roche analyst event - roche - doing now what …aacdf299-ac1c-4a55-bef5-6a...robert a. burger et al,...
TRANSCRIPT

1
46th ASCO Annual Meeting
Roche Analyst Event
Sunday, June 6, 2010 - Chicago
2
This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as ‘believes’, ‘expects’, ‘anticipates’, ‘projects’, ‘intends’, ‘should’, ‘seeks’, ‘estimates’, ‘future’ or similar expressions or by discussion of, among other things, strategy, goals, plans or intentions. Various factors may cause actual results to differ materially in the future from those reflected in forward-looking statements contained in this presentation, among others:
1. pricing and product initiatives of competitors;
2. legislative and regulatory developments and economic conditions;
3. delay or inability in obtaining regulatory approvals or bringing products to market;
4. fluctuations in currency exchange rates and general financial market conditions;
5. uncertainties in the discovery, development or marketing of new products or new uses of existing products, including without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products;
6. increased government pricing pressures;
7. interruptions in production;
8. loss of or inability to obtain adequate protection for intellectual property rights;
9. litigation;
10. loss of key executives or other employees; and
11. adverse publicity and news coverage.
Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to mean that Roche’s earnings or earnings per share for this year or any subsequent period will necessarily match or exceed the historical published earnings or earnings per share of Roche.
For marketed products discussed in this presentation, please see full prescribing information at www.roche.com or www.gene.com.
All mentioned trademarks are legally protected.

3
Agenda
• Setting the standard of care in oncology
– Pascal Soriot, Chief Operating Officer Roche Pharmaceuticals
• Avastin in ovarian cancer, GOG-0218 study
– Jakob Dupont, M.D., Associate Group Medical Director, Avastin Global Clinical Development, Genentech
• Overview of Avastin development program
– Stefan Frings, M.D., Avastin Franchise Director, Roche
• MabThera/Rituxan maintenance in previously untreated patients with follicular lymphoma (PRIMA study)
– Professor Gilles Salles, M.D., Ph.D., Principal Investigator of PRIMA study, Centre Hospitalier Lyon-Sud, France
• Summary and Q&A: Mondher Mahjoubi and Karl Mahler
4
Setting the standard of care in oncology
Pascal Soriot, COO Roche Pharmaceuticals

5
Focus on improving the standard of care
Improve outcome with existing products
Clin
ical
ben
efit New products
• Roche’s own products• Combinations
Improving treatment within a class / product
Advances through medical breakthroughs / novel mechanisms
6
Our starting point: Superior clinical efficacyThe example of Avastin
mCRC mNSCLC mBC
1. Hurwitz, et al. NEJM 2004; 2. Saltz, et al. JCO 2008; 3. Sandler, et al. NEJM 2006; 4. Reck, et al. JCO 2009; 5. Gray, et al. JCO 2009; 6. Avastin SmPC; 7. Robert, et al. ASCO 2009; 8. Brufsky, et al, SABCS 2009; 9. Burger, et al, ASCO 2010; 10. Giantonio et al. JCO 2007
AVF2107g1
OS: HR=0.66p<0.001
NO169662
PFS: HR=0.83p=0.0023
E45993
OS: HR=0.79p=0.003
E21005
PFS: HR=0.48p<0.0001
AVAiL4
PFS: HR=0.75/0.82p=0.003/0.03
AVADO6
PFS: HR=0.67p=0.0002
RIBBON-17
PFS: HR=0.69/0.64p=0.0002/0.0001
Ovarian
GOG-02189
PFS: HR=0.717/0.645p=<0.0001
RIBBON-28
PFS: HR=0.78p=0.0072
E320010
OS: HR=0.75p=0.001

7
Improving clinical outcome with existing products
Maximizing the clinical benefit
Longer treatment duration
Maintenance treatment
Treatment through Multiple Lines (TML)
8
Bevacizumab 15 mg/kg
15 months
Carboplatin+Paclitaxel
Placebo
PlaceboBevacizumab
15 mg/kg
I
II
III
Arm
Carboplatin+Paclitaxel
Carboplatin+Paclitaxel
Avastin in 1st line ovarian cancerFirst clinical breakthrough in over a decade
Primary endpoint: Avastin+chemo followed by Avastin alone for up to 15 months significantly increased median PFS
Impact on ovarian cancer therapy*
2008
2018
*Decision Resources, May 2010
Longer treatment duration

9
Treatment through Multiple Lines (TML)ARIES: Avastin benefit beyond progression in mCRC
ARIES study (n=1,547 patients)Median OS:
Avastin-based treatment: 27.5 months
Non-Avastin regimen: 18.7 months
Chemotherapy+Avastin→PD → Chemotherapy +/-Avastin
Design
FPI Q1 2006Status
Overall survivalPrimary Endpoint
5 mg/kg q2 weeks or 7.5 mg/kg q3 weeks
Avastin Dose
N=810# of Patients
Phase IIIML18147
Treatment through Multiple Lines (TML)
Phase/Study
Metastatic Colorectal Cancer
Patient Population
TML prospective study
Enrollment completed June 2010
Treatment through Multiple Lines (TML)
BRiTE registry (n=1,953 patients)Median OS:
Avastin-based treatment: 31.8 months
Non-Avastin regimen: 19.9 months
Cohn, et al. ASCO 2010, Abstract #3596
10
Rituxan helps patients stay in remission for longer
Transforming cancer into a chronic disease
• Follicular lymphoma incurable
Pattern of relapse and repeated therapy
• Disease control is the key treatment goal
• PRIMA - potentially changing the treatment paradigms
• Additional 2 years of treatment after induction therapy
PRIMA: 2-year maintenance treatment with Rituxanfollowing induction therapy with Rituxan and
chemotherapy
Maintenance treatment
Even
t-fr
ee r
ate
Rituxan maintenanceN=505
Time (months)
ObservationN=513
60 12 18 24 30 36 42
0.8
0.6
0.4
0.2
0
1.0 82%
66%
HR = 0.50 [95% CI= 0.39, 0.64] p-value < 0.0001

