rmh cardiac anaesthesia cardiac... · welcome to cardiac anaesthesia cardiac surgery presents the...
TRANSCRIPT
1
RMH Cardiac Anaesthesia
An Introduction to Cardiac Anaesthesia at RMH Feb 2009
Reny Segal
Gerard Stainsby Garry Donnan
Dept. of Anaesthesia & Pain Management Royal Melbourne Hospital

2
RMH Cardiac Anaesthesia
Contents
WELCOME TO CARDIAC ANAESTHESIA ............................................................................................................... 3 GENERAL PLAN OF THE OPERATION.................................................................................................................... 3 PREOPERATIVE ASSESSMENT .............................................................................................................................. 4 THEATRE PREPARATION...................................................................................................................................... 7 ANAESTHETIC ROOM........................................................................................................................................... 7 THE SWAN-GANZ DEBATE .................................................................................................................................. 8 PRE-INDUCTION................................................................................................................................................... 9 INDUCTION ........................................................................................................................................................ 10 MAINTENANCE .................................................................................................................................................. 11 TRANSOESOPHAGEAL ECHO.............................................................................................................................. 11 PRE-BYPASS ...................................................................................................................................................... 12 RUNNING ON BYPASS ........................................................................................................................................ 13 PACING.............................................................................................................................................................. 14 COMING OFF BYPASS ........................................................................................................................................ 16 POST-BYPASS .................................................................................................................................................... 18 ICU ................................................................................................................................................................... 19 MODIFIED BYPASS: OPCAB AND PADCAB .................................................................................................... 22 BLEEDING.......................................................................................................................................................... 19 REDO CARDIAC SURGERY ................................................................................................................................. 23 REMOVAL OF PERMANENT PACING LEAD SYSTEMS ......................................................................................... 24 INTERVENTIONAL CARDIOLOGY ....................................................................................................................... 26 APPENDIX A: INDUCTION IN SELECTED PATHOPHYSIOLOGICAL STATES.................................................... 27 APPENDIX B: ANTICIPATING THE SURGICAL STEPS ................................................................................... 29 APPENDIX C: CARDIO-PULMONARY BYPASS .............................................................................................. 31 APPENDIX D: DRUGS.................................................................................................................................. 33 APPENDIX E: IABP .................................................................................................................................... 34 APPENDIX F: SEPARATION FROM CPB FLOWCHART.................................................................................. 37 APPENDIX G: EPONYMS.............................................................................................................................. 38
About this document This document has been based on Dr Reny Segal’s Guide to Cardiac Anaesthesia at Wellington, written in 2002 – 2003. It is intended to provide an introduction to the RMH Way of Cardiac Anaesthesia, with occasional pointers/tips/suggestions & (hopefully) helpful guidelines. We hope that if you are new to cardiac anaesthesia it will give you an idea of what to expect, and what is expected of you. If you have had experience elsewhere, it will help you to adapt to local institutional habits. This is by no means a definitive text; techniques continue to evolve, and practice is not necessarily uniform among anaesthetists. The chapters are intended to follow the course of a typical operation; appendices deal with issues that would otherwise interfere with the exciting narrative momentum (such as it is). While our intentions are good, this document probably represents Class V evidence: what a bunch of us reckon we do (and in some cases what we think other people do). Although we consider the risk slight, it is possibly worth explicitly stating that readers should not perform cardiac anaesthesia without a thorough grounding in the relevant intellectual disciplines and a suitable period of supervised practice. The document is under constant revision, attempting to improve clarity and readability, but also reflecting changes in techniques and the results of feedback from readers. Some errors are identified and corrected with each revision, and of course new errors are quietly introduced. Feedback and suggestions are solicited and, of course, always welcome. - GS/GD/RS Feb 2009

3
Welcome to Cardiac Anaesthesia
Cardiac surgery presents the anaesthetist with many challenges. Every organ system is directly or indirectly involved, either in the disease process or the surgery . Invasive monitoring, issues such as neuro- and renal protection, active temperature management, and cardiovascular and respiratory pathophysiology are routine; serious coronary and/or structural heart disease are of course universal; and major co-morbidities are often present. Transoesophageal echocardiography is a fundamental skill and takes the role of the anaesthetist into the diagnostic realm. The interaction between the surgical and anaesthetic teams is far closer than in any other specialty. Preamble (Aims, Words of Wisdom & General Ramble): • We know it’s not for everyone. Unless you want it, we don’t expect to make you a
“cardiac anaesthetist”. • Familiarise yourself with the College aims for the cardiothoracic modules. If there are
specific things you need from any one session/list, let your consultant know. • Do not panic or feel out of your depth. You will be well supported at all times. You will
gain skills that will be of use to you in all (well, most) areas of anaesthesia practice. You will see fantastic physiology and pharmacology in action. You will get your module signed off!
• If you are an advanced trainee, use the opportunity to develop a feel for cardiac anaesthesia and to hone your skills with sick patients, lines, infusion management, inotropes, advanced monitoring, TOE, the theatre/ICU interface etc. Once you have demonstrated reasonable ability, many consultants will permit you to take control of cases.
• Fellows should expect to take control of cases once they have seen enough of the routine to be comfortable doing so.
• Remember that cardiac anaesthesia is still anaesthesia. The fundamentals apply, and oxygen remains a good thing etc.
• It can be challenging (!) to cope with the variations in the techniques and philosophies of the various consultants – although this is by no means unique to cardiac anaesthesia. Discuss the cases, see them together if possible, let them show you their individual tricks and so on. Many are enthusiastic teachers and have particular areas of strength to take advantage of.
• Avoid “passive spectator mode”. You will do, learn and enjoy more if you take an active role.
• Have a great time – or else!1
General Plan of the Operation
Usually, something like this: Pre-induction • establish non-invasive & invasive monitoring Pre-Bypass • prep & drape • conduit harvest & sternotomy • heparinisation & cannulation for bypass Cardiopulmonary Bypass 1 or else you won’t have a great time.

4
• pre-clamp • cross-clamp • post-clamp Post-Bypass • decannulation • closure • transfer & ICU handover As always, the whole things starts with an adequate assessment & preoperative planning…
Preoperative Assessment
For elective patients, this is generally done in Pre-Admission Clinic in 2E, days or weeks preoperatively. Some patients bypass this process and may require assessment in the ward. The 2E patients are generally easier because of the support systems that have been set up. While particular attention is paid to cardiac issues, a holistic approach remains important for what is essentially major whole-body surgery. • 2E patients are generally seen by the anaesthetist rostered to CPB; fellows/senior
registrars may be asked to help out. • In general, cardiac investigations should be relatively complete; however it is dangerous
to assume this is always the case. Note: the following concentrates on the things that are different or especially important to cardiac anaesthesia. Routine questions – medications/allergies, etc still need to be covered. History: • Basics
− what is the planned operation? − age, weight & height (important for CPB, haemodynamic indices, TCI pumps). − medications including herbal and complementary products
• Cardiac − functional status / failure? − risk factors and associated conditions − IHD
− angina stable/unstable? Recent MI? − incidental valvular disease?
− Valve surgery − valve lesion(s) and severity − incidental coronary disease?
• Vascular − atherosclerosis is a systemic disease − may have implications for conduit and peripheral arterial cannulation − cerebrovascular disease? AAA? renal artery stenosis?
• Respiratory − significant lung disease – pre-op optimization (consider physio, bronchodilators,
steroids), intra-op and ICU management − smoking - the College has a policy document. Reinforce the need to stop, bearing in
mind that everyone else will have told them already. Why should they listen to you? • Renal
− impaired? discuss with surgeon, perfusionist, renal medicine and ICU pre-op. − avoid nephrotoxins such as gentamicin
5
• Endocrine − DM – very common – may not have been formally diagnosed
− control (diet, OHG, insulin). HbA1c? − end organ damage?
• Neurology − baseline cognitive impairment?
− beware the older patient who is attended by their capable spouse and who is unsure of their personal medical history, medications, etc.
− pre-existent neurological deficits? − document baseline function
− unfortunately at present it is next-to-impossible to get formal cognitive function testing for surgical patients at RMH.
• Musculoskeletal/Connective tissue/Genetic anomalies − Marfan’s? − fixed joint deformities can make positioning very difficult
Physical examination:
− like any other, including airway − peripheral arteries − carotid bruits? − baseline heart rate, rhythm and BP are useful but easy to forget in the environment of
echo, angiography, nuclear medical scans and cardiac CT.
Investigations: • bloods
− UEC, FBE, glucose, coag − Extended Group & Save for routine cases
− crossmatch for small or anaemic patients, aortic and redo surgery • general
− 12 lead ECG − CXR − lung function if indicated
• vascular − carotid duplex scan (there is a protocol to identify patients requiring this)
• cardiac − There should be a coronary angiogram and/or an echocardiogram in the pre-
admission bundle or (for inpatients) progress notes. They clarify the anatomy, the lesions and the cardiac function. The angiogram: − shows you the coronary anatomy, and may indicate potential targets. Beware
significant Left Main Stem disease! − Outlines ventricular ejection and systolic function − may give the LVEDP − won’t tell you much about the valves
− The echocardiogram will: − outline systolic and diastolic cardiac function and ejection fraction (note: EF
misleadingly high with valvular incompetence) − indicate valve function / gradients − show chamber dilatation, hypertrophy, and thrombi. − not tell you anything about the coronaries.
− A myocardial perfusion scan (if available) can identify myocardium at risk. − At present cardiac CT seems to be used for screening rather than definitive anatomical
delineation of coronary lesions Things to actually do
6
• Document your assessment • Consent (or: Informed Decision Making)
− ask the patient whether they have “seen the video” − provide information without overwhelming the patient − address the patient’s specific concerns − provide a balanced view of the risks
− the surgery is generally far more dangerous than the anaesthesia − the patient’s untreated surgical condition is more dangerous still − the total anaesthetic risk is a small fraction of the overall risk
− involve the patient’s family in the process − document the discussion, and have the patient sign the anaesthetic consent
• Investigations − Ask the 2E staff to chase up anything that has been done but is not at hand − Routine bloods, CXR etc should have been ordered by the HMO − The 2E staff can help arrange other investigations if required.
• Medications − In general, don’t change prescription medications − do stop herbals − aspirin strategy depends on patient and surgeon − stop clopidogrel 7 – 10 days2 preop if possible − continue β-blockers − specify preop management of diabetes for patient while fasting
− provide clear written instructions • Dental
− Patients with obvious oral hygiene problems and all patients for valve / aortic surgery need to see a dentist at their own expense. The 2E nurses can coordinate this.
Inpatients: Inpatients tend to be somewhat more difficult than patients admitted through 2E, because they are often acutely unwell, and also because the system is generally set up for PAC / DOSA. • If they have not been to the PAC, it is likely that you are the first anaesthetist to see them
for this operation. If you are around the day before, it is ideal to see them then. • Before you see the patient, go over the notes. This will provide context to focus your
clinical assessment. • Don’t rush. You’ll miss stuff and your patient generally will need all the reassurance they
can get. Allow 30 mins or more to see one patient. • Assessment: see the previous topic. • Check what antiplatelet agents / thrombolytics have been administered. • The patients will probably not have had the benefit of “the video”. They may not be
aware of invasive monitoring and postoperative ventilation in ICU. Calm reassurance and decent explanations are called for – if you have not yet developed this skill, use your cardiothoracic cases to do so.
• Chart sedation if appropriate. Bear in mind the patient might be subject to last-minute list changes or cancellation, and that the patient’s active involvement in further medical consultations may be required – heavy duty premeds are potentially counter-productive. Temazepam 20 – 30mg on-call is generally satisfactory.
• Sort out your notes & inform the nursing staff of premed and other requirements. Discuss the patient with your supervising consultant.
Send for inpatients early – getting patients to theatre is not a high priority for busy wards.
2 The clopidogrel hysteria continues. Realistically 5 – 7 days would be plenty, but try telling a surgeon…

