observed to be not as productive as those in favorable
conditions because they have to cope with many hazards and other factors that put
their safety at peril for example too much noise, handling and using dangerous
equipment or machines that may cause injury or health problems to them.
Though the significance of the study of ergonomics is undisputable it has been
observed that there is an insufficient awareness about the subject and its applications
in the diverse occupations and professional groups varying from manual workers to
IT professionals (Pandve, 2016). In a pilot study on ergonomics awareness (Pual,
2012) found that 53% of the nurses were not aware about ergonomics and safety
measures and 75% were not following ergonomics and improper lifting and patient
handling techniques could have led to musculoskeletal injuries among them.
This research aims to study employee and management awareness on the concept of
workplace ergonomics, the extent to which employees are satisfied with the
8
ergonomics at their work stations and thus bring to light the role of workplace
ergonomics in the public health sector so that decision makers (the Hospital’s
Management and the Government) will put more efforts in improving workplace
ergonomics in public health facilities.
1.3 Objectives of the Study
1.3.1 General Objective
The main objective of this study is to assess the role of workplace ergonomics on
healthcare employee’s performance, the case of Muhimbili National Hospital in
Tanzania.
1.3.2 Specific Objectives
The specific objectives for this study are:
i. To determine the extent to which workplace ergonomics influence
healthcare employees’ performance at workplace, the case of
Muhimbili National Hospital.
ii. To examine healthcare employees’ awareness about ergonomics design
of the workplaces, the case of Muhimbili National Hospital.
iii. To document the barriers towards ergonomic design of workplaces as
a tool for improving employees’ performance in healthcare facilities,
the case of Muhimbili National Hospital.
1.4 Research Questions
The study was guided by the following research questions: -
i. To what extent does workplace ergonomics influence the performance of
healthcare employees at Muhimbili National Hospital?
9
ii. Are the healthcare employees aware about ergonomics design of
workplaces, at Muhimbili National Hospital?
iii. What are the barriers towards ergonomic design of the workplaces as a
tool for improving employees’ performanceat Muhimbili National
Hospital?
1.5 Significance of the Study
This study aims at assessing the role of ergonomics to the performance of employees
in the healthcare industry with the aim of also assessing the awareness of both the
employees and the management on the subject of ergonomics. The findings from this
study provided the management with the clear picture on the role of ergonomics of the
workplace and the importance of taking it into consideration when developing its
strategies to improve productivity and the institutional performance. The significance
of this study is not only limited to MNH but the health services at large. Being the
national referral Hospital in Tanzania, Muhimbili National Hospital has significance
influence on other public and private hospitals hence any improvement at MNH is
mostly likely to trickle down and impact the health sector in Tanzania.
1.6 Limitations of the Study
The conduction of this research faced some of limitations which were most of the
employees in the public health sector and specifically at the Muhimbili National
Hospital have tight work schedules due to the sensitivity and high demanding nature
of the services being provided by them hence timely response to questionnaires was a
challenge. In addressing this issue, the researcher used online google forms whereby
the questionnaire forms were shared through the google forms link through WhatsApp,
this was only for few respondents who failed to respond timely and found it harder to
fill manual forms. Furthermore, there was scanty local literature on this subject, the
researcher used the available international literature just to fill that gap.
10
1.7 Organization of the Report
This study is organized into five chapters as follows:
Chapter one provides an introduction covering background of the study covering an
overview of workplace ergonomics and how it is being practiced in both developed
countries, developing countries and the situation in Tanzania. The chapter further
presents statement of the research problem, the research objectives, research questions
and significance of the study.
Chapter two presents and examines the various concepts on the subject of workplace
ergonomics by reviewing relevant previous studies’ findings and contributions on the
same. The chapter provides an understanding on the concept of workplace ergonomics
and explores on workplace ergonomics in health delivery. It further provides
theoretical review and critical review on empirical literature in the area of study and
provides the conceptual framework.
Chapter three offers the manner in which sources and information for the study were
obtained. It covers the research design for this study, study area, sample and sampling
procedures, data sources and types, data collection techniques and data analysis.
Chapter four, chapter five, chapter sixoffer the presentation of all the findings from
the field, the discussions of all the findings in relation to theories and empirical studies,
the conclusions, recommendations and areas for further studies respectively.

11
CHAPTER TWO
LITERATURE REVIEW
2.1 Conceptual Definitions
2.1.1 Ergonomics
Ergonomics is a scientific study on the interactions between people and some aspects
in their use including the general environment, equipment and systems (International
Ergonomics Association, 2010). In workplace ergonomics all the aspects in contact or
in use by a person should take into consideration the suitability on such person to allow
easy and smooth implementation of tasks, reduce the likelihood of injuries including
any repetitive movements that strain the body and cause muscular discomfort and
injury. The aim of ergonomics is to facilitate designing of tools, machines,
workstations and systems that are well fitted for human beings and consider human
abilities and limitations (Roeloelofsen, 2002). The IEA uses the word human factors
and ergonomics interchangeably or separately as units because one cannot separate
human factors and ergonomics (IEA, 2012).
Ergonomics is categorized into two braches i.e. macro-ergonomics and micro-
ergonomics. Macro-ergonomics is focused on the wider aspect of social-cultural and
organizational system issues which include culture (attitude, religious beliefs etc.),
infrastructure and climate. On the other hand, micro-ergonomics focuses on the
individual and his/her physiological, psychological and cognitive aspects i.e. the man-
machine interaction (Dul and Weerdmeester, 2008). According to O’Neill and Albin
(2011), office ergonomics should have a holistic approach integrating not only
engineering and cognitive aspects but also a wider aspect of issues that are to be
considered in designing the workplace and the work. The holistic approach to
ergonomics looks into the physical, psychological and social factors in the application
of ergonomics.

12
Figure 2.1: Holistic ergonomics
(Source: (O’Neill and Albin, 2011))
The physical factors of ergonomics relate to physical activity and include the force
used to fulfill the task, duration of the task and frequency of the task. Such activities
include lifting of objects, handling of machines and other materials, working postures
as well as the design, health and safety of the workplace. The psychological or mental
aspects of ergonomics are related to the compatibility of the machines, tools and
systems with the cognitive ability of the user. These factors focus on the user’s human
perception, reasoning and memory and they are sometimes referred to as cognitive
psychological factors. As for the social aspect of ergonomics, this refers to the social
component of employee’s collaboration within the organization and includes factors
like employee’s mentoring and learning, participation in the organization’s systems,
structures, policies and processes (McCormick and Sanders, 1992).
13
2.1.2 Workplace
The term workplace generally means the area in which employees perform their work
and it includes the work and non-work area, the equipment and all other facilities used
in the performance of work (Chim, 2017).
2.1.3 Workplace Ergonomics
Workplace ergonomics is the consideration of various human factors in designing
effective, safe work stations and systems of the workplace. These factors include
environmental conditions, sitting postures, movements, weight lifting and body strain.
Various researchers have defined the concept of workplace ergonomics in related
terms. By some it has been defined as a branch of science concerned with the
achievement of optimal relationships between workers and their work environment
(Tayyari and Smith, 1997). On the other hand, according to Fernandez (1995)
workplace ergonomics is about designing the work equipment, machines, tools,
product, environment and systems by taking into account the human’s physical,
physiological, biomechanical, and psychological capabilities in order to optimize the
effectiveness and productivity of work systems while assuring safety, health and
wellbeing of the workers. In general terms, in workplace ergonomics emphasis in
designing is to fit the workplace and work to the individual and not vice versa. It is
further asserted that a variety of conditions of a workplace can affect the worker’s
comfort and health and these include factors like workstation design, tool and machine
design, furniture (chair) design, heavy lifting, motion and other environmental factors
like temperature, noise, vibration and lightning (Jaffar et al. 2011).
2.1.4 Ergonomics Risk Factors (ERFs)
Risk factors can be defined as all those conditions or circumstances that increase the
likelihood of occurrence of an accident or injury. ERFs include repetitive movements,
awkward positioning of the body, heavy lifting and extreme temperatures in the office
or working environment, which if not well addressed may affect performance
(Jagannath and Adalarasu, 2012). A workplace ergonomics design or improvement
14
process removes all of these risk factors that have been found to be the cause of
musculoskeletal injuries and disorders and allows for an improved human
performance and productivity (Chim, 2017).
2.1.5 Musculoskeletal Injury and Disorders (MSD)
Musculoskeletal injuries and disorders are injuries or pains in the musculoskeletal
system of the human body, including joints, ligaments, muscles, nerves, tendons and
the structures that provide support to the limbs, neck and back such as the spinal disks
(Kumar, 2001). According to the Centre for Disease Control and Prevention (CDC),
(2015), injuries can be caused by a sudden or sustained exposure to repetitive motion,
vibration, use of force and awkward positioning of the body. MSDs result from the
human body’s interaction with physical factors, ergonomics and occupational factors
(Gatchel and Kishino, 2011). MSDs have been an issue of increasing concern globally
and it is among the leading causes of disability (ILO, 2013). The risk factors for MSDs
have been categorized into biomechanical factors, individual differences,
psychosocial and occupational factors.
2.1.6 Employee Performance
Employee performance is defined as the level of execution of job related activities
(Karakas, 2010). Normally, every organization has its goals, objectives and activities
and such goals are assigned to the employees in their respective roles which are then
measured to determine performance. Therefore, the dimensions of employee
performance evolve around setting strategic goals, maintaining standards, motivation
and supervision of subordinates to ensure accomplishment of tasks (Tripathy, 2014).
2.1.7 Performance Management
Performance management is the systematic and ongoing process of managing the
achievement of the organizational goals which include planning, monitoring,
evaluating and reviewing the performance. The process involves setting of strategic
objectives, identifying activities and indicators for performance, feedback provision
and review of the results (Pradhan and Jena, 2016). Performance management not only
15
assists an organization in meeting its strategic plans but also in making decisions with
regards to improvement of working conditions, employee development, employee
motivation and the overall management of the human resource (Pulakos, 2004).
2.1.8 Performance Review
This is a method through which organizations measure the implementation of
activities assigned to individual employees on a frequent basis such as semiannual or
annual reviews (DeNisi and Pritchard, 2006). According to Hellriegel (2014),
performance management is an essential part of human resources management and an
effective performance management system is imperative for organizational success.
2.2 Theoretical Literature Review
The following are the theories that relate to this study and help in understanding the
whole concept and relationship between workplace ergonomics and employee
performance in an in-depth and broader understanding.
2.2.1 Ergonomics Science Theory
The theories on ergonomics science started approximately 80 years ago during the
Second World War from the need to address the complex handling of military
equipment when it was realized that use of knowledge on technology and human
sciences was needed, in a systematic and coordinated manner (Sanders, 1992). This
included the use of interdisciplinary approach involving Physiologists, Psychologists,
Anthropologists, Medical Doctors, Engineers and Work Scientists to address the
challenges. After such successful developments, the interest in ergonomics grew fast
especially in the European countries and in 1949 the International Ergonomics
Association with representation from more than 40 countries was established (Ghosh
et al. 2011). This theory has significantly contribution and is what later led to what is
called workplace ergonomics. Based on the ergonomics science theory, several
ergonomic recommendations have been suggested in various empirical studies in
respect of conditions of work places and have been providing guidance in designing
of workplaces, systems and operations (Pickson, 2017).
16
2.2.2 Theories on Employees’ Motivation for performance and Ergonomics
It is important to understand the role of motivation on employee performance, since
workplace ergonomics has been identified as one of the motivational factors for
performance (Tarus, 2011). The following theories on employee’s motivation are
discussed in relation to workplace ergonomics and performance.
Maslow’s Theory of Hierarchy of Needs
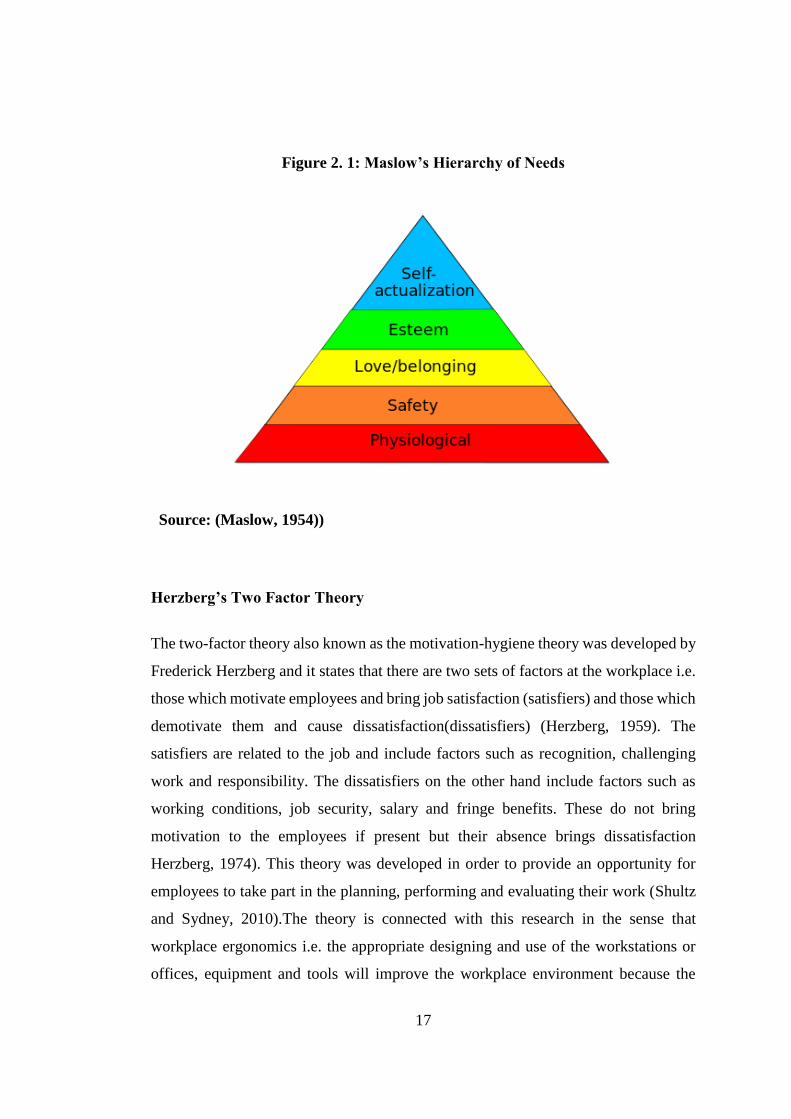
This theory which is also referred to as Maslow’s Triangle was developed by Abraham
Maslow, it suggests that people are motivated with needs categorized in five levels
which are physiological needs, safety, belonging, esteem and self-actualization in the
same hierarchy (Maslow, 1954). The two basic level needs in the theory are relevant
in understanding the relationship between workplace ergonomics and employee
performance which are physiological and safety needs. As shown in figure 1, the
physiological level are the basic needs for sustaining human life such as food, water,
shelter, health, clothes and sleep. These according to Maslow are what are considered
in internal motivation. The theory further states that people are compelled to have
these needs fulfilled first before pursuing other higher level needs (Deckers, 2018). It
is suggested that once the physiological needs are fulfilled, the safety needs are next
in importance and these include among others safety needs against accidents, injuries
and illnesses which are the important factors in employee performance.
17
Figure 2. 1: Maslow’s Hierarchy of Needs
Source: (Maslow, 1954))
Herzberg’s Two Factor Theory
The two-factor theory also known as the motivation-hygiene theory was developed by
Frederick Herzberg and it states that there are two sets of factors at the workplace i.e.
those which motivate employees and bring job satisfaction (satisfiers) and those which
demotivate them and cause dissatisfaction(dissatisfiers) (Herzberg, 1959). The
satisfiers are related to the job and include factors such as recognition, challenging
work and responsibility. The dissatisfiers on the other hand include factors such as
working conditions, job security, salary and fringe benefits. These do not bring
motivation to the employees if present but their absence brings dissatisfaction
Herzberg, 1974). This theory was developed in order to provide an opportunity for
employees to take part in the planning, performing and evaluating their work (Shultz
and Sydney, 2010).The theory is connected with this research in the sense that
workplace ergonomics i.e. the appropriate designing and use of the workstations or
offices, equipment and tools will improve the workplace environment because the

18
absence of such favourable environment may bring dissatisfaction to employees and
affect their performance.
Both theories concentrate on the human factors i.e. the physiological and
psychological factors which motivate employees to perform optimally. For instance,
motivation is considered as an important element in the design and creation of working
equipment (Maslow, 1954). Since workplace ergonomics is all about having a
workplace that meets the needs of the user i.e. the employee, the theories help in
providing a deeper understanding of the importance of workplace ergonomics on
employees’ motivation and performance.
2.3. Empirical Review
Several studies have been made on the science of workplace ergonomics and its
implications on employee performance in the various sectors. This is because it is
undisputable that employees are the most valuable asset in any organization or
company and most employers would want to address any factors that may hinder the
optimization of the human resource. As stated in the theoretical review, some scholars
tried to establish the factors enhancing or affecting performance by trying to
understand what motivates them to perform and what demotivates them.
2.3.1 Factors Affecting Performance
It is important in this study to review literature of employee performance and factors
affecting it. Some studies have indicated the existence of a strong relationship between
the work environment, including work place design and use of machines and tools,
and the level of employee performance. Mendis (2016) in a study on operational level
employees in the apparel industry of Sri Lanka, found that improvement of work place
ergonomics (equipment, workplace layout, lighting and ventilation) resulted into
increased performance of the employees. In yet another study, Al Anzi (2009)
concluded that employee performance is affected by two categorized factors namely
the management driven factors and factors related to the office or factory design. The
management driven factors include organizational plans, job descriptions and

19
management support while those related to the premises include availability of work
space, furniture ventilation and humidity as well as temperature.
However, Al Anzi (2009) did not consider cognitive factors to be equally important
factors affecting performance but concentrated only on managerial issues and
premises which by themselves only may not enhance performance. This is because
even the best premises and equipment must be complemented with the employee’s
cognitive skills in optimizing them. The cognitive skills include correct reasoning and
judgment as well as a good memory and perception. This approach was also taken by
Leblebici (2012) who considered the factors affecting performance in two categories
of physical components and behavioural components. The physical components are
office layout and space, ventilation, temperature, physical security and overall comfort
of the employee. The behavioural components on the other side include the
employee’s level of interaction and distraction with the physical environment and
equipment.
In a study on the effect of ergonomics on employee performance in the butchering and
trimming line of canned food in Ghana, Pickson et al. (2017), established that there
was a positive correlation between workplace ergonomics and employee performance.
Furthermore, it was found that the physical environment and comfort of the workplace
had a direct link to the office occupants’ performance, although it was observed that
comfortability could be subjective and that there was no clear and generally accepted
description of what a comfortable workplace would be assessed (Haynes, 2008).
However, there are several studies on what would be regarded as a comfortable work
place as seen through various publications including those by the IEA and other
ergonomic associations around the world which provide the dimensions of a
comfortable work place, furniture, equipment and even the job itself (Fernandez,
1995).

