rights / license: research collection in copyright - non ...48237/... · usability and effects of...
TRANSCRIPT

Research Collection
Doctoral Thesis
Using virtual reality as a home-based stroke rehabilitationapproach
Author(s): Wüest, Seline
Publication Date: 2015
Permanent Link: https://doi.org/10.3929/ethz-a-010546679
Rights / License: In Copyright - Non-Commercial Use Permitted
This page was generated automatically upon download from the ETH Zurich Research Collection. For moreinformation please consult the Terms of use.
ETH Library

USING VIRTUAL REALITY AS A HOME-BASED STROKE REHABILITATION APPROACH—
Seline Wüest

DISS.ETHNO.22848
USINGVIRTUALREALITYASAHOME-BASED
STROKEREHABILITATIONAPPROACH
Athesissubmittedtoattainthedegreeof
DOCTOROFSCIENCESofETHZURICH
(Dr.sc.ETHZurich)
presentedby
SELINEWÜEST
MScETHinHMS
bornon01-02-1985
citizenofGrosswangen(Lucerne)
acceptedontherecommendationof
PDDr.ElingD.deBruinProf.Dr.DavidP.Wolfer
2015

TableofContents
1Prologue 1–112Computationalintelligenceandgamedesignforeffectiveat-homestroke 12–27rehabilitationGamesforHealthJournal2013;2(2):81-883Designconsiderationsforatheory-drivenexergame-basedrehabilitation 28–47programtoimprovewalkingofpersonswithstrokeEuropeanReviewofAgingandPhysicalActivity2014;11(2):119-1294Usabilityandeffectsofanexergame-basedbalancetrainingprogram 48–66GamesforHealthJournal2014;3(2):106-1145Reliabilityandvalidityoftheinertialsensor-basedTimedUpandGotestin 67–95post-strokeindividualsJournalofRehabilitationResearch&Development2015,inpress6Epilogue 96–107Summary/Zusammenfassung 108–114DanksagungenCurriculumvitae

1
1
Prologue

2
Stroke is a centralnervous systempathology that theWorldHealthOrganization (WHO)definesas “a
clinical syndrome, of presumed vascular origin, typified by rapidly developing signs of focal or global
disturbanceofcerebralfunctions”[1].Thesymptomsofstrokepersistformorethan24hoursandmight
leadtodeath[1].Astrokeoccurswhenbloodsupplytothebrainisinterrupted,damagingaffectedbrain
areas. The resulting loss of brain function commonly implies serious cognitive, visual and motor
complaintsinthosesurvivingastroke[2].Withover15millionoccurrenceseachyear,strokeconstitutes
one of themost important causes of death and disability [3] and can be said to be one of themost
devastating diseases worldwide [4]. The concern over stroke becomes even more pressing if one
considers thedemographic changes thatarecurrently leading toaneverhigherquotaofpeopleaged
65+: Stroke is bothmost prevalent andmost devastating in this age group. According to theWHO’s
Europeanpopulationprojections,thenumberofnewstrokeeventseveryyearisestimatedtoincrease
from1.1millionin2000tomorethan1.5millionin2050solelyduetodemographicshiftstowardsolder
populations[5].
Given this shift, stroke rehabilitation should be a primary focus of attention in stroke research. The
present doctoral thesis represents an effort to improve long-term stroke rehabilitation. Its main
hypothesis is that home-based stroke rehabilitation programs specifically targeting balance have the
potentialtosupportrecoveryoflocomotorfunction–oneofthemostimportantdeterminantsofquality
oflifeafterstroke.
1.1Stroke-inducedmotordeficits
Large research efforts are directed at the prevention of stroke. Here the primary focus is on lifestyle
factorsrelatedtostrokerisk.However,becausetheaforementioneddemographicdevelopment istoa
largeextentgiven,strokerehabilitationisanimportantlineofattackaswell.Althoughstrokecausesa
widerangeofproblems(e.g.,pain,memoryproblems,speechimpairments, lossofvision,alteredlevel
of consciousness), patients often express impaired locomotor function as a main cause of decreased
qualityoflife.Thelossoflocomotorfunctionisoftencausedbystroke-inducedhemiparesis–aone-side
partiallossofmotorfunction[6-7].Ithasbeennoticedthatalargeproportionofhemiparalizedpatients
showdiminishedbalanceskillsandadeviatedwalkingpattern [8-10] involvingreducedwalkingspeed,
cadence, stride length and an increased left-right asymmetry: so-called ‘hemiparetic gait’. Not
surprisingly,thereisagreatneedinstrokerehabilitationtoachieveahighlevelofwalkingskillsaimedat
regaining independence in walking. In this context balance, endurance, muscle strength and motor

3
coordinationarekeycontributingfactorsaffectingstrokepatients’walkingfunction[11-13].Sincegood
balance iswidelyconsideredasan indispensableprerequisite fornormalwalking[14-15], the focuson
balance in rehabilitative interventions seems mandatory. Accordingly, a therapy program targeting
balanceshouldconstituteapromisingapproachtoimprovewalking–andhencequalityoflife–instroke
survivors.
Alargeliteraturebodyexistssuggestingthattheinitialrecoveryperiodafterstrokeisthemostsensitive
phaseintermsofmotordeficitrestoration[16-17].Specifically,thefirstthreemonthsofrehabilitation
seem critical formotor recovery after stroke [18].Nevertheless, there is an increased awareness that
meaningful improvementscanstillbeachievedinthelaterphasesofrehabilitation[18].Consequently,
strokerehabilitationshouldnotberestrictedtoonlytheinitialperiodfollowingstroke;itwillhavetobe
continued on a long-term basis. Since the treatment of stroke sufferers in hospitals or specialized
rehabilitation units is expensive and hence places a large burden on theNationalHealth Service, it is
oftennotfeasibletoextendthelengthofstayinrehabilitationfacilities.Consequently,forbestrecovery
results,long-termandcost-effective(i.e.,largelyautonomous)rehabilitationisneededafterpatientsare
dischargedfromrehabilitationfacilities.
In what follows, the development of a treatment approach that enables long-term rehabilitation for
strokepatientsdischargedfromhospitalsorrehabilitationunitswillbepresented.Thisdoctoralthesisis
basedonresearcheffortswithintheproject‘RehabilitativeWayoutInResponsivehomeEnvironments’
(REWIRE) [19] funded by the European Commission under the FP7 framework. As such, the idea that
strokesufferersmightbenefitfromanintensivehome-therapyprogramusingvirtualreality(VR)formed
thegeneralframeworkforthisdoctoralthesis.
1.2Virtualrealityforrehabilitation
BecauserecentliteratureexposedavarietyofbenefitsassociatedwiththeuseofVRinhealthcare,this
technologyhasbecomeagrowingareawithin rehabilitation interventions [20-21].Apotent featureof
VRisitsgreatpotentialtocreateawidevarietyofrealisticscenariosadaptedtopatients’characteristics
and needs. By simulating interactive environments, rehabilitation practice under controlled and safe
conditionsisprovided.Afterall,avirtualenvironmentcanbecontrolledmoreeasilythanarealone,and
anyaccidentswillmerelybevirtualaswell.Furthermore,VRseemstofarewell intermsofmotivating

4
patientsforrehabilitationandbetterengagingtheminthetreatmentplan[20,22-25].Thiswill leadto
improvedcontinuity,whichinturnpositivelyimpactsrecovery[26].
Thegamingindustryhasrecentlyprovidedasetofmodernlow-cost,VR-basedgamingconsoles(i.e.,the
NintendoWii,theSonyPlayStation,andMicrosoftX-box)thatallowmotion-controlledinteractionswith
thesystem.Byreliablytrackingandrespondingtousers’naturalbodymovements,thesecommercially
available gaming consoles have revolutionized the way videogames are played. Videogames have
become more intuitive and, thereby, more accessible to a wider audience [27]. As such, they have
become a source of inspiration for health care researchers and sparked the introduction of a novel
gaming approachwithin rehabilitation interventions. In one study, the commercial VR gaming system
NintendoWiiFitwasusedasabalancetrainingtoolforolderadults[28].Thestudyincluded12healthy
participantsaged53to91yearswithahistoryoffallsandreportedimprovementsinbalancefollowing
use of the Wii Fit system. The actual clinical effect induced by Wii Fit training in the presence of
pathologies, however, remains speculative. A study by Deutsch et al. [29] suggested that VR-based
approacheshavegreatpotentialtopositivelyaffectrehabilitation.A13-years-oldpatientdiagnosedwith
cerebral palsywas included in this study. The training intervention consisted of playing commercially
available games provided by the Nintendo Wii Fit sports software and resulted in positive therapy
outcomes[29].Similarly,astudyperformedbyFlynnetal.[30]appliedalow-costcommerciallyavailable
gaming platform to promote the post-stroke recovery process. The study intervention included the
PlayStation2Eyetoysoftwarewhichconsistedof23differentvideogames.Flynnetal.[30]reportedthat
VRcreatedanengagingandmotivatingtherapysituationand,moreimportantly,thatthegamingsystem
beneficially impacted the recovery process andwas able to reduce functional impairments stemming
from stroke [30]. This study had one substantial limitation though: Based on participant’s feedback,
some of the PlayStation 2 Eyetoy games were perceived as too complex for the use by functionally
impaired individuals [30]. Therefore, the authors emphasized the need for customization in order to
optimallyaddresstherapeuticneeds.Thisdrawbackisnotsurprising,giventhatthePlayStation2gaming
systemwas (and is stillbeing)developed for the leisure industry. In linewith the resultofFlynnetal.
[30], several other studies highlighted that videogames designed for entertainment rather than
therapeuticpurposesarenotperfectlysuitablefortheuseinrehabilitation[3,24,31-32].Inall,thereis
clearlyaplaceforVR-basedsystemsinrehabilitation,butthesesystemsmustbetailoredtothecognitive
andphysicalconstraints–aswellasthetreatmentgoals–ofthetargetpopulation.

5
Recently, the development of such tailored videogames has begun. For example, the VR-based
RehabilitationGamingSystem(RGS)proposedbyCameirãoetal.[33]focusedonthetreatmentofupper
extremity disorders following stroke. Likewise, the ongoing EU funded project FITREHAB [34] aims at
developingaVR-based rehabilitationand trainingplatform toprovidea customizedexerciseprogram.
Althoughthis isdefinitelyawelcomedevelopment,wefeelthatthesepioneeringstudiessufferfroma
lackoftightcooperationbetweenrehabilitationspecialistsandgamedevelopers.Moreconcretely,since
establishedgamedesignprincipleswere largelyunheeded, ratherboringandunattractivevideogames
resulted, which arguably lessened the aforementionedmotivationalmerit of the gaming approach to
rehabilitation. Importantly, rehabilitation games should not only be tailored to therapeutic goals in
which both therapist and patient needs are explicitly considered, but also be based on fundamental
gamedesignprinciplesmakingvideogamesfascinatingand,thereby,rehabilitationmoreengaging.
1.3Gentile’smotorskilltaxonomyforrehabilitation
Strongevidenceexists thataneffective therapyprogram in rehabilitation shouldbe theory-basedand
guidedbyestablishedmotorlearningprinciples[35-39].Foursuchprinciplesaretask-specificity[40-42],
highrepetitionintensity[43],variablepractice [44-48]andprogression[49-50],allofwhichpromisean
increased motor recovery effect and hence serve to ground a physical rehabilitation program
theoretically.However,severalresearchershaverecognized–andcriticized–theabsenceofapractical
framework within which such principled training programs can be developed.What is required is an
adequate template to createagraduallyprogressing rehabilitationprogram including task-relatedand
variabletrainingexercises.Gentile’staxonomy–aclassificationsystemtodifferentiatemotorskills[51]
– provides just such a template and hence constitutes a practical tool for developing theory-based
trainingprograms.Inthefollowing,IwilldescribeGentile’staxonomyinmoredetail.
Gentile posits that anymotor skill can be specified according to two general dimensions; namely the
skill’senvironmentalcontextandtheskill’sfunction[51-52].Shesubsequentlydivideseachofthesetwo
orthogonaldimensions(i.e.,environmentalcontextandactionfunction)intofourdiscretelevelssothat
they form a 4x4-table of 16 so-called skill categories (see Table 3.1, Chapter 3). This table of skill
categoriesformsthebasicframeworkofthetaxonomy.
Within the firstdimension (environmentalcontext), the four levelsaredefinedwithtwo indicators: (a)
regulatory conditions (i.e., relevantobjectsorpeople influencingaperson’s skill performance)and (b)
intertrialvariability.Theregulatoryconditionscaneitherbestationary(stationaryregulatoryconditions)

6
or in motion (in-motion regulatory conditions) and these, hence, represent the first two levels of
environmental context. Indicator (b) then furtherdivideseachof these levels according towhetheror
not these regulatoryconditionsvary fromtrial to trial: intertrial variabilityandno intertrial variability,
respectively.
Theseconddimension(actionfunction)alsoconsiderstwoindicators:(a)bodyorientationand(b)object
manipulation.Thetermbodyorientation indicateswhetherachangeinbodylocationisrequired(body
transport)ornot(bodystability)inordertoperformaskillsuccessfully.Thisindicatorformsthefirsttwo
levelsofactionfunction.Indicator(b)thenfurtherdivideseachoftheselevelsaccordingtowhetheror
nottheskillrequiresobjectmanipulation:objectmanipulationandnoobjectmanipulation,respectively
(seeTable3.1,Chapter3).
Gentile’s structured differentiation of 16 skill categories is simple yet accommodates all four training
principlesmentioned above: It ensures (1) variable practicebecause each of the 16 skill categories is
characterized by unique features and (2) systematicprogressionbecause difficulty increases from the
top left to lower right taxonomy corner. Furthermore, it allows for the flexible definition of (3) task-
specific skill practice and (4) high repetition intensity. These favorable characteristics instigated the
developmentofavirtualrehabilitationapproachbasedonthetaxonomyproposedbyGentile.
1.4TheinstrumentedTimedUpandGotestforrehabilitationefficacyassessment
Monitoring activities performed by individuals with chronic conditions (e.g., stroke) participating in
home-based treatment programs has been considered a matter of paramount importance [53]. A
valuabletoolforthecliniciansindiseasemanagementwouldbetheuseofwearablesensortechnology
toautomateclinical testingprocedures [53].Thepatientscouldbeable toperformtheclinical testing
procedures independently at home. This would make the regular assessment of the effectiveness of
home-basedrehabilitationinterventionspossible.Well-establishedtoolsformotorfunctionassessment
are,therefore,neededtooptimize–foreachindividualpatient–monitoringofthechangeprocessafter
stroke.Onefundamentalpreconditionofsuchatool isthefulfillmentofreliabilityandvaliditycriteria.
Moreover, in a training program focusing on regaining normal walking function, the assessment tool
shoulddetectbalanceandmobility impairmentswithhighsensitivitysothat interventioneffectiveness
canbeadequatelyevaluated.TheTimedUpandGotest(TUG)hasbeenshowntomeetallthosecriteria
[54-57]andhenceitcomesatnosurprisethatitisoneofthemostfrequentlyusedmotorfunctiontests

7
inthestrokepopulation[54,58-59].TheTUGdoes,however,havethedrawbackoffocusingonlyonthe
singleoutcomeparameter ‘time’neededtocompletetheentire testprocedure [57,60].Furthermore,
the TUG procedure is only considered as a whole and does not allow separate analysis of the
subcomponentsincludedinthetest(i.e.,sit-to-walk,gait,turningandturn-to-sit)[57,60].
In order to overcome the limitations associated with the original test protocol, the TUG has been
‘instrumented’ in the sense that small inertial sensors are strategically placed on patients’ bodies. By
means of these sensors,many additional gait- and transition-related outcomes can be revealed [60].
Previous studiesdemonstrated that this so-called instrumentedTUG (iTUG) is a reliable and valid gait
analysissysteminbothhealthypeopleandsubjectswithParkinson’sdisease(PD).Althoughthisclearly
renderstheiTUGapromisingtoolinclinicalpractice[57,60],itsreliabilityandvalidityasabalanceand
mobilityassessmenttoolinpeoplewithstroke-inducedmotordeficitsremainstobeconfirmed.
1.5Theaimandscopeofthisdoctoralthesis
Overall,thepresentthesisattemptstodevelopandevaluateatreatmentapproachusingVRforat-home
rehabilitation following stroke. The thesis focuses on the development and testing of VR-based
rehabilitationgamestargetingchronicstroke.
Chapter 2 offers the technical context by describing the main gaming functionalities that determine
rehabilitationoutcome.Specifically,itcoversthedevelopmentofanadaptivegameenginesystemusing
specifically designed rehabilitation games based on Gentile’s two-dimensional classification system of
motorskills.
InChapter3, the focus ison themainclinicalguidelines thatcontribute topositivemotor recovery. It
discusses Gentile’s taxonomy as a promising framework for the development of virtual treatment
programsthatareconsistentwithprimarymotor learningprinciples.Aprogramispresentedthatuses
sixbasicrehabilitationgamestogenerate16virtualrehabilitationscenariosthateachrepresentoneof
Gentile’s16 skill categories. Finally, a formalprocedure forguidingpatients through the rehabilitation
processisdiscussed.
Chapter4and5constitutetheexperimentalsectionofthisdoctoralthesis.
Chapter4isbasedonausabilitystudyinwhichnovelrehabilitationgames–developedinthecontextof
the REWIRE project – were applied. The study aimed to investigate whether the VR-based approach

8
wouldbeusableandeffective in improvingpeoples’ gait andbalance. Themethodological framework
recommended by Campbell et al. [61] was used as a basis for this study. Accordingly, the study
represents a preliminary exploratory phase (i.e., with untrained healthy elderly) of the large-scale
REWIREprojectthatfocusesonstrokepatients.
Since, to our knowledge, no study used the sensor-based iTUG tomeasure functional recovery post-
stroke, the study described inChapter 5of this thesis served to investigate the iTUG’s reliability and
validityinpeoplewithstroke.Thischapterprovidestheresultsofanexperimenttoassessthetest-retest
reliabilityandvalidityofgait-andtransition-relatedmetricsduring iTUGperformance.Fourteenstroke
patients and 25 healthy controls were observed by one researcher in two measurement sessions.
Outcomemeasuresweretherelativereliability(i.e.,intraclasscorrelationcoefficient(ICC)),theabsolute
reliability (i.e., standard error ofmeasurement (SEM), limits of agreement (LOA) and smallest clinical
detectabledifference (SDD))and the iTUGmetrics’discriminatorycapabilitiesbetweenstrokepatients
andhealthycontrols.
Finally,Chapter 6 provides a general discussion of themain results presented in this doctoral thesis.
WithrespecttosubsequentresearchstudiesintheframeworkoftheREWIREproject,implicationsofthe
results and limitations are considered.Additionally, new researchquestions generatedby thepresent
resultsandgeneralconclusionsarepresented.

9
References
1. Cerebrovasculardisorders:aclinicalandresearchclassification.Geneva:WorldHealthOrganization.
1978.2. TruelsenT,BonitaR.Theworldwideburdenofstroke:currentstatusandfutureprojections.HandbClin
Neurol.2008;92:327-36.3. KnüwerJ.“Wii-habilitation”:Theuseofmotion-basedgameconsolesinstrokerehabilitation;asystematic
review.2014.4. LaverK,GeorgeS,ThomasS,DeutschJE,CrottyM.Cochranereview:virtualrealityforstroke
rehabilitation.EurJPhysRehabMed.2012;48(3):523-30.5. TruelsenT,Piechowski-JóźwiakB,BonitaR,MathersC,BogousslavskyJ,BoysenG.Strokeincidenceand
prevalenceinEurope:areviewofavailabledata.EurJNeurol.2006;13(6):581-98.6. PeriE,AmbrosiniE,PedrocchiA,PaglianoE,RivaD,BaranelloG,ArnoldiMT,FoscanM,CorlattiA,Marchi
A.Volitionalcyclingaugmentedbyfunctionalelectricalstimulationinhemipareticadolescents:acaseseriesstudy.JAutomatContr.2013;21(1):37-42.
7. FisherS,LucasL,ThrasherTA.Robot-assistedgaittrainingforpatientswithhemiparesisduetostroke.TopStrokeRehabil.2011;18(3):269-76.
8. HornbyTG,StraubeDS,KinnairdCR,HolleranCL,EchauzAJ,RodriguezKS,WagnerEJ,NarducciEA.Importanceofspecificity,amount,andintensityoflocomotortrainingtoimproveambulatoryfunctioninpatientspoststroke.TopStrokeRehabil.2011;18(4):293-307.
9. BoudarhamJ,RocheN,PradonD,BonnyaudC,BensmailD,ZoryR.Variationsinkinematicsduringclinicalgaitanalysisinstrokepatients.PLoSOne.2013;8(6):e66421.
10. HsuA-L,TangP-F,JanM-H.Analysisofimpairmentsinfluencinggaitvelocityandasymmetryofhemiplegicpatientsaftermildtomoderatestroke.ArchPhysMedRehabil.2003;84(8):1185-93.
11. FritzSL,PittmanAL,RobinsonAC,OrtonSC,RiversED.Anintenseinterventionforimprovinggait,balance,andmobilityforindividualswithchronicstroke:apilotstudy.JNeurolPhysTher.2007;31(2):71-6.
12. KautzSA,DuncanPW,PereraS,NeptuneRR,StudenskiSA.Coordinationofhemipareticlocomotionafterstrokerehabilitation.NeurorehabilNeuralRepair.2005;19(3):250-8.
13. FlansbjerUB,MillerM,DownhamD,LexellJ.Progressiveresistancetrainingafterstroke:effectsonmusclestrength,muscletone,gaitperformanceandperceivedparticipation.JRehabilMed.2008;40(1):42-8.
14. EngJJ,TangPF.Gaittrainingstrategiestooptimizewalkingabilityinpeoplewithstroke:asynthesisoftheevidence.ExpertRevNeurother.2007;7(10):1417-36.
15. YavuzerG,EserF,KarakusD,KaraoglanB,StamHJ.Theeffectsofbalancetrainingongaitlateafterstroke:arandomizedcontrolledtrial.ClinRehabil.2006;20(11):960-9.
16. LaiSM,DuncanPW.StrokerecoveryprofileandthemodifiedRankinassessment.Neuroepidemiology.2001;20(1):26-30.
17. PickardAS,JohnsonJA,FeenyDH.Responsivenessofgenerichealth-relatedqualityoflifemeasuresinstroke.QualLifeRes.2005;14(1):207-19.
18. HendricksHT,vanLimbeekJ,GeurtsAC,ZwartsMJ.Motorrecoveryafterstroke:asystematicreviewoftheliterature.ArchPhysMedRehabil.2002;83(11):1629-37.
19. REWIRE-RehabilitativeWayoutInResponsivehomeEnvironments[Internet].[cited2015].Availablefrom:https://sites.google.com/site/projectrewire/.
20. BurkeJW,McNeillMDJ,CharlesDK,MorrowPJ,CrosbieJH,McDonoughSM.Optimisingengagementforstrokerehabilitationusingseriousgames.VisComput.2009;25(12):1085-99.
21. MeriansAS,JackD,BoianR,TremaineM,BurdeaGC,AdamovichSV,RecceM,PoiznerH.Virtualreality–augmentedrehabilitationforpatientsfollowingstroke.PhysTher.2002;82(9):898-915.
22. HodaM,DongH,ElSaddikA.Recoverypredictionintheframeworkofcloud-basedrehabilitationexergame.Universalaccessinhuman-computerinteractionAgingandassistiveenvironments:Springer;2014.p.256-65.
23. RizzoA,KimGJ.ASWOTanalysisofthefieldofvirtualrealityrehabilitationandtherapy.Presence-TeleopVirt.2005;14(2):119-46.

10
24. deBruinED,SchoeneD,PichierriG,SmithST.Useofvirtualrealitytechniqueforthetrainingofmotorcontrolintheelderly:sometheoreticalconsiderations.ZGerontolGeriatr.2010;43(4):229-34.
25. ElliottV,deBruinED,DumoulinC.Virtualrealityrehabilitationasatreatmentapproachforolderwomenwithmixedurinaryincontinence:afeasibilitystudy.NeurourolUrodyn.2014.
26. González-FernándezM,Gil-GómezJ-A,AlcañizM,NoéE,ColomerC.eBaViR,easybalancevirtualrehabilitationsystem:astudywithpatients.StudHealthTechnolInform.2010;154:61-6.
27. PirovanoM,MainettiR,Baud-BovyG,LanziPL,BorgheseNA,editors.Self-adaptivegamesforrehabilitationathome.ComputationalIntelligenceandGames(CIG),2012IEEEConferenceon;2012:IEEE.
28. BateniH.ChangesinbalanceinolderadultsbasedonuseofphysicaltherapyvstheWiiFitgamingsystem:apreliminarystudy.Physiotherapy.2012;98(3):211-6.
29. DeutschJE,BorbelyM,FillerJ,HuhnK,Guarrera-BowlbyP.Useofalow-cost,commerciallyavailablegamingconsole(Wii)forrehabilitationofanadolescentwithcerebralpalsy.PhysTher.2008;88(10):1196-207.
30. FlynnS,PalmaP,BenderA.FeasibilityofusingtheSonyPlayStation2gamingplatformforanindividualpoststroke:acasereport.JNeurolPhysTher.2007;31(4):180-9.
31. AndersonF,AnnettM,BischofWF.LeanonWii:physicalrehabilitationwithvirtualrealityWiiperipherals.StudHealthTechnolInform.2010;154:229-34.
32. TseklevesE,WarlandA,KilbrideC,ParaskevopoulosI,SkordoulisD.TheuseoftheNintendoWiiinmotorrehabilitationforvirtualrealityinterventions:aliteraturereview.Virtual,AugmentedRealityandSeriousGamesforHealthcare1:Springer;2014.p.321-44.
33. CameirãoMS,BadiaSB,OllerED,VerschureP.NeurorehabilitationusingthevirtualrealitybasedRehabilitationGamingSystem:methodology,design,psychometrics,usabilityandvalidation.JNeuroengRehabil.2010;7(1):48.
34. FITREHAB-Innovationforwelfare[cited2015].Availablefrom:http://www.innovation4welfare.eu/287/subprojects/fitrehab.html.
35. AmmannBC,KnolsRH,BaschungP,deBieRA,deBruinED.Applicationofprinciplesofexercisetraininginsub-acuteandchronicstrokesurvivors:asystematicreview.BMCNeurol.2014;14(1):167.
36. AskimT,IndredavikB,EngenA,RoosK,AasT,MørkvedS.Physiotherapyafterstroke:towhatextentistask-orientedpracticeapartofconventionaltreatmentafterhospitaldischarge?PhysiotherTheoryPract.2013;29(5):343-50.
37. MulderT.Aprocess-orientedmodelofhumanmotorbehavior:towardatheory-basedrehabilitationapproach.PhysTher.1991;71(2):157-64.
38. Tudor-LockeCE,MyersAM,RodgerNW.Developmentofatheory-baseddailyactivityinterventionforindividualswithtype2diabetes.DiabetesEduc.2001;27(1):85-93.
39. deBruinED,vanhetReveE,MurerK.Arandomizedcontrolledpilotstudyassessingthefeasibilityofcombinedmotor–cognitivetraininganditseffectongaitcharacteristicsintheelderly.ClinRehabil.2013;27(3):215-25.
40. DeanCM,RichardsCL,MalouinF.Task-relatedcircuittrainingimprovesperformanceoflocomotortasksinchronicstroke:arandomized,controlledpilottrial.ArchPhysMedRehabil.2000;81(4):409-17.
41. O'DellMW,LinC-CD,HarrisonV.Strokerehabilitation:strategiestoenhancemotorrecovery.AnnuRevMed.2009;60:55-68.
42. SalbachN,MayoN,Wood-DauphineeS,HanleyJ,RichardsC,CoteR.Atask-orientatedinterventionenhanceswalkingdistanceandspeedinthefirstyearpoststroke:arandomizedcontrolledtrial.ClinRehabil.2004;18(5):509-19.
43. KwakkelG,WagenaarRC,KoelmanTW,LankhorstGJ,KoetsierJC.Effectsofintensityofrehabilitationafterstroke.Aresearchsynthesis.Stroke.1997;28(8):1550-6.
44. GuadagnoliMA,LeeTD.Challengepoint:aframeworkforconceptualizingtheeffectsofvariouspracticeconditionsinmotorlearning.JMotBehav.2004;36(2):212-24.
45. HallKG,MagillRA.Variabilityofpracticeandcontextualinterferenceinmotorskilllearning.JMotBehav.1995;27(4):299-309.
46. KrakauerJW.Motorlearning:itsrelevancetostrokerecoveryandneurorehabilitation.CurrOpinNeurol.2006;19(1):84-90.

11
47. MuratoriLM,LambergEM,QuinnL,DuffSV.Applyingprinciplesofmotorlearningandcontroltoupperextremityrehabilitation.JHandTher.2013;26(2):94-103.
48. SheaCH,KohlRM.Specificityandvariabilityofpractice.ResQExercSport.1990;61(2):169-77.49. FellDW.Progressingtherapeuticinterventioninpatientswithneuromusculardisorders:aframeworkto
assistclinicaldecisionmaking.JNeurolPhysTher.2004;28(1):35.50. EliassonAC,SundholmLK,ShawK,WangC.Effectsofconstraint-inducedmovementtherapyinyoung
childrenwithhemiplegiccerebralpalsy:anadaptedmodel.DevMedChildNeurol.2005;47(4):266-75.51. MagillRA.Motorlearningandcontrol:conceptsandapplications.7thed.Boston:McGraw-Hill;2004.xiv,
400p.p.52. AdamsDL.Developbettermotorskillprogressionswithgentile'staxonomyoftasks.AmJHealthEduc.
1999;70(8):35-8.53. PatelS,ParkH,BonatoP,ChanL,RodgersM.Areviewofwearablesensorsandsystemswithapplication
inrehabilitation.JNeuroengRehabil.2012;9.54. NgSS,Hui-ChanCW.Thetimedup&gotest:itsreliabilityandassociationwithlower-limbimpairments
andlocomotorcapacitiesinpeoplewithchronicstroke.ArchPhysMedRehabil.2005;86(8):1641-7.55. KitsosG,HarrisD,PollackM,HubbardIJ.AssessmentsinAustralianstrokerehabilitationunits:a
systematicreviewofthepost-strokevalidityofthemostfrequentlyused.DisabilRehabil.2011;33(25-26):2620-32.
56. FariaCD,Teixeira-SalmelaLF,NadeauS.Predictinglevelsofbasicfunctionalmobility,asassessedbytheTimed"UpandGo"test,forindividualswithstroke:discriminantanalyses.DisabilRehabil.2013;35(2):146-52.
57. ZampieriC,SalarianA,Carlson-KuhtaP,AminianK,NuttJG,HorakFB.Theinstrumentedtimedupandgotest:potentialoutcomemeasurefordiseasemodifyingtherapiesinParkinson'sdisease.JNeurolNeurosurgPsychiatry.2010;81(2):171-6.
58. FlansbjerUB,HolmbackAM,DownhamD,PattenC,LexellJ.Reliabilityofgaitperformancetestsinmenandwomenwithhemiparesisafterstroke.JRehabilMed.2005;37(2):75-82.
59. deOliveiraCB,deMedeirosIRT,FrotaNAF,GretersME,ConfortoAB.Balancecontrolinhemipareticstrokepatients:Maintoolsforevaluation.JRehabilResDev.2008;45(8):1215-26.
60. SalarianA,HorakFB,ZampieriC,Carlson-KuhtaP,NuttJG,AminianK.iTUG,asensitiveandreliablemeasureofmobility.IEEETransNeuralSystRehabilEng.2010;18(3):303-10.
61. CampbellM,FitzpatrickR,HainesA,KinmonthAL,SandercockP,SpiegelhalterD,TyrerP.Frameworkfordesignandevaluationofcomplexinterventionstoimprovehealth.BMJ.2000;321(7262):694–6.