1111
Avastin
Anti-P
IGF
Anti-N
RP
1
Anti-EG
FL7
G-secretase
inh
Herceptin
Pertuzum
ab
T-DM
1
Tarceva
GA
201
Xeloda
MabThera/R
ituxan
Anti-C
D20/G
A101
BR
AF
Inh
RG
7167/CIF (M
EKi)
RG
7420(M
EKi)
RG
7321(P
I3Ki)
RG
7422 (PI3K
/mTor)
RG
7440 (Akti)
Dulanerm
in
Bcl-2/A
BT-263
MD
M2
Antagonist
RG
7304/CK
I27
Hedgehog Inh
Anti-M
et/MetM
Ab
huMA
bG
lypican-31
Topoisomerase
I inh1
Breast cancer
Lung cancer
Colon cancer
Melanoma
Glioblastoma
Solid Tumors
Hematology
Halozyme
Pathway/MOA Angiogenesis HER2 HER1 B-Cell PI3K/Akt/MEK/BRAF Apo Other
Oncology: Setting the standard of careCombining products in our portfolio
1 Opt-in opportunity from Chugai
12
Combining targeted therapies and changing medical practice
CLEOPATRA ph III1L mBC, HER2+Herceptin + pertuzumab
Ph Ib/IIHeavily pretreated mBC, HER2+T-DM1 + pertuzumab
MARIANNE phase III*1L mBC, HER2+T-DM1 + pertuzumab
Ph Ib2L mBC, HER2+PI3Ki (RG7321) + T-DM1
Ph IbSolid tumorsPI3Ki (RG7321)+MEKi (RG7420)
NeoSphere rand ph IIneo-adjuvant BC HER2+Herceptin + pertuzumab
AVEREL ph III1L mBC , HER2+Herceptin + Avastin
TrialIndicationCombination
*in preparation

13
Transforming cancer care
In 2010, it is estimated that 250,000 patients will be treated with Avastin
New paradigm shift in cancer treatment: benefit with increased treatment duration
Providing access to the new treatment regimens (e.g. longer duration)
Strong portfolio with focus on personalized healthcare
14
Jakob Dupont, M.D.Associate Group Medical Director, Genentech
Avastin: Phase III GOG-0218
Phase III trial of bevacizumab in the primary treatment of advanced epithelial ovarian, primary peritoneal, or fallopian tube cancer: A Gynecologic Oncology Group (GOG) study
Robert A. Burger et al, ASCO 2010
15
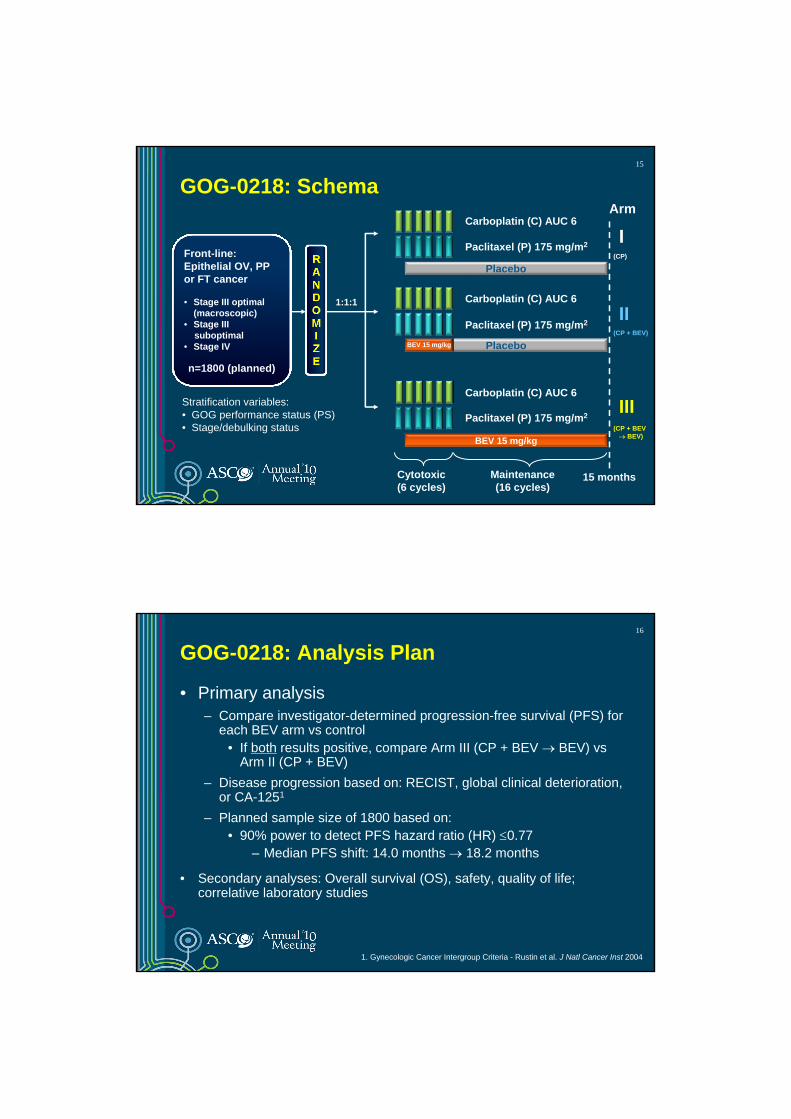
GOG-0218: Schema
Front-line: Epithelial OV, PP or FT cancer
• Stage III optimal (macroscopic)
• Stage III suboptimal
• Stage IV
n=1800 (planned)
Stratification variables:• GOG performance status (PS)• Stage/debulking status
1:1:1
15 months
Paclitaxel (P) 175 mg/m2
Carboplatin (C) AUC 6
Placebo
IArm
Cytotoxic(6 cycles)
Maintenance(16 cycles)
(CP)
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2
PlaceboBEV 15 mg/kg
II(CP + BEV)
BEV 15 mg/kg
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2III
(CP + BEV→ BEV)
16
GOG-0218: Analysis Plan
• Primary analysis– Compare investigator-determined progression-free survival (PFS) for
each BEV arm vs control• If both results positive, compare Arm III (CP + BEV → BEV) vs
Arm II (CP + BEV)– Disease progression based on: RECIST, global clinical deterioration,
or CA-1251
– Planned sample size of 1800 based on:• 90% power to detect PFS hazard ratio (HR) ≤0.77
– Median PFS shift: 14.0 months → 18.2 months
• Secondary analyses: Overall survival (OS), safety, quality of life; correlative laboratory studies
1. Gynecologic Cancer Intergroup Criteria - Rustin et al. J Natl Cancer Inst 2004