7
Theatre Preparation
• Arrive at 0710 – 07153 • ICU beds are guaranteed for morning cases – there is no need to check4. • Put correct TOE probe into OPA (observe protective precautions) • Perform machine check. Check monitoring. Position echo machine & IV poles. • Check
− At least 2 or 3 TCI pumps available, depending on whether TIVA is planned. − IMED with GTN – 2 channel pump if possible. − Ensure mains power ON to all pumps – it is axiomatic that batteries will fail at a
critical moment − Defibrillator with pacing is mounted on anaesthetic machine; check relevant cables
and defib pads are available − Blood in PACU fridge for redo & high-risk cases − Bair Hugger at foot of table.
• Prepare the drugs you expect to need for the patient (see Appendix E: Drugs ) • Infusions made up, labelled, loaded into pumps, primed, pump parameters set and ready
to go. Check that IMED giving sets have been de-aired. • Monitoring – default Cardiac profile should be satisfactory. While you can make changes
to suit special situations, reconfiguring the monitor defaults can result in abrupt termination of your life functions. You have been warned.
Anaesthetic Room
• Before you start, double check: − Planned operation. You’d be surprised how often the plan can change, or a radial
artery suddenly becomes required. Perhaps have another chat with the surgeons. − Laboratory results & blood availability
• Morning case – lines inserted on table in theatre. For afternoon case generally done in anaesthetic room to reduce turnaround time. Most important stuff is set up by RNs but you need to check and let them know if anything special is needed.
• Find your patient in the admission bay. • Check that you have the right patient! Look at the consent form and the label on the
patient’s arm. Most patients will have been to PAC and already had appropriate information and consent, but inpatients have often bypassed this step. Does your patient have any last-minute questions or concerns?
• Use whatever techniques you have developed to establish rapport and gain the patient’s confidence.
• Review the medication chart. Was a premed given? Was a drug given that should not have been?
• If the lines are to be done in theatre, transfer the patient onto the table. Take steps to minimize discomfort, including active warming.
Get ready to insert lines
− Give O2 via Hudson mask. Help establish routine non-invasive monitoring (ECG, oximetry).
3 Yes we know you’re not paid until 0730. Nor are we. 4 So they say. Sometimes morning cases are put on hold for an inconvenient interval, but actually cancelling one is almost unheard of.

8
− Midazolam or low-dose propofol TCI +/- fentanyl can be titrated to effect to facilitate line placement.
− The requirement for one or both radial arteries to be harvested can sometimes be anticipated but it is often better to speak directly with the surgeon. If in doubt, assume both radials are needed.
− Even if no radial artery harvest is needed, it is preferable to cannulate the right radial artery because of the way the pressure transducers have been set up and because the left may be required on short notice by the surgeons.
− Perform ultrasound mapping if desired. • Peripheral lines:
− 16 – 14G x 1. If there is no suitable peripheral vein (e.g. both arms are needed for surgery), just put something small in and use the neck line for giving volume. Several anaesthetists are no longer using large peripheral IVs for routine cases.
• Arterial line: − Aseptic procedure. Some operators like to use an arm board and chair. − Right radial or femoral artery unless required by the surgeon. Brachial or left axillary
artery can be used. − When it just won’t happen, try ultrasound. Don’t hesitate to get a colleague!
• Central Venous lines: − check that last-minute cancellation isn’t on the cards. − Generally awake5 at RMH, but some anaesthetists will consider asleep insertion in
suitable cases for patient comfort. (Note: this may increase turnaround time for pm case).
− Sterile procedure, gloves, gown, mask +/- ultrasound. − Usually via right internal jugular vein. Use ultrasound to check for a suitable vein
before you start. − Single or dual lumen Arrow sheaths. (ICU prefers dual lumen.)
• PA Catheter: − used for most cases at RMH – see “The Swan Ganz Debate”.
• Epidural: − practice varies from ‘nearly always’ to ‘occasional’ to ‘never’. Heparinisation related
to CPB is not a contra-indication. If an epidural is to be placed, it is best done after placement of the peripheral IV. Consider glycopyrrolate 200 mcg IV to reduce the risk of vasovagal response. High thoracic; not for the beginner.
• If you start an IV infusion at this stage, ensure the rate is controlled – do not permit administration of excessive crystalloid. Fluid warmer is routine – ensure turned ON for Off-Pump case.
• Maintain reassuring verbal contact with your patient. • If the opportunity arises, consider giving the antibiotic at this stage.
The Swan-Ganz Debate
Cardiac surgery at RMH has included the routine use of Pulmonary Artery Catheters (PACs) since the unit was established. There is little evidence-based support for this continued practice, and over recent years the risk – benefit ratio of routine placement of the PAC has come into question, as there have been several serious adverse outcomes (including deaths), with a cluster of cases in the early 00’s6.
5 the patient, not the anaesthetist. The anaesthetist should endeavour to remain awake regardless. 6 my, how time flies!

9
Nevertheless it remains the stated policy of the Cardiac Surgical Unit itself that PAC catheters be used. Several anaesthetists have challenged this directive and are using a variety of criteria to implement selective PAC placement. Patients in whom the perceived potential benefit is low (in general, patients with good LV performance, normal RV pressures, absence of serious valvular disease, and primary – rather than redo – surgery), or where the potential risk is high (elderly, frail females, pulmonary hypertension) would instead have a short triple-lumen CVC placed via a R IJV sheath. Some anaesthetists also prefer this CVC where off-pump surgery is planned. Some of the cardiac surgeons have complained that intraoperative management is only a relatively small part of the patient’s care and that postoperative care of the patient is difficult without the PAC. They have requested that the unit policy be followed. Registrars and fellows should expect to place a PAC unless a specific contra-indication exists or the anaesthetist in charge has directed that it not be used. If there is a difference in the views of the surgeon and the anaesthetist in this regard, we suggest that you do the arterial line and leave the neck line to the boss. Where a PAC is placed, it has now become standard practice not to wedge the catheter – it is advanced just a few centimetres past where the PA trace is obtained. This ensures that the tip of the catheter does not retract into the RVOT when the balloon is deflated, as dysrhythmias including VF can be induced otherwise. The final position of the tip of the catheter should be confirmed intraoperatively using TOE, and documented. Ideally the tip of the catheter should be in the proximal right pulmonary artery during diastole.
Pre-induction
The morning patient will generally have had their lines inserted in theatre. Subsequent cases will be on a trolley with more or less complete invasive monitoring set up. Bring them into theatre and help the RN set up the monitoring. • Encourage a bit of quiet until your patient is asleep. • Ensure correct monitoring is available, attached and working. Check transducers have
been zeroed and heights correct, BIS working, etc. • Attach infusions to appropriate sites. Ensure fluids are running correctly. • Do not induce patients with critical aortic stenosis, left main stem disease, cardiac
tamponade or ongoing ischaemia, without presence of a senior surgeon, nursing team scrubbed and set up, and clinical perfusionist immediately available.
• Have all your induction and haemodynamic support drugs ready to go. • Proceed to induction in a calm, unhurried manner. • Patient will be anaesthetized slowly. Reassure them that this is normal. Trap for beginners7 – if a PAC has only been inserted to the RA (e.g. tricuspid valve surgery, Ross procedure) make sure nothing is attached to the white or blue lumens.
7 experience lets you recognise your mistakes when you make them again

10
Induction
The Basics: • Induction is in theatre. • Maintain reassuring verbal contact with the patient. • Cast your eyes around & double-check things are ready. • Pre-oxygenate. • The drug recipes are many and varied. The exact recipe is less important than the desired
outcome – an asleep patient with haemodynamic stability. • Suggested generic formula:
− Give antibiotic pre-induction if possible − Midazolam to 5 mg, depending on pt condition and age − Fentanyl ≈ 500 mcg given slowly. − Propofol TCI ≈ 2 mcg/ml or 20 - 40 mg
− Some anaesthetists not using propofol at present, instead using an inhalational technique with sevoflurane and/or desflurane
− Sleep will be associated with ↓ BP – degree varies with the induction agent used & the condition (especially age) of the patient. May need to support with a pressor pending intubation.
− Remember that there is a lag time for the BIS to respond to changes in anaesthetic depth and a further lag for the BP to respond
− Rocuronium 50 - 100 mg +/- pancuronium 4 - 8mg. − Ventilate, intubate. These cases are generally not good ones for the HMO to practice
on – show off your smoothest, slickest, least stimulating intubation. − Secure the ETT. − Support blood pressure as indicated.
− metaraminol 0.25 - 0.5 mg increments or infusion − ephedrine 3 mg increments − inotrope infusion with induction should be considered for sick patients.
− Reduce maintenance anaesthetic during prep & drape • Eye tapes – must be waterproof as iodine/alcohol used by surgeons will dissolve corneas. • Insert TOE – don’t forget the bite block. • Insert CVC (sheath) ± PA catheter if not yet done. (You can use TOE to image the wire in
the SVC) • Surgical HMO will catheterise the patient. Catheter bag to our end of the table.
− If DHCA likely, insist on catheter with inbuilt temperature probe. • Insert nasopharyngeal temperature probe. • Positioning:
− Supine with the head on a head ring. − Most surgeons request a shoulder roll. Avoid excessive neck extension. − Apply adhesive defib pads if required
− redo’s − modified access cases − r/o PPM leads − patient with deactivated ICD
− Arms by side (unless radial to be used), palms facing inwards, elbows padded, arms secured by “over & under” folded sheet. Ensure ulnar nerves free from pressure.
− Check at the end of this routine that all your lines are still running, arterial trace present, and pressure points are protected.
− Head frame positioned over head at level of upper lip. Check clearance height. • Patients’ legs will be lifted if prepped. This will transiently increase central blood volume
and BP. This situation will also reverse when the legs are lowered. Do not overreact. • Once CV line in situ, connect and start infusions (see Maintenance). • Vasodilators and inotropes are connected to dedicated ports on the CV line/Swan

11
− the use of a carrier line is highly recommended if multiple infusions are to be used. • Move transducers to headframe. Support lines on head frame or Soeding support™
− ensure IV injection ports are conveniently accessible
Maintenance
Aims generally the same as most GAs: • Asleep (BIS 40-50) with IV or volatile maintenance with the mixture of your choice:
− opioids already given for induction. Titrate more if indicated. − remifentanil is infrequently used in cardiac surgery at RMH
− propofol infusion 10-30ml/hr or TCI 1-2 mcg / ml − volatile – sevo or desflurane − N2O is contra-indicated in cardiac anaesthesia. Air can be used before the chest is
opened but 100% O2 is recommended during IMA harvest because long apnoeas can be required.
• Neuromuscular blockade: Hard to monitor, there’s an ICU bed, and the surgeon will decompensate with even small amounts of diaphragmatic movement → better to over- than under-dose.
• check the patient from time to time, independent of the monitor − skin perfusion, diaphoresis, urine output
• Don’t give too much fluid. • Temperature management will depend on the nature of the case
− off-pump cases temperature maintenance more critical − most teams use mild hypothermia (34 – 35° C) for bypass
• There may be time for some “house-keeping” and TOE but if you are busy leave the paperwork for later.
• On pump cases, prepare for going on to bypass (see the next section).
Transoesophageal Echo
TOE was introduced into RMH by a small number of pioneers in the early to mid ‘90’s. It has quickly become adopted into routine cardiac surgery at RMH such that now there are few cases in which it is not used. Indications: • Cardiac: pretty much any cardiac surgery. • Non-cardiac: assessment of unexpected cardiovascular instability
diagnostic use in trauma, etc. Contra-indications: • Absolute (all very rare)
− oesophageal trauma, stricture, vascular rings − oesophagectomy
• Relative − oesophageal varices − frailty − cervical spine instability.
In theatre: • Enter the patient’s details so that the examination can be archived • Obtain an ECG signal if possible