12
2
Computational intelligence and game design for effective at-home
stroke rehabilitation
BorgheseNA1,PirovanoM1,2,LanziPL2,WüestS3,deBruinED3
1DepartmentofComputerScience,UniversityofMilan,Italy
2DipartimentodiElettronica,InformazioneeBioingegneria–PolitecnicodiMilano,Italy
3InstituteofHumanMovementSciencesandSport,DepartmentofHealthSciencesandTechnology,ETH
Zurich,Switzerland
GamesforHealthJournal2013;2(2):81-88

13
Abstract
Objective:Theaimofthisarticleistodescribeagameenginethathasallthecharacteristicsneededto
supportrehabilitationathome.Thelow-costtrackingdevicesrecentlyintroducedintheentertainment
market allowmeasuring reliably at home, in real time, players’motionwith a ‘hands-free’ approach.
Such systems have also become a source of inspiration for researchers working in rehabilitation.
Computer games appear suited to guide rehabilitation because of their ability to engage the users.
However, commercial videogames and game engines lack the peculiar functionalities required in
rehabilitation: Games should be adapted to each patient’s functional status, and monitoring the
patient’smotionismandatorytoavoidmaladaptation.Feedbackonperformanceandprogressionofthe
exercises should be provided. Lastly, several tracking devices should be considered, according to the
patient’spathologyandrehabilitationaims.
SubjectsandMethods:Wehaveanalyzedtheneedsof thecliniciansandofthepatientsassociated in
performingrehabilitationathome,identifyingthecharacteristicsthatthegameengineshouldhave.
Results:Theresultofthisanalysishas ledustodevelopthe IntelligentGameEngineforRehabilitation
(IGER) system, which combines the principles upon which commercial games are designed with the
needsofrehabilitation.IGERisheavilybasedoncomputationalintelligence:Adaptationofthedifficulty
leveloftheexerciseiscarriedoutthroughaBayesianframeworkfromtheobservationofthepatient’s
successrate.Monitoringisimplementedinfuzzysystemsandbasedonrulesdefinedfortheexercisesby
clinicians.SeveraldevicescanbeattachedtoIGERthroughaninputabstractionlayer,liketheNintendo®
(Kyoto, Japan)WiiTM Balance BoardTM, theMicrosoft® (Redmond,WA) Kinect, the Falcon fromNovint
Technologies(Albuquerque,NM),ortheTyromotion(Graz,Austria)Tymo®platebalanceboard.IGERis
complementedwithvideogamesembeddedinaspecifictaxonomydevelopedtosupportrehabilitation
progressionthroughtime.
Conclusion:Afewgamesaimedatposturalrehabilitationhavebeendesignedanddevelopedtotestthe
functionalitiesoftheIGERsystem.Thepreliminaryresultsoftestsonnormalelderlypeopleandpatients
with the supervision of clinicians have shown that the IGER system indeed does feature the
characteristicsrequiredtosupportrehabilitationathomeandthatitisreadyforclinicalpilottestingat
patients’homes.

14
2.1Introduction
Novel tracking devices, like the Nintendo® (Kyoto, Japan)WiiTM and Balance BoardTM andMicrosoft®
(Redmond,WA)Kinect,havemadetheinterfacewithvideogamesmorenaturalandintuitive,leadingto
the success of these devices and their associated games. The capability of measuring the players’
movements has been early recognized as a major step forward in realizing cheap and reliable
rehabilitationsystemsinwhichthepatientcanbeguidedthroughrehabilitationexercisesbyadequate
videogames. Such capabilityhasbeenexplored in the rehabilitation field [1-3] andby recently funded
EuropeanCommissionprojects[4-7].
However,itwassoonrecognizedthatthevideogamesdevelopedfortheentertainmentmarketarenot
adequateforthepaceandthegoalsofrehabilitation[8-10]:Theirfastinteraction,whichcanbebarely
matched to the patient’s residual functional abilities, and thewealth of targets and distractorsmake
usabilitylowandmayproducestrainandanxiety.Thus,onehurdlefacingthesuccessfuluseofexercise
videogames (or exergames) in older adults and functionally impaired population is thatmany off-the-
shelf videogames are too complex for use by these groups [8]. Videogames must, therefore, be
developedtotakeintoconsiderationthecognitiveandphysicallimitationsofthepopulation(s)forwhich
theyareintended.Thisisthereasonwhygamesexplicitlydedicatedtorehabilitationhavebeenrecently
developed.
In addition, in the REWIRE [4] project, the need for developing game engines of a new generation,
specificallytargetedforrehabilitationpurposes,hasbeenclearlyidentified.Suchenginesshouldhavea
twofoldgoal:The first, commontoallgameengines, is toprovideall functionalities for thegameplay,
andthesecond,associatedwiththeirtherapeuticrole,istoprovidereal-timemonitoringandadviceto
thepatient.Rehabilitationgameenginesshould(1)adaptthedifficultyandthegameplaytothepatients’
abilities to avoid frustration and, most importantly, (2) should monitor maladaptation and wrong
postures,asthesewouldmakerehabilitationmoreharmfulthaneffective.Thegameengineshouldalso
beable(3)togiveanadequatereal-timefeedbacktothepatientwhileexercising.
Another open problem when applying games in rehabilitation is the definition of a rehabilitation
schedule based on important training principles (e.g., objective progression in the therapy, with an
increasinglevelofdifficultymappedontotherehabilitationplanandgoals).
In the following, we discuss how these issues have been addressed inside the REWIRE platform. In
particular, we illustrate the Intelligent Game Engine for Rehabilitation (IGER) system, developed

15
specificallytosupportrehabilitationthroughgames,andhowthiscanbeintegratedwiththedefinition
of an adequate taxonomy for rehabilitation progression through time inspired by thework ofGentile
[11].
2.2Materialsandmethods
Thedevelopmentofaneffectivegameengineforrehabilitationhastobebasedoninputsfromclinicians
andpatients. Severalmeetings havebeenorganized to elicit such specifications. The key issue is that
rehabilitation games cannot work as stand-alone applications but must be included into a broader
structure involving patients, therapists, clinicians, hospitals, and institutions at the regional/national
level. This is specifically the approach pursued inside the REWIRE project, recently funded by the
EuropeanCommission.TheREWIREplatformimplementssuchabroadperspectivebyintegratingthree
mainhierarchicalcomponents:Ahospitalstation(HS),anetworkingstation(NS),andapatientstation
(PS),undertheassumptionthatsuchastructureenableseffectivesupportofat-homerehabilitation.
The HS is used by clinicians to define and schedule the rehabilitation at home. It also monitors the
patient’s progression remotely and supports a virtual communityof patients and clinicians thathelps,
educates,andmotivatesthepatients.TheNSisinstalledatthehealthprovidersite,ataregionallevel.It
providesadvanceddatamining functionalities todiscoverpatterns in rehabilitation treatmentsamong
hospitals and regions. ThePS is installed at patients’ homes andhas at its core the IGER (Figure 2.1),
which guides patients through their actual rehabilitation schedule using engaging and targeted
videogamesandmonitorspatients’movementsandtheircorrectexecutionoftheexercises.
An additional hospital communication module of the station allows patients to interact with the
clinicians at the hospital and to download the rehabilitation program and the configuration of the
associated games. REWIRE contains also a lifestyle module that collects data on the patient’s daily
activitythroughabodysensornetworkthatisused,alongwithenvironmentalandphysiologicaldata,to
tunethegames’difficultylevel,assesspotentialrisks,andadvisecliniciansonthetherapy.
Finally,avirtualcommunitymodule,managedbythehospital,actsasaclientofthepatients’community
andallowspatientstointeractwithapeergroup.

16
Figure2.1:TheIntelligentGameEngineforRehabilitation(IGER)anditsgameandcontrolmodules.Theconnectionswiththepatient and the therapist at the hospital and the virtual therapist, which provides real-time feedback to the patient, arehighlighted.
Rehabilitationscheduling
Rehabilitation exercises are designed by therapistswith specific goals, for example, (1) to increase or
maintainmobilityofthejointsandsurroundingsofttissues,(2)todevelopcoordinationthroughcontrol
ofindividualmuscles,(3)toincreasemuscularstrengthandendurance,or(4)topromoterelaxationand
reliefoftension[12].
For each exercise, therapists define the correct way to perform it, and, in one-on-one sessions, they
check that patients perform only correct movements and maintain correct postures so as to avoid
maladaptationand,therefore,inadequaterehabilitation.
Thevarietyofexercisesisquitelargeanddependsonthetherapists’idiosyncrasies.Thus,itisdifficultto
map the therapists’ rehabilitation exercises, their goals, and the mandatory posture/movement
constraintstotheirimplementationasvideogames.
In our work, we guide the mapping between therapy and engaging videogames by using Gentile’s
taxonomy of motor skills [11], which identifies high-level features of rehabilitation routines and
organizestheminahierarchicalstructure(Figure2.2).
Gentile’staxonomy[11] isatwo-dimensionalmatrixthatcontainsexerciseswith increasingcomplexity
oftheaddressedfunctionality(frombodystabilitytobodymovement)initscolumns.Initsrowsarethe

17
conditions under which the exercises are executed, from simple static environments to time-varying
situationswithintertrialvariability.
With this taxonomy, it becomes easier to design and configure games for rehabilitation. In fact, any
exerciseformotorskillrehabilitation(proposedbyanytherapist)canbeclassifiedinoneelementofthe
taxonomy according to a progression in recovering functionality. At the same time, rehabilitative
videogamescanbedevelopedbytargetingoneelementofthetaxonomyratherthanaspecificexercise
proposedbyaspecifictherapist,thusbroadeningthenumberoftherapistsandpatientswhomightuse
it.
Figure2.2:Gentile’s taxonomy[11],withapossiblemappingofexercisesandapossibleprogression forbalanceandposturerehabilitation.Thearrowindicatesapossibleprogressionofthepatientandthepossiblemappingsofthe‘Fruitcatcher’gamedescribedhereafter.
TheIGERgameengine
TheIGERisthecorecomponentofthePS.Itcomprehendsagameengineandagamecontrolunit.The
formerprovidesallthebasicgamingfunctionalities(inputdata,animation,collisiondetection,rendering,
andgamelogic);thelattercontrolsthegame,andithasbeendevelopedtomatchtheneedsofgames
forrehabilitation:

18
1. Itschedulesthegames,chosenandconfiguredaccordingtotheframeworkshowninFigure2.2.
2. It adapts the game difficulty level to the actual patient’s performance capacity, so that an
adequatechallengelevelismaintained.
3. It supervises thegamingsessionsandmonitorswhetheror if thepatient’smovementscomply
withthespecificationssetbythetherapist.
4. Itdisplaysavirtualtherapist(VT)toadviseandprovidefeedbacktothepatientonthetherapy.
Games defined for rehabilitation have to be parametric. Specifically, games should be defined by
parameters that can be regulated and adapted, depending on the level of game difficulty. Such
parameters are initialized inside the hospital, where the clinician prescribes the therapy and are
continuously adapted to each patient’s progression. Such parameters can be, for instance, either the
frequencyof theobstaclesandof the targets inside thegameor therangeofmovements required to
complete a game successfully. The control unit implements a real-time adaptation of the parameters
through a Bayesian model [10]: The patient’s performance is monitored, and the success rate is
computedonline. Theparameters are then increasedor decreased such that a certain success rate is
maintained,wheretheamountofchangeisprovidedbythemodel.
Thepatient’smovement isalsoused formonitoring.To thisaim,a setof rulesof correctexecution is
defined inside theHS.Suchrules representaknowledgebase fromthe therapist’sexperienceandare
coded into logical propositions like, for instance, “do not bend the trunk” or “keep your feet slightly
apart”. Such rules are then fuzzyfied, defining a maximum range allowed for correct execution (e.g.,
maximum trunk bending allowed in 20°) and associating automatically intermediate ranges with the
valuesinbetween(Figure2.3).Avisualinterface,showinganavatarinsidethegameenvironment,helps
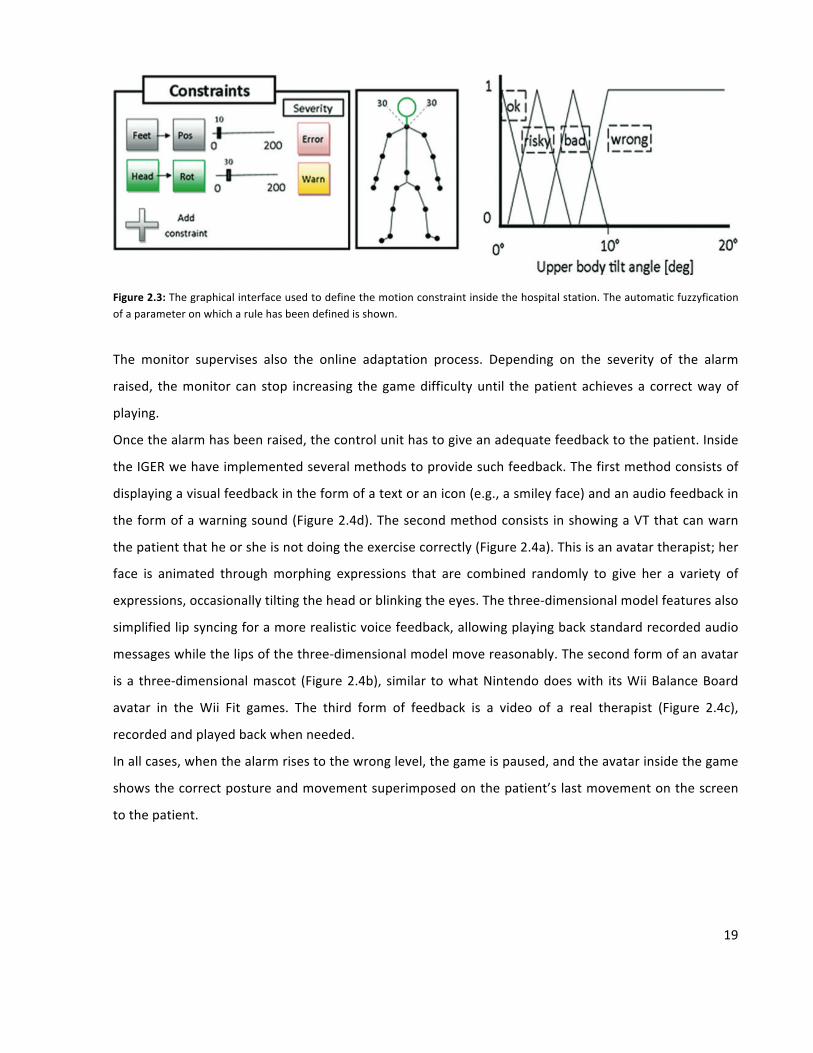
thetherapistsindefiningtheconstraintsonthepatient’smotion.
Atrun-timetheknowledge-basedmonitor insidethecontrolunit(Figure2.1)comparesthemovement
ofallthebodysegmentswiththerulesdefinedinsidetheHSbythecliniciansandraisesanalarmlevel
thatcanbegraded:riskysituation,badmovement,orwrongmovement.Ifmorethanoneconstraintis
violated, the most severe alarm level is raised, implicitly combining the fuzzy rules with the logical
operator.
19
Figure2.3:Thegraphicalinterfaceusedtodefinethemotionconstraintinsidethehospitalstation.Theautomaticfuzzyficationofaparameteronwhicharulehasbeendefinedisshown.
The monitor supervises also the online adaptation process. Depending on the severity of the alarm
raised, themonitor can stop increasing thegamedifficultyuntil thepatientachievesa correctwayof
playing.
Oncethealarmhasbeenraised,thecontrolunithastogiveanadequatefeedbacktothepatient.Inside
theIGERwehaveimplementedseveralmethodstoprovidesuchfeedback.Thefirstmethodconsistsof
displayingavisualfeedbackintheformofatextoranicon(e.g.,asmileyface)andanaudiofeedbackin
theformofawarningsound(Figure2.4d).Thesecondmethodconsists inshowingaVTthatcanwarn
thepatientthatheorsheisnotdoingtheexercisecorrectly(Figure2.4a).Thisisanavatartherapist;her
face is animated throughmorphing expressions that are combined randomly to give her a variety of
expressions,occasionallytiltingtheheadorblinkingtheeyes.Thethree-dimensionalmodelfeaturesalso
simplifiedlipsyncingforamorerealisticvoicefeedback,allowingplayingbackstandardrecordedaudio
messageswhilethelipsofthethree-dimensionalmodelmovereasonably.Thesecondformofanavatar
isa three-dimensionalmascot (Figure2.4b), similar towhatNintendodoeswith itsWiiBalanceBoard
avatar in the Wii Fit games. The third form of feedback is a video of a real therapist (Figure 2.4c),
recordedandplayedbackwhenneeded.
Inallcases,whenthealarmrisestothewronglevel,thegameispaused,andtheavatarinsidethegame
showsthecorrectpostureandmovementsuperimposedonthepatient’slastmovementonthescreen
tothepatient.

20
Figure2.4:ThefeedbackimplementedinsidetheIntelligentGameEngineforRehabilitation:(a)avirtualtherapist,(b)amascot,(c)arealtherapist,and(d)anicon(smileyface)showninsidethegame.
Principlesofgamedesign
Wehavebuiltthroughourframeworkasetofminigames,eachdesignedaccordingtothegoalsandthe
requirements of the underlying exercises and on the good game design practice [13-15]:Meaningful
play,flowtheory,andsenseofpresencehavebeenallincorporatedintothedesign.
Meaningfulplaystatesthateachgameactionmusthaveadirectandclearlydistinguishablefeedbackas
wellasareasonablylastingeffect.Thishelpsthepatientinunderstandingwhatheorshecanandcannot
do. Itwas achievedhere through a clear video-audio feedbackof the success or failure of a patient’s
action,representedrespectivelywitha‘P’greensymboldisplayedonthescreenandanicebeepanda
‘X’redsymbolandanannoyingbeep.
Thesecondbasicprincipleisthetheoryofflow,whichstatesthatwhentheskillsoftheuserarematched
bythelevelofchallengeposedbythegame,theuserentersastateofcompletefocusandimmersionin
whichheorshelosestrackoftime[14].Thepatient’sappropriatelevelofexercisedifficultyisachieved
inside IGER through an adaptation mechanism based on a Bayesian framework [10]. Scenarios and
positionoftargetsanddistractorsofeachgamearerandomized,makingthepatientfeelchallengedby
always different situations. Music matched to the game scenarios is played during the rehabilitation
sessions. The scoring system reflects the rehabilitation nature of the games [8-10, 16]: No negative
pointsaregiven,orno ‘death’occurs,andanactualscorevaluereflects theaccuracyand/orspeedof

21
execution of the movement. Former scores are shown along with the actual score to demonstrate
improvement over time. All these elements contribute to create a flow experience that, in turn,
contributes in focusing on the game. This hides the burden of therapeutic repetitive tasks and the
difficulties arising from impairments, under the entertaining experience of a game. This is evenmore
importantwhenweconsiderthatpost-strokepatientsoftenfallintodepression[17].
ThesenseofpresenceisanotherstrongpointassociatedwithIGER.Astheavatarfollowsthepatient’s
movementswithnoappreciabledelays, thepatientcanfeel that theavatarrepresentshim-orherself
insidethevirtualenvironmentand,therefore,thepatienthasastrongperceptionofbeingtheactorin
thegame[18].Thisisassociatedwiththeuseof‘hands-free’trackingofmotion,whichdoesnotrequire
attachinganydevicetothepatient,allowingthemostnaturalinterfacingwiththegames.
Gamesforrehabilitation
Inourwork,weaimtocreateasetofminigamesbuiltonclinicallyvalidexercisesandcomprehending
bothmonitoringandadaptability.Wedesignedandrealizedseveralgameconceptsthataddressposture
andbalancerehabilitation.ThesegamescanbemappedonasetofexercisesdefinedthroughGentile’s
taxonomy [11] and share the same theme (in our case, the farm theme) to provide a continuity in
gaming during the patient’s rehabilitation process. To exemplify, we present here two of these
minigames:‘Animalfeeder’and‘Fruitcatcher’(Figure2.5),whichhighlighttheflexibilityofourapproach
andthemonitoringandadaptationcapabilities.
Figure2.5:Twominigamesofthepatientstation:(a)‘Animalfeeder’and(b)‘Fruitcatcher’.
The‘Animalfeeder’minigameaimstotrainpatients’balancebyimplementingadualtask.Theexercise
requires thepatient to kneel in frontof thedisplay and tomove the impairedarm to touchdifferent
targets,whicharerepresentedbythreehungrycowsthathavetobefed.Thecowskeeprequestingfood

22
bymooingwhileopening theirmouths (Figure2.5a). Theplayer controls a virtualhand in first-person
view.Heorshehasfirsttocollectsomehayandthenfeedittooneofthehungrycows;whenthecow
has been fed, the player’s score increases. If a cow remains hungry for too long, it groans, and the
player’sscoredecreases.Inaddition,apitchforkpositionedtotheleftoftheplayermustbekeptupright
bytheplayerwithhisorherotherhand.Iftheplayerfailstodoso,thepitchforkbreaks,andtheplayer’s
scoredecreases. ‘Animal feeder’ canbecurrentlyplayedwithdifferentdevices. Inparticular,here the
player’shandwastrackedthroughaKinectcamerapositionedabovethedisplay,whilethepitchforkwas
controlledbyNovintTechnologies(Albuquerque,NM)Falcon®hapticdevice,whichproducesanelastic
force to the patient’s hand proportional to the hand displacement. Note that devices not used for
gameplaycanstillbeusedforadditionalmonitoringofthepatient.Forinstance,Figure2.5bshowshow
Nintendo’sBalanceBoardisusedtomonitorthepositionofthefootcenterofpressurewhileperforming
agame.Inthiscase,theoscillationsdonotaffectthegameplay,butprovideusefulinformationinterms
ofapatient’sbalancecapability.
The‘Fruitcatcher’game(Figure2.5b)isbuiltontwodifferentexercises.Forthefirstexercise,thepatient
isrequiredtoshifthisorherupperbodytotheleftandtotherightside,whilekeepingthefeetstillon
theground.Forthesecondexercise,thepatientmustmove laterally insidetheminigame. Inthebasic
conceptof ‘Fruitcatcher’, theplayermustcatchfruits falling fromthetopofatree.Theplayeravatar
standsbelowthetreewithavirtualbasketonitsheadandcanmovethebodylaterallytocatchthefruits
with the basket. The player’s score increases when a fruit falls into the basket. The fruits fall from
differentheightsandfromdifferentpositionsonthehorizontalaxisandatadifferentfrequency.Likethe
‘Animal feeder’game, itcanbeplayedwithdifferentdevices (e.g., theNintendoWiiBalanceBoardor
theMicrosoftKinect).Thechoiceoftheinputdevice,inthiscase,dependsalsoontheexerciserationale,
showinganexampleofseparationbetweengameandexercise.Whenusing theNintendoWiiBalance
Board,theplayerisconstrainedtokeepthefeetontheboard.Thus,onlythefirstexercisecanbedone
inthisway.WhenusingtheMicrosoftKinect,instead,theplayercanmovefreelyaroundtheplayarea.
Inthislattercase,theexercisecanbeeitherofthetwodescribedabove.InFigure2.2,wecanseewhere
thetwoexercisesaremappedoverGentile’staxonomy[11].Apossibleprogressioninsidethetaxonomy
isshowninFigure2.2:Thepatientstartswithanexerciseclassifiedas1A,whichbelongstothelowest
classification,defininganeasyexercise. In thiscase,using the ‘Fruitcatcher’gameasanexample, the
patientmayonlyhavetostandstillandnottomoveinordertonotdisturbthetree;otherwise,itsfruits
wouldfalldown.Asthepatientprogressesandimprovesstrengthandbalancecapability,thegamemay
movetowardthe1Dbox,addingbothbodytransport(requiringthepatienttomovearound)andobject

23
manipulation(addingthebasketontheheadandtherequirementtocatchfruits).Then,thepatientmay
be presented with intertrial variability, moving the classification to 2D. At last, the patient may be
required tomeetbirds flyingaround thevirtual areaanddisturbinghisorher focus, thusmoving the
classificationtoward4D.
Toaccommodatesuchavarietyoftrackingdevices,wehaveinsertedanInputAbstractionLayerinside
theIGER.OurprototypecurrentlysupportstheSony(Tokyo,Japan)PlayStation®PS3TMEyecamera,the
Microsoft Kinect camera and its microphone array, theWii Balance Board, or the Tyromotion (Graz,
Austria)Tymo®plateandtwohapticdevices(theOmni®Phantom®[SensableTechnologies,Wilmington,
MA] and the Novint Falcon). The input devices can be combined for additional control over game
elementsorforimplementingdualtasks.
2.3Discussion
Manyauthorshaveacknowledgedthepowerofimmersionassociatedwithvirtualrealityandgamesin
particular [19, 20]. This is referred to as presence; it would facilitate the rehabilitation sessions by
providingafun,interactiveenvironmentthatchallengestheskillsoftheplayerandimmersestheplayer
in a virtual world. Such an approach would limit the typical boredom and fatigue in traditional
rehabilitation:Thepatient,whileexercising,shouldfeellikeaplayer,focusedonhavingfunwhileplaying
thegame.Tofullyachievethis,gamesshouldbedesignedaccordingtogoodgamesdesignprinciplesto
avoidcomingupshortinengagingthepatients.
However, engaging games are not enough: Adaptation, monitoring, and real-time evaluation of the
movements should be provided to the patient in real time. Such functionalities are not provided by
commercial games, but are indeed incorporated inside the IGER system. In fact, (1) IGER allows
configuring thegame inside theHS, setting theparametersassociatedwith the levelofdifficultymost
adequate to the patient’s functional status, and then it continuously adapts these parameters to the
patient’sperformancetocontinuouslychallengethepatientattheproperlevelatanypointduringthe
rehabilitationprocess.(2)IGERallowsthecontinuousmonitoringofpatients’actionsandpostureswithin
thegameengine,and itaimstoenforceacorrectexecutionoftherehabilitationmovements. (3) IGER
integrates a real-time feedback to the patient of his or her performance and of possible wrong
movements,accordingtotherulessetbythetherapists.
Monitoringandreal-timefeedbackhavebeendesignedtosubstitutefor,althoughtoa limiteddegree,
thetherapist.Inone-on-onesessions,thesefunctionsareprovidedbythehumantherapist,whocannot

24
be present at home during rehabilitation. Themonitoring role is achieved by the fuzzymonitor that
implementstheruledefinedbythetherapisthim-orherself,mainlytoavoidmaladaptation.Therules
operateinrealtimeonthemotiondataandaredownloadedfromtheHSatgameconfigurationtime.
The social aspects of rehabilitation are very important for patients and must be considered when
designing a platform for home rehabilitation. For instance, in one-on-one sessions, the therapist is a
major source of motivation for the patient [21], but this component is missing during home
rehabilitation.Toavoidisolation,whichdiminishestheappealofarehabilitationsession,IGERprovides
aninformativeevaluationtothepatient,besidesdisplayingabalancedscorethatreflectsperformance
ontheactualexercise,bymeansofaVTthat, throughspeech,evaluatesthepatient’sperformanceof
theexercise.
Giventheimportanceoftheissue,wehaveevaluatedseveralfeedbackmodalities.Icons(e.g.,asmiley
face)andsoundsareespeciallyusefulbecausetheyprovideimmediateandeasilyunderstoodfeedback
tothepatient.Moreover,visual iconsandsoundshaveamoreimmediateeffectthantheVT;theyare
less intrusiveandlessannoyingwhenrepeatedoften.Forthisreason,weusethemforthesimpleand
morefrequentwarnings.
TheVT,becauseofitsresemblancetoarealtherapist,allowsthepatienttofeelthepresenceofamore
seriouscharactersupervisinghisorheractivity.Themascot,ontheotherhand,canbebeneficialasa
motivatorbecauseofitsfunnyaspectandmovements,enhancingtheplayfulaspectoftheapplication.
Thevideoisusefulbecauseofitsrealismandthepresenceofarealperson,whocouldbepreferredby
the patient for a greater degree of empathywith the therapist. This implies a somehow stereotyped
videostyle,astheamountofvariabilityinthevideoappearanceismuchlessthanwithmascotsorthree-
dimensionalmodels.Webelievethatthereisnotasinglebestfeedback,buteachpatientwillhavehisor
herownpreference,dependingonpersonalidiosyncrasies.
The VT and themascot can also be displayed between two games (exercises) of the same session to
introduce the exercises and accompany the patient along his or her training period. In addition, they
appear during the introduction of the game to explain its rules and during the course of the game,
encouragingandmotivating theplayers according to theirperformance. Lastly, theyappearwhen the
gameisstoppedbecauseofwrongmovements,explainingtothepatientwhatwentwrongandwhatthe
patientshoulddo.

25
A proper game design and games specifically designed for therapeutic purposes are not sufficient. A
complete rehabilitation program is required, and this can be defined only by a clinician. Besides the
game engine, a clear definition of a rehabilitation path is required to support intensive prolonged
rehabilitation processes. The therapist has still the fundamental role of the supervisor, although
remotelyfromthehospital.Thesuccessionofgamesinsidetherehabilitationprogramiscustomizedby
the therapist for each patient according to his or her impairments; the program is defined at the
hospital,accordingtotherehabilitationgoalssetwiththepatientandthecurrentpositionofthepatient
inside the taxonomy (Figure 2.2). The therapist can also fully configure each game, thus tailoring the
underlying exercise to the patient’s health status. For instance, the therapist can define, for each
exercise,what inputdeviceshouldbeused,howlongtheexerciseshould last,howfarthetargetscan
travel,andhowfasttheycanmove.Finally,thetherapisthasanimportantroleconcerningthedefinition
oftheknowledgebaseonwhichtherulesmonitorapatient’smovementsandhisorherconstraintsare
builtupon.Apersonalizedrehabilitationprogramcanthereforebeobtained.
2.4Conclusion
Thisworkistheresultofatightcollaborationamonggamedevelopers,humanmovementscientists,and
physicaltherapistsandaimsatbuildingengaginggamesthatimplementtherapeuticexercisestargeted
toat-homerehabilitation.WedesignedtheIGERplatformtotakeupsomeofthetherapist’sfunctions
duringhomerehabilitation.Althoughcompletelyreplacingthetherapist’sskillisbeyondreach,theIGER
system can make rehabilitation at home a viable option, especially if intertwined with periodic
rehabilitation sessionsat the referencehospitalwith the reference cliniciansmaintaining, therefore, a
personalrelationshipthatispresumablyfundamentalforprolongedrehabilitation.
Authors’contributions
NABcontributedtotheconceptionanddesignof themanuscript,andwritingthemanuscript.MPand
PLL have been involved in drafting the manuscript and critically revised the manuscript. SW made
substantial contributions to conceptionanddesignof themanuscript, andparticipated indrafting the
manuscript. EDdB participated in drafting the manuscript and revising it critically for important
intellectualcontent.Allauthorsreadandapprovedthefinalmanuscript.

26
Acknowledgments
This work was partially supported by the REWIRE project (www.rewire-project.eu), funded by the
EuropeanCommissionundertheFP7frameworkwithcontract287713.
Conflictofintereststatement
Nocompetingfinancialinterestsexist.