17
Adverse event (grade when limited), n (%)
Arm ICP
(n=601)
Arm IICP + BEV(n=607)
Arm IIICP + BEV → BEV
(n=608)GI eventsa (grade ≥2) 7 (1.2) 17 (2.8) 16 (2.6)
Hypertension (grade ≥2) 43 (7.2)b 100 (16.5)b 139 (22.9)b
Proteinuria (grade ≥3) 4 (0.7) 4 (0.7) 10 (1.6)
Pain (grade ≥2) 250 (41.7) 252 (41.5) 286 (47.1)
Neutropenia (grade ≥4) 347 (57.7) 384 (63.3) 385 (63.3)
Febrile neutropenia 21 (3.5) 30 (4.9) 26 (4.3)
Venous thromboembolic event 35 (5.8) 32 (5.3) 41 (6.7)
Arterial thromboembolic event 5 (0.8) 4 (0.7) 4 (0.7)
CNS bleeding 0 0 2 (0.3)
Non-CNS bleeding (grade ≥3) 5 (0.8) 8 (1.3) 13 (2.1)
RPLS 0 1 (0.2) 1 (0.2)
GOG-0218: Select Adverse EventsOnset between cycle 2 and 30 days after date of last treatment
RPLS = reversible posterior leukoencephalopathy syndromeaPerforation/fistula/necrosis/leak
bp<0.05
CP (Arm I)
Arm I CP
(n=625)
Patients with event, n (%) 423 (67.7)
Median PFS, months 10.3Stratified analysis HR (95% CI)One-sided p-value (log rank)
GOG-0218: Investigator-Assessed PFS
+ BEV (Arm II)
ap-value boundary = 0.0116
+ BEV → BEV maintenance (Arm III)Prop
ortio
n su
rviv
ing
prog
ress
ion
free
Months since randomization
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 12 24 36
Arm IIICP + BEV → BEV
(n=623)
360 (57.8)14.10.717
(0.625–0.824)<0.0001a
18
Arm IICP + BEV(n=625)
418 (66.9)11.20.908
(0.759–1.040)0.080a

19
GOG-0218: Subgroup Analyses of PFSCP + BEV → BEV (Arm III) vs CP (Arm I)
Hazard ratio
Experimental arm (CP + BEV → BEV;
Arm III) betterControl arm
(CP; Arm I) better
Stage 3 optimal (n=434) 0.618
Stage 3 suboptimal (n=496) 0.763
Stage 4 (n=318) 0.698
PS 0 (n=616) 0.710
PS 1/2 (n=632) 0.690
Age <60 years (n=629) 0.680
Age 60–69 years (n=409) 0.763
Age ≥70 years (n=210) 0.678
Treatment hazard ratio
0.33 0.5 0.67 1.0 1.5 2.0 3.0
20GOG-0218: Ramification of Using CA-125 as Determinant of Progression
0.6450.717Hazard ratio
0.00010.0001p-value
Protocol-definedPFS analysis
CA-125-censoredPFS analysis
Regulatory analysis
Median PFS, months
CP (Arm I) 10.3 12.0
CP + BEV → BEV (Arm III) 14.1 18.0
Absolute difference in median PFS (months) 3.8 6.0
Censored for CA-125, %
CP (Arm I) 0 20
CP + BEV → BEV (Arm III) 0 29

21
GOG-0218: Overall Survival (OS)
• Events observed in 24% of patients at time of data lock• After primary endpoint changed from OS to PFS
– Unblinding to treatment assignment allowed at time of disease progression
OutcomeArm I
CP(n=625)
Arm IICP + BEV(n=625)
Arm IIICP + BEV → BEV
(n=623)
Deaths, n (%) 156 (25.0)
150 (24.0)
138 (22.2)
1-year survival, % 90.6 90.4 91.3
22
GOG-0218: Conclusions
• GOG-0218 met the primary objective in the front-line treatment of advanced ovarian (epithelial OV, PP and FT) cancer; PFS withCP + BEV → BEV maintenance (Arm III) statistically superior to CP alone (Arm I)– PFS with CP + BEV (Arm II) not statistically superior to CP (Arm I)
• Interpretation of survival analysis limited
• Treatment regimen generally well tolerated; adverse events (including GI perforation) similar to previous BEV studies
• BEV – first molecular targeted and first anti-angiogenic agent to demonstrate benefit in this population
• CP + BEV → BEV maintenance should be considered one standard option

23
Avastin for advanced ovarian cancer should be considered one standard option*
• This is the first Phase III study of an anti-angiogenic medicine in advanced ovarian cancer to meet its primary endpoint.
• Another phase III trial of Avastin in front line ovarian cancer (ICON-7) will report in 2010.
• We plan to discuss these data with the FDA and other health authorities.
• Additionally, a second line platinum-sensitive Avastin phase III trial will report in 2011.
*Robert A. Burger et al, ASCO 2010
24
Building on our understanding of Avastin’s potential
Stefan Frings, M.D.Avastin Franchise Director