12
• Prepare the probe, including the relevant paperwork • Insert the probe gently, after intubation but before the head frame is positioned • Do not use the friction brake or use large control deflections for long periods • Prioritise your examination so that you make important findings early. • Do not be distracted or pre-occupied by the TOE examination.
− The desire to perform a complete study must be considered in context. • When idle, leave a useful live image (4CH or LVSAX)
− Do not leave the machine in a Doppler imaging mode • If you are uncertain, say so. It may feel unsatisfactory to appear uncertain; it is worse to
be wrong in an important aspect of diagnostic work. • Ensure you are treating the live image, and not a loop. • Document your findings The TOE probe: • Is expensive and delicate • Check for mechanical function before sterilising • Check electronics (calibration) before insertion • Remove after chest closure; clean and/or sterilise according to protocol • The handle is not waterproof! Only the insertion piece is to be immersed during cleaning! The book: • Royse, Donnan & Royse: Pocket Guide to Perioperative and Critical Care
Echocardiography includes a fantastic CD!
Pre-bypass
The pre-bypass period extends from induction through to establishment of full CPB. This section deals with the end of the pre-bypass period, during which preparations are made for running onto bypass. Generally the surgical steps are: heparinisation is requested, the heart and great vessels are exposed and pericardial stay sutures placed. The sterile heart-lung machine tubing (“lines”) are taken onto the surgical field, and a pressure monitoring line is passed to you to attach to the CVP transducer. Purse-string sutures are placed in the aorta and right atrium. The aortic cannula is placed first, generally causing little haemodynamic disturbance and permitting subsequent administration of volume from the heart-lung machine. The venous line is placed via an incision into the right atrial appendage. The surgeon will then place the retrograde cardioplegia catheter – you will need to flush the pressure monitoring line and then watch the coronary sinus on TOE. The anterograde cardioplegia needle is then placed (either before or just after running on bypass) but does not typically require intervention on our part. If an LV vent is used it is usually placed via the right upper pulmonary vein. TOE is used to confirm correct placement of the catheter within the left ventricular cavity. • Heparin 0.4 kIU/kg (usually 20 – 30 000 units) given into central line when requested
− generally at the end of LIMA harvest (CABG) or after pericardiotomy (valve) − Confirm for surgeon that heparin given − Expect ↓ BP with large bolus heparin − Patients who have had recent or ongoing exposure to heparin (including LMWHs) can
exhibit significant heparin resistance. • ACT checked after ~ 3 minutes and ≥ 480. • Pericardial stay sutures may impede atrial filling, exacerbating ↓ BP • Manipulation and placement of purse-string sutures in the right atrium can cause AF. If
poorly tolerated consider − temporary support with pressors & volume from CPB machine

13
− synchronised DCR (unpopular with surgeon as clutters the field with paddles/cables) − run on bypass
• Cannulation of the great vessels requires coordination between the surgeon and anaesthetist − ↓ BP for aortic cannulation. Check before giving aramine that the surgeon isn’t about
to cannulate. With luck, it is possible to make a low BP look deliberate. − lungs off for retrograde purse-string − TOE for retrograde cannulation & placement of LV vent (if req’d)
• After the aortic cannula has been placed, volume can be given from the CPB machine. Check the arterial line for bubbles – the surgeon has a limited field of view through their loupes.
• Discuss anaesthetic issues with the perfusionist. They will usually have a good handle on the patient anyway but Communication Is A Good Thing.
Running on Bypass
The venous line clamp is removed, diverting the venous return from the right heart to the venous reservoir and pump/oxygenator. The lungs are isolated from the circulation and should be deflated to optimise surgical access. • Double-check the ACT, should be ≥ 480 secs • Turn the lungs off
− ventilator lever to bag mode, exhaust valve fully open − ventilator to CPB mode − do NOT turn O2 fully off (this is to avoid subatmospheric pressures in the breathing
system due to continued uptake by the lungs.) I usually leave 1 – 2 lpm running, as this is safe if I forget to turn up the O2 flows post-bypass.
− vaporiser off − inform the perfusionist if you need them to give a volatile agent
− some anaesthetists prefer to open or disconnect the breathing system • IV off • GTN off • Draw the PA catheter back a few cm…
− unless you’ve positioned it in the proximal pulmonary vascular tree under TOE − avoid pulling the catheter tip back into the RVOT.
• Anaesthesia − if you’re giving propofol, ensure the route is appropriate (i.e. has not been excluded
from the circulation by the mechanics of CPB). This is sometimes a problem with bi-caval cannulation e.g. for mitral valve surgery.
− if you’re relying on a volatile, make sure the perfusionist knows to continue it on bypass.
− make sure the perfusionist can see the BIS − consider giving another dose of your favourite NMB
• Pass the metaraminol to the perfusionist − standard concentration used by perfusion is 0.5 mg/ml
− really − regardless of what the anaesthetic consultant says
• If not already done, have a chat with the perfusionist about particular goals for the case. • Repeat the ACT about 3 minutes after running on, and a blood gas about 3 mins after
cardioplegia has been given. • DO NOT TOUCH THE HEART-LUNG MACHINE WITHOUT THE PERMISSION OF
THE CLINICAL PERFUSIONIST.

14
− really − this includes such apparently trivial interventions as blood sampling or drug
administration.
Pacing
• Epicardial pacing wires are generally placed during payback (i.e. after removal of the cross-clamp, prior to the wean from bypass) − Sinus bradycardia is common post-bypass.
− Bradycardia is relative: target heart rate usually 84 – 86 bpm. − Atrial wires generally adequate − Ventricular wires if the AV node is at risk (e.g. aortic valve surgery) or if the atria
cannot be counted on to drive the ventricles (e.g. AF). Some surgeons routinely place ventricular wires.
• At RMH, pairs of unipolar leads are used (as opposed to bipolar leads) − Atrial wires to RA near appendage − Ventricular wires to ant wall of RV
• Lead will be passed to you, usually colour-coded − Blue for A, White for V − … but of course, which lead does what depends on what they’re attached to!
• Plug the lead into the pacing box. • Familiarise yourself with the controls. The important ones are:
− Rate − Atrial current − Ventricular current (Set to 0 for atrial-only modes) − Mode (access via the Menu button)

15
• Remember the 3-letter classification of pacing modes: CHAMBER PACED CHAMBER SENSED RESPONSE TO SENSING V = Ventricle V = Ventricle I = Inhibited A = Atrium A = Atrium T = Triggered O = None O = None O = None D = Dual D = Dual D = Dual (I & T) • Commonly used modes at RMH are:
− AAI: good for sinus brady, even if V as well as A wires placed. Just turn the V output to zero.
− AOO: good for sinus brady, ignores diathermy (and everything else). − VVI: brady if AV node non-functioning. − DDD: AV sequential pacing. May be preferable to use AAI or increase AV interval
to permit normal depolarisation pattern – better contractility. • All of the synchronous modes are potentially susceptible to diathermy interference. • Defibrillation must be immediately available (i.e. external pads applied) if the
ventricle is to be asynchronously paced! − Resume synchronous pacing ASAP.
Basic operation: • Turn pacemaker box ON
− The box will wake up in DDD with reasonable defaults − Check for the presence of a Low Battery indicator & change the battery if needed
− The pacemaker can pace for a few seconds during a battery change, but it’s less stressful to do it beforehand!
• Set the target heart rate. 86 is quite a good number for weaning, but sometimes lower rates are used during payback.
• Set the desired pacing mode. AOO often useful post-bypass because it is not inhibited by diathermy.
• Plug the leads into the pacing box. • Test the pacing threshold of the leads. Pace at a rate comfortably higher than the patient’s
intrinsic rate. Reduce the output current until pacing fails. Increase it until it is recaptured. Lower = Better. − Regardless of the threshold, it’s usual to pace at ≥ 10mA − changing the polarity of the electrodes (done by the surgeons) can sometimes reduce
(improve) the threshold • Common settings
− Most settings can be left at the default values (except while checking thresholds) − Rate: 86 /min − increase the A-V interval if you’re trying to encourage intrinsic conduction
• Recheck for successful pacing, especially with closure of the pericardium and chest. • Take a bit of time and familiarise yourself with the pacing box (settings, controls, etc)
before the case. It’s far less painful than trying to work it out on the spot. Permanent Pacemakers: • liaise with cardiology dept • approach will depend on whether pt is pacemaker dependent • generally, ignore or set to slow DDD • the surgeon will apply atrial leads, enabling rate control • ignore pacemaker and pacing spikes during induced arrest. AICDs:

16
• will diagnose diathermy as a malignant arrhythmia and deliver anti-tachyarrhythmia therapy (i.e. programmed shock)
• disable shock delivery during surgery: − inhibit with a magnet placed over the device, or − ask cardiology pacemaker tech to reprogram to disable defibrillation
• apply external defib paddles • ensure device re-enabled at early opportunity postop.
Coming off Bypass
This is the moment of truth – they are about to take away the nice CPB machine and make the circulation your problem again! Communication with the surgeon and perfusionist is critical. The job is especially challenging because the heart is recovering from ischaemia, cardioplegia, handling, and reperfusion. You should have an idea of the degree of support the heart is likely to need by its pre-bypass function and the nature of the surgery. Beware that the heart can sometimes look artificially ‘good’ pre-bypass (e.g. mitral incompetence); the full degree of LV dysfunction is revealed after the valve has been repaired. Checklist:
− Ventilator on, lungs inflated − Cardiac rhythm stable, adequate rate (pace if necessary) − Cardiac chambers closed, de-aired. − Major bleeding controlled − Physiology OK:
− ABG, Hb, K+ − Hb ≥ 7-ish
− Temperature > 36 ºC − LV capable of ejection
− adequate payback − inotropes running and in patient (beware deadspace, 3-way tappisms)
Partial Bypass & Wean: • the perfusionist will partially clamp the venous line and blood will be diverted through
the right heart and lungs. This blood should then be ejected from the LV. • the lungs must be ventilated during periods of partial bypass – otherwise the pulmonary
blood-flow through the deflated lungs serves as a shunt, and can cause desaturation. − as always, apnoeas might be required for surgical access. Keep them brief, or go back
on full flows • the partial bypass period can help give an idea of LV performance. Look for snappy
contraction and a brisk upstroke on the systemic arterial waveform. Beware a poopy-looking ventricle, one that doesn’t eject, or one with dyskinetic segments, especially since, in general,
“All hearts look good on bypass” (Goldblatt’s Second Law8) • If the heart looks crappy at this stage, consider more payback or start some inotropes and
wait until they hit the circulation. If the situation is really poor, IABP may be required.
8 Goldblatt’s First Law: “the person who answers the phone won’t know what’s going on. The people who do know what’s going on are too busy working to answer the phone.” Also, see the section on Eponyms.