20
2.3.2 Ergonomic Considerations at the Workplace
It has been suggested that a workplace which has considered ergonomic principles in
its design will result in less musculoskeletal discomfort, increased performance and
efficiency, reduce operational costs and even enhance more utilization of the human
resources (Al-Anzi, 2009). According to Carmen (2013) ergonomic considerations
include the overall comfortability of the workplace with regards to temperature,
humidity and airflow. The ergonomic considerations and interventions should be able
to address both macro-ergonomic factors and micro-ergonomic factors hence
ergonomic interventions should address the factors discussed below.
Work stations Design
Work station refers to the overall location in which employees perform their work and
includes all facilities and equipment used for performing the work. In most offices the
work station would include the layout, space, desk, chair, space, and a computer set
up (Chinyere, 2014). All these should be designed and fitted to the physical and
psychological comfort of the employees and enhance their performance (Olabode et
al. 2017).
Working Posture
Posture is the automatic and unconscious body positioning assumed for purposes of
providing body balance when in space (Carini et al. 2017). The IEA has established
that working postures and movement are among the issues in physical ergonomics
when addressing musculoskeletal health, together with material handling and
workplace layout. Working postures and movement are considered important factors
in occupational health and must be considered in the physical exertions that cause
musculoskeletal disorders (Vieira and Kumar, 2004). According to Kumar (2001),
“awkward, constrained, asymmetric, repeated and prolonged posture can overload
tissues and exceed their thresholds of tolerable stress, causing injury due to
overexertion or imbalance”.
21
Although Mc Neill et al. (2000) argued that awkward posture may vary from culture
to culture giving an example of sitting posture which are considered normal in the
Indian culture, a posture cannot be ideal if it poses as a risk factor in musculoskeletal
injury. It has been emphasized in literature that although there may not be an “ideal”
working posture, there are inarguably postures that are healthier and more comfortable
than others (Marmaras and Nathanael, 2016). In a study on safe postures in manual
lifting work for construction workers, Adeyemi et al. (2014), revealed that safe posture
among the workers who handle manual lifting work was very low and had significant
impact in musculoskeletal stress.
Noise
Noise is any unwanted and unpleasant sound that is disruptive to the human being.
There are many factors that affect human performance among them being the working
conditions including noise (Kahya, 2007). Noise is among the factors that constitute
the working environment and noise management is a significant factor in ergonomics
considerations (Qutubuddin et al. 2012). Nassiri et al. (2013) found that the impact of
noise was significant in reducing human performance and responsible for making
difficult working environment conditions at the workplace.
Manual Lifting
Lifting is defined as the act of carrying or moving something from one position to
another (Coenen et al. 2014). It has been established in some studies that there is a
strong association between manual frequent lifting and incidences of LBP and that
lifting more than 25kgs potentially increased the rate of LBP incidences by 4.3%
(Coenenet al. 2014). Manual lifting of objects and patients was found to be the leading
factors of LBP among nurses in a cross sectional study in the Benghazi Medical Centre
in Libya whereas it was found that half of the nurses cited LBP as the reason for their
absenteeism and low performance (Mukhtad, 2017). In a study on employees at a
medical warehouse at a hospital in Belgium it was concluded that proper lifting
22
techniques can help in reducing the time spent on postures that are harmful for the
back which increase incidences of LBP (Matthys et al. 2019).
2.3.4 Workplace ergonomics and Healthcare Employees
Health/healthcare is one of the most important sectors in any society as it has a
significant contribution to the economic development as it is indisputable that a
healthy population is a productive population. It has been argued that health
improvement is one of the determinants and methods to facilitate the economic
development and poverty reduction in any society (Husain, 2010). According to the
WHO, health workforce is among the six pillars of a successful health delivery system
and it is of utmost importance. Hospitals and health services facilities generally
provide health services, patient care and other supportive non- health services hence
hospital workforce comprises of diverse groups of professions (Janowitz et al. 2006).
It has been reported in various studies that hospital employees face various risks which
expose them to work related injuries and diseases such as MSDs especially those who
are involved in direct patient care.
Hospital employees are exposed to greater risks of muscles strains such as back strains
and other MSDs caused by their work, at a higher rate than employees working in the
manufacturing, mining and construction industries (Kim, 2017). In assessing
ergonomics risks for Hospital employees, Jagannath and Adalarasu (2012) concluded
that workers had multiple musculoskeletal issues which had a significant effect on the
performance of their activities and life. Some of the reasons sighted for poor
performance included improper work plans, lack of enough professions to meet
requirements of high patients’ admissions, inappropriate furniture and quality of
equipment.
Empirically, it has been found that consideration of workplace ergonomic factors in
design and operationalization of equipment, systems, processes and jobs led to
increased patient safety (Carayon et al. 2013). Some reports have shown that factors

23
related to workplace conditions had a direct influence on the errors in the health
service delivery. Consequently, workplace ergonomics has been recognized as a
mitigation factor in reducing errors and elimination of hazards (Ulmer et al. 2008). In
addition to that, workplace ergonomics applications in health care domain has been
found to maximize the overall performance while ensuring the health, safety and
comfort of not only the health worker but also the patient (Gurses et al. 2009).
Furthermore, some studies found that the benefits of good workplace ergonomics were
seen not only on the health worker’s performance but also the workers’ quality of life
improved due to the reduced work load and body discomfort (Smith et al. 2009).
In the hospitals, apart from office ergonomics for which considerations are to be made
in office set up, furniture, computers and work stations set up, noise and temperatures,
workplace ergonomics are diverse according to the nature of work. In addressing
workplace ergonomics in hospitals, a holistic approach is needed to look into the
nature of each work and its risk factors. For example, for nurses, patients handling
including lifting and reposition are important factors while for laboratory, surgeons
and other theatre workers the workplace ergonomics issues would include static and
awkward postures and repetitive movements. In a study by Davis and Kotowski
(2015), nurses and nursing aides were found to have been exposed to lower back,
shoulder and neck pains which in many studies have been linked with patient handling
especially lifting and repositioning heavy patients. In the nursing work, especially in
the developing countries which have challenges in keeping up with advancements in
technology, patient turning and lifting cannot be avoided. It was concluded by
Driessen et al (2009) that Information Technology applications can fundamentally
impact the nature of some work in healthcare and reduce physical strains that may lead
to MSDs.
The risk factors in hospital workplace ergonomics can be removed by putting more
efforts on the reliable measures, it is important that organizations take the measures
appropriate to address each risk factor. Kim (2017) recommended that management

24
of workplace ergonomics risk factors in health care should have a “holistic,
multidimensional handling, evidence-based models of causation that consider a
combination of hazards”. The same should be supported by considerable empirical
evidence on the cause and effect of the existing problem that can support the
management to make the correct interventions. In a study on workplace ergonomics
in theatres, involving surgeons, Shiromani et al. (2016) found that musculoskeletal
complaints and frequent absence from work was present among surgeons whereas out
of 127 respondents, 56 had musculoskeletal complaints and 30 had had such
complaints in previous times.
In another study on MSDs among obstetrics and gynaecology professionals, Jadhav et
al. (2019), found that there was a high prevalence of the MSDs among the
professionals, which was related to inappropriate and awkward body postures. In that
study it was found that 85% of the doctors had experienced MSDs in a period of 12
months. It was recommended that increased awareness of ergonomics including
knowledge on appropriate working postures and assessing the ergonomic risk factors
would help eliminate work related injuries.
2.3.5 Workplace Ergonomics Awareness
Despite the importance of workplace ergonomics as observed in various research,
awareness on the subject is still low for various professional groups (Pandve, 2016).
The importance of increasing efforts to create and improve workplace ergonomics
awareness cannot be over emphasized. Several measures have to be taken in increasing
workplace ergonomics awareness for employees especially at management level
(Deros et al. 2015). Proper training and awareness on office design to fit the needs of
the employee, manual handling of materials, lifting techniques which do not strain the
body and comfortable working postures have been found to have significance in
reducing MSDs. It has been recommended in some studies that orientation and training
on workplace ergonomics through seminars and conferences should be an ongoing
activity so that employees would be aware of its benefits (Olabode et al. 2017).
25
According to Ismaila (2010), the limited level of awareness on workplace ergonomics
observed among employees was attributed to the fact that most employees, regardless
of educational background and qualification, do not know of its benefits both on their
work and human daily activities. The management, however, is expected to take active
and aggressive role in enhancing awareness and therefore it should itself possess
sufficient awareness on the subject. In an assessment of the role of workplace
ergonomics for employees in the health sector in Kenya, Kahare (2012) concluded that
management awareness and support on workplace ergonomics were critical in
enhancing employees’ performance.
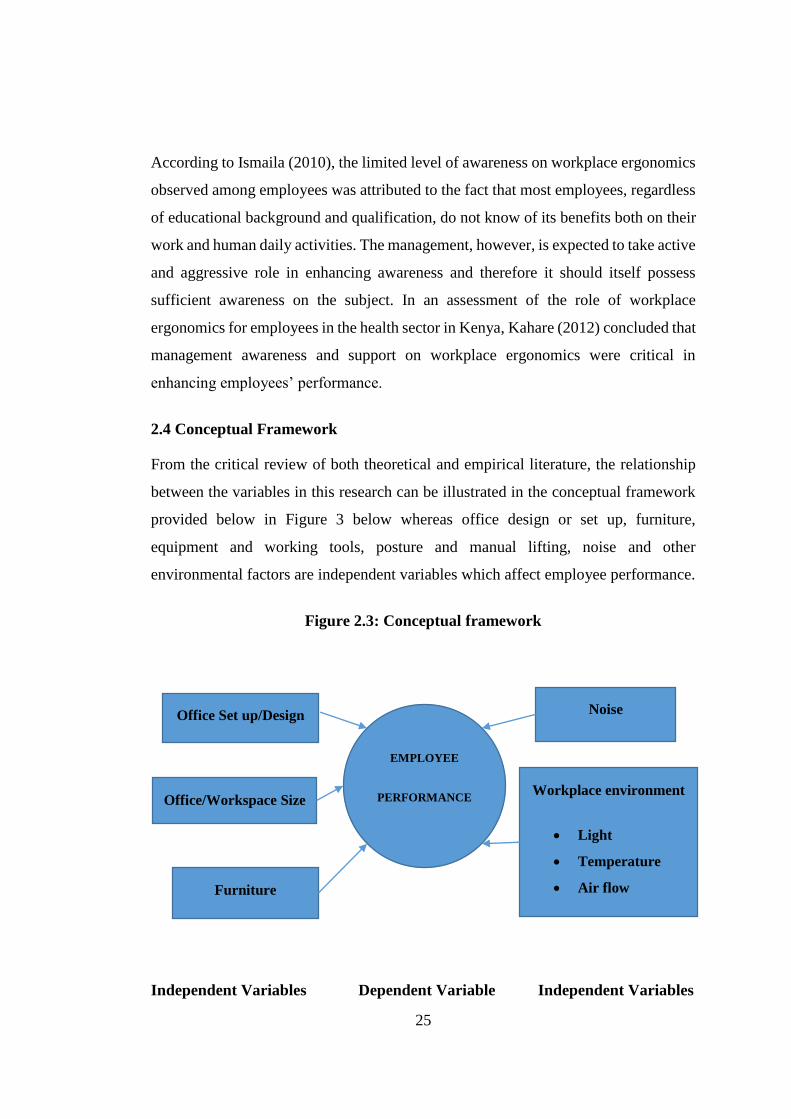
2.4 Conceptual Framework
From the critical review of both theoretical and empirical literature, the relationship
between the variables in this research can be illustrated in the conceptual framework
provided below in Figure 3 below whereas office design or set up, furniture,
equipment and working tools, posture and manual lifting, noise and other
environmental factors are independent variables which affect employee performance.
Figure 2.3: Conceptual framework
Independent Variables Dependent Variable Independent Variables
Office Set up/Design
Furniture
Noise
Workplace environment
Light
Temperature
Air flow
EMPLOYEE
PERFORMANCE Office/Workspace Size

26
Source: (Developed by the Researcher’s from literature review, 2020)
From the theoretical an empirical literature reviewed, it is clear that employees’
performance and specifically for this study healthcare employees’ performance is
influenced by various factors which are all important. The conceptual framework
depicted above shows the relation between the dependant variable which is
employees’ performance and various ergonomic factors which are the independent
variables. The independent variables which may affect employee’ performance that
were considered in reaching the findings for this study are office design and set up,
furniture, equipment and working tools, working postures, manual lifting, noise level
and the general work environment factors which would normally include thermal
comfortability of the workplace and illumination which should be suitable to allow
optimal performance.
As seen from the various literatures reviewed as stated in this chapter, these factors
were found to have an impact on employee performance in various industries. In this
research which looks into role of workplace ergonomics in the health service delivery,
the researcher examined the role which each of the mentioned independent variables
has on the working environment at MNH and how they affect the healthcare
employees’ performance at the Hospital.

27
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Study Area
This study was conducted at the MNH located in Upanga, Ilala District, Dar es Salaam.
The Hospital was chosen as it is the national referral Hospital and it is expected to set
the desired standard when it comes to healthcare delivery for both private and public
hospitals. Also as the national referral Hospital, MNH helps in the development or
improvement in Policies and Guidelines that are relevant in improving healthcare
delivery in both private and public sectors.
These are the justifications for choosing MNH as the case study in this research. MNH
has 8 directorates namely Medical services, Surgical Services, Nursing & Quality
Services, Clinical Support Services, Human Resources, Finance and Planning,
Technical Services, and Information & Communications Technology and a workforce
of around 2,700 employees who are a mix of clinical and supportive employees, all
termed as healthcare employees (World Health Organization , 2010).
Apart from being the national referral hospital, MNH offers the ideal choice of using
it as the case study for analyzing the workplace ergonomics on healthcare employee’s
performance simply because of the nature and capacity of that hospital both in terms
of working environment facilities and human capital resources. The findings of this
research can be generalized to understand the role of workplace ergonomics in health
service delivery.
3.2 Research Paradigm
Research paradigm can be defined as the general consideration of knowledge,
perceptions, beliefs, and awareness of different theories and practices used to carry
out a scientific research (Cohen et al., 2007). This study followed the
interpretivist/constructivist paradigm which is used to understand the human
experience or viewpoint of the subjects being studied (Kivunja and Kuyini, 2017).