25
What’s important for Avastin at ASCO 2010?
• Avastin – a potential new standard of care in ovarian cancer
• Insights into optimal treatment duration
– Longer duration of Avastin therapy demonstrated to be more effective than shorter in ovarian cancer
– In mCRC, treatment beyond progression may yield superior OS
• Strong data solidifying Avastin’s essential role in our core indications
– ARIES in mCRC
– Meta-analysis in mBC
– ARIES in mNSCLC
• New phase III data on Avastin in gastric and prostate cancers
25
26
Results from ARIES observational cohort studyResults from ARIES observational cohort study
Pts alive 2 months after
1st PD (n=1026)
Pts alive 2 months after
1st PD (n=1026)
BBP (n=408)(BV and CT) < 2mo after PD
BBP (n=408)(BV and CT) < 2mo after PD
No BBP (n=336)(CT < 2mo after PD) and
(no BV after PD)
No BBP (n=336)(CT < 2mo after PD) and
(no BV after PD)
Other* (n=282)No treatment ever, BV and/or CT ≥ 2mo
after PD (not included in analysis)
Other* (n=282)No treatment ever, BV and/or CT ≥ 2mo
after PD (not included in analysis)
11
22
33
MDs choice of therapy
MDs choice of therapy
Objective: To evaluate the association between early exposure to Bevacizumab (Avastin) beyond 1st PD (BBP) and survival beyond 1st PD

27
Avastin treatment beyond progression may yield superior overall survival
t0= PD+2mos
Surv
ival
Bey
ond
Prog
ress
ion
No BBPBBP 7.5 14.1
Months
ARIESARIES
Cohn, et al. ASCO 2010, Abstract #3596 Grothey, A. et al. JCO, 2008
BRiTEBRiTE
9.2 16.8
Months
% S
urvi
val B
eyon
d Pr
ogre
ssio
n
2828
ARIES confirms BRiTE data
ARIES study
Median OS from initiation of 1st line therapy
Avastin-based treatment: 27.5 months
Non-Avastin regimen: 18.7 months
BRiTE registry
Median OS from initiation of 1st line therapy
Avastin-based treatment: 31.8 months
Non-Avastin regimen: 19.9 months
Multivariate Analysis of Pre- and Post-Treatment Variables on SBP
HR = 0.51 for BBP
(95% CI, 0.42 to 0.63)
Multivariate Analysis of Pre- and Post-Treatment Variables on SBP
HR = 0.52for BBP
(95% CI, 0.42 to 0.63)

2929
Avastin Treatment through Multiple Lines (TML)Phase III in Metastatic Colorectal Cancer – ML18147
Standardfirst-line
chemotherapy + Avastin Standard
second-line chemotherapy
+ Avastin
Standardsecond-line
chemotherapy
First-line Second-line
Progression
Primary endpoint = OSFPI Q1 2006 - enrolment completed June 2010
RANDOMISATION
(n=810)
3030
Summary of data on Treatment through Multiple Lines (TML)
• ARIES data strengthens the hypothesis generated by BRiTE that longer treatment duration with Avastin, i.e. treatment through multiple lines, may provide meaningful benefits for patients.
• We look forward to results from the prospective Phase III Avastin study in mCRC(ML18147) to further understand how duration of therapy impacts outcome for patients.
31
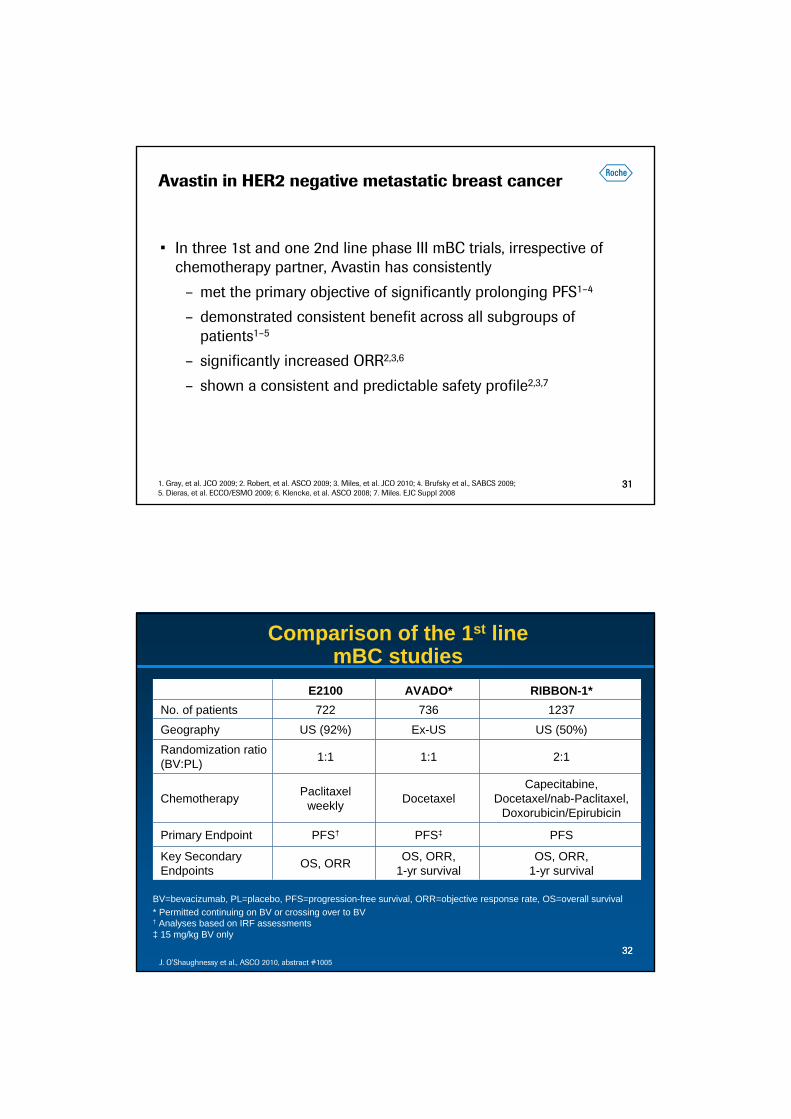
Avastin in HER2 negative metastatic breast cancer
• In three 1st and one 2nd line phase III mBC trials, irrespective of chemotherapy partner, Avastin has consistently
– met the primary objective of significantly prolonging PFS1–4
– demonstrated consistent benefit across all subgroups of patients1–5
– significantly increased ORR2,3,6
– shown a consistent and predictable safety profile2,3,7
311. Gray, et al. JCO 2009; 2. Robert, et al. ASCO 2009; 3. Miles, et al. JCO 2010; 4. Brufsky et al., SABCS 2009; 5. Dieras, et al. ECCO/ESMO 2009; 6. Klencke, et al. ASCO 2008; 7. Miles. EJC Suppl 2008
3232
BV=bevacizumab, PL=placebo, PFS=progression-free survival, ORR=objective response rate, OS=overall survival* Permitted continuing on BV or crossing over to BV† Analyses based on IRF assessments ‡ 15 mg/kg BV only
Comparison of the 1st line mBC studies
E2100 AVADO* RIBBON-1*No. of patients 722 736 1237Geography US (92%) Ex-US US (50%)
Randomization ratio (BV:PL) 1:1 1:1 2:1
Chemotherapy Paclitaxelweekly Docetaxel
Capecitabine,Docetaxel/nab-Paclitaxel,
Doxorubicin/Epirubicin
Primary Endpoint PFS† PFS‡ PFS
Key Secondary Endpoints OS, ORR OS, ORR,
1-yr survivalOS, ORR,
1-yr survival
J. O’Shaughnessy et al., ASCO 2010, abstract #1005

