risk factor reduction - heart group gp talks... · ~80% of cvd attributable to preventable risk ......
TRANSCRIPT

Risk factor reduction
AHG symposium,2014
Dr Niels van Pelt

Cardiovascular disease- single most common
cause of death in NZ men and women...’leading
cause of death world wide and respects no
borders’(WHO)
~80% of CVD attributable to preventable risk
factors
CVD is often preventable (or at least deferred)

Steve is 57 yr old accountant. He jogs regularly
and is well
He smokes (especially if stressed at work), TC
4.65 mmmol/L, HDL 0.9, LDL 3, TG 1.7 and
TC/HDL ratio 5.2. His BP is 130/85, BMI 25 and
blood glucose is normal. Both parents have
hypertension.
A
case...


AHA/ACC published new guidelines in Circulation
2013- treatment of cholesterol to reduce
atherosclerotic cardiovascular risk in adults
They also developed a new risk calculator, using
a number of longitudinal studies, designed to be
more representative of the US population
The RAWG risk calculator assesses Steves 10
year risk at 10.9%

Framingham risk model over estimated risk in the
low risk and underestimates risk in high risk
groups (elderly, maori) in NZ
Predict database actively recruiting - will lead to a
more accurate NZ based risk assessment tool

What are the new ACC/AHA recommendations
statin therapy recommended for primary
prevention
for persons with LDL >4.9 mmol/L
for patients with diabetes if LDL >1.8 mmol/L
if the 10 year risk is >7.5% (using the RAWG
calculator) and LDL is >1.8 mmol/L
Monitoring of cholesterol levels on statins is not
recommended
Low/moderate/high intensity therapy


why changes in the recommendations?
lack of evidence of specific targets such as
LDL<1.8mmol/L
reduced adherence and concern about side effects
if treatment intensified to meet targets ( note small
risk of developing type 2 DM, increased risk of
myopathy with higher doses)
but actual number treated with statins is increased

Should Steve receive a statin?
a) Start atorvastatin now (as recommended by
ACC/AHA guideline)
b) Start a fibrate
c) Lifestyle modification (particularly smoking
cessation) and review need for statins in 6-12
months
d) Start statin and aspirin

Steve is at moderate (to high) risk at 14% 5 year
risk for MI, stroke- is any intervention required?
From June 2012-13, 588 patients<60yrs presented with first MI at MMH
30% diabetes, 40 % current smoker
The ‘average’ risk profile for MMH patients presenting with MI <60yrs is 12% five year risk-make up approx 50% of the patients
Intervention in Steve’s case is indicated

90% of ‘young’ people(<45yrs) who have a heart attack are smokers
smoking is the most important life style factor and cessation is most effective lifestyle intervention

Difficult to achieve- approx 50% smokers stop
after acute MI

Steve’s risk after 12 months of smoking
cessation

Physical activity
In healthy subjects physical activity and cardiac
fitness associated with up to 25-30% reduction
in CVD mortality
similar observations in secondary prevention
lifestyle interventions under utilised and success
in maintaining exercise variable
in established CVD <50% of people achieve
lifestyle goals- in primary prevention this is
even less
Successful lifestyle changes requires
motivated, informed person with good support
from GP and ‘health’ team’

12% relative reduction in major cardiovascular
events (primary prevention)
probably balanced by the small increase in
bleeding risk- aspirin not generally
recommended for primary prevention

Fibrates?- bezofibrate or gemfibrozil
No definite role in primary prevention, unless
diabetic patients with significant dyslipidaemia
(low HDL)
Accord study 2010 suggested small benefit in
this group

low HDL is probably not causal but associated
with other risk factors (metabolic syndrome)

Gemfibrozil significantly reduced events
(secondary prevention)
My approach with Steve
strongly encourage smoking cessation
review progress over the next 6-12 months- if stops
smoking risk is in low to intermediate range and
statins not required
if still smoking , then reasonable to reduce risk by
adding statin..if Steve concerned about long term
statin then reasonable to perform CT calcium score
to aid management

I often start atorvastatin at 20mg once a day
(moderate intensity) for primary prevention.
In secondary prevention atorvastatin 40-80mg
If side effects (myalgia) reduce dose, consider
alternate days, trial rosuvastatin
I don’t use ezetimibe

Steve’s case appeared recently in NEJM
Readers were given 3 options and polled
(n=1600)
not starting statin- 57%
starting statin and monitoring LDL-26%
starting statin and not monitoring LDL-17%

Maybe we should measure his lipoprotein a
level?
Lp(a) consists of cholesterol laden LDL particle
bound to plasminogen like glycoprotein
apolipoprotein(a)

Lp(a) levels are determined by LPA gene coding
for apolipoprotein(a)