28
3.3 Research Design
Research design is the arrangement of conditions for collection and analysis of data in
a manner that aims to combine relevance to the research purpose (Kothari, 2004). This
study adopted a descriptive case study design which is defined as an empirical research
method used to investigate a contemporary phenomenon on the dynamics of the case,
within its real life context (Yin, 2003). Case studies are conducted with various goals
including description or testing of theories and in this study helped the researcher to
investigate the theories on role of workplace ergonomic on healthcare employees’
performance.
Furthermore, Harrison et al. (2017) argued that case study research design is
pragmatic, flexible research design that is capable of giving out the comprehensive in-
depth understanding of various phenomenon. Case study design is used for researches
which aim to get understanding of a phenomenon by answering the “how” and the
“why” (Baxter and Jack, 2008). Following that, the research design chosen is suitable
for this research which aims to establish how workplace ergonomics has an impact on
health service delivery. Apart from the intention of gaining the deep understanding of
workplace ergonomic factors, the adoption of the case study research design allowed
the flexibility in data collection methods whereby both qualitative and quantitative
techniques for data collection were used.
3.4 Population, Sample method and Sample size
3.4.1 Study population
This study’s target population was all healthcare employees who are working at MNH
located in Upanga, Ilala District, Dar es Salaam. This means that the population of this
study comprised of employees who are working in clinical and the supportive
functions. Generally, MNH has employed a workforce of around 2,700 employees,
this number include both clinical and supportive employees.
The reason for targeting all employees who are working in the clinical and supportive
functions was mainly because the delivery of standard healthcare services is facilitated

29
to a significant extent by the performance of the supportive services such as
administration, human resource management, finance, procurement, engineering
works and information and communication technology in particular area.
3.4.2 Sampling procedures
In this research, a small group of respondents were involved in order to offer opinions
or views of the others (Kothari, 2004). The study sample was obtained mainly using
non – probability sampling technique, this basically involved the use of purposive
sampling technique where by convenient sampling techniques and judgmental
sampling technique were employed. Convenient sampling techniques involves
contacting respondents due to their availability and accessibility, on the other hand
judgmental sampling technique which involved respondents depending on the
researchers’ assumption that they fit into the study due to their knowledge and their
deep understanding on underlined ergonomic factors in the relation employee’s
performance.
3.4.3 Sample Size
The portion chosen to represent the population is the sample size from which a
researcher obtained primary data (Milanzi, 2009). By using this number as the total
population of the study, then the targeted sample to be used in this study was
determined by using the following formula which was proposed by (Israel, 1992) as a
simplified formula in calculating sample size.
n =
n = Sample size
N = Population 2,700
N
1+N (e2)

30
e = Level of precision (sampling error) 10 percent or 0.1
n= 2,700/1+2,700(0.01)
n =2,700/1+27
n=2,700/28
n=96.4285 = 96
The determined sample size was 96 respondents.
Using provided formula,the sample size of this study included 96 respondents,
whereas 16 respondents were from the Management (Directors and Heads of
Department), 20 were non-clinical staff, 30 nursing staff and 30 clinical staff of
various cadres.
Table 3. 1: Sample of Informants and its Distribution
Target Population Sample Size
Management 16
Non-clinical staff 20
Nursing staff 30
Clinical staff 30
Total 96
Source: Researcher’s own construct, 2020
3.5 Types of Data and Data Collection Techniques
In order to undertake this study, the collection of primary data was involved.
3.5.1 Primary Data
The study’s primary data was gathered from the field targeting employees who are
working at MNH in Dar es Salaam. The primary data collection techniques that were
used in this study were questionnaires and interviews.

31
3.5.1.1 Questionnaire
Questionnaire involves setting up of questions which are printed or typed and mailed
to the participants with the expectation that the said participants will read, understand
and respond to those questions (Kothari, 2004). The questions were designed to
address workplace ergonomics variables which assisted in determination of the extent
to which workplace ergonomics influence healthcare employees’ performance, the
awareness about workplace ergonomics design and in identification of the barriers that
are hindering workplace ergonomics design of the workplaces in healthcare facilities.
In order to achieve all these, the questionnaire guide for this study comprised of both
structured and unstructured questions for purposes of giving a room of obtaining clear
understanding of the variables under this study.
Questionnaire is the set of questions printed or typed and mailed to respondents who
are expected to read, understand and reply on the questions stated in the particular
form (Kothari, 2004).
3.5.1.2 Interview
Interview method is a series of questions usually open-ended questionnaire used on
one to one dialogue like discussion between the researchers and respondents in order
to gather information about a certain issue (Foddy, 1994). The main reason of using
interview in undertaking this study is to complement the data collected through the
use of questionnaire method.
3.6 Validity and Reliability
Validity as the accuracy of information that were used by this study was assured by
the use of multiple data collection tools and multiple respondent samples (Best and
Khan 1993). Therefore, in assuring validity of data the study used questionnaire and
interview guides in order to supplement information that was collected from different
respondents. Reliability of the study findings was ensured by conducting the intensive
32
literature review on issues related to workplace ergonomics variables and healthcare
employee’s performance.
3.7 Data Measurement and Analysis
The methods that were adopted in collecting data relating to the pointed research
questions gave out both qualitative and quantitative data. The data obtained from the
Respondents on the variables was measured by using the nominal and ordinal scales
of measurement. Furthermore, the quantitative data relating to the influence of
workplace ergonomics factors to healthcare employees’ performance and the
awareness about workplace ergonomics design were analyzed descriptively by using
tabulation analysis, which has been presented through charts, tables and graphs.
On the other hand, qualitative information relating to identification of those factors
that are hindering workplace ergonomics design of the workplaces in healthcare
facilities were analyzed by using content analysis and this was mainly from the
responses that were obtained from unstructured questions and interview method.
In addition, the relationship between workplace ergonomics variables and healthcare
employees’ performance was analyzed by the use of correlation and multiple
regression analysis, the study used SPSS version 25 to present the frequencies, tables
and charts analyzed by the program.
3.8 Ethical Issues
Academic researches must adhere to the ethical principle that guide the way of
conducting and disseminating of research findings (Akaranga, 2016). Permission to
conduct this study was granted from Mzumbe University and from MNH which is the
study area. Consent to collect information from respondents was sought from
respondents after they were provided with full information about the purposes of this
study and their rights to engage or not to engage in the study. Confidentiality was
observed whereas respondents’ identity was kept anonymous and protected against

33
any harm. Before actual data collection respondents were made aware of the purposes
of the study.

34
CHAPTER FOUR
PRESENTATION OF FINDINGS
4.1 Introduction
This chapter presents the analysis of the findings that were collected by using
questionnaire method whereby the total of 96 questionnaires were distributed to MNH
staff. The questions were designed to address workplace ergonomics variables in
relation to healthcare employees’ performance, to determine the workplace
ergonomics design awareness among MNH staff and to identify those factors that are
hindering workplace ergonomics design of the workplaces in healthcare facilities. In
completing the questionnaire method, the findings from those few staff who were
contacted through interview method were also presented. This chapter has been
divided into two sections which are respondents’ characteristics and data findings on
the specific questions.
4.2. Socio-demographic data of the respondents
This section presents the general profile of all the respondents who were engaged in
the conduction of this study.
4.2.1 Gender of respondents
Out of 96 respondents, 45 respondents which is equivalent to 47% were male and on
the other hand, 51 respondents which is equivalent to 53% were female.
Table 4. 1: Gender of respondents
Variable measure Frequency (N) Valid Percent (%)
Male 45 47%
Female 51 53%
Total 96 100%
Source: Survey Data, (2020)
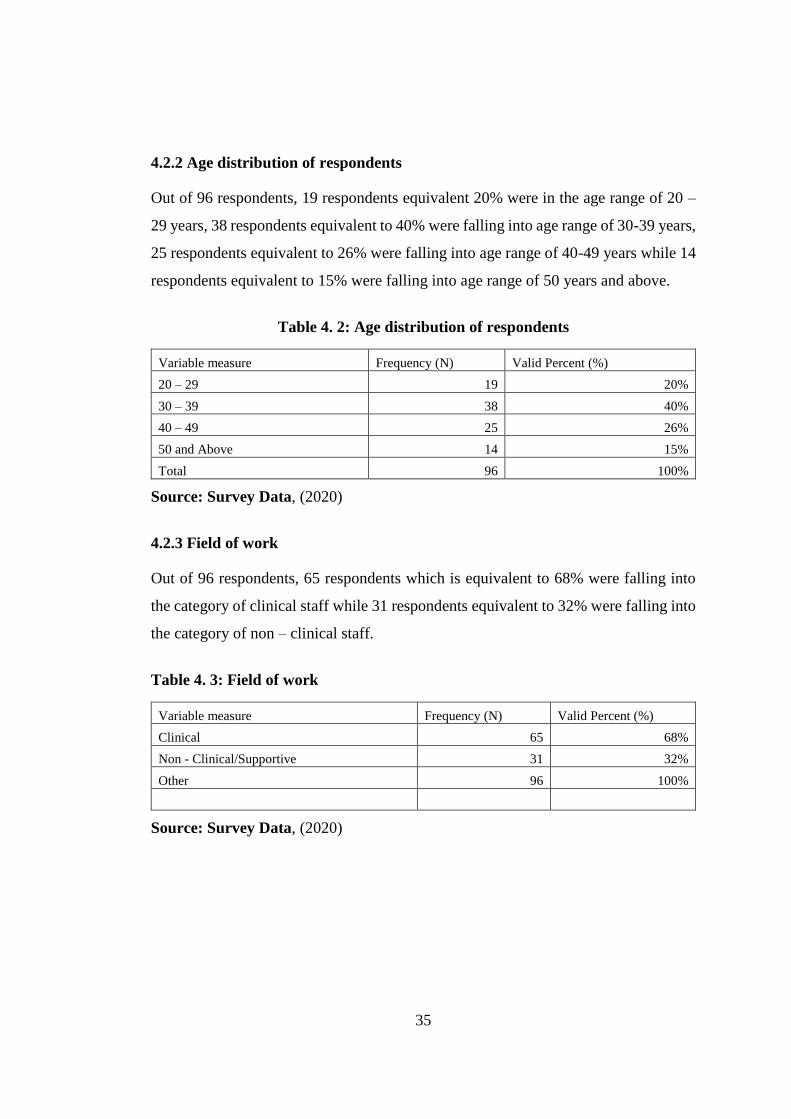
35
4.2.2 Age distribution of respondents
Out of 96 respondents, 19 respondents equivalent 20% were in the age range of 20 –
29 years, 38 respondents equivalent to 40% were falling into age range of 30-39 years,
25 respondents equivalent to 26% were falling into age range of 40-49 years while 14
respondents equivalent to 15% were falling into age range of 50 years and above.
Table 4. 2: Age distribution of respondents
Variable measure Frequency (N) Valid Percent (%)
20 – 29 19 20%
30 – 39 38 40%
40 – 49 25 26%
50 and Above 14 15%
Total 96 100%
Source: Survey Data, (2020)
4.2.3 Field of work
Out of 96 respondents, 65 respondents which is equivalent to 68% were falling into
the category of clinical staff while 31 respondents equivalent to 32% were falling into
the category of non – clinical staff.
Table 4. 3: Field of work
Variable measure Frequency (N) Valid Percent (%)
Clinical 65 68%
Non - Clinical/Supportive 31 32%
Other 96 100%
Source: Survey Data, (2020)

36
4.2.4 Level of work
Out of 96 respondents, 24 respondents equivalent 25% were in junior staff level, 34
respondents equivalent to 35% were in middle level, 22 respondents equivalent to 23%
were in senior level while 16 respondents equivalent to 17% were in managerial level.
Table 4. 4: Level of work
Variable measure Frequency (N) Valid Percent (%) Junior Staff 24 25% Middle Level Staff 34 35% Senior Staff 22 23% Management 16 17% Total 96 100%
Source: Survey Data, (2020)
4.2.5 Department/unit
Out of 96 respondents, 32 respondents equivalent 33% were working in Nursing and
quality services, 32 respondents equivalent to 33% were working in clinical support
services, 6 respondents equivalent to 6% were working in technical services, 5
respondents equivalent to 5% were working in medical services, 5 respondents
equivalent to 5% were working in finance and planning, 5 respondents equivalent to
5% were working in surgical services and 5respondents equivalent to 5% were
working in information and communication technology.
Table 4. 5: Directorates
Variable measure Frequency (N) Valid Percent (%) Nursing & Quality Services 32 33% Clinical Support Services 32 33%
Human Resource 6 6% Technical Services 6 6% Medical services 5 5%
Finance and Planning 5 5% Surgical Services 5 5% Information and Communication Technology 5 5%
Total 96 100%
Source: Survey Data, (2020)