3333
Chemotherapy use in First-line HER2-negative Metastatic Breast Cancer
US Top 4 EU
*Single agent or combination treatment
14%17%
20%
15%
11%
23%
Paclitaxel Paclitaxel protein-boundDocetaxel Taxane DoubletsXeloda Other/Anthracycline
27%
16% 16%
8%
33%
Paclitaxel* Docetaxel*Anthracycline XelodaOther
3434
Overview of Efficacy Results from the Individual Studies in the Pooled Analysis
E2100 AVADO* RIBBON-1 (Cape)RIBBON-1
(Tax/Anthra)Non-BV BV Non-
BV BV Non-BV BV Non-BV BV
Median PFS, mo 5.8 11.3 8.0 8.8 5.7 8.6 8.0 9.2
StratifiedHR (95% CI)
0.48(0.39–0.61)
0.61(0.48–0.68)
0.69(0.56–0.84)
0.64(0.52–0.80)
p-values p<0.0001 p=0.0003 p=0.0002 p<0.0001
BV=bevacizumab, Cape=capecitabine, Tax/Anthra=taxane/anthracycline* 15 mg/kg cohort
• The safety profile of BV was consistent across Phase III MBC trials.
J. O’Shaughnessy et al., ASCO 2010, abstract #1005

35
Results of Meta-analysis of Phase III Studies: Progression-Free and Overall Survival
J. O’Shaughnessy et al., ASCO 2010, abstract #1005
Non-BV(n=1008)
BV(n=1439)
Median, mo 26.4 26.7
HR (95% CI) 0.97 (0.86–1.08)
1-yr survival rate (%) 77 82
Non-BV(n=1008)
BV(n=1439)
Median, mo 6.7 9.2
HR (95% CI) 0.64 (0.57–0.71)
Progression-free survival Overall survival
36
Considerations on PFS and OS in mBC trials
• Advanced breast cancer is an incurable disease; lengthening the time women live without the cancer worsening is clinically meaningful by sparing patients…
– for as long as possible from symptoms of progressive breast cancer
– toxic effects of subsequent therapies
– the psychological burden and uncertainty that comes with progression
• Avastin has demonstrated clinically meaningful PFS benefit but no significant OS improvement across 3 first-line HER2-neg mBC studies & in pooled analysis Of note,
– The objective of the trials was to demonstrate superior PFS
– OS outcome may have been confounded by• Uncontrolled use of further lines of anti-cancer therapies• Cross-over with Avastin to control-arm patients
– There is a greater chance of affecting OS in populations with shorter PPS
36Broglio and Berry. 2009. J Natl Cancer Inst. 101:1642-49; Saad, Katz, and Buyse. 2010. J Clin Oncol. 28:1958-62; Burzykowski, et al. J Clin Oncol. 26:1987-92; Miller. 2008. NEJM. 358: 1637-1638

37
Avastin phase III trials in gastric and prostate cancer
37
AVAGAST: A Randomized Double-Blind Placebo- Controlled Phase III Study
Starting dose of bev/placebo: 30 minutes, subsequent doses: 15 minutes
Capecitabine*/Cisplatin (XP)
+ Placebo q3w
Capecitabine*/Cisplatin (XP)
+ Bevacizumab q3w
Locally advancedor metastatic gastric cancer
R
Primary endpoint: OS
Secondary: PFS, TTP, ORR, duration of response, safety, QoL, biomarkers

39
AVAGAST: Efficacy results
Kang et al., ASCO 2010, LBA4007
XPn=387
XP + Avastin(n=387)
Median OS, mo 10.1 12.1
HR 0.87
P-value 0.1002
XPn=387
XP + Avastin(n=387)
Response rate (%) 29.5 38.0
P-value 0.0121
Median PFS, mo 5.3 6.7
HR 0.80
p-value 0.0037
40
AVAGAST: Regional Differences in Efficacy
Overall survival
Hazard ratio
Asia Europe Pan-America
20
18
16
14
12
10
8
6
4
2
0
1.0
0.8
0.6
0.4
0.2
0.0
XP + Placebo XP + Avastin
0.97
0.85
0.63