17
• Beware LV distension. If the heart cannot eject and fills, discuss with the surgeon either re-applying the cross-clamp with retrograde perfusion, or inserting an LV vent.
• Air in the right coronary artery is a common occurrence and results in impressive ST-segment elevation and inferior SWMAs. Treat with − time − raised perfusion pressure − pulsatile perfusion − GTN
• To wean from bypass, the perfusionist further clamps the venous line and displaces blood volume from the venous reservoir to the patient
− systemic pressure becomes more pulsatile − PAP & ETCO2 rise as pulmonary capillary flow returns − drugs administered into the venous reservoir might not get to the patient
− IV drugs go via our vascular access − remember to turn on the vaporiser! − re-route drugs being given into the heart-lung machine
Difficult or failed wean (see Appendix: Separation Flowchart) • maintain two-way communication with the surgeons
− do not merely prop up the BP with metaraminol • maintain perfusion pressure • check the basics:
− blood oxygen content OK? − check O2 from wall outlets to patient − check ventilation (MV, lungs inflated)
− rhythm / heart rate / pacing mode & capture − conduits unclamped? − CO / wedge
• TOE examination − volume
− adequate? esp. for non-compliant ventricles (diastolic dysfunction) − excessive? (ventricle distended)
− global LV function − SWMA − acute valvular dysfunction
• if dire, consider a further period of full or partial support on bypass • volume- or pressure-loaded RV needs plenty of perfusion pressure • don’t forget anaphylaxis (or similar) as a cause of circulatory failure
− protamine & blood products Inotropes • decision to use inotropes (rather than temporising with calcium and pressors) and
selection of a particular agent or combination depends is sometimes more of an art than a science and depends on − LV performance − pulmonary vascular resistance / PAP − measured parameters such as BP & CO − surgeon’s and anaesthetist’s innate preferences and experience

18
• combinations include − dopamine
− like low dose adrenaline − adrenaline
− when you’re not mucking around − noradrenaline
− where CO is maintained or high but hypotension is the problem − dobutamine − milrinone / noradrenaline combination
− we usually use about ½ of the ‘low dose’ regimen − milrinone 25 mcg / kg load, then 0.25 mcg / kg / min infusion
(usually 2 mg load then 10 ml/hr of standard (120 mcg / ml) brew)
Post-bypass
The bypass cannulae are removed and the cannulation sites secured. Heparin is reversed with protamine and definitive surgical haemostasis is achieved. The pericardium is closed, then the sternum wired. The circulating blood volume is adjusted in response to clinical and TOE assessment. Anaesthesia including neuromuscular blockade is maintained. Preparations for transfer to the ICU bed are made. Decannulation: • clinical perfusionist announces “venous is clamped” • venous cannula removed usually promptly • volume given via aortic cannula as required • commence protamine (see below) • systolic BP 90 – 100 for removal of aortic cannula • transient aggressive hypotension (~ 60 mmHg) is sometimes required if haemostasis of
aortic cannula site is a problem − Do NOT give or continue protamine in this situation because it precludes the use of
cardiotomy suction Protamine: • After full wean from bypass • subject to surgical clearance
− pt looking reasonable & separation likely to be successful − valve repair or prosthesis satisfactory − primary surgical haemostasis reasonable
• dose based on heparin dose − usually described as equal to the heparin dose (see Appendix D) − anaesthetists vary in their approach to protamine dosing if additional heparin given
• test dose (10 – 20mg), then slowly to ⅓rd of the planned total dose (approx 20 – 30 mg/min)
• at ⅓rd, make announcement and stop − arterial line removed (ensure systolic BP 90 – 100) − surgeons will have “last suck” with cardiotomy suction − continue protamine after aortic haemostasis confirmed, surgical clearance, &
cardiotomy off • announce full protamine dosage given • ACT 3 mins later. Target ~ 105 – 140 secs, lower is better. Protamine reaction: • any combination of:

19
− hypotension, hypoxia, pulmonary hypertension, pulmonary oedema, circulatory collapse − often a diagnosis of presumption after attempts to exclude other causes
− potentially lethal − can require re-establishment of CPB
− give more heparin! − so, how to reverse heparin in this situation? Usually protamine, on the basis that
there are few other options (polybrene has been used, but is very difficult to get hold of), and that the second attempt with protamine is usually surprisingly well tolerated.
Closure: • Closing the pericardium reduces cardiac chamber compliance
− may need volume and / or pressor • Closing the sternum reduces chest wall compliance
− use volume (not pressure) target for ventilation − ensure adequate paralysis
• Surgical stimulation is relatively slight during the post-bypass period and the maintenance anaesthetic can often be reduced. − monitor the BIS − maintain systolic BP 100 – 110 (but some surgeons prefer higher BP) − GTN / fentanyl or hypnotic to treat hypertension
Bleeding
Few things strike fear into the heart of the cardiac anaesthetist so much as the prospect of bleeding9. Broadly speaking, troublesome bleeding can be classified as audible haemorrhage (torrential, exsanguinating haemorrhage, for example, arising from a surgical misadventure), surgical, and coagulopathic haemorrhage. Although cardiopulmonary bypass results in platelet injury and factor consumption, in most patients reasonable haemostasis can be obtained with adequate reversal of heparin (protamine) and meticulous surgical technique (prolene). Some fundamentals: • bleeding causes bleeding; take prompt action to control haemorrhage • avoid physiological states that favour bleeding such as hypertension and hypothermia • anticipate difficulties in haemostasis and consider pre-emptive management strategies
− redo surgery − complex surgery such as Ross, Bentall, or compound operations − deep hypothermia − prolonged bypass − perioperative antiplatelet or thrombolytic treatment − massive transfusion
• most cases of surgical haemostatic unhappiness respond to adequate doses of protamine, and early administration of platelets − use a heparinase ACT (cuvettes in the refrigerator in the perfusion room) to rule out
residual heparin effect − the Blood Bank (ext 27275 / 27276) understands CPB-related platelet dysfunction and
will issue platelets without a platelet count for these patients. 9 inter alia, it has the potential to make the case go late

20
If bleeding continues despite these simple measures: • establish liaison with the Blood Bank and a transfusion haematologist. • platelets, FFP, cryo. More platelets, more FFP, more cryo. More prolene. • Send coag studies (make it clear whether the patient is heparinised or not) • keep control of the BP • if clot lysis seems to be the problem, consider adding an antithrombolytic. (For most of
the cases above, the patient will have been on aprotinin or tranexamic acid anyway.) • facilitate / encourage the surgical team’s efforts at primary haemostasis • Novo 7 (eptacog alpha, or recombinant Factor VIIa) can make a remarkable difference.
It’s a little hard to get because of the cost involved – suggest it early. Make sure there is enough substrate around for it to make a difference (platelets, cryoprecipitate). May not help that much if bleeding is associated with a synthetic graft.
Surgical haemorrhage: • While we are dependent on the efforts of the surgeon to gain control10, meticulous
attention to BP control, provision / replacement of platelets and clotting factors is necessary. It is sometimes necessary to over-treat presumptive coagulopathy to demonstrate that the haemostatic defect is, indeed, surgical. − Many of the surgical efforts effectively plug holes from the outside. Hypertension can
sabotage these efforts. • Novo 7 can have a role here: whatever size hole will stop bleeding without Novo 7, a
bigger hole will stop with it. Audible haemorrhage: • Hope that the surgeons can regain control. If not, prepare to do some paperwork. • Consider heparinising & using cardiotomy suction to collect blood into the pump
reservoir. If the arterial anatomy is sufficiently intact the situation can sometimes be salvaged by using “sucker bypass” until definitive control is achieved. − if selective perfusion is necessary, remember that retrograde cerebral and myocardial
perfusion can buy time. At the end of a difficult (in the haemostatic sense) case, send off repeat coag studies & FBE prior to heading off to ICU. It’ll take an hour off the time for ICU to get a result.
ICU
Postoperative ventilation in ICU remains a notable feature of the routine care of patients after cardiac surgery. The rationale for this is largely pragmatic: patients seem to do better11. A combination of potentially large fluid shifts and altered capillary permeability may predispose to circulatory instability, cerebral & pulmonary oedema. Having the ICU bed also means that the anaesthetist can use techniques, such as high-dose opioid-based anaesthesia, that would otherwise not be available. Most patients are extubated after 4 – 6 hours. • There is no need to check for a bed for the morning case (but there’ll occasionally be a
delay for its availability). For subsequent cases the patients are not released by 2E unless a bed is available. − if there is uncertainty, speak directly with the ICU Bed Manager (ext 24105)
10 it’s axiomatic that difficult surgical bleeding is from somewhere impossible to get to, around the back of the heart. 11 and many people have tried.
21
• ICU require a call ½ hr before the patient arrives12. The anaesthetic nurse will usually do this, you but can sometimes save embarrassment by checking that it has been done.
Transfer: • Move patient onto ICU bed; transfer monitoring
− ECG, SpO2, Art, PA, ETCO2 − ICU appreciate transducers on pole to patient’s left hand side
• Patient ventilated on 100% O2 on transport ventilator, usually an Oxylog. − Check primary & backup O2 cylinders
• Sedation / hypnosis / analgesia & NMB as appropriate • Routine extra equipment includes:
− transport kit - self-inflating bag, laryngoscope, etc − defibrillator at foot of bed but not usually attached to pt
• Drugs to bring: − hypnotic of choice − pressor
• Infusion safety: ensure infusions that are not in pumps are turned off (3-way tap), to prevent uncontrolled administration
• ‘Outside’ tech will help move bed. The surg reg/fellow will accompany you to ICU ICU handover: Identify the RN who will look after the patient; wait for the intensivists Handover should include relevant background, as well as important intraoperative events • patient identity, presenting history & relevant risk factors; significant co-morbidities
− functional status • operation/s performed • notable intraoperative events
− anaesthetic technique − intubation difficulties; ventilation issues − unexpected findings (e.g. on TOE) − complications − difficulty with wean from CPB
− arrhythmias associated with r/o cross-clamp are usually inconsequential − haemodynamic issues; inotrope or pressor support − haemostasis issues − pacing
• antibiotics given • make sure any infusions running are clearly labelled and pharmacologically sane. Delay for ICU bed • maintain sedation / analgesia
− switch to propofol infusion if maintenance has been with a volatile agent • continue IPPV. Add PEEP and reduce FiO2 now that apnoeas are no longer likely • continue full haemodynamic monitoring • continue suction on drains, etc. • manage circulatory volume with pump blood, colloids and/or crystalloid.
− do the routine initial ICU bloods & manage the results − CXR if there’s time
• if the wait is long, ensure pressure care • if the patient is very well behaved, consider extubation 12 Exactly why this should be is unclear. One theory is that the phone call is a trigger to scatter obstacles along the path through ICU

22
Morning case can sometimes be moved into PACU • check with DA nurse-in-charge first! • This allows the theatre to be used for the second case13, but will take an anaesthetist and a
nurse out of play • if the delay is likely to be short, the transport ventilator and monitoring can be used
− don’t forget to plug power & O2 into wall outlets! • otherwise use a spare anaesthetic machine to provide IPPV & full monitoring.
Modified Bypass: OPCAB and PADCAB
Background: In late 90’s & early 00’s, there was widespread surgical enthusiasm for Off-Pump Coronary Artery Bypass (OPCAB) and, to a lesser extent, Perfusion Assisted Direct Coronary Artery Bypass (PADCAB). This was largely in an attempt to mitigate adverse surgical outcomes believed to be due to CPB or to cross-clamping, e.g. neuropsychological defects, coagulopathy, and myocardial ischaemia14.
A variety of techniques were developed to manipulate the heart so that the target sites could be accessed, and immobilising devices with names like Octopus™ or Platypus™ were a healthy source of income for company reps. Temporary shunts were sometimes used to allow coronary perfusion during the anastomosis.
Unfortunately, the hoped-for neuropsychological and other outcome benefits were largely unrealised. PTCA has taken most of the ‘easy’ candidates for CABG, and some surgeons consider that there is potential compromise in the selection of targets and in the anastomoses.
As a result, the techniques have fallen somewhat out of favour, although there are some cases which remain suitable. In particular, be on the lookout for cases where few grafts are planned (esp. CABG x 1 – 2 on LAD +/- PDA systems only)
OPCAB • Very poor correlation between booked OPCAB and actual OPCAB • Our setup (monitoring, patient positioning, etc) basically as for on-pump case. Some
anaesthetists prefer to avoid use of PA catheter for OPCAB. • Speak up if you don’t think the patient will cope (e.g. poor cardiac output with marginal
BP requiring support). • While doing a case off pump is principally a surgical decision, factors such as the
coronary anatomy, the patient’s cardiac function, and the presence of calcification or severe atheroma of the great vessels (esp. the ascending aorta) are important.
• The heart-lung machine is prepared and available on standby. • Heparinisation is still required. Start with 200 – 250 U / kg. Aim for an ACT > 380. • Recheck ACT every 20-30 min. Heparin 2500 – 5000 U prn to maintain ACT. • Surgeon may request for reduced tidal volume. Compensate with higher resp rate, or
accept ↑ CO2 • Have a pressor available – administer in small doses (e.g. metaraminol 0.1 – 0.25 mg) or
by infusion. Judicious volume loading may also be needed to maintain systemic perfusion pressure.
• temporary pacing can be needed if the AV node misbehaves, e.g. during PDA grafts • If you need to reduce the blood pressure, do it gently. Take some GTN from the infusion
bag into a syringe and administer 0.25 – 0.5 ml ( = 150 – 300 mcg) • The surgeon will usually want the systolic pressure around 90-100 mmHg.
13 of course, there’ll now be a delay for the second bed, too. Better ring home, you’re gonna be late . 14 Well, there may have been some me too-ism as well.

