road to qbl - california maternal quality care collaborative
TRANSCRIPT

Road to QBL
How to Avoid the Bumps & Potholes
Cynthia Sawyer, MSN, CNS, RNC-OB, CLE

DISCLOSURES
• No disclosures
2

OBJECTIVES
• At the conclusion of this presentation the participant will be able to: – Describe the difference between estimated blood
loss and quantitative blood loss (QBL) – Verbalize the need for QBL for all vaginal and
cesarean deliveries – Identify the tools necessary for the staff to assist
them performing QBL – Evaluate the process of QBL for vaginal and
cesarean deliveries – Discuss ways to overcome obstacles and barriers
to rolling out QBL and sustaining the change
3

BACKGROUND • Estimated blood loss (EBL) has been done for
post deliveries since the 1800’s
• Purpose of EBL was to determine the need for a blood transfusion
– Physicians trained to visually estimate the blood loss
• In the 1960’s researchers demonstrated that visual EBL was underestimated in large blood loss and overestimated in small blood loss
– Underestimations were by one third to one half
(AWHONN, 2014; Williams, 2014; Schorn, 2010) 4

EBL
Care provider visually estimates blood loss on laps based on saturation
Visually determines blood concentration of fluid in suction canister to determine amount
Visually estimates run off blood loss on chux under patient
Estimates total blood loss
5

QBL
Weighed • For each 1 g equals 1 mL of water
Measured • Each mL approximately
equates mL blood loss
Quantified • Totals are
added cumulatively
6

COMPARISON
EBL
Quick & easy
Subjective
Visual estimation
High rate of error
Not 100% accurate
QBL
Can be laborious
Objective
Quantifiably measured
Lower rate of error
Not 100% accurate
(AWHONN, 2014) 7

• Uterine atony cause in 50% of cases
• Change in practice with over use of inductions & cesarean sections
OB hemorrhage rate increased 26% from 1994-2006 in U.S.
• Quick recognition & treatment can prevent progression of blood loss
• OB hemorrhage is low volume, but high risk event
Physiological changes in pregnancy lends women capable of
losing large amounts of blood
• Denial & delay
• Under estimation of blood loss
• Lack skill in accurately assessing QBL
Problems with recognition,
treatment, & poor communication
contribute to maternal death
WHY QBL FOR ALL DELIVERIES? OB hemorrhage a leading cause of maternal mortality & morbidity, yet highly preventable
8 (Bingham, 2012; California Department of Public Health, 2015)

THE JOURNEY BEGINS
• Looking back on the road less traveled
– Two maternal deaths from a specific patient population
– High incidence of severe
obstetric hemorrhage
– Physician and office
signage instructed no tea
or vitamins after 36 weeks
9

LESSONS LEARNED • Set up multidisciplinary & interdepartmental
simulations – Return demonstration of
• Blood transfusion equipment
• OB hemorrhage cart & weighing
• Uterine balloon
• CMQCC OB hemorrhage protocol
• ACLS
• Code OB
• OB Hemorrhage Order Set • Massive blood transfusion
10

Low Risk Medium Risk
High Risk
No history of postpartum hemorrhage
Elective primary Cesarean section, uncomplicated
≤ 4 previous vaginal births
No previous uterine incision
No known bleeding disorder
Normal vaginal delivery
Singleton pregnancy
Prior Cesarean birth or uterine surgery
Uterine
overdistention: ▪ Multiple gestation ▪ Polyhydramnios History of previous
postpartum hemorrhage
Chorioamnionitis
Large uterine fibroids
Placenta previa, no bleeding
Oxytocin use > 18 hours
Platelets ≤ 100,000
> 4 vaginal births
≥ 3 previous Cesarean sections
Active bleeding (greater than show on admission)
Suspected placenta accrete or percreta
Platelets < 75,000 Hct ≤ 30 AND other
risk factors Placenta previa,
bleeding Known
coagulopathy
Recommended Action
Hold Clot Type & Screen Type & Cross 2 Units
OB Hemorrhage Risk Assessment
11

OB HEMORRHAGE CART
12

OB HEMORRHAGE CHECK LIST
13

THE BACK SIDE
14

NEW CODE OB SHEET
15

PRACTICE MAKES PERFECT • Super User Program
– Resource person
every weekend &
every shift
– Rapid infuser
– Blood warmer
– Uterine balloon
– OB hemorrhage cart
16

BEST LAID PLANS
• Demonstrate weighing laps at skills lab
– Too many new projects
– Not enough time for
demonstrations
• Should have piloted
a team of champions
— Stronger infrastructure
for roll out to support change
17

MAPPING IT OUT
• Obtain buy in from key stake holders
– Anesthesiologists
– Obstetricians
– Administration
– Influential staff
– OB techs
18
TOOK A WRONG TURN
• Should have’s:
– Practiced more with the OB techs
– Participated on more cases
– Really developed a core team
– Reached out to more
hospitals on workflow
19

FORK IN THE ROAD
• What to do next?
20

OVERCOMING OBSTACLES
• Alleviating frustrated staff
– Labor intensive at time of delivery
• Instituted buddy program
• Marking pen attached to suction canister
– Developed QBL scratch sheet
– Calculator attached to scale
– Preweights on scale
– Practicing doing mock QBL
21

RECYCLE YOUR OLD STUFF
22

TAKING THE SHOW ON THE ROAD
• Remediation
• Winning them over
• Justification
– Best practice
– Examples of how
EBL didn’t work
– Know how to do
it in an emergency
23