Kringle IV type polymorphisms strongly
associated with Lp(a) levels
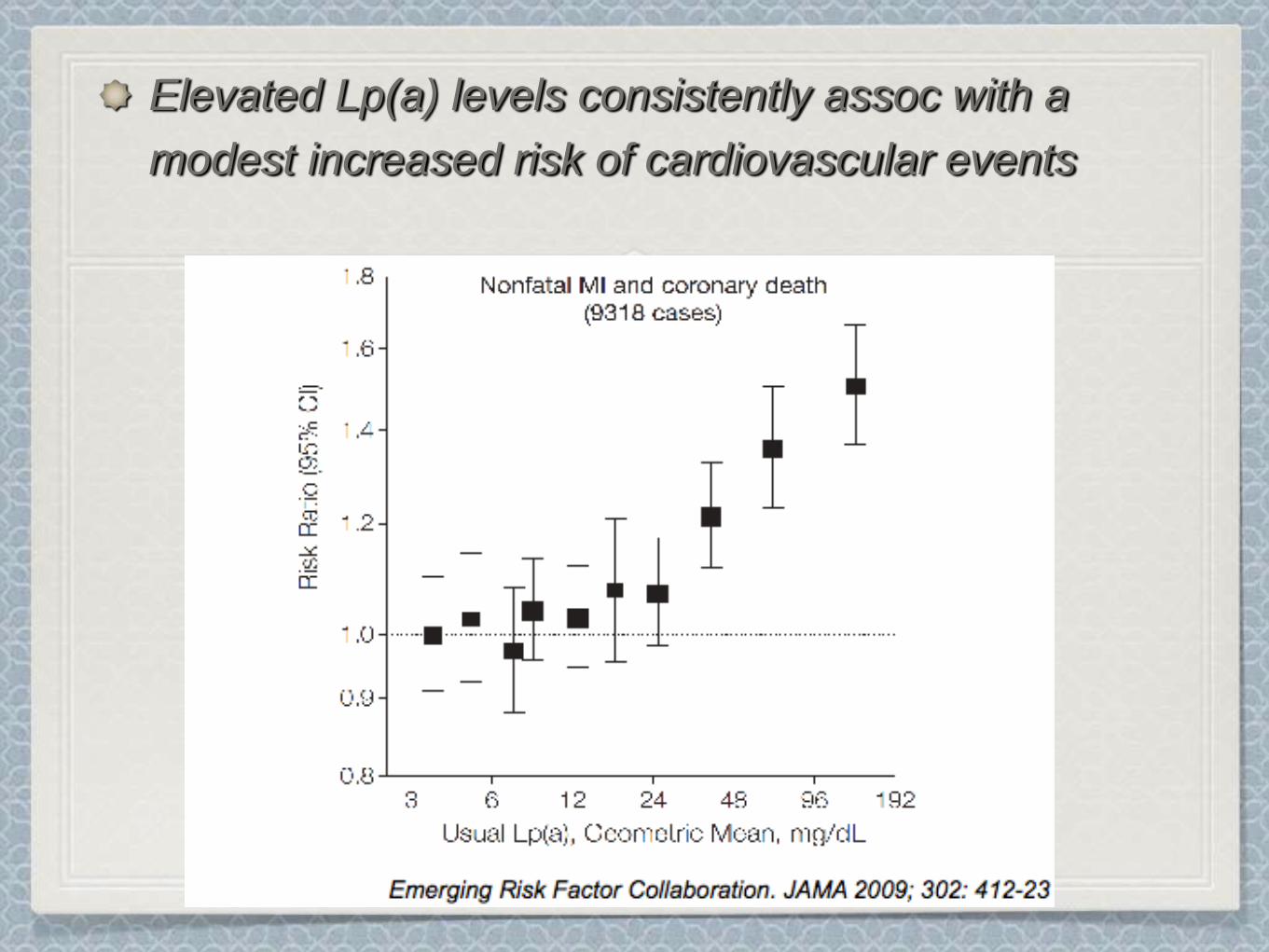
Elevated Lp(a) levels consistently assoc with a
modest increased risk of cardiovascular events

there are 3 factors
increased Lp(a) levels are associated with increased CVD risk
Kringle IV type 2 polymorphisms assoc with increased Lp(a) levels
Kringle IV type 2 polymorphisms assoc with increased CVD risk
Strongly suggests Lp(a) is a strong, independent risk factor


Should we measure Lp(a)?
no consistent assays and risk assoc is modest
but consider in patients who have CV events
when seemingly at low risk, those with strong
family history and those at intermediate risk
a high level (>50 mg/dl) may reclassify patients
to high risk and prompt more aggressive risk
reduction (BP, LDL)
Niacin (fibrates) reduces Lp(a) levels- but no
evidence yet that CVD events reduced

QuickTime™ and aYUV420 codec decompressor
are needed to see this picture.

Final comments
Risk assessment and risk reduction is
mandatory
Patients risk can be simply and effectively
reduced by lifestyle factors and when
appropriate drug therapy
Any statin is better than none- long term
adherence is the key


Professor Rod Jackson, School of Population Health ,
University of Auckland
NTT=59