41
AVAGAST: Safety Events
Number of patients (%)XP + Placebo
N=381XP + Bev
N=386
Hypertension 0.5 6.2
Hemorrhage 3.9 3.9
Wound-healing complications 0.0 0.5
GI-perforations 0.3 2.3
ATE 2.1 1.3
VTE 9.4 6.4
60-day mortality rate 5.8 3.1Kang et al., ASCO 2010, LBA4007
42
AVAGAST Summary & Conclusions
• Primary endpoint of OS not met
• Secondary efficacy endpoints (PFS, best ORR) significantly improved, indicating clinical activity of Avastin + chemo in AGC
• Heterogeneous efficacy results in both treatment arms across geographic regions
Hypothesis generating with regard to tumor burden, patient status, practice patterns, genetics?
• No unexpected / new safety signals for Avastin
• Further analysis ongoing, including preplanned biomarker analysis

43
Hormone-resistant prostate cancer study CALGB 90410: Treatment Schema
RA
ND
OM
IZE
(1:1
)R
AN
DO
MIZ
E (1
:1)
Arm 2Dexamethasone 8 mg po x 3 doses Docetaxel 75 mg/m2 on day 1 q 21 daysPrednisone 10 mg po dailyPlacebo1 IV on day 1 q 21 days
Arm 1Dexamethasone 8 mg po x 3 dosesDocetaxel 75 mg/m2 on day 1 q 21 daysPrednisone 10 mg po dailyBevacizumab1 15 mg/kg IV on day 1 q 21 days
•ASA 325 mg encouraged in all patients that can tolerate 1In the event of intolerable toxicity to Docetaxel the Bevacizumab\placebo may be continued alone until POD
Primary endpoint: Overall Survival (OS)
Secondary endpoint:
50% decline in PSA1
Progression Free Survival (PFS)1
Toxicity
44
0 6 12 18 24 30 36 42Time(months)
0.0
0.2
0.4
0.6
0.8
1.0
Ove
rall
Surv
ival
(pro
babi
lity)
Placebo+DoceBev+Doce, log-rank p=0.181
Kaplan-Meier Overall Survival Curves by Treatment Arm
526 480 390 305 199 100 44 22524 484 417 327 217 117 52 23
Placebo+DoceBev+Doce
Number of Patients at Risk
Median DP = 21.5 (20.0-23.0)Median DPB=22.6 (21.1-24.5) HR= 0.91 (0.78-1.05)

45
0 6 12 18 24 30 36 42Time(months)
0.0
0.2
0.4
0.6
0.8
1.0
PFS
(pro
babi
lity)
Placebo+DoceBev+Doce, log-rank p<0.0001
Kaplan-Meier PFS Curves by Treatment Arm
526 303 134 75 34 8 4 0524 381 194 97 44 15 5 1
Placebo+DoceBev+Doce
Number of Patients at Risk
Median DP = 7.5 (6.7-8.0)Median DPB=9.9 (9.1-10.6) HR= 0.77 (0.68-0.88)
46
Secondary Endpoints: Objective Response and 50% Decline in PSA
Clinical Endpoint
Arm 1DP+B
(N=524)
Arm 2 DP
(N=526)
p-value
≥50% decline in PSA(95% CI)
69.5% (65.2-73.5)
57.9% (53.3-62.3)
0.0002
Objective Response(95% CI) (# with measurable disease)
53.2%(46.8-59.6)
(248)
42.1% (36.2-48.2)
(273)
0.0113

47
Conclusions• The addition of bevacizumab to DP showed a non-significant
trend in OS in men with mCRPC– 21.5 mo. vs 22.6 mo., p=0.181 (HR = 0.91)
• The addition of bevacizumab to DP compared to DP in metastatic CRPC resulted in a significantly greater
– PFS 9.9 mo. vs. 7.5 mo., p < 0.0001 – objective response rate 53.2% vs. 42.1% , p= 0.0113– PSA decline in PSA 69.5% vs. 57.9%, p= 0.0002
48
Conclusions
• Differences in primary and secondary endpoints may be related to:
– Underpowered Study: OS in the control arm of 21.5 months exceeds the 19.2 month OS reported in the TAX327 trial (Berthold et al. JCO 2008;26:242-45)
• Stage migration• Reflection of good risk population (47%)
– Impact of subsequent therapy on OS
– Discordance between OS and PFS\overall response
• Exploratory analyses which subgroups obtain potential clinical benefit are ongoing

49
Gastric and prostate cancer conclusions
• Based on current data sets there will be no regulatory filings for gastric and prostate cancer.
• We will determine next steps particularly for gastric cancer.
5050
Avastin takeaways ASCO 2010 Continuing advance our understanding of Avastin’s potential
• Avastin – a potential new standard of care in ovarian cancer
• Patients benefit from longer Avastin treatment
• Strong data solidifying Avastin’s essential role in our core indications
• Avastin has activity in gastric and prostate cancer

51
Prof. Gilles Salles, M.D., Ph.D.Principal Investigator of PRIMA studyHospices Civils de Lyon, France
Rituximab: PRIMA study
Rituximab Maintenance for 2-Years in Patients with Untreated High Tumor Burden Follicular Lymphoma After Response to Immunochemotherapy
G. A. Salles, J. F. Seymour, P. Feugier, F. Offner, A. Lopez-Guillermo, R. Bouabdallah, L. M. Pedersen, P. Brice, D. Belada, L. Xerrion behalf of PRIMA investigators
52
Rationale for the PRIMA study• Follicular lymphoma: the second most common lymphoma subtype
• Usually remains incurable despite efficient therapy (rituximab + chemotherapy) providing disease control for variable time periods
• Median life expectancy is 12–15 years; patients may suffer from several recurrences of their lymphoma
• Length of remission decreases at each treatment recurrence
• Rituximab is an anti-CD20 monoclonal antibody that has been shown to improve outcome for follicular lymphoma patients when used in combination with chemotherapy
• Previous studies suggested that rituximab maintenance may benefit patients with relapsed or previously untreated follicular lymphoma