23
• Access to the LAD and PDA territories is usually straightforward. Grafting the posterior surface of the heart (grafts to the obtuse marginals) is more difficult and requires substantial displacement of the heart.
• With the heart dislocated, there is a degree of interference with both venous return and forward flow − Keep the surgeon informed. If BP does not come up with volume loading & some
pressor, it may be necessary to reduce the displacement or abandon the off-pump approach.
− The VTI of descending aortic flow can be used to monitor stroke volume • The surgeon may apply a side-biting clamp to the aorta to sew top ends.
− Tight control of the BP is important – hypertension can cause the clamp to slip or cause aortic injury.
− There is the risk of plaque embolisation. This is largely out of our hands, but good BP control can make initial placement of the clamp easier and therefore less likely to need repositioning. Encourage the surgeon to do an epiaortic study.
• Blood loss can be insidious but substantial. Encourage the surgeons to use the cell-saver suction. Keep an eye on the patient’s volume status.
• Keep the patient warm − Raise the room temperature − Forced air warmer on as much of the patient as you can.
• Check gases regularly throughout the procedure. • Protamine is given in reduced dose. Usually only partial heparin reversal is desired. • Transfer to ICU intubated and ventilated PADCAB This is basically doing the case on-pump, but without applying the cross-clamp. As a result, the heart continues to beat (a nuisance for the surgeon and therefore bad) but the myocardium is not subject to ischaemia & cardioplegia, and systemic perfusion is maintained even with aggressive cardiac displacement (good). Sometimes viewed by surgeons as combining the worst features of all of the available techniques! • Sometimes suitable for patients who cannot be cross-clamped because of aortic disease
(“porcelain aorta”), severe atheroma, etc. • Obviously, set-up and heparinisation etc is as for standard on-pump case. • Lungs off, as for on-pump, unless the BP is pulsatile (i.e. partial bypass), in which case,
ventilate with ↓ MV. Don’t forget to ↑ again when pump off! • Unlikely to have to worry about side-biting aortic clamp (we’re doing this because of
aortic disease, right?) • Some R-sided open cardiac procedures can be done in a similar fashion (e.g. pulmonary
valve). For others, such as ASD repair, most surgeons just use a cross-clamp to get the benefit of an immobile heart
• Monitor for LV distension. If the heart fibrillates (or just stops), it is crucial to − restore the cardiac rhythm (zap or pace) or − apply a cross clamp and give cardioplegia or − insert an LV vent
• The heart should bounce off bypass. Problems should prompt a search for factors that have changed since pre-bypass – specifically, technical issues with the grafts.
Redo Cardiac Surgery
Re-operation months or years after cardiac surgery is moderately common, and confers substantial additional risk such that special consideration of the issues is warranted. In particular, the pericardial sac is largely obliterated after cardiac surgery. The RV can be adherent to the sternum. It is usually impossible to deploy internal paddles in the pre-bypass

24
phase, so external defib pads are applied in case defibrillation is required. Internal cardiac massage can be impossible. Sudden, massive blood loss can occur, and can be effectively uncontrollable (refer audible haemorrhage in the Bleeding section.) Non-cardiac factors: • Patients will generally be older • Conduit may be in short supply Anaesthetic: • Consent often a little easier (had it all before) but surgical risks are substantially greater.
− Much greater likelihood of transfusion of blood or products; use of coagulation factors or platelets post-bypass almost universal
− Possibly ↑ risk of drug reaction (protamine, aprotinin) with previous exposure • Apply external defib pads pre-induction • Have blood in room for sternotomy • Use of antithrombolytics almost universal • Discuss with surgeon
− cannulation pre-sternotomy? − cannulation sites? − conduit at risk (e.g. graft crossing beneath sternotomy)?
Cardiac and surgical factors: • May require establishment of CPB pre-sternotomy (e.g. via femoral cannulation) • Modified sternotomy technique • Painstaking dissection of adhesions, identification of old grafts. • No ready access to cannulation sites (RA, ascending aorta) • Patent existing IMA grafts must be clamped in addition to application of cross-clamp • Patent existing IMA grafts must be unclamped on r/o cross-clamp! • Typically, sternotomy is followed by enough dissection to cannulate, then more
dissection performed on bypass (allowing more aggressive manipulation of the heart). • Adhesiolysis leaves bleeding raw surfaces. Everything bleeds.
Removal of Permanent Pacing Lead Systems
Dr Neil Strathmore is an RMH cardiologist with special expertise in this field, such that most such procedures within SE Australia are referred to him and performed at RMH. The procedures are performed in the operating theatre because the potential complications are serious and may require urgent cardiac surgical intervention, including sternotomy and/or institution of CPB. A cardiac surgical team is on standby, and during difficult stages a surgeon is in attendance. Removal of the generator is straightforward but the pacing lead systems are not designed for easy removal and tend to be firmly adherent to endocardium and adjacent great vessels. Patients are of all ages but tend toward the elderly. Infection is the commonest reason for lead extraction, and can be limited to the site of the generator or involve the leads with frank endocarditis. Patients with ICDs often have poor ventricular function. Clearly, some patients will be pacemaker dependent; a temporary pacing system must be placed before the PPM is detached in these patients. TOE and II are used throughout the procedures, which generally take from 1½ to 3 hours.

25
Many patients have had previous cardiac surgery: on the one hand, they are less likely to develop cardiac tamponade because the pericardial sac is obliterated; on the other, if sternotomy is required for salvage, this is extremely difficult. Complications include: • cardiac perforation +/- tamponade • acute tricuspid valvular incompetence • pulmonary embolism (e.g. of lead vegetations) • rhythm disturbances • blood loss is rarely spectacular but over the course of a long case can be significant.
Check that a valid group & screen has been performed, and a cross-match for high-risk cases.
• Rarely, extrapericardial vessel perforation can result in haemothorax. • inadvertent activation of ICD. Check with the proceduralist that the ICD has been de-
activated. In general, the difficulty of removal, likelihood of serious complications, and duration of surgery are all proportional to the time the lead system has been in place. WARNING: the ‘general’ cardiac workup of these patients is sometimes incomplete, tending to focus on the PPM lead system. It is often worth chasing echocardiograms, angiograms etc, which may have been performed in other institutions. Set-up: Mostly as for a routine heart • Table – rotated 180° (for II to fit) • Large-bore peripheral IV (or IV on side-arm of CVC, if placed) • Arterial line • External defib pads • CVC (can often be inserted after patient asleep) if
− target PPM leads in-situ for ≥ 5 years − patient sick and needing one anyway − inadequate peripheral venous access − proceduralist worried
• Routine non-invasive cardiac monitoring − 5-lead ECG, temp, BIS − usually no IDC unless proceduralist really worried − ETT
• TOE • Head frame, shoulder roll, head-ring Conduct: • ‘Routine’ GA with a view to extubation & PACU. • traction on lead system → cardiac distortion → hypotension. • cases not intrinsically very painful. TOE: • used to monitor for complications, as above • sometimes will need to withdraw probe if obscures II of leads.