27
References
1. MainettiR,SeddaA,RonchettiM,BottiniG,BorgheseNA.Duckneglect:video-gamesbasedneglect
rehabilitation.TechnologyandHealthCare2013;inpress.2. BurkeJ,McNeillM,CharlesD,etal.Optimisingengagementforstrokerehabilitationusingseriousgames.
VisComput2009;25:1085.3. JackD,BoianR,MeriansAS,etal.Virtualreality-enhancedstrokerehabilitation.IEEETransNeuralSystems
RehabEng2011;9:308.4. www.rewire-project.eu/(accessedMarch7,2013).5. www.istoppfalls.eu/(accessedMarch7,2013).6. www.scriptproject.eu/(accessedMarch7,2013).7. www.cogwatch.eu/(accessedMarch7,2013).8. deBruinED,SchoeneD,PichierriG,SmithST.Useofvirtualrealitytechniqueforthetrainingofmotor
controlintheelderly.Sometheoreticalconsiderations.ZGerontolGeriatr2010;43:229.9. CameirãoMS,BadiaSB,OllerED,VerschureP.Neurorehabilitationusingthevirtualrealitybased
RehabilitationGamingSystem:Methodology,design,psychometrics,usabilityandvalidation.JNeuroengRehabil2010;3:7–48.
10. PirovanoM,MainettiR,Baud-BovyG,LanziPL,BorgheseNA.Self-adaptivegamesforrehabilitationathome.Proc.IEEEConferenceonComputationalIntelligenceandGames.IEEEPress;2012:179–186.
11. GentileAM.Skillacquisition:Action,movementandneuromotorprocesses.In:CarrJH,ShepherdRB,GordonJ,GentileAM,HeldJM.(eds.)MovementScience:FoundationsforPhysicalTherapyinRehabilitation,2nded.Rockville,MD:Aspen;2000:111–187.
12. Exerciseandphysicalfitness.www.nlm.nih.gov/medlineplus/exerciseandphysicalfitness.html(accessedMarch7,2013).
13. KosterR.ATheoryofFunforGameDesign.Scottsdale,AZ:ParaglyphPress;2004.14. SchellJ.TheArtofGameDesign:BookofLenses.NewYork:Elsevier;2008.15. SalenK,ZimmermanE.RulesofPlay:GameDesignFundamentals.Cambridge,MA:Massachusetts
InstituteofTechnology;2003.16. GoudeD,BjörkS,RydmarkM.Gamedesigninvirtualrealitysystemsforstrokerehabilitation.StudHealth
TechnInform2007;125:146–148.17. LanghorneP,CouparF,PollockA.Motorrecoveryafterstroke:Asystematicreview.LancetNeurol2009;
8:741.18. SlaterMSpanlangB,Sanchez-VivesM,BlankeO.Firstpersonexperienceofbodytransferinvirtualreality.
PLoSOne2010;5:5.19. BrownE,CairnsP.Agroundedinvestigationofgameimmersion[abstract].In:CHI’04ExtendedAbstracts
onHumanFactorsinComputingSystems.ACM;2004:1297.20. RizzoA,KimGJ.ASWOTanalysisofthefieldofvirtualrealityrehabilitationandtherapy.Presence2005;
14:119.21. MacleanN,PoundP,WolfeC,RuddA.Theconceptofpatientmotivation.Aquantitativeanalysisofstroke
professionals’attitudes.Stroke2002;33:444.
28
3
Design considerations for a theory-driven exergame-based rehabilitation program to improve walking of persons with stroke
WüestS1,vandeLangenbergR1,deBruinED1
1InstituteofHumanMovementSciencesandSport,DepartmentofHealthSciencesandTechnology,ETH
Zurich,Switzerland
EuropeanReviewofAgingandPhysicalActivity2014;11(2):119-129

29
Abstract
Virtualrehabilitationapproachesforpromotingmotorrecoveryhasattractedconsiderableattentionin
recent years. It appears to be a useful tool to provide beneficial and motivational rehabilitation
conditions. Following a stroke, hemiparesis is one of themost disabling impairments and, therefore,
manyaffectedpeopleoftenshowsubstantialdeficitsinwalkingabilities.Hence,oneofthemajorgoals
of stroke rehabilitation is to improve patients' gait characteristics and hence to regain their highest
possible levelofwalkingability.Becauseprevious studies indicatea relationshipbetweenwalkingand
balanceability,thisarticleproposesastrokerehabilitationprogramthattargetsbalanceimpairmentsto
improve walking in stroke survivors. Most currently, available stroke rehabilitation programs lack a
theory-driven,feasibletemplateconsistentwithwidelyacceptedmotorlearningprinciplesandtheories
in rehabilitation. To address this hiatus, we explore the potential of a set of virtual reality games
specificallydevelopedforstrokerehabilitationandorderedaccordingtoanestablishedtwo-dimensional
motorskillclassificationtaxonomy.Wearguethattheensuing‘exergame’-basedrehabilitationprogram
warrantsindividuallytailoredbalanceprogressioninalearningenvironmentthatallowsvariablepractice
andhenceoptimizestherecoveryofwalkingability.
Keywords:Strokerehabilitation,Gentile'staxonomy,Virtualreality,Exergames,Motorlearning

30
3.1Introduction
Virtual reality technique can be combined with targeted exergames development with the aim to
promotemotorrehabilitation.Recently,anumberofresearchershavepointedtothepotentialofvirtual
reality applications in health care [6, 20, 28, 36, 47, 49] and hence sparked the introduction of this
technologywithinrehabilitationmedicine.Theuseofso-called‘exergames’–virtualrealitygamesthat
involve physical exercise – has been proposed as a valuable instrument to encourage participation in
rehabilitationandimprovetheadherencetotherapyprogramsbecauseofengagingtheuser[6,12,47].
For example, a study by Rizzo and Kim [47] demonstrated that virtual reality-based games reduce
patients'drearinessandsimultaneouslyincreasetheirmotivationforrehabilitationpractice.Accordingly,
virtualrealityprovidesthecapacitytosimulatescenariosthatareeffectiveinattractingtheperformers'
attention.Simulatedcircumstancescanbeused toelicita thrillingambience,whereas thepatient can
stillperformmovementandbehaviorsinasafeandcontrolledenvironment.
For best results in rehabilitation, videogames specifically designed for therapy should be used [5].
Becauseconventional videogameswereprimarilydeveloped forentertainmentpurposes [62],mostof
these are not practical for rehabilitation [5]. One hurdle facing the successful use of exergames in
rehabilitation is thatmany off-the-shelf videogames are too complex for use by functionally impaired
personsorelderlypeople[12].Videogamesmustthereforebedevelopedtotakeintoconsiderationthe
cognitiveandphysicallimitations,aswellastheinterestsets,ofthetrainees[12].Todate,however,the
vastmajorityofresearchhasfocusedongamesdevelopedfortheentertainmentmarketwhichfailsto
adaptthegameplayaccordingtopatients'rehabilitationrequirements[43].
FP7 is the short name for the ‘Seventh Framework Programme for Research and Technological
Development’,theEuropeanUnion'smaininstrumentforfundingresearchinEuroperunningfrom2007
to2013.FP7isalsodesignedtorespondtoEurope'semploymentneeds,competitiveness,andqualityof
life[c.f.http://ec.europa.eu/research/fp7/index_en.cfm].Theresearchproject‘RehabilitativeWayoutIn
ResponsivehomeEnvironments’(REWIRE)[45],whichisfundedbyFP7,aimstodevelop,integrate,and
fieldtestaninnovativevirtualreality-basedrehabilitationplatformforpeoplewithstroke.Theplatform
shouldallowpatients,dischargedfromthehospital,tocontinueintensiverehabilitationathomeunder
remote monitoring by the hospital. The main idea is to combine off-the-shelf components (e.g., the
trackingdeviceMicrosoftKinect[30],theforceplateTymo[57])inarobustandreliablewayandrender
asystemthatcanbeusedinthestrokepatients'homes.InthecontextoftheREWIREproject,theneed
hasbeenrecognizedforexergamesspecificallytargetedatwalkingrehabilitation[5].

31
When creating a virtual reality-based stroke treatment approach, the development of suitable
exergamesisundoubtedlyanimportantrequirement.Therehavebeen,todate,somestudiesthatdeal
with the development of videogames adequate for therapy purposes. Based on specific game design
principles,theyintendtoprovideengagingandchallengingtreatmentconditionstoachieveahighlevel
ofmotivation for rehabilitation practicing [1, 6, 7, 24, 33, 42, 58].Moreover, it is important that the
developed exergames are functionally integrated in a well-elaborated therapy program. On the one
hand,therehabilitationprogramshouldbeaimedatappropriaterehabilitationgoals.That is, itshould
be aimed at those goals that are considered to be essential for (andby) stroke victims.On the other
hand,therehabilitationprogramshouldbeconsistentwithestablishedtrainingprinciplestosuccessfully
reach these goals. In this article, we describe how tailored exergames for stroke patients can be
developedbasedonatheoreticalframework.Wewilldiscusskeyexergamedesignandtrainingprogram
contentconsiderations forpatientswithstroke,whichmaybetheoretically linkedto impairedwalking
performanceduetothestrokeevent.
3.2Stroke-inducedmotorimpairmentsandtheirtreatmentapproach
In the United States of America1, there are about 4.8million survivors of stroke of whom about 1.1
million suffer lasting functional disabilities [14]. The specific disabilities caused by stroke vary greatly
dependingonthebrainareathatisdamaged.Hemiparesis–aparalysisthatcharacteristicallyaffectsan
armandlegononesideofthebody–isoneofthemostcommonstroke-inducedimpairments[34]and
often leadstoanumberofnegativewalking-relatedconsequences.Thetypical ‘hemipareticgait’post-
strokeisassociatedwithareducedwalkingvelocity,cadenceandstridelength,withgaitasymmetry,and
withaprolongeddoublesupportandstancephasedurationofboth lowerextremities [15,26,27,44,
60].Itisforthisreasonthatmanystrokevictimsshowmarkeddeficitsinwalkingabilities[50].Thereis
generalagreementthatanassociationexistsbetweenthedegreeofindependentmobilityandqualityof
life [46, 53, 55]. Consequently, a central goal of stroke rehabilitation should be to improve gait
characteristics and to retrain the patient to the highest possible level of walking ability [16, 34]. The
findings demonstrated by Vincent et al. [59] confirmed the importance of enhancing stroke patients'
functionalmobility through rehabilitation. Vincent and colleagues [59] set out to reveal rehabilitation
needsfromtheperspectiveoffourdifferentpartiesinvolvedinthestrokerehabilitationprocess(stroke
patients,caregivers,healthprofessionals,andhealthcaremanagers)soastobetterplanthepost-stroke
treatment service. According to patients' statements – which, in our view, should have high priority
1This doctoral thesis considers the corrigendum to:Design considerations for a theory-driven exergame-basedrehabilitationprogramtoimprovewalkingofpersonswithstroke,EuropeanReviewofAgingandPhysicalActivity2014;11(2):119-12911(2):119-129

32
when designing rehabilitation programs – continued rehabilitation should focus primarily on motor
activities,suchaswalking.Patients'statementsthusfurtherhighlighttheimportanceofgaitrecovery.
Goodbalanceskillsareanimportantdeterminantofwalkingperformanceandimpairedbalanceabilityis
assumedtoberelatedtoadecreasedlocomotorfunction[18,61].Consideringthathemiparesisnotonly
affectsgaitcharacteristics,butalsooftenleadstodiminishedbalanceskills,apost-strokerehabilitation
programtargetingdeficitsinstaticanddynamicbalancemaybeaneffectivewaytorestoreindependent
functionalwalking.Inrecentyears,anotherfactorcontributingtowalkingrecoveryhasbeensuggested:
Several authorsnoted that task-relatedactivities lead to greater improvements inpost-strokewalking
competency thannon-task-relatedpractices [13,41,48]. Specifically, they suggested that intervention
protocolsthatincludeactualwalkingtasksimprovewalkingskillstoagreaterextentthanrehabilitation
programsthatdonot.Additionally,thereisrobustevidenceinthemotorlearningliteraturethatthebest
outcomes in termsof long-termretentionand transferof skillsareachievedwhenprinciplesofmotor
learning are integrated into treatment protocols. In rehabilitation, it is widely accepted that more
practiceisbetterandthatanintensestructuredtherapyprogramwithnumerousrepetitionsofvarious,
challenging tasks supports motor skill acquisition [38]. Specifically, two important elements in our
considerationare themotor learningprinciplesvariablepractice andprogression. Theseprinciplesare
known to positively affect gait rehabilitation and, hence, should be considered in developing a
rehabilitationprogram.
The literature todatehas found thatvariablepractice leads tobetter transferand retentionofmotor
skills than if a constant practice structure is used [22, 23, 31, 38, 51]. Insteadof performingone task
repeatedly and always in the same manner (constant practice), a specific task should be practiced
differentlythroughoutatreatmentsessionbyvaryingtheconditionsofpractice(variablepractice)[38].
Krakauer[31]–inhiscontributionpublishedintheCurrentOpinioninNeurology–statedthatvariable
practice is a fundamental principle in terms of retaining learning over time and that a consistent
agreement inthe literatureexists indicatingthatvariedpractice issuperiortorepetitive identicaltasks
when it comes to motor learning. The principle of progression holds that motor learning and
rehabilitationprogramsbenefit froma continuous adaptationof task difficulty to increasing skill level
[19]. For successful learning, an optimal challenging training situation should be given providing an
appropriate task difficulty level according to individuals' capacities [17]. Furthermore, it can be
hypothesizedthatthetrainingeffectswillbeenhancedwhenthelocomotorpracticegetscombinedwith
direct feedback; e.g., visual feedback. Visual feedback can be used to provide information about a

33
patient'smovementortheresultofamovementandisknowntopromoteposturalcontrolandstability
[2,19,25,52,61].
From the above, it follows that rehabilitation programs for stroke survivors are well-advised to train
balanceandwalkingskillsbymeansofavarietyofbalance-andwalking-specificexercises,thedifficulty
ofwhich isprogressivelyadapted topatients' skill level, in combinationwithdirectvisual feedbackon
performance.
Althoughpreviousstudieshaveemphasizedtheimportanceoftheory-basedpracticeandrehabilitation
[3, 11, 37, 56], there is still a lack of established concepts underlying the practical implementation of
motorskill learningprinciplesandtheories inrehabilitation.Adesirabletemplatewouldbeonethat is
simpleandfeasibleandthatfacilitatesthetask-specific,progressive,andvariabletrainingofbalanceand
walking skills. The motor skill taxonomy proposed by Gentile [21] seems to constitute just such a
templateforrehabilitationprogramsbecauseitprovidesatwo-dimensionalbasisforclassifyingavariety
of motor skills. Based on the above, the aim of this article is to develop and describe a tailored
exergame-basedstrokerehabilitationprogramthatisbasedonatheoreticalframework.
3.3Methods
Fourprevalentclassificationsystemsexistforidentifyingcommoncharacteristicsofmotorskills.Threeof
these categorize motor skills according to one common characteristic of the skill and lead to one-
dimension classification systems. In contrast, Gentile's taxonomy considers two general skill
characteristics and offers, therefore, a broader concept leading to a two-dimensional classification
system of motor skills. To highlight the high potential of Gentile's two-dimensional approach, it is
worthwhile to focus at first on the one-dimensional classification systems and discus some of their
limitations:
A description of these classification systems is given by Magill [35] (pp. 5–16). One one-dimension
classificationsystemdifferentiatesskillsdependingonthesizesoftheprimarymusclegroupsrequiredto
produceanaction(grossmotorskillsvs.finemotorskills).Asecondone-dimensionalsystemconsiders
thespecificityofamovement'sbeginningandendpoints tocategorizemotorskills (continuousmotor
skills vs. discrete motor skills). The third one-dimension classification system makes a distinction
according to the stability of the environmental context in which an action is being performed (open
motor skills vs. closed motor skills) [35, 38]. These one-dimensional classification systems raise the

34
problemthattheyfail tocapturethecomplexityofmanymotorskills [35]byonlyfocusingonasingle
aspectofmotorskills.
3.4Gentile'smotorskilltaxonomy
Gentilepresentedasystematicclassificationsystemtocategorizemotorskillsandmovementaccording
totwogeneraldimensionsofphysicalactions[32].Thefirstdimension,environmentalcontext,refersto
the environmental conditions towhich the performer has to react in order to successfully perform a
task. This dimension is characterized by two indicators: (a) regulatory conditions and (b) intertrial
variability.Theregulatoryconditionsindicaterelevantenvironmentalfeaturesthatconstrainmovement
execution and may either be stationary (stationary regulatory conditions) or moving (in-motion
regulatoryconditions).Withtheindicatorintertrialvariability,Gentile'staxonomydifferentiatesbetween
regulatory conditions that change between trials (intertrial variability) and those that do not (no
intertrialvariability).Theseconddimension,actionfunction, isalsocharacterizedbytwoindicators:(a)
bodyorientationand(b)objectmanipulation.Bodyorientationindicateswhetheranactionrequiresthe
performer to move from one location to another (body transport) or not (body stability). Object
manipulation indicateswhether an object has to be controlled during the action performance (object
manipulation)ornot(noobjectmanipulation).
Through the interaction of the resulting four environmental context characteristics and four action
functioncharacteristics,Gentiledefines16differentmotorskillcategoriesthatprovideacomprehensive
template toclassifymotorskills (Table3.1).The taxonomy isagoodmeansofbecomingawareof the
skill characteristics thatmakeskillsdistinct from,aswell as related to,other skills, and isanexcellent
guideforestablishingpracticeortrainingroutines[35].
AccordingtoGentile,theeasiestskillcategorycanbefoundatthetopleftposition(1A).Movingeither
rightwardordownward in the table renders theskill categorymoredifficult, so that themostdifficult
skillcategorycanbefoundatthebottomrightofthetable(4D).Fortheactionfunctiondimension,this
implies thatbody transport ismoredifficult thanbodystabilityandobjectmanipulationmoredifficult
than no object manipulation. Importantly, it also assumes a hierarchy in the action function
characteristics:skills involvingbodytransportbutnoobjectmanipulationaremoredifficult thanthose
involving objectmanipulations but not body transport. For the environmental context dimension, the
samepatternofprogressionisassumed.

35
Thus, Gentile's taxonomy allows a systematic progression in difficulty of motor tasks and meets the
demandofthemotor learningprincipleprogression.Moreover,eachofthe16categories isassociated
withuniquefeaturesbasedonthetwo-dimensionalapproachand,consequently,thetaxonomyinvolves
taskvariations.Obviously,Gentile'sclassificationsystemisconsistentwiththemotor learningprinciple
variablepractice.
Table3.1:Gentile’staxonomyofmotorskills[35].
There are several reasons for assuming that this taxonomy provides a valuable tool for developing a
theory-based rehabilitation program using virtual reality. Considering the explanations above, it is
evidentthatGentile'staxonomyis inaccordancewiththegenerallyacceptedmotor learningprinciples
progression and variable practice. The taxonomy provides a well-structured framework and the 4×4-

36
table can serve as a useful guide for preparing a systematically coherentmotor learning concept in a
simplemanner. For implementingGentile's taxonomy-based approach, exergamesmight demonstrate
anoptimalopportunityforprovidingbeneficialtreatmentconditions.Ontheonehand,aswereferred
above,there ishighpotential forcreatingamotivatingrehabilitationenvironmentusingvirtualreality.
Ontheotherhand, thetaxonomyseemssuitedforvirtual realityapplicationswheretheenvironment,
task complexity, and other contextual factors related to exercise performance can be manipulated.
Exergameparameterscanbeeasilymodifiedand,thereby,adjustedtothedemandsofthetaxonomy-
includedskillcategories.
3.5 Gentile's taxonomy-based exergames to improve stroke patients' balance and walking
skills
To provide a post-stroke rehabilitation program focused on improved balance skills in standing and
walking inaccordancewithGentile's framework,wedesigned sixbasicexergames.Basedon these six
basicexergames,wecreated16virtualrealityscenarios,eitherbymakinggameparametermodifications
or by substituting another basic game. Each scenario corresponds to one of the 16 skill categories
includedinthetaxonomy(Table3.2).
In accordance with a phased iterative approach suggested by Campbell et al. [8], this paper
demonstratesthetheoreticalphase–thefirststep–whendevelopingandevaluatingcomplexresearch-
basedinterventionsto improvehealth.Thus,asetofsixbasicexergamesappearstobeappropriate in
theresearchprocessofdesigninganexergame-basedstrokerehabilitationprogram.Itkeepsthenumber
ofgamesthathavetobedevelopedmanageableand–withthesamegamebeingimplementedacross
adjacentskillcategories–itrenderssystematicprogressionmorestraightforward.

37
Table3.2:ExergamescenarioscorrespondingtoGentile’sskillcategories.
Below,wewillbrieflydescribethecontentofeachofthe16skillcategories.
1A
Thefirstphaseoftherehabilitationprogramfocusesonthebasicphysicalskillofstandingquietly.Inthis
exergame, the patient is represented as a scarecrow avatar and is required to maintain a cursor
indicatingthebody'scenterofpressure(COP)withinapredefinedmarkedcircleonacomputerscreen
[39].Theexergamefocusesonstancesteadiness(sway)thatdemonstratesarelevantaspectrelatedto
an individual's balance ability [39].Due to hemiparesis after stroke, patients often showan increased
amountofposturalsway[39].

38
1B
Whereas the game Scarecrow described for skill category 1A demands a centered and stable COP
position, this game (called Blueberry collector) uses controlled COP displacements for successful
performance. This exergame targets stroke patients' dynamic stability, because subjects with
hemiparesisoftensufferfromreducedlimitsofstability[39].Thevirtualenvironmentrepresentsafield
ofblueberries,whichhavetobecollectedbyavirtualfarmer.Thefarmer'smovingiscontrolledbythe
patient'sweightshiftingtasksand,inthisway,theblueberriescanbegathered.Becausethepositionof
the berries in the field is fixed and unvarying between the different exergame trials, stationary
regulatory conditions are given and no intertrial variability. To meet the requirement of object
manipulation,avirtualbaskedfilledwithblueberriesisplacedonthefarmer'shead.Inordertoprevent
berriesfromfallingdown,thepatientmustadoptanidealuprightbodyposture.
1C
Previous exercise interventions have shown that stepping exercises indicate an effective treatment
method to improve postural stability and balance [9, 29, 40]. Accordingly, this exergame (called Frog
jumping) requires the control of the COP displacements during stepping movements. The virtual
environmentrepresentsapondwithseveralstonesplacedinit.Bydoingstepsinaspecificdirection,the
patientcancontrolafrogjumpingfromonestonetoanother.Avirtualarrowindicateswhichparticular
stonehas tobe targetedby thepatient. In accordancewith the taxonomy conditions, thepositionof
each stone within the pond is fixed (stationary regulatory conditions) and the order of the targeted
stonesunchangeablefromoneexergametrialtothenext(nointertrialvariability).
1D
According to Gentile's taxonomy, the skill category 1D can be seen as a progression of 1C. Thus, the
game Frog jumping described for 1C can be extended by integrating an object manipulation task.
Specifically, in this game, the virtual frog is wearing a crown and it is the patient's task to perform
steppingtaskswithanuprightbodypositioninordertokeepthevirtualcrowncorrectlypositioned.
2A
The gameBlueberry collector described above is not only adequate for skill category 1B, but also for
category2Abymakingsmalladaptations.Ontheonehand,thevirtualbasketonthefarmer'sheadhas
to be removed to get the condition no object manipulation. On the other hand, because intertrial
variabilityisrequired,thepositionoftheberriesvarieswithinexergametrials.

39
2B
Forskillcategory2B,theexergameBlueberrycollector forcategory2Acanbeextendedwithanobject
manipulation task. Thus, thevirtual farmer isbalancingabasketonhishead suchas in theexergame
describedforskillcategory1B.
2C
We use the game Frog jumping described for category 1C with the only modification of providing a
randomorderoftargetedstones–markedbythearrow–torealizeintertrialvariability.Consequently,
each time when the game has been played, a unique step performance pattern is required by the
patient.
2D
Tomeet the taxonomy requirements in skill category 2D, the game Frog jumping of category 2C can
easilybeadapted.Theonlymodificationthathastobedoneconcernstheneedforobjectmanipulation.
Hence,inthisgame,thefrogiswearingacrownforwhichthepatienthastocontrolhisorherposition
whileplayingthegame.
3A
Forskillcategory3A,wecreatedagamecalledTractordriver.Theexergamepresentsamovingtractor
forwhichthedrivingspeedisdefaultedbythevideogame.Thedirectionofdrivingiscontrolledbythe
patient's weight shifting movements. When playing this exergame, the ability to move the COP in a
standing posture without loss of balance (dynamic stability) is being trained [39]. Specifically, the
purposeofthisgameistoforkuphaybalesthroughdirectingthemovingtractorfromonehaybaleto
another.Thehaybalesarewidelyspreadoverthesoil.Consideringthatthespeedofthemovingtractor
is default and cannot bemanipulated by the patient themselves, in-motion regulatory conditions are
given.There isa fixedpositionofeachhaybaleunchangeable fromoneexergametrial to thenext to
ensurenointertrialvariability.
3B
Inthisexergame(calledFruitcatcher),thepatientisrepresentedasanavatarbalancingafruitbasketon
thehead.Virtual apples are fallingdown froma tree (in-motion regulatory conditions) that shouldbe
caught by the basket. The patient has to perform target-oriented COP shifts to get an optimal avatar
positionand theapplesare falling into thebasket. Thisexergame focusesondynamic stabilitydue to
controlled weight shifting movements to selected targets. For presenting no intertrial variability, the
gameparametersarealwaysthesame,evenwhenthegameisrepeatedlyplayed.

40
3C
According to Gentile's taxonomy, this exergame (called Worm hurdler) requires stepping tasks.
Specifically, the patient represented as an avatar has to overstep a crawling worm coming closer
alternately from the right and the left side (in-motion regulatory conditions). The parameters of the
gameareunchangeableand,thus,nointertrialvariabilityisgiven.
3D
TheexergameWormhurdlerdescribedin3Ccaneasilybemodifiedforskillcategory3D.Byintegratinga
virtualwaterjarthathastobebalancedontheavatar'shead,anobjectmanipulationtaskisintegrated.
Toavoidwaterspillage,thepatienthastoadoptanidealuprightbodyposture.
4A
For skill category4A,weadapted thegameTractordriver described for category3Aby implementing
intertrialvariability.Specifically,toprovidevaryingregulatoryconditions,thehaybalepositionschange
fromoneexergametrialtoanother.
4B
The exergame Fruit catcher described for skill category 3B needed a slight modification to meet the
categoryrequirements for4B. In thisgame, therearenotonly fallingappleswhichhavetobecaught,
but various kinds of fruits. On the one hand, the fruits have different sizes and, on the other hand,
differentfallingspeeds.Obviously,intertrialvariabilityisgiven.
4C
WhenplayingthegameWormhurdlerdesignedforcategory3C,butwithchangingregulatoryconditions
betweentheexergametrials, intertrialvariability isensured.Accordingly, in thisgame, thewormsare
crawlingwithvaryingspeedsandarecomingeitherfromtherightortheleftsideinrandomorder.
4D
Forintegratinganobjectmanipulationtask,theexergameWormhurdlerdescribedforskillcategory4C
canbeadvancedbybalancingavirtualwaterjarontheavatar'shead.Consequently,whileoverstepping
the randomly approaching crawling worms, the patient has to adopt an ideal upright body position
ensuringthatnowaterisspillingout(fromthejar).
3.6Practicalapplicationofthetaxonomy-basedrehabilitationprogramusingexergames
When implementing a therapeutic program to improve stroke victims’ motor skills, therapists must
selectexercisesthataretailoredtothedemandsoftheindividualpatient.Toachieveoptimaloutcomes

41
inrehabilitation,theactivitiesshouldbematchedtoapatient'sfunctionalabilitiesandlimitations.Ina
well-elaborated training plan, the (exercise) tasks which have to be performed should maintain an
optimal challenge for the patient [7, 19].Obviously, for providing a perfectly tuned exercise difficulty
levelatanypointintimethroughouttherehabilitationperiod,modifyingthetherapyplanisanessential
need and an ongoing process.When a patient is making progress, more challenging tasks should be
involved into the rehabilitation program. For selecting functionally appropriate activities during
rehabilitation,wehighlightthepracticalvalueofusingGentile'staxonomy.Basedontheconsideration
thatthetaxonomy-basedskillcategoriespresentastructuregoingfromsimpletocomplexmotortasks,
weprovidea formalprocedure forguidingpatients fromthetop leftof the table to thebottomright.
CloserinspectionofTable3.1revealsthatthetaxonomycanbedividedintosevendifficultylevels.More
specifically,startingfrom1ofthe16skillcategories,acategory-basedprogressionintaskdifficultycan
beachievedeitherthroughahorizontalshifttotherightoraverticalshiftdownward.Accordingly,seven
levels of difficulty can be distinguishedwhich define a progressive increase of complexity in diagonal
direction(Table3.3).
Consideringtheallocationoftheskillcategoriestooneofthesevendifficultylevels,Gentile'staxonomy
offers a simple and easy-to-followway for incorporating an ongoing progression into a rehabilitation
process.Specifically,forselectingappropriateactivitiesthatproviderehabilitationattheoptimallevelof
challenge,weproposethefollowingprocedure:Apatientmayonlymoveuponelevelofdifficultywhen
allskillcategorieswithinthecurrentlevelarecompleted.Forclarification,beginningwithskillcategory
1Aindifficultylevel1,thepatientisrequiredtomovetotheskillcategoriesindifficultylevel2(i.e.,1B
and2A)assoonascategory1Aissuccessfullyperformed.Withinlevel2,patientsandtreatingtherapists
arefreetochoosetheorderofexecutionofthebelongingskillcategories.Onceapatientiscapableto
performboth skill categories1Band2A successfully, thenextdifficulty level3has tobe incorporated
into rehabilitation.Thisprocedure canbe continueduntil thepatient finally achieves skill category4D
and, consequently, the highest level of difficulty (i.e., level 7). In this way, challenging situations are
ensuredatanypointintimeduringrehabilitationandthepatientsareencouragedtoexercisetowards
theirfunctionallimits.Followingtheproceduresuggestedtoguidesomeone'stherapyplan,oneensures
that the selectionof skill categories is constrained.Due to this constraint, a variationof both general
dimensions defined by Gentile's taxonomy will be considered during the rehabilitation process.
Accordingly,theprocedurepreventsaskillcategory-basedprogressiononlyinonedirectionandincludes
themodificationofboththeenvironmentalcontextandtheactionfunctioncharacteristics.
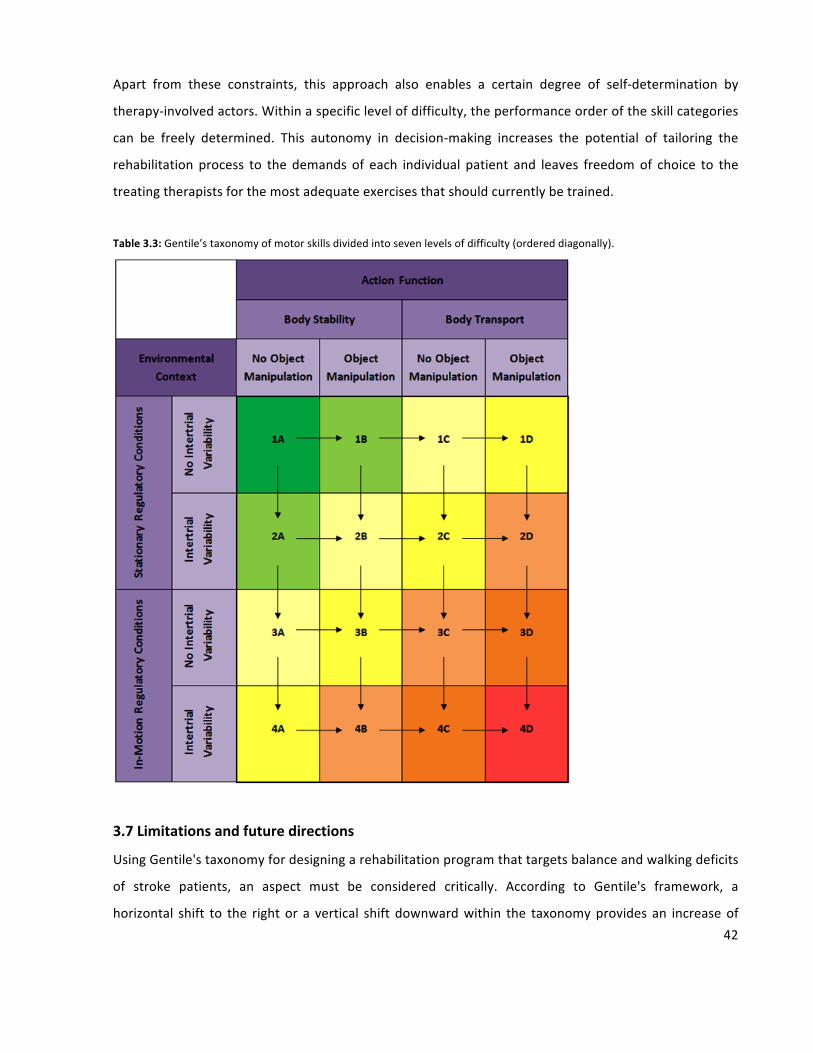
42
Apart from these constraints, this approach also enables a certain degree of self-determination by
therapy-involvedactors.Withinaspecificlevelofdifficulty,theperformanceorderoftheskillcategories
can be freely determined. This autonomy in decision-making increases the potential of tailoring the
rehabilitation process to the demands of each individual patient and leaves freedomof choice to the
treatingtherapistsforthemostadequateexercisesthatshouldcurrentlybetrained.
Table3.3:Gentile’staxonomyofmotorskillsdividedintosevenlevelsofdifficulty(ordereddiagonally).
3.7Limitationsandfuturedirections
UsingGentile'staxonomyfordesigningarehabilitationprogramthattargetsbalanceandwalkingdeficits
of stroke patients, an aspect must be considered critically. According to Gentile's framework, a
horizontal shift to the rightor a vertical shift downwardwithin the taxonomyprovides an increaseof

43
taskcomplexity.However,whenwefocusonamotortasksuchasstandingstillononeleg,apotential
inconsistency in Gentile's approach emerges. Standing still on one leg can be categorized by the
taxonomydimensionbodystabilitythatrepresentslesscomplextasksthanmotorskillsthatrequirebody
transport (e.g.,walking). Inour view,maintaining aone-leg stancepositionneeds goodbalance skills.
Therefore, this activitymight beperceivedby some strokepatients as an advancedmotor taskwhich
challenges them more than a body transport activity. Furthermore, where this theoretical approach
focusedonthe‘generalstrokepatientpopulation’,weareawareofthefactthatdifferentaccompanying
diseases and impairments; e.g., dizzinessormuscleweaknessdue to stroke,may causedifferences in
howpatientsperceive tasks asbeingmoreor lessdifficult. It canbehypothesized that somepatients
have more difficulty maintaining a given posture without loss of balance whereas others experience
performingabodytransporttaskasmoredifficult.Wethink,however,thatthesepotentialdifferences
mayberesolvedbycliniciansthattreatandmonitorpatientsanddecide,togetherwiththepatientsand
accordingtheirskilllevels,howandwhentoprogressthroughthetaxonomy.Itiscleartousthatseveral
pilot studies assessing feasibility and usability in several reference and subpopulations are needed as
necessary next step in our program development process. Feasibility studies are comparative
randomized trials designed to provide preliminary evidence on the clinical efficacy of a drug or
intervention [54]. Usability evaluation is away to ensure that interactive systems are adapted to the
usersandshouldbepartofafundamentalstepintheuser-centereddesignprocess[4].
In thispaper,weelucidate the theoreticalbasis fora theory-driven rehabilitationprogramto improve
stroke sufferers' balance skills and walking capability using exergames. According to the framework
proposed by Campbell et al. [8], investigating relevant theory prior to an exploratory trial is of great
importance.Considering the theoretical knowledgegathered,anoptimal study interventiondesign for
pilot studies can be worked out that focus on the relevance and effectiveness of the rehabilitation
programsuggested.Dependingontheusabilityandfeasibilitytestingresultsobtained,refinementsand
extensionsoftheexergamescanbemadeandthepresentsetofsixbasicexergamesmaybeextended
to amaximumof 16 different exergames.Hence, a comprehensive and practical theory-driven stroke
rehabilitationprogrambasedonGentile'staxonomycanbeachieved.
3.8Conclusion
Withstroke,thechangesinthecentralnervoussystemandlifestylemayimpairanindividual'sabilityto
regainand/ormaintaincertainlevelsofmotorfunctioning.Byusingvirtualreality,wemightbeableto

44
offer continued rehabilitation in an attractive andmeaningful way. Specific targeted exergames have
been designed that aim to minimize stroke-induced walking impairments. Considering the aim of
presenting a well-elaborated training concept with a strong theoretical rationale, in this paper we
demonstrate thatGentile's taxonomypresentsa feasible templateprovidingassistance fordeveloping
and implementing a theory-driven rehabilitation program. The motor skill taxonomy suggested by
Gentile defines two general dimensions and structures a table that consists of 16 different skill
categories(Table3.1).Ontheonehand,basedontheseskillcategories,thetaxonomyprovidesvariable
training scenarios. Thus, a therapy programwhichmeets the demand of themotor learning principle
variable practice can be created. On the other hand, the taxonomy allows a systematic progression
during the rehabilitation process. Accordingly, themotor learning principle of progression is explicitly
considered. Due to the advantages of Gentile's two-dimensional approach, the taxonomy suits our
purposes and was used as underlying framework to build up a post-stroke exergame rehabilitation
program for enhancing balance and walking skills. Based on the literature reviewed here, clinical
approachestomaintainingandimprovingphysicalfunctioningoverlongertimeperiodsinpersonswith
strokemaybecombinedwithnovelexergame-basedapproachesthatsustainphysicalfunctioning.
Authors’contributions
SWperformed literature reviewanddesign considerations and contributed towriting themanuscript.
RvdL performed design considerations and contributed to writing the manuscript. EDdB initiated the
study, assisted in both literature review and design considerations and contributed to writing the
manuscript.Allauthorsreadandapprovedthefinalmanuscript.
The authors declare that the submitted paper, the data, and the results have not been published
anywherebefore.
Acknowledgments
This work was partially supported by the REWIRE project (www.rewire-project.eu), funded by the
EuropeanCommissionundertheFP7frameworkwithcontract287713.
Conflictofintereststatement
Seline Wüest, Rolf van de Langenberg, and Eling D. de Bruin declare that they have no conflict of
interest.