ALONG FOR THE RIDE • Make them sign it!
– Ward conference
– Log book
24

QBL FOR VAGINAL DELIVERY
After delivery of infant the OB notes amount of amniotic fluid
At the end of the delivery procedure OB notes level of graduated bag and subtracts amniotic fluid for QBL
If blue towels, gauze, or pads are soaked with blood, they will be weighed, dry weights subtracted, and added to total
25

GOT AMNIOTIC FLUID?
• RN prompts OB to look at amniotic fluid level
26

GOT IT IN THE BAG
27
After Delivery of Infant After Delivery of Placenta

QBL FOR CESAREAN Blood loss from suction canister
Mark amount after tech has suction
gutters after delivery of baby
Note total amount of fluid before
irrigation
Subtract amniotic fluid from total
Blood loss from laps
Before closing add up preweights –
wet & dry
Weigh entire holder of laps
Subtract preweights from lap holder weight
28

WHAT IS WHAT?
29

IT WEIGHS HOW MUCH?
30

WEIGH THAT LAP
31

MATH IS NOT EASY FOR MOST
32
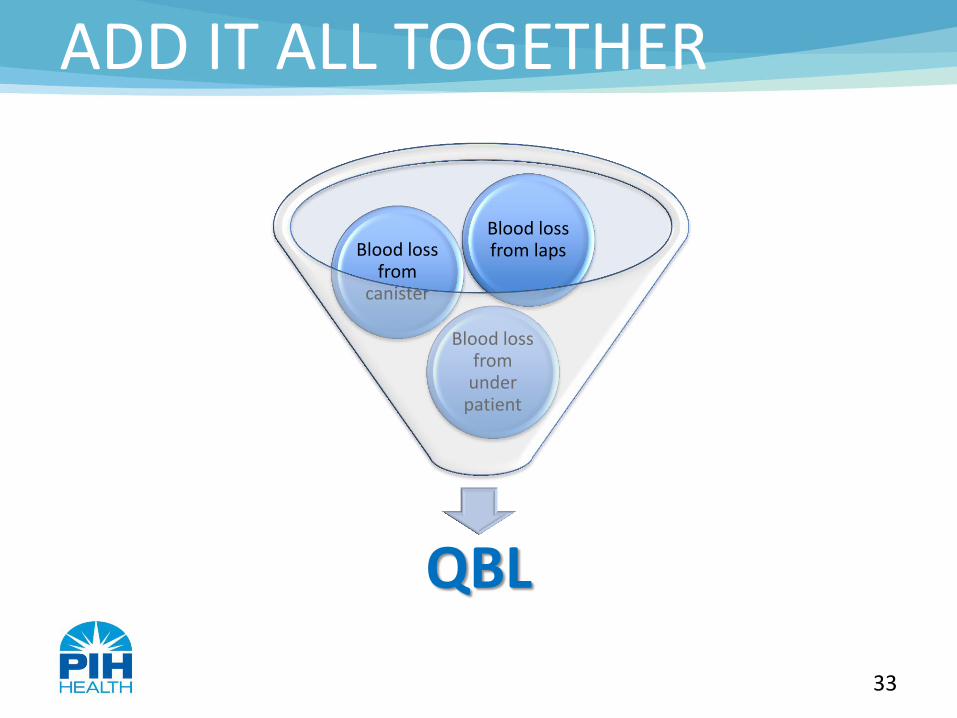
ADD IT ALL TOGETHER
QBL
Blood loss from
under patient
Blood loss from
canister
Blood loss from laps
33

ONE STEP AT A TIME
• Debriefing with tool
• Social work consults added
to order sets
34

MAKE LEARNING FUN
35

BRIBERY NEVER HURTS
36

JOURNEY STILL AHEAD
37

COMING SOON
38

SMOOTH OUT THE ROAD
• Working with IT to develop
– E-calculator
– OB hemorrhage pick list
39

DO NOT REINVENT THE WHEEL
40

ONE SIZE FITS MOST
41

KEEP IT SIMPLE
42

SUSTAINABILITY • PACU log audits
• Simulations
43

AWHONN VIDEO
• Quantification of Blood Loss
44 (AWHONN, 2014)

Questions?
Thank you

REFERENCES
Association of Women’s Health, Obstetric and Neonatal Nurses. (2014). Quantification of blood loss: AWHONN practice brief
number 1. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 00, 1–3. DOI: 10.1111/1552-6909.12519. Retrieved from:
http://www.pphproject.org/downloads/awhonn_qbl.pdf
Association of Women’s Health, Obstetric and Neonatal Nurses. (2014). How to quantify blood loss. Retrieved from:
https://www.youtube.com/watch?v=F_ac-aCbEn0
Bingham, D. (2012). Obstetric hemorrhage-related maternal mortality and morbidity. Journal of Women’s Health, 21(9), 901-902.
doi: 10.1089/jwh.2012.3873.
California Department of Public Health. (2015). OB hemorrhage toolkit. California Maternal Quality Care Collaborative. Retrieved
from: https://www.cmqcc.org/resource/obstetric-hemorrhage-20-toolkit
Schorn, M. N. (2010). Measurement of blood loss: Review of the literature. Journal of Midwifery & Women’s Health, 55(1), 20-27.
Retrieved from: http://www.medscape.com/viewarticle/716622_4
Williams Obstetrics, 24th (ed.) (2014). Cunningham, F. G., Leveno, K. J., Bloom, S. L., Spong, C. Y., Dashe, J. S., Hoffman, B. L., Casey,
B. M., and Sheffield, J. S . (Eds.). New York, NY: Mc Graw Hill Education
45