26
Interventional Cardiology
The RMH Cardiology Dept has an interventional unit. Electrophysiological procedures range from ICD implantation & testing, to minor pathway ablations, through to extensive 3D mapping that can take 6 – 8 hours. Structural procedures include ASD & PFO closure, and stenting coarcts. We also have an occasional role in the salvage / resuscitation of patients with acute crises such as coronary dissection. Some fundamentals: • In cath lab on 2nd floor
− one lab has been set up for EP work; the other has better imaging and is used for the structural stuff
• Patients usually DOSA via 2E. • Despite several attempts, cardiologists are unable to appreciate the difference between
their (cardiology) preadmission process, and ours. As a result, the patient will generally not have had an anaesthetic assessment and from time to time significant anaesthetic issues are only picked up at the last moment.
• Usually GA, occasionally proceduralist will request IVS − on rare, blissful occasions, standby − for ICD & test, ICD implantation under LA/sedation then single-shot propofol for
ICD test is often reasonable. • For most procedures the proceduralist stands to the patient’s right and we end up on the
patient’s left near the head. Peripheral vascular access via the left upper limb is generally suitable. − ICDs the proceduralist stands at the patient’s left and we need to move to the right.
− The anaesthetic machine needs a very long O2 (white) supply hose • Sometimes access via the R IJV is required, for placement of a coronary sinus electrode. • II is extensively used. Since we do not necessarily face the X-ray source, ‘wrap around’
lead protection is required. Monitoring: • 3-lead ECG (in addition to ECG of external defib & EPS surface electrode array.) • Defib pads (placed by EP technician) • Art line for most cases (can be done asleep for well patient) • BIS & neuromuscular monitoring • IDC for long cases e.g. pulmonary vein isolation for AF, or 3D mapping (“Carto”)
− really (despite the potential disinclination of the cardiologists) Induction & Maintenance: • Rotate table to permit access to head/airway • ETT if TOE required • Route airway tubing away from the area that the X-Ray tube needs to rotate.
− for EPs the X-Ray tube rarely needs to move beyond 45%; for structural work true laterals may be required – move equipment to provide clearance.
• Long and frequent apnoeas are required. − maintain on 100% O2 − opportunistic ventilation between burns − (IIPPV = Intermittent Intermittent Positive Pressure Ventilation) − beware the patient with limited respiratory reserve, who cannot catch up again before
the next apnoea − if necessary, suppress spontaneous respiration with NMB or opioid.
• Trans-septal approach to LA may require TOE guidance • Cardiologists may occasionally request TOE examination to exclude haemopericardium.
27
• Beware excessive administration of crystalloid. With an irrigated ablation catheter, pt can have 1 – 2 L fluid in addition to what we give.
• Inform the cardiologists if hypotension occurs. Often pacing related, but can trigger a request to check for cardiac perforation.
• The patient will often be paced (from various sites within the heart) for most of the case. The pacing rate is often given as cycle length, in milliseconds. Hence ‘pace at 600’ means 100 bpm.
• Ask the cardiologist for some pacing if bradycardia is a problem. • Heparin ~ 100 - 150 U/kg will be requested if catheters are to be placed in the LA. The
target ACT will generally be 300 – 350 seconds, monitored ½ hourly. Low dose heparin ~ 2500 U may be requested for less critical work.
• Protamine is usually not given. • Isoprenaline is often to initiate the target dysrhythmia. The cardiology staff will make up
a syringe (100mcg/ml → 6ml/hr = 1 mcg/min ) & provide a pump. • Structural work sometimes requires that the patient’s arms are positioned above their
heads. Ensure adequate IV/art line tubing lengths & freedom of movement. Emergence & Recovery: • To 3rd-floor PACU. Give them a ring a few minutes before turning up. • Post-procedure pain rarely severe, but may sometimes require IV paracetamol +/- opioid.
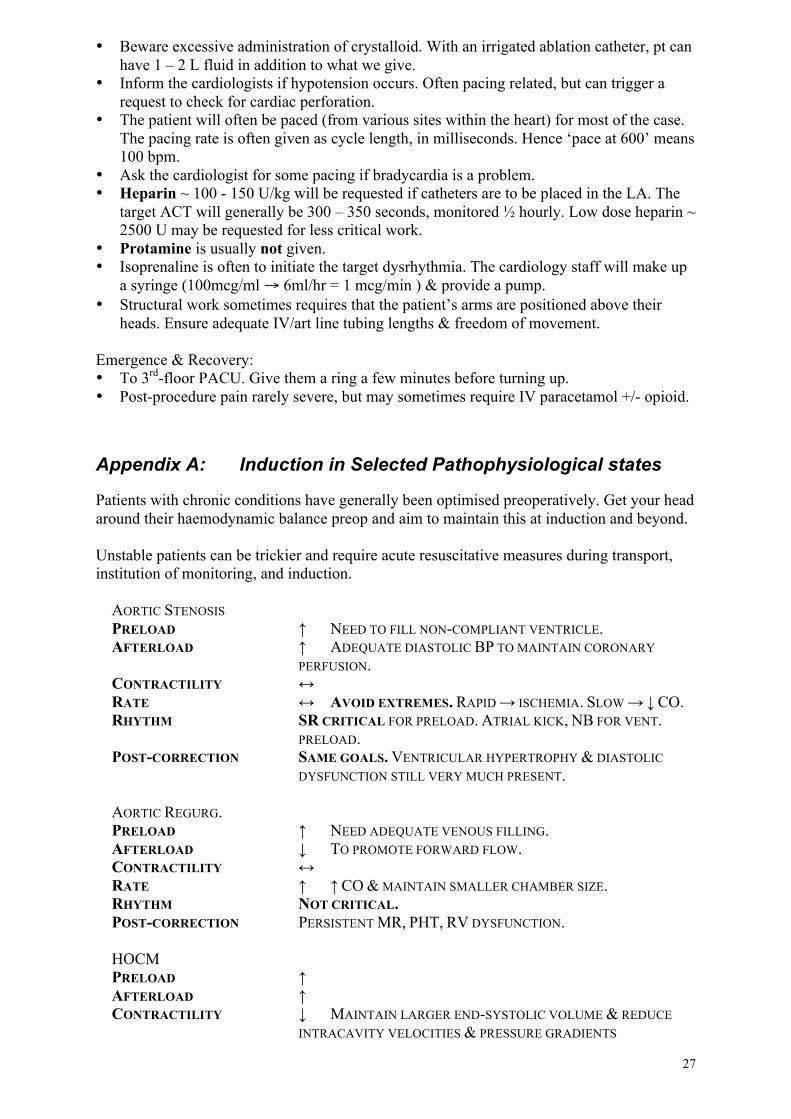
Appendix A: Induction in Selected Pathophysiological states
Patients with chronic conditions have generally been optimised preoperatively. Get your head around their haemodynamic balance preop and aim to maintain this at induction and beyond. Unstable patients can be trickier and require acute resuscitative measures during transport, institution of monitoring, and induction.
AORTIC STENOSIS PRELOAD ↑ NEED TO FILL NON-COMPLIANT VENTRICLE. AFTERLOAD ↑ ADEQUATE DIASTOLIC BP TO MAINTAIN CORONARY
PERFUSION. CONTRACTILITY ↔ RATE ↔ AVOID EXTREMES. RAPID → ISCHEMIA. SLOW → ↓ CO. RHYTHM SR CRITICAL FOR PRELOAD. ATRIAL KICK, NB FOR VENT.
PRELOAD. POST-CORRECTION SAME GOALS. VENTRICULAR HYPERTROPHY & DIASTOLIC
DYSFUNCTION STILL VERY MUCH PRESENT.
AORTIC REGURG. PRELOAD ↑ NEED ADEQUATE VENOUS FILLING. AFTERLOAD ↓ TO PROMOTE FORWARD FLOW. CONTRACTILITY ↔ RATE ↑ ↑ CO & MAINTAIN SMALLER CHAMBER SIZE. RHYTHM NOT CRITICAL. POST-CORRECTION PERSISTENT MR, PHT, RV DYSFUNCTION.
HOCM PRELOAD ↑ AFTERLOAD ↑ CONTRACTILITY ↓ MAINTAIN LARGER END-SYSTOLIC VOLUME & REDUCE
INTRACAVITY VELOCITIES & PRESSURE GRADIENTS
28
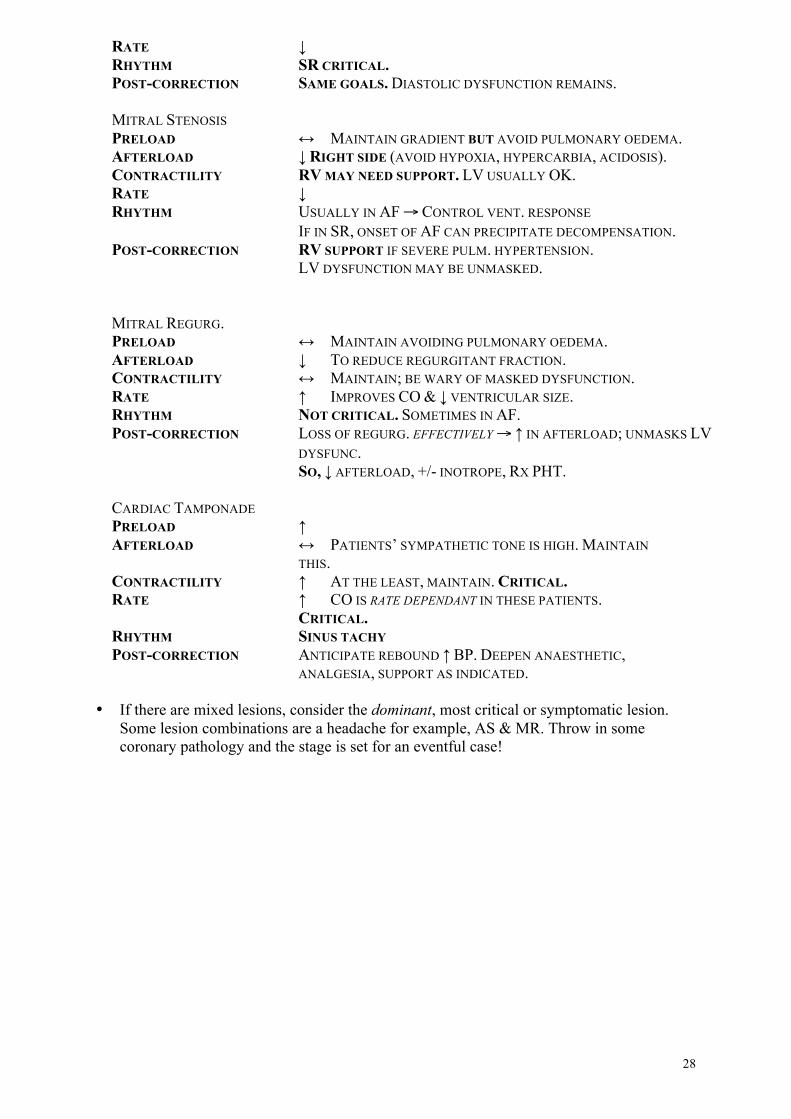
RATE ↓ RHYTHM SR CRITICAL. POST-CORRECTION SAME GOALS. DIASTOLIC DYSFUNCTION REMAINS.
MITRAL STENOSIS PRELOAD ↔ MAINTAIN GRADIENT BUT AVOID PULMONARY OEDEMA. AFTERLOAD ↓ RIGHT SIDE (AVOID HYPOXIA, HYPERCARBIA, ACIDOSIS). CONTRACTILITY RV MAY NEED SUPPORT. LV USUALLY OK. RATE ↓ RHYTHM USUALLY IN AF → CONTROL VENT. RESPONSE
IF IN SR, ONSET OF AF CAN PRECIPITATE DECOMPENSATION. POST-CORRECTION RV SUPPORT IF SEVERE PULM. HYPERTENSION.
LV DYSFUNCTION MAY BE UNMASKED.
MITRAL REGURG. PRELOAD ↔ MAINTAIN AVOIDING PULMONARY OEDEMA. AFTERLOAD ↓ TO REDUCE REGURGITANT FRACTION. CONTRACTILITY ↔ MAINTAIN; BE WARY OF MASKED DYSFUNCTION. RATE ↑ IMPROVES CO & ↓ VENTRICULAR SIZE. RHYTHM NOT CRITICAL. SOMETIMES IN AF. POST-CORRECTION LOSS OF REGURG. EFFECTIVELY → ↑ IN AFTERLOAD; UNMASKS LV
DYSFUNC. SO, ↓ AFTERLOAD, +/- INOTROPE, RX PHT.
CARDIAC TAMPONADE PRELOAD ↑ AFTERLOAD ↔ PATIENTS’ SYMPATHETIC TONE IS HIGH. MAINTAIN
THIS. CONTRACTILITY ↑ AT THE LEAST, MAINTAIN. CRITICAL. RATE ↑ CO IS RATE DEPENDANT IN THESE PATIENTS.
CRITICAL. RHYTHM SINUS TACHY POST-CORRECTION ANTICIPATE REBOUND ↑ BP. DEEPEN ANAESTHETIC,
ANALGESIA, SUPPORT AS INDICATED. • If there are mixed lesions, consider the dominant, most critical or symptomatic lesion.
Some lesion combinations are a headache for example, AS & MR. Throw in some coronary pathology and the stage is set for an eventful case!

29
• Memory jogger: − Regurgitant lesions: Full, Fast & Forward − Stenotic lesions: Slow & Steady
• The patient with IHD: you already have your head around the balance of O2 supply &
demand from your regular lists. Unless the patient is acutely ischaemic or haemodynamically compromised, the general rule is that maintaining the patient’s haemodynamic state at baseline, day-to-day values patient is reasonably safe. If variation are required, gradual changes are better tolerated than sudden ones.
• Congenital lesions are infrequently seen at RMH. You may see the occasional ASD, bicuspid aortic valve for Ross in a young person, Marfans, or redo in young adult with past paediatric cardiac surgery. It is sensible to appreciate the basic concepts of: − Cyanotic and Non-cyanotic lesions − PDA − PFO / ASD − Tetralogy of Fallot − Non-cardiac surgery for the patient with a transplanted heart.
Appendix B: Anticipating the Surgical Steps
Cardiac anaesthesia must cope with a wide range in the degree of surgical stimulation, from intubation to prepping, from sternotomy to harvesting the LIMA. The surgeon is also uniquely prone to interfere with what we usually consider our exclusive territory – manipulation of the heart and great vessels can even result in transient circulatory arrest, and it is not uncommon for the surgeon to require prolonged periods of apnoea during the harvesting of the IMA. In general, it is better to anticipate rather than react to the results of these events. Failure to do so may result in rollercoaster haemodynamics: unanticipated surgical insult → precipitous physiological response → late response with over-correction on your part → physiological response requiring correction again → potential surgical sarcasm. On the other hand it is important not to over-anticipate; sometimes sitting tight is called for. Always have an eye on the surgical field (stand on a step if you need). There is no other way to put into context what you are seeing on your monitors.
STEP ACTION PRE-INDUCTION MANAGE ANXIETY INDUCTION CONTROL PRESSOR RESPONSE TO INTUBATION PREP/DRAPE ↓ ANAESTH DEPTH INCISION/STERNOTOMY ↑ ANAESTH DEPTH CARDIAC MANIPULATION SIT TIGHT! IMA HARVEST ↓ TV
100% O2 – LONG APNOEAS ↓ ANAESTH DEPTH HEPARIN READY (0.4 KIU / KG)
HEPARINISATION EXPECT ↓ BP CHECK ACT AFTER 3 MINS
EPIAORTIC SCAN HELP WITH IMAGE ACQUISITION AND INTERPRETATION AORTIC CANNULATION ↓ BP ~ 100/- FOR MOST SURGEONS ATRIAL PURSE-STRINGS LUNGS OFF FOR RETROGRADE SUTURE.
MAY PRECIPITATE AF.