37
4.2.6 Working experience
Out of 96 respondents, 22 respondents equivalent 23% have been in that service for
the range of 1 – 3 years, 27 respondents equivalent to 28% have been in that service
for the range of 4 -6 years, 31 respondents equivalent to 32% have been in that service
for the range of 7 – 10 years while 16 respondents equivalent to 17% have been in that
service for more than 10years.
Table 4. 6: Working experience
Variable measure Frequency (N) Valid Percent (%) 1 - 3 years 22 23%
4 - 6 years 27 28% 7 - 10 years 31 32%
More than 10 years 16 17% Total 96 100%
Source: Survey Data, (2020)
4.3 Research Question 2: Level of health care employee’s awareness on
workplace ergonomics
Table 4.7 presents the findings on level of awareness to these employees concerning
ergonomics issues at the workplace. Ergonomic variables which were discussed were
office set up, equipment and workplace, office furniture, environment, working
posture and manual lifting and level of noise. The findings revealed that out of all 96
respondents, 32 respondents equivalent to 33% agreed that the office set up and design
should consider workplace ergonomics, 58 respondents equivalent to 60% were
neutral 6 respondents equivalent to 6% disagreed on the same statement. The overall
results show that, 33% of all the respondents were aware about the consideration of
office set and design towards workplace ergonomics.
The respondents were asked whether the working equipment should consider
workplace ergonomics to allow for the comfortability to the worker and minimization
of risks and accidents. Out of all 96 respondents, 6 respondents equivalent to 6%
agreed that equipment and working tools should consider the workplace
ergonomics,10 respondents equivalent to 10% strongly agreed on the same while 80
38
respondents equivalent to 83% were neutral on the same statement. The overall results
show that, 17% of all the respondents were aware about the consideration of
equipment and working tools towards workplace ergonomics.
The respondents were asked whether the office furniture should consider workplace
ergonomics to allow for the comfortability to the worker. Out of all 96 respondents,
27 respondents equivalent to 28% agreed that office furniture should consider the
workplace ergonomics, 57 respondents equivalent to 59% were neutral while
12respondents equivalent to 13% disagreed on the same statement. The overall results
that, 28% of all the respondents were aware about the consideration of office furniture
towards workplace ergonomics.
The respondents were asked whether the environment issues like ventilation and
illumination should be considered in the design of rooms/offices in observing
workplace ergonomics. Out of all 96 respondents, 37 respondents equivalent to 39%
agreed that the environment should consider the workplace ergonomics, 59
respondents equivalent to 61% were neutral on the same statement. The overall results
show that 39 % of all the respondents were aware about the consideration of the
environment and the workplace ergonomics.
The respondents were asked whether the working posture and manual lifting should
consider workplace ergonomics and their awareness on the health effect they have if
not well designed. Out of all 96 respondents, 36 respondents equivalent to 38% agreed
that working posture and manual lifting should consider the workplace ergonomics,
39 respondents equivalent to 41% were neutral while 21 respondents equivalent to
22% were disagreed on the same statement. The overall results that, 38% of all the
respondents were aware about the consideration of working posture and manual lifting
towards workplace ergonomics.
The respondents were asked whether the workplace that is subjected to excessive noise
can cause lack of concentration and health effects. Out of all 96 respondents, 52
respondents equivalent to 54% agreed that they were aware about the level of noise
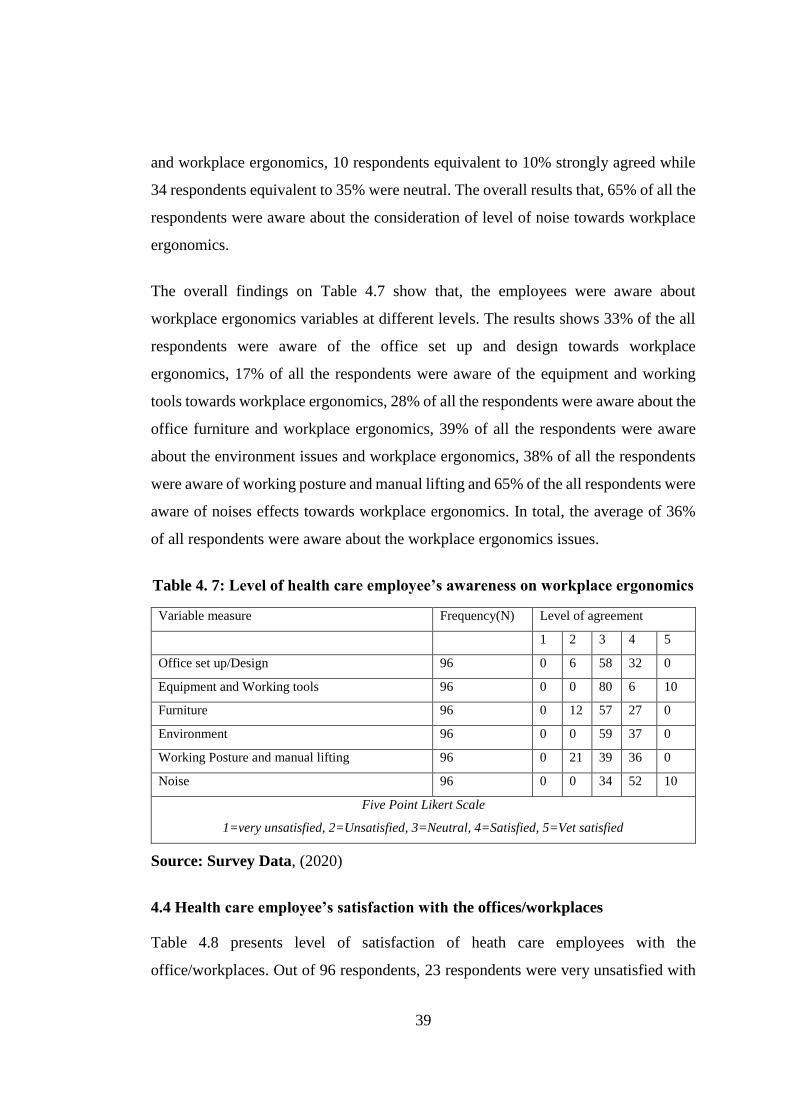
39
and workplace ergonomics, 10 respondents equivalent to 10% strongly agreed while
34 respondents equivalent to 35% were neutral. The overall results that, 65% of all the
respondents were aware about the consideration of level of noise towards workplace
ergonomics.
The overall findings on Table 4.7 show that, the employees were aware about
workplace ergonomics variables at different levels. The results shows 33% of the all
respondents were aware of the office set up and design towards workplace
ergonomics, 17% of all the respondents were aware of the equipment and working
tools towards workplace ergonomics, 28% of all the respondents were aware about the
office furniture and workplace ergonomics, 39% of all the respondents were aware
about the environment issues and workplace ergonomics, 38% of all the respondents
were aware of working posture and manual lifting and 65% of the all respondents were
aware of noises effects towards workplace ergonomics. In total, the average of 36%
of all respondents were aware about the workplace ergonomics issues.
Table 4. 7: Level of health care employee’s awareness on workplace ergonomics
Variable measure Frequency(N) Level of agreement
1 2 3 4 5
Office set up/Design 96 0 6 58 32 0
Equipment and Working tools 96 0 0 80 6 10
Furniture 96 0 12 57 27 0
Environment 96 0 0 59 37 0
Working Posture and manual lifting 96 0 21 39 36 0
Noise 96 0 0 34 52 10
Five Point Likert Scale
1=very unsatisfied, 2=Unsatisfied, 3=Neutral, 4=Satisfied, 5=Vet satisfied
Source: Survey Data, (2020)
4.4 Health care employee’s satisfaction with the offices/workplaces
Table 4.8 presents level of satisfaction of heath care employees with the
office/workplaces. Out of 96 respondents, 23 respondents were very unsatisfied with

40
the existence general design of the office, 17 respondents were unsatisfied, 30
respondents were neutral, 14 respondents were satisfied and 12 respondents were very
satisfied. On the state and suitability of office furniture, 23 respondents were very
unsatisfied with the office furniture, 25 respondents were unsatisfied, 15 respondents
were neutral, 24 respondents were satisfied and 9 respondents were very satisfied.
On the size of the space allocated to their workplace, 31 respondents were very
unsatisfied with the size of the space allocated, 21 respondents were unsatisfied, 7
respondents were neutral, 25 respondents were satisfied and 12 respondents were very
satisfied. On the state of working equipment, 31 respondents were very unsatisfied
with the working equipment, 21 respondents were unsatisfied, 7 respondents were
neutral, 25 respondents were satisfied and 12 respondents were very satisfied.
Concerning room temperature, airflow and illumination, 15 respondents were very
unsatisfied with the room temperature, airflow and illumination, 30 respondents were
unsatisfied, 19 respondents were neutral, 23 respondents were satisfied and 9
respondents were very satisfied. On level of noise, 16 respondents were very
unsatisfied with the noise level in the particular workplace, 23 respondents were
unsatisfied, 20 respondents were neutral, 13 respondents were satisfied and 24
respondents were very satisfied.
The overall satisfaction level shows that, out of 96 respondents, 42% were unsatisfied
with the general design of the office while 27% were satisfied, 50% of the respondents
were unsatisfied with the state and suitability of the office furniture while 34% were
satisfied, 56% of the respondents were unsatisfied with the size of space allocated to
their workplace while 35% were satisfied, 54% of the respondents were unsatisfied
with state of working equipment while 39% were satisfied, 47% of the respondents
were unsatisfied with the room temperature, airflow and illumination while 33% were
satisfied, 41% of the respondents were unsatisfied with level of noise while 39% were
satisfied.

41
Table 4. 8: Level of health care employee’s satisfaction with office
Variable measure Frequency (N) Level of agreement
1 2 3 4 5
General Design of the office 96 23 17 30 14 12
State and suitability of office furniture 96 23 25 15 24 9
Size of space allocated to your workplace 96 26 28 8 22 12
State of the working equipment 96 31 21 7 25 12
Room temperature and airflow and illumination 96 15 30 19 23 9
Level of noise 96 16 23 20 13 24
Five Point Likert Scale
1=very unsatisfied, 2=Unsatisfied, 3=Neutral, 4=Satisfied, 5=Vet satisfied
Source: Survey Data, (2020)
4.5 Workplace ergonomics and employee’s health and safety
Figure 4.1 presents the impact of the present state of workplace ergonomics towards
the employee’s health and safety whereby out of 96 respondents, 58 respondents
equivalent to 60% agreed that the office space is insufficient, 12 respondents
equivalent to 13% were neutral and 26 respondents equivalent to 27% agreed that the
space is sufficient.
Figure 4. 1. Office space and workplace ergonomics
Source: Survey Data, (2020)
Figure 4.2 presents manual lifting and workplace ergonomics whereby out of 96
respondents, 32 respondents agreed that their work involves heavy manual lifting of
materials, 31 respondents agreed that not much of their works involves manual lifting
60%13%
27%
Insufficiently Spaced
Neutral
Sufficiently Spaced

42
while 33 respondents said their work is very much subjected to the heavy lifting of
materials and other objects.
Figure 4. 2. Office space and workplace ergonomics
Source: Survey Data, (2020)
Figure 4.3 presents the level of stress resulted from the workplace environment such
as design, set up, furniture, air conditioning and noise. Out of 96 respondents, 40
respondents equivalent to 42% were not stressed by workplace environment, 13
respondents equivalent to 13% were neutral and 43respondents equivalent to 45%
were very much stressed.
33%
32%
35%
Never
Not much
Very much
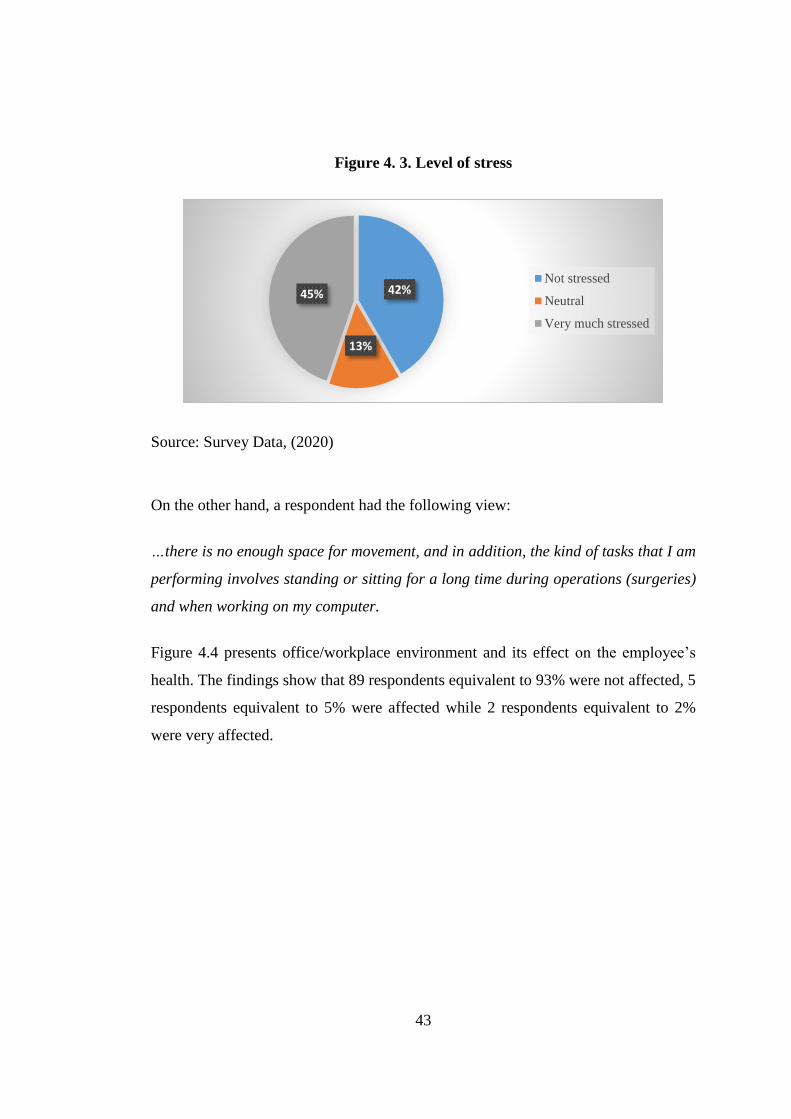
43
Figure 4. 3. Level of stress
Source: Survey Data, (2020)
On the other hand, a respondent had the following view:
…there is no enough space for movement, and in addition, the kind of tasks that I am
performing involves standing or sitting for a long time during operations (surgeries)
and when working on my computer.
Figure 4.4 presents office/workplace environment and its effect on the employee’s
health. The findings show that 89 respondents equivalent to 93% were not affected, 5
respondents equivalent to 5% were affected while 2 respondents equivalent to 2%
were very affected.
42%
13%
45%Not stressed
Neutral
Very much stressed
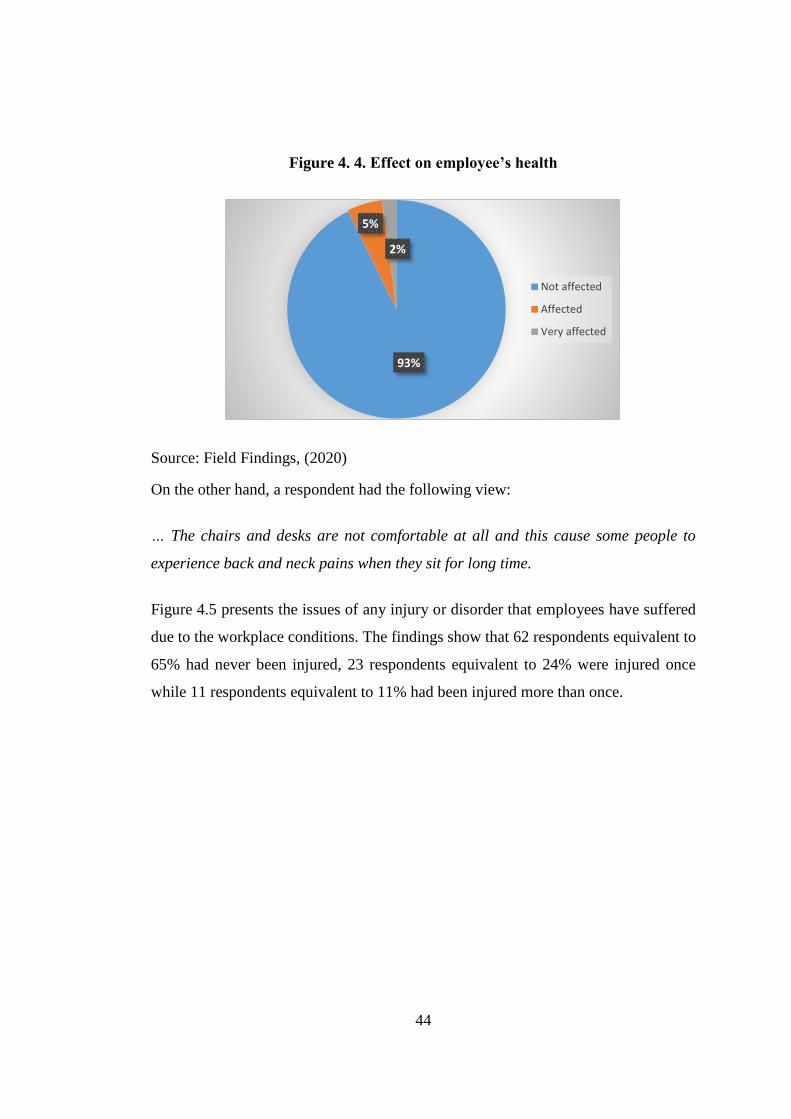
44
Figure 4. 4. Effect on employee’s health
Source: Field Findings, (2020)
On the other hand, a respondent had the following view:
… The chairs and desks are not comfortable at all and this cause some people to
experience back and neck pains when they sit for long time.
Figure 4.5 presents the issues of any injury or disorder that employees have suffered
due to the workplace conditions. The findings show that 62 respondents equivalent to
65% had never been injured, 23 respondents equivalent to 24% were injured once
while 11 respondents equivalent to 11% had been injured more than once.
93%
5%
2%
Not affected
Affected
Very affected
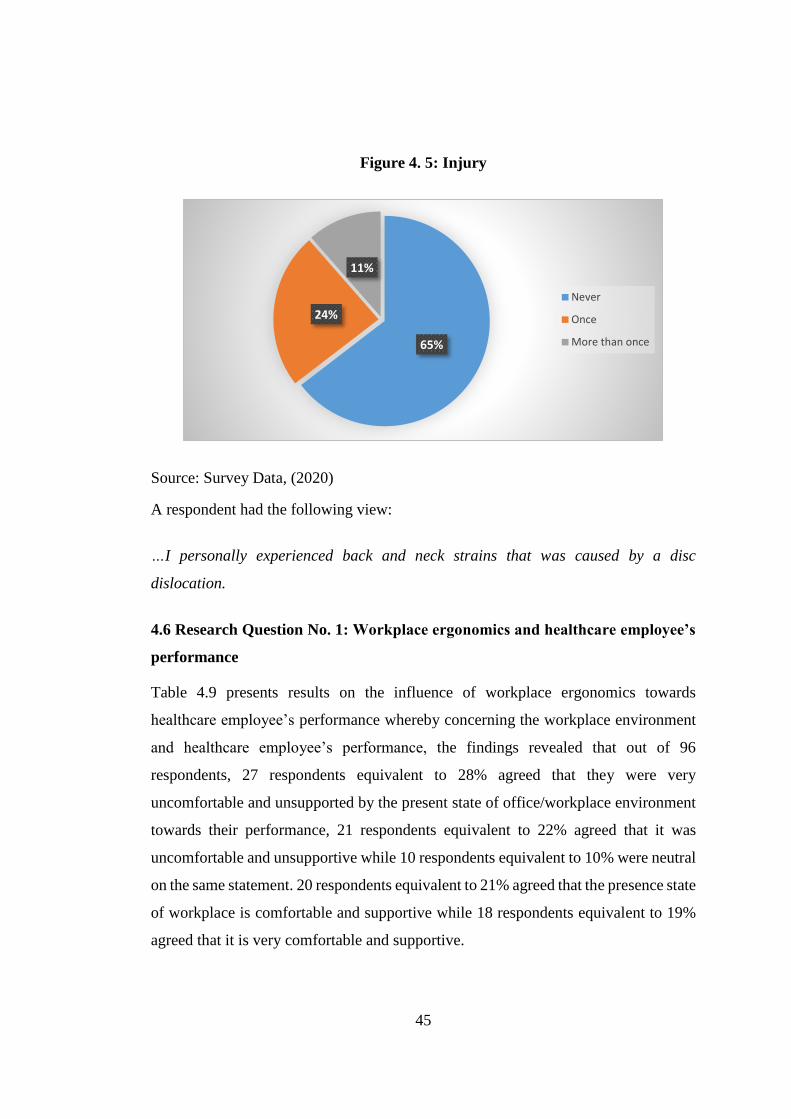
45
Figure 4. 5: Injury
Source: Survey Data, (2020)
A respondent had the following view:
…I personally experienced back and neck strains that was caused by a disc
dislocation.
4.6 Research Question No. 1: Workplace ergonomics and healthcare employee’s
performance
Table 4.9 presents results on the influence of workplace ergonomics towards
healthcare employee’s performance whereby concerning the workplace environment
and healthcare employee’s performance, the findings revealed that out of 96
respondents, 27 respondents equivalent to 28% agreed that they were very
uncomfortable and unsupported by the present state of office/workplace environment
towards their performance, 21 respondents equivalent to 22% agreed that it was
uncomfortable and unsupportive while 10 respondents equivalent to 10% were neutral
on the same statement. 20 respondents equivalent to 21% agreed that the presence state
of workplace is comfortable and supportive while 18 respondents equivalent to 19%
agreed that it is very comfortable and supportive.
65%
24%
11%
Never
Once
More than once