53
PRIMA: primary objective and design
• To assess whether 2-year maintenance treatment with rituximabafter induction immunochemotherapy is able to improve the progression-free survival (PFS) of untreated follicular lymphoma patients in need of first-line therapy
A study coordinated by the
No responseoff study
Maintenance12 x rituximab(q2mo for 24 mo)
Observation
Untreated follicular NHL
High tumor burden
Induction8 x rituximab
Chemotherapy(6 x CHOP or 8 x CVP or
6 x FCM)
RESPONSE1217 patients
1018 patients
54
• Rituximab maintenance significantly reduced the risk of lymphoma progression by 50% (HR=0.50, 95% CI 0.39; 0.64)
HR=0.50p<0.0001
Time (months)
Rituximab maintenanceN=505
ObservationN=513
60 12 18 24 30 36
Prog
ress
ion-
free
rate 0.8
0.6
0.4
0.2
0
1.082%
66%
Patients at risk505513
472 443 336 230 103 18469 411 289 195 82 15
Primary endpoint (PFS) met at the planned interim analysis
55
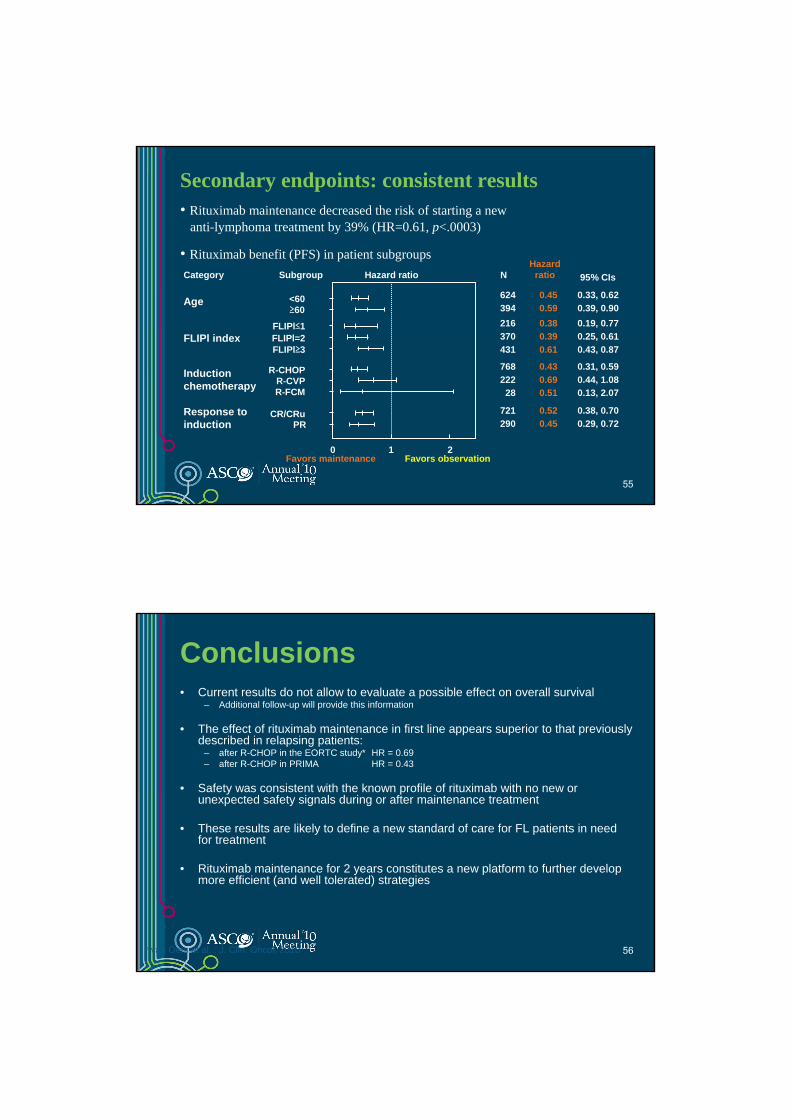
Secondary endpoints: consistent results
624394216370431
76822228
721290
0.450.590.380.390.61
0.430.690.51
0.520.45
0.33, 0.620.39, 0.900.19, 0.770.25, 0.610.43, 0.87
0.31, 0.590.44, 1.080.13, 2.07
0.38, 0.700.29, 0.72
Subgroup
<60≥60
FLIPl=2FLIPl≤1
FLIPl≥3
R-CHOPR-CVPR-FCM
CR/CRuPR
0 1 2
Hazard ratio
Response to induction
Induction chemotherapy
FLIPl index
Age
Category 95% CIsHazard
ratioN
• Rituximab maintenance decreased the risk of starting a newanti-lymphoma treatment by 39% (HR=0.61, p<.0003)
Favors maintenance Favors observation
• Rituximab benefit (PFS) in patient subgroups
56
Conclusions • Current results do not allow to evaluate a possible effect on overall survival
– Additional follow-up will provide this information
• The effect of rituximab maintenance in first line appears superior to that previously described in relapsing patients:
– after R-CHOP in the EORTC study* HR = 0.69– after R-CHOP in PRIMA HR = 0.43
• Safety was consistent with the known profile of rituximab with no new or unexpected safety signals during or after maintenance treatment
• These results are likely to define a new standard of care for FL patients in need for treatment
• Rituximab maintenance for 2 years constitutes a new platform to further develop more efficient (and well tolerated) strategies
* van Oers et al. ; J. Clin. Oncol, 2010