45
References
1. AdamovichSV,MeriansAS,BoianR,LewisJA,TremaineM,BurdeaGS,RecceM,PoiznerH(2005)Avirtual
reality-basedexercisesystemforhandrehabilitationpost-stroke.Presence-TeleopVirt14(2):161-174.doi:10.1162/1054746053966996
2. AlahakoneAU,SenanayakeSA(2010)Areal-timesystemwithassistivefeedbackforposturalcontrolinrehabilitation.Mechatronics,IEEE/ASMETrans15(2):226–233.
3. AskimT,IndredavikB,EngenA,RoosK,AasT,MorkvedS(2012)Physiotherapyafterstroke:towhatextentistask-orientedpracticeapartofconventionaltreatmentafterhospitaldischarge?PhysiotherTheoryPract.doi:10.3109/09593985.2012.734008
4. BastienJMC(2010)Usabilitytesting:areviewofsomemethodologicalandtechnicalaspectsofthemethod.IntJMedInform79(4):E18–E23.doi:10.1016/j.ijmedinf.2008.12.004
5. BorgheseNA,PirovanoM,LanziPL,WüestS,deBruinED(2013)Computationalintelligenceandgamedesignforeffectiveat-homestrokerehabilitation.GamesHealthJ2(2):81–88.doi:10.1089/g4h.2013.0073
6. BurkeJW,McNeillMDJ,CharlesDK,MorrowPJ,CrosbieJH,McDonoughSM(2009)Optimisingengagementforstrokerehabilitationusingseriousgames.VisualComput25(12):1085–1099.doi:10.1007/s00371-009-0387-4
7. CameiraoMS,BadiaSB,OllerED,VerschurePF(2010)NeurorehabilitationusingthevirtualrealitybasedRehabilitationGamingSystem:methodology,design,psychometrics,usabilityandvalidation.JNeuroengRehabil7:48.doi:10.1186/1743-0003-7-48
8. CampbellM,FitzpatrickR,HainesA,KinmonthAL,SandercockP,SpiegelhalterD,TyrerP(2000)Frameworkfordesignandevaluationofcomplexinterventionstoimprovehealth.BrMedJ321(7262):694–696.doi:10.1136/bmj.321.7262.694
9. CartyCP,CroninNJ,LichtwarkGA,MillsPM,BarrettRS(2012)Mechanismsofadaptationfromamultipletoasinglesteprecoverystrategyfollowingrepeatedexposuretoforwardlossofbalanceinolderadults.PLoSONE7(3):e33591.
10. CohenJ(1988)Statisticalpoweranalysisforthebehavioralsciences.Routledge,NewYork.11. deBruinED,vanhetReveE,MurerK(2013)Arandomizedcontrolledpilotstudyassessingthefeasibilityof
combinedmotor-cognitivetraininganditseffectongaitcharacteristicsintheelderly.ClinRehabil27(3):215–225.doi:10.1177/0269215512453352
12. deBruinED,SchoeneD,PichierriG,SmithST(2010)Useofvirtualrealitytechniqueforthetrainingofmotorcontrolintheelderly.Sometheoreticalconsiderations.ZGerontolGeriatr43(4):229–234.doi:10.1007/s00391-010-0124-7
13. DeanCM,RichardsCL,MalouinF(2000)Task-relatedcircuittrainingimprovesperformanceoflocomotortasksinchronicstroke:arandomized,controlledpilottrial.ArchPhysMedRehab81(4):409–417.
14. DeJongG,HornSD,ConroyB,NicholsD,HealtonEB(2005)Openingtheblackboxofpoststrokerehabilitation:strokerehabilitationpatients,processes,andoutcomes.ArchPhysMedRehab86(12):S1–S7.doi:10.1016/j.apmr.2005.09.003
15. DicksteinR,DunskyA,MarcovitzE(2004)Motorimageryforgaitrehabilitationinpost-strokehemiparesis.PhysTher84(12):1167–1177.
16. DombovyML,SandokBA,BasfordJR(1986)Rehabilitationforstroke—areview.Stroke17(3):363–369.17. EliassonAC,Krumlinde-sundholmL,ShawK,WangC(2005)Effectsofconstraint-inducedmovement
therapyinyoungchildrenwithhemiplegiccerebralpalsy:anadaptedmodel.DevMedChildNeurol47(4):266–275.
18. EngJJ,TangPF(2007)Gaittrainingstrategiestooptimizewalkingabilityinpeoplewithstroke:asynthesisoftheevidence.ExpertRevNeurother7(10):1417–1436.doi:10.1586/14737175.7.10.1417
19. FellDW(2004)Progressingtherapeuticinterventioninpatientswithneuromusculardisorders:aframeworktoassistclinicaldecisionmaking.JNeurolPhysTher28(1):35.doi:10.1097/01.NPT.0000284776.32802.1b

46
20. GeijtenbeekT,SteenbrinkF,OttenB,Even-ZoharO(2011)D-flow:immersivevirtualrealityandreal-timefeedbackforrehabilitation.In:Proceedingsofthe10thInternationalConferenceonVirtualRealityContinuumandItsApplicationsinIndustry,HongKong.ACM,pp201–208.doi:10.1145/2087756.2087785
21. GentileA(2000)Skillacquisition:action,movement,andneuromotorprocesses.MovSciFoundPhysTherRehabil2:111–187.
22. GuadagnoliMA,LeeTD(2004)Challengepoint:aframeworkforconceptualizingtheeffectsofvariouspracticeconditionsinmotorlearning.JMotBehav36(2):212–224.doi:10.3200/Jmbr.36.2.212-224
23. HallKG,MagillRA(1995)Variabilityofpracticeandcontextualinterferenceinmotorskilllearning.JMotBehav27(4):299–309.
24. HarleyL,RobertsonS,GandyM,HarbertS,BrittonD(2011)Thedesignofaninteractivestrokerehabilitationgamingsystem.Human-ComputInteractUsersApplPtIv6764:167–173.
25. HatzitakiV,VoudourisD,NikodelisT,AmiridisI(2009)Visualfeedbacktrainingimprovesposturaladjustmentsassociatedwithmovingobstacleavoidanceinelderlywomen.GaitPosture29(2):296–299.
26. HornbyTG,StraubeDS,KinnairdCR,HolleranCL,EchauzAJ,RodriguezKS,WagnerEJ,NarducciEA(2011)Importanceofspecificity,amount,andintensityoflocomotortrainingtoimproveambulatoryfunctioninpatientspoststroke.TopStrokeRehabil18(4):293–307.doi:10.1310/Tsr1804-293
27. HsuAL,TangPF,JanMH(2003)Analysisofimpairmentsinfluencinggaitvelocityandasymmetryofhemiplegicpatientsaftermildtomoderatestroke.ArchPhysMedRehabil84(8):1185–1193.
28. JackD,BoianR,MeriansAS,TremaineM,BurdeaGC,AdamovichSV,RecceM,PoiznerH(2001)Virtualreality-enhancedstrokerehabilitation.IeeeTNeurSysReh9(3):308–318.
29. KennedyMW,SchmiedelerJP,CrowellCR,VillanoM,StriegelAD,KuitseJ(2011)EnhancedfeedbackinbalancerehabilitationusingtheNintendoWiiBalanceBoard.In:e-HealthNetworkingApplicationsandServices(Healthcom),201113thIEEEInternationalConferenceon.IEEE,pp162–168.
30. KinectforWindows.http://www.microsoft.com/en-us/kinectforwindows.Accessed12Oct201331. KrakauerJW(2006)Motorlearning:itsrelevancetostrokerecoveryandneurorehabilitation.CurrOpin
Neurol19(1):84–90.32. LagunaPL(2008)Taskcomplexityandsourcesoftask-relatedinformationduringtheobservational
learningprocess.JSportSci26(10):1097–1113.doi:10.1080/0264041080195656933. LangeB,FlynnS,RizzoA(2009)Initialusabilityassessmentofoff-the-shelfvideogameconsolesforclinical
game-basedmotorrehabilitation.PhysTherRev14(5):355–363.34. MackoRF,HaeuberE,ShaughnessyM,ColemanKL,BooneDA,SmithGV,SilverKH(2002)Microprocessor-
basedambulatoryactivitymonitoringinstrokepatients.MedSciSportExer34(3):394–399.35. MagillRA(2004)Motorlearningandcontrol:conceptsandapplications,7thedn.McGraw-Hill,Boston.36. MeriansAS,JackD,BoiauR,TremaineM,BurdeaGC,AdamovichSV,RecceM,PoiznerH(2002)Virtual
realityaugmentedrehabilitationforpatientsfollowingstroke.PhysTher82(9):898–915.37. MulderT(1991)Aprocess-orientedmodelofhumanmotorbehavior—towardatheory-based
rehabilitationapproach.PhysTher71(2):157–164.38. MuratoriLM,LambergEM,QuinnL,DuffSV(2013)Applyingprinciplesofmotorlearningandcontrolto
upperextremityrehabilitation.JHandTher26(2):94–103.39. NicholsDS(1997)Balanceretrainingafterstrokeusingforceplatformbiofeedback.PhysTher77(5):553–
558.40. NnodimJO,StrasburgD,NaboznyM,NyquistL,GaleckiA,ChenS,AlexanderNB(2006)Dynamicbalance
andsteppingversusTaiChitrainingtoimprovebalanceandsteppinginatriskolderadults.JAmGeriatrSoc54(12):1825–1831.
41. O'DellMW,LinCCD,HarrisonV(2009)Strokerehabilitation:strategiestoenhancemotorrecovery.AnnuRevMed60:55–68.doi:10.1146/annurev.med.60.042707.104248
42. PapangelisA,MouchakisG,TexasAB,KosmopoulosD,KarkaletsisV,MakedonF(2012)Agamesystemforremoterehabilitationofcerebralpalsypatients.In:Proceedingsofthe5thInternationalConferenceonPervasiveTechnologiesRelatedtoAssistiveEnvironments.ACM,p19.
43. PirovanoM,MainettiR,Baud-BovyG,LanziPL,BorgheseNA(2012)Self-adaptivegamesforrehabilitationathome.In:ComputationalIntelligenceandGames(CIG),2012I.E.ConferenceonIEEE.pp179–186.

47
44. PuhU,BaerG(2009)Acomparisonoftreadmillwalkingandovergroundwalkinginindependentlyambulantstrokepatients:apilotstudy.DisabilRehabil31(3):202–210.doi:10.1080/09638280801903039
45. REWIRE—RehabilitativeWayoutinResponsiveHomeEnvironments.http://www.rewire-project.eu/about-rewire.Accessed22Feb2013
46. RichardsCL,MalouinF,WooddauphineeS,WilliamsJI,BouchardJP,BrunetD(1993)Task-specificphysicaltherapyforoptimizationofgaitrecoveryinacutestrokepatients.ArchPhysMedRehab74(6):612–620.
47. RizzoA,KimGJ(2005)ASWOTanalysisofthefieldofvirtualrealityrehabilitationandtherapy.Presence-TeleoperatorsVirtualEnviron14(2):119–146.doi:10.1162/1054746053967094
48. SalbachNM,MayoNE,Wood-DauphineeS,HanleyJA,RichardsCL,CoteR(2004)Atask-orientatedinterventionenhanceswalkingdistanceandspeedinthefirstyearpoststroke:arandomizedcontrolledtrial.ClinRehabil18(5):509–519.doi:10.1191/0269215504cr763oa
49. SchultheisMT,RizzoAA(2001)Theapplicationofvirtualrealitytechnologyinrehabilitation.RehabilPsychol46(3):296–311.
50. ShaughnessyM,MichaelKM,SorkinJD,MackoRF(2005)Stepsafterstroke—capturingambulatoryrecovery.Stroke36(6):1305–1307.doi:10.1161/01.Str.0000166202.00669.D2
51. SheaCH,KohlRM(1990)Specificityandvariabilityofpractice.ResQExercSport61(2):169–177.52. SrivastavaA,TalyAB,GuptaA,KumarS,MuraliT(2009)Post-strokebalancetraining:roleofforce
platformwithvisualfeedbacktechnique.JNeurolSci287(1):89–93.53. Teixeira-SalmelaLF,OlneySJ,NadeauS,BrouwerB(1999)Musclestrengtheningandphysicalconditioning
toreduceimpairmentanddisabilityinchronicstrokesurvivors.ArchPhysMedRehab80(10):1211–1218.54. ThabaneL,MaJ,ChuR,ChengJ,IsmailaA,RiosLP,RobsonR,ThabaneM,GiangregorioL,GoldsmithCH
(2010)Atutorialonpilotstudies:thewhat,whyandhow.BMCMedResMethodol10:1.doi:10.1186/1471-2288-10-1
55. TilsonJK,SettleSM,SullivanKJ(2008)Applicationofevidence-basedpracticestrategies:currenttrendsinwalkingrecoveryinterventionspoststroke.TopStrokeRehabil15(3):227–246.doi:10.1310/Tsrl503-227
56. Tudor-LockeCE,MyersAM,RodgerNW(2001)Developmentofatheory-baseddailyactivityinterventionforindividualswithtype2diabetes.DiabetesEduc27(1):85–93.
57. Tyromotion.http://tyromotion.com/en/products/tymo/overview.Accessed12Oct201358. UzorS,BaillieL(2013)Exploring&designingtoolstoenhancefallsrehabilitationinthehome.In:
ProceedingsoftheSIGCHIConferenceonHumanFactorsinComputingSystems,2013.ACM,pp1233–1242.
59. VincentC,DeaudelinI,RobichaudL,RousseauJ,ViscogliosiC,TalbotLR,DesrosiersJ(2007)Rehabilitationneedsforolderadultswithstrokelivingathome:perceptionsoffourpopulations.BMCGeriatr7:20.doi:10.1186/1471-2318-7-20
60. VonschroederHP,CouttsRD,LydenPD,BillingsE,NickelVL(1995)Gaitparametersfollowingstroke—apracticalassessment.JRehabilResDev32(1):25–31.
61. YavuzerG,EserF,KarakusD,KaraoglanB,StamHJ(2006)Theeffectsofbalancetrainingongaitlateafterstroke:arandomizedcontrolledtrial.ClinRehabil20(11):960–969.
62. ZydaM(2005)Fromvisualsimulationtovirtualrealitytogames.Computer38(9):25–32.

48
4
Usability and effects of an exergame-based balance training program
WüestS1,BorgheseNA2,PirovanoM2,MainettiR2,vandeLangenbergR1,deBruinED1,3,4
1InstituteofHumanMovementSciencesandSport,DepartmentofHealthSciencesandTechnology,ETH
Zurich,Switzerland
2DepartmentofComputerScience,UniversityofMilan,Italy
3DepartmentofEpidemiology,CAPHRISchoolforPublicHealthandPrimaryCareand4Centrefor
EvidenceBasedPhysiotherapy,MaastrichtUniversity,Netherlands
GamesforHealthJournal2014;3(2):106-114

49
Abstract
Background:Post-strokerecoverybenefitsfromstructured,intense,challenging,andrepetitivetherapy.
Exergames have emerged as promising to achieve sustained therapy practice and patientmotivation.
Thisstudyassessedtheusabilityandeffectsofexergamesonbalanceandgait.
SubjectsandMethods:Sixteenelderlyparticipantswereprovidedwiththestudyinterventionbasedon
fivenewlydevelopedexergames.Theparticipantswererequiredtoattend36trainingsessions; lasting
for20minuteseach.Adherence,attritionandacceptancewereassessedtogetherwith(1)BergBalance
Scale,(2)7-mTimedUpandGo,(3)ShortPhysicalPerformanceBattery,(4)forceplatformstancetests,
and(5)gaitanalysis.
Results: Thirteen participants completed the study (18.8 percent attrition), without missing a single
trainingsession(100percentadherence).Participantsshowedhighacceptanceoftheintervention.Only
minoradaptationsintheprogramwereneededbasedontheusers’feedback.Nochangesincenterof
pressure area during quiet stance on both stable and unstable surfaces and no changes of walking
parametersweredetected.ScoresfortheBergBalanceScale(p=0.007;r=0.51),the7-mTimedUpand
Go (p = 0.002; r = 0.56), and the Short Physical Performance Battery (p = 0.013; r = 0.48) increased
significantlywithmoderatetolargeeffectsizes.
Conclusion: Participants evaluated the usability of the virtual reality training intervention positively.
Resultsindicatethattheinterventionimprovesgait-andbalance-relatedphysicalperformancemeasures
inuntrainedelderly. Thepresent resultswarrant a clinical explorative study investigating theusability
andeffectivenessoftheexergame-basedprograminstrokepatients.

50
4.1Introduction
Acute stroke rehabilitation servicesare limited–primarilybecauseof cost constraints [1]–andmany
individuals return home with residual gait impairment [2]. The decision to discharge patients from
furthertherapyisoftenjustifiedwitha‘plateau’inmotorrecovery[3].However,furtherfunctionalgains
afteracuterehabilitationarepossible,eveninthechronicstage[1,4].
Following a stroke, approximately 80 percent of patients experience hemiparesis accompanied by
considerable walking deficits [5]. The typical ‘hemiplegic gait’ post-stroke is associated with several
negativeconsequences(e.g.,gaitasymmetry,reducedwalkingvelocity,cadence,andstridelength)[5-9].
Sixmonthspost-stroke,one-thirdofelderlystrokesurvivorsarenotabletowalkindependently[10].
An intense, structured therapy program offering numerous repetitions of various, challenging tasks
improves motor skills [11]. For best recovery results, a rehabilitation program should be conducted
regularly over an extended period of time.When patients find a treatment program enjoyable, their
willingnesstokeepat it is increased.Ahighlevelofmotivationshouldleadtohighadherenceandlow
attritionandhencepositivelyaffecttreatmentoutcomes[12].
Virtual reality applications in health care have recently received considerable attention. Virtual reality
canbeusedtoprovideengagingscenariosandimproveadherencetotherapy[13-17].Videogamesare
most practical and effective in rehabilitation when they have been specifically designed for therapy
purposes [18-20].Given the importanceof gait recoverypost-stroke, games shouldbeaimed towards
walkingrecovery.Anadditionaladvantageofvideogame-basedprogramsisthattheycanbeperformed
independentlyathomewithminimalequipment[16].
The researchproject ‘RehabilitativeWayout InResponsivehomeEnvironments’ (REWIRE) [21], funded
by FP7, created such a rehabilitation program based on exergames. Exergames are defined as “any
number of types of video games/multimedia interactions that require the game player to physically
moveinordertoplay”[22].FiveexergameshavebeendevelopedinthecontextoftheREWIREproject–
bygamedevelopersincollaborationwithhumanmovementscientistsandrehabilitationspecialists.The
processforgamedevelopmentwithinatheoreticalframeworkhasbeendescribedelsewhere[23].The
underlying exercises – specifically targeting balance and walking recovery – were designed to be
performedindependentlyathomeandremotelymonitoredbyhealthcareprofessionals.Moreover,the
rehabilitationprogramexplicitlyconsideredvariablepracticeandindividuallytailoredprogression,hence
keepingparticipantsengagedandappropriatelychallenged[18,23,24].

51
InaccordancewiththephasediterativeapproachsuggestedbyCampbelletal.[25],thisarticleaimsto
evaluate(1)theusabilityoftherehabilitationprogramintermsofacceptance,adherence,andattrition
and(2)theeffectoftheprogramonmeasuresofbalanceandgaitinuntrainedhealthyelderly.
4.2Subjectsandmethods
Studydesign
Weassessedusabilitybymeansofauser-centeredinteractiondesign.TheETHZurichEthicsCommittee
grantedethicalapproval (protocolnumberEK2013-N-12).Allparticipantswere fully informedprior to
participationandsignedaconsentform.
Participants
Usabilityandeffectswereassessedinanuntrainedelderlyconveniencesample,inwhichsomebalance
andgait impairmentscanbeassumed[26-30].SixteenparticipantswererecruitedinthecityofZurich,
Switzerland, through contact persons of different institutions. Participantswere included if they lived
independently,wereolderthan64yearsofage,wereabletowalk independently for20m,andhada
Mini-MentalStateExaminationscoreofatleast22.Excludedwereindividualswith(1)acuteorunstable
chronic diseases, (2) rapidly progressingor terminal illnesses, (3)Alzheimer’s diseaseor dementia, (4)
otherseverehealthproblems,and/or(5)arecentheadinjury.
Intervention
The intervention program consisted of exergame-based balance training performed while standing
directlyonaforceplatform(TymoplatebyTyromotion,Graz,Austria)[31]oronacompliantfoammat
placedontopofthisplatform.Theinterventionwasperformedthreetimesperweekforaperiodof12
weeks for a total of 36 sessions. Each one-on-one sessionwas partitioned in three parts: 10minutes
training,10minutesbreak,and10minutes training.Allparticipantswereexpected tocompleteall36
sessions while being monitored by an instructor, who systematically observed them throughout the
intervention.Participantswereencouragedto‘thinkaloud’whileoperatingthesoftwareandplayingthe
exergames.Accordingly,anyexpressedcommentsfromtheparticipantsrelatedtotheirdemandswere
documentedbytheinstructorinwritingtoidentifybothproblemareasandwhatpeoplelike.Theaimof
thisprocedurewastoassessstrengthsandweaknessesoftheexergame-basedtrainingprogramonline

52
inarealisticsetting.Consequently,basedonparticipants’feedback,desiredexergameadaptationscould
becarriedout.
Exergames
Asetof fiveexergames– fourof themwithdifferent levelsofdifficulty (Table4.1givesdetails)–was
used for the intervention. In each exergame, a therapist avatar provided real-time feedback. The
exergamesaimedtotrainquietstance (‘Scarecrow’ [Figure4.1]),mediolateralweightshifting (‘Tractor
driver’[Figure4.2]and‘Fruitcatcher’[Figure4.3]),mediolateralweightshiftingcombinedwithsingleleg
stance (‘Wormhurdler’ [Figure 4.4]), andmediolateralweight shifting combinedwith anteroposterior
weightshifting(‘Mixsoup’[Figure4.5]).Adetaileddescriptionofthegamescanbefoundelsewhere[18,
23,24].
Table4.1:Exergamedifficultylevels.
Scarecrow Tractordriver Fruitcatcher Wormhurdler Mixsoup
Nodifficultyleveladaptation
Difficultyleveladaptation:
speedofthemovingtractor
Difficultyleveladaptation:
fruitfallingfrequency&fruitfallingrange
Difficultyleveladaptation:speedofthecrawlingworm
Difficultyleveladaptation:
lifespanofthebubbles
Primaryoutcomes
Acceptance of the training technology. An abridged version [32] of the technology acceptancemodel
(TAM)questionnaireevaluatedparticipants’perceivedacceptanceoftheinterventionpost-training[33-
35](Figure4.6).
Responseswere recorded using a 7-point Likert scale ranging from ‘strongly disagree’ (rated as 1) to
‘stronglyagree’(ratedas7).
Attrition and adherence. For attrition, the number of participants lost during the intervention was
recorded.Foradherence,participants’engagementwiththeinterventionwasassessed.Adherencewas
calculatedasthenumberofcompletedtrainingsessionsasapercentageofthemaximalpossibletraining
sessions(i.e.,36).

53
Figure4.1:Screenshotoftheexergame‘Scarecrow’. Figure4.2:Screenshotoftheexergame‘Tractordriver’.
Figure4.3:Screenshotoftheexergame‘Fruitcatcher’. Figure4.4:Screenshotoftheexergame‘Wormhurdler’.
Figure4.5:Screenshotoftheexergame‘Mixsoup’.

54
Figure4.6:ResearchmodelbyMasrom[32].
Secondaryoutcomes
BergBalanceScale.BalanceabilitywhileperformingfunctionaltaskswasassessedwiththeBergBalance
Scale.Thistestconsistsof14mobilitytasksthatsimulatecommondailylifeactivitiesandisreliableand
valid in geriatrics [36]. By using a 5-point scale, ranging from0 (most impaired balance) to 4 (normal
balance), a person’s functional capability can be defined for each test. The possible cumulative score
rangesfrom0to56points.
TimedUpandGo.TheTimedUpandGo[37,38]requiresparticipantstostandupfromasittingposition,
walkfor3m,turn180°,walkback3m,andturntositdownagain.Weusedanextendedtestversion
witha7-mwalkingdistance[39].Thetestwasrepeatedthreetimeswith30-secondbreaksinbetween,
andthetotaltimetocompleteeachtrialwasmeasured.Theaveragetimewasusedforfurtheranalysis.
Forceplatform.Tomeasureposturalbalancecontrol,participantsstoodquietlyonaKistler(Winterthur,
Switzerland)forceplate(type9286B)undertwodifferenttestconditions:(1)onastablesurfaceand(2)
onanunstablesurface(foammat).Verticalgroundreactionforceswerecollectedatafrequencyof1000
Hz. Inbothconditions,participantswere instructedto focusonaredcrossdisplayedateye levelona
whitewallatadistanceof30cm.Ineachcondition,three20-secondtrialswereperformedwitha30-
secondbreakinbetween.Foreachtrial,centerofpressure(COP)areawasquantifiedastheareaofthe
smallest ellipse containing95%ofCOPdatapoints.MeanCOPareawas computed foreach condition
andusedforstatisticalanalysis.

55
Short Physical Performance Battery. The Short Physical Performance Battery, composed of a balance
test,a3-mwalkingtest,andafive-chair-risestest,resulted inscoresbetween0(notabletocomplete
the task) and 4 (good function) points per test. The sum of these scores represents the total Short
PhysicalPerformanceBatteryscore.Ahigherscoreindicatesbetterlowerextremityfunction[40-42].
Gait analysis. Spatiotemporal gait parameterswere assessedwith theGAITRite® system (CIR Systems,
Havertown,PA)consistingofanelectronicwalkwaywithgaitanalysis software.Theactiveareaof the
walkway(i.e.,theareaequippedwithpressuresensors)measures7.3m.Toeliminateaccelerationand
deceleration effects on calculated gait parameters, the walkway contains an additional 2.5 m at the
beginningandendof theactivearea.Participantswere towalkover theelectronicwalkwayata self-
selected comfortable walking speed. Three successful trials were collected, and the mean values of
velocity (cm/second), cadence (steps/minute), step time (seconds), step length (cm), and swing time
symmetry(ratio)werecalculated.Gaitsymmetrywascalculatedfromthefollowingratio[43]:
Symmetryratio=swingtimerightside/swingtimeleftside
Statisticalanalysis
All statistical analyses were performed using SPSS version 21.0 software (SPSS Inc., Chicago, IL).
Secondaryoutcomeswereonlycalculatedandanalyzedforparticipantswhocompletedtheintervention
as per protocol. AWilcoxon signed-rank testwas used to compare pre- and post-test results. Results
were deemed statistically significant at a p-value of ≤0.05. Effect size (r) was calculated as r = Z/√N,
where Z represents the approximation of the observed difference in terms of the standard normal
distribution and N is the total number of observations. Regarding effect size magnitude, r = 0.1 is
consideredasmall,r=0.3amedium,andr=0.5alargeeffect[44].
4.3Results
Primaryoutcomes
Sixteenparticipantswereenrolledinthestudy,13ofwhomreceivedthefullallocatedtrainingprogram
(Figure4.7). Twoparticipantsdroppedoutbecauseof injuries sustainedoutside the training, andone
discontinued because of self-reported lack of time. All reasons were unrelated to the content of the
training.

56
Figure4.7:Studyflowchart.BBS,BergBalanceScale;MMSE,Mini-MentalStateExamination;n,samplesize;SPPB,ShortPhysicalPerformanceBattery;TAM,technologyacceptancemodel;TUG,TimedUpandGo.
Table 4.2 presents completers’ demographics and clinical characteristics. Adherencewas 100percent.
Noneof the13participantssufferedanyadverseeventsduring the intervention.Theexergameswere
seen as easy to use and useful. The participants expressed a positive attitude toward using the
exergamesaswellasanintentiontocontinueusingthegames(Table4.3).