46
Concerning office furniture and healthcare employee’s performance, the findings
revealed that out of 96 respondents, 25 respondents equivalent to 26% agreed that they
were very uncomfortable and unsupported by the present state of office furniture
which hinders their performance, 27 respondents equivalent to 28% agreed that it is
uncomfortable and unsupportive while 7 respondents equivalent to 7% were neutral
on the same. Further, 26 respondents equivalent to 27% agreed that the present state
of office furniture is comfortable and supportive while 11 respondents equivalent to
11% agreed that it is very comfortable and supportive.
Concerning space size allocated in the office and healthcare employee’s performance,
the findings revealed that out of 96 respondents, 28 respondents equivalent to 29%
agreed that they were very uncomfortable and unsupported by their office space which
hinders their performance, 30 respondents equivalent to 31% agreed that it was
uncomfortable and unsupportive while 6 respondents equivalent to 6% were neutral
on the same. Further, 21 respondents equivalent to 22% agreed that the present office
space was comfortable and supportive while 11 respondents equivalent to 11% agreed
that it was very comfortable and supportive.
Concerning the level of noise and healthcare employee’s performance, the findings
revealed that out of all 96 respondents, 10 respondents equivalent to 10% agreed that
they were very uncomfortable and unsupported by level of noise and it hinders their
performance at work, 13 respondents equivalent to 14% agreed that it is uncomfortable
and unsupportive while 36 respondents equivalent to 38% were neutral on the same
statement. Furthermore, 13 respondents equivalent to 14% agreed they were
comfortable with the level of noise at their workplaces while 24 respondents
equivalent to 25% agreed that it was very comfortable and supportive.
Concerning workplace temperature, airflow and light flow and healthcare employee’s
performance, the findings shows that out of all 96 respondents, 23 respondents
equivalent to 24% agreed that they were very uncomfortable and with the workplace
temperature, airflow and light flow and it also was not supportive of their performance
at work, 30 respondents equivalent to 31% agreed that it was uncomfortable and
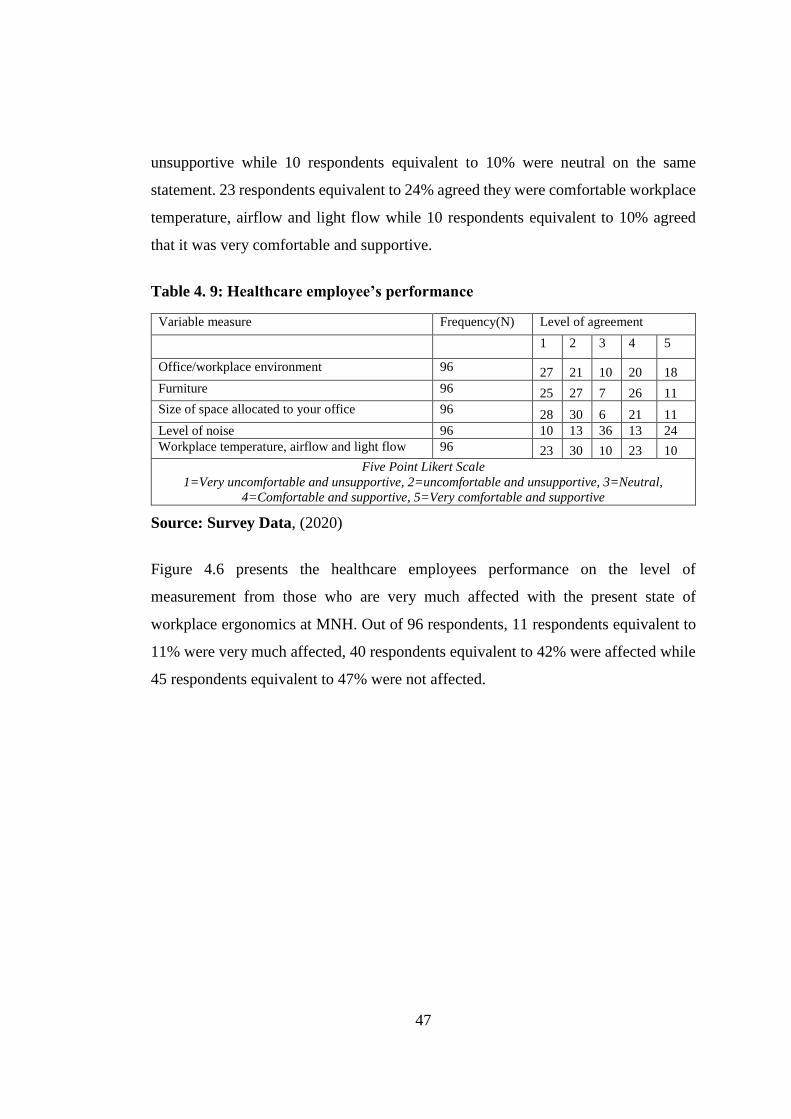
47
unsupportive while 10 respondents equivalent to 10% were neutral on the same
statement. 23 respondents equivalent to 24% agreed they were comfortable workplace
temperature, airflow and light flow while 10 respondents equivalent to 10% agreed
that it was very comfortable and supportive.
Table 4. 9: Healthcare employee’s performance
Variable measure Frequency(N) Level of agreement
1 2 3 4 5
Office/workplace environment 96 27 21 10 20 18
Furniture 96 25 27 7 26 11
Size of space allocated to your office 96 28 30 6 21 11
Level of noise 96 10 13 36 13 24
Workplace temperature, airflow and light flow 96 23 30 10 23 10
Five Point Likert Scale
1=Very uncomfortable and unsupportive, 2=uncomfortable and unsupportive, 3=Neutral,
4=Comfortable and supportive, 5=Very comfortable and supportive
Source: Survey Data, (2020)
Figure 4.6 presents the healthcare employees performance on the level of
measurement from those who are very much affected with the present state of
workplace ergonomics at MNH. Out of 96 respondents, 11 respondents equivalent to
11% were very much affected, 40 respondents equivalent to 42% were affected while
45 respondents equivalent to 47% were not affected.
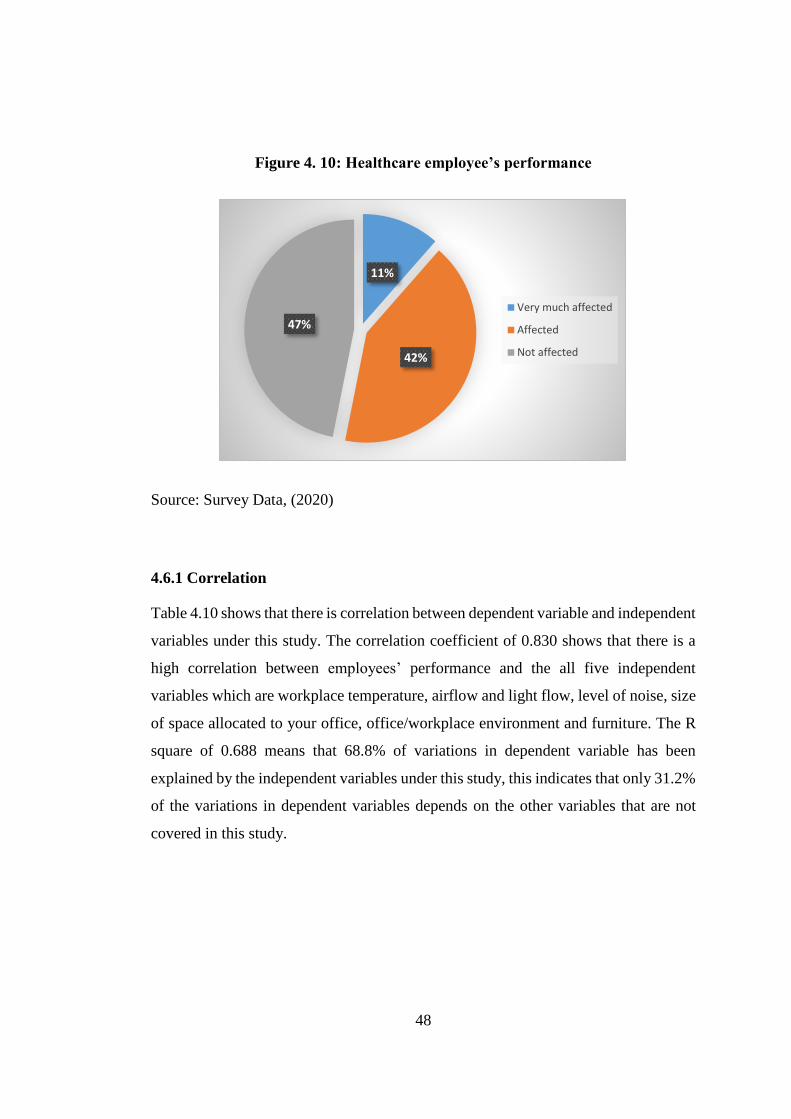
48
Figure 4. 10: Healthcare employee’s performance
Source: Survey Data, (2020)
4.6.1 Correlation
Table 4.10 shows that there is correlation between dependent variable and independent
variables under this study. The correlation coefficient of 0.830 shows that there is a
high correlation between employees’ performance and the all five independent
variables which are workplace temperature, airflow and light flow, level of noise, size
of space allocated to your office, office/workplace environment and furniture. The R
square of 0.688 means that 68.8% of variations in dependent variable has been
explained by the independent variables under this study, this indicates that only 31.2%
of the variations in dependent variables depends on the other variables that are not
covered in this study.
11%
42%
47%
Very much affected
Affected
Not affected

49
Table 4. 10: Model summary of the study
Model R R Square Adjusted R Square Std. Error of the Estimate
1 .830a .688 .671 .39011
a. Predictors: (Constant), Workplace temperature, airflow and light flow, Level of noise, Size of space
allocated to the office, Office/workplace environment, Furniture
b. Dependent Variable: Healthcare employees’ performance
4.6.2 Regression
Table 4.11 presents the significance of independent variables in predicting the
outcome in dependent variable. Following this analysis, it was found that all the five
independent variables which are workplace environment in terms of temperature,
airflow and light flow, level of noise, size of space allocated to the office,
office/workplace set up and design and furniture were significant in predicting the
outcome in dependent variable which is employee’s performance at the significance
level of .000
Table 4. 11: ANOVAa Model Sum of Squares df Mean Square F Sig.
1 Regression 30.262 5 6.052 39.769 .000b
Residual 13.697 90 .152
Total 43.958 95
a. Dependent Variable: Healthcare employees’ performance
b. Predictors: (Constant), Workplace temperature, airflow and light flow, Level of noise, Size of
space allocated to your office, Office/workplace environment, Furniture
Source – Survey Data, 2020.
Table 4.12 presents the coefficients of each independent variables and their influence
towards the performance of employees at MNH. Office/workplace set up and design
as an independent variable has positive influence towards employee’s performance at
the significance level of 0.123, furniture as an independent variable has a positive
influence towards employee’s performance at the significance level of 0.093, size of
space allocated has a negative influence towards employee’s performance at the
significance level of 0.590, level of noise has a positive influence towards employee’s
performance at the significance level of 0.006 while workplace temperature, airflow
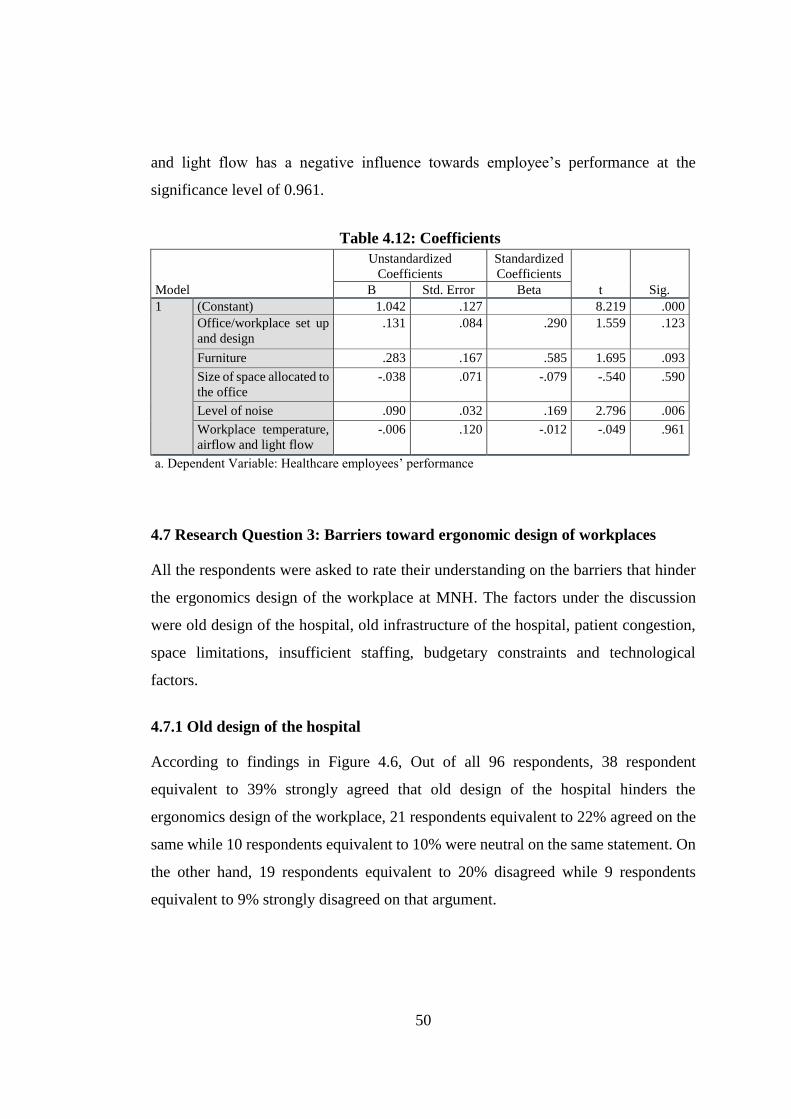
50
and light flow has a negative influence towards employee’s performance at the
significance level of 0.961.
Table 4.12: Coefficients
Model
Unstandardized
Coefficients Standardized
Coefficients t Sig. B Std. Error Beta
1 (Constant) 1.042 .127 8.219 .000
Office/workplace set up
and design .131 .084 .290 1.559 .123
Furniture .283 .167 .585 1.695 .093
Size of space allocated to
the office -.038 .071 -.079 -.540 .590
Level of noise .090 .032 .169 2.796 .006
Workplace temperature,
airflow and light flow -.006 .120 -.012 -.049 .961
a. Dependent Variable: Healthcare employees’ performance
4.7 Research Question 3: Barriers toward ergonomic design of workplaces
All the respondents were asked to rate their understanding on the barriers that hinder
the ergonomics design of the workplace at MNH. The factors under the discussion
were old design of the hospital, old infrastructure of the hospital, patient congestion,
space limitations, insufficient staffing, budgetary constraints and technological
factors.
4.7.1 Old design of the hospital
According to findings in Figure 4.6, Out of all 96 respondents, 38 respondent
equivalent to 39% strongly agreed that old design of the hospital hinders the
ergonomics design of the workplace, 21 respondents equivalent to 22% agreed on the
same while 10 respondents equivalent to 10% were neutral on the same statement. On
the other hand, 19 respondents equivalent to 20% disagreed while 9 respondents
equivalent to 9% strongly disagreed on that argument.