30
CORONARY SINUS CANNULATION
IMAGE WITH TOE
POST-CANNULATION CHECK FOR AIR IN LINES; VOLUME OR PRESSOR FOR BP ON BYPASS (SEE SECTIONS SPECIFICALLY RELATING TO MANAGEMENT OF PT ON CPB)
LUNGS OFF MONITOR & VENTILATOR TO CPB MODE IV OFF GTN OFF PA CATHETER BACK CONFIRM ANAESTHESIA MAINTENANCE WITH PERFUSION
ANTEROGRADE C’PLEGIA MONITOR FOR LV DISTENSION DE-AIRING MANOEUVRES AS REQUIRED – MAY INCLUDE VENTILATION,
PARTIAL BYPASS, MOVING THE TABLE, ASSESSMENT OF RESIDUAL AIR WITH TOE
LUNG INFLATION (CARE WITH LIMA GRAFT – UNDER SURGEON’S SUPERVISION) DEFIBRILLATION 10 – 20 J; ANNOUNCE WHEN CHARGED; ZAP IMMEDIATELY ON
SURGEON’S “GO” PACING SEE PACING SECTION WEAN FROM BYPASS SEE COMING OFF BYPASS SECTION
MAINTAIN ANAESTHESIA DECANNULATION PRESSURE ↓ ~ 100/- PROTAMINE SUBJECT TO SURGICAL CLEARANCE:
10 – 20 MG AS TEST DOSE 1/3RD OF DOSE PRIOR TO AORTIC DECANNULATION REST OF DOSE AFTER AORTIC CANNULATION SITE SECURED
POST BYPASS CV CHANGES
VOLUME LOADING; PRESSORS; GTN FOR MAINTENANCE OF CIRCULATION; INOTROPES IN CONSULTATION WITH SURGEON
CHEST CLOSURE LUNGS DEFLATED FOR STERNAL APPROXIMATION EXPECT ↓ BP WITH ↑ MEAN INTRATHORACIC PRESSURE PARALYSIS
TRANSFER TO ICU SEE ICU MATTERS SECTION • Don’t forget that drugs – especially fentanyl – take a while to have their peak effect. With
a little effort it is possible to give the drug too late, resulting in ineffective control of the surgical stimulus, with subsequent hypotension.
• Tricks for ↓ BP acutely include: − GTN bolus (0.5 – 1.0 ml = 0.3 – 0.6 mg) − reverse Trendelenberg − ventricular pacing, if wires in-situ − phentolamine 0.5 - 1mg – like aramine in reverse − transiently increasing depth of anaesthesia
• If the lungs get in the way the surgeon may ask for deflation. With the lungs out of the way, there is nothing to remind the surgeon to permit ventilation again. Keep an eye on what they’re doing, and remind them that you need to ventilate when they’ve finished their lung-free delicate bit. Ensure apnoea or ventilator alarms are enabled to remind you to ventilate before embarrassment occurs.
• Things vary from case to case and from surgeon to surgeon, and the above list is not exhaustive. After doing a few of these lists, you’ll get into the swing of things and will anticipate well enough.
• Valve surgery is generally similar. Differences include: no vessel harvest → shorter pre-bypass period; TOE assessment focus on relevant valve/s; aggressive de-airing required.
Interpret all observations in the light of what the surgeon is doing. Anticipate and pre-empt but don’t over-react.
31
Appendix C: Cardio-pulmonary bypass
This is intended to complement the section on CPB in the main text. • Hopefully you have familiarised yourself with the bones of the CPB machine before your
first case. Here is a line diagram just in case any confusion remains:
• The machine is primed with ~ 2l of heparinised crystalloid or colloid. Blood prime is
occasionally used for small or anaemic patients. • Going on bypass:
− Aortic (ascending aorta) & venous cannulae (RA to IVC +/- SVC) in place. − Anterograde (ascending aorta below cross clamp) & retrograde cardioplegia cannula
(coronary sinus) are placed. − ACT checked. − Perfusionist gradually releases clamp on venous line. − Right heart return reduces as blood is diverted to the venous reservoir − The arterial pump returns this blood into the aorta, via the oxygenator / heat
exchanger − Right heart return & ejection fall. The left heart empties. − Ventricular ejection decreases. Pulsatility at this stage implies:
− obstruction of the venous line (may be deliberate) − significant aortic regurgitation − unusual things like PDA
− Flow ~ 2.4 – 3 l/min/m² − Pressure at 50-80mmHg
− hypotension lasting for a few minutes often occurs with running on. Large doses of metaraminol may be required to ↑ the BP
• Cross-clamping with cardioplegia is another separate step − some surgery can be performed on bypass with the heart still beating − renders the heart ischaemic and therefore the need for myocardial protection
− anterograde and retrograde cardioplegia
32
• Some real disasters can occur on bypass. “Clean kills in Perfusion” include:
− Massive air embolus − No oxygen in the oxygenator − No heparin. − Mechanical pump or circuit failure
• Get the perfusionist to show you the safety protocols that avoid these. • Review the plan for massive air embolus on pump (stop pump, steep Trendelenberg,
thiopentone, rapid cooling, de-air pump,? retrograde perfusion). Maintenance on CPB: • BP control: Pressure 50 – 80 mmHg. Some patients (e.g. impaired autoregulation,
diseased cerebral arteries) may need the pressure kept on the higher end. Managed by altering flow, administration of vasoactives and anaesthetic agents including opioids.
• ACT every 30min. > 480. More frequent if normothermic • Blood gases
− PaCO2 40mmHg – set by altering gas flow (“sweep”) through oxygenator − PaO2 > 100mmHg – set with O2 % through oxygenator − BE ≤ 2.5. Acidosis can be due to inadequate perfusion or poor distribution.
• Hb 7.5 – 10 g/dl • Temperature:
− Somewhat dependent on surgical philosophy − usually ~ 34ºC − 16-18ºC for deep hypothermic cardiac arrest (DHCA). − If DHCA, monitor 2 sites (usually nasopharynx & bladder), and be aware of
differentials between them. • ECG
− asystole is generally good − ventricular electrical activity signifies the need for repeat cardioplegia.
• Urine output: Oliguria (≤ 1ml/kg/hr) − Pump flow adequate? − MAP adequate?
• The above is managed by the perfusionist. Although you do not control the pump, being
ignorant to them is not kosher either. • During CPB, drugs are injected directly into the pump reservoir via the perfusionist. • At RMH, Bypass Time is useful for
− catching up on the paperwork − short tea break (or lunch) − getting the next patient around & plumbed
DHCA: • Infrequent – several cases per year, mostly for aortic arch work (dissections etc) • Meticulous glucose control required to ↓ risk of neurological injury • Slow rewarming – no more than 1ºC core temp per 3min. • Stop rewarming at core temp. of 36-37ºC • These patients bleed and will usually get aprotinin tranexamic acid and generally need
platelets & factors, sometimes even Novo 7 • These operations are subject to meticulous planning; where possible, anterograde or
retrograde cerebral perfusion is used to minimise cerebral ischaemic time. Adverse effects of CPB: General: loss of pulsatile perfusion → peripheral perfusion mismatch CNS: micro & macro emboli

33
Resp: ↓ blood flow; deflation / atelectasis → impaired gas exchange mechanics circulating mediators → ↑ capillary permeability → ↑ extravascular lung water Systemic: Activation of humoral cascades (coag, fibrinolytic, complement, kallikrein) → SIRS Haematological: dilutional anaemia; platelet activation & dysfunction. DIC Endocrine: ↑ catecholamines, “stress hormones”; hyperglycaemia GIT: ↓ splanchic blood flow; ↓ gastric pH; endotoxaemia Renal: ↓ tubular function
Appendix D: Drugs
There is ongoing evolution in cardiac anaesthetic practice; in particular, there is presently a mixed view of TIVA with propofol, and volatile-based techniques are becoming more common. The drug layout in the drawers is somewhat different in the cardiac theatres. Take particular care that you are drawing up the correct drug!! Reminder: parecoxib is specifically contraindicated in CABG surgery! Drugs and preferred concentrations vary, but in general: Standard Anaesthetic Drugs fentanyl 500 – 1500 mcg undiluted in 10 ml syringe morphine 10 – 20 mg diluted to 1mg/ml midazolam 5mg undiluted rocuronium 50 – 100 mg red syringe or 10 ml syringe pancuronium 8 mg red syringe Make BP More Bigger metaraminol 10 mg diluted to 20ml → 0.5 mg/ml phenylephrine 10 mg diluted to 50 – 100 ml ephedrine 30 mg diluted to 10ml → 3 mg/ml Make BP Less Bigger
phentolamine 10 mg diluted to 1mg/ml in 10 ml syringe 0.5 – 1 mg prn
Bypass management heparin15 30 kIU undiluted in 35 ml syringe
protamine 300 – 400 mg; equal to the original heparin dose test dose (10 – 20 mg) after surgical clearance then
⅓rd total dose @ 25 - 30 mg/min then remainder after aortic cannulation site has been secured.
15 For the purposes of calculating the protamine dose: heparin activity is approx 80 U/mg. If a reference to mg is made, this is generally rounded to 100 U/mg. Thus if “300mg heparin” is given, it really means 30 kIU, actually closer to 375mg. Partly for this reason, it is common to bump the protamine dose a little.

34
Other routine / semi-routine drugs GTN 50 mg / 83 ml IMED pump 1 ml / hr ≡ 10 mcg / min insulin 50 U / 50ml
Antibiotics flucloxacillin 2 g slow IV vancomycin 1 g v slow IV ceftriaxone 1 g (VIDS approval or approved indication) gentamicin 3 mg / kg slow IV Most cases: fluclox & genta. Vanco replaces fluclox if allergic or inpatient. Ceftriaxone replaces genta in renal impairment and for Ross procedure. Antithrombolytics – case by case basis aprotinin 1 MU / 100 ml IMED pump 1 ml test dose then 200 ml IV, 200 ml into pump prime, 50 ml / hr until chest closure TXA 2.5 g undiluted in 20 ml syringe 1 g with sternotomy then 0.5 g/hr Fill in IPU form! Other infusions Almost any drug may be required on short notice – either: use the official ICU protocols if they are known (see wall chart) or: use a generic formula such as 6mg / 100 ml (or equivalent)
Appendix E: IABP
The correctly adjusted intra-aortic balloon pump augments systemic diastolic pressure and reduces afterload. It is used in unstable coronary syndromes where other available techniques have failed to control ischaemia. Occasionally it is commenced intraoperatively, when LV performance is poor, to facilitate weaning from CPB or reduce inotrope requirements. In general, where the IABP has been established pre-operatively, it is continued postoperatively even though the indication (e.g. ischaemia) has been addressed. General principles: • Inflates in diastole, boosting diastolic pressure, typically to levels above those generated
by the heart in systole − “systolic” pressure on monitor is actually the augmented diastolic pressure.
• Deflates in systole, reducing the pressure load on the LV during ejection • Improves coronary perfusion & LV performance. • Serves to decouple myocardial perfusion from myocardial performance IABP system • console, with tubing and monitoring connections to the patient. The IABP itself consists
of a multilumen catheter with a 20-40ml balloon. • Catheter size selected according to patient size. • Console incorporates ECG and pressure monitoring
− adjustable parameters include inflation/deflation fine-tuning, augmentation volume, assist ratio, alarm limits.