57
Table4.2:Completers’baselinecharacteristics.
Characteristics Value
Numberofparticipants 13
Age(years) 76.5±5.4(65-85)
Sex(female/male) 10/3
Height(cm) 163.6±8.5(152-177)
Weight(kg) 71.6±9.7(57.4-90.5)
MMSE(points)a 28.9±1.6(25-30)
Education
Collegeeducatedorhigher 2
Inasittingpositionpastprofession 5
Healthstatus
≥2self-reportedchronicdiseases 8
Feelpaindaily 4
Estimatedexcellent/goodhealthstatus 10
Estimatedexcellent/goodbalanceability 7
Dataarenumberofsubjectsormean±standarddeviation(range)valuesasindicated.aTheminimumscorewas0,andthemaximumscorewas30(ahigherscoreindicatesbettercognitivefunctioning).MMSE,Mini-MentalStateExamination.
Table4.3presentstheTAMitemsthatwereevaluatedpost-intervention.
During the intervention, participants reported some minor problems with using the games and
progressing through the exercises. In response, the exergames were adapted online (Table 4.4 gives
details)andsubsequentlyre-assessedforusability.

58
Table4.3:Evaluatedtechnologyacceptancemodelquestionnaireitems.
Item Score
PerceivedEaseofUse 5.9±1.7(1-7)
PerceivedUsefulness 6.4±1.0(4-7)
AttitudeTowardUsing 6.5±1.1(2-7)
BehavioralIntentiontoUse 6.0±1.3(3-7)
Dataaremean±standarddeviation(range)values.
Table4.4:Descriptionoftheonlineexergameadaptationsperformed.
Scarecrow Tractordriver Fruitcatcher Wormhurdler Mixsoup
Addedtwodifficultylevelstooriginalthree
Addedtwodifficultylevelstooriginalthree
Addedtwodifficultylevelstooriginalthree
Addedtwodifficultylevelstooriginalthree
Addedtwodifficultylevelstooriginalthree
Improvedconsistencyofstatementsandscoresprovidedbyvirtualtherapist
Improvedconsistencyofstatementsandscoresprovidedbyvirtualtherapist
Improvedconsistencyofstatementsandscoresprovidedbyvirtualtherapist
Improvedconsistencyofstatementsandscoresprovidedbyvirtualtherapist
Improvedconsistencyofstatementsandscoresprovidedbyvirtualtherapist
Addedpreviouslyabsentobstacles
Increasedwormsizeandhencevisibility
Secondaryoutcomes
The results of the pre-and post-comparisons are presented in Table 4.5. Significant improvements in
BergBalance Scale, TimedUpandGo, and Short Physical PerformanceBattery scoreswereobserved.
Separate analyses of each of the three Short Physical Performance Battery components (standing
balance, repeated chair rises, and gait speed) revealed that only standing balance changed. No
significantchangesweredetectedin(1)COPareaduringquietstanceand(2)anyofthegaitparameters
(allp-values>0.1).

59
Table4.5:Participants’baselineandpost-interventionphysicaloutcomemeasures.
Mean±standarddeviation
Baseline Post-intervention pwithin r Z
BBS(points) 51.7±3.3 54.8±1.4 0.007a 0.51b 2.590
7-mTUG(seconds) 19.8±2.8 17.5±2.4 0.002a 0.56b 2.830
COParea(mm2)
Stablesurface 2.47±1.64 4.43±4.17 0.191 0.27 1.363
Unstablesurface 10.42±7.73 17.69±18.54 0.414 0.17 0.874
SPPB(points)
Total 9.9±1.0 11.2±0.8 0.013a 0.48c 2.436
Balance 3.1±0.9 4.0±0.0 0.008a 0.51b 2.585
Chairrises 3.2±0.8 3.4±0.7 0.375 0.26 1.342
Gaitspeed 3.7±0.5 3.8±0.6 1.000 0.07 0.378
Gaitanalysis
Velocity(cm/second) 122.4±17.3 128.4±21.4 0.497 0.14 0.734
Cadence(steps/minute) 115.2±8.7 119.1±9.3 0.244 0.24 1.223
Steptime(seconds) 0.52±0.04 0.51±0.04 0.273 0.23 1.153
Steplength(cm) 63.6±6.0 64.4±6.9 0.542 0.13 0.664
Swingtimesymmetry(ratio) 0.99±0.03 1.00±0.04 0.127 0.31c 1.572aSignificantwithin-groupdifferencespre-post(pwithin≤0.05)calculatedwithWilcoxonsigned-ranktest.Foreffectsizer,r=0.1indicatesasmalleffect,cr=0.3indicatesamediumeffect,andbr=0.5indicatesalargeeffect.BBS,BergBalanceScale;COP,centerofpressure;pwithin,p-valueforwithin-groupcomparisons;SPPB,ShortPhysicalPerformanceBattery;TUG,TimedUpandGo;Z,approximationoftheobserveddifferenceintermsofthestandardnormaldistribution.

60
4.4Discussion
This study assessed – in untrained elderly – (1) the usability of the program in terms of acceptance,
adherence,andattritionand(2)theeffectoftheprogramonbalanceandgait.Thefindingsrevealeda
high levelofacceptancewithconcomitanthighadherencerates.HighscoresforeachofthefourTAM
itemswerefound.Onaverage,participantsfoundtheexergameseasytouse,clear,andunderstandable
without requiring much mental effort to operate. Perceived Usefulness results showed that the
exergames were perceived as a useful means to increase training effectiveness, productivity, and
performance.Moreover,therewasabroadconsensusintermsofAttitudeTowardUsing:Allparticipants
expressed a positive attitude towards the program. In addition, Behavioral Intention to Use results
showedthatparticipantslikedtheideaofcontinuingtheiruseofexergamesonaregularbasis.Thehigh
acceptancerateobtainedinthecurrentstudyseemsatoddswithapreviousstudybyLaveretal. [45]
thatrevealedskepticismabouttheuseofcommerciallyavailablevideogamesingeriatricrehabilitation.
Alikelyexplanationmaybefoundingamedesign:WhereLaveretal.[45]usedanoff-the-shelfsystem
without patient-specific adaptations, the exergames used in this studywere specifically designed and
developed for rehabilitationandwereadapted to thecognitiveandphysical limitationsof functionally
impaired persons or elderly. This explanation is in line with Cameirão et al. [46], who found high
acceptanceofagamingsystemspecificallydesignedtotreatpost-strokemotordeficits,andwithLewis
etal. [4],whodemonstratedpositive results fornewlydevelopedexergamesaimedto improvestroke
patients’armfunction.Ourfindingsalsocorroboratethehighacceptanceratesofspecificallydesigned
exergamesfoundbyBacklundetal.[47].
Thirteenofthe16participants(81percent)completedthefullallocatedtrainingprogramandattended
theretestingassessments.Consideringthemedianrateforattrition infallspreventioninterventions in
communitysettingsforclinicaltrials[48],a10percentattritionratecanbedeemedacceptable. Inour
study, we achieved a slightly higher rate. It should be noted, however, that the reasons for
discontinuationoftheinterventionwereunrelatedtotheintervention.Incontrasttothesomewhatlow
attrition rate,adherencewas100percentacross the36 training sessions.Thisperfectadherence is in
linewiththehighacceptancerevealedbytheTAMsurvey.Thehighadherenceandacceptanceratesin
thepresentstudymayberelatedtotheonlineadaptationsofthetrainingintervention:Theexergames
weresubjectedtoseveralonlineadaptationsbasedonparticipants’feedbackduringthetrainingperiod,
whichmighthavepositivelyimpactedbothusabilityandeffectiveness.

61
Weexpectedtheexergamesto improveparticipants’balanceandgait.The interventionhadapositive
effectonclinicalmeasuresofbalance.ThisisinlinewithastudybyLaietal.[49]thatreportedsimilar
results through a 6-week interactive videogame-based intervention. Although body sway during quiet
stancedidnotchangesignificantly,bothstandingonastableandunstablesurfaceyieldedlargeraverage
COPareas in thepost-testcomparedwith thepre-test.Given thatbetterbalance isusuallyassociated
withsmallerCOPareas,thistrendissurprising.Althoughspeculative, itmightnonethelessconstitutea
positive interventioneffect:Note that fourof the fiveexergames trainedeffectivecontrol rather than
minimizationofCOPmovement.Giventhat–tobeprecise–posturalstabilitylikewiserequireseffective
controlofCOP(inordertominimizecenterofmassmovement)ratherthanitsminimization,COPmight
notbe thebest indicatorofpostural stability,particularly in thepresent study [50].Measurementsof
center of mass movements (e.g., during walking) would have given a better insight into the actual
participants’dynamicposturalbalancecontrol.
The absence of gait-related effects in this study constitutes a confirmation of results by Szturmet al.
[51],whoalso examinedanexergame-based interventionwith goal-directedweight shifting tasks and
foundnosignificantimprovementinspatiotemporalgaitparameters.Hence,exerciseswithastationary
baseofsupportdonotseemtopresentthemosteffectivewaytoimprovewalkinginuntrainedelderly.
However, the absence of significant effects on gaitmight also be related to the lowpower of testing
togetherwiththeratherhighlevelofwalkingfunctioninoursample.Effectsizesweremediumorclose
tomediumand–withapreferredgaitspeedbetween1.0and1.4m/second–ourparticipantsshouldbe
classified as normal walkers [52]. A logical next step would therefore be to apply the present
intervention to community-dwelling chronic stroke populations that exhibit mildly abnormal (0.6–1.0
m/second)orseriouslyabnormalgaitspeed(below0.6m/second)andre-assessinterventioneffectson
gait in this actual target population [52]. Given that gait speed is an important factor related to
communitywalking in stroke patients,which in turn is strongly determined by balance [53], it seems
likelythatourexergames–whichexplicitlytargetthisskill–willimprovewalkinginchronicpatients.
Futurework
Weperformedan‘aprioripoweranalysis’todeterminetheminimumsamplesizeforsuchafuturetrial
[54].Specifically,weassessedtherequirementsforarandomizedcontrolledstudywithanexperimental
group(receivingexergame-basedtherapyandusualstrokerehabilitation)andacontrolgroup(receiving
usualstrokerehabilitationonly).Assuminganeffectsizeofr=0.30(basedonourobservedvalueforgait
symmetry),acceptabletypeIandIIerrorprobabilities(0.05and0.20,respectively)maybeobtainedwith

62
aminimumsampleof12participantspergroupforatwo-grouppre-andpost-testdesign.Toaccountfor
attrition,initialsamplesizeshouldbeincreasedto15participantspergroup.
Limitations
Some limitations of this study shouldbediscussed. First, this study featured a rather small sampleof
healthy untrained elderly, which resulted in limited statistical power for gait analysis. The validity of
using elderly persons to test the usabilitymay be questioned. However, (1) the primary focus of this
studywasonusability,whereasampleof fiveparticipants issufficient fordetecting80percentofthe
usability problems [55], and (2) untrained elderly normally show both balance and gait impairments,
whichshouldrenderthemanadequatepopulationforassessingeffectivenessaswell.Second,thestudy
may suffer from volunteer bias: It can be hypothesized that our volunteer participants were more
interested in technology than the average elderly, whichmight explain in part their positive attitude
towardtheintervention.Boththeselimitationswouldnotapplyinacontrolledtrialwithstrokepatients,
which–incombinationwiththepromisingresultsofthepresentstudy–highlightstheneedforsucha
trial.Athirdlimitationconcernsthegenderdistributioninoursample,withwomenoutnumberingmen.
However, sexdisparity in strokeprevalencepersists,withwomenbeingmoreaffected thenmen [56].
Thismakesitimportanttoespeciallytestacceptanceandfeasibilityinwomen.
4.5Conclusion
Small-scale interventions focusingonusability representan importantstagewhendevelopingcomplex
theory-based interventions to improve health [25]. Usability studies provide invaluable results for
informationtechnologydevelopersandrehabilitationspecialistsusinginnovativesystemsandmightbe
highlyrelevantforfurtheringthedevelopmentofnewemergingvirtualreality-basedrehabilitation.Our
resultscorroboratepreviousfindingsinshowingthatvirtualtrainingapproachesforperformingbalance
traininghavegreatpotential.Specifically,thisstudydemonstratesthattheexergame-basedintervention
wasperceivedasusableandhadapositiveeffectonbothstandingbalanceanddailylifetasks.

63
Authors’contributions
SWcontributedtotheconceptionofthework,theacquisition,analysisandinterpretationofdata,and
writing the manuscript. NAB, MP, and RM contributed to the development of the software and
exergames.RvdLassistedintheacquisitionofdataandcontributedtotheanalysisandinterpretationof
data and towriting themanuscript. EDdB initiated the study, assisted in the acquisition of data, and
contributedtowritingthemanuscript.Allauthorsreadandapprovedthefinalmanuscript.
Acknowledgments
This work was partially supported by the REWIRE project (www.rewire-project.eu), funded by the
EuropeanCommissionundertheFP7frameworkwithcontract287713.
Conflictofintereststatement
Nocompetingfinancialinterestsexist.

64
References
1. DuncanP,StudenskiS,RichardsL,etal.Randomizedclinicaltrialoftherapeuticexerciseinsubacute
stroke.Stroke2003;34:2173–2180.2. SchwartzI,SajinA,FisherI,etal.Theeffectivenessoflocomotortherapyusingrobotic-assistedgait
traininginsubacutestrokepatients:Arandomizedcontrolledtrial.PMR2009;1:516–523.3. DemainS,WilesR,RobertsL,McPhersonK.Recoveryplateaufollowingstroke:Factorfiction?Disabil
Rehabil2006;28:815–821.4. LewisGN,WoodsC,RosieJA,McPhersonKM.Virtualrealitygamesforrehabilitationofpeoplewith
stroke:Perspectivesfromtheusers.DisabilRehabil2011;6:453–463.5. HornbyTG,StraubeDS,KinnairdCR,etal.Importanceofspecificity,amount,andintensityoflocomotor
trainingtoimproveambulatoryfunctioninpatientspoststroke.TopStrokeRehabil2011;18:293–307.6. DicksteinR,DunskyA,MarcovitzE.Motorimageryforgaitrehabilitationinpost-strokehemiparesis.Phys
Ther2004;84:1167–1177.7. HsuAL,TangPF,JanMH.Analysisofimpairmentsinfluencinggaitvelocityandasymmetryofhemiplegic
patientsaftermildtomoderatestroke.ArchPhysMedRehabil2003;84:1185–1193.8. PuhU,BaerG.Acomparisonoftreadmillwalkingandovergroundwalkinginindependentlyambulant
strokepatients:Apilotstudy.DisabilRehabil2009;31:202–210.9. vonSchroederHP,CouttsRD,LydenPD,etal.Gaitparametersfollowingstroke:Apracticalassessment.J
RehabilResDev1995;32:25–31.10. StuartM,BenvenutiF,MackoR,etal.Community-basedadaptivephysicalactivityprogramforchronic
stroke:Feasibility,safety,andefficacyoftheEmpolimodel.NeurorehabilNeuralRepair2009;23:726–734.11. MuratoriLM,LambergEM,QuinnL,DuffSV.Applyingprinciplesofmotorlearningandcontroltoupper
extremityrehabilitation.JHandTher2013;26:94–103.12. LanghorneP,BernhardtJ,KwakkelG.Strokerehabilitation.Lancet2011;377:1693–1702.13. BurkeJW,McNeillMDJ,CharlesDK,etal.Optimisingengagementforstrokerehabilitationusingserious
games.VisComput2009;25:1085–1099.14. deBruinED,SchoeneD,PichierriG,SmithST.Useofvirtualrealitytechniqueforthetrainingofmotor
controlintheelderly.ZGerontolGeriatr2010;43:229–234.15. RizzoA,KimGJ.ASWOTanalysisofthefieldofvirtualrealityrehabilitationandtherapy.Presence2005;
14:119–146.16. MarstonHR,SmithST.Interactivevideogametechnologiestosupportindependenceintheelderly:A
narrativereview.GamesHealthJ2012;1:139–152.17. NapHH,deKortYAW,IJsselsteijnWA.Seniorgamers:Preferences,motivationsandneeds.
Gerontechnology2009;8:247–262.18. BorgheseNA,PirovanoM,LanziPL,etal.Computationalintelligenceandgamedesignforeffectiveat-
homestrokerehabilitation.GamesHealthJ2013;2:81–88.19. IJsselsteijnWA,NapHH,deKortYAW,PoelsK.Digitalgamedesignforelderlyusers.In:Proceedingsofthe
2007ConferenceonFuturePlay.NewYork:ACM.2007:17–22.20. GerlingKM,SchildJ,MasuchM.Exergamedesignforelderlyusers:ThecasestudyofSilverBalance.In:
Proceedingsofthe7thInternationalConferenceonAdvancesinComputerEntertainmentTechnology.NewYork:ACM.2010:66–69.
21. REWIRE.Rehabilitativewayoutinresponsivehomeenvironments.www.rewire-project.eu/about-rewire(accessedOctober1,2013).
22. OhY,YangS.Definingexergamesandexergaming.In:MeaningfulPlay2010ConferenceProceedings(http://meaningfulplay.msu.edu/proceedings2010/);October21–23,2010EastLansing,MI,USA(MichiganStateUniversity).
23. WüestS,vandeLangenbergR,deBruinED.Designconsiderationsforatheory-drivenexergame-basedrehabilitationprogramtoimprovewalkingofpersonswithstroke.EurRevAgingPhysAct2013:DOI:10.1007/s11556-013-0136-6,1–11.

65
24. BorgheseNA,PirovanoM,MainettiR,LanziPL.IGER:Anintelligentgameengineforrehabilitation.In:ConvergingClinicalandEngineeringResearchonNeurorehabilitation.NewYork:Springer;2013:947–950.
25. CampbellM,FitzpatrickR,HainesA,etal.Frameworkfordesignandevaluationofcomplexinterventionstoimprovehealth.BMJ2000;321:694.
26. BohannonRW.Comfortableandmaximumwalkingspeedofadultsaged20–79years:Referencevaluesanddeterminants.AgeAgeing1997;26:15–19.
27. ChettaA,ZaniniA,PisiG,etal.Referencevaluesforthe6-minwalktestinhealthysubjects20–50yearsold.RespirMed2006;100:1573–1578.
28. deBruinED,vanhetReveE,MurerK.Arandomizedcontrolledpilotstudyassessingthefeasibilityofcombinedmotor-cognitivetraininganditseffectongaitcharacteristicsintheelderly.ClinRehabil2013;27:215–225.
29. TroostersT,GosselinkR,DecramerM.Sixminutewalkingdistanceinhealthyelderlysubjects.EurRespirJ1999;14:270–274.
30. WinterDA,PatlaAE,FrankJS,WaltSE.Biomechanicalwalkingpatternchangesinthefitandhealthyelderly.PhysTher1990;70:340–347.
31. Tyromotion.http://tyromotion.com/en/products/tymo/overview(accessedOctober1,2013).32. MasromM.Technologyacceptancemodelande-learning.In:12thInternationalConferenceonEducation,
SultanHassanalBolkiahInstituteofEducation,May21–24,2007,BruneiDarussalam.2007:1–10.33. DavisFD.Perceivedusefulness,perceivedeaseofuse,anduseracceptanceofinformationtechnology.
MISQ1989;13(3):319–340.34. DavisFD,BagozziRP,WarshawPR.Useracceptanceofcomputertechnology:Acomparisonoftwo
theoreticalmodels.ManageSci1989;35:982–1003.35. VenkateshV,DavisFD.Atheoreticalextensionofthetechnologyacceptancemodel:fourlongitudinalfield
studies.ManageSci2000;46:186–204.36. HasselgrenL,OlssonLL,NybergL.Islegmusclestrengthcorrelatedwithfunctionalbalanceandmobility
amonginpatientsingeriatricrehabilitation?ArchPhysMedRehabil2011;52:E220–E225.37. BergKO,MakiBE,WilliamsJI,etal.Clinicalandlaboratorymeasuresofposturalbalanceinanelderly
population.ArchPhysMedRehabil1992;73:1073–1080.38. ThompsonM,MedleyA.Performanceofcommunitydwellingelderlyonthetimedupandgotest.Phys
OccupTherGeriatr1995;13:17–30.39. SalarianA,HorakFB,ZampieriC,etal.iTUG,asensitiveandreliablemeasureofmobility.IEEETransNeural
SystRehabilEng2010;18:303–310.40. GuralnikJM,FerrucciL,PieperCF,etal.Lowerextremityfunctionandsubsequentdisability:Consistency
acrossstudies,predictivemodels,andvalueofgaitspeedalonecomparedwiththeshortphysicalperformancebattery.JGerontolABiol2000;55:M221–M231.
41. GuralnikJM,SimonsickEM,FerrucciL,etal.Ashortphysicalperformancebatteryassessinglowerextremityfunction:Associationwithself-reporteddisabilityandpredictionofmortalityandnursinghomeadmission.JGerontol1994;49:M85–M94.
42. NelsonME,LayneJE,BernsteinMJ,etal.Theeffectsofmultidimensionalhome-basedexerciseonfunctionalperformanceinelderlypeople.JGerontolABiolSciMedSci2004;59:154–160.
43. PattersonKK,GageWH,BrooksD,etal.Evaluationofgaitsymmetryafterstroke:Acomparisonofcurrentmethodsandrecommendationsforstandardization.GaitPosture2010;31:241–246.
44. FieldA.DiscoveringStatisticsUsingSPSS.London:SagePublications;2009.45. LaverK,RatcliffeJ,GeorgeS,etal.IstheNintendoWiiFitreallyacceptabletoolderpeople?:Adiscrete
choiceexperiment.BMCGeriatr2011;11:64.46. CameirãoMS,BadiaSB,OllerED,VerschureP.Neurorehabilitationusingthevirtualrealitybased
rehabilitationgamingsystem:Methodology,design,psychometrics,usabilityandvalidation.JNeuroengRehabil2010;7:48.
47. BacklundP,TaylorA-SA,EngströmH,etal.Gamesonprescription!EvaluationoftheElinorconsoleforhome-basedstrokerehabilitation.In:TransactionsonEdutainmentIX.NewYork:Springer;2013:49–64.
48. NymanSR,VictorCR.Olderpeople’sparticipationinandengagementwithfallspreventioninterventionsincommunitysettings:AnaugmenttotheCochraneSystematicReview.AgeAgeing2012;41:16–23.

66
49. LaiCH,PengCW,ChenYL,etal.Effectsofinteractivevideo-gamebasedsystemexerciseonthebalanceoftheelderly.GaitPosture2013;37:511–515.
50. AoyamaH,GotoM,NaruoA,etal.Thedifferencebetweencenterofmassandcenterofpressure:Areviewofhumanposturalcontrol.AinoJ2006;5:25–31.
51. SzturmT,BetkerAL,MoussaviZ,etal.Effectsofaninteractivecomputergameexerciseregimenonbalanceimpairmentinfrailcommunity-dwellingolderadults:Arandomizedcontrolledtrial.PhysTher2011;91:1449–1462.
52. StudenskiS.Bradypedia:Isgaitspeedreadyforclinicaluse?JNutrHealthAging2009;13:878–880.53. vandePortIG,KwakkelG,LindemanE.Communityambulationinpatientswithchronicstroke:Howisit
relatedtogaitspeed?JRehabilMed2008;40:23–27.54. FaulF,ErdfelderE,LangA-G,BuchnerA.G*Power3:Aflexiblestatisticalpoweranalysisprogramforthe
social,behavioral,andbiomedicalsciences.BehavResMethods2007;39:175–191.55. VirziRA.Refiningthetestphaseofusabilityevaluation:Howmanysubjectsisenough?HumFactors1992;
34:457–468.56. TowfighiA,MarkovicD,OvbiageleB.PersistentsexdisparityinmidlifestrokeprevalenceintheUnited
States.CerebrovascDis2011;31:322–328.

67
5
Reliability and validity of the inertial sensor-based Timed Up and Go test in post-stroke individuals
WüestS1,MasséF2,AminianK2,GonzenbachR3,deBruinED1
1InstituteofHumanMovementSciencesandSport,DepartmentofHealthSciencesandTechnology,ETH
Zurich,Switzerland
2LaboratoryofMovementAnalysisandMeasurement,EcolePolytechniqueFédéraledeLausanne,
Switzerland
3DepartmentofNeurology,UniversityHospitalZurich,Switzerland
JournalofRehabilitationResearch&Development2015,inpress

68
Abstract
The instrumented Timed Up and Go test (iTUG) has the potential for playing an important role in
providing clinically useful information regarding an individuals’ balance and mobility that cannot be
derivedfromtheoriginalsingle-outcomeTUGprotocol.Thepurposeofthisstudywastodeterminethe
reliabilityandvalidityoftheiTUGusingbody-fixedinertialsensorsinpeopleaffectedbystroke.Fortest-
retest reliability analysis, 14 individualswith stroke and 25 healthy elderlywere assessed. For validity
analysis,anage-matchedcomparisonof12strokepatientsand12healthycontrolswasperformed.Out
ofthe14computediTUGmetrics,themajorityshowedexcellenttest-retestreliabilityexpressedbyhigh
intraclass correlation coefficients (ICCs range 0.431-0.994) together with low standard error of
measurement (SEM and SEM%, respectively) and smallest detectable difference (SDD and SDD%,
respectively) values. Bland and Altman plots demonstrated good agreement between two repeated
measurements.Significantdifferencesbetweenstrokepatientsandhealthycontrolswerefoundinnine
of 14 iTUG parameters analyzed. Consequently, these results warrant the future application of the
inertial sensor-based iTUGtest for theassessmentofphysicaldeficitspost-stroke in longitudinal study
designs.
Keywords:Test-retestreliability,Validity, InstrumentedTimedUpandGotest,Stroke, Inertialsensors,
Motorfunctiontest,Rehabilitation

69
5.1Introduction
After a stroke, many individuals suffer from hemiparesis which often leads to an impaired walking
patternwithalteredgaitcharacteristics[1-7].Specifically,thehemiplegicgaitistypicallyassociatedwith
a reduced gait speed [1-3, 5, 8], cadence [2, 5, 8], stride length [2, 8] and an increased left-right
asymmetryduringwalking[1,3,9]whencomparedtohealthy,age-matchedcontrols.Furthermore,itis
often characterized by an increased stance phase duration [2]. Hemiparesis not only leads to gait
impairments,butmayalsoaffectbalanceandpostural transfers (i.e.,changingposition fromsitting to
standing, and vice versa) further impeding the patients’ mobility and independence [6, 10-12]. It is
thereforea central goalof stroke rehabilitation to improve thepatient’s independenceand functional
capacitybyimprovinghisorhermobility[13].
TheTimedUpandGotest(TUG)isoftenusedtoevaluatebalanceandmobilityinstrokepatients[14],
withgoodreliabilityandvalidity[15-17].TheTUGrequiresapersontorisefromachair,walkadistance
of3metersataself-pacedcomfortablespeed,turnaround,andreturntothechairtositdownagain.
Thetotaltimeforcompletionisrecordedandusedasmeasureofmobility.However,althoughtheTUG
is commonly used to evaluate mobility post-stroke, it has some drawbacks. First, it only uses the
outcomeparameter ‘time’ and fails todetect otherbalance- andmobility-relatedparameters [18-19].
Second, although it consists of a number of consecutive tasks it does not allow analyzing these
separately[18-19].Recently,severalresearchersinstrumentedtheTUGinanefforttoovercomesomeof
thedrawbacks.Forexample,Vernonetal.[20]usedaMicrosoftKinectcamera-basedTUGmethodfor
analyzing the specific subcomponents of the test. Furthermore, Zampieri et al. [19] revealed the
potentialbenefitofaninstrumentedTUG(iTUG)systemusingwearableinertialsensorswhileassessing
individualswithParkinson’sdisease(PD).While10ofthe21gaitandposturaltransitionparametersthat
were identifiablewith the iTUG showed significant differences between PD and healthy controls, the
total test performance time was not diverging. Obviously, the iTUG seemed to exhibit a greater
sensitivitythantheconventionalTUGtestintermsofmobilitydeficitdetectioninPD[18].
Therecentuseofbody-fixedsensorssuggeststhattheycouldserveasatoolforanalyzingmeasuresof
physicalfunctioningofpatients[21-22].Itcouldpotentiallydelivermoredetailedandclinicallyrelevant
informationonastrokepatient’sgaitandmobility than theconventionalTUG,whichonly reports the
time to complete the task. To the best of our knowledge, no study exists applying an inertial sensor-
basediTUGsysteminpeopleaffectedbystroke.Tobeclinicallyuseful,anassessmentproceduremust

70
have a small measurement error to detect a real change and must be able to distinguish between
subpopulations;e.g.,strokepatientsinvariousstagesandhealthycontrols.Atest-retestdifferenceina
patientwithavaluesmallerthanthestandarderrorofthemeasurement(SEM)islikelytobetheresult
of‘measurementnoise’andisunlikelytobedetectedreliablyinpractice;adifferencegreaterthanthe
smallest real difference is highly likely (with 95% confidence) to be a real difference [23-25]. Another
exampleof these statistics is the smallestdetectabledifference (SDD) [24,26].Thepresent studywas
conducted toassess the reliabilityandvalidityof inertial sensor-based iTUGmetrics in strokepatients
andage-matchedhealthycontrolelderly.
5.2Methods
Studydesign
The study was designed as an observational study where all participants were tested by the same
observer.EthicalapprovalforthisstudywasgrantedbythelocalETHZurichEthicsCommittee(protocol
numberEK2012-N-32)andthecantonalEthicsCommitteeoftheCantonofSt.Gallen(protocolnumber
EKSG12/002/1B).Priortoparticipation,allparticipantswerefullyinformedaboutthecompleteresearch
protocolandrequestedtosignaconsentform.
Participants
Participants were recruited on a voluntary basis through researchers from the Institute of Human
MovementSciencesandSportatETHZurich, Switzerland, andby contactingphysiciansand therapists
fromtheRehabilitationCenterValens,Switzerland.Thereweretwogroupsofparticipants:1)fourteen
patients at any stage after ischemic or hemorrhagic stroke aged over 18 years. Participants were
excluded from the study if any known comorbid disabilities other than stroke were present (e.g.,
musculoskeletal illness,cardiovasculardisordersorotherneurologicdiseases)thatmighthaveaffected
performanceinthetestprocedures;2)twenty-fivehealthybyself-reportcontrolparticipantsagedover
65 years who had no history of neurological, cardiovascular or musculoskeletal pathologies. To be
eligibleforthestudy,individualshadtobeabletowalkunassistedforatleast15meters.Theuseofone
crutchforwalkingwasacceptedfor inclusion. Individualswhowerenotabletogive informedconsent
wereexcluded.