51
Figure 4. 6: Old design of the hospital
Source: Field Findings, (2020)
4.7.2 Old infrastructure of the hospital
Figure 4. 7: Old infrastructure of the hospital
Source: Survey Data, (2020)
Figure 4.7 presents that out of all 96 respondents, 19 respondents equivalent to 20%
strongly agreed that old infrastructure of the hospital hinders the ergonomics design
9%
20%
10%
22%
39%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
15%
29%
6%
30%
20%
0%
5%
10%
15%
20%
25%
30%
35%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree

52
of the workplace, 29 respondents equivalent to 30% agreed on the same while 6
respondents equivalent to6% were neutral on the same statement. On the other hand,
28 respondents equivalent to 29% disagreed while 14 respondents equivalent to 15%
strongly disagreed on that argument.
4.7.3 Patient congestion
Figure 4.9 presents that out of all 96 respondents, 12 respondents equivalent to 13%
strongly agreed that patient congestion hinders the ergonomics design of the
workplace, 22 respondents equivalent to 23% agreed on the same while 8 respondents
equivalent to 8% were neutral on the same statement. On the other hand, 28
respondents equivalent to 29% disagreed while 26 respondents equivalent 27%
strongly disagreed on that argument.
Figure 4. 8: Patient congestion
Source: Survey Data, (2020)
27%29%
8%
23%
13%
0%
5%
10%
15%
20%
25%
30%
35%
Strongly
Disagree
Disagree Neutral Agree Strongly Agree
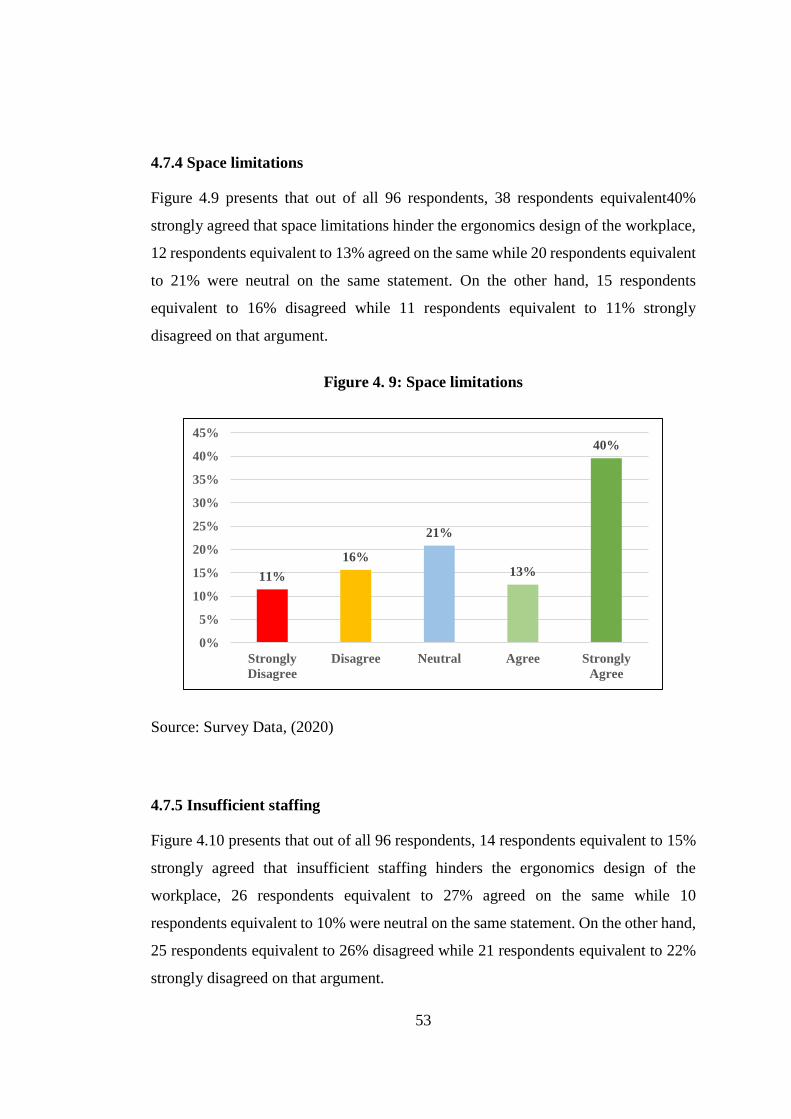
53
4.7.4 Space limitations
Figure 4.9 presents that out of all 96 respondents, 38 respondents equivalent40%
strongly agreed that space limitations hinder the ergonomics design of the workplace,
12 respondents equivalent to 13% agreed on the same while 20 respondents equivalent
to 21% were neutral on the same statement. On the other hand, 15 respondents
equivalent to 16% disagreed while 11 respondents equivalent to 11% strongly
disagreed on that argument.
Figure 4. 9: Space limitations
Source: Survey Data, (2020)
4.7.5 Insufficient staffing
Figure 4.10 presents that out of all 96 respondents, 14 respondents equivalent to 15%
strongly agreed that insufficient staffing hinders the ergonomics design of the
workplace, 26 respondents equivalent to 27% agreed on the same while 10
respondents equivalent to 10% were neutral on the same statement. On the other hand,
25 respondents equivalent to 26% disagreed while 21 respondents equivalent to 22%
strongly disagreed on that argument.
11%
16%
21%
13%
40%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
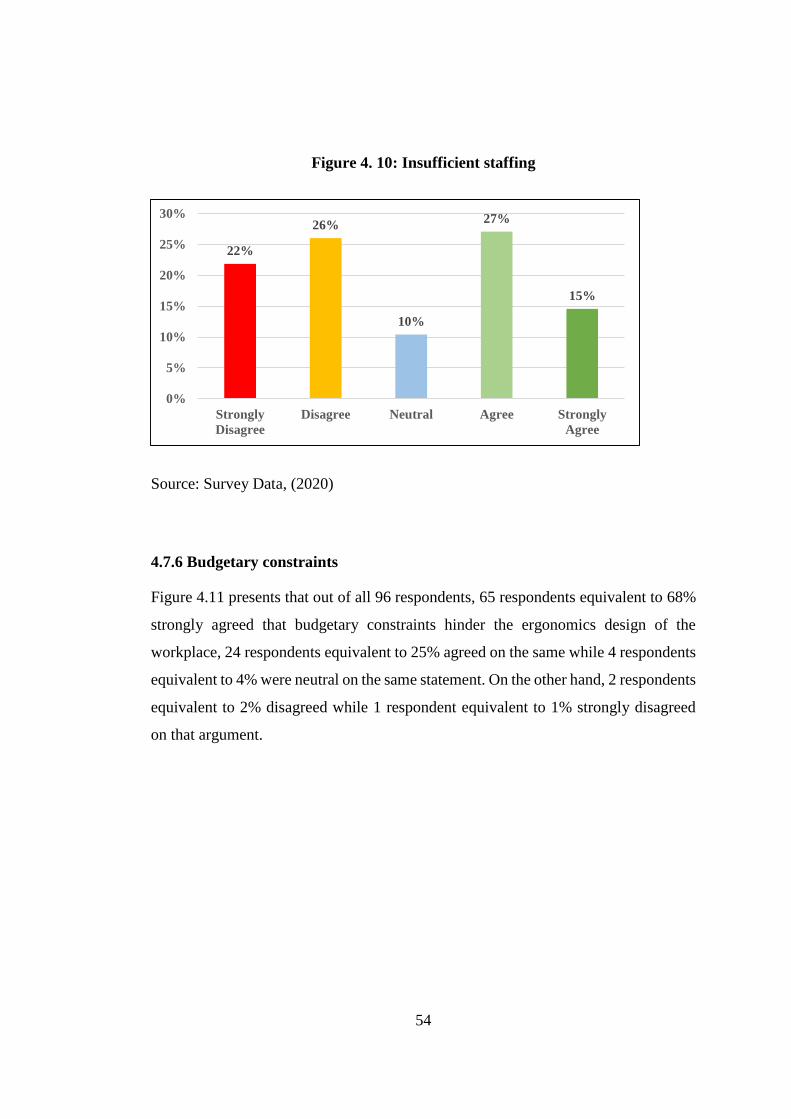
54
Figure 4. 10: Insufficient staffing
Source: Survey Data, (2020)
4.7.6 Budgetary constraints
Figure 4.11 presents that out of all 96 respondents, 65 respondents equivalent to 68%
strongly agreed that budgetary constraints hinder the ergonomics design of the
workplace, 24 respondents equivalent to 25% agreed on the same while 4 respondents
equivalent to 4% were neutral on the same statement. On the other hand, 2 respondents
equivalent to 2% disagreed while 1 respondent equivalent to 1% strongly disagreed
on that argument.
22%
26%
10%
27%
15%
0%
5%
10%
15%
20%
25%
30%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree

55
Figure 4. 11: Budgetary constraints
Source: Survey Data, (2020)
4.7.7 Technological factors
Figure 4.12 presents that out of all 96 respondents, 59 respondents equivalent to 61%
strongly agreed that technological factors hinder the ergonomics design of the
workplace, 23 respondents equivalent to 24% agreed on the same while 8 respondents
equivalent to 8% were neutral on the same statement. On the other hand, 5 respondents
equivalent to 5% disagreed while 1 respondent equivalent to 1% strongly disagreed
on that argument.
1% 2% 4%
25%
68%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
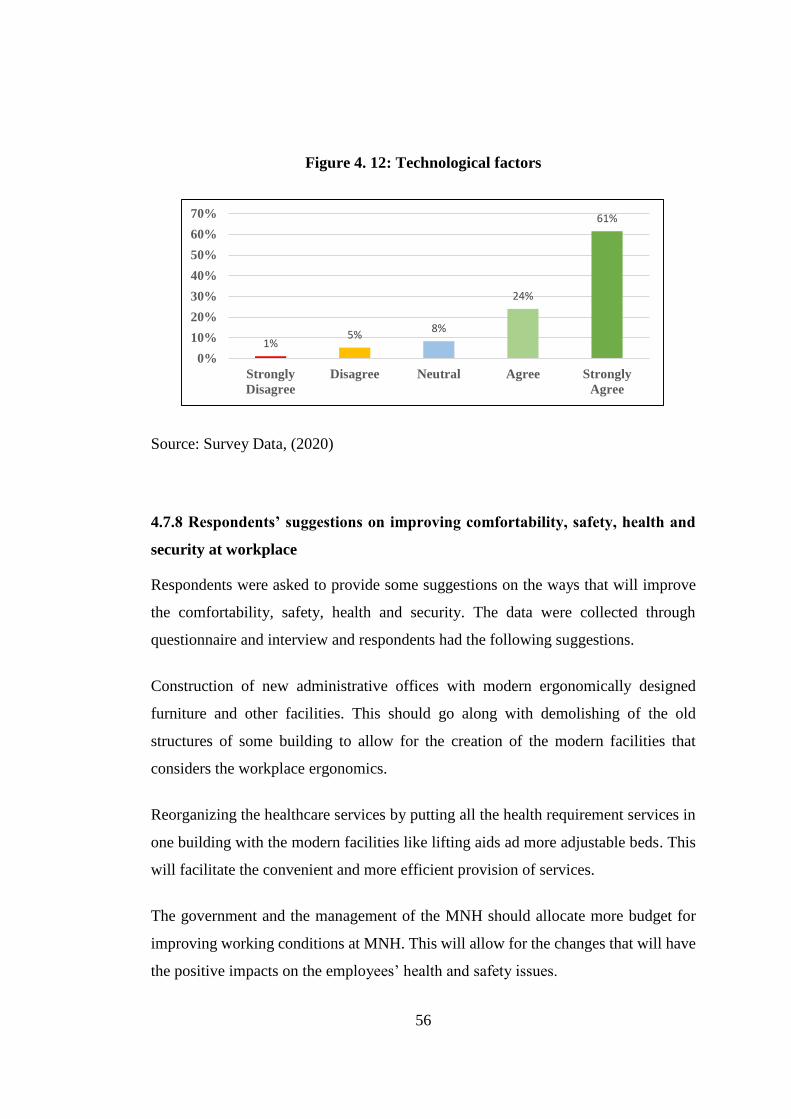
56
Figure 4. 12: Technological factors
Source: Survey Data, (2020)
4.7.8 Respondents’ suggestions on improving comfortability, safety, health and
security at workplace
Respondents were asked to provide some suggestions on the ways that will improve
the comfortability, safety, health and security. The data were collected through
questionnaire and interview and respondents had the following suggestions.
Construction of new administrative offices with modern ergonomically designed
furniture and other facilities. This should go along with demolishing of the old
structures of some building to allow for the creation of the modern facilities that
considers the workplace ergonomics.
Reorganizing the healthcare services by putting all the health requirement services in
one building with the modern facilities like lifting aids ad more adjustable beds. This
will facilitate the convenient and more efficient provision of services.
The government and the management of the MNH should allocate more budget for
improving working conditions at MNH. This will allow for the changes that will have
the positive impacts on the employees’ health and safety issues.
1%5%
8%
24%
61%
0%
10%
20%
30%
40%
50%
60%
70%
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree

57
There should be the continuous provision of seminars and trainings so as to create
more awareness to all employees regarding workplace ergonomics. This should be
aligned with the formulation of rules and regulations that will provide the guidance
for the employees to comply.
58
CHAPTER FIVE
DISCUSSION OF FINDINGS
5.1 Introduction
This chapter provides the interpretations and discussions on the findings that were
realized based on the research questions under this study. The core issue on this
chapter is to interpret and discuss the findings in relation to theoretical and empirical
results. The findings on all research objectives were discussed and interpreted
accordingly. This research was designed to provide answers for the following
objectives; to determine the extent to which workplace ergonomics influence
healthcare employees’ performance at workplace, the case of MNH, to examine
healthcare employees’ awareness about ergonomics design of the workplaces, the case
of MNH and document the barriers towards ergonomic design of workplaces as a tool
for improving employees’ performance in healthcare facilities, the case of MNH.
5.2 Workplace ergonomics and healthcare employee’s performance
The respondents were asked about the influence of workplace ergonomics towards
healthcare employee’s performance. The questions were designed to assess each
workplace ergonomics variable and its influence on the employee’s performance. The
findings revealed that out of 96 respondents,48 respondents equivalent to 50% agreed
that they were uncomfortable with the present state of office/workplace environment
and hence it has affected their performance while 38 respondents equivalent to 40%
disagreed on the same. The findings on the present state of office furniture and its
influence on the performance revealed that out of all 96 respondents, 52 respondents
equivalent to 54% of the respondents agreed that they were uncomfortable with the
present state of office furniture and hence it affected their performance while 37
respondents equivalent to 38% disagreed on the same.

59
The findings on the size of office space and its influence on the performance revealed
that out of all 96 respondents, 58 respondents equivalent to 60% agreed that they were
uncomfortable with office space and hence it affected their performance while 33
respondents equivalent to 33% disagreed on the same. The findings on the level of
noise and its influence on the performance revealed that out of all 96 respondents, 23
respondents equivalent to 24% agreed that they were uncomfortable with level of noise
and hence it affected their performance while 37 respondents equivalent to 39%
disagreed on the same.
The findings on the workplace temperature, airflow and light flow and its influence
on the performance revealed that out of all 96 respondents, 53 respondents equivalent
to 55% agreed that they were uncomfortable with workplace temperature, airflow and
light flow and hence it affected their performance while 33 respondents equivalent to
34% disagreed on the same. In ranking these variables according to the level of their
influence on performance, it can be concluded that office size, workplace temperature,
airflow and light, office furniture, workplace environment and level of noise all affect
employees’ performance.
According to motivation-hygiene theory which was developed Frederick Herzberg,
two sets of factors were identified and grouped into satisfiers factors and dissatisfiers
factors. Relating to these findings, all the workplace ergonomics variables were
identified to have the significant impact on healthcare employee’s performance.
The findings of this study supports the findings by Mendis (2016) in a study of
operational level employees of the apparel industry in Sri Lanka where it was found
that the improvement of work place ergonomics such as equipment, workplace layout,
lighting and ventilation resulted into increased performance of the employees.
Leblebici (2012) highlighted that the physical components which are office layout and
space, ventilation, temperature, physical security and overall comfort of the employee
are among factors which affect the performance of employees. In addition, Pickson et.
al. (2017) identified a positive correlation between workplace ergonomics and
employee performance.