57
Setting the standard of care in oncologySummary and Q&A
K. Mahler, Head of Investor Relations, Roche
58
107
77
5845 51 50 47
29
113 5 1
25
9
10
1511 8 10
9
9
26 4 6 4
22
2 21
3
1
11
1 2
1
0
20
40
60
80
100
120
140
160 PlenaryClinical Science SymposiumOralPoster DiscussionPoster
n=66n=67n=71
n=86
n=143
n=65 n=63
n=41
n=13n=5 n=5 n=3 n=2
n=1
No.
of A
bstr
acts
ASCO 2010: News flow and clinical benefit driving standard of care
Avastin
Herceptin
Nexavar
Tarceva
XelodaErbitu
xSutent
Rituxan
Panitumumab
T-DM1
Recentin
AZD2281BSI-2
01
Pertuzumab

5959
Major clinical data newsflow for our late-stage oncology NMEs in 2010-2011
Hedgehog Pathway InhibitorPh II advanced Basal Cell Carcinoma
Hedgehog Pathway InhibitorPh II met. Ovarian cancer
RG7204 (BRAF inh.)Ph II 2nd/3rd line met. Melanoma
RG7204 (BRAF inh.)Ph III 1st line met. Melanoma
Pertuzumab+HerceptinPh II Neoadjuvant BC
NEOSPHERE
T-DM1 vs:Herceptin+docetaxel
Ph II 1st line met. BC
Pertuzumab+HerceptinPh III 1st line met. BC
CLEOPATRA
= pivotal data
2010 2011
Hedgehog Pathway InhibitorPh II 1st line met. Colorectal cancer
= proof of concept data
RG7159/GA101Ph II H2H vs. Rituxan, iNHL
60
Back-up slides
61
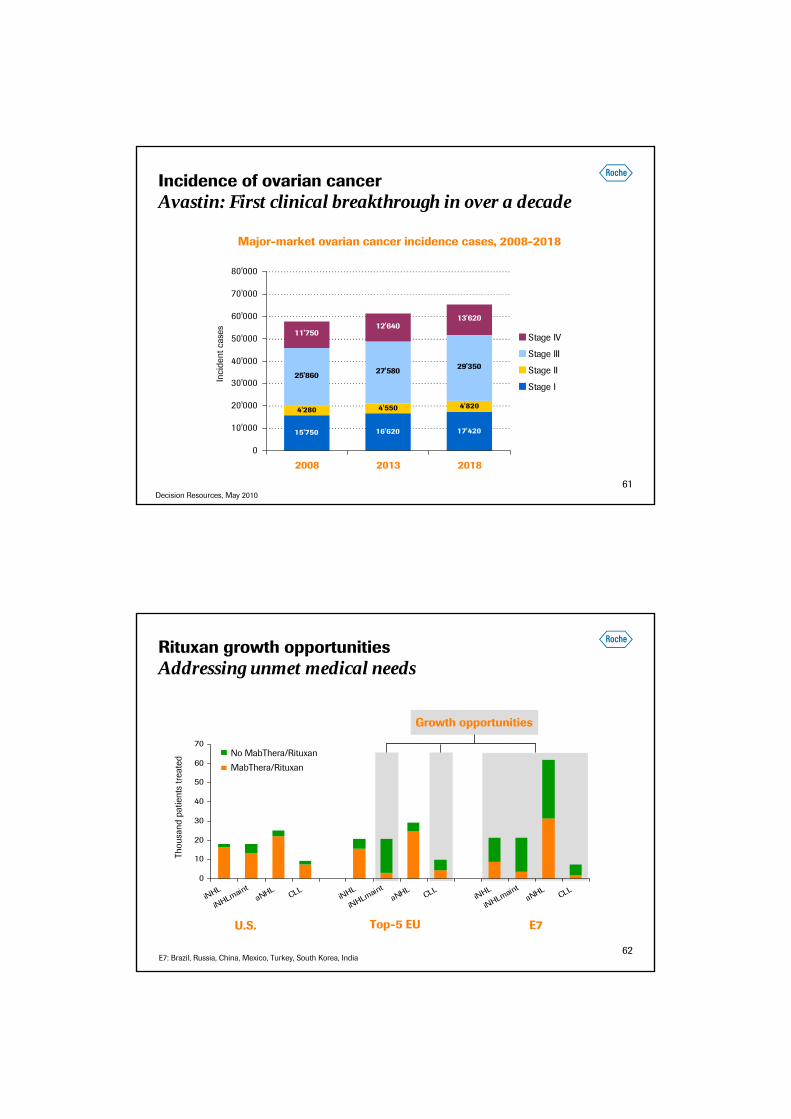
Incidence of ovarian cancerAvastin: First clinical breakthrough in over a decade
Major-market ovarian cancer incidence cases, 2008-2018
Inci
dent
cas
es
15'750 16'620 17'420
4'280 4'550 4'820
25'860 27'580 29'350
11'75012'640
13'620
0
10'000
20'000
30'000
40'000
50'000
60'000
70'000
80'000
2008 2013 2018
Stage IV
Stage III
Stage II
Stage I
Decision Resources, May 2010
62
Rituxan growth opportunitiesAddressing unmet medical needs
0
10
20
30
40
50
60
70
iNHL
iNHLmaint
aNHLCLL
iNHL
iNHLmaint
aNHLCLL
iNHL
iNHLmaint
aNHLCLL
U.S. Top-5 EU E7
Growth opportunities
Thou
sand
pat
ient
s tr
eate
d No MabThera/Rituxan
MabThera/Rituxan
E7: Brazil, Russia, China, Mexico, Turkey, South Korea, India

63
We Innovate Healthcare