71
Apparatus
Intotal,eightbody-fixeddevices(Physilog®,GaitUp,CH)wereplacedonparticipants’body:thesensor
configurationdescribed inthe iTUGprocedurebySalarianetal. [18]–oneoneachwrist,oneoneach
shank,andoneonthetrunk–wascomplementedwithonedeviceoneachfootandoneontheback(L3)
for further analysis. The sensor located on patient’s back was taped using hypoallergenic breathable
straps to ensure firm attachment to the skin. Every other sensor devices were firmly affixed to the
patientusingelasticstraps.
The devices recorded to an on-boardmemory card the signals from a calibrated inertial sensor (3D-
accelerometer and 3D-gyroscope) at 500 Hz [27]. Before any processing, the inertial signals, sampled
synchronouslyacrossdevices,wereresampledbysoftware(Matlab2014a,Mathworks,USA)at200Hz
asdescribedintheoriginaliTUGstudy[18].
Measurementprotocol
Eachpatientwas firstequippedwith thewearable sensor set.Then, inaccordancewithSalarianetal.
[18],weusedanextendediTUGtestversionwitha7-meterwalkingdistance.Thereby,moregaitcycles
were recorded thanwhenusing the original TUG test protocol. All participants completed the testing
sessioneitherinagaitlaboratoryoftheInstituteofHumanMovementSciencesandSportatETHZurich,
Switzerland,orinsuitablelocationsattheRehabilitationCenterValens,Switzerland.
Thetestingsessionincludedthefollowingprocedure:Initially,eachparticipantwasequippedwithaset
of sensors.Once the sensorshadbeenattachedon theappropriateparticipants’ bodypositions, they
performedthe first iTUGmeasurementsessioncomposedof threerepeated iTUGtrials (measurement
session 1). Between each trial, a 30-second rest periodwas applied. After completing the three iTUG
trials, the participantswere instructed to relax for 15minuteswhile removing the sensors from their
body. Then, the sensors were reattached to participants’ body and the same protocol repeated
(measurementsession2).Eachtestingsessionwasrecordedwithavideocameraallowingresearchers
laterinspectionifnecessary.
Inordertogetsufficientinformationabouttheassessmenttool’sreliabilityandvaliditycharacteristics,
weidentified1)therelativereliabilitybyusingtheintraclasscorrelationcoefficient(ICC),2)theabsolute
reliabilitytoidentifyarealimprovementbycalculatinga)thestandarderrorofmeasurement(SEM)for
groups of subjects, b) the limits of agreement (LOA) for a single person and c) the smallest clinical
detectabledifference(SDD)whichalsorevealsthe limitsfortherealchangeforasinglepersonand3)

72
thediscriminatorycapabilitiesontheiTUGmetricsbycomparingstrokepatientstohealthyage-matched
controls.
Dataanalysis
Based on algorithms described elsewhere [18-19, 28-29], different parameters of gait and postural
transitionduringiTUGperformanceweremeasured:
• iTUGtotalduration(sec):TotaldurationoftheiTUGtrialinseconds
Sit-to-walkmetrics
• Sit-to-walkduration(sec):Durationofthesit-to-walktransitioninseconds
• Peak sit-to-walk velocity (deg/sec): Maximum angular trunk velocity in degrees per secondduringthesit-to-walktransition
Gaitmetrics
• Gait cadence (steps/min): Walking cadence in number of steps per minute; normalized toparticipants’height
• Gaitstancephase(%):Stancephaseasapercentageofgaitcycletime
• Gait limp phase (%): Difference between initial and terminal double support phase as apercentageofgaitcycletime
• Gaitvelocity(m/sec):Walkingspeedinmeterspersecond;normalizedtoparticipants’height
• Gaitstridelength(m):Distanceinmetersbetweentwoconsecutivefootfallsatthemomentsofinitialcontact;normalizedtoparticipants’height
• Gait peak swing velocity (deg/sec): Maximum angular shank velocity in degrees per secondduringonestride
• Gaitasymmetry:Symmetryratio relatedto theswingphaseperformedbyeach leg;calculatedwiththeformula=|1-((limbwithlowervalue)/(limbwithhighervalue))|
Turningmetrics
• Turningduration(sec):Durationof180°turninseconds
• Peak turning velocity (deg/sec):Maximum angular trunk velocity in degrees per secondwhileturning
Turn-to-sitmetrics
• Turn-to-sitduration(sec):Durationoftheturn-to-sittransitioninseconds

73
• Peakturn-to-sitvelocity(deg/sec):Maximumangulartrunkvelocityindegreespersecondduringtheturn-to-sittransition
ThereliabilityandvalidityassessmentsapplytotheiTUGmeasuredforthreetimesandaveragedvalues
asopposedtotheoriginalTUGwhereasinglemeasureafterapracticetrialistakenastheoutcome.For
data analysis, the mean value of the iTUG total duration across the three iTUG trials performed in
measurementsession1andmeasurementsession2,respectively,wasused.Themedianofthemetrics
of the straight walking gait, the transitions and turns across the three iTUG trials performed in
measurement session 1 and measurement session 2, respectively, was used to eliminate possible
outliers.Exceptoftheparameter‘gaitasymmetry’whichisbasedontheswingphaseperformedbyeach
leg,theaveragevalueofbothlegswasused.
Statisticalanalysis
Descriptive statistical analysis was carried out to describe the study population. The one-sample
Kolmogorov-Smirnovtest, skewnessandkurtosiswereusedtotestnormalityof thedata.Theprimary
test-retestreliabilitycalculationswerebasedontheentirestudypopulation.Areliabilitysubanalysisonly
includingthestrokepatientswasperformedseparately.Thereliabilitysubanalysisincorporatedthefive
gait iTUG metrics ‘cadence’, ‘stance phase’, ‘velocity’, ‘stride length’ and ‘asymmetry’. For assessing
differencesbetweenstrokepatientsandhealthyelderly(age-matched),twogroupswerecreated(stroke
& healthy control) and compared with the paired t-test or the non-parametric equivalent where
appropriate.AllstatisticalanalyseswereperformedusingSPSSversion21.0software(SPSSInc.,Chicago,
IL).Thecriticalα-levelwassetatp≤0.05.
Reliability
Several statistical methods of assessing test-retest reliability were performed. Heteroscedasticity was
tested by calculating the square value of Pearson’s correlation coefficient (r2) between the absolute
differenceandthemeanofeachpairofmeasurements.Ifvaluesofr2aregreaterthan0.1,thenthedata
are heteroscedastic [30]. The ICC with the 95% confidence interval (CI) was used as an estimate of
relative reliability [30]. The ICC is commonly used to determine the consistency or reproducibility
betweenrepeatedmeasurementsandtoassesstheSEM[31].Inthisarticle,theICC1,kone-wayanalysis
ofvariance(ANOVA)wasconsideredforthefollowingreasons:Thesamedeviceandsameparticipants
tested by the sole rater were used for assessing test-retest reliability. Furthermore, the two

74
measurementsessionsperformedduringthestudywereseparatedbyatimeperiodofonly15minutes.
Therefore,weassumedthatparticipants’gaitpatternwouldnothavechangedoverthistime.
The interpretation of the ICC valueswas according to Shrout and Fleiss [32] inwhich values of >0.75
indicate excellent reliability, 0.75-0.40 fair to good reliability and <0.40 poor reliability. Since the ICC
score depends greatly on the range of values in the analyzed sample [30] and is not able to provide
informationabouttheaccuracyforaspecificindividual,theSEMandtheSDDforeachparameterwere
calculated. TheSEM indicatesa real improvement in thegroupof individuals andwasassessedusing:
SEM=SD√(1-ICC),inwhichSDrepresentsthesamplestandarddeviation[30].TheSDDcanbeusedasan
indicatorforassessingrealchangebeyondmeasurementerrorinasingleperson.Itwasderivedfromthe
SEM through: 1.96 x √2 x SEM [26]. The SEM and SDD can be expressed as a percentage which are
independentof theunitsofmeasurementand, therefore, suitable tocompare theamountof random
error between measurement parameters: SEM% = ((SEM/mean of the two measurements)*100) and
SDD%= ((SDD/meanof the twomeasurements)*100).Discrepanciesbetween themeasurementswere
also investigatedbyperformingBlandandAltman’s95%LOAanalysis. Itexpressesthedegreeoferror
proportional tothemean.TheBlandandAltmanmethod includesascatterplotproviding information
about the degree of error (measurement 1 – measurement 2) proportional to the mean of the two
measurementswith95%LOA(meandifference±1.96xSDofthedifference)[24,33-34].
Validity
Thepaired t-test and theWilcoxon signed-rank testwere performed to examinedifferences between
stroke patients and the age-matched healthy controls, depending on normality of data. Groupmean
values of the iTUG metrics are expressed as mean ± SD. Effect sizes are presented as Pearson’s
correlationcoefficient(r)whichcanbecalculatedfromthet-statisticsconvertedintor-statisticsbythe
formular=t2/(t2+df)orfromtheZvalueusingtheequationr=Z/√N[35].dfrepresentsthedegreesof
freedom,Z theapproximationof theobserveddifference in termsof thestandardnormaldistribution
andNthetotalnumberofobservations.Theeffectsizemagnitudeofr=0.1indicatesasmall,r=0.3a
medium and r = 0.5 a large effect [35]. The results of the first measurement session were used for
analysis.Since thegaitparameterswalkingspeed,stride lengthandcadencearerelatedtosomeone’s
bodyheight,theseparameterswerenormalizedtoheight(actualparametervalue/height)[36].

75
5.3Results
Atotalof39participantswereenrolledinthestudy,whereof25werehealthyelderly.Thecharacteristics
ofthisstudypopulationaredescribedinTable5.1.Sincethetwogroupsdifferedinmeanage,anage-
matched comparison of 12 stroke patients and 12 age-matched healthy controls was performed for
validityanalysis.ThecharacteristicsofthoseparticipantsarepresentedinTable5.2.
Reliability
Out of the 14 analyzed iTUGmetrics, the ICCs of 12 variables showed excellent test-retest reliability
(ICC1,k = 0.855-0.994). Only the two sit-to-walk parameters ‘duration’ and ‘peak sit-to-walk velocity’
reported a lower relative reliability coefficient (ICC1,k = 0.431 and ICC1,k = 0.674). The ICC values with
corresponding95%CIarereportedtogetherwiththeSEMandSEM%,theSDDandSDD%,andthe95%
LOA inTable5.3.Valuesof r2basedon theabsolutedifferencesbetweenmeasurementsession1and
measurementsession2andthemeanvalueofbothmeasurementsessionswereforalliTUGparameters
below 0.1 indicating no evidence of heteroscedasticity. Bland and Altman plots graphically support
homoscedasticity in all iTUG variables analyzed (Figures 5.1-5.14). Eleven of the 14 analyzed iTUG
parameters showed lowSEMandSEM%values (ranging fromSEM%=0.220 to7.109%),and lowSDD
andSDD%values (ranging fromSDD%=0.659 to19.706%).HighSEMandSEM%values (ranging from
SEM%=15.819to20.600%),andhighSDDandSDD%values(rangingfromSDD%=43.848to57.134%)
werefoundforbothsit-to-walkparametersandforthegaitparameterrelatedtothelimpphase.
ThereliabilitysubanalysisofthegaitiTUGmetrics‘cadence’,‘stancephase’,‘velocity’,‘stridelength’and
‘asymmetry’ revealed similar results to thosebasedon theentire studypopulation (Table5.4): Forall
five iTUGmetricsmeasured,excellent test-retest reliability (ICC1,k=0.958-0.991)withconcomitant low
SEMandSEM%(rangingfromSEM%=0.431to2.701%),and lowSDDandSDD%values(rangingfrom
SDD%=1.292to7.481%)werefound.
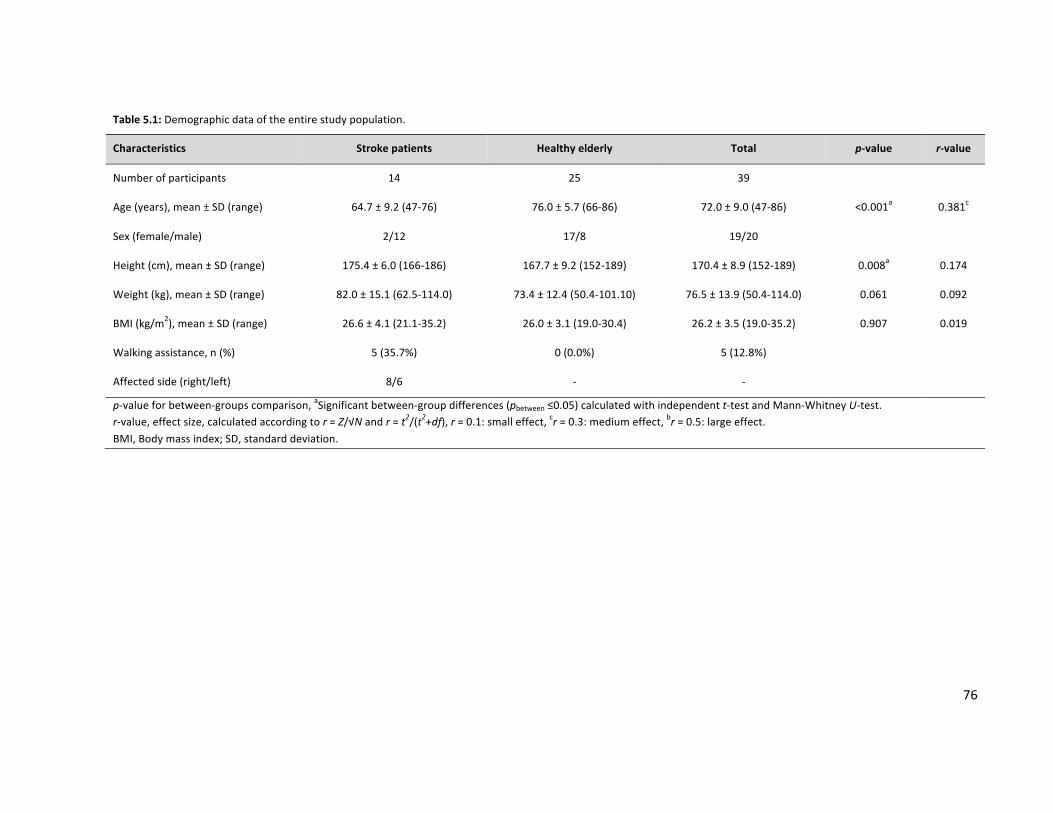
76
Table5.1:Demographicdataoftheentirestudypopulation.
Characteristics Strokepatients Healthyelderly Total p-value r-value
Numberofparticipants 14 25 39
Age(years),mean±SD(range) 64.7±9.2(47-76) 76.0±5.7(66-86) 72.0±9.0(47-86) <0.001a 0.381c
Sex(female/male) 2/12 17/8 19/20
Height(cm),mean±SD(range) 175.4±6.0(166-186) 167.7±9.2(152-189) 170.4±8.9(152-189) 0.008a 0.174
Weight(kg),mean±SD(range) 82.0±15.1(62.5-114.0) 73.4±12.4(50.4-101.10) 76.5±13.9(50.4-114.0) 0.061 0.092
BMI(kg/m2),mean±SD(range) 26.6±4.1(21.1-35.2) 26.0±3.1(19.0-30.4) 26.2±3.5(19.0-35.2) 0.907 0.019
Walkingassistance,n(%) 5(35.7%) 0(0.0%) 5(12.8%)
Affectedside(right/left) 8/6 - -
p-valueforbetween-groupscomparison,aSignificantbetween-groupdifferences(pbetween≤0.05)calculatedwithindependentt-testandMann-WhitneyU-test.r-value,effectsize,calculatedaccordingtor=Z/√Nandr=t2/(t2+df),r=0.1:smalleffect,cr=0.3:mediumeffect,br=0.5:largeeffect.BMI,Bodymassindex;SD,standarddeviation.
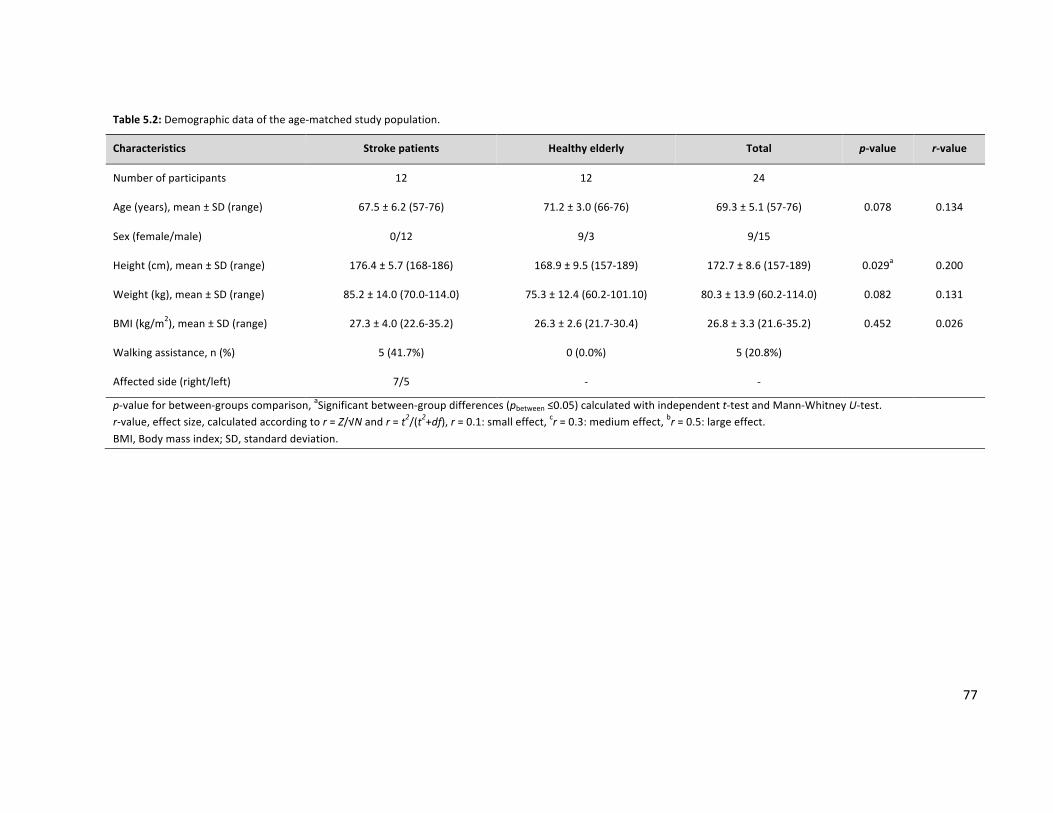
77
Table5.2:Demographicdataoftheage-matchedstudypopulation.
Characteristics Strokepatients Healthyelderly Total p-value r-value
Numberofparticipants 12 12 24
Age(years),mean±SD(range) 67.5±6.2(57-76) 71.2±3.0(66-76) 69.3±5.1(57-76) 0.078 0.134
Sex(female/male) 0/12 9/3 9/15
Height(cm),mean±SD(range) 176.4±5.7(168-186) 168.9±9.5(157-189) 172.7±8.6(157-189) 0.029a 0.200
Weight(kg),mean±SD(range) 85.2±14.0(70.0-114.0) 75.3±12.4(60.2-101.10) 80.3±13.9(60.2-114.0) 0.082 0.131
BMI(kg/m2),mean±SD(range) 27.3±4.0(22.6-35.2) 26.3±2.6(21.7-30.4) 26.8±3.3(21.6-35.2) 0.452 0.026
Walkingassistance,n(%) 5(41.7%) 0(0.0%) 5(20.8%)
Affectedside(right/left) 7/5 - -
p-valueforbetween-groupscomparison,aSignificantbetween-groupdifferences(pbetween≤0.05)calculatedwithindependentt-testandMann-WhitneyU-test.r-value,effectsize,calculatedaccordingtor=Z/√Nandr=t2/(t2+df),r=0.1:smalleffect,cr=0.3:mediumeffect,br=0.5:largeeffect.BMI,Bodymassindex;SD,standarddeviation.

78
Table5.3:ReliabilityoftheiTUGmetricsbasedontheentirestudypopulation(strokepatientsandhealthyelderly).
iTUGmetrics ICC1,k CI95%forICC1,k SEM CI95%forSEM SDD SEM% SDD% LALB LAUB
iTUGtotalduration(sec) 0.935 0.876-0.966 1.487 ±2.914 4.122 6.435 17.838 -12.865 9.997
Sit-to-walkmetrics
Sit-to-walkduration(sec) 0.431 -0.079-0.701 0.346 ±0.679 0.960 15.908 44.138 -0.900 0.858
Peaksit-to-walkvelocity(deg/sec) 0.674 0.382-0.828 12.923 ±25.330 35.821 15.819 43.848 -38.700 50.025
Gaitmetrics
Gaitcadence(steps/min) 0.985 0.971-0.992 0.487 ±0.955 1.350 0.453 1.257 -7.142 8.432
Gaitstancephase(%) 0.947 0.900-0.972 0.317 ±0.622 0.880 0.516 1.434 -3.003 2.400
Gaitlimpphase(%) 0.855 0.725-0.924 0.680 ±1.334 1.886 20.600 57.134 -4.007 2.997
Gaitvelocity(m/sec) 0.991 0.982-0.995 0.006 ±0.011 0.016 0.470 1.302 -0.114 0.126
Gaitstridelength(m) 0.994 0.989-0.997 0.003 ±0.006 0.009 0.220 0.659 -0.077 0.083
Gaitpeakswingvelocity(deg/sec) 0.988 0.977-0.993 1.618 ±3.172 4.486 0.466 1.293 -28.105 29.807
Gaitasymmetry 0.963 0.930-0.981 0.666 ±1.305 1.846 6.777 18.783 -7.617 5.951
Turningmetrics
Turningduration(sec) 0.985 0.972-0.992 0.064 ±0.126 0.178 1.914 5.323 -1.209 0.845
Peakturningvelocity(deg/sec) 0.905 0.820-0.950 8.057 ±15.791 22.332 5.502 15.251 -48.866 53.599
Turn-to-sitmetrics
Turn-to-sitduration(sec) 0.951 0.908-0.974 0.242 ±0.474 0.670 5.549 15.363 -2.200 2.079
Peakturn-to-sitvelocity(deg/sec) 0.862 0.739-0.928 6.461 ±12.664 17.909 7.109 19.706 -29.150 39.030
ICC1,k,intraclasscorrelationcoefficient(one-wayanalysis);CI95%,confidenceinterval95%;SEM,standarderrorofmeasurement;SDD,smallestdetectabledifference;LALB,limitsofagreementlowerboundary;LAUB,limitsofagreementupperboundary.

79
Figure5.1:BlandandAltmanplotofiTUGtotalduration.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.2:BlandandAltmanplotofsit-to-walkduration.Closedcircles=strokepatients,opencircles=healthyelderly.

80
Figure5.3:BlandandAltmanplotofsit-to-walkvelocity.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.4:BlandandAltmanplotofgaitcadence(notnormalizeddata).Closedcircles=strokepatients,opencircles=healthy
elderly.

81
Figure5.5:BlandandAltmanplotofgaitstancephase.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.6:BlandandAltmanplotofgaitlimpphase.Closedcircles=strokepatients,opencircles=healthyelderly.

82
Figure5.7:BlandandAltmanplotofgaitvelocity(notnormalizeddata).Closedcircles=strokepatients,opencircles=healthy
elderly.
Figure5.8: BlandandAltmanplotof gait stride length (notnormalizeddata). Closed circles = strokepatients, open circles =
healthyelderly.

83
Figure5.9:BlandandAltmanplotofgaitpeakswingvelocity.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.10:BlandandAltmanplotofgaitasymmetry.Closedcircles=strokepatients,opencircles=healthyelderly.

84
Figure5.11:BlandandAltmanplotofturningduration.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.12:BlandandAltmanplotofpeakturningvelocity.Closedcircles=strokepatients,opencircles=healthyelderly.

85
Figure5.13:BlandandAltmanplotofturn-to-sitduration.Closedcircles=strokepatients,opencircles=healthyelderly.
Figure5.14:BlandandAltmanplotofpeakturn-to-sitvelocity.Closedcircles=strokepatients,opencircles=healthyelderly.

86
Table5.4:ReliabilityoftheiTUGmetricsbasedonthestrokepatients.
iTUGmetrics ICC1,k CI95%forICC1,k SEM CI95%forSEM SDD SEM% SDD% LALB LAUB
Gaitmetrics
Gaitcadence(steps/min) 0.983 0.948-0.994 0.488 ±0.957 1.354 0.512 1.421 -3.603 11.081
Gaitstancephase(%) 0.958 0.873-0.986 0.327 ±0.641 0.907 0.522 1.448 -4.198 2.059
Gaitvelocity(m/sec) 0.985 0.955-0.995 0.007 ±0.014 0.020 0.746 2.131 -0.057 0.173
Gaitstridelength(m) 0.991 0.973-0.997 0.005 ±0.011 0.015 0.431 1.292 -0.087 0.136
Gaitasymmetry 0.981 0.942-0.994 0.464 ±0.910 1.285 2.701 7.481 -6.810 6.078
ICC1,k,intraclasscorrelationcoefficient(one-wayanalysis);CI95%,confidenceinterval95%;SEM,standarderrorofmeasurement;SDD,smallestdetectabledifference;LALB,limitsofagreementlowerboundary;LAUB,limitsofagreementupperboundary.

87
Validity
TheresultsofthevalidityanalysisarepresentedinTable5.5.Consideringthetotaltimedurationneeded
foriTUGcompletion,therewasastatisticallysignificantdifferencebetweenthetwogroups.Thestroke
patientsrequiredmoretimetocompetetheiTUGtestcomparedtotheage-matchedhealthycontrols.
Among the 13 computed iTUG subcomponent parameters, eight showed significant between-group
differences.
5.4Discussion
Thisstudywasperformedtoanalyzeinertialsensor-basediTUGmetricsregarding1)test-retestreliability
inagroupcomposedof strokepatientsandhealthyelderlyand2) theability todiscriminatebetween
individualswithstrokeandage-matchedhealthycontrols.Thepresentstudyrevealedthatallbuttwoof
thecomputediTUGmetricsreachedICCsabove0.75,whichindicatesexcellentrelativereliability.Both
variablesthatdidnotachieveexcellentrelativereliabilityvalueswererelatedtotheiTUGsubcomponent
‘sit-to-walk’.ComparableresultsfoundinthisstudywerereportedbySalarianetal.[18],whoperformed
the inertialsensor-based iTUG inpatientssufferingPDandhealthyparticipants.Three,outof the four
major iTUGsubcomponents ‘sit-to-stand’, ‘steady-stategait’, ‘turning’and‘turn-to-sit’showedgoodto
excellentreliabilityformostoftheircontributingmetrics[18].Inlinewithourfindings,theparameters
‘cadence’ and ‘stance phase’ have pointed out as one of the most reliable iTUG variables with ICCs
greaterthan0.90.Regardingthesubcomponents‘turning’and‘turn-to-sit’,therewasconsensusthatthe
parameter‘duration’seemstobethemostreliable.Moreover,inaccordancetoourstudy,Salarianetal.
[18]revealedthesit-to-standsubcomponentasleastreliablepartoftheiTUGtest.
BesidehighICCs,ameasurementtoolshouldexhibitsmallmeasurementerrorsandbeabletoidentify
realchangesinthegroupandinsingleindividuals[37].Theabsolutereliabilityanalysisperformedinthis
study corroborates the good relative reliability of the inertial sensor-based iTUGmetrics. Specifically,
small SEMand SEM%values togetherwith small SDDand SDD%valueswere found in 11of the total
computed14iTUGparameters.Thoselowvaluesindicategoodprecisionofthemeasurementtool.
Exceptforafewoutliers,mostofthedifferencevaluesbetweenthetworepeatedmeasurementswere
lyingwithinthe95%LOAintheBlandandAltmanplotsandwerewelldistributedaroundzero(dashed
zero line in Figures 5.1-5.14) demonstrating good agreement between the data of repeated
measurements(Figures5.1-5.14).

88
Table5.5:DifferencesbetweenthegroupsfortheiTUGmetrics.
iTUGmetrics Strokepatients Healthyelderly Meandiff±SD CI95%formeandiff p-value r-value
iTUGtotalduration(sec) 27.66±12.73 18.19±1.84 9.477±11.860 1.941-17.013 0.002a 0.577b
Sit-to-walkmetrics
Sit-to-walkduration(sec) 2.17±0.47 2.10±0.29 0.073±0.570 -0.289-0.435 0.945 0.021
Peaksit-to-walkvelocity(deg/sec) 69.77±26.48 97.81±20.33 28.043±34.812 5.925-50.162 0.018a 0.414c
Gaitmetrics
Gaitcadence(steps/min) 54.6±10.9 68.9±7.4 14.278±12.801 6.144-22.411 0.005a 0.544b
Gaitstancephase(%) 62.20±4.19 61.01±1.39 1.187±4.809 -1.868-4.243 0.850 0.048
Gaitlimpphase(%) 3.64±2.87 2.80±1.86 0.841±3.981 -1.689-3.370 0.850 0.048
Gaitvelocity(m/sec) 0.57±0.17 0.85±0.06 0.282±0.192 0.160-0.404 0.001a 0.609b
Gaitstridelength(m) 0.69±0.16 0.88±0.05 0.187±0.184 0.070-0.303 0.002a 0.577b
Gaitpeakswingvelocity(deg/sec) 297.56±59.24 391.38±34.43 93.824±80.058 42.957-144.690 0.001a 0.609b
Gaitasymmetry 15.60±11.28 6.42±3.39 9.179±13.655 0.503-17.854 0.092 0.352c
Turningmetrics
Turningduration(sec) 5.15±2.83 2.16±0.35 2.994±2.776 1.230-4.757 <0.001a 0.624b
Peakturningvelocity(deg/sec) 95.34±24.47 180.13±28.44 84.788±36.971 61.297-108.278 <0.001a 0.852b
Turn-to-sitmetrics
Turn-to-sitduration(sec) 5.98±3.63 3.17±1.19 2.812±2.758 1.060-4.564 <0.001a 0.625b
Peakturn-to-sitvelocity(deg/sec) 97.51±36.81 88.71±19.42 8.804±37.729 -15.168-32.776 0.733 0.080
p-valueforbetween-groupscomparison,aSignificantbetween-groupdifferences(pbetween≤0.05)calculatedwithpairedt-testandWilcoxonsigned-ranktest.
r-value,effectsize,calculatedaccordingtor=Z/√Nandr=t2/(t2+df),r=0.1:smalleffect,cr=0.3:mediumeffect,br=0.5:largeeffect.Meandiff,meandifference=(meanofthegroupwiththehighervalue)-(meanofthegroupwiththelowervalue);SD,standarddeviationofthedifference;CI95%,confidence
interval95%.

89
Onaverage thepatients improvedbetween the firstand the secondmeasurement (BlandandAltman
plots in Figures 5.1-5.14). This is likely a learning effect between the first and secondmeasurement.
Performinganinitialtesttrialpriortotheactualmeasurementmayhavepreventedthislearningeffect.
Several studies described the typical ‘hemiplegic gait’ post-stroke with a decreased walking velocity,
cadence and stride length [1-3, 5, 8]. Moreover, an increase in stance phase duration and left-right
asymmetryseemstobeacharacteristicfeatureofstrokepatients’gait[1-3,9].Accordingly,inthisstudy,
those five iTUG metrics were highlighted by a separate reliability analysis where the group ‘stroke
patients’wereseparated fromthehealthyelderlycontrols (Table5.4).Thesubanalysis showedsimilar
relative test-retest reliabilityvaluesas found in theentirestudypopulation.Specifically,excellent ICCs
above 0.75 were achieved. Furthermore, all five iTUGmetrics in the subanalysis demonstrated good
absolute test-retest reliability expressedby small SEMand SEM%values togetherwith small SDDand
SDD% values. These findings warrant further investigations of the iTUG in larger samples of stroke
survivorsand,thus,furtherexploringtheclinicalrelevanceofthesystem.
In clinical settings, theassessmentofmobility andbalance in stroke survivors is important for several
reasons; e.g., to accurately perform a diagnosis, to plan the treatment method for each individual
patientandtoadequatelyevaluatetherehabilitationeffectiveness.The iTUGsystemhasthepotential
forplayingan importantrole inprovidingclinicallyuseful informationbyobjectivelyassessingastroke
patient’sbalanceandmobility.Thishighlightsitspotentialrelevanceforapplicationinclinicalpractice.
Outofthe14analyzediTUGmetrics,nineshowedasignificantdifferencebetweenstrokepatientsand
healthy controls (Table 5.5). Among the variableswhichwere significantly different between the two
groups,alldemonstratedhigheffectsizevaluescloseto0.50andlarger.Incontrast,smallereffectsizes
rangingfrom0.021to0.352weremeasuredforthosefiveparameterswhichdidnotdifferbetweenthe
twogroups.Specifically,therewerenosignificantdifferencesinthedurationrequiredforcompletingthe
iTUGsubcomponent‘sit-to-walk’,inthepercentagevaluesrelatedto‘stancephase’and‘limpphase’of
gait cycle timeduring steady-state gait, in the left-right gait asymmetry, and in themaximumangular
trunkvelocityduringturn-to-sittransition.
Frompreviousstudieswehave indicationthatstroke leads towalking-andbalance-related limitations
and negatively affects patients’ functional mobility. Research by Ng and Hui-Chan [15] indicates that
therewasasignificantdifferencebetweenchronicstrokepatientsandhealthyelderlyofthedurationit
tookforTUGtestperformance.Inlinewithourstudy,thestrokepatientsneededmoretimetofinishthe

90
TUG procedure. Furthermore, significant higher values forwalking speed, cadence and step length in
favorofthehealthyindividualswerefound.Regardingthevariable‘stancetime’,NgandHui-Chan[15]
revealedadiscrepancybetweenthetwogroups,butonlywhentheoutcomebasedonstrokepatients’
unaffected side was considered. In our study, no separate body-side related analysis was done and,
therefore, no specific information regarding the paretic and non-paretic side available. Hence, we
recommendthatthisshouldbepartoffuturestudies.OlneyandRichards[38]statedanincreaseofthe
stance phase proportion within the gait cycle in stroke patients. In the present study, however, no
significant difference was found between stroke patients and age-matched healthy controls. The
inconsistencybetweenthestudiesmayberelatedtodifferencesinstrokecharacteristicsandseverity.
Gait symmetry represents an indicator of normalwalking [39]. Since stroke often results in unilateral
symptomscontralateraltotheinfarct,normalizationofgaitsymmetrymaybeanindicatorforrecovery
of gait. For gait symmetry evaluation, variousmetrics can be considered. According to literature, the
most common symmetrymetrics used for gait assessment are swing time, single support time, pelvic
and/or trunkmovement, and ground reaction forces [39-40]. Patterson et al. [40] concluded that the
parameter ‘swing time’ is suitable to analyze gait symmetry post-stroke and, therefore, highly
recommended.Hence,thisstudyfocusedonthegaitvariable‘swingphase’forsymmetrymeasure.Our
resultsofthegaitsymmetryevaluationare,however,atoddswiththefindingsrevealedbyPattersonet
al.[40].Pattersonetal.[40]reportedamoreasymmetricgaitpatterninstrokepatientswhencompared
with healthy individuals. In the current study, no significant asymmetry difference was found.
Nonetheless, the effect size for gait asymmetry exceeded the 0.30 level and showed, consequently, a
mediumeffect.Onepossible reason for thismightbetherathersmall sampleofstrokesurvivorswith
insufficient between-subjects variance. Future studies should, therefore, repeat our study design in
largersamplesofstrokepatientsindifferentpost-strokerecoveryphases.
Another interesting parameter to be considered for gait analysis of stroke patients is arm swing.
Indicationexiststhattheasymmetriesfrequentlyseen ingaitparameterspost-strokealsoaffectupper
body movements resulting in asymmetric arm swing patterns [41]. The hemiparetic gait of stroke
patientsisoftenassociatedwithanadductedarmwithnoorlimitedarmswingontheaffectedside.A
normalizationofthearmswingontheaffectedsidemightbeaparameterforrecoveryofnormalgait.
Zampierietal.[19]identifiedtheiTUGparameter‘peakarmswingvelocity’asoneofthemostsensitive

91
deficits inearlyPD. Itmightbethattheparameter ‘armswing’ isalsoofclinicalrelevancepost-stroke.
Futureresearchiswarrantedthatincludesarmswingparametersasoutcomevariable.
5.5Limitations
Somelimitationsofthisstudyshouldbeconsidered.Afirstlimitationisthelackofdetailedinformation
regardingtheseverity,typeandanatomical lesionlocation(s)ofthestroke.Furtherstudiesareneeded
thatfocusonspecificsubgroupsinthestrokepopulation(e.g.,sub-acuteorchronicpatients,first-everor
recurrent stroke) to substantiate our findings of the inertial sensor-based iTUG application in clinical
settings. Moreover, the pertinence of using elderly to test the iTUG may be questioned. However,
untrainedelderlynormallyshowbothbalanceandgaitimpairments[42-46],whichshouldrenderthem
anadequatepopulation forassessing reliabilityaswell. Thegenderdistribution inour samplemaybe
anotherlimitationwithadifferencebetweenthestrokepatientsandtheage-matchedhealthycontrols
withrespecttosex:Allthestrokepatientsweremaleswhereasonlythreeof12healthycontrolswere
males. This may be a source of bias confounding the results. Furthermore, sex disparity in stroke
prevalencepersistswithwomenbeingmoreaffected thenmen [47]making it important toespecially
test reliability inwomen in futurestudies.A further limitationof this study is thesmall sample size in
relationtoreliabilitystudies.Anadequatesamplesizefortheassessmentoftheagreementparameter,
basedonageneral guidelinebyAltman [48], is lyingaroundat least50. The sample sizeof14 stroke
survivors and 25 healthy elderly individuals we used is, however, a realistic group size to find first
estimates for theassumedrelationbetweenstrokeandfunctionally importanttasksasmeasuredwith
the iTUG and results in preliminary data as a basis for further examinations including larger samples.
Furthermore,thereliabilitysubanalysishastobeinterpretedwithcaution:Otherthanthedatausedfor
the primary reliability analysis based on the entire study population, the subanalysis data were not
checkedforheteroscedasticity.
5.6Conclusion
Excellenttest-retestreliabilitywasfoundformostoftheiTUGmetricsmeasuredandtheinertialsensor-
basediTUGisabletodistinguishstrokepatientsfromhealthycontrols.Thesefindingssuggestthatthe
inertialsensor-basediTUGmeasuresareusefultoassessfunctionalmobilityinstrokepatients.However,
thestudyshouldberepeatedwithalargergroupofpatientstoinvestigateitsdiscriminatorycapabilities
betweendifferentsubgroupsofstrokepatients.

92
Authors’contributions
SWcontributed to the conceptionof thework, to theacquisition, analysis and interpretationofdata,
andtowritingthemanuscript.FMcontributedtothedevelopmentoftheiTUGsoftware,assistedinthe
acquisitionandanalysisofdata.KAcontributedtotheconceptionoftheworkandthedevelopmentof
theiTUGsoftware.RGassistedintheacquisitionandanalysisofdataintheclinicalsettingandcritically
revisedthemanuscript.EDdBinitiatedthestudy,assistedintheacquisitionofdata,andcontributedto
writingandcriticallyrevisingthemanuscript.Allauthorsreadandapprovedthefinalmanuscript.
Acknowledgments
This work was partially supported by the REWIRE project (www.rewire-project.eu), funded by the
European Commission under the FP7 frameworkwith contract 287713.We thank Prof. Dr.med. Jürg
Kesselring,GabrielaWyttenbachandSusanneMüller,ClinicsofValens,forsupportwithorganizationand
recruitingofpatients.
Conflictofintereststatement
Theauthorsdeclarethattheyhavenocompetingfinancialinterests.

93
References
1. HornbyTG,StraubeDS,KinnairdCR,HolleranCL,EchauzAJ,RodriguezKS,WagnerEJ,NarducciEA.
Importanceofspecificity,amount,andintensityoflocomotortrainingtoimproveambulatoryfunctionin
patientspoststroke.TopStrokeRehabil.2011;18(4):293-307.
2. DicksteinR,DunskyA,MarcovitzE.Motorimageryforgaitrehabilitationinpost-strokehemiparesis.Phys
Ther.2004;84(12):1167-77.
3. HsuAL,TangPF,JanMH.Analysisofimpairmentsinfluencinggaitvelocityandasymmetryofhemiplegic
patientsaftermildtomoderatestroke.ArchPhysMedRehabil.2003;84(8):1185-93.
4. PuhU,BaerGD.Acomparisonoftreadmillwalkingandovergroundwalkinginindependentlyambulant
strokepatients:apilotstudy.DisabilRehabil.2009;31(3):202-10.
5. vonSchroederHP,CouttsRD,LydenPD,BillingsE,Jr.,NickelVL.Gaitparametersfollowingstroke:a
practicalassessment.JRehabilResDev.1995;32(1):25-31.
6. ChenG,PattenC,KothariDH,ZajacFE.Gaitdeviationsassociatedwithpost-strokehemiparesis:
improvementduringtreadmillwalkingusingweightsupport,speed,supportstiffness,andhandrailhold.
GaitPosture.2005;22(1):57-62.
7. BoudarhamJ,RocheN,PradonD,BonnyaudC,BensmailD,ZoryR.Variationsinkinematicsduringclinical
gaitanalysisinstrokepatients.PLoSOne.2013;8(6).
8. LennonS.Gaitre-educationbasedontheBobathconceptintwopatientswithhemiplegiafollowing
stroke.PhysTher.2001;81(3):924-35.
9. DietzV.Quadrupedalcoordinationofbipedalgait:implicationsformovementdisorders.JNeurol.
2011;258(8):1406-12.
10. BarrecaS,SigouinCS,LambertC,AnsleyB.Effectsofextratrainingontheabilityofstrokesurvivorsto
performanindependentsit-to-stand:arandomizedcontrolledtrial.JGeriatrPhysTher.2004;27(2):59-64.
11. AdaL,WestwoodP.Akinematicanalysisofrecoveryoftheabilitytostandupfollowingstroke.AustJ
Physiother.1992;38(2):135-42.
12. CameronDM,BohannonRW,GarrettGE,OwenSV,CameronDA.Physicalimpairmentsrelatedtokinetic
energyduringsit-to-standandcurb-climbingfollowingstroke.ClinBiomech(Bristol,Avon).
2003;18(4):332-40.
13. WüestS,vandeLangenbergR,deBruinED.Designconsiderationsforatheory-drivenexergame-based
rehabilitationprogramtoimprovewalkingofpersonswithstroke.EurRevAgingPhysAct.2014;11(2):119-
29.
14. SibleyKM,StrausSE,InnessEL,SalbachNM,JaglalSB.Balanceassessmentpracticesanduseof
standardizedbalancemeasuresamongOntariophysicaltherapists.PhysTher.2011;91(11):1583-91.
15. NgSS,Hui-ChanCW.Thetimedup&gotest:itsreliabilityandassociationwithlower-limbimpairments
andlocomotorcapacitiesinpeoplewithchronicstroke.ArchPhysMedRehabil.2005;86(8):1641-7.
16. KitsosG,HarrisD,PollackM,HubbardIJ.AssessmentsinAustralianstrokerehabilitationunits:a
systematicreviewofthepost-strokevalidityofthemostfrequentlyused.DisabilRehabil.2011;33(25-
26):2620-32.
17. FariaCD,Teixeira-SalmelaLF,NadeauS.Predictinglevelsofbasicfunctionalmobility,asassessedbythe
Timed"UpandGo"test,forindividualswithstroke:discriminantanalyses.DisabilRehabil.2013;35(2):146-
52.
18. SalarianA,HorakFB,ZampieriC,Carlson-KuhtaP,NuttJG,AminianK.iTUG,asensitiveandreliable
measureofmobility.IEEETransNeuralSystRehabilEng.2010;18(3):303-10.
19. ZampieriC,SalarianA,Carlson-KuhtaP,AminianK,NuttJG,HorakFB.Theinstrumentedtimedupandgo
test:potentialoutcomemeasurefordiseasemodifyingtherapiesinParkinson'sdisease.JNeurol
NeurosurgPsychiatry.2010;81(2):171-6.
20. VernonS,PatersonK,BowerK,McGinleyJ,MillerK,PuaYH,ClarkRA.QuantifyingIndividualComponents
oftheTimedUpandGoUsingtheKinectinPeopleLivingWithStroke.NeurorehabilNeuralRepair.2014.
21. deBruinED,HartmannA,UebelhartD,MurerK,ZijlstraW.Wearablesystemsformonitoringmobility-
relatedactivitiesinolderpeople:asystematicreview.ClinRehabil.2008;22(10-11):878-95.

94
22. AlletL,KnolsRH,ShiratoK,deBruinED.Wearablesystemsformonitoringmobility-relatedactivitiesin
chronicdisease:asystematicreview.Sensors(Basel).2010;10(10):9026-52.
23. HartmannA,KnolsR,MurerK,deBruinED.Reproducibilityofanisokineticstrength-testingprotocolofthe
kneeandankleinolderadults.Gerontology.2009;55(3):259-68.
24. deBruinED,HubliM,HoferP,WolfP,MurerK,ZijlstraW.Validityandreliabilityofaccelerometer-based
gaitassessmentinpatientswithdiabetesonchallengingsurfaces.JAgingRes.2012;2012:954378.
25. SoleG,HamrenJ,MilosavljevicS,NicholsonH,SullivanSJ.Test-retestreliabilityofisokineticknee
extensionandflexion.ArchPhysMedRehabil.2007;88(5):626-31.
26. deBruinED,RozendalRH,StussiE.Reliabilityofphase-velocitymeasurementsoftibialbone.PhysTher.
1998;78(11):1166-74.
27. FerrarisF,GrimaldiU,ParvisM.Procedureforeffortlessin-fieldcalibrationofthree-axialrategyroand
accelerometers.SensorsandMaterials.1995;7(5):311-30.
28. AminianK,NajafiB,BulaC,LeyvrazPF,RobertP.Spatio-temporalparametersofgaitmeasuredbyan
ambulatorysystemusingminiaturegyroscopes.JBiomech.2002;35(5):689-99.
29. SalarianA,RussmannH,VingerhoetsFJ,DehollainC,BlancY,BurkhardPR,AminianK.Gaitassessmentin
Parkinson'sdisease:towardanambulatorysystemforlong-termmonitoring.IEEETransBiomedEng.
2004;51(8):1434-43.
30. AtkinsonG,NevillAM.Statisticalmethodsforassessingmeasurementerror(reliability)invariables
relevanttosportsmedicine.SportsMed.1998;26(4):217-38.
31. HuangSL,HsiehCL,WuRM,TaiCH,LinCH,LuWS.Minimaldetectablechangeofthetimed"up&go"test
andthedynamicgaitindexinpeoplewithParkinsondisease.PhysTher.2011;91(1):114-21.
32. ShroutPE,FleissJL.Intraclasscorrelations:usesinassessingraterreliability.PsycholBull.1979;86(2):420-
8.
33. EuserAM,DekkerFW,leCessieS.ApracticalapproachtoBland-Altmanplotsandvariationcoefficientsfor
logtransformedvariables.JClinEpidemiol.2008;61(10):978-82.
34. AgebergE,BennellKL,HuntMA,SimicM,RoosEM,CreabyMW.Validityandinter-raterreliabilityof
medio-lateralkneemotionobservedduringasingle-limbminisquat.BMCMusculoskeletDisord.
2010;11:265.
35. FieldA.DiscoveringstatisticsusingSPSS.London:SagePublications;2009.
36. SendenR,MeijerK,HeyligersIC,SavelbergHH,GrimmB.Importanceofcorrectingforindividual
differencesintheclinicaldiagnosisofgaitdisorders.Physiotherapy.2012;98(4):320-4.
37. HadzicV,UrsejE,KalcM,DervisevicE.Reproducibilityofshouldershortrangeofmotioninisokineticand
isometricstrengthtesting.JExercSciFit.2012;10(2):83-9.
38. OlneySJ,RichardsC.Hemipareticgaitfollowingstroke.PartI:characteristics.GaitPosture.1996;4(2):136-
48.
39. Hodt-BillingtonC.Measuresofsymmetryingait.Methodologicalprinciplesandclinicalchoices[PhD
thesis]:UniversityofBergen;2012.
40. PattersonKK,GageWH,BrooksD,BlackSE,McIlroyWE.Evaluationofgaitsymmetryafterstroke:a
comparisonofcurrentmethodsandrecommendationsforstandardization.GaitPosture.2010;31(2):241-
6.
41. Hodt-BillingtonC,HelbostadJL,Moe-NilssenR.Shouldtrunkmovementorfootfallparametersquantify
gaitasymmetryinchronicstrokepatients?GaitPosture.2008;27(4):552-8.
42. BohannonRW.Comfortableandmaximumwalkingspeedofadultsaged20-79years:referencevaluesand
determinants.AgeAgeing.1997;26(1):15-9.
43. ChettaA,ZaniniA,PisiG,AielloM,TzaniP,NeriM,OlivieriD.Referencevaluesforthe6-minwalktestin
healthysubjects20-50yearsold.RespirMed.2006;100(9):1573-8.
44. deBruinED,vanHetReveE,MurerK.Arandomizedcontrolledpilotstudyassessingthefeasibilityof
combinedmotor-cognitivetraininganditseffectongaitcharacteristicsintheelderly.ClinRehabil.
2013;27(3):215-25.
45. TroostersT,GosselinkR,DecramerM.Sixminutewalkingdistanceinhealthyelderlysubjects.EurRespirJ.
1999;14(2):270-4.

95
46. WinterDA,PatlaAE,FrankJS,WaltSE.Biomechanicalwalkingpatternchangesinthefitandhealthy
elderly.PhysTher.1990;70(6):340-7.
47. TowfighiA,MarkovicD,OvbiageleB.PersistentsexdisparityinmidlifestrokeprevalenceintheUnited
States.CerebrovascDis.2011;31(4):322-8.
48. AltmanDG.Practicalstatisticsformedicalresearch.London:ChapmanandHall;1991.

96
6
Epilogue

97
Thenumberofstrokepatientsincreasesyearafteryear[1].Moreover,thereisanincreasedawareness
that stroke patients benefit strongly from a rehabilitation program that well exceeds the critical first
threemonthsafterstroke[2].Clearly,theneedforalong-termapproachtostrokerehabilitationforan
ever larger number of stroke patients cannot be realized by cost-intensive inpatient care alone.
Autonomous home-based rehabilitation programs are required. Interactive rehabilitation games
representapromisingtooltosupportintensiveandprolongedhome-basedstrokerehabilitation.
Accordingly, the overarching theme of this doctoral thesis was home-based long-term stroke
rehabilitationusingrehabilitationgamesspecificallydesignedforthispurpose.First,thisthesisdescribed
the Intelligent Game Engine for Rehabilitation (IGER) – a game engine designed for building
rehabilitation games that are functional, accessible and entertaining. Second, it discussed the two-
dimensional taxonomy framework suggested by Gentile as a template for providing beneficial virtual
reality(VR)-basedrehabilitationcircumstancesinaccordancewithestablishedmotorlearningprinciples.
Third,itpresentedaninterventionstudyfollowingauser-centeredinteractiondesignmethodology.This
study assessed the usability and effects of a 12-week rehabilitation program based on the newly
developedrehabilitationgamesandorganizedaccordingGentile’staxonomy.
In order to quantify intervention effects, a reliable method for measuring stroke victims’ physical
functioningisneeded.Tothisend,thisthesisevaluatedaninstrumentedversionoftheTimedUpandGo
test(TUG)abbreviatedas iTUG.Specifically, itwasevaluatedwhetherthe iTUGusingwearable inertial
sensorsrepresentsareliableandvalidassessmenttoolformobilitydeficitdetectionpost-stroke.
Inthisepilogue,Iwill(1)detailthemainfindingsofthethesis(2)outlinemethodologicalissuesand(3)
providedirectionsforfutureresearch.
6.1.Computational intelligenceandgamedesign foreffectiveat-homestroke rehabilitation
(Chapter2)
VR technique was hypothesized to offer a broad spectrum of advantages for providing beneficial
treatment conditions in clinical practice. It is not surprising, therefore, that interactive videogames
availablefortheentertainmentmarketfoundtheirwayintothefieldofhealthcareandinfluencedthe
directionofresearchinthisarea.However,todate,themajorityofgamesappliedinhealthcarelacked
the features needed to support rehabilitation at home. In our view, the following features must be
ensured:First,a flexibleadaptationof thegamechallenge levelaccording topatient’sactual statusof
functional abilities is required. A proper level of exercise difficulty ensures that the rehabilitation

98
exerciseisneitherperceivedastooeasyandboringnorastoodifficultandfrustrating.Thishelpstokeep
individuals’trainingmotivationhigh.Second,continuousmonitoringofthepatientisneededtobeable
tocorrectharmfulpostureandbadmovements.Third,andrelated,giventheabsenceofcliniciansand
therapistsinpatients’homeenvironments,automaticreal-timepatientfeedbackisofgreatimportance.
The patient can then be warned upon incorrectmovement execution or gameplay, thereby ensuring
patientsafety.Moreover,thefeedbackfeaturecanalsoserveasamotivationaltool.
Inordertoachievepleasurablegameplayexperiences,itisimportanttoexplicitlyconsidergamedesign
principles widely applied in games developed for the leisure industry. Three such principles are
meaningfulplay, flowtheoryandsenseofpresence.Theprincipleofmeaningfulplayreferstothe link
betweenaplayer’sparticularactionanditsconsequenceswithinthegame.Byprovidingdirectandclear
feedback,thislinkisensuredandtheplayerunderstandsthegame’sinternallogicandfeelsincontrolof
gameevents[3].Furthermore,accordingtothetheoryofflow,ithasbeenfoundthatbyappropriately
adaptingthechallengeandcomplexityofavideogametoapatient’scognitiveandphysicalcapabilities,
theplayerwillachieveahigh levelof focusandfeel trulypresent inthevirtualworld.Thiscouldeven
reach a stage in which patients forget that they are performing therapeutic exercises [4].Moreover,
thereisevidencethattheplayer’srealbodymovementsshouldbetrackedandintegratedinthegamein
real time; i.e., well-synchronized with the game’s virtual environment. Thereby, the player gets an
enhanced sense of autonomy and regards him- or herself as being the actor [5]. We assume that
rehabilitation games that meet these requirements are more successful at motivating patients for
treatmentpracticethanthosewhodonot.
In order to optimize home-based rehabilitation, games should not be treated as stand-alone
components. There is a need for overarching system architecture to connect relevant parties
contributing to successful rehabilitation outcomes. Specifically, the rehabilitation games must be
integratedintoabroaderstructurecomprisedofpatients,rehabilitationspecialists,hospitalsandhealth
providers.WithintheREWIREproject,threemaincomponentsmakeupamulti-layeredstructure:(1)the
patientstation(PS),(2)thehospitalstation(HS)and(3)thenetworkingstation(NS).ThePS–installedin
thepatient’shome–includesfourmodulesthatenablethefollowingtasks:hospitalcommunicationfor
downloadinggameconfigurations,datacollectionofpatients’dailylifeactivities,patientcommunityfor
interactingwithpeersandguidanceof the rehabilitationprocessbasedon the IGER.The IGER system
represents the core component of the PS allowing game configurability and flexibility, feedback
realization, real-time adaptation andmonitoring [4]. Its functioning is based on a game engine and a
game control unit. TheHS – conceived as aweb application – is a therapymanagement tool used at

99
hospital. Itgeneratesavirtualcommunitybetweenpersonsinvolvedintherehabilitationprocess(e.g.,
patients,therapists,clinicians)tosupportpatients’therapypractice.Additionally,theHSenablesinsight
intopatients’rehabilitationoutcomesaswellasthespecificationandmonitoringoftreatmentsessions.
TheNS– installed at a regional level at thehealthprovider site – is responsible for datamining. This
stationrevealsfeaturesandtrendsofrehabilitationtreatmentandallowsacomparisonof,e.g.,different
hospitals,geographicregionsandsocio-economicgroupings.
The structure and characteristics described here are likely to ensure a motivating, safe and well-
supervisedrehabilitationenvironmentandhencerender long-termhome-basedrehabilitationfeasible.
However, a set of targeted videogames embedded in overarching system architecture – although
necessary – is not yet sufficient for providing a comprehensive approach to rehabilitation. The
videogames must be embedded in a structured, theory-based therapy program so that continuous
progressacrossallrelevantdimensionsofmotorfunctionisensured.
6.2. Design considerations for a theory-driven exergame-based rehabilitation program to
improvewalkingofpersonswithstroke(Chapter3)
Inthecontextofthisdoctoralthesis,Gentile’staxonomywasconsideredasatherapyprogramtemplate.
Chapter 3 explained how Gentile’s taxonomy constitutes a practical template, which allows the
development of a therapy program according to the motor learning principles variable practice and
progression. Concretely, based on a 4x4-table (see Table 3.1, Chapter 3), 16 different categories to
classify motor skills are characterized. Each skill category is defined by unique features through two
general dimensions (i.e.,environmental contextandaction function).Due to thepositioningof the16
skillcategorieswithinthetaxonomy,asystematicprogressionintaskdifficultycouldbeperformedina
structured and simplemanner. Gentile’s taxonomy allows VR rehabilitation scenarios to be efficiently
created.Sincethebeginningofthe1990s,evidencehasaccumulatedthatvirtualenvironmentsareable
tofacilitatetheacquisitionofmotorskills[6].Consequently,VRhasbeguntobeappliedasapotential
tool for motor rehabilitation. A key advantage of this technology is the possibility of tailoring the
environmental conditions for therapy purposes. Furthermore, numerous studies emphasize that VR
provides engaging treatment situations and, thereby, enhances patients’motivation for rehabilitation
practice. This, in turn, might lead to better clinical outcomes [7]. Accordingly, we developed six
exergames and used them to create 16 virtual rehabilitation scenarios organized in accordance with
Gentile’staxonomy.

100
The16 scenariosorganized thusaccommodate thedescriptionof seven levelsof taskdifficulty,which
areorderedalongthediagonalofthe4x4-taxonomy(seeTable3.3,Chapter3).Basedonthisstructure,
wepresentedaformalprocedurefordefiningmeaningfultherapyplans.Concretely,rehabilitationstarts
with skill category 1A in the upper left corner of the taxonomy, which represents difficulty level 1.
Difficulty may be increased either by a vertical shift to the adjacent row (skill category 1B), or a
horizontal shift to the adjacent column (skill category 2A). Hence, skill categories 1B and 2A together
formdifficultylevel2.Fromeitherofthetwoskillcategoriesindifficultylevel2,wecanobtaindifficulty
level3byagainshiftingeitherhorizontallyorvertically.Whencontinuingthisprocess,weendupinskill
category 4D,which represents the seventh and final difficulty level in the taxonomy. Importantly, the
procedureproposed isnot limitedtoskillcategory-basedshifts inonlyonedirectionyet involvesboth
horizontal and vertical shifts and hence a modification of both environmental context and action
function. Additionally, persons involved in the therapy may freely choose the order in which skill
categoriesinthesamedifficultylevelaretraversed,thusallowingthetherapyprogramtobetweakedto
each patient’s individual rehabilitation requirements. Due to these advantages, Gentile’s taxonomy
constitutes a valuable template for the systematic development of coherent VR-based rehabilitation
programs to improvepost-strokemotor deficits. Future exploratory studies are neededwith focus on
usabilityandfeasibilityofrehabilitationinterventionsbasedonGentile’staxonomyusingVR.
6.3.Usabilityandeffectsofanexergame-basedbalancetrainingprogram(Chapter4)
Hemiparesis isregardedasamajor impairmentofstrokepatientswhichresults inanimpairedwalking
patternanddiminishedbalanceskills.Intactwalkingabilitiesare,however,centralforthepreservation
of autonomousmobility and the achievement of a high quality of life [8]. Intensive therapy sessions
performedrepeatedlyoveraprolongedperiodoftimehavebeenproventoguaranteeagood levelof
motor recovery post-stroke [9]. Previous studies were able to demonstrate that one of the best
predictors of successful rehabilitation outcome was a high level of motivation. High motivation
corresponds to high adherence and low attrition and contributes to optimal functional recovery from
stroke[10].Unfortunately,however,strokepatientsoftenperceivetherapeutic interventionsbasedon
usualrehabilitationexercisesasmonotonousandboringandtheirmotivationforrehabilitationpractice
is correspondingly low. Because VR represents a promising tool for turning boring rehabilitation
exercises intoentertainingones,videogamescouldbeagoodtooltopromote long-termrehabilitation
viaincreasedmotivation.

101
With this in mind, we designed an intervention program based on a set of five rehabilitation games
designedwithintheREWIREproject.Theprogramaimedtoreducestroke-inducedwalkingandbalance
impairments.Chapter4reportsapilotprojectinwhichtheprogramisappliedinhealthyelderly.Inline
with the phased iterative approach proposed by Campbell et al. [11], the pilot project represents a
discrete exploratory phase, which is to be followed by a prospective study with stroke patients.
Specifically,thepilotprojectfocusedonusabilityandeffectivenessoftheexergame-basedprogram.The
trainingsessionswereperformedthreesessionsperweekfor12weeksforagrandtotalof36sessions.
Thirteenofthe16enrolledparticipantscompletedthestudyintervention(18.8percentattrition)witha
remarkableadherencerateof100percent.Furthermore,basedonparticipants’feedback,ahighlevelof
trainingtechnologyacceptancewasexpressedand fewmodificationsof therehabilitationgameswere
suggested.After the intervention, no significant changeswere found in center of pressure (COP) area
duringquitestanceandinwalkingparameters.However,theBergBalanceScale(p=0.007;r=0.51),the
7-mTimedUpandGotest(p=0.002;r=0.56)andtheShortPhysicalPerformanceBattery(p=0.013;r=
0.48)showedsignificant improvementwithmoderateto largeeffectsizes.Obviously,thestudyresults
suggest that theexergame-based interventionwasperceivedasusableandable to influencegait-and
balance-relatedphysicalperformancemeasurespositively.Innextresearchsteps,itwouldbeinteresting
toevaluatetheinterventionpresentedhereonstrokesurvivors,firstperformedinclinicalsettingsand
thereafterinpatients’homes.
6.4.Reliabilityandvalidityofthe inertialsensor-basedTimedUpandGotest inpost-stroke
individuals(Chapter5)
For evaluating and tailoring a stroke treatment program to the patients’ specific requirements, an
accurateassessmentofphysicalfunctioningisofgreatrelevance.TheinstrumentedversionoftheTUG
based on wearable inertial sensors resulted in improved discriminative capabilities for balance and
mobility evaluation compared to the original test protocol [12]. Yet the iTUG has only been used –
invariablywith positive results – in healthy elderly andpatientswith Parkinson’s disease (PD).Hence,
althoughvalidityandreliabilityhaveneverbeentestedinstrokepatients,itcanbehypothesizedthatthe
iTUGmightalsobeausefultoolfortestingbalanceandmobilitylimitationsinthispopulation.
ThestudypresentedinChapter5analyzediTUG-basedgaitandtransitionmetricsintermsoftest-retest
reliabilityanditsabilitytodiscriminatebetweenindividualswithstrokeandage-matchedhealthyelderly
controls. To investigate test-retest reliability, a repeated-measures designwas used composedof two

102
measurementsessionswitha15-minutebreakinbetween.Withineachmeasurementsession,theiTUG
was repeated three times with a 30-second break in between. One observer tested a mixed study
population including both stroke patients (n = 14) and healthy elderly (n = 25). To examine the
discriminatory capabilities of the iTUGmetrics, an age-matched group of 12 patients and 12 healthy
individualswascreatedbyrandomselection.
Thefollowing14iTUGmetricswereanalyzed:iTUGtotalduration,sit-to-walkduration,peaksit-to-walk
velocity,gaitcadence,gaitstancephase,gaitlimpphase,gaitvelocity,gaitstridelength,gaitpeakswing
velocity,gaitasymmetry,turningduration,peakturningvelocity,turn-to-sitdurationandpeakturn-to-sit
velocity. The sit-to-walkmetrics ‘duration’ and ‘peak sit-to-walk velocity’ showed fair to good relative
test-retest reliability; all othermetrics showedexcellent relative reliability. Thehigh relative reliability
wascorroboratedbysmall‘standarderrorofmeasurement’and‘smallestdetectabledifference’values
found in11outof 14 iTUGmetrics.Additionally, the iTUGparameterswere revealed tobe in a good
agreement inBlandandAltmanplots,withmostof thedata lyingcloseto themeandifferencewithin
narrow limits of agreement. The analysis of validity indicates that the inertial sensor-based iTUG
represents a valid assessment method allowing a distinction between stroke patients and healthy
elderly.Concretely,outofthe14analyzed iTUGmetrics,nineshowedasignificantdifferencebetween
the two groups with large effect sizes. A future study could use a pre- and post-design to explore
whether the iTUG represents a valuable tool for efficacy assessment of home-based stroke
rehabilitation.
6.5.Methodologicalissues
Theresultsofthestudiesreportedinthisdoctoralthesis(Chapters2-5)shouldbeinterpretedwithinthe
contextofthemethodologicallimitationsoutlinedbelow.
Thisthesisshowsastrongfocusonbalanceandlargelydisregardstheimportanceofmuscularstrength.
Previous stroke studies have shown that – besides balancedeficits –muscleweakness seems to be a
relevantcontributing factor for impairedwalking function[13-14].Muscleweakness is recognizedasa
frequent negative consequence of stroke and as a limiting factor of gait performance [13, 15-16].
Therefore, the ideal stroke rehabilitation intervention should include strength training in addition to
balancetraining.
Inadditiontothemotordeficitsthatarethemainfocusofthisthesis,cognitivedeficits,whichnegatively
affect both independence and quality of life [17-18], are also common after stroke. Although no

103
generalizedandunitaryprofileofcognitiveproblemsafterstrokecurrentlyexists,itisnowthoughtthat
stroke often has a great negative impact on patients’ executive functioning [17-19]. Executive
functioningstandsforcognitiveabilitiesassociatedwithgoal-directedself-regulatorybehaviorincluding
response inhibition, planning,workingmemory, task switching, and attention. Earlier studies highlight
that executive functioning is related towalking performance in bothhealthy and cognitively impaired
older adults and in patients suffering from neurological diseases (e.g., stroke) [20-21]. A substantial
literaturedemonstratespositiveeffectsoncognitive functioningpost-strokecausedbyan intervention
program that emphasized various aspects of executive functions (e.g., planning, strategy, decision-
making, and learning) besides physical and social activities [19]. Obviously, a rehabilitation program
includinganenrichedenvironmentandafocusonbothphysicalactivitiesandexecutivefunctioningmay
effectively promote bothmotor performance and brain function [22]. Based onmy own experiences
withVRgatheredduring theREWIREproject,VRhasgreatpotential to theseconditionsandhence to
effectively promote both cognitive andmotor functioning. However, inmy view, the current REWIRE
rehabilitation games, with their strong focus on balance, should be developed further in order to
become more cognitively challenging. Specifically, structured cognitive stimuli such as response
inhibition, attention,dual tasksanddecision-makingopportunities shouldbe included in the future to
moreeffectivelytrainexecutivefunctioningand,hence,moreeffectivelyimprovewalkingperformance.
The study presented in Chapter 4 aimed at the improvement of individuals’ balance and walking
competency. The intervention was based on a set of five rehabilitation games which required, for
successfulgame-playing,postural controlandstabilitywhile standingonaCOPsensing forceplatform
(i.e., Tymo plate by Tyromotion, Graz, Austria [23]). Interestingly, the intervention did not result in
significant changesofwalkingparameters.As I alreadynotedpreviously, it iswell established that, in
ordertosuccessfullymasteramotorskill(e.g.,walking),task-specificpracticeisparamount[24].Hence,
steppingexercisesmighthavebeenmoreeffectiveforimprovingwalkingfunctionthanexerciseswitha
stationary base of support. Unfortunately, stepping movements cannot be performed safely in the
existingsetup,sincetheTymoplatformistoosmall(32x51cm).Anotherinteractingdeviceisrequiredif
steppingistobeincludedingameplay.TheMicrosoftKinect(Microsoft,Redmond,WA)motionsensing
camera[25]–acommerciallyavailablebodymotiontrackingdevice–maybesuchadevice.Inmyview,
stroke rehabilitation guided by Gentile’s taxonomy should harness the advantages of both the Tymo
plateandadeviceliketheMicrosoftKinect:When,accordingtothetaxonomy,anexerciserequiresbody
stability,usingtheTymoplate ispreferableas itprovides informationaboutpatients’COPmovements
(andhence their stability),even ifboth feetare stationary.Whenbody transport is required,walking-

104
related stepping movements should be performed and tracked by using a device like the Microsoft
Kinect.
6.6.Clinicalimplicationsandfuturedirections
The fundamental idea of the REWIRE project and likewise of this doctoral thesis is to develop an
innovative VR-based rehabilitation platform, which allows patients to continue intensive home
rehabilitation under remote monitoring after being discharged from hospital. Such a home-based
rehabilitationapproachisrequiredbecause,asthenumberofstrokevictimscontinuestoincrease,the
cost-intensiverehabilitationservicesinspecializedstrokeunitsorhospitalswillposeaneverincreasing
burdentotheNationalHealthService.Therefore,there isapressuretoshortenthedurationofstroke
rehabilitationinspecializedcentersandreplaceitbymorecost-extensive–yeteffective–home-based
rehabilitation. The recently launched Tymo force plate and Microsoft Kinect camera open new
possibilities for providing this important service.Given the low cost and small footprint of suchnovel
typesofhardware,theyhavethepotentialtoofferstrokepatientsahighlymotivatingandcustomizable
VR-basedrehabilitationprogramwithinthecomfortsoftheirownhomes.Withthesystemarchitecture
developed in theREWIREproject (i.e., thePS, theHSandtheNS;seeChapter2) thepatient isalways
undersupervisionbycliniciansandconnectedwithotherpatients.Hence,professionalsupervisionand
customizationoftherehabilitationprocess,positivepeerpressureandasenseofcommunitycombineto
createanoptimalrehabilitationenvironment.ParticularlythepositiveeffectsofbothVRandthesense
of community on motivation might be crucial. After all, for best recovery results, discharged stroke
patients should practice rehabilitation exercises on a regular basis formanymonths on end,which is
well-nighimpossiblewithoutmotivatingexercisesandthepresenceofacommunityofpeers.Thehigh
acceptance towards the REWIRE rehabilitation games presented in Chapter 4 shows that the newly
developedgamesare indeedmotivating.Thispositiveresultwarrantsasubsequentclinicalexplorative
studyusingthisinterventionapproachwithactualstrokepatients.
Inourstudyonlyfivebalancegameswereused.Thissetofexercisesshouldbeexpandedtoincludethe
aforementioned strength and cognitive elements. It might even be a good idea to generate a set of
gamesthatallowsthedevelopmentof twoparallel taxonomies:one focusingonbalance,andanother
focusing on muscular strength. All exercises – and hence both taxonomies – should include a
pronouncedcognitiveelementtoprovideamultifacetedcomplexchallengethatwillnotonlychallenge
balanceorstrength,butalsopatients’executivefunctioning.