60
5.3 Health care employee’s awareness on workplace ergonomics
The findings on healthcare employee’s awareness on workplace ergonomics revealed
that, 32 respondents equivalent to33% of the all respondents were aware of the office
set up and design in workplace ergonomics, 16 respondents equivalent to 17% of all
the respondents were aware of the equipment and working tools in workplace
ergonomics, 27 respondents equivalent to 28% of all the respondents were aware about
the office furniture and workplace ergonomics, 37 respondents equivalent to 39 % of
all the respondents were aware about the environment issues and workplace
ergonomics, 36 respondents equivalent to 38% of all the respondents were aware of
working posture and manual lifting and 62 respondents equivalent to 65% of the all
respondents were aware of noises effects towards workplace ergonomics. In total, the
average of 35 respondents equivalent to 36% of all respondents were aware about the
workplace ergonomics elements.
According to Maslow’s theory of Hierarchy of Needs, developed by Abraham
Maslow, which categorized five levels of needs which includes physiological needs,
safety, belonging, esteem and self-actualization. The findings revealed that 36% of all
respondents were aware about the workplace ergonomics issues, this was congruent
with the theory as it shows that employees are aware about their needs at the workplace
especiallyphysiological and safety needs as stipulated by the theory. However, the low
rate on employee awareness supports the findings in the study byPandve, (2016) where
it was revealed that awareness on the importance of workplace ergonomics was still
very low for various professional groups. In addition, Olabode et al., (2017
recommended that orientation and training on workplace ergonomics through
seminars and conferences should be an ongoing activity so that employees would be
aware of its benefits.
5.4 Barriers toward ergonomic design of workplaces
The study considered various barriers that hinder the ergonomics design of the
workplace at MNH, the factors on considerations were old design of the hospital, old
infrastructure of the hospital, patient congestion, space limitations, insufficient

61
staffing, budgetary constraints and technological factors. Findings revealed that, out
of all 96 respondents, 59 respondents equivalent to 61% agreed that old design of the
hospital hinders the ergonomics design of the workplace while, 28 respondents
equivalent to 29% disagreed on that argument.
Out of all 96 respondents, 48 respondents equivalent to 50% agreed that old
infrastructure of the hospital hinders the ergonomics design of the workplace while 42
respondents equivalent to 44% disagreed on that argument. Out of all 96 respondents,
34 respondents equivalent to 36% agreed that patient congestion hinders the
ergonomics design of the workplace while 54 respondents equivalent to 56%
disagreed on that argument. Out of all 96 respondents, 50 respondents equivalent to
53% agreed that space limitations hinder the ergonomics design of the workplace
while 26 respondents equivalent to 27% disagreed on that argument. Out of all 96
respondents, 40 respondents equivalent to 42% agreed that insufficient staffing
hinders the ergonomics design of the workplace while 46 respondents equivalent to
48% disagreed on that argument.
Out of all 96 respondents, 89 respondents equivalent to 93% agreed that budgetary
constraints hinder the ergonomics design of the workplace while 3 respondents
equivalent to 3% disagreed on that argument. Out of all 96 respondents, 82
respondents equivalent to 85% agreed that technological factors hinder the ergonomics
design of the workplace while 6 respondents equivalent to 6% disagreed on that
argument. In ranking these barriers towards ergonomics design, it can be concluded
that budgetary constraints, technological factors, old design of the hospital, space
limitations, old infrastructure of the hospital, insufficient staffing and patient
congestion are barriers towards work place ergonomics design at MNH.
According to motivation-hygiene theory which was developed Frederick Herzberg,
the two sets of factors were identified and grouped into satisfiers factors and
dissatisfiers factors. Relating to these findings, barriers identified under this study fall
within the dissatisfiers factors that hinder the ergonomic design of the workplaces.The
findings in this study concur with those of Rasmussen et al., (2017) who listed
62
insufficient financial resources as among the barriers towards workplace ergonomics
design. Furthermore, the study validated the observations on factors hindering
ergonomics applications in the developing countries particularly lesser advancements
in technology (O’Neil, 2000). As also found in this study, poor infrastructure of the
Hospital inhibited by the old design was among the barriers toward workplace
ergonomic considerations confirming one of the challenges toward ergonomics
applications in the developing countries being poor infrastructure to facilitate and
support ergonomic applications and interventions (Jafry and O'Neil, 2000).

63
CHAPTER SIX
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
6.1 Introduction
This chapter presents the summary of the study findings, conclusions,
recommendations, and areas for further research.
6.2 Summary
The main objective of this study was to assess the role of workplace ergonomics on
healthcare employee’s performance, the case of Muhimbili National Hospital in
Tanzania.The specific objectives of the study were: to determine the extent to which
workplace ergonomics influence healthcare employees’ performance at workplace, to
examine healthcare employees’ awareness about ergonomics design of the workplaces
and to document the barriers towards ergonomic design of workplaces as a tool for
improving employees’ performance in healthcare facilities.
The study employed quantitative collection of data whereas questionnaires were
distributed to 96 respondents, who are employees at MNH. The collected data were
descriptively analyzed through the use of frequencies which were presented in tables,
figures and histograms.
The findings of the study revealed that the employee’s performance is affected by
office size, workplace temperature, airflow and light, office furniture, workplace
environment and level of noise. Also it was found that the average of 35 respondents
equivalent to 36% of all the respondents were aware about the workplace ergonomics
issues. Lastly, the budgetary constraints, technological factors and old design of the
hospital were ranked as the top barriers towards ergonomics design at MNH.

64
6.3 Conclusion
Workplace ergonomics and healthcare employee’s performance, following the
assessment that was done regarding the role of workplace ergonomics on healthcare
employees’ performance. It has been found that employees’ performance is affected
by the following workplace ergonomics factors such as office size, workplace
temperature, airflow and light, office furniture, workplace environment and level of
noise. All of these factors were having a significantly impact on the performance of
employees and this calls for various stakeholders to put into consideration on these
factors in making decision concerning general performance of the institutions and the
employees’ welfare.
Health care employee’s awareness on workplace ergonomics, it has been found
that the level of workplace ergonomics awareness among the employees is slightly
low. This has been the case for many developing countries whereby poverty and
technological backwardness hinders the process. In order to address this problem, all
stakeholders must emphasize on the need to conduct trainings and seminars to
employers and employees so as to create strong awareness that will guide and bring
positive changes to the workplace ergonomics issues.
Barriers toward ergonomic design of workplaces, it has been found that budgetary
constraints, technological factors and old design of the hospital were ranked as the top
barriers towards ergonomics design at MNH. In order to make sure that the workplace
ergonomics design is adhered, the management of MNH should allocate the enough
budget and invest much in technological innovation so as to make the improvement
on the required state of the ergonomics considerations.
Maslow’s theory of Hierarchy of Needs, Abraham Maslow categorized five levels of
needs among them are physiological needs and safety needs, these needs were
identified to have a direct connection with workplace ergonomics considerations. In
Motivation-hygiene, Frederick Herzberg identified two factors which are satisfiers and
dissatisfiers which were also related to work place ergonomics variables and
65
healthcare employee’s performance. The findings from this study imply that there is a
need for improvement of workplace ergonomics in healthcare facilities and
development of awareness on ergonomic design of workplaces in the facilities. Further
there is a need for more investment on technological advancement to support
workplace ergonomics and allocation of sufficient financial resources to facilitate
ergonomic design of workplaces. The study calls for the considerations of workplace
ergonomics design so as to improve performance of employees. These findings attract
the attention of all the stakeholders especially in healthcare institutions to factor in
workplace ergonomics variables in appraising the performance of their employees.
6.4 Recommendations
Following the objectives of this study and the findings that were revealed from the
assessment that was conducted on role of workplace ergonomics on healthcare
employee’s performance by using the case of MNH in Tanzania. The study provides
recommendations the healthcare service providers in the country as follows.
The study recommends more training that will boost up the employee’s awareness on
workplace ergonomics especially in the healthcare industry. This has been the case for
most of the industrially developing countries whereby most people have been found
to be unaware of the workplace ergonomics issues hence it exposed them to some
health and safety risks in their performance at work.
Investment on technology and allocation of more financial and human resources on
improvement of workplace ergonomics. Healthcare institutions should invest more on
the adoption of reliable and modern technology that will enhance the improvement of
workplace ergonomics. This should go together will allocation of more and enough
resources on implementation of the workplace ergonomics strategies.
Lastly, healthcare facilities should be designed in a way that considers and supports
the existence of modern facilities, provides enough space that allow the flexibility and
convenient movement of the workers, tools and equipment. The building designs must

66
also consider and support for the natural control of working environment issues such
as temperature, airflow and illumination.
6.5 Areas for further study
This study was conducted to assess the role of workplace ergonomics on healthcare
employee’s performance and other related issues. The findings show that there is
significant impact of workplace ergonomics on healthcare employee who are working
at MNH which is a public hospital in Tanzania. Despite these findings, this study
offers a need for further studies to be carried on investigate more or the same
workplace ergonomics variables for the employees who are working in the private
health sector. Following this, it will be easy to make the relevant conclusions for the
whole health sector in the country.
67
REFERENCES
Adeyemi, H. O., Adejuyigbe, S. B., Akanabi, O. G., Ismaila, S. O., & Adekoya, A. F.
(2014). Decree of Safe Postures in Manual Lifting Tasks among Some
Groups of Contsruction Workers in Southwestern Nigeria. International
Journal of Ergonomics, 24-32.
Al-Anzi, N. (2009). Workplace Environment and Its Impact on employee
Performance. MBA Thesis submitted to Open University of Malaysia.
Malaysia.
Alli, B. O. (2008). Fundamental Principles of Occupational Health and Safety.
Geneva: ILO Office-Geneva.
Baxter, P., & Jack, S. (2008). Qualitative Case Study Mthodology: Study Design and
Implementation for Novce Researchers. The Qualitative Report, 544-559.
Carayon, P. Kianfar, S. & Xie, A. (2013), Human Factors and Ergonomics as a Patient
Safety Practice. BMJ Quality & Safety Journal, 1-10.
Carini, F., Mazzila, M., & Giovanni, T. (2017). Posture and Posturology, Anatomical
and Physiological Profiles: Overview and Current Status of Art. Acta Bio-
Medica, 11-16.
Carmen, C. (2013). office-design-affects-employee performance. Retrieved from
www.carmenrealestate.com:
http://www.carmenrealestate.com/blog/bid/317204/office-design-affects-
employee performance
Chim, J. M. (2017). Creating an Ergonomic Workplace by Design. Proceedings of the
2nd Asian Conference on Ergonomics and , (pp. 376-379).

68
Chinyere, I. N. (2014). Influence of Workstation and Posture Ergonomics on Job
Satisfaction of Librarians in the Federal and State University Libraries in
Southern Nigeria. Journal of Humanities and Social Science, 78-84.
Coenen, P., Gouttebarge, V., & Van der Burght, A. S. (2014). The Effect of Lifting
during work and Low Back Pain: A Health Impact Assessment based on a
meta-analysis. Occupational Environment Medicine.
Cohen L, Manion L, Morrison KRB. Research Methods in Education. 6th ed. UK:
Routledge, Oxon; 2007. 657 p. ISBN-10: 0415368782, ISBN-13: 978-
0415368780
Davis, K., & Kotowski, S. E. (2015). Prevalence of Musculoskeletal Disorders for
Nurses in Hospitals, Long term Care Facilities and Home Healthcare: A
Comprehensive Review. Human Factors, 754-792.
Deckers,, L. (2018). Motivation: Biological, Psychological and Environmental.
Routledge Press.
DeNisi, A. S., & Pritchard, R. D. (2006). Performance Appraisal, Performance
Management and Improving Individual Performance: A Motivational
Framework. Management and Organization Review, 253-277.
Deros, B. M., Darius, D. D., & Basir, I. M. (2015). A Study on Ergonomic Awareness
among Workers Performing Manual Material Handling Activities. Procedia
Social and Behavioral Sciences, 1666-1673.
Driessen, M.T, Proper, K., Tulder, M.W., Anema, J.R., Bongers, P.M., &Beek, A.J.
(2009). The Effectiveness of physical and organizational ergonomic
interventions on low back pain and neck pain: a systematic review. BMJ;
Occupational &Environmental Medicine, Vol. 67, Issue 4.
69
Dul, J., & Weerdmeester, B. (2008). Ergonimics for Beginners. Boca Raton: CRC
Press.
Fernandez, J. E. (1995). Ergonomics in the Workplace. Journal of Facilities, 20-27.
Gatchel, R. J., & Kishino, N. (2011). Pain, Musculoskeletal injuries and return to
work. In J. C. Quick, & L. E. Tetrick, Handbook of Occupational Health
Psychology (2nd Ed.). Washington DC: American Psychological
Association.
Ghosh, S., Bagchi, A., Sen, B., & Bandyopadhyay, P. (2011). Ergonomics: Bridge
between Fundamentals and Applied Research. Indian Journal of
Occupational and Environmental Medicine, 14-17.
Gurses, A.P., Carayon, P. & Wall, M. (2009). Impact of performance obstacles on
Intensive care Nurses' Workload, perceived quality and safety of care and
quality of working life. Health Service. Res., 422-443.
Harrison, H., Birks, M., Franklin, R., & Mills, J. (Eds.) (2017). Case study research:
Foundations and methodological orientations. : Vol. 18.
Haynes, B. P. (2008). The Impact of Office Comfort on Productivity. Journal of
Facilities Management, 6: https://doi.org/10.1108/14725960810847459,
37-51.
Helriegel, D., Jackson, S. E., & Slocum, J. (2004). Management. Cape Town, South
Africa: Oxford University Press.
Herzberg, F. (1974). Motivation-hygiene profiles. Organizational Dynamics, 18-29.
Herzberg, F. (n.d.). Motivation-Hygiene profiles. Organizational Dynaics.

70
Huck-soo, L., & Richardson, S. (2012). Ergonomics in Industrially Developing
Countries: A Literature Review. Journal of Humanities and Ergonomics
(Tokyo), 1-16.
Husain, M. J. (2010). Contribution of Health to Economic Development: A Survey
and Overview. Economics E-Journal , 1-52.
International Labour Organization. (2013). The Prevention of Occupational Diseases.
Geneva: ILO.
Ismaila, S. O. (2010). A Study on Ergonomics Awareness in Nigeria. Australian
Journal of Basic and Applied Sciences, 731-734.
Israel, Glenn D. (1992): Determining sample size.
Jadhav, A. P., Dharmapuri, V. M., Ashok, S., & Sancheti, P. K. (2019). Prevalence,
Severity and Characteristics of Work Related Musculoskeletal Disorders
Amongst Obstetrics and Gynaecology Professionals. International Journal
of Community Medicine and Public Health, 2605-2609.
Jaffar, N., Abdul-Tharim, A. H., Mohd-Kamar, I. F., & Lop, N. S. (2011). A Literature
Review of Ergonomics Risk Factors in Construction Indusrty. Precedia
Engineering, 89-97.
Jafry, T., & O'Neil, D. H. (2000). The Application of Ergonomics in Rural
Developement: A Review. Applied Ergonomics, 1391-1402.
Jagannath, M., & Adalarasu, K. (2012). An Ergonomics Risk Assessment for Hospital
Workers. International Journal of Engineering Research and Applications
(IJERA), 864-867.
Janowitz, I. L., Gillen, M., Rempel, D., & Trupin, L. (2006). Measuring the Physical
Demands of Work in Hospital Settings: Design and Implemetation of an
Ergonomics Assessment. Applied Ergonomics, 641-658.