35
• Uses helium for inflation because of its favourable flow (low density) characteristics. Insertion • Either in the cath lab by a cardiologist and cardiac tech, or by the surgeon in theatre, with
the adjustments made by the perfusionist. You may be part of the decision-making process (and may have to look after it in ICU on your ICU rotation), so it is worth becoming familiar with the controls & principles.
• Placed in the descending aorta, under fluoroscopic or TOE guidance. The tip of the catheters should be just distal to the left subclavian artery.
• Modern catheters usually sheathless, inserted by cut-down or percutaneous (Seldinger) technique.
Timing • Usually automatic. Some manual adjustment may be possible/required. • Rapidly inflated during early diastole by the console • Timing is usually by ECG, modern machines can also use the pressure signal and
autoselect the best trigger − tachycardia, AF reduce efficiency of augmentation − diathermy can be a problem in the operating theatre → pressure trigger − beware inadvertent disconnection of IABP ECG when setting up a case
• may need to set up ‘slave’ cable from anaesthetic monitor if IABP inserted during case in theatre. − Mistiming can increase the workload on the heart − Careful attention to balloon synchronisation with ECG and arterial wave.
− Inflation: occurs just following the dicrotic notch and results in a distinct M wave on the arterial tracing.
− Deflation: should precede ejection so that a distinct diastole is evident. • Setting the balloon to inflate every other beat (2:1), may help with adjustment of timing,
after which 1:1 assistance can be resumed. Indications: • unstable coronary syndromes unresponsive to medical therapy • cardiogenic shock • acute LV failure (less useful than VAD) Absolute contra-indication: • Aortic dissection Relative contra-indications: • moderate to severe aortic regurgitation • severe aortic atheroma • severe peripheral vascular disease Risks / Complications include • aortic damage/dissection • embolic complications including CVA • limb ischaemia (relating to the insertion site)
• IABP is only a short-term solution and should not be considered for the patient with
irreversible cardiogenic shock. It is a temporising measure to get the patient to surgery or to get the patient off CPB and give the myocardium a chance to recover.
• For severe LV failure (failure to wean despite IABP and inotropes) LVAD may be required (if patient considered salvageable), and can serve as a bridge-to-transplant.
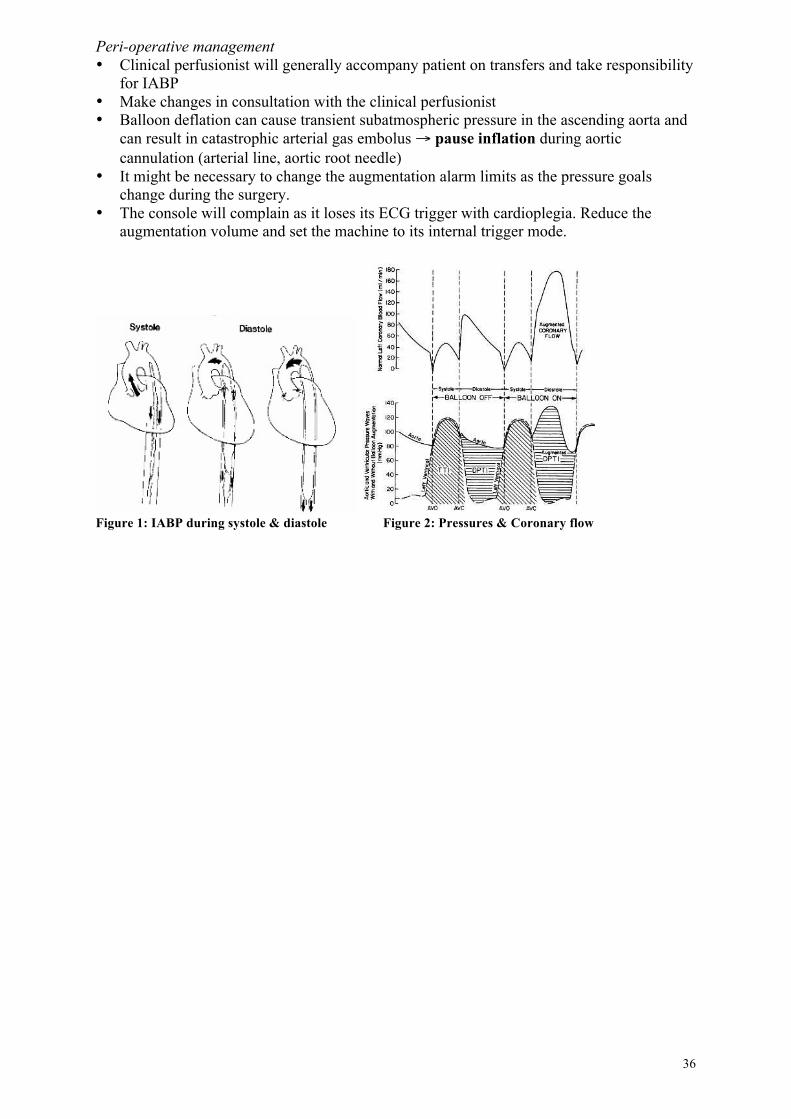
36
Peri-operative management • Clinical perfusionist will generally accompany patient on transfers and take responsibility
for IABP • Make changes in consultation with the clinical perfusionist • Balloon deflation can cause transient subatmospheric pressure in the ascending aorta and
can result in catastrophic arterial gas embolus → pause inflation during aortic cannulation (arterial line, aortic root needle)
• It might be necessary to change the augmentation alarm limits as the pressure goals change during the surgery.
• The console will complain as it loses its ECG trigger with cardioplegia. Reduce the augmentation volume and set the machine to its internal trigger mode.
Figure 1: IABP during systole & diastole Figure 2: Pressures & Coronary flow
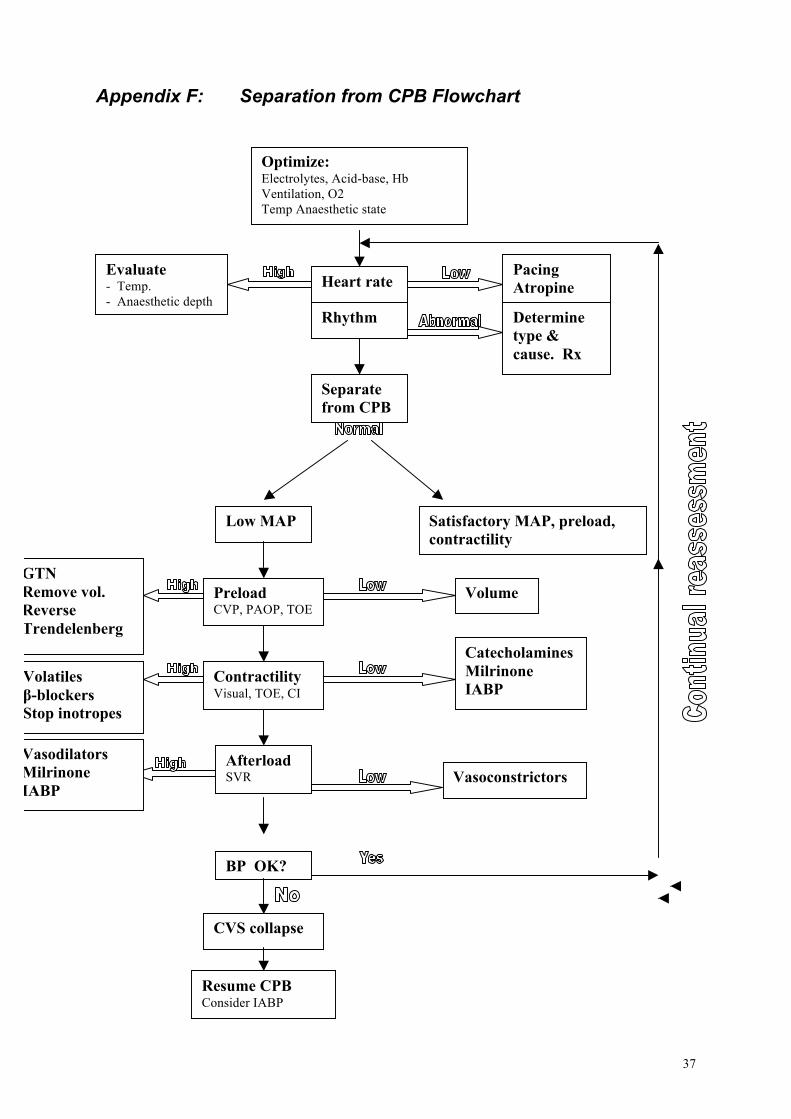
37
Appendix F: Separation from CPB Flowchart
Low MAP
Preload CVP, PAOP, TOE
Contractility Visual, TOE, CI
Satisfactory MAP, preload, contractility
Volume
Catecholamines Milrinone IABP
Afterload SVR Vasoconstrictors
Heart rate Rhythm
Separate from CPB
Pacing Atropine
Determine type & cause. Rx
Evaluate - Temp. - Anaesthetic depth
Optimize: Electrolytes, Acid-base, Hb Ventilation, O2 Temp Anaesthetic state
BP OK?
CVS collapse
Resume CPB Consider IABP
GTN Remove vol. Reverse Trendelenberg
Vasodilators Milrinone IABP
Volatiles β-blockers Stop inotropes

38
Appendix G: Eponyms
Surgeons fear obscurity. They can die happy if they have something named after them16. They learn and earnestly use eponymous terms in the hope and expectation that one day their own idiosyncrasies will likewise be propagated along the sewers of time. Here, for the rest of us, is what I’ve been able to make out of their incoherent ramblings: Ross Procedure: aortic autograft and pulmonary homograft. The native pulmonary valve is transferred into the aortic position. The coronaries are re-implanted. Somebody’s spare pulmonary valve is implanted to replace the missing valve. Long case. Bentall’s [operation]: compound aortic valve & ascending aorta replacement, often using a valved conduit (big piece of dacron graft with a prosthetic aortic valve at the bottom end). Requires re-implanting the coronary arteries. Moderately long case. David Procedure: Like a Bentall’s, but without the AVR part. Still requires reimplantation of the coronaries. O’Brien [valve]: stentless aortic valve replacement. Complicated way of doing an AVR. Alfieri [suture]: technique for mitral valve repair. A cunningly placed stitch converts MR into MS. Generally combined with other methods of repair (annuloplasty, etc). Occasionally seen at RMH (survivors of surgery for congenital conditions): Fontan procedure (rarely performed in adults; Fontan physiology refers to a patient who has had a Fontan procedure or who has an equivalent physiological state): bypassing the right ventricle so that systemic venous return is diverted directly to the pulmonary arteries. Often the SVC is attached to the right pulmonary artery, and the right atrium (minus the SVC) is attached to the main pulmonary artery (therefore flowing to the left lung). Avoid situations that cause increased pulmonary vascular resistance; IPPV will be tolerated better than hypoxia or hypercarbia, but minimise airway pressures. Keep fluids up. Norwood: for hypoplastic left heart – essentially, attaching part of the RV outflow to the aorta. If all of the RV outflow is diverted to the systemic circulation, the patient ends up with Fontan physiology. Rastelli: internal Gore-Tex baffle placed to divert oxygenated blood to the aorta, etc. Used in various forms of scrambled heart. Rarely seen at RMH (obsolete, done elsewhere, etc): Blalock (-Taussig) Shunt: aorto-pulmonary shunt, now often done utilising a synthetic conduit between the distal aortic arch or its branches, and the left pulmonary artery. Performed in infancy to improve pulmonary blood flow in many cyanotic congenital cardiac conditions.
16 Not wanting to encourage them, I’ve made no attempt to find out who any of these people are, except that Taussig was a cardiologist, and not a surgeon.
39
Gott shunt: heparin-bonded shunt bypassing the operative site of the descending thoracic aorta. Rare because cardiothoracic surgeons would use pump-oxygenator; vascular surgeons would use a stent. Glenn (bi-directional) shunt: kind of a half-Fontan, used in single-ventricle situations. The SVC is plugged into the R PA and the main PA is ligated. Results in low pulmonary flows (only the SVC return), which is advantageous if pulmonary vascular resistance is high, as in early infancy. Can be later converted to a Fontan. Mustard procedure: atrial baffle used for transposition of the great arteries (TGA). It leaves the arteries transposed, but diverts systemic venous return to the lungs via the LV. The RV perfuses the body and can eventually fail. Obsolete – most patients now have an arterial switch instead, which gives the patient a normal circulation. Maze operation: series of incisions made into the atria, intended to control AF by preventing free propagation of the action potential. Made largely obsolete by percutaneous techniques (pulmonary vein isolation) in the EP lab. … And a few eponymous conditions: Ebstein’s anomaly: the tricuspid leaflets are displaced towards the apex of the RV, leaving an inadequate RV cavity (much of the RV cavity is ‘atrialised’). The patient has poor exercise tolerance because their RV output is limited. May present in adulthood for tricuspid valve surgery. Fallot’s tetralogy, the classic cyanotic congenital cardiac condition, occasionally surviving into adulthood (more so now that repairs are done in early childhood): VSD, ‘overriding’ aorta (collects output from both ventricles), pulmonary stenosis, RV hypertrophy. Patients will often have had complete repair, but some patients have had partial repairs or symptomatic relief with a Blalock shunt.