105
In further clinical trials, I also recommend using the iTUG to replace the traditional TUG test for the
objective assessment of motor functions. The iTUG provides a more comprehensive insight into the
effectsofatraininginterventiontoimprovegaitandmobility.ThestudyofferedinChapter5usedagait
analysis system for iTUG metrics assessment based on eight inertial sensors. However, for clinical
practice, a smaller number of sensors is preferable, if this does not significantly affectsmeasurement
accuracy.Asmallernumberofsensorswouldreducethetimeneededtoattachthesensorsandreduce
thesystem’sweighttherebyenhancingwearingcomfort.Basedonpreviousstudies[26-31],Iproposesix
inertial sensors located as follows: One sensor on each wrist (to assess upper limbmovement), one
sensoroneachtibiaplatemid-shank(toassessgaitpattern),onesensoronthemid-thoracicspine(to
assessbodyposture)andonesensoronthesacrum(i.e.,nearthecenterofmass,toaccuratelyassess
balance). This proposal for a reduced number of sensors for the iTUG should be tested in future
experiments.Aiming thedevelopmentof instrumentedassessmentprocedures that canbeperformed
independentlyatpatients’homes,reducingthenumberofsensorsmightbeofgreatrelevance.Onecan
assumethatonlyasystemdesignedforeasyself-applicationavoidsfrustrationinducedbytheinability
touse it.Furthereffort shouldbedirectedtowardsusabilityevaluationof the independentuseof the
iTUGbypatients.
Inanextresearchstep,theeffectoftheexergame-basedinterventiononpatients’physicalfunctioning
shouldbeanalyzed.Beforeconcludingthattheinterventiontrulyrepresentsatherapeuticadvance,an
RCT including stroke patients should ideally be performed. The proposed study would compare two
groups: one experimental group, which performs the game intervention in addition to conventional
physicaltherapyandonecontrolgroup,whichonlyperformsconventionalphysicaltherapyforatotalof
36 training sessions. The main outcome measures would be pre- and post-test results of relevant
walking-relatedparameters.

106
References
1. GiannakourisK.AgingcharacterizesthedemographicperspectiveintheEuropeansocieties.Eurostat,
Statisticsinfocus.2008;72:1-12.
2. HendricksHT,vanLimbeekJ,GeurtsAC,ZwartsMJ.Motorrecoveryafterstroke:asystematicreviewof
theliterature.ArchPhysMedRehabil.2002;83(11):1629-37.
3. BorgheseNA,PirovanoM,MainettiR,LanziPL,editors.Anintegratedlow-costsystemforat-home
rehabilitation.18thInternationalConferenceonVirtualSystemsandMultimedia(VSMM);2012:IEEE.
4. BorgheseNA,MurrayD,Paraschiv-IonescuA,deBruinED,BulgheroniM,SteblinA,LuftA,ParraC.
Rehabilitationathome:acomprehensivetechnologicalapproach.Virtual,augmentedrealityandserious
gamesforhealthcare1:Springer;2014.p.289-319.
5. SlaterM,SpanlangB,Sanchez-VivesMV,BlankeO.Firstpersonexperienceofbodytransferinvirtual
reality.PloSOne.2010;5(5):e10564.
6. BarzilayO,WolfA.Adaptiverehabilitationgames.JElectromyogrKinesiol.2013;23(1):182-9.
7. BrütschK,SchulerT,KoenigA,ZimmerliL,Mérillat(-Koeneke)S,LünenburgerL,RienerR,JänckeL,Meyer-
HeimA.Influenceofvirtualrealitysoccergameonwalkingperformanceinroboticassistedgaittrainingfor
children.JNeuroengRehabil.2010;7:15.
8. TilsonJK,SettleSM,SullivanKJ.Applicationofevidence-basedpracticestrategies:currenttrendsin
walkingrecoveryinterventionspoststroke.TopStrokeRehabil.2008;15(3):227-46.
9. MuratoriLM,LambergEM,QuinnL,DuffSV.Applyingprinciplesofmotorlearningandcontroltoupper
extremityrehabilitation.JHandTher.2013;26:94-103.
10. LanghorneP,BernhardtJ,KwakkelG.Strokerehabilitation.Lancet.2011;377:1693-1702.
11. CampbellM,FitzpatrickR,HainesA,KinmonthAL,SandercockP,SpiegelhalterD,TyrerP.Frameworkfor
designandevaluationofcomplexinterventionstoimprovehealth.BrMedJ.2000;321(7262):694-6.
12. ZampieriC,SalarianA,Carlson-KuhtaP,AminianK,NuttJG,HorakFB.Theinstrumentedtimedupandgo
test:potentialoutcomemeasurefordiseasemodifyingtherapiesinParkinson'sdisease.JNeurol
NeurosurgPsychiatry.2010;81(2):171-6.
13. KimCM,EngJJ,MacIntyreDL,DawsonAS.Effectsofisokineticstrengthtrainingonwalkinginpersonswith
stroke:adouble-blindcontrolledpilotstudy.JStrokeCerebrovascDis.2001;10(6):265-73.
14. NakamuraR,WatanabeS,HandaT,MorohashiI.Therelationshipbetweenwalkingspeedandmuscle
strengthforkneeextensioninhemipareticstrokepatients:afollow-upstudy.TohokuJExpMed.
1988;154(2):111-3.
15. CanningCG,AdaL,O'DwyerN.Slownesstodevelopforcecontributestoweaknessafterstroke.ArchPhys
MedRehab.1999;80(1):66-70.
16. NadeauS,GravelD,ArsenaultAB,BourbonnaisD.Plantarflexorweaknessasalimitingfactorofgaitspeed
instrokesubjectsandthecompensatingroleofhipflexors.ClinBiomech.1999;14(2):125-35.
17. CummingTB,MarshallRS,LazarRM.Stroke,cognitivedeficits,andrehabilitation:stillanincomplete
picture.IntJStroke.2013;8(1):38-45.
18. NysGMS,vanZandvoortMJE,deKortPLM,JansenBPW,deHaanEHF,KappelleLJ.Cognitivedisordersin
acutestroke:prevalenceandclinicaldeterminants.CerebrovascDis.2007;23(5-6):408-16.
19. Liu-AmbroseT,EngJJ.Exercisetrainingandrecreationalactivitiestopromoteexecutivefunctionsin
chronicstroke:aproof-of-conceptstudy.JStrokeCerebrovasc.2015;24(1):130-7.
20. PersadCC,JonesJL,Ashton-MillerJA,AlexanderNB,GiordaniB.Executivefunctionandgaitinolderadults
withcognitiveimpairment.JGerontolABiolSciMedSci.2008;63(12):1350-5.
21. Yogev-SeligmannG,HausdorffJM,GiladiN.Theroleofexecutivefunctionandattentioningait.Mov
Disord.2008;23(3):329-42.
22. YanJH,ZhouCL.Effectsofmotorpracticeoncognitivedisordersinolderadults.EurRevAgingPhysAct.
2009;6(2):67-74.
23. Tyromotion[Internet].[cited201503/03/2015].Availablefrom:
http://tyromotion.com/en/products/tymo/overview.

107
24. PageSJ.Intensityversustask-specificityafterstroke:howimportantisintensity?AmJPhysMedRehab.
2003;82(9):730-2.
25. KinectforXboxOne[Internet].[cited201503/03/2015].Availablefrom:http://www.xbox.com/en-
US/xbox-one/accessories/kinect-for-xbox-one.
26. SalarianA,RussmannH,VingerhoetsFJG,BurkhardPR,AminianK.Ambulatorymonitoringofphysical
activitiesinpatientswithParkinson'sdisease.IEEETransBiomedEng.2007;54(12):2296-9.
27. ManciniM,SalarianA,Carlson-KuhtaP,ZampieriC,KingL,ChiariL,HorakFB.ISway:asensitive,validand
reliablemeasureofposturalcontrol.JNeuroengRehabil.2012;9.
28. SalarianA,HorakFB,ZampieriC,Carlson-KuhtaP,NuttJG,AminianK.iTUG,asensitiveandreliable
measureofmobility.IeeeTNeurSysReh.2010;18(3):303-10.
29. GaneaR,JeannetPY,Paraschiv-IonescuA,GoemansNM,PiotC,VandenHauweM,AminianK.Gait
assessmentinchildrenwithduchennemusculardystrophyduringlong-distancewalking.JChildNeurol.
2012;27(1):30-8.
30. AdaL,WestwoodP.Akinematicanalysisofrecoveryoftheabilitytostandupfollowingstroke.AustJ
Physiother.1992;38(2):135-42.
31. NajafiB,AminianK,LoewF,BlancY,RobertPA.Measurementofstand-sitandsit-standtransitionsusinga
miniaturegyroscopeanditsapplicationinfallriskevaluationintheelderly.IEEETransBiomedEng.
2002;49(8):843-51.

108
Summary / Zusammenfassung

109
Summary
Stroke is considered as one of themain causes of acquired adult disability. In themajority of cases,
stroke causes hemiparesis and, hence, diminished balance and walking ability. Locomotor function
deficits are often considered by stroke patients as a primary reason for decreased quality of life.
Therefore, recovery of walking is a major focus in almost all rehabilitation efforts for stroke victims.
Strokerehabilitationinhospitalsorspecializedrehabilitationunitsisexpensive.Asthenumberofstroke
patientscontinuestoincrease,thereisapressuretoreducethetreatmentdurationinspecializedstroke
facilities.Home-basedstrokerehabilitationrepresentsalesscostlyapproachand,therefore,apromising
tooltosupportrehabilitationonalong-termbasis.
Indications exist that virtual reality technology has the potential to promote motor recovery in
rehabilitation.However,videogamesthathavebeenoriginallydevelopedfortheleisureindustryarenot
optimally suited for therapeutic purposes. Specific gaming functionalities (i.e., game difficulty level
adaptation, continuousmonitoring of the patient, real-time feedback) needed for providing beneficial
rehabilitation situations for intensive home-based therapy rehabilitation are lacking. Moreover, for
creatingmotivating rehabilitationgames, it is crucial toexplicitly considergamedesignprinciples (i.e.,
meaningful play, flow theory and sense of presence). These game design principles might be largely
responsible for eliciting attractive gameplay scenarioswhich, in turn, arepresumably fundamental for
prolongedrehabilitationadherence.Allthosegamingcharacteristics,describedinmoredetailinChapter
2, are considered toprovidebeneficial andengaging rehabilitation conditions ina safeand controlled
environment.
Rehabilitationgamesmustbeembeddedinawell-elaboratedtherapyprogramsothatcontinuousmotor
functionprogressbecomespossible.However,todate,nosimpleandfeasibleconceptisavailablethat
facilitates the development of a therapy program consistent with widely accepted motor learning
principles and theories. Specifically, there is a need for an adequate template which allows the
developmentofagraduallyprogressingtherapyprogramincludingtask-specificandvariableexercises.In
thisdoctoralthesis,Gentile’staxonomy,describedinmoredetailinChapter3,wasconsideredassucha
template. It demonstrates a classification system that categorizes motor skills based on a 4x4-table
according to two basic dimensions (i.e., environmental context and action function). Concretely, 16
categories toclassifymotorskillsaredefined;eachof thosedescribedbyunique features.The16skill

110
categoriesarepositionedinsuchawaythatsevenlevelsofdifficultyaredistinguishable.Thisstructure
allows a skill category-basedprogression and challenging rehabilitation situations at anypoint in time
duringrehabilitation.
Virtual reality has been shown to be a valuable and flexible technology for tailoring rehabilitation
exercisesbasedonGentile’staxonomy.
Giventheimportanceofwalkingrecoverypost-stroke,theresearchquestiondealtwithinChapter4was
whetherthevirtualreality-basedapproachwouldbeusableandeffective in improving individuals’gait
andbalance.Inordertoprovidepreliminaryresults,apilotprojectwasappliedinhealthyelderlyandthe
usabilitytested.Thestudyincludedatri-weeklybalancetrainingprogramperformedfor12weeks.The
firstobjectiveofthestudywastodeterminetheusabilityoftheinterventionbasedonnewlydeveloped
interactiverehabilitationgames.Thefindingsrevealedahighlevelofacceptanceandagoodadherence
rate and, furthermore, that theparticipants’ perceived the virtual reality-based treatmentprogramas
usableandmotivating.Thesecondobjectivewastoevaluatetheeffectivenessoftheintervention.The
results of the pre- and post-comparisons revealed statistically significant changes in the Berg Balance
Scale, the 7-m Timed Up and Go test and the Short Physical Performance Battery. It is therefore
concluded that the virtual reality-based intervention positively influenced gait- and balance-related
physicalperformancemeasures.
For adequately evaluating the effectiveness of a rehabilitation program and tailoring the treatment
method to the patients’ individual requirements, an accurate assessment of physical functioning is of
greatimportance.ThestudypresentedinChapter5evaluatedaninstrumentedmethodoftheTimedUp
and Go test (iTUG) using inertial sensors. The purpose of this study was to estimate the test-retest
reliability andvalidityof iTUG-basedgait and transitionmetrics in strokepatientsandhealthyelderly.
The results revealed that the majority of the iTUG metrics measured showed excellent test-retest
reliability.Moreover, the iTUG has shown to be able to distinguish stroke patients from healthy age-
matchedelderlycontrols.
The present doctoral thesis emphasizes that virtual reality technology has great potential to provide
beneficial conditions for home rehabilitation. However, it is not entirely settled whether the virtual
reality-based rehabilitation approach can be practically implemented in patients’ home environments
andeasilybeusedindependentlybystroke-affectedindividuals.Furthermore,itsactualclinicaleffecton

111
motorperformance(e.g.,walking)amongstrokevictimsisstilluncertain.Theseopenquestionsprovide
anincentiveforfurtherresearchtofosterthedevelopmentofeffectiveat-homerehabilitationfollowing
stroke.

112
Zusammenfassung
Der Schlaganfall gilt als eine derHauptursachen einer erworbenenBehinderung im Erwachsenenalter.
Nach einem Schlaganfall kommt es in denmeisten Fällen zu einer Hemiparese und einhergehend zu
einer verminderten Gleichgewichts- und Gehfähigkeit. Eine beeinträchtigte Fortbewegungsfunktion
nehmen die betroffenen Menschen häufig als eine der wichtigsten Gründe für eine Einbusse an
Lebensqualität wahr. DieWiederherstellung und Verbesserung der Gehfähigkeit hat deswegen in der
SchlaganfallrehabilitationeinehohePriorität.DieRehabilitationinspezialisiertenZentrenistjedochmit
hohenBehandlungskostenverbunden.DadieZahlanSchlaganfallpatientenstetigansteigt,erhöhtsich
der Druck nach einer Einschränkung der Behandlungsdauer in spezialisierten Einrichtungen. Ein
Rehabilitationsprogramm für zu Hause stellt eine kostensparende Möglichkeit für eine Therapie auf
langfristigerBasisdar.SiegewinntdeshalbzunehmendanBedeutung.
Hinweise existieren, dass durch die Verwendung von virtueller Realität die motorische Rehabilitation
begünstigtwerdenkann.Zuanerkennen istaber,dass sichVideogamesausderUnterhaltungsbranche
für den therapeutischen Einsatz nicht optimal eignen. Es fehlt ihnen an spezifischen Eigenschaften
(Anpassung der Schwierigkeitsstufe, Monitoring des Patienten, Feedback-Funktion), um optimale
Rehabilitationsbedingungen für zu Hause zu gewährleisten. Des Weiteren ist entscheidend, dass die
Videogames nach bewährten Game-Design-Richtlinien (‚meaningful play‘, ‚flow theory‘, ‚sense of
presence‘) konzipiert sind. Es wird angenommen, dass durch die Berücksichtigung der Game-Design-
Richtlinien faszinierende Szenarien geschaffen werden, was eine langfristige Aufrechterhaltung der
Rehabilitation unterstützt. All diese Charakteristiken (beschrieben in Kapitel 2) werden als wichtig
erachtet,umförderlicheundspannendeRehabilitationsbedingungenineinersicherenundkontrollierten
Umgebungzuermöglichen.
Videogames sollen für den therapeutischen Gebrauch in ein gut ausgearbeitetes Therapieprogramm
eingebettet sein, um möglichst optimale Fortschritte zu erreichen. Bis heute konnte sich noch kein
Konzept etablieren, welches die Ausarbeitung eines Therapieprogramms – übereinstimmend mit
motorischenLernprinzipienundTheorien–unterstützt.EntsprechendisteinKonzepterwünscht,umein
progressives Rehabilitationsprogramm zu definieren, das sich durch aufgabenspezifische und variable
Übungen auszeichnet. In der vorliegenden Doktorarbeit wird Gentile’s Taxonomie (beschrieben in
Kapitel 3) als ein dafür sich eignendes Konzept beurteilt. Gentile’s Taxonomie beschreibt ein

113
Klassifikationssystem,basierendaufeiner4x4-Tabelle,ummotorischeFertigkeitenzukategorisieren.Es
werden zwei grundlegende Dimensionen berücksichtigt:Anforderungen der Umwelt und Funktion der
Aktion. Die beiden Dimensionen sind jeweils in zwei Komponenten unterteilt, so dass sich eine
Taxonomiemit 16 Kategorien ergibt. Jede dieser 16 Kategorienweist einen spezifischenmotorischen
Fertigkeitscharakter aufundgrenzt sichdadurch vondenanderenab.Die Taxonomie vermagdeshalb
variableÜbungenzubieten.DieAnordnungder16KategorienermöglichteineEinteilunggemässderer
Komplexität, woraus sieben Schwierigkeitsstufen resultieren. Es bietet sich ein strukturierter
RehabilitationsverlaufvoneinfachenzuschwierigenÜbungen.
Durch die Verwendung von virtueller Realität lassen sich Rehabilitationsübungen entsprechend der
TaxonomievonGentiledefinieren.
AngesichtsderBedeutung,dieGehfunktionvonSchlaganfallpatientenzuoptimieren,wurdeinKapitel4
die Benutzbarkeit und der Effekt eines virtuell-realitätsbasierten Rehabilitationsprogramms zur
Förderung derGleichgewichts- undGehfähigkeit untersucht. In einer Pilotstudie absolvierten gesunde
Senioren dreimal pro Woche ein Gleichgewichtstraining über eine Zeitspanne von 12 Wochen. Das
primäreZielder Studiewar,dieBenutzbarkeitder virtuell-realitätsbasierten Intervention zuermitteln,
welchedenEinsatzvonneuentwickelteninteraktivenVideogamesgewährte.DieResultatezeigteneine
hoheAkzeptanzundAdhärenz.Zudemwurdeerkannt,dassdieProbandendievirtuell-realitätsbasierte
Interventionalsbenutzbarundmotivierendbeurteilten.DesWeiterenverfolgtedieStudiedasZiel,die
Effektivitätder Interventionzuerfassen.EinPrä-undPost-VergleichergabsignifikanteVeränderungen
hinsichtlich folgenden Tests: ‚Berg Balance Scale‘, ‚7-m Timed Up and Go‘ und ‚Short Physical
Performance Battery‘. Diese Ergebnisse lassen den Schluss zu, dass die virtuell-realitätsbasierte
Intervention einen positiven Effekt auf Gleichgewichts- und Gehfähigkeits-bestimmende Parameter
bewirkt.
Die Effektivitätsbestimmung und Anpassung eines Rehabilitationsprogramms an individuelle
Erfordernisse bedarf präzise Messmethoden. In der Studie (präsentiert in Kapitel 5) wurde eine
instrumentalisierte Methode des ‚Timed Up and Go‘-Tests (iTUG) unter Verwendung von
Inertialsensoren evaluiert. Das Ziel der Studie war, die Zuverlässigkeit und die Validität von iTUG-
Parametern bei Schlaganfallpatienten und gesunden Senioren zu untersuchen. Die Ergebnisse dieser
StudieverdeutlicheneinehoheZuverlässigkeitfürdieMehrheitdererhobeneniTUG-Parameter.Zudem

114
zeigtesichderiTUGalsfähigeMethode,umSchlaganfallpatientenvongesunden,gleichaltrigenSenioren
zuunterscheiden.
DievorliegendeDoktorarbeitunterstreichtdasgrossePotential,welchesdieVerwendungvonvirtueller
RealitäthinsichtlichförderlicherMassnahmeneinerRehabilitationfürzuHauseaufweist.Esistallerdings
nochunklar,obsichdievirtuell-realitätsbasierteMethodepraktischzuHauseumsetzenlässtundsichfür
dieselbstständigeDurchführungdurchSchlaganfallpatienteneignet.ZudemistdieklinischeWirksamkeit
hinsichtlich motorischer Leistungsfähigkeiten (z.B. der Gehfähigkeit) bei Schlaganfallpatienten noch
ungewiss.DieseoffenenFragenstelleneineLegitimationfürweitereForschungdar,umdieEntwicklung
voneffektivenSchlaganfall-RehabilitationsmassnahmenfürzuHausevoranzutreiben.

115
Danksagungen
AndieserStellebenutzeichgernedieGelegenheit,michbeidenvielenMenschenzubedanken,diemich
währendderZeitmeinesDoktoratsbegleitetundunterstützthaben.
EingrosserDankgehtanmeinenDoktorvater,PDDr.ElingD.deBruin.
DubistmirinjederPhasemeinesDoktoratsstetsunterstützendzurSeitegestanden.AllunsereREWIRE-
Reisenwaren fürmich eine grosse Bereicherung;wir nutzten diese Zeit für spannendeberuflichewie
auchprivateGespräche.WährendmeinesgesamtenDoktoratsdurfteichimmerwiederaufdeinereiche
berufliche Kompetenz zählen und nebst den fachlichen Inputs auch deinen persönlichen Rückhalt
erfahren.DeinezuversichtlicheArtbewogmich immerwieder,„Stolpersteine“ ineinpositivesLichtzu
rückenunddiesealsChancezunutzen.Esfreutmich,unsereberuflicheTätigkeitfortzusetzenundauch
zukünftigmiteinanderinKontaktzubleiben.
MeinDankgiltProf.Dr.KurtMurer.
Kurt,ichdankedir,dassdumirstetseinAnsprechpartnerwarst,infachlichenwieauchinpersönlichen
Angelegenheiten. Ich schätzte deinen Freiraum, den dumir bei der Arbeit eingeräumt hast, dies liess
michimmerwiederdeinVertrauenspüren.
MeinDankgiltProf.Dr.DavidP.Wolfer.
Ichbedankemichfür Ihr InteresseanmeinerDoktorarbeitundfür IhreBereitschaftalsCo-Referentzu
fungieren.
Ein weiteres Dankeschön widme ichmeinenMitarbeiterinnen undMitarbeiter des IBWS, die meinen
täglichenAlltagbereicherten:
Eva, icherinneremichnochgut anmeinenerstenArbeitstag.DankdeinerherzlichenundoffenenArt
fühlteichmichimIBWS-Teamsofortgutaufgehoben.InzwischensindeinigeJahrevergangen,eswuchs
eineFreundschaftheran,dieichnichtmehrmissenmöchte.Ichdankedir,dassichmichaufdich–deine
Hilfe,deineUnterstützung,deinVerständnisunddeineMotivation–jederzeitverlassendurfte.Ichhätte
mirkeinwertvolleresDoktoranden-sowiedividat-„Gspändli“wünschenkönnen.AufunsereZukunft!
Rolf, ichhabeindirnichtnureinenäusserstkompetentenArbeitskollegen,sondernaucheinenFreund
gefunden. Dank unseren gemeinsamen Interessen, insbesondere aber unserer gemeinsamen Freude
über „Gott und dieWelt“ zu diskutieren, hast dumir viele bereicherndeMomente geschenkt. Deine
lehrreichen fachlichen Anregungen und deine sorgfältige Durchsicht meinerManuskript-Entwürfe mit

116
denkonstruktivenKommentaren,habenviel zumGelingenmeinerDoktorarbeitbeigetragen. Ichhabe
eineMengevondirgelernt,soauch,etwasGelassenheitzubewahren.
Brigitte,unsereJogging-Rundenbedeutetenmirsehrviel.Siegabenmirfixe,wöchentlicheZeitfenster,
auf welche ich mich immer freute. Sie boten mir Raum dir Dinge anzuvertrauen, die mich gerade
beschäftigten.DeineRatschläge,deineMeinungunddeineUnterstützungbedeutetenmirsehrviel.
Rahel,dieTageam IBWSverbrachte ichgernemitdir.DankdeinerumgänglichenundnatürlichenArt
konnten wir Wichtigkeiten und Nichtigkeiten unseres „Doktorandinnen-Alltags“ austauschen. Du
konntestmichindenrichtigenMomentenmotivieren,vielenDankdafür.
Patrick, ichgenossnichtnurdie jeweiligenWochentage,andenenwir zusammenam IBWSanwesend
waren, sondern freutemich auch immer per SMS von dir zu hören.Durch dich bin ich ein „richtiger“
Fussball-Fangeworden…vielleichtschaffenwiresja,einmalzusammeneinenMatchzubesuchen,hopp
FCL!
AndreaundGiusy,wiegernehätteichunseregemeinsameZeitamIBWSverlängert, ihrhabtmirnach
euremAbschlussgefehlt.DarankonntenichteinmaldieÜbernahmedes schönstenDoktoranden-Pult-
PlatzesmitderherrlichenAussichtaufdenKäferbergetwasändern(ichhattejaschliesslichauchkaum
Zeit, aus dem Fenster zu schauen… *hihihii*). Ich danke euch für die kurze, aber sehr schöne Zeit
zusammenamIBWS.
Alexandra,eswarschön,dichwährendden letztenMonatenmeinesDoktoratesalsPult-Nachbarinzu
haben. Ich habe dich als aufgeschlossene und unkomplizierte Person kennen gelernt, die sich nicht
einmalüberBücherundMaterialienärgerte,welchesichvonmeinerPult-Seitezudeinerdrängten.Für
deineweitereDoktorandenzeitwünscheichdirallesGuteundvielFreudeandeinerArbeit.
Andi, Federico, Franziska, Laura, Oli, Regula, Roger, Roli, Sarah, Sämi und Yvonne, ein grosses
Dankeschön gilt auch euch. Ihr habt viel zu einem harmonischen Arbeitsklima beigetragen und –
insbesonderewährend denMittagspausen – für fröhliche Stimmung gesorgt. Ich fühltemich in eurer
Gesellschaftimmerwillkommen.
DesWeiterendankeichdemgesamtendividat-Team:
Bujar, Eling, Eva,Hans, Joris undMarco, euer unermüdlicher Einsatz und Engagement für dividat ist
„Weltklasse“. IchdankefüreuergrossesVerständnisbezüglichmeinerknappenZeitressourcewährend
derFertigstellungderDoktorarbeit.Obwohl ichkaumaktiv tätigseinundmitwirkenkonnte, fühlte ich
michstetsalsTeildesTeams.EingrossesDankeschön!

117
VonganzemHerzenbedankeichmichbeimeinenwertvollstenFreunden:
Céline,Maika,RamiundSandra,ihrseid„minhellschtStärnamHimmel,minFelsideBrandig,ohniüch
fühlechmechwienesZältohniHering“.Danke,füreureeinmaligeFreundschaft.
MeineabschliessendenWortewidmeichmeinenElternEstherundGregorundmeinerSchwesterCarla.
IhrschenktmirLebensmut,LebensfreudeundLiebe–jedenTagvonNeuem.
MeinDankaneuchistgrösser,alsichauszudrückenvermag.

118
Curriculumvitae
Name SelineWüest
Dateofbirth 01-02-1985
Citizenof Grosswangen,Lucerne,Switzerland
Education
2011–2015 PhDinScienceattheInstituteofHumanMovementSciencesandSport,
ETHZurich,Switzerland
2008–2010 MasterofScienceDegreeinHumanMovementSciencesandSport,ETH
ZurichwithMajorinMotorControlandMotorLearning
2004–2008 Bachelor of Science Degree in HumanMovement Sciences and Sport,
ETHZurich
1999–2003 AcademicUpperSecondarySchool,Matura
Masterthesisandacademicinternships
11/2009–06/2010 Master thesis ETH Zurich, Switzerland [completed as an exchange
studentatCardiffUniversity,UnitedKingdom]
“Reliability and validity of a ‘Real Time Location System’ as a tool for
peoplelocatingandinactivitymeasuring”
04/2009–06/2009 Academic internship II in sports therapy at the RehabilitationHospital
Hasliberg,Switzerland
10/2008–12/2008 Academic internship I in physical activity assessment at ETH Zurich,
Switzerland