71
Kahare, E. W. (2012). Assessment of the Role of Strategic Ergonomics on Employee
Performance in the Health Sector in Kenya: A Study of Health Workers in
Nakuru County. International Journal of Science and Research (IJSR),
2101-2107.
Kahya, E. (2007). The Effects of Job Characteristics and Working Conditions on Job
Performance. International Journal of Industry and Ergonomics, 515-523.
Karakas, F. (2010). Sprirituality and Perfofmance in Organizations: A Literature
Review. Journal of Business Ethics, 89-106.
Kim, I. (2017). Ergonomic Explorations for the Safety and Health Improvement in
Hospital and Healthcare Professions. Journal of Ergonomics, 1-3.
Kingsley, A. (2012). The Impact of Office Ergonomics on Employee Performance; A
Case Study of the Ghana National Petroleum Corporation. A Thesis
submitted to the Institute of Distance Learning, Kwame Nkrumah University
of Science and Technology. Ghana.
Kivunja, P.C., & Kuyini, A.B. (2017). Understanding and Applying Research
Paradigms in Educational Contexts. International Journal of Higher
Education, Vol. 6, 26-41.
Kothari, C. R. (2004). Research methodology: Methods & techniques (2nd rev. ed.).
New Delhi: New Age International (P) Ltd.
Kumar, S. (2001). Theories of Musculoskeletal Injuries Causation. Ergonomics, 17-
47.
Leblebici, D. (2012). Impact of Workplace Quality on Employee's Productivity: Case
Study of a bank in Turkey. Journal of Business, Ergonomics and Finance,
38-40.
72
Marmaras, N., & Nathanael, D. (2016). Workplace Design. In G. Salvendy, Workplace
Design. Handbook of Human Factors & Ergonomics, 3rd Ed. (pp. 1-23).
New York: John Wiley & Sons.
Maslow, A. H. (1954). Motivation and Personality. New York: Harper.
Matthys, H., Bohets, W., & Hermans, V. (2019). Effectiveness of Specific Lifting
Techniques and Tools on Workload in a Lifting Situation-A Case Study.
Healthcare Ergonomics, 640-647.
Mc Neill, M., Parsons, K. C., & Neill, D. O. (2000). Ergonomics in Industrially
Developing Countries. Journal of Ergonomics .
McCormic, J., & Sanders, M. S. (1992). Human Factors in Engineeriing and Design.
McGraw Hill International.
McCormick, J., & Sanders, M. S. (1992). Human Factors in EEngineering and
Design. McGraw Hill International.
Mendis, M. (2016). Workplace Design and Job Performance: A Study of Operational
Level Employees in the Apparel Indusry of Sri Lanka. International Journal
of Scientific and Research Publications, 148-153.
Milanzi, N. C. (2009). Research Methods in Social Sciences: Theory, Philosophy,
Methodology and Observation. Morogoro: Mzumbe University.
Muhimbili National Hospital. (2017). Muhimbili National Hospita's Strategic Plan
2017-2022. Dar Es Salaam: Muhimbili National Hospital.
Muhimbili National Hospital. (2019). Muhimbili National Hospital Annual Report
2018-2019. Dar Es Salaam: Muhimbili National Hospital.

73
Mukhtad, A. A. (2017). Prevalence and Risk Factors for Low Back Pain Among
Nurses at Benghazi Medical Centre, Libya. International Journal of Medical
and Surgical Science, 88-91.
Museru, L. M., & Grob, U. (2003). Public/Private Mix: An Alternative Funding for
Public Hospitals in Developing Countries: A 5 Years Experience of
Muhimbili Orthopedics Institute Dar es Salaam-Tanzania. East&Central
Africa Journal of Surgery, Vol 8 (1), 11-14.
Nassiri, P., Monazam, M., & Fouladi, D. B. (2013). The Effect of Noise on Human
Performance: A Clinical Trial. International Journal of Occupational
Environment and Medicine, 87-95.
Nchimbi, A. (2019). Implementation of Open Performance Review and Appraisal in
Tanzania Local Government Authorities: Some Observations and Remarks.
International Journal of African and Asian Studies.
Occupational Health and Safety Authority of Ireland. (2015). Ergonomics: Good
Practice in the Irish Workplace. Dublin: The Health and Safety Authority.
Olabode, S. O., Adesanya, A. R., & Bakare, A. A. (2017). Ergonomics Awareness and
Employee Performance: An Exploratory Study. Economic and
Environmental Studies, 813-829.
O'Neill, D. (2000). Ergonomics in Industrially Developing Countries: Does its
Application Differ from that in Industrially Developed Countries? Applied
Ergonomics, 631-640.
O'Neill, M., & Albin, T. (2011). Holistic Ergonomics for the Evolving Nature of Work.
New York: Knoll Inc.
Pandve, H. T. (2016). Awareness about Ergonomics. Journal of Ergonomics, VL 06,
1-2.
74
Pickson, R. B. (2017). Investigating the Effect of Ergonomics on Employee
Productivity: A Case Study of the Butchering and Trimming Line of Pioneer
Food Cannery in Ghana. Modern Economy,8, 1561-1574.
Pradhan, R. K., & Jena, L. K. (2016). Employee Performance at Workplace:
Conceptual Model and Empirical Validation. Business Perspectives and
Research, 1-17.
Pual, A. (2012). A pilot study on Awareness of Ergonomics and Prevalence of
Muskuloskeletal Injuries among Nursing Professionals. International
Journal of Nursing Education,4, 1-4.
Pulakos, E. D. (2004). Performance Management. USA: Society for Human Resource
Management.
Qutubuddin, S. M., Hebbal, S. S., & Kumar, A. S. (2013). A Review on Effect of
Industrial Noise on the Performance of Worker and Productivity.
International Review of Applied Engineering Research, 43-54.
Rasmussen, C. D. N., Lindberg, N. K., Ravn, M. H., Jørgensen, M. B., Søgaard, K.,
& Holtermann, A. (2017). Processes, barriers and facilitators to
implementation of a participatory ergonomics program among eldercare
workers. Applied ergonomics, 58, 491–499.
Roeloelofsen, P. (2002). The Impact of Office Environment on Employees
Performance: The Design of the Workplace as a Strategy for Productivity
Enhacement . Journal of Facilities Management, 247-264.
Sanders M.S., M. J. (1992). Human Factors in Engineering and Design. McGraw Hill
International.
Shahnavaz, H. (2000). Role of Ergonomics in Transfer of Technology to Industrially
Developing Countries. Journal of Ergonomics, 903-907.

75
Shengli, N. (2010). Ergonomics and Occupational Health and Safety : An ILO
Perspective. Applied Ergonomics, 744-753.
Shiromani, J., Mulder, E. A., & Ijzermans, J. N. (2016). Ergonomics in the Operating
Room. Surgical Endoscopy, 2457-2466.
Smith, M.J., Carayon, P. & Cohen, W. (2002). Design of Computer Workstations.
Human-Computer Interaction Fundamentals, 289-302 Boca Ranton, FL:
CRC Press.
Shultz, D. P., & Sydney, E. (2010). An Introduction to Industrial and Organizational
Psychology (10th ed.). New York City: Prentice Hall.
Tarus, H. K. (2011). Employee Perceptions of Factors Affecting Productivity At Aga
Khan University Hospital, A Reserach Submitted in Partial Fulfilment of the
Award of Degree of Masters of Business Administration, University of
Nairobi.
Tarus, H. K. (n.d.). Employee Perceptions of Factors Affecting Productivity At The
Aga Khan University Hospital, Nairobi, A research Project Submitted in
Partial Fulfilment of the Requireents For the Award Of The Degree of
Masters of Business Administration (MBA), University .
Tayyari, F., & Smith, J. L. (1997). Occupational Ergonomics: Principles and
Applications. London: Chapman and Hall.
Te-Hsin, P., & Kleiner, B. H. (2001). New Developments Concerning the
Occupational Safety and Health. Journal of Managerial Law, 138-146.
Tripathy, S. P. (2014). Impact of Motivation on Job Performance of Contractual Staff
in Devi Ahilya University . Indian Journal of Research, 1-5.
Vieira, E. R., & Kumar, S. (2004). Working Postures: A Literature Review. Journal
of Occupational Rhabilitation, 143-159.

76
World Health Organization . (2010). Monitoring the Building Blocks of Health
Systems: A Handbook of Indicators And Their Measurement Strategies.
Geneva: WHO Press.
Yankson, E. (2012). The Effect of Health and Safety Standards on Productivity in
Ghana Rubber Estates Limited. Unpublished Master's Thesis, Institute of
Distance Learning, Kwame Nkrumah University of Science and Technology,
Kumasi. Ghana.
Yin, R. K. (2003). Case Study Research: Design and Methods. Sage Publications.
77
APPENDIX I
QUESTIONNAIRE FOR DATA COLLECTION
TOPIC: ROLE OF WORKPLACE ERGONOMICS ON HEALTHCARE
EMPLOYEES’ PERFORMANCE; A CASE OF MUHIMBILI NATIONAL
HOSPITAL, TANZANIA
INTRODUCTION:
This is an academic work aimed at collecting primary data to assist in the findings of
the research study titled above. Your voluntary cooperation by providing open, correct
and honest answers will assist the researcher in coming with true and correct findings
and will be highly appreciated. Thank you very much in advance.
Please tick the correct response
PART A: SOCIO-DEMOGRAPHIC DATA OF THE RESPONDENT
1. Gender 1. Male [ ] 2. Female [ ]
2. Age 1. 20-29 years [ ] 2. 30-39 years [ ] 3. 40-49 years [ ] 4.
50 years and above [ ]
3. Field of work 1. Clinical [ ] 2. Non-
clinical/supportive [ ]
4. Level of work 1. Junior staff [ ] 2. Middle level staff [ ] 3. Senior Staff [ ] 4.
Management [ ]
5. Department/Unit
_____________________________________________________

78
6. Working experience at MNH 1. 1-3 years [ ] 2. 4-6 years [ ] 3.
7-10 years [ ] 4. More than 10 years [ ]
PART B: LEVEL OF HEALTH CARE EMPLOYEE’S AWARENESS ON
WORKPLACE ERGONOMICS
7. Ergonomics is defined as a scientific study on the interactions and
compatibility between people and other aspects of his life or environment
including machines, tools and systems; the same applies to workplace
ergonomics.
Please indicate your level of awareness on the ergonomics design of the
workplace from 1 to 5 by rating your agreement on the following statements
about ergonomic design of workplaces:
Variable Measure Level of Awareness
1 2 3 4 5
Employers should consider workplace ergonomics when
designing work and workplaces
Work stations should have ergonomic considerations to
allow comfortability to the worker and avoid risks and
accidents
Working equipment should have ergonomic considerations
to allow comfortability to the worker and avoid risks and
accidents
Office furniture should have ergonomic considerations to
allow comfortability to the worker
Well ventilated rooms/offices affects workers performance
Manual lifting work may have health effects to workers if
not well designed
Some tasks may lead the workers to sit in awkward postures
which may have health effects if not well designed

79
Office/Workplace that is subjected to excessive noise can
cause lack of concentration and even health effects to the
workers
1=Strongly Disagree; 2=Disagree; 3=Neutral; 4= Agree; 5=Strongly Agree;
PART C: LEVEL OF HEALTH CARE EMPLOYEE’S SATISFACTION WITH
OFFICE DESIGN AND ENVIRONMENT
8. Please indicate your level of satisfaction with workplace ergonomics elements
of your workplace as indicated below:
Workplace Ergonomics Elements Level of Satisfaction
1 2 3 4 5
General design of the office
State and suitability of office furniture
Size of space allocated to your workplace
State of the working equipment
Room temperature
And air flow and illumination
Level of noise (from speech or equipment)
1= Very Unsatisfied; 2= Unsatisfied; 3= Neutral; 4= Satisfied; 5=; Very Satisfied
PART D: WORKPLACE ERGONOMICS AND EMPLOYEE’S HEALTH AND
SAFETY
9. Does your office have enough space for easy movement while working?
1. Insufficiently spaced [ ] 2. Neutral [ ] 3. Sufficiently spaced [ ]
80
10. Does your work involve heavy manual lifting of materials and other objects?
1. Never [ ] 2. Not much [ ] 3. Very much [ ]
11. Have you ever felt stressed by your workplace environment (design, set up,
furniture, air conditioning, noise etc)
1. Not stressed [ ] 2. Stressed [ ] 3. Very Stressed [ ]
If stressed why?
___________________________________________________________
___________________________________________________________
__
12. Do you feel that your office/workplace environment (chair, desk, and
computer) has affected your health in any way?
1. Not Affected [ ] 2. Affected [ ] 3. Very Affected [ ]
If affected, how?
______________________________________________________________
______________________________________________________________
__
13. Do you feel that how you handle your work (posture, lifting, and necessary
bending) has affected your health in any way?
1. Not Affected [ ] 2. Affected [ ] 3. Very much affected [ ]
If affected, how?
______________________________________________________________
____________________________________________________
81
14. Have you ever suffered any injury/disorder due to your current work or
workplace conditions?
1. Never[ ] 2.[ ] Once 3. More than once [ ]
If you have suffered any injury or disorder please state, the nature of illness/disorder
and the attributed cause:
____________________________________________________________________
_______________________________________________________________
15. To what extent did the illness/disorder affect your job performance?
1. Not affected [ ] 2. Affected [ ] 3. Very much affected [ ]
Please elaborate how your job performance was affected by the illness/disorder
suffered:
____________________________________________________________________
____________________________________________________________________
16. Have you ever been absent from work because of an injury/illness you suffered
at work?
1. Once [ ] 2. Never 3. More than once [ ]

82
PART E: PHYSICAL WORKPLACE ENVIRONMENT ON EMPLOYEE’S
PERFORMANCE
17. Please indicate the level of performance on the following elements of the
physical workplace environment descriptions.
Description of physical workplace environment description
toward employee’s performance
Level of Agreement
1 2 3 4 5
Office/workplace environment
Furniture
Size of space allocated to your office/workplace
Level of noise at your office/workplace
Office/Workplace temperature
And air flow and illumination
Air and light flow at your office/workplace
1= Very uncomfortable and unsupportive; 2= Uncomfortable and unsupportive; 3=
Neutral; 4= Comfortable and supportive; 5= Very comfortableand supportive;
83
PART F: BARRRIERS TOWARD ERGONOMIC DESIGN OF
WORKPLACES AT MNH
18. Please indicate your understanding on what factors could be hindering the
ergonomics design of the workplace at MNH from 1 to 5 by rating your
agreement on the following:
Factors Level of Agreement
1 2 3 4 5
Old design of the Hospital
Old infrastructure of the Hospital
Patient congestion
Space limitations
Insufficient staffing
Budgetary constraints
Technological factors
1=Strongly Disagree; 2=Disagree; 3=Neutral; 4= Agree; 5=Strongly Agree;
19. Please offer any suggestions that will improve your comfortability, safety,
health and security at the workplace:
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
THANK YOU VERY MUCH FOR YOUR COOPERATION AND RESPONSES!

84
APPENDIX II
INTERVIEW GUIDE
1. Which department do you work in?
2. Are you in clinical or supportive services?
3. How long have you been working at MNH?
4. Are you aware of the concept of workplace ergonomics?
5. Do you agree that it is important for employers to consider workplace ergonomics
in designing workplaces and jobs to fit the workers?
6. Do you agree that work stations should provide comfortability to the workers and
avoid the likelihood of injury/illness?
7. Do you agree that office furniture should provide comfortability to the worker to
allow smooth performance?
8. Do you agree that manual lifting of objects or patients can cause health risks to the
workers?
9. Do you agree that some working postures may cause health risks to the workers?
10. Do you agree that excessive noise in the working area may have effect on
performance?
11. Are you satisfied with the following in your working environment?
i. General design of the office
ii. State and suitability of office furniture
iii. Size of space allocated to your workplace
85
iv. State and suitability of the working equipment
v. Room temperature
vi. And air flow and illumination
vii. Level of noise (from speech or equipment)
12. Does your office have enough space for easy movement while working?
13. Does your work involve heavy manual lifting of materials and other objects?
14. Have you ever felt stressed by your workplace environment (design, set up,
furniture, air conditioning, noise etc)
If stressed why?
15. Do you feel that your office/workplace environment (chair, desk, and computer)
has affected your health in any way?
If affected, how?
16. Do you feel that how you handle your work (posture, lifting, and necessary
bending) has affected your health in any way?
If affected, how?
17. Have you ever suffered any injury/disorder due to your current work or workplace
conditions?
If you have suffered any injury or disorder please state, the nature of illness/disorder
and the attributed cause:
18. To what extent did the illness/disorder affect your job performance?

86
Please elaborate how your job performance was affected by the illness/disorder
suffered:
19. Have you ever been absent from work because of an injury/illness you suffered at
work?
20. How do you feel the following factors provide comfortability and support toward
your performance?
i. Office/workplace environment
ii. Furniture
iii. Size of space allocated to your office/workplace
iv. Level of noise at your office/workplace
v. Office/Workplace temperature
vi. And air flow and illumination
vii. Air and light flow at your office/workplace
21. What do you think could be the barriers toward ergonomics design of the
workplace at MNH
22. Please offer any suggestions that will improve your comfortability, safety, health
and security at the workplace: